Psychology Research Outline: Treating Sleep Problems in Depression
VerifiedAdded on 2023/04/07
|16
|3454
|92
Homework Assignment
AI Summary
This research outline explores the complex relationship between sleep problems and depression, focusing on various treatment methods. It highlights that depression often leads to sleep disturbances, such as insomnia, which in turn can exacerbate depressive symptoms. The outline references several studies discussing the efficacy of both pharmacological and non-pharmacological interventions, including Cognitive Behavioral Therapy (CBT), stimulus control instructions, sleep restriction, and pharmacotherapy using SSRIs and benzodiazepines. It emphasizes the importance of addressing comorbid sleep disorders like sleep apnea and restless legs syndrome in depressed patients. The document also touches on the potential benefits of modafinil for treating sleepiness in individuals with Major Depressive Disorder (MDD). The outline concludes that a comprehensive assessment of sleep problems is crucial for effectively treating depression, often requiring a combination of psychotherapy and medication to improve both sleep quality and mood.
Psychology
Name
Institution
Professor
Course
Date
Name
Institution
Professor
Course
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
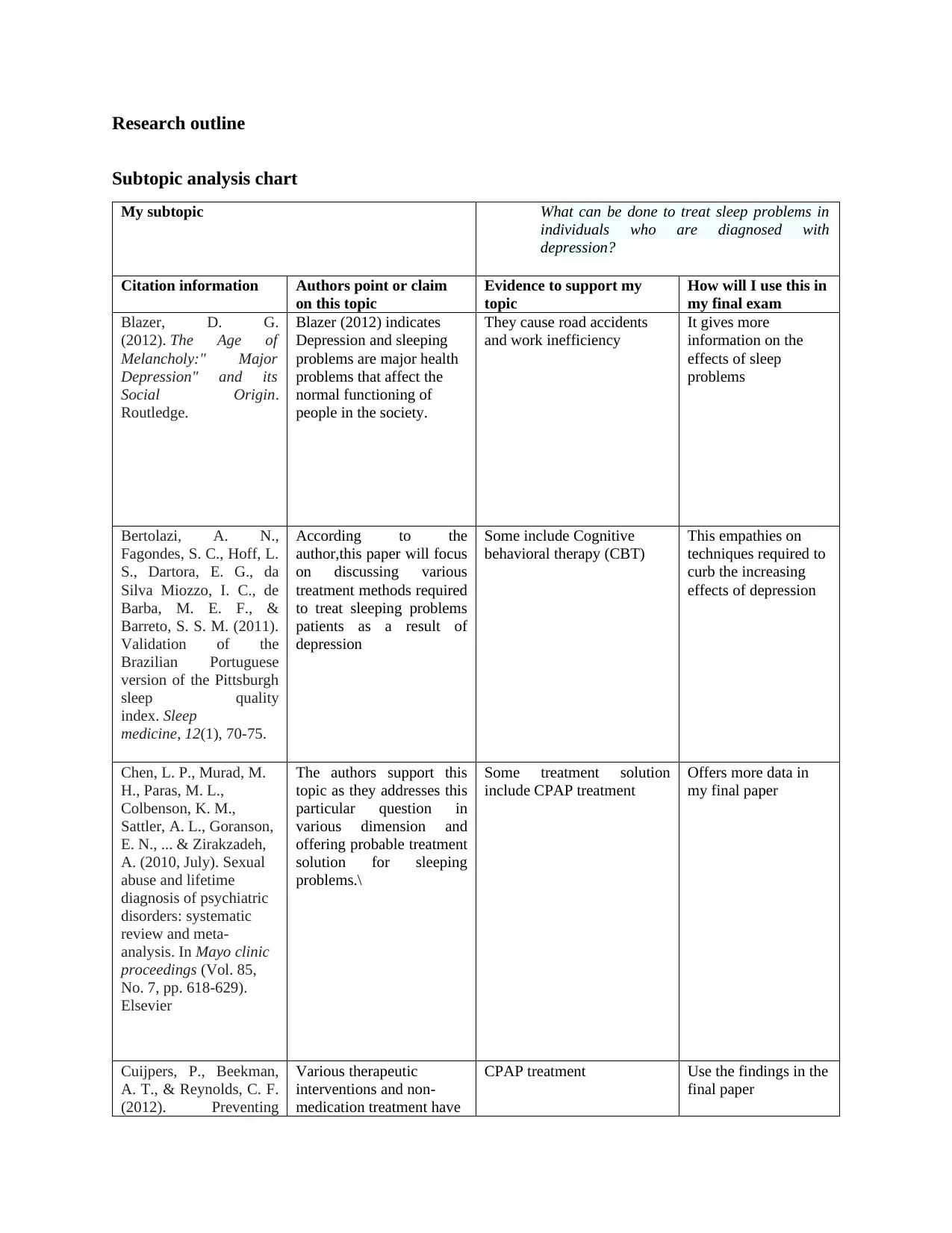
Research outline
Subtopic analysis chart
My subtopic What can be done to treat sleep problems in
individuals who are diagnosed with
depression?
Citation information Authors point or claim
on this topic
Evidence to support my
topic
How will I use this in
my final exam
Blazer, D. G.
(2012). The Age of
Melancholy:" Major
Depression" and its
Social Origin.
Routledge.
Blazer (2012) indicates
Depression and sleeping
problems are major health
problems that affect the
normal functioning of
people in the society.
They cause road accidents
and work inefficiency
It gives more
information on the
effects of sleep
problems
Bertolazi, A. N.,
Fagondes, S. C., Hoff, L.
S., Dartora, E. G., da
Silva Miozzo, I. C., de
Barba, M. E. F., &
Barreto, S. S. M. (2011).
Validation of the
Brazilian Portuguese
version of the Pittsburgh
sleep quality
index. Sleep
medicine, 12(1), 70-75.
According to the
author,this paper will focus
on discussing various
treatment methods required
to treat sleeping problems
patients as a result of
depression
Some include Cognitive
behavioral therapy (CBT)
This empathies on
techniques required to
curb the increasing
effects of depression
Chen, L. P., Murad, M.
H., Paras, M. L.,
Colbenson, K. M.,
Sattler, A. L., Goranson,
E. N., ... & Zirakzadeh,
A. (2010, July). Sexual
abuse and lifetime
diagnosis of psychiatric
disorders: systematic
review and meta-
analysis. In Mayo clinic
proceedings (Vol. 85,
No. 7, pp. 618-629).
Elsevier
The authors support this
topic as they addresses this
particular question in
various dimension and
offering probable treatment
solution for sleeping
problems.\
Some treatment solution
include CPAP treatment
Offers more data in
my final paper
Cuijpers, P., Beekman,
A. T., & Reynolds, C. F.
(2012). Preventing
Various therapeutic
interventions and non-
medication treatment have
CPAP treatment Use the findings in the
final paper
Subtopic analysis chart
My subtopic What can be done to treat sleep problems in
individuals who are diagnosed with
depression?
Citation information Authors point or claim
on this topic
Evidence to support my
topic
How will I use this in
my final exam
Blazer, D. G.
(2012). The Age of
Melancholy:" Major
Depression" and its
Social Origin.
Routledge.
Blazer (2012) indicates
Depression and sleeping
problems are major health
problems that affect the
normal functioning of
people in the society.
They cause road accidents
and work inefficiency
It gives more
information on the
effects of sleep
problems
Bertolazi, A. N.,
Fagondes, S. C., Hoff, L.
S., Dartora, E. G., da
Silva Miozzo, I. C., de
Barba, M. E. F., &
Barreto, S. S. M. (2011).
Validation of the
Brazilian Portuguese
version of the Pittsburgh
sleep quality
index. Sleep
medicine, 12(1), 70-75.
According to the
author,this paper will focus
on discussing various
treatment methods required
to treat sleeping problems
patients as a result of
depression
Some include Cognitive
behavioral therapy (CBT)
This empathies on
techniques required to
curb the increasing
effects of depression
Chen, L. P., Murad, M.
H., Paras, M. L.,
Colbenson, K. M.,
Sattler, A. L., Goranson,
E. N., ... & Zirakzadeh,
A. (2010, July). Sexual
abuse and lifetime
diagnosis of psychiatric
disorders: systematic
review and meta-
analysis. In Mayo clinic
proceedings (Vol. 85,
No. 7, pp. 618-629).
Elsevier
The authors support this
topic as they addresses this
particular question in
various dimension and
offering probable treatment
solution for sleeping
problems.\
Some treatment solution
include CPAP treatment
Offers more data in
my final paper
Cuijpers, P., Beekman,
A. T., & Reynolds, C. F.
(2012). Preventing
Various therapeutic
interventions and non-
medication treatment have
CPAP treatment Use the findings in the
final paper
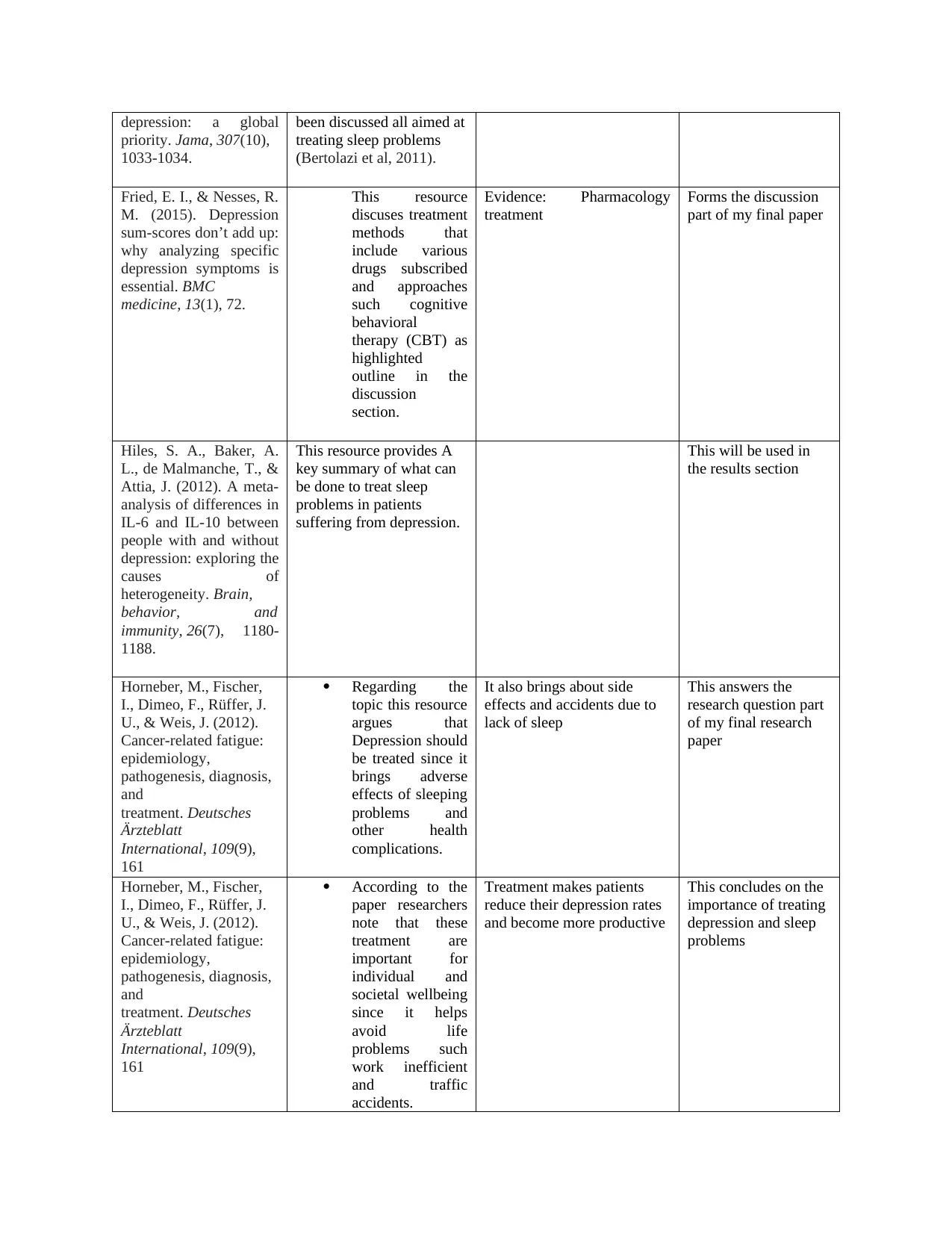
depression: a global
priority. Jama, 307(10),
1033-1034.
been discussed all aimed at
treating sleep problems
(Bertolazi et al, 2011).
Fried, E. I., & Nesses, R.
M. (2015). Depression
sum-scores don’t add up:
why analyzing specific
depression symptoms is
essential. BMC
medicine, 13(1), 72.
This resource
discuses treatment
methods that
include various
drugs subscribed
and approaches
such cognitive
behavioral
therapy (CBT) as
highlighted
outline in the
discussion
section.
Evidence: Pharmacology
treatment
Forms the discussion
part of my final paper
Hiles, S. A., Baker, A.
L., de Malmanche, T., &
Attia, J. (2012). A meta-
analysis of differences in
IL-6 and IL-10 between
people with and without
depression: exploring the
causes of
heterogeneity. Brain,
behavior, and
immunity, 26(7), 1180-
1188.
This resource provides A
key summary of what can
be done to treat sleep
problems in patients
suffering from depression.
This will be used in
the results section
Horneber, M., Fischer,
I., Dimeo, F., Rüffer, J.
U., & Weis, J. (2012).
Cancer-related fatigue:
epidemiology,
pathogenesis, diagnosis,
and
treatment. Deutsches
Ärzteblatt
International, 109(9),
161
Regarding the
topic this resource
argues that
Depression should
be treated since it
brings adverse
effects of sleeping
problems and
other health
complications.
It also brings about side
effects and accidents due to
lack of sleep
This answers the
research question part
of my final research
paper
Horneber, M., Fischer,
I., Dimeo, F., Rüffer, J.
U., & Weis, J. (2012).
Cancer-related fatigue:
epidemiology,
pathogenesis, diagnosis,
and
treatment. Deutsches
Ärzteblatt
International, 109(9),
161
According to the
paper researchers
note that these
treatment are
important for
individual and
societal wellbeing
since it helps
avoid life
problems such
work inefficient
and traffic
accidents.
Treatment makes patients
reduce their depression rates
and become more productive
This concludes on the
importance of treating
depression and sleep
problems
priority. Jama, 307(10),
1033-1034.
been discussed all aimed at
treating sleep problems
(Bertolazi et al, 2011).
Fried, E. I., & Nesses, R.
M. (2015). Depression
sum-scores don’t add up:
why analyzing specific
depression symptoms is
essential. BMC
medicine, 13(1), 72.
This resource
discuses treatment
methods that
include various
drugs subscribed
and approaches
such cognitive
behavioral
therapy (CBT) as
highlighted
outline in the
discussion
section.
Evidence: Pharmacology
treatment
Forms the discussion
part of my final paper
Hiles, S. A., Baker, A.
L., de Malmanche, T., &
Attia, J. (2012). A meta-
analysis of differences in
IL-6 and IL-10 between
people with and without
depression: exploring the
causes of
heterogeneity. Brain,
behavior, and
immunity, 26(7), 1180-
1188.
This resource provides A
key summary of what can
be done to treat sleep
problems in patients
suffering from depression.
This will be used in
the results section
Horneber, M., Fischer,
I., Dimeo, F., Rüffer, J.
U., & Weis, J. (2012).
Cancer-related fatigue:
epidemiology,
pathogenesis, diagnosis,
and
treatment. Deutsches
Ärzteblatt
International, 109(9),
161
Regarding the
topic this resource
argues that
Depression should
be treated since it
brings adverse
effects of sleeping
problems and
other health
complications.
It also brings about side
effects and accidents due to
lack of sleep
This answers the
research question part
of my final research
paper
Horneber, M., Fischer,
I., Dimeo, F., Rüffer, J.
U., & Weis, J. (2012).
Cancer-related fatigue:
epidemiology,
pathogenesis, diagnosis,
and
treatment. Deutsches
Ärzteblatt
International, 109(9),
161
According to the
paper researchers
note that these
treatment are
important for
individual and
societal wellbeing
since it helps
avoid life
problems such
work inefficient
and traffic
accidents.
Treatment makes patients
reduce their depression rates
and become more productive
This concludes on the
importance of treating
depression and sleep
problems
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
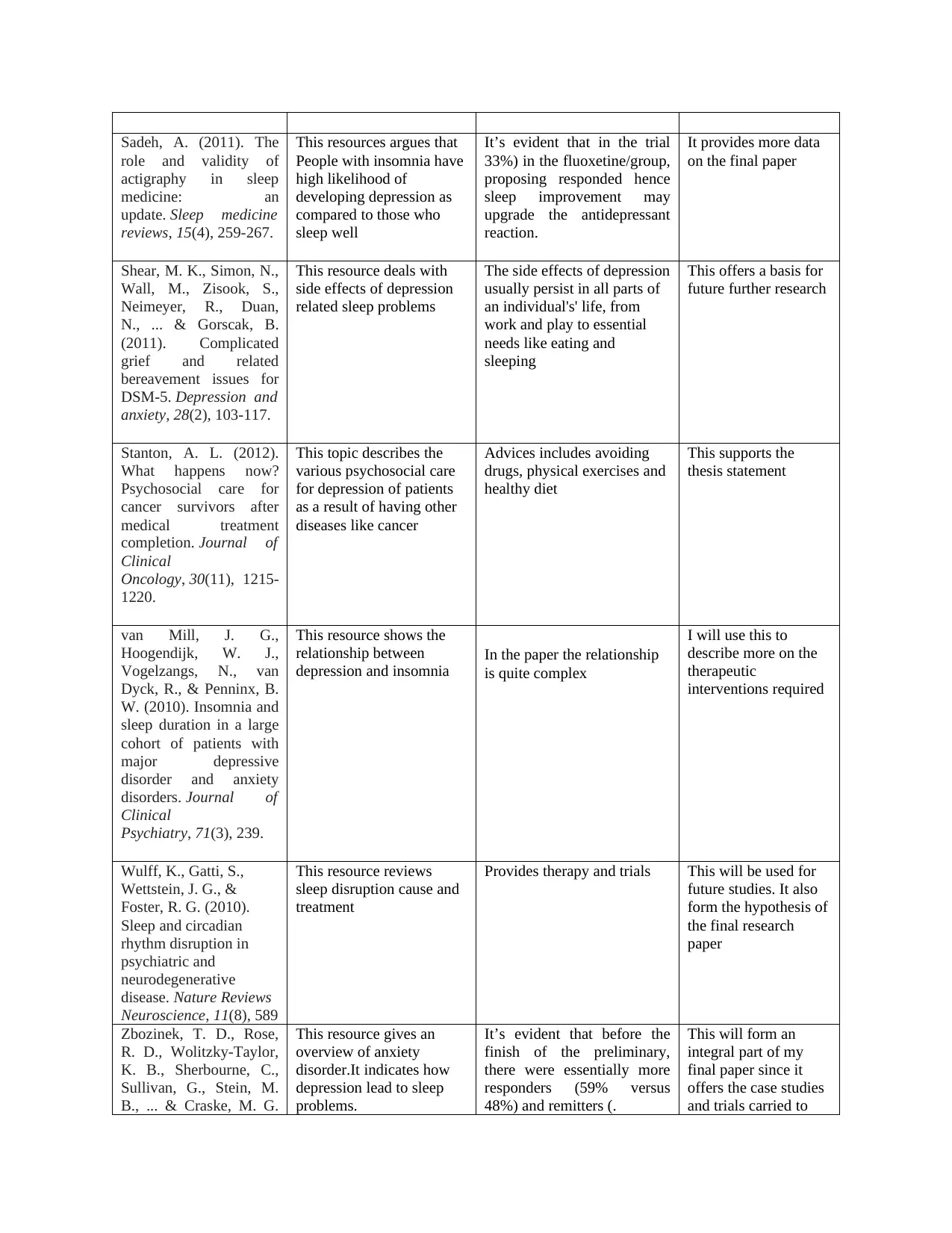
Sadeh, A. (2011). The
role and validity of
actigraphy in sleep
medicine: an
update. Sleep medicine
reviews, 15(4), 259-267.
This resources argues that
People with insomnia have
high likelihood of
developing depression as
compared to those who
sleep well
It’s evident that in the trial
33%) in the fluoxetine/group,
proposing responded hence
sleep improvement may
upgrade the antidepressant
reaction.
It provides more data
on the final paper
Shear, M. K., Simon, N.,
Wall, M., Zisook, S.,
Neimeyer, R., Duan,
N., ... & Gorscak, B.
(2011). Complicated
grief and related
bereavement issues for
DSM‐5. Depression and
anxiety, 28(2), 103-117.
This resource deals with
side effects of depression
related sleep problems
The side effects of depression
usually persist in all parts of
an individual's' life, from
work and play to essential
needs like eating and
sleeping
This offers a basis for
future further research
Stanton, A. L. (2012).
What happens now?
Psychosocial care for
cancer survivors after
medical treatment
completion. Journal of
Clinical
Oncology, 30(11), 1215-
1220.
This topic describes the
various psychosocial care
for depression of patients
as a result of having other
diseases like cancer
Advices includes avoiding
drugs, physical exercises and
healthy diet
This supports the
thesis statement
van Mill, J. G.,
Hoogendijk, W. J.,
Vogelzangs, N., van
Dyck, R., & Penninx, B.
W. (2010). Insomnia and
sleep duration in a large
cohort of patients with
major depressive
disorder and anxiety
disorders. Journal of
Clinical
Psychiatry, 71(3), 239.
This resource shows the
relationship between
depression and insomnia
In the paper the relationship
is quite complex
I will use this to
describe more on the
therapeutic
interventions required
Wulff, K., Gatti, S.,
Wettstein, J. G., &
Foster, R. G. (2010).
Sleep and circadian
rhythm disruption in
psychiatric and
neurodegenerative
disease. Nature Reviews
Neuroscience, 11(8), 589
This resource reviews
sleep disruption cause and
treatment
Provides therapy and trials This will be used for
future studies. It also
form the hypothesis of
the final research
paper
Zbozinek, T. D., Rose,
R. D., Wolitzky‐Taylor,
K. B., Sherbourne, C.,
Sullivan, G., Stein, M.
B., ... & Craske, M. G.
This resource gives an
overview of anxiety
disorder.It indicates how
depression lead to sleep
problems.
It’s evident that before the
finish of the preliminary,
there were essentially more
responders (59% versus
48%) and remitters (.
This will form an
integral part of my
final paper since it
offers the case studies
and trials carried to
role and validity of
actigraphy in sleep
medicine: an
update. Sleep medicine
reviews, 15(4), 259-267.
This resources argues that
People with insomnia have
high likelihood of
developing depression as
compared to those who
sleep well
It’s evident that in the trial
33%) in the fluoxetine/group,
proposing responded hence
sleep improvement may
upgrade the antidepressant
reaction.
It provides more data
on the final paper
Shear, M. K., Simon, N.,
Wall, M., Zisook, S.,
Neimeyer, R., Duan,
N., ... & Gorscak, B.
(2011). Complicated
grief and related
bereavement issues for
DSM‐5. Depression and
anxiety, 28(2), 103-117.
This resource deals with
side effects of depression
related sleep problems
The side effects of depression
usually persist in all parts of
an individual's' life, from
work and play to essential
needs like eating and
sleeping
This offers a basis for
future further research
Stanton, A. L. (2012).
What happens now?
Psychosocial care for
cancer survivors after
medical treatment
completion. Journal of
Clinical
Oncology, 30(11), 1215-
1220.
This topic describes the
various psychosocial care
for depression of patients
as a result of having other
diseases like cancer
Advices includes avoiding
drugs, physical exercises and
healthy diet
This supports the
thesis statement
van Mill, J. G.,
Hoogendijk, W. J.,
Vogelzangs, N., van
Dyck, R., & Penninx, B.
W. (2010). Insomnia and
sleep duration in a large
cohort of patients with
major depressive
disorder and anxiety
disorders. Journal of
Clinical
Psychiatry, 71(3), 239.
This resource shows the
relationship between
depression and insomnia
In the paper the relationship
is quite complex
I will use this to
describe more on the
therapeutic
interventions required
Wulff, K., Gatti, S.,
Wettstein, J. G., &
Foster, R. G. (2010).
Sleep and circadian
rhythm disruption in
psychiatric and
neurodegenerative
disease. Nature Reviews
Neuroscience, 11(8), 589
This resource reviews
sleep disruption cause and
treatment
Provides therapy and trials This will be used for
future studies. It also
form the hypothesis of
the final research
paper
Zbozinek, T. D., Rose,
R. D., Wolitzky‐Taylor,
K. B., Sherbourne, C.,
Sullivan, G., Stein, M.
B., ... & Craske, M. G.
This resource gives an
overview of anxiety
disorder.It indicates how
depression lead to sleep
problems.
It’s evident that before the
finish of the preliminary,
there were essentially more
responders (59% versus
48%) and remitters (.
This will form an
integral part of my
final paper since it
offers the case studies
and trials carried to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
(2012). Diagnostic
overlap of generalized
anxiety disorder and
major depressive
disorder in a primary
care sample. Depression
and anxiety, 29(12),
1065-1071.
various patients. My
final paper will be
based on accurate data
on the methodology
part.
overlap of generalized
anxiety disorder and
major depressive
disorder in a primary
care sample. Depression
and anxiety, 29(12),
1065-1071.
various patients. My
final paper will be
based on accurate data
on the methodology
part.
Introduction
The relationship between sleep problems and depression is quite complex. Depression cause
sleep problems in individuals. People with insomnia have high likelihood of developing
depression as compared to those who sleep well (Blazer,2012). Evidently sleep problems are
center indications depression. Both depression and serious rest issues are significant hazard
factors for suicide and medical issues like coronary illness, other mental clutters, and smoking.
Individuals with misery experience difficulty being beneficial in work or school, which can
affect their vocation and public activity. The rest issues are regularly one reason discouraged
individuals search out proficient help. Lack of sleep have critical impacts like cognitive
impairment, increased depression, risk of injury and road accidents.
The side effects of depression usually persist in all parts of an individual's' life, from work and
play to essential needs like eating and sleeping. Inside the bigger classification of gloom, there
are a few distinct sorts of sorrow which accompany their very own sleep issues.
Discussion
A sleeping disorder and other sleep problems frequently go unrecognized; however, treating a
sleeping disorder may reduce depression effects and ensure fast recovery (Cuijpers, Beekman, &
Reynolds, 2012). The most grounded, proof originates from an ongoing treatment controlled,
investigation in which 545 patients meeting criteria for both MDD and sleep problem got
fluoxetine (a particular serotonin reuptake inhibitor, SSRI) toward the beginning of the day and
were haphazardly allocated to fake cszopiclonc (a benzodiazepine receptor agonist) at night .
The relationship between sleep problems and depression is quite complex. Depression cause
sleep problems in individuals. People with insomnia have high likelihood of developing
depression as compared to those who sleep well (Blazer,2012). Evidently sleep problems are
center indications depression. Both depression and serious rest issues are significant hazard
factors for suicide and medical issues like coronary illness, other mental clutters, and smoking.
Individuals with misery experience difficulty being beneficial in work or school, which can
affect their vocation and public activity. The rest issues are regularly one reason discouraged
individuals search out proficient help. Lack of sleep have critical impacts like cognitive
impairment, increased depression, risk of injury and road accidents.
The side effects of depression usually persist in all parts of an individual's' life, from work and
play to essential needs like eating and sleeping. Inside the bigger classification of gloom, there
are a few distinct sorts of sorrow which accompany their very own sleep issues.
Discussion
A sleeping disorder and other sleep problems frequently go unrecognized; however, treating a
sleeping disorder may reduce depression effects and ensure fast recovery (Cuijpers, Beekman, &
Reynolds, 2012). The most grounded, proof originates from an ongoing treatment controlled,
investigation in which 545 patients meeting criteria for both MDD and sleep problem got
fluoxetine (a particular serotonin reuptake inhibitor, SSRI) toward the beginning of the day and
were haphazardly allocated to fake cszopiclonc (a benzodiazepine receptor agonist) at night .
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Depressed patients suffer from insomnia related problems like having challenges falling asleep,
over-sleepiness, difficulty staying asleep and unrefreshed sleep
Eminently, before the finish of the preliminary, there were essentially more responders (59%
versus 48%) and remitters (42% versus 33%) in the fluoxetine/group, proposing that sleep
improvement may upgrade the antidepressant reaction.
Patients allocated to the hypnotic had improved self-announced rest, daytime capacity, and
prosperity. In this way, pharmacotherapy for sleep deprivation did not disable the energizer
reaction in patients who had just reacted to pharmacotherapy for depression (Fried, & Nesse,
2015). Research in which benzodiazepines, for example, clonazepam, lorazepam, and
lormetazepam were utilized as an adjunctive treatment, likewise demonstrated that depressed
individual patients had improved rest without increasing of depression. (Chen et al,2013).Every
one of these examinations proposed that, adjunctive benzodiazepines might be related with
improved reaction, increasingly fast reaction, more prominent consistence, or a more prominent
level of responders towards treatment of sleep problems as a result of depression.
There bend less examinations researching non pharmacological mediations for sleep deprivation
in depression. Various behavioral interventions incorporate improvement control instructions and
sleeping restriction. Cognitive –behavioral treatment for a sleeping disorder (CBT-I) for the most
part incorporates an extra cognitive segment, for example, remedying dysfunctional beliefs
regarding sleep.
Self-improvement treatment that comprised of stimulus control, relaxing, and psychological
components63; enhancements in rest were additionally connected with critical, decreases in self
reported depression related sleep disorder.
over-sleepiness, difficulty staying asleep and unrefreshed sleep
Eminently, before the finish of the preliminary, there were essentially more responders (59%
versus 48%) and remitters (42% versus 33%) in the fluoxetine/group, proposing that sleep
improvement may upgrade the antidepressant reaction.
Patients allocated to the hypnotic had improved self-announced rest, daytime capacity, and
prosperity. In this way, pharmacotherapy for sleep deprivation did not disable the energizer
reaction in patients who had just reacted to pharmacotherapy for depression (Fried, & Nesse,
2015). Research in which benzodiazepines, for example, clonazepam, lorazepam, and
lormetazepam were utilized as an adjunctive treatment, likewise demonstrated that depressed
individual patients had improved rest without increasing of depression. (Chen et al,2013).Every
one of these examinations proposed that, adjunctive benzodiazepines might be related with
improved reaction, increasingly fast reaction, more prominent consistence, or a more prominent
level of responders towards treatment of sleep problems as a result of depression.
There bend less examinations researching non pharmacological mediations for sleep deprivation
in depression. Various behavioral interventions incorporate improvement control instructions and
sleeping restriction. Cognitive –behavioral treatment for a sleeping disorder (CBT-I) for the most
part incorporates an extra cognitive segment, for example, remedying dysfunctional beliefs
regarding sleep.
Self-improvement treatment that comprised of stimulus control, relaxing, and psychological
components63; enhancements in rest were additionally connected with critical, decreases in self
reported depression related sleep disorder.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Further controlled preliminaries are expected to duplicate these discoveries, to look at whether
the goals of a sleeping disorder following CBT-I or potentially pharmacotherapy prompts longer
times of depression reduction, and whether sleeping disorder treatment positively effect, rest and
depression in people whose sleeping disorder develops amid treatment or remains a lingering
indication following a satisfactory antidepressant trial.
Modafinil is a novel psychostimulant affirmed to treat oversleeping during the day in narcolepsy
rest apnea. It also treats shift work sleep problem. Modafinil has a few properties that make it a
potential possibility to treat sleep and weariness in MDD; it is generally very much endured, and
dissimilar to great stimulants, modafinil has less euphoric impacts and is thought, to have lower
effects. A few uncontrolled, open-mark preliminaries in depression indicate that the treatment
reduces depression related sleep disorder. Patients suffering from depression and suffering from
sleep problems respond highly to this kind of treatment.
In depressed individual patients with sleep problems, referral to a specialist may assist decide if
there is a hidden comorbid sleeping issue, for example, rest apnea or fretful legs disorder that,
may cause or add to the side effects of misery. In spite of the fact that a sleeping disorder that
bring about depression.
In light of the discoveries investigated above, it is critical for clinicians to painstakingly assess
sleep problems effects in patients with depression. The developing perspective that a sleeping
disorder is generally comorbid with depression, recommending that, both a sleeping disorder and
depression may warrant, explicit treatment, much of the time (Hiles,Baker, de Malmanche, &
Attia,2012). In spite of the fact that there have been few randomized, controlled treatment
the goals of a sleeping disorder following CBT-I or potentially pharmacotherapy prompts longer
times of depression reduction, and whether sleeping disorder treatment positively effect, rest and
depression in people whose sleeping disorder develops amid treatment or remains a lingering
indication following a satisfactory antidepressant trial.
Modafinil is a novel psychostimulant affirmed to treat oversleeping during the day in narcolepsy
rest apnea. It also treats shift work sleep problem. Modafinil has a few properties that make it a
potential possibility to treat sleep and weariness in MDD; it is generally very much endured, and
dissimilar to great stimulants, modafinil has less euphoric impacts and is thought, to have lower
effects. A few uncontrolled, open-mark preliminaries in depression indicate that the treatment
reduces depression related sleep disorder. Patients suffering from depression and suffering from
sleep problems respond highly to this kind of treatment.
In depressed individual patients with sleep problems, referral to a specialist may assist decide if
there is a hidden comorbid sleeping issue, for example, rest apnea or fretful legs disorder that,
may cause or add to the side effects of misery. In spite of the fact that a sleeping disorder that
bring about depression.
In light of the discoveries investigated above, it is critical for clinicians to painstakingly assess
sleep problems effects in patients with depression. The developing perspective that a sleeping
disorder is generally comorbid with depression, recommending that, both a sleeping disorder and
depression may warrant, explicit treatment, much of the time (Hiles,Baker, de Malmanche, &
Attia,2012). In spite of the fact that there have been few randomized, controlled treatment

preliminaries on sleep deprivation comorbid with high level depression, the accessible proof
recommends the viability of a few treatment approaches.
Treatment for depression related sleeping disorder normally includes a mix of psychotherapy and
additionally pharmacological (drug) treatment. Every one of these treatments might be utilized to
treat both depression and insomnia and treatment for sleep problems is typically a significant part
in depression therapy for patients (Horneber,Fischer, Dimeo, Rüffer, & Weis,2012).
Treating depression is often complicated by sleeping problems. For instance, patients with both
OSA and depression ought to abstain from using antidepressant medicines because of their
capability to smother breathing and exacerbate OSA. Prior to starting treatment for depression, a
patient should converse with the doctor about any sleep manifestations one is encountering. ,
adequately treating the sleep problem might be sufficient to lighten the manifestations of
depression.
Cognitive behavioral therapy (CBT) is a conduct way to deal with treating depression that is
progressively well known because of its viability and absence of side effects. The fundamental
nature of CBT for depression incorporate intellectual rebuilding, a procedure that aim at those
particular thoughts which brings about depressive feelings and sleep problems, and behavioral
activation technique, which targets conduct that may propagate depression. Similarly, CBT
might be utilized to treat insomnia and depression in individuals
According to Stanton,(2012) there are various distinctive prescriptions used to treat a sleeping
disorder, and the doctor will work with patients to figure out which is the best for each
individual. Probably the most widely recognized medication medicines for depression are:
recommends the viability of a few treatment approaches.
Treatment for depression related sleeping disorder normally includes a mix of psychotherapy and
additionally pharmacological (drug) treatment. Every one of these treatments might be utilized to
treat both depression and insomnia and treatment for sleep problems is typically a significant part
in depression therapy for patients (Horneber,Fischer, Dimeo, Rüffer, & Weis,2012).
Treating depression is often complicated by sleeping problems. For instance, patients with both
OSA and depression ought to abstain from using antidepressant medicines because of their
capability to smother breathing and exacerbate OSA. Prior to starting treatment for depression, a
patient should converse with the doctor about any sleep manifestations one is encountering. ,
adequately treating the sleep problem might be sufficient to lighten the manifestations of
depression.
Cognitive behavioral therapy (CBT) is a conduct way to deal with treating depression that is
progressively well known because of its viability and absence of side effects. The fundamental
nature of CBT for depression incorporate intellectual rebuilding, a procedure that aim at those
particular thoughts which brings about depressive feelings and sleep problems, and behavioral
activation technique, which targets conduct that may propagate depression. Similarly, CBT
might be utilized to treat insomnia and depression in individuals
According to Stanton,(2012) there are various distinctive prescriptions used to treat a sleeping
disorder, and the doctor will work with patients to figure out which is the best for each
individual. Probably the most widely recognized medication medicines for depression are:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
• Selective serotonin reuptake inhibitors (SSRIs) – SSRIs successfully improve state of
mind in numerous patients, yet they may likewise cause or compound sleep deprivation.
• Tricyclic antidepressants – tricyclic antidepressants are commonly steadying, yet they
may likewise convey genuine reactions, for example, hypertension.
• Mood settling anticonvulsants and lithium – these medications are usually used to treat
bipolar confusion.
Notwithstanding the above treatment choices, patients who experience the ill effects of sadness
may use bright light therapy (Murray, et al 2011). Light treatment may include presentation to
normal (light from the sun) or treatment with a light box. Light treatment is viewed as safe,
however little proof exists to help its adequacy at treating depression or different types of sleep
problems.
Patients should be advised that treating depression related sleeping problems often take a lot of
time. Medication usually take weeks in order to take full effects and patients may require to try
out various drugs in order to establish the most convenient one. Patients should not stop taking
the medication since symptom s might arise and increase causing other side effects. Proper
consultation with the health care should be done in case of depression therapy change.
Tending to rest indications are of basic significance to recuperation from wretchedness. Make
sure to talk about any rest issues that persevere as disposition improves. Such issues may flag the
nearness of a hidden rest issue.
Pharmacology treatment
mind in numerous patients, yet they may likewise cause or compound sleep deprivation.
• Tricyclic antidepressants – tricyclic antidepressants are commonly steadying, yet they
may likewise convey genuine reactions, for example, hypertension.
• Mood settling anticonvulsants and lithium – these medications are usually used to treat
bipolar confusion.
Notwithstanding the above treatment choices, patients who experience the ill effects of sadness
may use bright light therapy (Murray, et al 2011). Light treatment may include presentation to
normal (light from the sun) or treatment with a light box. Light treatment is viewed as safe,
however little proof exists to help its adequacy at treating depression or different types of sleep
problems.
Patients should be advised that treating depression related sleeping problems often take a lot of
time. Medication usually take weeks in order to take full effects and patients may require to try
out various drugs in order to establish the most convenient one. Patients should not stop taking
the medication since symptom s might arise and increase causing other side effects. Proper
consultation with the health care should be done in case of depression therapy change.
Tending to rest indications are of basic significance to recuperation from wretchedness. Make
sure to talk about any rest issues that persevere as disposition improves. Such issues may flag the
nearness of a hidden rest issue.
Pharmacology treatment
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Albeit both sadness and sleep deprivation can be treated without medications, there are
pharmacological intercessions for both, and not incidentally, both can be tended to with
antidepressants (Shear, et al, 2011). The most well-known stimulant prescriptions today are
specific serotonin reuptake inhibitors (SSRIs). Those with a sleeping disorder who begin taking
one of those medications regularly discover help for their sleeping problems.
The pharmacological treatment for idiopathic hypersomnia is generally a stimulant – something
that works inverse of dozing pills. That is the reason it is imperative for specialists to assess
whether long-sleeping individual patients may have depression and be a superior participant for
existing anti-depressant medication.
CPAP treatment
Sadeh, (2011) States that patients with obstructive sleeping apnea can be helped using
continuous positive airway pressure (CPAP) system. These are incredibly successful for treating
OSA and related a sleeping disorder – and evidently depression, as well. People with co-sullen
dejection demonstrated noteworthy improvement each time after f utilizing this particular
treatment gadget.
Individual with OSA and sadness should be watchful about taking tricyclic antidepressants, since
narcotics can intensify indications of OSA.
Coping
Depression and lack of sleep can be unpleasant and depleting. It can likewise make an individual
to feel defenseless and sad. In addition to treating the problem with medical and mental health
specialist, the following are other treatment advices that are important for individual to cope with
pharmacological intercessions for both, and not incidentally, both can be tended to with
antidepressants (Shear, et al, 2011). The most well-known stimulant prescriptions today are
specific serotonin reuptake inhibitors (SSRIs). Those with a sleeping disorder who begin taking
one of those medications regularly discover help for their sleeping problems.
The pharmacological treatment for idiopathic hypersomnia is generally a stimulant – something
that works inverse of dozing pills. That is the reason it is imperative for specialists to assess
whether long-sleeping individual patients may have depression and be a superior participant for
existing anti-depressant medication.
CPAP treatment
Sadeh, (2011) States that patients with obstructive sleeping apnea can be helped using
continuous positive airway pressure (CPAP) system. These are incredibly successful for treating
OSA and related a sleeping disorder – and evidently depression, as well. People with co-sullen
dejection demonstrated noteworthy improvement each time after f utilizing this particular
treatment gadget.
Individual with OSA and sadness should be watchful about taking tricyclic antidepressants, since
narcotics can intensify indications of OSA.
Coping
Depression and lack of sleep can be unpleasant and depleting. It can likewise make an individual
to feel defenseless and sad. In addition to treating the problem with medical and mental health
specialist, the following are other treatment advices that are important for individual to cope with
depression and eventually be able to solve their sleeping problems( van Mill,
Hoogendijk,Vogelzangs, N., van Dyck, & Penninx, 2010).
• Keep a customary sleep/wake plan
• Get into brilliant light not long after waking up each morning
• Get some type of activity consistently
• Avoid afternoon sleep in the event that the patient have evening time sleeping disorder
• Limit caffeine and liquor
Eating of a healthy and mood boosting diet
What people eat definitely have a direct impact on the way they perceive or feel. A person with
depression is advised to go for a decent eating routine of low-fat protein, complex starches, and
foods grown from the ground. A person should lessen eating of food substances that can
unfavorably influence the cerebrum and state of mind, for example, caffeine, liquor, Tran’s fats,
soaked fats, and nourishments with abnormal amounts of synthetic additives or hormones.
A person should try not to skip dinners. Going excessively long between suppers can make a
person feel crabby and tired, so expect to eat something somewhere around each three to four
hours.
Limit sugar .Concentrate on complex starches. Sustenance’s, for example, prepared potatoes,
entire wheat pasta, oats, and entire grain breads can help serotonin levels without effects (Wulff,
Gatti, Wettstein, & Foster,2010).
Lift your nutrients, eat more citrus organic product, verdant greens, beans, chicken, and eggs.
Attempt super wealthy supplements that can help mind-set, for example, bananas, dark colored
Hoogendijk,Vogelzangs, N., van Dyck, & Penninx, 2010).
• Keep a customary sleep/wake plan
• Get into brilliant light not long after waking up each morning
• Get some type of activity consistently
• Avoid afternoon sleep in the event that the patient have evening time sleeping disorder
• Limit caffeine and liquor
Eating of a healthy and mood boosting diet
What people eat definitely have a direct impact on the way they perceive or feel. A person with
depression is advised to go for a decent eating routine of low-fat protein, complex starches, and
foods grown from the ground. A person should lessen eating of food substances that can
unfavorably influence the cerebrum and state of mind, for example, caffeine, liquor, Tran’s fats,
soaked fats, and nourishments with abnormal amounts of synthetic additives or hormones.
A person should try not to skip dinners. Going excessively long between suppers can make a
person feel crabby and tired, so expect to eat something somewhere around each three to four
hours.
Limit sugar .Concentrate on complex starches. Sustenance’s, for example, prepared potatoes,
entire wheat pasta, oats, and entire grain breads can help serotonin levels without effects (Wulff,
Gatti, Wettstein, & Foster,2010).
Lift your nutrients, eat more citrus organic product, verdant greens, beans, chicken, and eggs.
Attempt super wealthy supplements that can help mind-set, for example, bananas, dark colored
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.