Project Management Aspects of Anterior Surgical Approach in AIS
VerifiedAdded on 2023/06/13
|57
|12942
|164
Report
AI Summary
This report investigates the application of project management principles to anterior surgical approaches in treating Adolescent Idiopathic Scoliosis (AIS). It begins by introducing AIS, its prevalence, and common surgical treatments: anterior, posterior, and thoracoscopic spinal fusion. The research aims to compare the efficacy of these surgical methods and identify project management strategies for optimizing recovery, particularly with anterior surgery. A systematic literature review was conducted to compare surgical outcomes, focusing on blood loss, pulmonary function, and recovery rates. The study highlights the benefits of anterior surgery and proposes a project management framework for its successful implementation. The report covers various aspects of project management, including stakeholder management, process groups, and knowledge areas, emphasizing the importance of a structured approach to healthcare projects. It includes a detailed comparison of posterior, thoracoscopic, and anterior surgeries, ultimately advocating for anterior surgery due to its superior outcomes when coupled with effective project management strategies. The findings aim to provide healthcare organizations with insights for improving surgical practices and resource allocation in AIS treatment. Desklib offers a range of similar solved assignments and past papers to aid students in their studies.

Running head: BIOMEDICAL ENGINEERING
Biomedical Engineering
Name of student:
Name of university:
Author note:
Biomedical Engineering
Name of student:
Name of university:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1BIOMEDICAL ENGINEERING
Abstract
Adolescence Idiopathic Scoliosis (AIS) is a multi-factorial health condition that causes almost
80% of the spine deformity among the adolescence. The main treatment options that are
available for scoliosis is observation, bracing and then surgery. The principal objective of AIS
surgery is solid fusion and proper trunk. There are three different types of solid fusion namely
anterior spinal fusion, posterior spinal fusion and thorasocopic spinal fusion, The aim of the
research is to elucidate the usefulness and efficacy of all these three forms of fusion surgeries
that are used for treating AIS. The result of this comparative study will then be utilised to frame
a proper project management framework for successful implementation of the surgical procedure
and thereby attaining success in treating AIS. In order to achieve the aims and the objectives of
the research, the researcher has followed a systematic review approach. The comparative study
revealed that anterior spine surgery is better than the other two surgeries in the domain of the
blood loss, pulmonary functions and recovery rate. Following the identification of the best spinal
surgery form, project management principal was proposed for proper implementation of the
spinal surgery techniques.
Abstract
Adolescence Idiopathic Scoliosis (AIS) is a multi-factorial health condition that causes almost
80% of the spine deformity among the adolescence. The main treatment options that are
available for scoliosis is observation, bracing and then surgery. The principal objective of AIS
surgery is solid fusion and proper trunk. There are three different types of solid fusion namely
anterior spinal fusion, posterior spinal fusion and thorasocopic spinal fusion, The aim of the
research is to elucidate the usefulness and efficacy of all these three forms of fusion surgeries
that are used for treating AIS. The result of this comparative study will then be utilised to frame
a proper project management framework for successful implementation of the surgical procedure
and thereby attaining success in treating AIS. In order to achieve the aims and the objectives of
the research, the researcher has followed a systematic review approach. The comparative study
revealed that anterior spine surgery is better than the other two surgeries in the domain of the
blood loss, pulmonary functions and recovery rate. Following the identification of the best spinal
surgery form, project management principal was proposed for proper implementation of the
spinal surgery techniques.
2BIOMEDICAL ENGINEERING
Table of Contents
Chapter 1- Introduction....................................................................................................................4
1.1 The background for the investigation....................................................................................4
1.2 Research Aim.........................................................................................................................4
1.3 Research objectives...............................................................................................................5
1.4 Research questions and the hypothesis..................................................................................5
1.5 Most commonly used surgical methods to correct AIS.........................................................5
1.6 Outcomes and results.............................................................................................................6
1.7 Significance...........................................................................................................................6
Chapter 2: Literature review............................................................................................................7
2.1 Concept of management........................................................................................................7
2.2 Project Management Theory..................................................................................................9
2.3 Literature Gap......................................................................................................................13
2.4 Summary..............................................................................................................................13
Chapter 3: Research Methodology................................................................................................15
3.1 Research philosophy............................................................................................................15
3.2 Research approach...............................................................................................................15
3.3 Research strategy.................................................................................................................15
3.3.1 Inclusion criteria...........................................................................................................16
3.3.2 Exclusion criteria..........................................................................................................16
Table of Contents
Chapter 1- Introduction....................................................................................................................4
1.1 The background for the investigation....................................................................................4
1.2 Research Aim.........................................................................................................................4
1.3 Research objectives...............................................................................................................5
1.4 Research questions and the hypothesis..................................................................................5
1.5 Most commonly used surgical methods to correct AIS.........................................................5
1.6 Outcomes and results.............................................................................................................6
1.7 Significance...........................................................................................................................6
Chapter 2: Literature review............................................................................................................7
2.1 Concept of management........................................................................................................7
2.2 Project Management Theory..................................................................................................9
2.3 Literature Gap......................................................................................................................13
2.4 Summary..............................................................................................................................13
Chapter 3: Research Methodology................................................................................................15
3.1 Research philosophy............................................................................................................15
3.2 Research approach...............................................................................................................15
3.3 Research strategy.................................................................................................................15
3.3.1 Inclusion criteria...........................................................................................................16
3.3.2 Exclusion criteria..........................................................................................................16
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3BIOMEDICAL ENGINEERING
3.4 Data collection tools............................................................................................................16
3.5 Time plan.............................................................................................................................16
3.6 Ethical Consideration...........................................................................................................17
3.7 Tasks....................................................................................................................................17
Chapter 4 Posterior spine surgery..................................................................................................18
Chapter 5 Thoracoscopic spine surgery.........................................................................................23
Chapter 6 Anterior spine surgery...................................................................................................27
Chapter 7 Detail comparison between these three surgeries (posterior, thoracoscopic surgery and
anterior)..........................................................................................................................................32
Chapter 8: Why anterior surgery is better than remaining two.....................................................37
Chapter 10: use project management principles to get quick recovery in anterior surgery compare
to remaining surgery......................................................................................................................42
Chapter 11: Recommendations and conclusion.............................................................................46
References......................................................................................................................................50
3.4 Data collection tools............................................................................................................16
3.5 Time plan.............................................................................................................................16
3.6 Ethical Consideration...........................................................................................................17
3.7 Tasks....................................................................................................................................17
Chapter 4 Posterior spine surgery..................................................................................................18
Chapter 5 Thoracoscopic spine surgery.........................................................................................23
Chapter 6 Anterior spine surgery...................................................................................................27
Chapter 7 Detail comparison between these three surgeries (posterior, thoracoscopic surgery and
anterior)..........................................................................................................................................32
Chapter 8: Why anterior surgery is better than remaining two.....................................................37
Chapter 10: use project management principles to get quick recovery in anterior surgery compare
to remaining surgery......................................................................................................................42
Chapter 11: Recommendations and conclusion.............................................................................46
References......................................................................................................................................50
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4BIOMEDICAL ENGINEERING
Topic: Investigation of project management aspects of the anterior surgical approach in
adolescence idiopathic scoliosis treatment
Chapter 1- Introduction
1.1 The background for the investigation
Scoliosis in patients aged between 10 and 18 years is known as adolescent scoliosis and the
underlying causes of the same are multi-factorial. The most commonly occurring form of
scoliosis in the adolescent period is adolescence idiopathic scoliosis (AIS), and what makes the
condition stand out from other forms of scoliosis is that that the cause of this condition remains
unknown. The condition is a three-dimensional health condition that corresponds to almost 80%
of all spine deformity cases. The prevalence of AIS is described as 2-3% on a global scale.
Around 0.5% of these cases are known to be progressive and require surgical treatment. The
symptoms of the condition do not lead to neurologic conditions. However the visible symptoms
related to the conditions are distinct (Lee et al., 2016). Treatment options to address concerns in
adolescent idiopathic scoliosis is divided into three main categories; observation, bracing and
surgery. The decision regarding treatment is based on the risk of curvature progression. The main
objective of AIS surgery is to achieve a proper trunk and solid fusion. Nevertheless, it has been
reported that though good radiological and clinical outcomes have been achieved, quality of life
for patients as determined by self-evaluation is poor (Sudo et al., 2016).
1.2 Research Aim
The first aim of the research was to comprehend the usefulness and efficacy of the three
forms of surgery, namely, anterior, posterior, and thoracic approach for treating AIS, and
undertake a comparative study of the three surgical forms. The second aim was to understand the
Topic: Investigation of project management aspects of the anterior surgical approach in
adolescence idiopathic scoliosis treatment
Chapter 1- Introduction
1.1 The background for the investigation
Scoliosis in patients aged between 10 and 18 years is known as adolescent scoliosis and the
underlying causes of the same are multi-factorial. The most commonly occurring form of
scoliosis in the adolescent period is adolescence idiopathic scoliosis (AIS), and what makes the
condition stand out from other forms of scoliosis is that that the cause of this condition remains
unknown. The condition is a three-dimensional health condition that corresponds to almost 80%
of all spine deformity cases. The prevalence of AIS is described as 2-3% on a global scale.
Around 0.5% of these cases are known to be progressive and require surgical treatment. The
symptoms of the condition do not lead to neurologic conditions. However the visible symptoms
related to the conditions are distinct (Lee et al., 2016). Treatment options to address concerns in
adolescent idiopathic scoliosis is divided into three main categories; observation, bracing and
surgery. The decision regarding treatment is based on the risk of curvature progression. The main
objective of AIS surgery is to achieve a proper trunk and solid fusion. Nevertheless, it has been
reported that though good radiological and clinical outcomes have been achieved, quality of life
for patients as determined by self-evaluation is poor (Sudo et al., 2016).
1.2 Research Aim
The first aim of the research was to comprehend the usefulness and efficacy of the three
forms of surgery, namely, anterior, posterior, and thoracic approach for treating AIS, and
undertake a comparative study of the three surgical forms. The second aim was to understand the

5BIOMEDICAL ENGINEERING
project management principles that can be applied for getting quick recovery in anterior surgery
as compared to other surgical forms.
1.3 Research objectives
To recognize the effectiveness of anterior surgical procedure for AIS
To understand the effectiveness of posterior surgical procedure for AIS
To identify the effectiveness of thoracic surgical procedure for AIS
To highlight why anterior surgery is better than remaining two
To assess the project management principles that can be applied for getting quick
recovery in anterior surgery
1.4 Research questions and the hypothesis
The research questions that was addressed through the paper are
Why anterior surgery is better than remaining two surgical forms?
What are the project management principles to get quick recovery in anterior surgery
compare to remaining surgery?
The hypothesis considered for the research was that “anterior surgery is better than
remaining two surgical forms”.
1.5 Most commonly used surgical methods to correct AIS
Surgical treatment for patients with AIS is considered for those whose curves are greater than
45 degree with continual growth in this angle. The goal of such surgery can be understood to be
two-fold. The first aim is to achieve prevention of curve progression. The second aim is to
achieve curve correction. The three commonly used surgical methods to correct AIS are as
follows-
project management principles that can be applied for getting quick recovery in anterior surgery
as compared to other surgical forms.
1.3 Research objectives
To recognize the effectiveness of anterior surgical procedure for AIS
To understand the effectiveness of posterior surgical procedure for AIS
To identify the effectiveness of thoracic surgical procedure for AIS
To highlight why anterior surgery is better than remaining two
To assess the project management principles that can be applied for getting quick
recovery in anterior surgery
1.4 Research questions and the hypothesis
The research questions that was addressed through the paper are
Why anterior surgery is better than remaining two surgical forms?
What are the project management principles to get quick recovery in anterior surgery
compare to remaining surgery?
The hypothesis considered for the research was that “anterior surgery is better than
remaining two surgical forms”.
1.5 Most commonly used surgical methods to correct AIS
Surgical treatment for patients with AIS is considered for those whose curves are greater than
45 degree with continual growth in this angle. The goal of such surgery can be understood to be
two-fold. The first aim is to achieve prevention of curve progression. The second aim is to
achieve curve correction. The three commonly used surgical methods to correct AIS are as
follows-
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6BIOMEDICAL ENGINEERING
Posterior spine surgery
Anterior spine surgery
Thoracoscopic spine surgery
1.6 Outcomes and results
The results of the study would be elementary in indicating the form of surgery that is
most appropriate for adolescence idiopathic scoliosis. Based on the research it would be easier to
understand whether anterior adolescence idiopathic scoliosis surgery is better as compared to
thoracic and posterior adolescence idiopathic scoliosis. The project management techniques that
are useful and effective in this regard would also be highlighted.
1.7 Significance
The significance of the study lies in the fact that on the basis of the results of the study
important changes can be brought about in practice of undertaking surgery for treating
adolescence idiopathic scoliosis. Healthcare organizations can consider changes in project
management practice in this regard and consider resource allocation accordingly.
Posterior spine surgery
Anterior spine surgery
Thoracoscopic spine surgery
1.6 Outcomes and results
The results of the study would be elementary in indicating the form of surgery that is
most appropriate for adolescence idiopathic scoliosis. Based on the research it would be easier to
understand whether anterior adolescence idiopathic scoliosis surgery is better as compared to
thoracic and posterior adolescence idiopathic scoliosis. The project management techniques that
are useful and effective in this regard would also be highlighted.
1.7 Significance
The significance of the study lies in the fact that on the basis of the results of the study
important changes can be brought about in practice of undertaking surgery for treating
adolescence idiopathic scoliosis. Healthcare organizations can consider changes in project
management practice in this regard and consider resource allocation accordingly.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7BIOMEDICAL ENGINEERING
Chapter 2: Literature review
2.1 Concept of management
Following a robust management method is pivotal in the successful completion of
surgery in healthcare settings. The healthcare landscape is changing in a rapid manner and an
increased focus is being given at present on access to quality care, reduction of care costs and
prevention of surgical complications. Despite immense opportunities for healthcare professionals
to engage in care techniques, varied constraints hamper progress to a considerable extent. Herein
lays the need of a strong project management strategy that involves application of suitable tools,
skills, knowledge and techniques for project activities for meeting the goal of care being
provided. Project management reflects the domains of quality, scope, integration, cost,
procurement, human resources, communications and risk management (Shirley, 2016).
Project management is referred to the practice of initiation, planning, execution, control
and closing of a work to achieve a set of goals and to meet a set of criteria within a stipulated
time. Such a management approach is needed for producing an end-result that suits the purpose
of the task being done. Healthcare practices such as surgeries are a leading domain at the
contemporary era and is growing effectively. With the shift towards need of safe practices the
need of effective management is harnessed. Cost of healthcare practices is also an issue at
present as a large number of advanced tools and aids are costly to be used at large (Ginter, 2018).
For effectively fulfilling their goals of better patient outcomes, surgeons treating
adolescence idiopathic scoliosis choose to work in teams of clinician from different fields.
Though teams augment the ability and skills of a surgeon in the care process, the added role of
addressing group workflow and managing team dynamics might pose significant challenges. For
Chapter 2: Literature review
2.1 Concept of management
Following a robust management method is pivotal in the successful completion of
surgery in healthcare settings. The healthcare landscape is changing in a rapid manner and an
increased focus is being given at present on access to quality care, reduction of care costs and
prevention of surgical complications. Despite immense opportunities for healthcare professionals
to engage in care techniques, varied constraints hamper progress to a considerable extent. Herein
lays the need of a strong project management strategy that involves application of suitable tools,
skills, knowledge and techniques for project activities for meeting the goal of care being
provided. Project management reflects the domains of quality, scope, integration, cost,
procurement, human resources, communications and risk management (Shirley, 2016).
Project management is referred to the practice of initiation, planning, execution, control
and closing of a work to achieve a set of goals and to meet a set of criteria within a stipulated
time. Such a management approach is needed for producing an end-result that suits the purpose
of the task being done. Healthcare practices such as surgeries are a leading domain at the
contemporary era and is growing effectively. With the shift towards need of safe practices the
need of effective management is harnessed. Cost of healthcare practices is also an issue at
present as a large number of advanced tools and aids are costly to be used at large (Ginter, 2018).
For effectively fulfilling their goals of better patient outcomes, surgeons treating
adolescence idiopathic scoliosis choose to work in teams of clinician from different fields.
Though teams augment the ability and skills of a surgeon in the care process, the added role of
addressing group workflow and managing team dynamics might pose significant challenges. For
8BIOMEDICAL ENGINEERING
surgeons carrying out vital surgeries, project management is a powerful tool for gaining
maximum efficiency and efficacy in the setting (Chiocchio, 2015). Whether working in teams
with professionals from different disciplines or independently, project management models can
drive success.
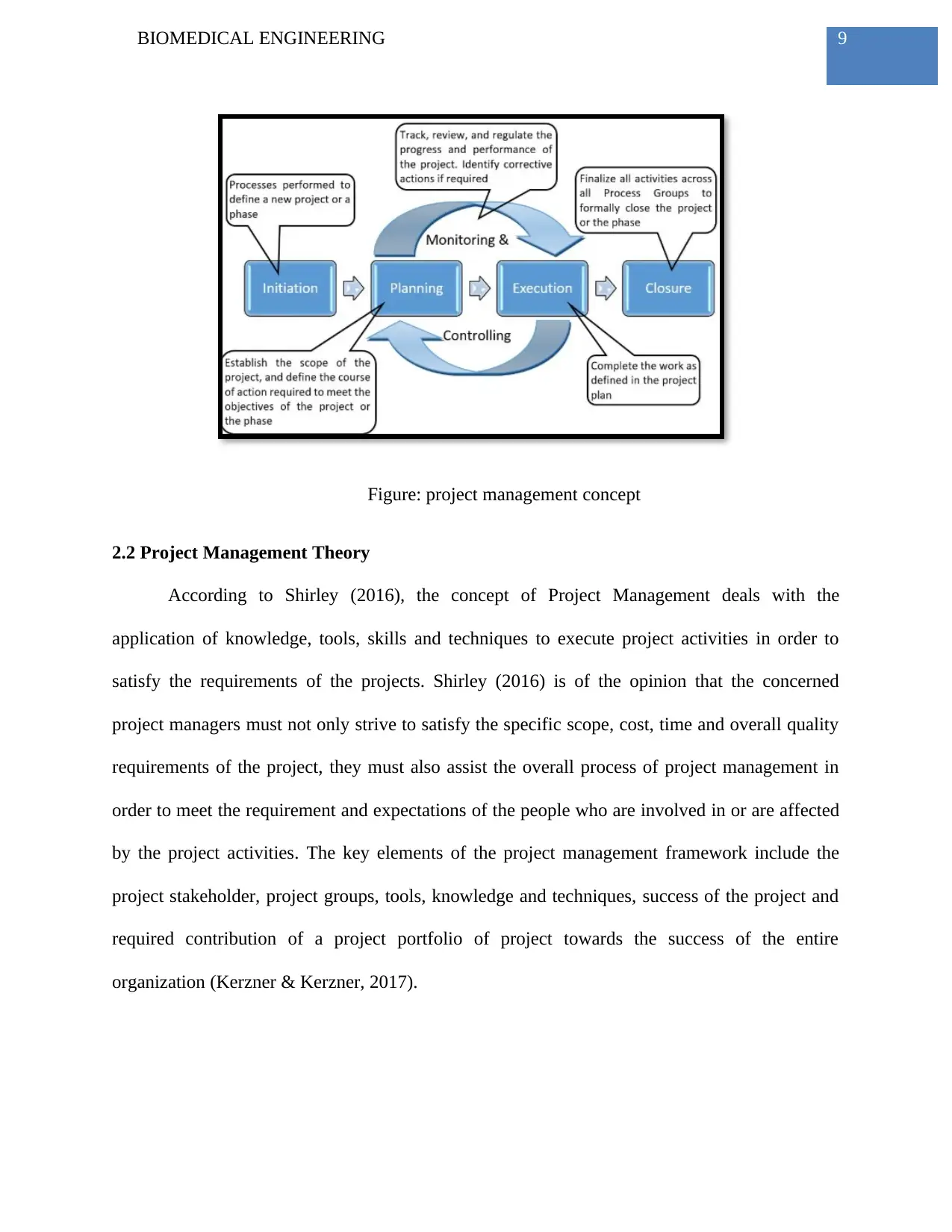
Management of healthcare projects is a challenging task as a number of roles and
responsibilities are to be fulfilled for gaining optimal results. Dividing the project into simpler
efforts is crucial for giving the project a structure and ensuring manageable steps. The five
phases of project management are project initiation; project planning; project execution project
monitoring and control; project closure. Project initiation is the initial phase considering
measurement of the feasibility and value of the project. Project planning refers to the thorough
and detailed planning that provides guidance for securing the resources. Project execution is the
key part wherein all the deliverables are fulfilled within a time frame. Monitoring of project
involves understanding the needs of further improvements. Lastly, project closure is the ending
of the project when the required task is completed. The primary challenge of application of such
project management concept in healthcare is to achieve the complete set of goals within the
constraints perceived. If the objectives and procedures of the project are ill-defined, it is likely
that there would be a detrimental effect on the decision making process (Babineau&Lessard,
2015).
surgeons carrying out vital surgeries, project management is a powerful tool for gaining
maximum efficiency and efficacy in the setting (Chiocchio, 2015). Whether working in teams
with professionals from different disciplines or independently, project management models can
drive success.
Management of healthcare projects is a challenging task as a number of roles and
responsibilities are to be fulfilled for gaining optimal results. Dividing the project into simpler
efforts is crucial for giving the project a structure and ensuring manageable steps. The five
phases of project management are project initiation; project planning; project execution project
monitoring and control; project closure. Project initiation is the initial phase considering
measurement of the feasibility and value of the project. Project planning refers to the thorough
and detailed planning that provides guidance for securing the resources. Project execution is the
key part wherein all the deliverables are fulfilled within a time frame. Monitoring of project
involves understanding the needs of further improvements. Lastly, project closure is the ending
of the project when the required task is completed. The primary challenge of application of such
project management concept in healthcare is to achieve the complete set of goals within the
constraints perceived. If the objectives and procedures of the project are ill-defined, it is likely
that there would be a detrimental effect on the decision making process (Babineau&Lessard,
2015).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9BIOMEDICAL ENGINEERING
Figure: project management concept
2.2 Project Management Theory
According to Shirley (2016), the concept of Project Management deals with the
application of knowledge, tools, skills and techniques to execute project activities in order to
satisfy the requirements of the projects. Shirley (2016) is of the opinion that the concerned
project managers must not only strive to satisfy the specific scope, cost, time and overall quality
requirements of the project, they must also assist the overall process of project management in
order to meet the requirement and expectations of the people who are involved in or are affected
by the project activities. The key elements of the project management framework include the
project stakeholder, project groups, tools, knowledge and techniques, success of the project and
required contribution of a project portfolio of project towards the success of the entire
organization (Kerzner & Kerzner, 2017).
Figure: project management concept
2.2 Project Management Theory
According to Shirley (2016), the concept of Project Management deals with the
application of knowledge, tools, skills and techniques to execute project activities in order to
satisfy the requirements of the projects. Shirley (2016) is of the opinion that the concerned
project managers must not only strive to satisfy the specific scope, cost, time and overall quality
requirements of the project, they must also assist the overall process of project management in
order to meet the requirement and expectations of the people who are involved in or are affected
by the project activities. The key elements of the project management framework include the
project stakeholder, project groups, tools, knowledge and techniques, success of the project and
required contribution of a project portfolio of project towards the success of the entire
organization (Kerzner & Kerzner, 2017).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10BIOMEDICAL ENGINEERING
Figure: Different steps of project management
(Source: Kerzner & Kerzner, 2017)
Project Stakeholders
Stakeholders: Stakeholders are the people are affected or involved by the activities of the
project and mainly involve the project sponsor, project team, support staffs, suppliers, customers
and opponents of the project. In case of the AIS and is subsequent treatment via surgery, the
main stakeholders who are involved in the project management include the sponsors of the
project that is the family members of the patients who make the complete payment for the
surgery, the patient over whom the entire procedure will be undertaken and the care givers that is
the healthcare professionals who are associated with the overall planning and the execution of
the project (Kerzner, 2018). There may or may not be opponents of the project as in this case.
Thus there are numerous stakeholders who are closely attached with the entire process of
StakeholdersneedandexpectationProjectgroupsInitiatingPlanningExecutingMonitoring/controllingClosingToolsandtechniquesProjectprotfolioEnterprisesuccess
Figure: Different steps of project management
(Source: Kerzner & Kerzner, 2017)
Project Stakeholders
Stakeholders: Stakeholders are the people are affected or involved by the activities of the
project and mainly involve the project sponsor, project team, support staffs, suppliers, customers
and opponents of the project. In case of the AIS and is subsequent treatment via surgery, the
main stakeholders who are involved in the project management include the sponsors of the
project that is the family members of the patients who make the complete payment for the
surgery, the patient over whom the entire procedure will be undertaken and the care givers that is
the healthcare professionals who are associated with the overall planning and the execution of
the project (Kerzner, 2018). There may or may not be opponents of the project as in this case.
Thus there are numerous stakeholders who are closely attached with the entire process of
StakeholdersneedandexpectationProjectgroupsInitiatingPlanningExecutingMonitoring/controllingClosingToolsandtechniquesProjectprotfolioEnterprisesuccess
11BIOMEDICAL ENGINEERING
effective treatment of adolescence idiopathic scoliosis and hence effective success of the project
of cure of the disease under the application of surgery is dependent on the expectations and needs
of the stakeholders (Kerzner, 2018). According to Kerzner (2018), a successful project manager
must develop healthy relationships with the concerned project stakeholders in order to
understand and subsequently meet the requirement of the project.
Project Management process groups and knowledge
The main five groups which are included inside the project management include
initiating, planning, execution, monitoring, controlling and proper closing of activities (Kerzner
& Kerzner, 2017). According to the theory of project management, Kerzner and Kerzner (2017)
is of the opinion that for a successful health care project, it is the duty of a health care
professional to develop key competencies towards that particular project in terms of knowledge
and theories for proper execution of the project. The main areas of knowledge and skills that a
project management managers must have as guided by the theory of project management include
1. Proper management of project integration
2. Proper management of the of the scope of the project via working with proper
stakeholders
3. Proper management of the time of the project that is how long will it take in complete
and how effective is this time in relation to the cost
4. Proper preparation and cost of the overall project
5. Proper quality management of the project
6. Proper management of the human resource associated with the project
effective treatment of adolescence idiopathic scoliosis and hence effective success of the project
of cure of the disease under the application of surgery is dependent on the expectations and needs
of the stakeholders (Kerzner, 2018). According to Kerzner (2018), a successful project manager
must develop healthy relationships with the concerned project stakeholders in order to
understand and subsequently meet the requirement of the project.
Project Management process groups and knowledge
The main five groups which are included inside the project management include
initiating, planning, execution, monitoring, controlling and proper closing of activities (Kerzner
& Kerzner, 2017). According to the theory of project management, Kerzner and Kerzner (2017)
is of the opinion that for a successful health care project, it is the duty of a health care
professional to develop key competencies towards that particular project in terms of knowledge
and theories for proper execution of the project. The main areas of knowledge and skills that a
project management managers must have as guided by the theory of project management include
1. Proper management of project integration
2. Proper management of the of the scope of the project via working with proper
stakeholders
3. Proper management of the time of the project that is how long will it take in complete
and how effective is this time in relation to the cost
4. Proper preparation and cost of the overall project
5. Proper quality management of the project
6. Proper management of the human resource associated with the project
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 57
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.