MRS432 CT Protocol Critique: Pulmonary Angiogram Analysis
VerifiedAdded on 2020/10/22
|12
|3051
|374
Report
AI Summary
This report offers a comprehensive critique of a CT protocol, specifically focusing on CT pulmonary angiogram (CTPA). It begins with an introduction to CT scans and the importance of adhering to protocols for accurate diagnosis. The report then delves into the CTPA protocol, explaining its purpose in diagnosing pulmonary embolism and its invasive nature. It discusses key elements such as contradictions, patient preparation, contrast needs, exposure risks, tube rotation time, beam collimation, reconstruction algorithms, slice thickness, patient alignment, contrast timing, scanning range, and post-processing requirements. The report highlights the importance of factors like contrast timing, radiation dose reduction techniques, and patient positioning in obtaining optimal image quality. It also addresses considerations like patient preparation, including breath-holding instructions and the removal of metallic objects. Furthermore, it examines the impact of factors like tube rotation time, beam collimation, pitch, and reconstruction algorithms on image quality and radiation dose. The report concludes by emphasizing the critical role of CT protocols in ensuring accurate diagnosis and patient safety in medical imaging.

Protocol critique
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENTS
AIM..................................................................................................................................................1
INTRODUCTION...........................................................................................................................1
PROTOCOL ...................................................................................................................................1
Contradictions and indications ....................................................................................................1
Contrast needs and room preparation .........................................................................................2
Considerations, adaptations and patient preparation ..................................................................2
Exposure risks and dose reduction ..............................................................................................3
Tube rotation time, beam collimation and pitch .........................................................................3
Windowing and reconstruction algorithm ..................................................................................3
Interval and reconstruction slice thickness .................................................................................4
Patient alignment and position ....................................................................................................4
Contrast timing and volumes ......................................................................................................4
Anatomy and scanning range ......................................................................................................5
Post processing requirements.......................................................................................................5
CONCLUSION ...............................................................................................................................5
REFERENCES ...............................................................................................................................6
AIM..................................................................................................................................................1
INTRODUCTION...........................................................................................................................1
PROTOCOL ...................................................................................................................................1
Contradictions and indications ....................................................................................................1
Contrast needs and room preparation .........................................................................................2
Considerations, adaptations and patient preparation ..................................................................2
Exposure risks and dose reduction ..............................................................................................3
Tube rotation time, beam collimation and pitch .........................................................................3
Windowing and reconstruction algorithm ..................................................................................3
Interval and reconstruction slice thickness .................................................................................4
Patient alignment and position ....................................................................................................4
Contrast timing and volumes ......................................................................................................4
Anatomy and scanning range ......................................................................................................5
Post processing requirements.......................................................................................................5
CONCLUSION ...............................................................................................................................5
REFERENCES ...............................................................................................................................6

AIM
To enhance the skills used in CT protocols development in clinical setting.
INTRODUCTION
Computed tomography is also known as CT scan and is an image test which is used for
the diagnosis of images of blood vessels, soft issues, internal organs and bones. CT provides
images in multiple planes and three dimensional images which can be analysed and shared. For
the precise diagnosis and analysis of CT it is essential for the clinicians to obey and consider
scanning instructions or the protocols (Vanier and Caplan, 2017). CT protocol describes the rules
and techniques as a reference for technologists and radiology residents. The report will discuss
the necessity and various elements of CT protocols such as its rotation time, adaptations,
scanning range and reconstruction algorithm.
PROTOCOL
CT pulmonary angiogram (CTPA) protocol explain the diagnosis principles of CT
angiography. It provides the image of pulmonary arteries for the diagnosing pulmonary
embolism (PE). It requires only intravenous line for the scanning purpose and thus is invasive in
nature. CTPA protocols assures that intravenous injection of contrast agent containing iodine is
provided to patient at high rate. As a result, images are obtained with the optimum radio opaque
contrast. In order to give the picture of blood vessels contrast dye is injected into blood vessels in
arm or groin. During the test x-ray or fluoroscopy is used to scan the dye and to generate the
image (Dekkers and et.al., 2016). When multi-detector CT scanner used for CTPA then best
results are obtained. However, it has been observed that individuals which have higher risk of
nephropahty dual energy CT can be used to lower the contrast amount. With the implications of
this protocol bolus tracking is used in the clinics or hospitals. Bolus tracking helps to commence
the scanning only when the level of contrast matches the level of pulmonary proximal.
Contradictions and indications in the scanning of blood clots in lungs
CTPA is widely used for the scanning of artery blockage in the lungs and thus for this
report lungs are scanned. CTPA scan demonstrates the mass filling defects like fat or embolus in
pulmonary vessels in the form of dark appearances. Thus, this protocol helps to diagnose the
blood clots in lungs which travels from pelvis or leg veins to cause a blockage in the flow of
blood. It is strictly ensured that scanning process must be accomplished before contrast reaches
to aorta or the left side of the heart. This protocol element is necessary as it indicates that there is
1
To enhance the skills used in CT protocols development in clinical setting.
INTRODUCTION
Computed tomography is also known as CT scan and is an image test which is used for
the diagnosis of images of blood vessels, soft issues, internal organs and bones. CT provides
images in multiple planes and three dimensional images which can be analysed and shared. For
the precise diagnosis and analysis of CT it is essential for the clinicians to obey and consider
scanning instructions or the protocols (Vanier and Caplan, 2017). CT protocol describes the rules
and techniques as a reference for technologists and radiology residents. The report will discuss
the necessity and various elements of CT protocols such as its rotation time, adaptations,
scanning range and reconstruction algorithm.
PROTOCOL
CT pulmonary angiogram (CTPA) protocol explain the diagnosis principles of CT
angiography. It provides the image of pulmonary arteries for the diagnosing pulmonary
embolism (PE). It requires only intravenous line for the scanning purpose and thus is invasive in
nature. CTPA protocols assures that intravenous injection of contrast agent containing iodine is
provided to patient at high rate. As a result, images are obtained with the optimum radio opaque
contrast. In order to give the picture of blood vessels contrast dye is injected into blood vessels in
arm or groin. During the test x-ray or fluoroscopy is used to scan the dye and to generate the
image (Dekkers and et.al., 2016). When multi-detector CT scanner used for CTPA then best
results are obtained. However, it has been observed that individuals which have higher risk of
nephropahty dual energy CT can be used to lower the contrast amount. With the implications of
this protocol bolus tracking is used in the clinics or hospitals. Bolus tracking helps to commence
the scanning only when the level of contrast matches the level of pulmonary proximal.
Contradictions and indications in the scanning of blood clots in lungs
CTPA is widely used for the scanning of artery blockage in the lungs and thus for this
report lungs are scanned. CTPA scan demonstrates the mass filling defects like fat or embolus in
pulmonary vessels in the form of dark appearances. Thus, this protocol helps to diagnose the
blood clots in lungs which travels from pelvis or leg veins to cause a blockage in the flow of
blood. It is strictly ensured that scanning process must be accomplished before contrast reaches
to aorta or the left side of the heart. This protocol element is necessary as it indicates that there is
1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

need of large contrast media dose. One of the contradiction associated with this protocol is its
usage during pregnancy (Gillespie and et.al., 2019). The ionizing radiations used in CTPA makes
it less suitable during pregnancy. During pregnancy the sensitivity of breasts increases and thus
can have adverse impact on thyroid gland of fetus.
(Source: CT angiography of the abdominal wall to study the inferior epigastric system for DIEP
flap breast reconstruction, 2011)
Contrast needs and room preparation
CTPA is carried out in radiology scanning room. The room consist of scanning table on
which patient can lay flat and head is positioned in docking pillow. The CT scanner donut is
movable and pass around patients so that scan can be completed. For creating the scan, a gantry
is also provided in the room which can travel from neck to abdomen. For the scanning and
diagnosis purpose intravenous contrast is selected. This contrast highlights and demonstrates the
pulmonary vessels
Considerations, adaptations and patient preparation
For the accurate results of CTPA timing is very critical parameter. Thus clear and
suitable instructions must be given by the radiographers to patient for holding breath as well as to
breath in and breath out. Since the test has contradictions and risks related to pregnancy it is
2
usage during pregnancy (Gillespie and et.al., 2019). The ionizing radiations used in CTPA makes
it less suitable during pregnancy. During pregnancy the sensitivity of breasts increases and thus
can have adverse impact on thyroid gland of fetus.
(Source: CT angiography of the abdominal wall to study the inferior epigastric system for DIEP
flap breast reconstruction, 2011)
Contrast needs and room preparation
CTPA is carried out in radiology scanning room. The room consist of scanning table on
which patient can lay flat and head is positioned in docking pillow. The CT scanner donut is
movable and pass around patients so that scan can be completed. For creating the scan, a gantry
is also provided in the room which can travel from neck to abdomen. For the scanning and
diagnosis purpose intravenous contrast is selected. This contrast highlights and demonstrates the
pulmonary vessels
Considerations, adaptations and patient preparation
For the accurate results of CTPA timing is very critical parameter. Thus clear and
suitable instructions must be given by the radiographers to patient for holding breath as well as to
breath in and breath out. Since the test has contradictions and risks related to pregnancy it is
2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
required that patients must informed regarding this prior to the test. From the safety purpose the
carers are not allowed to enter the scanning rooms. Metal objects and jewellery can lead to
unclear image or artefacts thus it must be assured that such objects are removed before test.
It must be assured that during the test arms are placed above head at rest so that arm
position can be maintained. The breathing instructions and patterns can also influences the
quality of images thus CTPA results can get affected (Vayntrub and et.al., 2017). The heart rate
are checked with ECG and intravenous is injected only if patient has normal heart rhythm. In
cases if heart rate is more than 60 bpm then for getting clear images beta blockers are provided to
patient. For the asthma patients few minutes before CTPA nitroglycerin is given so that arteries
can be expanded and better images are obtained.
It is recommended that before few hours of the commencement of the test patient must be
fasting and there should be no consumption of the food or water. However, after the completion
of scanning process plenty of fluids must be consumed. It is necessary as it helps to flush out the
contrast substance out-of-body. Patients must wear clothes which are comfortable and which
does not have zippers, snaps or metallic objects which can influence the scanning results. As
contrast and iodine is used thus professionals must also confirm that patient does not have
allergy from these substances (Siddiqui and et.al., 2016). For the patients suffering from diabetes
they may require stopping the consumption of some medicines before 24 hours of the test.
Another important consideration and preparation aspect is informed consent. Since CTPA
includes the use of intravenous (IV) medications which can lead to complications such as blood
clot, hematomam infiltration and several other complications. Thus, it is recommended within
protocols that patients informed consent must be taken so that such risk can be identified. The
informed consent is also requires making sure that patients are aware of radiation risk and they
provide their consent to the practitioners.
Exposure risks and dose reduction
The radiation risk is higher in pregnant woman and thus these exposure risks must be
analysed and considered. This imaging technique targets the ionizing radiations. As compare to
X-ray and other radiations used in imaging, ionizing rays are less harmful and has lower risk of
developing cancer. For CTPA accepted dosage for absorbed radiations is gray. The perfect and
safe radiation values depends upon the site of body, scanning range, thickness of slice and tube
3
carers are not allowed to enter the scanning rooms. Metal objects and jewellery can lead to
unclear image or artefacts thus it must be assured that such objects are removed before test.
It must be assured that during the test arms are placed above head at rest so that arm
position can be maintained. The breathing instructions and patterns can also influences the
quality of images thus CTPA results can get affected (Vayntrub and et.al., 2017). The heart rate
are checked with ECG and intravenous is injected only if patient has normal heart rhythm. In
cases if heart rate is more than 60 bpm then for getting clear images beta blockers are provided to
patient. For the asthma patients few minutes before CTPA nitroglycerin is given so that arteries
can be expanded and better images are obtained.
It is recommended that before few hours of the commencement of the test patient must be
fasting and there should be no consumption of the food or water. However, after the completion
of scanning process plenty of fluids must be consumed. It is necessary as it helps to flush out the
contrast substance out-of-body. Patients must wear clothes which are comfortable and which
does not have zippers, snaps or metallic objects which can influence the scanning results. As
contrast and iodine is used thus professionals must also confirm that patient does not have
allergy from these substances (Siddiqui and et.al., 2016). For the patients suffering from diabetes
they may require stopping the consumption of some medicines before 24 hours of the test.
Another important consideration and preparation aspect is informed consent. Since CTPA
includes the use of intravenous (IV) medications which can lead to complications such as blood
clot, hematomam infiltration and several other complications. Thus, it is recommended within
protocols that patients informed consent must be taken so that such risk can be identified. The
informed consent is also requires making sure that patients are aware of radiation risk and they
provide their consent to the practitioners.
Exposure risks and dose reduction
The radiation risk is higher in pregnant woman and thus these exposure risks must be
analysed and considered. This imaging technique targets the ionizing radiations. As compare to
X-ray and other radiations used in imaging, ionizing rays are less harmful and has lower risk of
developing cancer. For CTPA accepted dosage for absorbed radiations is gray. The perfect and
safe radiation values depends upon the site of body, scanning range, thickness of slice and tube
3
voltage. In order to reduce the radiation dosage in CTPA techniques such as iterative
reconstruction and kVp are used by the radiographers.
When tube voltage is lowered along with the intermediate tube current then, radiations is
lowered. Further the dose must not be too high or low instead it must be moderate so that it can
match the size of patient (Pitiyarachchi and et.al., 2019). Kvp is the primary strategy for reducing
the dosage. The variation in kVp also changes the optimum value of mA. At different values of
kV threshold value of bolus tracking is also variable. Thus, the manufacturers assure that the
scanners are properly calibrated with all clinical ranges of kVs.
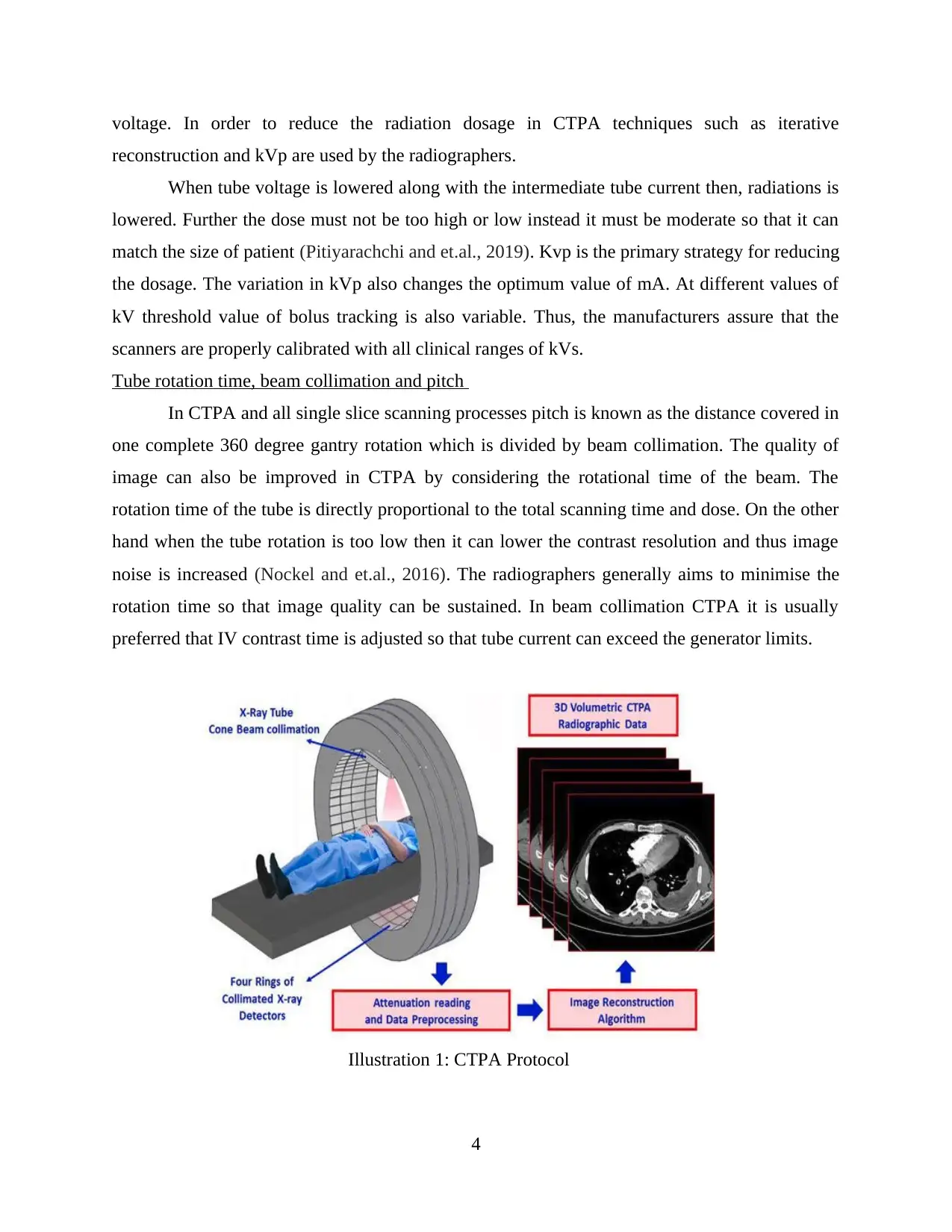
Tube rotation time, beam collimation and pitch
In CTPA and all single slice scanning processes pitch is known as the distance covered in
one complete 360 degree gantry rotation which is divided by beam collimation. The quality of
image can also be improved in CTPA by considering the rotational time of the beam. The
rotation time of the tube is directly proportional to the total scanning time and dose. On the other
hand when the tube rotation is too low then it can lower the contrast resolution and thus image
noise is increased (Nockel and et.al., 2016). The radiographers generally aims to minimise the
rotation time so that image quality can be sustained. In beam collimation CTPA it is usually
preferred that IV contrast time is adjusted so that tube current can exceed the generator limits.
4
Illustration 1: CTPA Protocol
reconstruction and kVp are used by the radiographers.
When tube voltage is lowered along with the intermediate tube current then, radiations is
lowered. Further the dose must not be too high or low instead it must be moderate so that it can
match the size of patient (Pitiyarachchi and et.al., 2019). Kvp is the primary strategy for reducing
the dosage. The variation in kVp also changes the optimum value of mA. At different values of
kV threshold value of bolus tracking is also variable. Thus, the manufacturers assure that the
scanners are properly calibrated with all clinical ranges of kVs.
Tube rotation time, beam collimation and pitch
In CTPA and all single slice scanning processes pitch is known as the distance covered in
one complete 360 degree gantry rotation which is divided by beam collimation. The quality of
image can also be improved in CTPA by considering the rotational time of the beam. The
rotation time of the tube is directly proportional to the total scanning time and dose. On the other
hand when the tube rotation is too low then it can lower the contrast resolution and thus image
noise is increased (Nockel and et.al., 2016). The radiographers generally aims to minimise the
rotation time so that image quality can be sustained. In beam collimation CTPA it is usually
preferred that IV contrast time is adjusted so that tube current can exceed the generator limits.
4
Illustration 1: CTPA Protocol
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

(Source: Computer-Aided Detection, Pulmonary Embolism, Computerized Tomography
Pulmonary Angiography: Current Status, 2018. )
Another important aspects which acts as an integral component of CTPA is the pitch.
Similar to the tube rotation the pitch also has its impact on contrast resolution, scanning time and
dosage. When the value of pitch is less than 1 then, slice thickness may increase while the higher
value of pitch needs current value to enhance the near limits.
Windowing and reconstruction algorithm
Reconstruction algorithm in CT scan process provides the tomographic image which is
obtained from the projection data acquired at multiple angles around patients. The reconstruction
algorithm has significant impact upon radiation dose and quality of image. This algorithm is
based upon iterative approach and thus initial guesses plays an important role for making the
further repetitive decisions.
5
Pulmonary Angiography: Current Status, 2018. )
Another important aspects which acts as an integral component of CTPA is the pitch.
Similar to the tube rotation the pitch also has its impact on contrast resolution, scanning time and
dosage. When the value of pitch is less than 1 then, slice thickness may increase while the higher
value of pitch needs current value to enhance the near limits.
Windowing and reconstruction algorithm
Reconstruction algorithm in CT scan process provides the tomographic image which is
obtained from the projection data acquired at multiple angles around patients. The reconstruction
algorithm has significant impact upon radiation dose and quality of image. This algorithm is
based upon iterative approach and thus initial guesses plays an important role for making the
further repetitive decisions.
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

(Source:Super-resolution CT Image Reconstruction Based on Dictionary Learning and Sparse
Representation, 2018.)
The window level in CTPA is known as the central point of CT numbers range. For
increasing the brightness of the scanned image window level is reduced while the increase in
window level can lower the image brightness. Windowing also enable radiographers to select
any specific segment from the total pixel range of dynamic receptors (Mokadam and et.al.,
2019). These receptors are then demonstrated with the pixel value in the range of gray shade
from white to black. The reprocessing using various types of Kernel does not include any dose
cost and can have wide differences in obvious to subtle differences.
Interval and reconstruction slice thickness
In CTPA helical scanning is performed with multiple detector rows. The scanning time of
the image can be reduced by around one tenth with this technique. Slice thickness is defined as
the axial resolution of the scanning and thus its increment refers to the motion of scanner to next
scanning slice. It may vary from 1 mm to 4 mm. When slice thickness is increased then, it leads
to increase the image noise. As a result the diagnosis content of the image is also affected
6
Illustration 1: Reconstruction algorithm
Representation, 2018.)
The window level in CTPA is known as the central point of CT numbers range. For
increasing the brightness of the scanned image window level is reduced while the increase in
window level can lower the image brightness. Windowing also enable radiographers to select
any specific segment from the total pixel range of dynamic receptors (Mokadam and et.al.,
2019). These receptors are then demonstrated with the pixel value in the range of gray shade
from white to black. The reprocessing using various types of Kernel does not include any dose
cost and can have wide differences in obvious to subtle differences.
Interval and reconstruction slice thickness
In CTPA helical scanning is performed with multiple detector rows. The scanning time of
the image can be reduced by around one tenth with this technique. Slice thickness is defined as
the axial resolution of the scanning and thus its increment refers to the motion of scanner to next
scanning slice. It may vary from 1 mm to 4 mm. When slice thickness is increased then, it leads
to increase the image noise. As a result the diagnosis content of the image is also affected
6
Illustration 1: Reconstruction algorithm
adversely. Contrary to this the reduction in slice thickness allows distinction of lesions and thus
partial volume effects are also decreased. When the slice thickness is in the range 3 to 6 mm then
images noises are identical while the slice thickness of 3 mm can be considered as the best
choice for the image processing.
Patient alignment and position
During the scanning process the patient must lie straight on and their hands are positioned
in a firm condition above the head. The supine position is helpful in obtaining multiple scanning
and to have detailed observation of the required body organ. In order to maintain the correct
position strips and pillows are also used so that correct alignment can be established between
patient and screen.
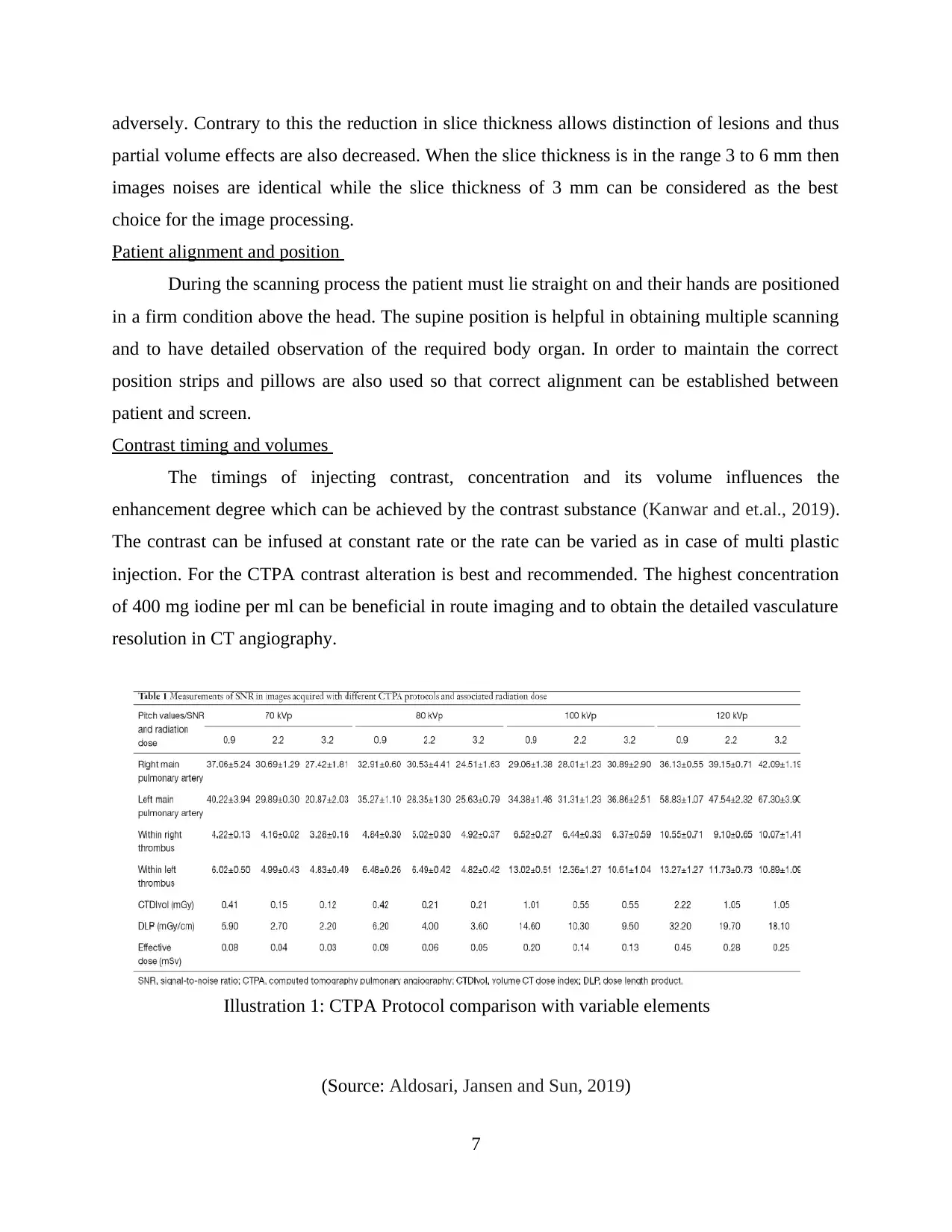
Contrast timing and volumes
The timings of injecting contrast, concentration and its volume influences the
enhancement degree which can be achieved by the contrast substance (Kanwar and et.al., 2019).
The contrast can be infused at constant rate or the rate can be varied as in case of multi plastic
injection. For the CTPA contrast alteration is best and recommended. The highest concentration
of 400 mg iodine per ml can be beneficial in route imaging and to obtain the detailed vasculature
resolution in CT angiography.
(Source: Aldosari, Jansen and Sun, 2019)
7
Illustration 1: CTPA Protocol comparison with variable elements
partial volume effects are also decreased. When the slice thickness is in the range 3 to 6 mm then
images noises are identical while the slice thickness of 3 mm can be considered as the best
choice for the image processing.
Patient alignment and position
During the scanning process the patient must lie straight on and their hands are positioned
in a firm condition above the head. The supine position is helpful in obtaining multiple scanning
and to have detailed observation of the required body organ. In order to maintain the correct
position strips and pillows are also used so that correct alignment can be established between
patient and screen.
Contrast timing and volumes
The timings of injecting contrast, concentration and its volume influences the
enhancement degree which can be achieved by the contrast substance (Kanwar and et.al., 2019).
The contrast can be infused at constant rate or the rate can be varied as in case of multi plastic
injection. For the CTPA contrast alteration is best and recommended. The highest concentration
of 400 mg iodine per ml can be beneficial in route imaging and to obtain the detailed vasculature
resolution in CT angiography.
(Source: Aldosari, Jansen and Sun, 2019)
7
Illustration 1: CTPA Protocol comparison with variable elements
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Anatomy and scanning range
The scanning and recovery procedure of CTPA can be of around three to four hours. The
technique is used to provide the image of pulmonary arteries and depends greatly on radionuclide
imaging of blood vessels of lungs. Though a single scanning can be completed in few minutes
but the accurate process needs multiple scanning (Nockel and et.al., 2016). It has been also used
for preventing medicine. This imaging technique can diagnose the head related tumours, brain
trauma, changes in lungs parenchyma and in visual inspection of venous and arterial vessels of
entire body. These blood vessels can range from brain to lungs, kidneys or arms.
Post processing requirements
There has been several improvements in the digital image processing and thus the post
image processing methods and requirements of CTPA have also changed significantly. The data
obtained from computerised tomography is reconstructed in two or three dimensional formats.
This reconstruction can help professionals to diagnose the organ and then to make operative
planning and assessment (Chung and et.al., 2015). For this purpose multi planar two dimensional
construction is also involved which can process the axial image of CTPA. Radiographers also
prefers mulilplanar reformatted (MPR) images which can be easily integrated with the real time
orientations.
CONCLUSION
It can be concluded from the assessment that CTPA provides valuable imaging and
anatomical information. Thus, for the accurate and precise imaging and diagnosis function it is
essential that several aspects like positioning of the patient, drug administration, timing, pre and
post process requirements of CTPA must be taken into considerations. It has analysed from the
study that pregnancy contradictions, allergies from iodine and rotation time of tube can also
influence the image quality. Thus, prior to the testing procedure radiographers and patients both
must understand and analyse the relevant protocols related to computerised tomography.
8
The scanning and recovery procedure of CTPA can be of around three to four hours. The
technique is used to provide the image of pulmonary arteries and depends greatly on radionuclide
imaging of blood vessels of lungs. Though a single scanning can be completed in few minutes
but the accurate process needs multiple scanning (Nockel and et.al., 2016). It has been also used
for preventing medicine. This imaging technique can diagnose the head related tumours, brain
trauma, changes in lungs parenchyma and in visual inspection of venous and arterial vessels of
entire body. These blood vessels can range from brain to lungs, kidneys or arms.
Post processing requirements
There has been several improvements in the digital image processing and thus the post
image processing methods and requirements of CTPA have also changed significantly. The data
obtained from computerised tomography is reconstructed in two or three dimensional formats.
This reconstruction can help professionals to diagnose the organ and then to make operative
planning and assessment (Chung and et.al., 2015). For this purpose multi planar two dimensional
construction is also involved which can process the axial image of CTPA. Radiographers also
prefers mulilplanar reformatted (MPR) images which can be easily integrated with the real time
orientations.
CONCLUSION
It can be concluded from the assessment that CTPA provides valuable imaging and
anatomical information. Thus, for the accurate and precise imaging and diagnosis function it is
essential that several aspects like positioning of the patient, drug administration, timing, pre and
post process requirements of CTPA must be taken into considerations. It has analysed from the
study that pregnancy contradictions, allergies from iodine and rotation time of tube can also
influence the image quality. Thus, prior to the testing procedure radiographers and patients both
must understand and analyse the relevant protocols related to computerised tomography.
8
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

REFERENCES
Books and Journals
Chung, J.H., and et.al., 2015. CT scan findings of probable usual interstitial pneumonitis have a
high predictive value for histologic usual interstitial pneumonitis. Chest. 147(2). pp.450-
459.
Dekkers, T., and et.al., 2016. Adrenal vein sampling versus CT scan to determine treatment in
primary aldosteronism: an outcome-based randomised diagnostic trial. The lancet
Diabetes & endocrinology. 4(9). pp.739-746.
Gillespie, C.D., and et.al., 2019. P008: The OPTICA (OPTImised CTPA In Pregnancy) study:
rationale and design of a prospective trial assessing the quality and safety of an optimised
CTPA protocol in pregnancy. Thrombosis Research. 175. p.S9.
Kanwar, M., and et.al., 2019. Characteristics and Management of Patients Following Pulmonary
Embolism: A Focus on Screening for Chronic Thromboembolic Pulmonary
Hypertension. The Journal of Heart and Lung Transplantation. 38(4). pp.S130-S131.
Mokadam, N.A., and et.al., 2019. Costs Associated with the First Clinical Trial Evaluating the
Safety and Efficacy of the Thoracotomy Approach for Implantation of a Small
Intrapericardial Centrifugal LVAD. The Journal of Heart and Lung
Transplantation. 38(4). pp.S131-S132.
Nockel, P., and et.al., 2016. Localization of insulinoma using 68Ga-DOTATATE PET/CT
scan. The Journal of Clinical Endocrinology & Metabolism. 102(1). pp.195-199.
Pitiyarachchi, O., and et.al., 2019. P007: Successful pregnancy outcome in a woman with
inherited factor V deficiency. Thrombosis Research. 175. p.S9.
Siddiqui, M.M.A., and et.al., 2016. Accurate Diagnosis of Pulmonary Embolism in ECG Taking
Computed Tomography Pulmonary Angiography (CTPA) As Gold Standard. PAKISTAN
JOURNAL OF MEDICAL & HEALTH SCIENCES. 10(1). pp.80-85.
Vanier, M. and Caplan, D., 2017. CT scan correlates of surface dyslexia. In Surface dyslexia.
(pp. 511-526). Routledge.
Vayntrub, Y., and et.al., 2017. Incidence Of Clinically Relevant Findings On CT Pulmonary
Angiography Negative For Pulmonary Embolism. In A69. LET IT GO:
CONTROVERSIES IN THROMBOEMBOLIC DISEASE. (pp. A2316-A2316). American
Thoracic Society.
Online
Aldosari,S., Jansen, S. and Sun, Zhonghua., 2019. Opitmization of computed tomography
pulmonary angiography protocols using 3D printed model with simulation of pulmonary
embolism. [Online]. Accessed through
<http://qims.amegroups.com/article/view/21792/22461>
Computer-Aided Detection, Pulmonary Embolism, Computerized Tomography Pulmonary
Angiography: Current Status. 2018. [Online]. Accessed through
<https://www.intechopen.com/online-first/computer-aided-detection-pulmonary-
embolism-computerized-tomography-pulmonary-angiography-current-st>
CT angiography of the abdominal wall to study the inferior epigastric system for DIEP flap
breast reconstruction. 2011. [Online]. Accessed through
<https://posterng.netkey.at/esr/viewing/index.php?
module=viewing_poster&task=viewsection&pi=107721&ti=333267&si=1042&searchke
y=&scrollpos=0>
9
Books and Journals
Chung, J.H., and et.al., 2015. CT scan findings of probable usual interstitial pneumonitis have a
high predictive value for histologic usual interstitial pneumonitis. Chest. 147(2). pp.450-
459.
Dekkers, T., and et.al., 2016. Adrenal vein sampling versus CT scan to determine treatment in
primary aldosteronism: an outcome-based randomised diagnostic trial. The lancet
Diabetes & endocrinology. 4(9). pp.739-746.
Gillespie, C.D., and et.al., 2019. P008: The OPTICA (OPTImised CTPA In Pregnancy) study:
rationale and design of a prospective trial assessing the quality and safety of an optimised
CTPA protocol in pregnancy. Thrombosis Research. 175. p.S9.
Kanwar, M., and et.al., 2019. Characteristics and Management of Patients Following Pulmonary
Embolism: A Focus on Screening for Chronic Thromboembolic Pulmonary
Hypertension. The Journal of Heart and Lung Transplantation. 38(4). pp.S130-S131.
Mokadam, N.A., and et.al., 2019. Costs Associated with the First Clinical Trial Evaluating the
Safety and Efficacy of the Thoracotomy Approach for Implantation of a Small
Intrapericardial Centrifugal LVAD. The Journal of Heart and Lung
Transplantation. 38(4). pp.S131-S132.
Nockel, P., and et.al., 2016. Localization of insulinoma using 68Ga-DOTATATE PET/CT
scan. The Journal of Clinical Endocrinology & Metabolism. 102(1). pp.195-199.
Pitiyarachchi, O., and et.al., 2019. P007: Successful pregnancy outcome in a woman with
inherited factor V deficiency. Thrombosis Research. 175. p.S9.
Siddiqui, M.M.A., and et.al., 2016. Accurate Diagnosis of Pulmonary Embolism in ECG Taking
Computed Tomography Pulmonary Angiography (CTPA) As Gold Standard. PAKISTAN
JOURNAL OF MEDICAL & HEALTH SCIENCES. 10(1). pp.80-85.
Vanier, M. and Caplan, D., 2017. CT scan correlates of surface dyslexia. In Surface dyslexia.
(pp. 511-526). Routledge.
Vayntrub, Y., and et.al., 2017. Incidence Of Clinically Relevant Findings On CT Pulmonary
Angiography Negative For Pulmonary Embolism. In A69. LET IT GO:
CONTROVERSIES IN THROMBOEMBOLIC DISEASE. (pp. A2316-A2316). American
Thoracic Society.
Online
Aldosari,S., Jansen, S. and Sun, Zhonghua., 2019. Opitmization of computed tomography
pulmonary angiography protocols using 3D printed model with simulation of pulmonary
embolism. [Online]. Accessed through
<http://qims.amegroups.com/article/view/21792/22461>
Computer-Aided Detection, Pulmonary Embolism, Computerized Tomography Pulmonary
Angiography: Current Status. 2018. [Online]. Accessed through
<https://www.intechopen.com/online-first/computer-aided-detection-pulmonary-
embolism-computerized-tomography-pulmonary-angiography-current-st>
CT angiography of the abdominal wall to study the inferior epigastric system for DIEP flap
breast reconstruction. 2011. [Online]. Accessed through
<https://posterng.netkey.at/esr/viewing/index.php?
module=viewing_poster&task=viewsection&pi=107721&ti=333267&si=1042&searchke
y=&scrollpos=0>
9
CT Pulmonary Angiogram. 2018. [Online]. Accessed through
<https://healthengine.com.au/info/ct-pulmonary-angiogram>
Super-resolution CT Image Reconstruction Based on Dictionary Learning and Sparse
Representation. 2018. [Online]. Accessed through
<https://www.nature.com/articles/s41598-018-27261-z>
10
<https://healthengine.com.au/info/ct-pulmonary-angiogram>
Super-resolution CT Image Reconstruction Based on Dictionary Learning and Sparse
Representation. 2018. [Online]. Accessed through
<https://www.nature.com/articles/s41598-018-27261-z>
10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.