Using realist synthesis to understand the mechanisms of interprofessional teamwork in health and social care
VerifiedAdded on 2023/06/10
|7
|7593
|384
AI Summary
This article introduces realist synthesis and its approach to identifying and testing the underpinning processes (or mechanisms) that make an intervention work, the contexts that trigger those mechanisms and their subsequent outcomes. A realist synthesis of the evidence on interprofessional teamwork is described. Thirteen mechanisms were identified in the synthesis and findings for one mechanism, called ‘‘Support and value’’ are presented in this paper.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

http://informahealthcare.com/jic
ISSN:1356-1820 (print),1469-9567 (electronic)
J Interprof Care,2014;28(6):501–506
! 2014 Informa UK Ltd.DOI:10.3109/13561820.2014.939744
ORIGINAL ARTICLE
Using realist synthesis to understand the mechanisms of
interprofessionalteamwork in health and social care
Gillian Hewitt1, Sarah Sims2 and Ruth Harris2
1Cardiff Schoolof SocialSciences,Cardiff University,Cardiff,UK and2Faculty of Health,SocialCare and Education,Kingston University and
St George’s,University of London,Kingston Upon Thames,Surrey,UK
Abstract
Realistsynthesisoffersa novel and innovative way to interrogate the large literature on
interprofessionalteamwork in health and socialcare teams.This article introducesrealist
synthesisand its approach to identifying and testing theunderpinning processes(or
‘‘mechanisms’’)that make an intervention work,the contexts that trigger those mechanisms
and their subsequentoutcomes.A realist synthesisof the evidence on interprofessional
teamwork is described.Thirteen mechanisms were identified in the synthesis and findings for
one mechanism,called ‘‘Support and value’’are presented in this paper.The evidence for the
other twelve mechanisms (‘‘collaboration and coordination’’, ‘‘pooling of resources’’, ‘‘individual
learning’’,‘‘role blurring’’,‘‘efficient,open and equitable communication’’,‘‘tacticalcommuni-
cation’’, ‘‘shared responsibility and influence’’, ‘‘team behavioural norms’’, ‘‘shared responsibility
and influence’’,‘‘critically reviewing performance and decisions’’,‘‘generating and implement-
ing new ideas’’and ‘‘leadership’’)are reported in a furtherthree papers in this series.The
‘‘support and value’’mechanism referred to the ways in which team members supported one
another,respected other’s skills and abilities and valued each other’s contributions.‘‘Support
and value’’was presentin some,but far from all,teams and a numberof contexts that
explained thisvariation were identified.The article concludeswith a discussion of the
challenges and benefits of undertaking this realist synthesis.
Keywords
Interprofessionalpractice,realist synthesis,
teamwork
History
Received 5 November 2013
Revised 20 February 2014
Accepted 25 June 2014
Published online 21 July 2014
Introduction
Interprofessionalteams are a common feature of modern health
and social care,where they are perceived as a means to enhance
care quality and efficiency and patientsafety and therefore
strongly advocated within the healthcare policy of many countries
(Reeves,Lewin, Espin, & Zwarenstein,2010).Increasingly,
patientshave complex and long term conditionsthatrequire
treatments from a range of health professionals and good quality
care is dependent upon those professionals collaborating together
in teams.Although there are numerous definitions of ‘‘teams’’,
a generalconsensus exists thatthey are ‘‘comprised of a small,
manageable number of members with an appropriate mix of skills
and expertise, who are all committed to a meaningful purpose and
have collective responsibility to achieve performance objectives
and outcomes’’(Harriset al., 2013,p. 22). A large body of
research on interprofessional teamwork exists,much of which is
descriptive and unempirical(Reeves etal., 2010).Furthermore,
the rapidly changing health and social care landscape in the UK
means the need persists for innovative research thatwill inform
the developmentand managementof increasinglycomplex
interprofessionalteams.The authorsand colleaguestherefore
adopted therealistapproach (Pawson & Tilley,1997)in a
multi-method study ofinterprofessionalteamwork along the
stroke care pathway (the Teams Study) (Harris et al.,2013).
The realistapproach wasdeveloped to evaluatecomplex
social interventions,namelyprogrammesthat offer one or
moreresources,but depend upon people’sresponsesto the
resourceto generatethe anticipatedoutcomes(Pawson,
Greenhalgh,Harvey,& Walshe,2005).Interprofessionalteam-
work was considered to be a complex social intervention becau
it provides individual professionals with a resource (the team a
its members),butthe impacts of teamwork depend on the ways
in which individualsrespond to theirteam membership.For
example,therapists and nurses might respond to being in a team
together by sharing their knowledge of a patient more frequent
or in greaterdepth.Such a responseis referredto as a
‘‘mechanism’’and realist researchersseek to identify the
mechanismsthat underpin complex social interventions.
Contexts thatdetermine whetheror notmechanisms are ‘‘trig-
gered’’ for particular groups of people or in particular situations
are also identified,along with context-dependentoutcomes.
Context-mechanism-outcome (CMO) configurations can then be
generated and used to address the realist question of, ‘‘What is
about teamwork that works for whom, in what circumstances a
why?’’(Pawson etal., 2005).This novelway ofinterrogating
interprofessional teamwork was used to identify the mechanism
of teamwork,thereby creating a conceptualframework foruse
in this study and others. As far as we are aware, this is the first
of the realistsynthesis method in the teamwork literature and
builds on earlier work with the method undertaken by Hammick
Correspondence:Professor Ruth Harris,Faculty of Health,SocialCare
and Education,Kingston University and StGeorge’s,University of
London,Kingston Hill Campus,Kingston Upon Thames,KT2 7LB,
Surrey,UK. E-mail: Ruth.Harris@sgul.kingston.ac.uk
ISSN:1356-1820 (print),1469-9567 (electronic)
J Interprof Care,2014;28(6):501–506
! 2014 Informa UK Ltd.DOI:10.3109/13561820.2014.939744
ORIGINAL ARTICLE
Using realist synthesis to understand the mechanisms of
interprofessionalteamwork in health and social care
Gillian Hewitt1, Sarah Sims2 and Ruth Harris2
1Cardiff Schoolof SocialSciences,Cardiff University,Cardiff,UK and2Faculty of Health,SocialCare and Education,Kingston University and
St George’s,University of London,Kingston Upon Thames,Surrey,UK
Abstract
Realistsynthesisoffersa novel and innovative way to interrogate the large literature on
interprofessionalteamwork in health and socialcare teams.This article introducesrealist
synthesisand its approach to identifying and testing theunderpinning processes(or
‘‘mechanisms’’)that make an intervention work,the contexts that trigger those mechanisms
and their subsequentoutcomes.A realist synthesisof the evidence on interprofessional
teamwork is described.Thirteen mechanisms were identified in the synthesis and findings for
one mechanism,called ‘‘Support and value’’are presented in this paper.The evidence for the
other twelve mechanisms (‘‘collaboration and coordination’’, ‘‘pooling of resources’’, ‘‘individual
learning’’,‘‘role blurring’’,‘‘efficient,open and equitable communication’’,‘‘tacticalcommuni-
cation’’, ‘‘shared responsibility and influence’’, ‘‘team behavioural norms’’, ‘‘shared responsibility
and influence’’,‘‘critically reviewing performance and decisions’’,‘‘generating and implement-
ing new ideas’’and ‘‘leadership’’)are reported in a furtherthree papers in this series.The
‘‘support and value’’mechanism referred to the ways in which team members supported one
another,respected other’s skills and abilities and valued each other’s contributions.‘‘Support
and value’’was presentin some,but far from all,teams and a numberof contexts that
explained thisvariation were identified.The article concludeswith a discussion of the
challenges and benefits of undertaking this realist synthesis.
Keywords
Interprofessionalpractice,realist synthesis,
teamwork
History
Received 5 November 2013
Revised 20 February 2014
Accepted 25 June 2014
Published online 21 July 2014
Introduction
Interprofessionalteams are a common feature of modern health
and social care,where they are perceived as a means to enhance
care quality and efficiency and patientsafety and therefore
strongly advocated within the healthcare policy of many countries
(Reeves,Lewin, Espin, & Zwarenstein,2010).Increasingly,
patientshave complex and long term conditionsthatrequire
treatments from a range of health professionals and good quality
care is dependent upon those professionals collaborating together
in teams.Although there are numerous definitions of ‘‘teams’’,
a generalconsensus exists thatthey are ‘‘comprised of a small,
manageable number of members with an appropriate mix of skills
and expertise, who are all committed to a meaningful purpose and
have collective responsibility to achieve performance objectives
and outcomes’’(Harriset al., 2013,p. 22). A large body of
research on interprofessional teamwork exists,much of which is
descriptive and unempirical(Reeves etal., 2010).Furthermore,
the rapidly changing health and social care landscape in the UK
means the need persists for innovative research thatwill inform
the developmentand managementof increasinglycomplex
interprofessionalteams.The authorsand colleaguestherefore
adopted therealistapproach (Pawson & Tilley,1997)in a
multi-method study ofinterprofessionalteamwork along the
stroke care pathway (the Teams Study) (Harris et al.,2013).
The realistapproach wasdeveloped to evaluatecomplex
social interventions,namelyprogrammesthat offer one or
moreresources,but depend upon people’sresponsesto the
resourceto generatethe anticipatedoutcomes(Pawson,
Greenhalgh,Harvey,& Walshe,2005).Interprofessionalteam-
work was considered to be a complex social intervention becau
it provides individual professionals with a resource (the team a
its members),butthe impacts of teamwork depend on the ways
in which individualsrespond to theirteam membership.For
example,therapists and nurses might respond to being in a team
together by sharing their knowledge of a patient more frequent
or in greaterdepth.Such a responseis referredto as a
‘‘mechanism’’and realist researchersseek to identify the
mechanismsthat underpin complex social interventions.
Contexts thatdetermine whetheror notmechanisms are ‘‘trig-
gered’’ for particular groups of people or in particular situations
are also identified,along with context-dependentoutcomes.
Context-mechanism-outcome (CMO) configurations can then be
generated and used to address the realist question of, ‘‘What is
about teamwork that works for whom, in what circumstances a
why?’’(Pawson etal., 2005).This novelway ofinterrogating
interprofessional teamwork was used to identify the mechanism
of teamwork,thereby creating a conceptualframework foruse
in this study and others. As far as we are aware, this is the first
of the realistsynthesis method in the teamwork literature and
builds on earlier work with the method undertaken by Hammick
Correspondence:Professor Ruth Harris,Faculty of Health,SocialCare
and Education,Kingston University and StGeorge’s,University of
London,Kingston Hill Campus,Kingston Upon Thames,KT2 7LB,
Surrey,UK. E-mail: Ruth.Harris@sgul.kingston.ac.uk
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Freeth,Koppel,Reeves,and Barr(2007)on interprofessional
education.
This article introducesthe realistapproachto evidence
synthesis and describes the realistsynthesis undertaken forthe
Teams Study.It presents findings for one mechanism (‘‘support
and value’’)as an example and concludes with reflections on
the process of undertaking a realist synthesis.This is the first in
a seriesof four articlesreporting the findingsof the realist
synthesis.The secondarticle reportsthe findingsfor the
‘‘collaborationand coordination’’,‘‘pooling of resources’’,
Individuallearning’’and ‘‘role blurring’’mechanisms(Sims,
Hewitt,& Harris, in press a). The third articlereportsthe
‘‘efficient,open and equitable communication’’,‘‘tacticalcom-
munication’’,‘‘shared responsibility and influence’’ and ‘‘team
behaviouralnorms’’mechanisms(Hewitt,Sims,& Harris, in
press). The fourth and final article reports ‘‘shared responsibility
and influence’’,‘‘critically reviewing performanceand deci-
sions’’,‘‘generating and implementing new ideas’’ and ‘‘leader-
ship’’ mechanisms drawing overall conclusions from the findings
of the synthesis and their implications for healthcare delivery and
further research (Sims,Hewitt, & Harris,in press b).
Realist synthesis
Realistsynthesis identifies and tests CMO configurations using
evidence from the literature.For a comprehensive description
readers are referred to Pawson,Greenhalgh,Harvey,and Walshe
(2004).Briefly,realist synthesis:
Identifies the mechanisms thatprogramme designers thought
would underpin the intervention.
Tests those mechanisms using empiricalevidence from the
literature.
Identifies and tests other,unforeseen mechanisms thatmight
underpin the intervention once it is implemented.
Explores which contexts ‘‘trigger’’ the mechanisms for which
people and in which circumstances.
Identifies positive and negative outcomes of the intervention,
depending on which contextsand mechanismsare present
(CMO configurations).
Synthesisesthe evidence in orderto refine the theory the
intervention rests on.
Realist synthesis is a more flexible and iterative process than
conventional systematic review. Its focus, for example, is directed
by the emerging evidence rather than being tightly defined at the
outset and the reviewer iteratively develops the search strategy as
the review progresses, meaning multiple, responsive searches are
conducted.There are,however,two main stages to the search
process.The first identifiesthe purportedmechanismsthat
underpin the intervention,using diverse sources such as policy
documents,editorials,otherreviewsand interviewswith key
informants. The second looks for empirical evidence that supports
or refutes the mechanisms.The reviewer now looks for contexts
thattriggerthe purported mechanisms and the outcomesthey
generate and also looksfor unforeseen mechanismsand their
associated contexts and outcomes.
Anotherarea in which realistsynthesis differs significantly
from conventional systematic review is in its approach to quality
appraisalof potentially relevantstudies.Instead ofassessing
methodologicalquality and judging a study’s acceptability for
inclusion on that basis, the realist reviewer looks at the quality of
the inference the author is making from their data and asks if their
inference makes a credible contribution to the mechanism being
tested (see Pawson,2006 forfurtherdetail).Realistsynthesis
thereforedrawson a much wider rangeof evidencethan
conventionalsystematic review and makes criticaland cautious
use of ‘‘methodologically weak’’ studies.
Methods
The realist synthesis,conducted in 2008–2010, aimed to identify
and explore the mechanisms of interprofessionalteamwork.The
initial review question was:‘‘Through whatmechanisms does
interprofessionalteam workingaffectclinical outcomesand
patientexperience,and how does contextinfluencethose
mechanisms?’’
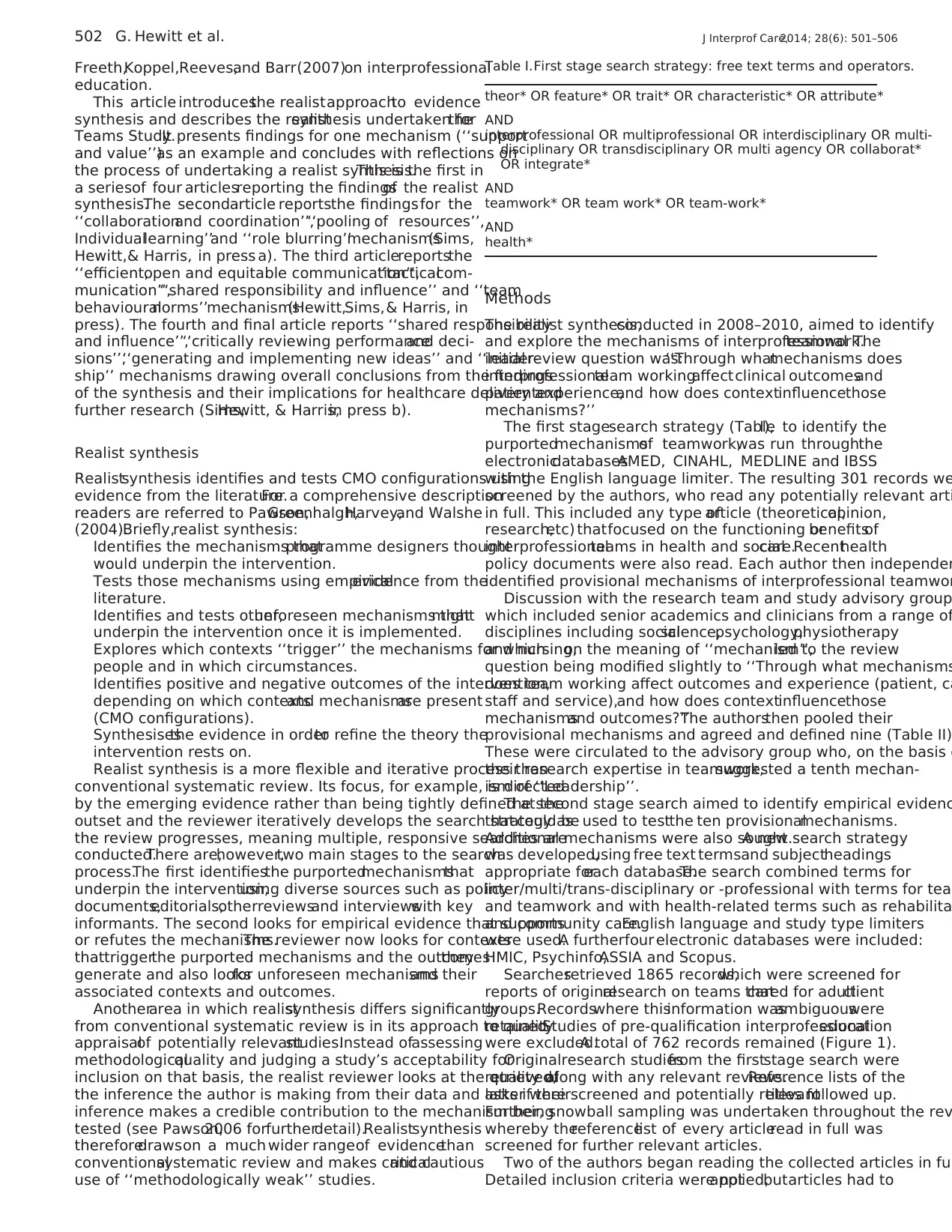
The first stagesearch strategy (TableI), to identify the
purportedmechanismsof teamwork,was run throughthe
electronicdatabasesAMED, CINAHL, MEDLINE and IBSS
with the English language limiter. The resulting 301 records we
screened by the authors, who read any potentially relevant arti
in full. This included any type ofarticle (theoretical,opinion,
research,etc) thatfocused on the functioning orbenefitsof
interprofessionalteams in health and socialcare.Recenthealth
policy documents were also read. Each author then independen
identified provisional mechanisms of interprofessional teamwor
Discussion with the research team and study advisory group
which included senior academics and clinicians from a range of
disciplines including socialscience,psychology,physiotherapy
and nursing,on the meaning of ‘‘mechanism’’,led to the review
question being modified slightly to ‘‘Through what mechanisms
does team working affect outcomes and experience (patient, ca
staff and service),and how does contextinfluencethose
mechanismsand outcomes?’’The authorsthen pooled their
provisional mechanisms and agreed and defined nine (Table II)
These were circulated to the advisory group who, on the basis o
their research expertise in teamwork,suggested a tenth mechan-
ism of ‘‘Leadership’’.
The second stage search aimed to identify empirical evidenc
that could be used to testthe ten provisionalmechanisms.
Additional mechanisms were also sought.A new search strategy
was developed,using free text termsand subjectheadings
appropriate foreach database.The search combined terms for
inter/multi/trans-disciplinary or -professional with terms for tea
and teamwork and with health-related terms such as rehabilita
and community care.English language and study type limiters
were used.A furtherfour electronic databases were included:
HMIC, Psychinfo,ASSIA and Scopus.
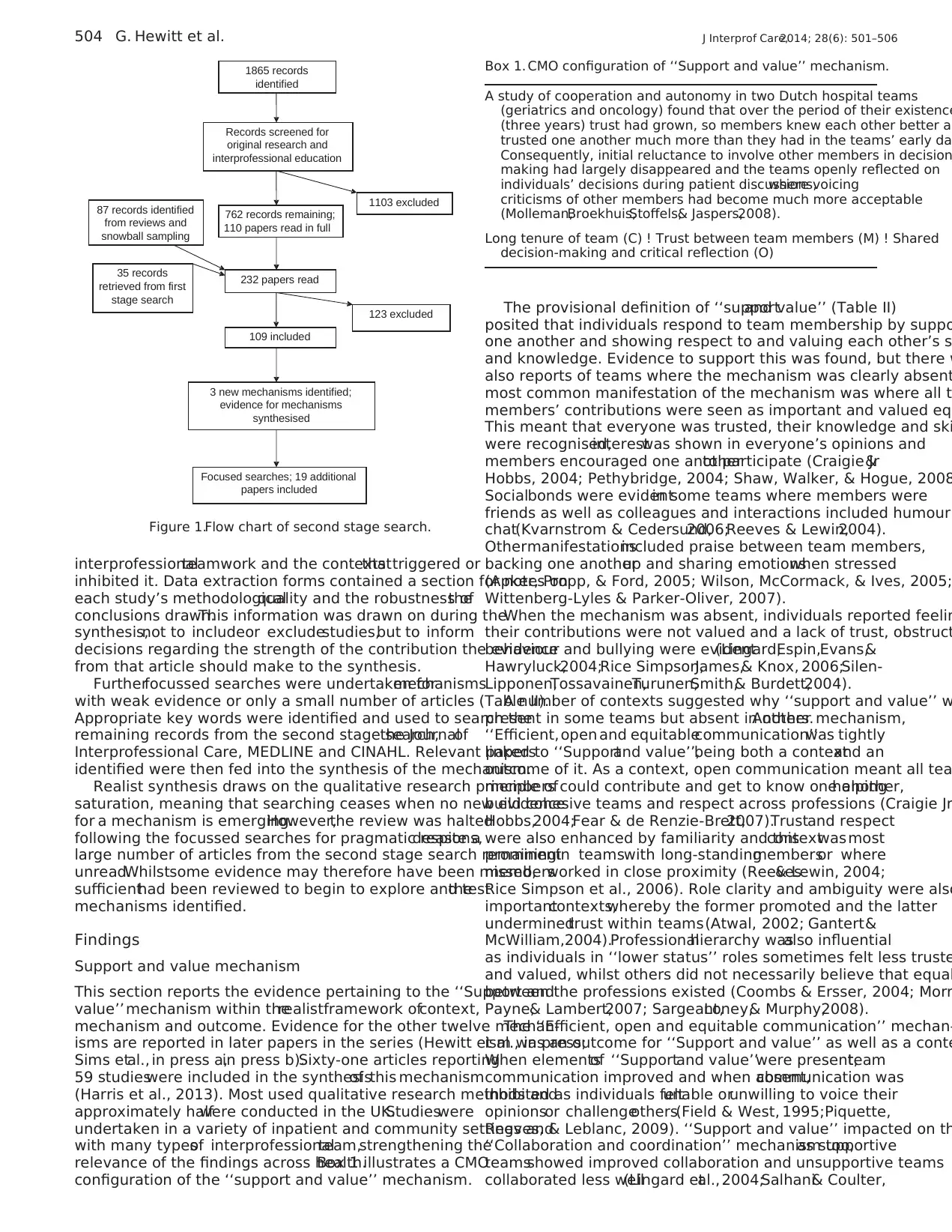
Searchesretrieved 1865 records,which were screened for
reports of originalresearch on teams thatcared for adultclient
groups.Recordswhere thisinformation wasambiguouswere
retained.Studies of pre-qualification interprofessionaleducation
were excluded.A total of 762 records remained (Figure 1).
Originalresearch studiesfrom the firststage search were
retrieved,along with any relevant reviews.Reference lists of the
latter were screened and potentially relevanttitles followed up.
Further, snowball sampling was undertaken throughout the rev
whereby thereferencelist of every articleread in full was
screened for further relevant articles.
Two of the authors began reading the collected articles in ful
Detailed inclusion criteria were notapplied,butarticles had to
Table I.First stage search strategy: free text terms and operators.
theor* OR feature* OR trait* OR characteristic* OR attribute*
AND
interprofessional OR multiprofessional OR interdisciplinary OR multi-
disciplinary OR transdisciplinary OR multi agency OR collaborat*
OR integrate*
AND
teamwork* OR team work* OR team-work*
AND
health*
502 G. Hewitt et al. J Interprof Care,2014; 28(6): 501–506
education.
This article introducesthe realistapproachto evidence
synthesis and describes the realistsynthesis undertaken forthe
Teams Study.It presents findings for one mechanism (‘‘support
and value’’)as an example and concludes with reflections on
the process of undertaking a realist synthesis.This is the first in
a seriesof four articlesreporting the findingsof the realist
synthesis.The secondarticle reportsthe findingsfor the
‘‘collaborationand coordination’’,‘‘pooling of resources’’,
Individuallearning’’and ‘‘role blurring’’mechanisms(Sims,
Hewitt,& Harris, in press a). The third articlereportsthe
‘‘efficient,open and equitable communication’’,‘‘tacticalcom-
munication’’,‘‘shared responsibility and influence’’ and ‘‘team
behaviouralnorms’’mechanisms(Hewitt,Sims,& Harris, in
press). The fourth and final article reports ‘‘shared responsibility
and influence’’,‘‘critically reviewing performanceand deci-
sions’’,‘‘generating and implementing new ideas’’ and ‘‘leader-
ship’’ mechanisms drawing overall conclusions from the findings
of the synthesis and their implications for healthcare delivery and
further research (Sims,Hewitt, & Harris,in press b).
Realist synthesis
Realistsynthesis identifies and tests CMO configurations using
evidence from the literature.For a comprehensive description
readers are referred to Pawson,Greenhalgh,Harvey,and Walshe
(2004).Briefly,realist synthesis:
Identifies the mechanisms thatprogramme designers thought
would underpin the intervention.
Tests those mechanisms using empiricalevidence from the
literature.
Identifies and tests other,unforeseen mechanisms thatmight
underpin the intervention once it is implemented.
Explores which contexts ‘‘trigger’’ the mechanisms for which
people and in which circumstances.
Identifies positive and negative outcomes of the intervention,
depending on which contextsand mechanismsare present
(CMO configurations).
Synthesisesthe evidence in orderto refine the theory the
intervention rests on.
Realist synthesis is a more flexible and iterative process than
conventional systematic review. Its focus, for example, is directed
by the emerging evidence rather than being tightly defined at the
outset and the reviewer iteratively develops the search strategy as
the review progresses, meaning multiple, responsive searches are
conducted.There are,however,two main stages to the search
process.The first identifiesthe purportedmechanismsthat
underpin the intervention,using diverse sources such as policy
documents,editorials,otherreviewsand interviewswith key
informants. The second looks for empirical evidence that supports
or refutes the mechanisms.The reviewer now looks for contexts
thattriggerthe purported mechanisms and the outcomesthey
generate and also looksfor unforeseen mechanismsand their
associated contexts and outcomes.
Anotherarea in which realistsynthesis differs significantly
from conventional systematic review is in its approach to quality
appraisalof potentially relevantstudies.Instead ofassessing
methodologicalquality and judging a study’s acceptability for
inclusion on that basis, the realist reviewer looks at the quality of
the inference the author is making from their data and asks if their
inference makes a credible contribution to the mechanism being
tested (see Pawson,2006 forfurtherdetail).Realistsynthesis
thereforedrawson a much wider rangeof evidencethan
conventionalsystematic review and makes criticaland cautious
use of ‘‘methodologically weak’’ studies.
Methods
The realist synthesis,conducted in 2008–2010, aimed to identify
and explore the mechanisms of interprofessionalteamwork.The
initial review question was:‘‘Through whatmechanisms does
interprofessionalteam workingaffectclinical outcomesand
patientexperience,and how does contextinfluencethose
mechanisms?’’
The first stagesearch strategy (TableI), to identify the
purportedmechanismsof teamwork,was run throughthe
electronicdatabasesAMED, CINAHL, MEDLINE and IBSS
with the English language limiter. The resulting 301 records we
screened by the authors, who read any potentially relevant arti
in full. This included any type ofarticle (theoretical,opinion,
research,etc) thatfocused on the functioning orbenefitsof
interprofessionalteams in health and socialcare.Recenthealth
policy documents were also read. Each author then independen
identified provisional mechanisms of interprofessional teamwor
Discussion with the research team and study advisory group
which included senior academics and clinicians from a range of
disciplines including socialscience,psychology,physiotherapy
and nursing,on the meaning of ‘‘mechanism’’,led to the review
question being modified slightly to ‘‘Through what mechanisms
does team working affect outcomes and experience (patient, ca
staff and service),and how does contextinfluencethose
mechanismsand outcomes?’’The authorsthen pooled their
provisional mechanisms and agreed and defined nine (Table II)
These were circulated to the advisory group who, on the basis o
their research expertise in teamwork,suggested a tenth mechan-
ism of ‘‘Leadership’’.
The second stage search aimed to identify empirical evidenc
that could be used to testthe ten provisionalmechanisms.
Additional mechanisms were also sought.A new search strategy
was developed,using free text termsand subjectheadings
appropriate foreach database.The search combined terms for
inter/multi/trans-disciplinary or -professional with terms for tea
and teamwork and with health-related terms such as rehabilita
and community care.English language and study type limiters
were used.A furtherfour electronic databases were included:
HMIC, Psychinfo,ASSIA and Scopus.
Searchesretrieved 1865 records,which were screened for
reports of originalresearch on teams thatcared for adultclient
groups.Recordswhere thisinformation wasambiguouswere
retained.Studies of pre-qualification interprofessionaleducation
were excluded.A total of 762 records remained (Figure 1).
Originalresearch studiesfrom the firststage search were
retrieved,along with any relevant reviews.Reference lists of the
latter were screened and potentially relevanttitles followed up.
Further, snowball sampling was undertaken throughout the rev
whereby thereferencelist of every articleread in full was
screened for further relevant articles.
Two of the authors began reading the collected articles in ful
Detailed inclusion criteria were notapplied,butarticles had to
Table I.First stage search strategy: free text terms and operators.
theor* OR feature* OR trait* OR characteristic* OR attribute*
AND
interprofessional OR multiprofessional OR interdisciplinary OR multi-
disciplinary OR transdisciplinary OR multi agency OR collaborat*
OR integrate*
AND
teamwork* OR team work* OR team-work*
AND
health*
502 G. Hewitt et al. J Interprof Care,2014; 28(6): 501–506
report empirical studies from the health literature that addressed
interprofessionalteamwork and wererelevantto one of the
provisional mechanisms or suggested a new mechanism. Bespoke
data extraction forms were designed to summarise articles and
record CMO configurationsidentified in thestudy findings.
Forms were also completed for excluded articles, with the reason
for exclusion recorded.Mostoften this was because the article
was not relevant,i.e. did not addressany mechanisms;other
reasons included lack of useful detail about mechanisms, unclear
methods and not reporting original research.
Early on, nine articles were read and discussed by the authors
to check consistency of data extraction. Discussion of all articles
read up to thatpointraised three more potentialmechanisms
(Table II) and these were defined and incorporated into the data
extraction form (Appendix).
As reading and data extraction progressed it became clear that
following the realistsynthesis method exactly as described by
Pawson etal. (2004)was too ambitiouswith the resources
available as numerous CMO configurations were being identified.
Instead,main findingspertainingto each mechanism were
summarised.Informationon contextsand on outcomesfor
patients,teams,staff and organisations was noted,but individual
CMO configurations (as in Box 1) were not recorded. A narrative
approach to synthesising the findings on mechanisms,contexts
and outcomes could then be adopted.The data extraction form
was amended accordingly.
After reviewing 232 articles,of which 109 were included
(Figure 1),evidence foreach mechanism wassynthesised by
drawing togetherthe information on contexts,mechanisms and
outcomes from the data extraction forms. The aim was to test a
develop the provisional definitions of the mechanisms (Table II)
Synthesis of the evidence started atthis pointratherthan after
reviewing all 762 records because the realist synthesis method
an iterative and cyclicalprocess,where reading,searching and
synthesis occur together and inform each other.
For each mechanism, relevant sections of articles were re-re
and similarities and differences in their findings sought in order
build a comprehensive description of the mechanism,its role in
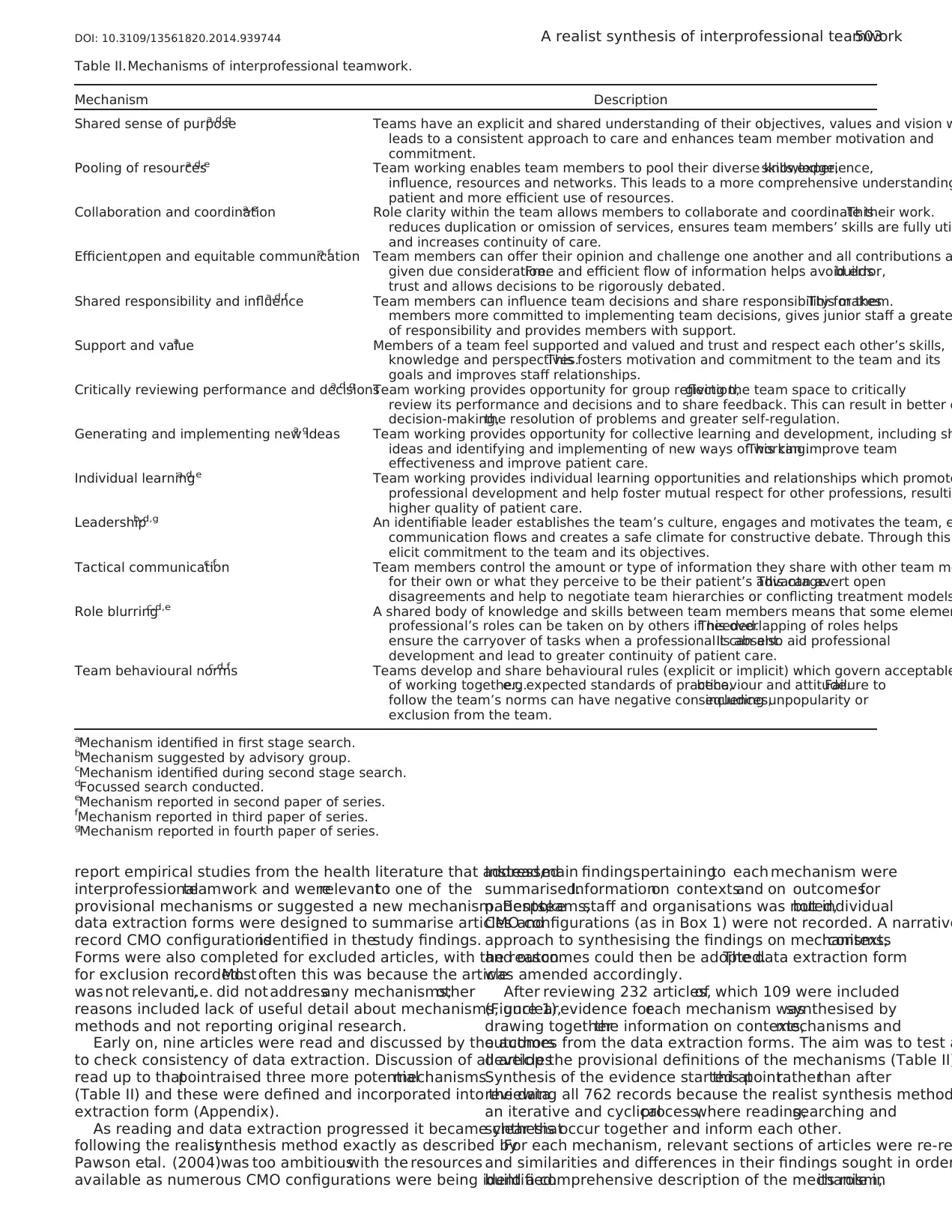
Table II.Mechanisms of interprofessional teamwork.
Mechanism Description
Shared sense of purposea,d,g Teams have an explicit and shared understanding of their objectives, values and vision w
leads to a consistent approach to care and enhances team member motivation and
commitment.
Pooling of resourcesa,d,e Team working enables team members to pool their diverse knowledge,skills,experience,
influence, resources and networks. This leads to a more comprehensive understanding
patient and more efficient use of resources.
Collaboration and coordinationa,e Role clarity within the team allows members to collaborate and coordinate their work.This
reduces duplication or omission of services, ensures team members’ skills are fully uti
and increases continuity of care.
Efficient,open and equitable communicationa,f Team members can offer their opinion and challenge one another and all contributions a
given due consideration.Free and efficient flow of information helps avoid error,builds
trust and allows decisions to be rigorously debated.
Shared responsibility and influencea,d,f Team members can influence team decisions and share responsibility for them.This makes
members more committed to implementing team decisions, gives junior staff a greate
of responsibility and provides members with support.
Support and valuea Members of a team feel supported and valued and trust and respect each other’s skills,
knowledge and perspectives.This fosters motivation and commitment to the team and its
goals and improves staff relationships.
Critically reviewing performance and decisionsa,d,g Team working provides opportunity for group reflection,giving the team space to critically
review its performance and decisions and to share feedback. This can result in better q
decision-making,the resolution of problems and greater self-regulation.
Generating and implementing new ideasa,g Team working provides opportunity for collective learning and development, including sh
ideas and identifying and implementing of new ways of working.This can improve team
effectiveness and improve patient care.
Individual learninga,d,e Team working provides individual learning opportunities and relationships which promote
professional development and help foster mutual respect for other professions, resulti
higher quality of patient care.
Leadershipb,d,g An identifiable leader establishes the team’s culture, engages and motivates the team, e
communication flows and creates a safe climate for constructive debate. Through this
elicit commitment to the team and its objectives.
Tactical communicationc,f Team members control the amount or type of information they share with other team me
for their own or what they perceive to be their patient’s advantage.This can avert open
disagreements and help to negotiate team hierarchies or conflicting treatment models
Role blurringc,d,e A shared body of knowledge and skills between team members means that some elemen
professional’s roles can be taken on by others if needed.This overlapping of roles helps
ensure the carryover of tasks when a professional is absent.It can also aid professional
development and lead to greater continuity of patient care.
Team behavioural normsc,d,f Teams develop and share behavioural rules (explicit or implicit) which govern acceptable
of working together,e.g.expected standards of practice,behaviour and attitude.Failure to
follow the team’s norms can have negative consequences,including unpopularity or
exclusion from the team.
aMechanism identified in first stage search.
bMechanism suggested by advisory group.
cMechanism identified during second stage search.
dFocussed search conducted.
eMechanism reported in second paper of series.
fMechanism reported in third paper of series.
gMechanism reported in fourth paper of series.
DOI: 10.3109/13561820.2014.939744 A realist synthesis of interprofessional teamwork503
interprofessionalteamwork and wererelevantto one of the
provisional mechanisms or suggested a new mechanism. Bespoke
data extraction forms were designed to summarise articles and
record CMO configurationsidentified in thestudy findings.
Forms were also completed for excluded articles, with the reason
for exclusion recorded.Mostoften this was because the article
was not relevant,i.e. did not addressany mechanisms;other
reasons included lack of useful detail about mechanisms, unclear
methods and not reporting original research.
Early on, nine articles were read and discussed by the authors
to check consistency of data extraction. Discussion of all articles
read up to thatpointraised three more potentialmechanisms
(Table II) and these were defined and incorporated into the data
extraction form (Appendix).
As reading and data extraction progressed it became clear that
following the realistsynthesis method exactly as described by
Pawson etal. (2004)was too ambitiouswith the resources
available as numerous CMO configurations were being identified.
Instead,main findingspertainingto each mechanism were
summarised.Informationon contextsand on outcomesfor
patients,teams,staff and organisations was noted,but individual
CMO configurations (as in Box 1) were not recorded. A narrative
approach to synthesising the findings on mechanisms,contexts
and outcomes could then be adopted.The data extraction form
was amended accordingly.
After reviewing 232 articles,of which 109 were included
(Figure 1),evidence foreach mechanism wassynthesised by
drawing togetherthe information on contexts,mechanisms and
outcomes from the data extraction forms. The aim was to test a
develop the provisional definitions of the mechanisms (Table II)
Synthesis of the evidence started atthis pointratherthan after
reviewing all 762 records because the realist synthesis method
an iterative and cyclicalprocess,where reading,searching and
synthesis occur together and inform each other.
For each mechanism, relevant sections of articles were re-re
and similarities and differences in their findings sought in order
build a comprehensive description of the mechanism,its role in
Table II.Mechanisms of interprofessional teamwork.
Mechanism Description
Shared sense of purposea,d,g Teams have an explicit and shared understanding of their objectives, values and vision w
leads to a consistent approach to care and enhances team member motivation and
commitment.
Pooling of resourcesa,d,e Team working enables team members to pool their diverse knowledge,skills,experience,
influence, resources and networks. This leads to a more comprehensive understanding
patient and more efficient use of resources.
Collaboration and coordinationa,e Role clarity within the team allows members to collaborate and coordinate their work.This
reduces duplication or omission of services, ensures team members’ skills are fully uti
and increases continuity of care.
Efficient,open and equitable communicationa,f Team members can offer their opinion and challenge one another and all contributions a
given due consideration.Free and efficient flow of information helps avoid error,builds
trust and allows decisions to be rigorously debated.
Shared responsibility and influencea,d,f Team members can influence team decisions and share responsibility for them.This makes
members more committed to implementing team decisions, gives junior staff a greate
of responsibility and provides members with support.
Support and valuea Members of a team feel supported and valued and trust and respect each other’s skills,
knowledge and perspectives.This fosters motivation and commitment to the team and its
goals and improves staff relationships.
Critically reviewing performance and decisionsa,d,g Team working provides opportunity for group reflection,giving the team space to critically
review its performance and decisions and to share feedback. This can result in better q
decision-making,the resolution of problems and greater self-regulation.
Generating and implementing new ideasa,g Team working provides opportunity for collective learning and development, including sh
ideas and identifying and implementing of new ways of working.This can improve team
effectiveness and improve patient care.
Individual learninga,d,e Team working provides individual learning opportunities and relationships which promote
professional development and help foster mutual respect for other professions, resulti
higher quality of patient care.
Leadershipb,d,g An identifiable leader establishes the team’s culture, engages and motivates the team, e
communication flows and creates a safe climate for constructive debate. Through this
elicit commitment to the team and its objectives.
Tactical communicationc,f Team members control the amount or type of information they share with other team me
for their own or what they perceive to be their patient’s advantage.This can avert open
disagreements and help to negotiate team hierarchies or conflicting treatment models
Role blurringc,d,e A shared body of knowledge and skills between team members means that some elemen
professional’s roles can be taken on by others if needed.This overlapping of roles helps
ensure the carryover of tasks when a professional is absent.It can also aid professional
development and lead to greater continuity of patient care.
Team behavioural normsc,d,f Teams develop and share behavioural rules (explicit or implicit) which govern acceptable
of working together,e.g.expected standards of practice,behaviour and attitude.Failure to
follow the team’s norms can have negative consequences,including unpopularity or
exclusion from the team.
aMechanism identified in first stage search.
bMechanism suggested by advisory group.
cMechanism identified during second stage search.
dFocussed search conducted.
eMechanism reported in second paper of series.
fMechanism reported in third paper of series.
gMechanism reported in fourth paper of series.
DOI: 10.3109/13561820.2014.939744 A realist synthesis of interprofessional teamwork503
interprofessionalteamwork and the contextsthattriggered or
inhibited it. Data extraction forms contained a section for notes on
each study’s methodologicalquality and the robustness ofthe
conclusions drawn.This information was drawn on during the
synthesis,not to includeor excludestudies,but to inform
decisions regarding the strength of the contribution the evidence
from that article should make to the synthesis.
Furtherfocussed searches were undertaken formechanisms
with weak evidence or only a small number of articles (Table II).
Appropriate key words were identified and used to search the
remaining records from the second stage search,the Journalof
Interprofessional Care, MEDLINE and CINAHL. Relevant papers
identified were then fed into the synthesis of the mechanism.
Realist synthesis draws on the qualitative research principle of
saturation, meaning that searching ceases when no new evidence
for a mechanism is emerging.However,the review was halted
following the focussed searches for pragmatic reasons,despite a
large number of articles from the second stage search remaining
unread.Whilstsome evidence may therefore have been missed,
sufficienthad been reviewed to begin to explore and testthe
mechanisms identified.
Findings
Support and value mechanism
This section reports the evidence pertaining to the ‘‘Support and
value’’ mechanism within therealistframework ofcontext,
mechanism and outcome. Evidence for the other twelve mechan-
isms are reported in later papers in the series (Hewitt et al., in press;
Sims etal., in press a,in press b).Sixty-one articles reporting
59 studieswere included in the synthesisof this mechanism
(Harris et al., 2013). Most used qualitative research methods and
approximately halfwere conducted in the UK.Studieswere
undertaken in a variety of inpatient and community settings and
with many typesof interprofessionalteam,strengthening the
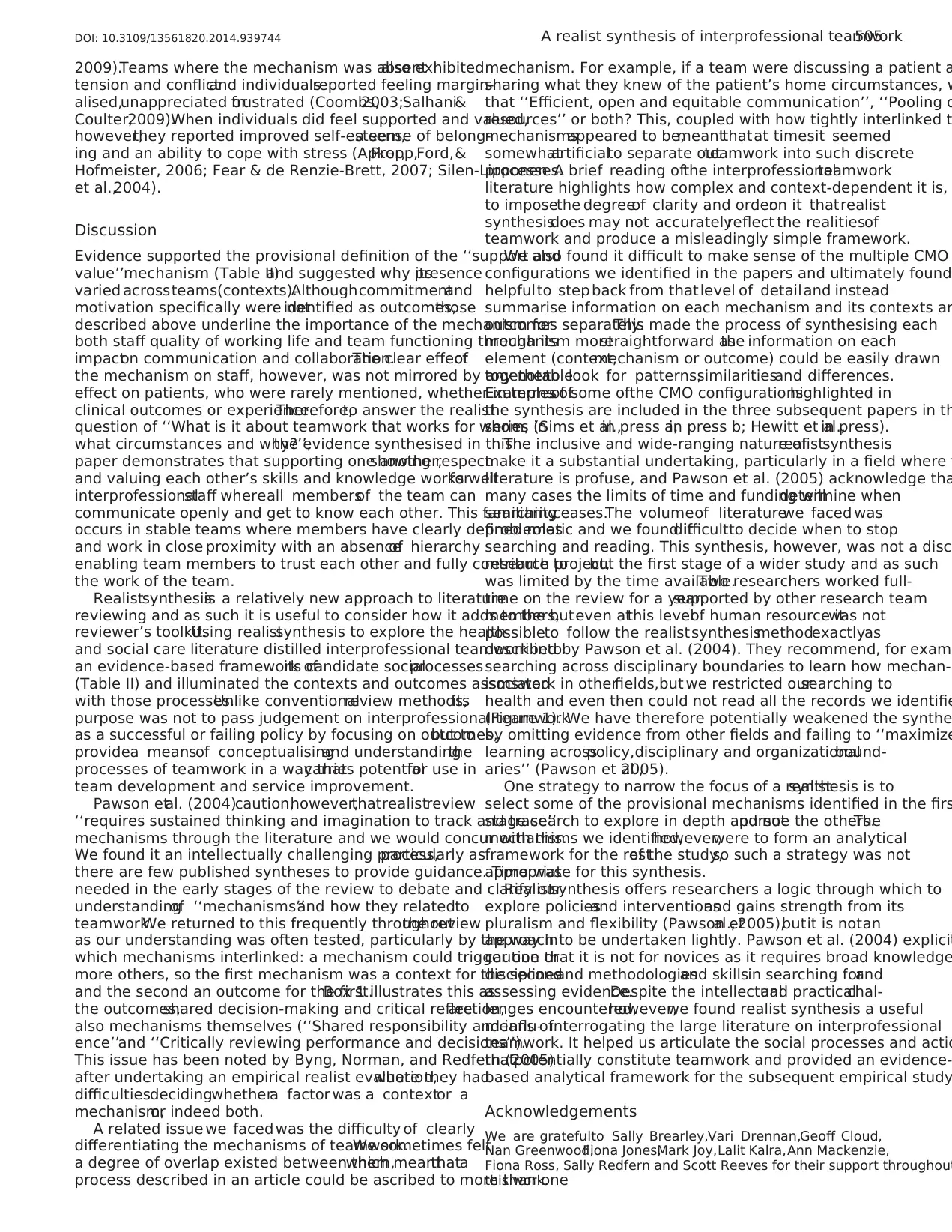
relevance of the findings across health.Box 1 illustrates a CMO
configuration of the ‘‘support and value’’ mechanism.
The provisional definition of ‘‘supportand value’’ (Table II)
posited that individuals respond to team membership by suppo
one another and showing respect to and valuing each other’s s
and knowledge. Evidence to support this was found, but there w
also reports of teams where the mechanism was clearly absent
most common manifestation of the mechanism was where all t
members’ contributions were seen as important and valued eq
This meant that everyone was trusted, their knowledge and ski
were recognised,interestwas shown in everyone’s opinions and
members encouraged one anotherto participate (Craigie Jr&
Hobbs, 2004; Pethybridge, 2004; Shaw, Walker, & Hogue, 2008
Socialbonds were evidentin some teams where members were
friends as well as colleagues and interactions included humour
chat(Kvarnstrom & Cedersund,2006;Reeves & Lewin,2004).
Othermanifestationsincluded praise between team members,
backing one anotherup and sharing emotionswhen stressed
(Apker, Propp, & Ford, 2005; Wilson, McCormack, & Ives, 2005;
Wittenberg-Lyles & Parker-Oliver, 2007).
When the mechanism was absent, individuals reported feelin
their contributions were not valued and a lack of trust, obstruct
behaviour and bullying were evident(Lingard,Espin,Evans,&
Hawryluck,2004;Rice Simpson,James,& Knox, 2006;Silen-
Lipponen,Tossavainen,Turunen,Smith,& Burdett,2004).
A number of contexts suggested why ‘‘support and value’’ w
present in some teams but absent in others.Another mechanism,
‘‘Efficient,open and equitablecommunication’’was tightly
linked to ‘‘Supportand value’’,being both a contextand an
outcome of it. As a context, open communication meant all tea
members could contribute and get to know one another,helping
build cohesive teams and respect across professions (Craigie Jr
Hobbs,2004;Fear & de Renzie-Brett,2007).Trustand respect
were also enhanced by familiarity and thiscontextwas most
prominentin teamswith long-standingmembersor where
membersworked in close proximity (Reeves& Lewin, 2004;
Rice Simpson et al., 2006). Role clarity and ambiguity were also
importantcontexts,whereby the former promoted and the latter
underminedtrust within teams(Atwal, 2002; Gantert&
McWilliam,2004).Professionalhierarchy wasalso influential
as individuals in ‘‘lower status’’ roles sometimes felt less truste
and valued, whilst others did not necessarily believe that equal
between the professions existed (Coombs & Ersser, 2004; Morr
Payne,& Lambert,2007; Sargeant,Loney,& Murphy,2008).
The ‘‘Efficient, open and equitable communication’’ mechan-
ism was an outcome for ‘‘Support and value’’ as well as a conte
When elementsof ‘‘Supportand value’’were present,team
communication improved and when absent,communication was
inhibited as individuals feltunable orunwilling to voice their
opinionsor challengeothers(Field & West, 1995;Piquette,
Reeves, & Leblanc, 2009). ‘‘Support and value’’ impacted on th
‘‘Collaboration and coordination’’ mechanism too,as supportive
teamsshowed improved collaboration and unsupportive teams
collaborated less well(Lingard etal., 2004;Salhani& Coulter,
Records screened for
original research and
interprofessional education
232 papers read
87 records identified
from reviews and
snowball sampling
109 included
123 excluded
3 new mechanisms identified;
evidence for mechanisms
synthesised
Focused searches; 19 additional
papers included
35 records
retrieved from first
stage search
1103 excluded
762 records remaining;
110 papers read in full
1865 records
identified
Figure 1.Flow chart of second stage search.
Box 1. CMO configuration of ‘‘Support and value’’ mechanism.
A study of cooperation and autonomy in two Dutch hospital teams
(geriatrics and oncology) found that over the period of their existence
(three years) trust had grown, so members knew each other better a
trusted one another much more than they had in the teams’ early da
Consequently, initial reluctance to involve other members in decision
making had largely disappeared and the teams openly reflected on
individuals’ decisions during patient discussions,where voicing
criticisms of other members had become much more acceptable
(Molleman,Broekhuis,Stoffels,& Jaspers,2008).
Long tenure of team (C) ! Trust between team members (M) ! Shared
decision-making and critical reflection (O)
504 G. Hewitt et al. J Interprof Care,2014; 28(6): 501–506
inhibited it. Data extraction forms contained a section for notes on
each study’s methodologicalquality and the robustness ofthe
conclusions drawn.This information was drawn on during the
synthesis,not to includeor excludestudies,but to inform
decisions regarding the strength of the contribution the evidence
from that article should make to the synthesis.
Furtherfocussed searches were undertaken formechanisms
with weak evidence or only a small number of articles (Table II).
Appropriate key words were identified and used to search the
remaining records from the second stage search,the Journalof
Interprofessional Care, MEDLINE and CINAHL. Relevant papers
identified were then fed into the synthesis of the mechanism.
Realist synthesis draws on the qualitative research principle of
saturation, meaning that searching ceases when no new evidence
for a mechanism is emerging.However,the review was halted
following the focussed searches for pragmatic reasons,despite a
large number of articles from the second stage search remaining
unread.Whilstsome evidence may therefore have been missed,
sufficienthad been reviewed to begin to explore and testthe
mechanisms identified.
Findings
Support and value mechanism
This section reports the evidence pertaining to the ‘‘Support and
value’’ mechanism within therealistframework ofcontext,
mechanism and outcome. Evidence for the other twelve mechan-
isms are reported in later papers in the series (Hewitt et al., in press;
Sims etal., in press a,in press b).Sixty-one articles reporting
59 studieswere included in the synthesisof this mechanism
(Harris et al., 2013). Most used qualitative research methods and
approximately halfwere conducted in the UK.Studieswere
undertaken in a variety of inpatient and community settings and
with many typesof interprofessionalteam,strengthening the
relevance of the findings across health.Box 1 illustrates a CMO
configuration of the ‘‘support and value’’ mechanism.
The provisional definition of ‘‘supportand value’’ (Table II)
posited that individuals respond to team membership by suppo
one another and showing respect to and valuing each other’s s
and knowledge. Evidence to support this was found, but there w
also reports of teams where the mechanism was clearly absent
most common manifestation of the mechanism was where all t
members’ contributions were seen as important and valued eq
This meant that everyone was trusted, their knowledge and ski
were recognised,interestwas shown in everyone’s opinions and
members encouraged one anotherto participate (Craigie Jr&
Hobbs, 2004; Pethybridge, 2004; Shaw, Walker, & Hogue, 2008
Socialbonds were evidentin some teams where members were
friends as well as colleagues and interactions included humour
chat(Kvarnstrom & Cedersund,2006;Reeves & Lewin,2004).
Othermanifestationsincluded praise between team members,
backing one anotherup and sharing emotionswhen stressed
(Apker, Propp, & Ford, 2005; Wilson, McCormack, & Ives, 2005;
Wittenberg-Lyles & Parker-Oliver, 2007).
When the mechanism was absent, individuals reported feelin
their contributions were not valued and a lack of trust, obstruct
behaviour and bullying were evident(Lingard,Espin,Evans,&
Hawryluck,2004;Rice Simpson,James,& Knox, 2006;Silen-
Lipponen,Tossavainen,Turunen,Smith,& Burdett,2004).
A number of contexts suggested why ‘‘support and value’’ w
present in some teams but absent in others.Another mechanism,
‘‘Efficient,open and equitablecommunication’’was tightly
linked to ‘‘Supportand value’’,being both a contextand an
outcome of it. As a context, open communication meant all tea
members could contribute and get to know one another,helping
build cohesive teams and respect across professions (Craigie Jr
Hobbs,2004;Fear & de Renzie-Brett,2007).Trustand respect
were also enhanced by familiarity and thiscontextwas most
prominentin teamswith long-standingmembersor where
membersworked in close proximity (Reeves& Lewin, 2004;
Rice Simpson et al., 2006). Role clarity and ambiguity were also
importantcontexts,whereby the former promoted and the latter
underminedtrust within teams(Atwal, 2002; Gantert&
McWilliam,2004).Professionalhierarchy wasalso influential
as individuals in ‘‘lower status’’ roles sometimes felt less truste
and valued, whilst others did not necessarily believe that equal
between the professions existed (Coombs & Ersser, 2004; Morr
Payne,& Lambert,2007; Sargeant,Loney,& Murphy,2008).
The ‘‘Efficient, open and equitable communication’’ mechan-
ism was an outcome for ‘‘Support and value’’ as well as a conte
When elementsof ‘‘Supportand value’’were present,team
communication improved and when absent,communication was
inhibited as individuals feltunable orunwilling to voice their
opinionsor challengeothers(Field & West, 1995;Piquette,
Reeves, & Leblanc, 2009). ‘‘Support and value’’ impacted on th
‘‘Collaboration and coordination’’ mechanism too,as supportive
teamsshowed improved collaboration and unsupportive teams
collaborated less well(Lingard etal., 2004;Salhani& Coulter,
Records screened for
original research and
interprofessional education
232 papers read
87 records identified
from reviews and
snowball sampling
109 included
123 excluded
3 new mechanisms identified;
evidence for mechanisms
synthesised
Focused searches; 19 additional
papers included
35 records
retrieved from first
stage search
1103 excluded
762 records remaining;
110 papers read in full
1865 records
identified
Figure 1.Flow chart of second stage search.
Box 1. CMO configuration of ‘‘Support and value’’ mechanism.
A study of cooperation and autonomy in two Dutch hospital teams
(geriatrics and oncology) found that over the period of their existence
(three years) trust had grown, so members knew each other better a
trusted one another much more than they had in the teams’ early da
Consequently, initial reluctance to involve other members in decision
making had largely disappeared and the teams openly reflected on
individuals’ decisions during patient discussions,where voicing
criticisms of other members had become much more acceptable
(Molleman,Broekhuis,Stoffels,& Jaspers,2008).
Long tenure of team (C) ! Trust between team members (M) ! Shared
decision-making and critical reflection (O)
504 G. Hewitt et al. J Interprof Care,2014; 28(6): 501–506
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
2009).Teams where the mechanism was absentalso exhibited
tension and conflictand individualsreported feeling margin-
alised,unappreciated orfrustrated (Coombs,2003;Salhani&
Coulter,2009).When individuals did feel supported and valued,
however,they reported improved self-esteem,a sense of belong-
ing and an ability to cope with stress (Apker,Propp,Ford,&
Hofmeister, 2006; Fear & de Renzie-Brett, 2007; Silen-Lipponen
et al.,2004).
Discussion
Evidence supported the provisional definition of the ‘‘support and
value’’mechanism (Table II)and suggested why itspresence
varied acrossteams(contexts).Althoughcommitmentand
motivation specifically were notidentified as outcomes,those
described above underline the importance of the mechanism for
both staff quality of working life and team functioning through its
impacton communication and collaboration.The clear effectof
the mechanism on staff, however, was not mirrored by any notable
effect on patients, who were rarely mentioned, whether in terms of
clinical outcomes or experience.Therefore,to answer the realist
question of ‘‘What is it about teamwork that works for whom, in
what circumstances and why?’’,the evidence synthesised in this
paper demonstrates that supporting one another,showing respect
and valuing each other’s skills and knowledge works wellfor
interprofessionalstaff whereall membersof the team can
communicate openly and get to know each other. This familiarity
occurs in stable teams where members have clearly defined roles
and work in close proximity with an absenceof hierarchy
enabling team members to trust each other and fully contribute to
the work of the team.
Realistsynthesisis a relatively new approach to literature
reviewing and as such it is useful to consider how it adds to the
reviewer’s toolkit.Using realistsynthesis to explore the health
and social care literature distilled interprofessional teamwork into
an evidence-based framework ofits candidate socialprocesses
(Table II) and illuminated the contexts and outcomes associated
with those processes.Unlike conventionalreview methods,its
purpose was not to pass judgement on interprofessional teamwork
as a successful or failing policy by focusing on outcomes,but to
providea meansof conceptualisingand understandingthe
processes of teamwork in a way thatcarries potentialfor use in
team development and service improvement.
Pawson etal. (2004)caution,however,thatrealistreview
‘‘requires sustained thinking and imagination to track and trace’’
mechanisms through the literature and we would concur with this.
We found it an intellectually challenging process,particularly as
there are few published syntheses to provide guidance. Time was
needed in the early stages of the review to debate and clarify our
understandingof ‘‘mechanisms’’and how they relatedto
teamwork.We returned to this frequently throughoutthe review
as our understanding was often tested, particularly by the way in
which mechanisms interlinked: a mechanism could trigger one or
more others, so the first mechanism was a context for the second
and the second an outcome for the first.Box 1 illustrates this as
the outcomes,shared decision-making and critical reflection,are
also mechanisms themselves (‘‘Shared responsibility and influ-
ence’’and ‘‘Critically reviewing performance and decisions’’).
This issue has been noted by Byng, Norman, and Redfern (2005)
after undertaking an empirical realist evaluation,where they had
difficultiesdecidingwhethera factor was a contextor a
mechanism,or indeed both.
A related issue we faced was the difficulty of clearly
differentiating the mechanisms of teamwork.We sometimes felt
a degree of overlap existed between them,which meantthata
process described in an article could be ascribed to more than one
mechanism. For example, if a team were discussing a patient a
sharing what they knew of the patient’s home circumstances, w
that ‘‘Efficient, open and equitable communication’’, ‘‘Pooling o
resources’’ or both? This, coupled with how tightly interlinked t
mechanismsappeared to be,meantthatat timesit seemed
somewhatartificialto separate outteamwork into such discrete
processes.A brief reading ofthe interprofessionalteamwork
literature highlights how complex and context-dependent it is,
to imposethe degreeof clarity and orderon it thatrealist
synthesisdoes may not accuratelyreflect the realitiesof
teamwork and produce a misleadingly simple framework.
We also found it difficult to make sense of the multiple CMO
configurations we identified in the papers and ultimately found
helpfulto step back from thatlevel of detailand instead
summarise information on each mechanism and its contexts an
outcomes separately.This made the process of synthesising each
mechanism morestraightforward asthe information on each
element (context,mechanism or outcome) could be easily drawn
togetherto look for patterns,similaritiesand differences.
Examplesof some ofthe CMO configurationshighlighted in
the synthesis are included in the three subsequent papers in th
series (Sims et al.,in press a,in press b; Hewitt et al.,in press).
The inclusive and wide-ranging nature ofrealistsynthesis
make it a substantial undertaking, particularly in a field where t
literature is profuse, and Pawson et al. (2005) acknowledge tha
many cases the limits of time and funding willdetermine when
searchingceases.The volumeof literaturewe faced was
problematic and we found itdifficultto decide when to stop
searching and reading. This synthesis, however, was not a disc
research project,but the first stage of a wider study and as such
was limited by the time available.Two researchers worked full-
time on the review for a year,supported by other research team
members,buteven atthis levelof human resource itwas not
possibleto follow the realistsynthesismethodexactlyas
described by Pawson et al. (2004). They recommend, for exam
searching across disciplinary boundaries to learn how mechan-
ismswork in otherfields,but we restricted oursearching to
health and even then could not read all the records we identifie
(Figure 1). We have therefore potentially weakened the synthe
by omitting evidence from other fields and failing to ‘‘maximize
learning acrosspolicy,disciplinary and organizationalbound-
aries’’ (Pawson et al.,2005).
One strategy to narrow the focus of a realistsynthesis is to
select some of the provisional mechanisms identified in the firs
stage search to explore in depth and notpursue the others.The
mechanisms we identified,however,were to form an analytical
framework for the restof the study,so such a strategy was not
appropriate for this synthesis.
Realistsynthesis offers researchers a logic through which to
explore policiesand interventionsand gains strength from its
pluralism and flexibility (Pawson etal., 2005),butit is notan
approach to be undertaken lightly. Pawson et al. (2004) explicit
caution that it is not for novices as it requires broad knowledge
disciplinesand methodologiesand skillsin searching forand
assessing evidence.Despite the intellectualand practicalchal-
lenges encountered,however,we found realist synthesis a useful
means ofinterrogating the large literature on interprofessional
teamwork. It helped us articulate the social processes and actio
thatpotentially constitute teamwork and provided an evidence-
based analytical framework for the subsequent empirical study
Acknowledgements
We are gratefulto Sally Brearley,Vari Drennan,Geoff Cloud,
Nan Greenwood,Fiona Jones,Mark Joy,Lalit Kalra,Ann Mackenzie,
Fiona Ross, Sally Redfern and Scott Reeves for their support throughout
this work.
DOI: 10.3109/13561820.2014.939744 A realist synthesis of interprofessional teamwork505
tension and conflictand individualsreported feeling margin-
alised,unappreciated orfrustrated (Coombs,2003;Salhani&
Coulter,2009).When individuals did feel supported and valued,
however,they reported improved self-esteem,a sense of belong-
ing and an ability to cope with stress (Apker,Propp,Ford,&
Hofmeister, 2006; Fear & de Renzie-Brett, 2007; Silen-Lipponen
et al.,2004).
Discussion
Evidence supported the provisional definition of the ‘‘support and
value’’mechanism (Table II)and suggested why itspresence
varied acrossteams(contexts).Althoughcommitmentand
motivation specifically were notidentified as outcomes,those
described above underline the importance of the mechanism for
both staff quality of working life and team functioning through its
impacton communication and collaboration.The clear effectof
the mechanism on staff, however, was not mirrored by any notable
effect on patients, who were rarely mentioned, whether in terms of
clinical outcomes or experience.Therefore,to answer the realist
question of ‘‘What is it about teamwork that works for whom, in
what circumstances and why?’’,the evidence synthesised in this
paper demonstrates that supporting one another,showing respect
and valuing each other’s skills and knowledge works wellfor
interprofessionalstaff whereall membersof the team can
communicate openly and get to know each other. This familiarity
occurs in stable teams where members have clearly defined roles
and work in close proximity with an absenceof hierarchy
enabling team members to trust each other and fully contribute to
the work of the team.
Realistsynthesisis a relatively new approach to literature
reviewing and as such it is useful to consider how it adds to the
reviewer’s toolkit.Using realistsynthesis to explore the health
and social care literature distilled interprofessional teamwork into
an evidence-based framework ofits candidate socialprocesses
(Table II) and illuminated the contexts and outcomes associated
with those processes.Unlike conventionalreview methods,its
purpose was not to pass judgement on interprofessional teamwork
as a successful or failing policy by focusing on outcomes,but to
providea meansof conceptualisingand understandingthe
processes of teamwork in a way thatcarries potentialfor use in
team development and service improvement.
Pawson etal. (2004)caution,however,thatrealistreview
‘‘requires sustained thinking and imagination to track and trace’’
mechanisms through the literature and we would concur with this.
We found it an intellectually challenging process,particularly as
there are few published syntheses to provide guidance. Time was
needed in the early stages of the review to debate and clarify our
understandingof ‘‘mechanisms’’and how they relatedto
teamwork.We returned to this frequently throughoutthe review
as our understanding was often tested, particularly by the way in
which mechanisms interlinked: a mechanism could trigger one or
more others, so the first mechanism was a context for the second
and the second an outcome for the first.Box 1 illustrates this as
the outcomes,shared decision-making and critical reflection,are
also mechanisms themselves (‘‘Shared responsibility and influ-
ence’’and ‘‘Critically reviewing performance and decisions’’).
This issue has been noted by Byng, Norman, and Redfern (2005)
after undertaking an empirical realist evaluation,where they had
difficultiesdecidingwhethera factor was a contextor a
mechanism,or indeed both.
A related issue we faced was the difficulty of clearly
differentiating the mechanisms of teamwork.We sometimes felt
a degree of overlap existed between them,which meantthata
process described in an article could be ascribed to more than one
mechanism. For example, if a team were discussing a patient a
sharing what they knew of the patient’s home circumstances, w
that ‘‘Efficient, open and equitable communication’’, ‘‘Pooling o
resources’’ or both? This, coupled with how tightly interlinked t
mechanismsappeared to be,meantthatat timesit seemed
somewhatartificialto separate outteamwork into such discrete
processes.A brief reading ofthe interprofessionalteamwork
literature highlights how complex and context-dependent it is,
to imposethe degreeof clarity and orderon it thatrealist
synthesisdoes may not accuratelyreflect the realitiesof
teamwork and produce a misleadingly simple framework.
We also found it difficult to make sense of the multiple CMO
configurations we identified in the papers and ultimately found
helpfulto step back from thatlevel of detailand instead
summarise information on each mechanism and its contexts an
outcomes separately.This made the process of synthesising each
mechanism morestraightforward asthe information on each
element (context,mechanism or outcome) could be easily drawn
togetherto look for patterns,similaritiesand differences.
Examplesof some ofthe CMO configurationshighlighted in
the synthesis are included in the three subsequent papers in th
series (Sims et al.,in press a,in press b; Hewitt et al.,in press).
The inclusive and wide-ranging nature ofrealistsynthesis
make it a substantial undertaking, particularly in a field where t
literature is profuse, and Pawson et al. (2005) acknowledge tha
many cases the limits of time and funding willdetermine when
searchingceases.The volumeof literaturewe faced was
problematic and we found itdifficultto decide when to stop
searching and reading. This synthesis, however, was not a disc
research project,but the first stage of a wider study and as such
was limited by the time available.Two researchers worked full-
time on the review for a year,supported by other research team
members,buteven atthis levelof human resource itwas not
possibleto follow the realistsynthesismethodexactlyas
described by Pawson et al. (2004). They recommend, for exam
searching across disciplinary boundaries to learn how mechan-
ismswork in otherfields,but we restricted oursearching to
health and even then could not read all the records we identifie
(Figure 1). We have therefore potentially weakened the synthe
by omitting evidence from other fields and failing to ‘‘maximize
learning acrosspolicy,disciplinary and organizationalbound-
aries’’ (Pawson et al.,2005).
One strategy to narrow the focus of a realistsynthesis is to
select some of the provisional mechanisms identified in the firs
stage search to explore in depth and notpursue the others.The
mechanisms we identified,however,were to form an analytical
framework for the restof the study,so such a strategy was not
appropriate for this synthesis.
Realistsynthesis offers researchers a logic through which to
explore policiesand interventionsand gains strength from its
pluralism and flexibility (Pawson etal., 2005),butit is notan
approach to be undertaken lightly. Pawson et al. (2004) explicit
caution that it is not for novices as it requires broad knowledge
disciplinesand methodologiesand skillsin searching forand
assessing evidence.Despite the intellectualand practicalchal-
lenges encountered,however,we found realist synthesis a useful
means ofinterrogating the large literature on interprofessional
teamwork. It helped us articulate the social processes and actio
thatpotentially constitute teamwork and provided an evidence-
based analytical framework for the subsequent empirical study
Acknowledgements
We are gratefulto Sally Brearley,Vari Drennan,Geoff Cloud,
Nan Greenwood,Fiona Jones,Mark Joy,Lalit Kalra,Ann Mackenzie,
Fiona Ross, Sally Redfern and Scott Reeves for their support throughout
this work.
DOI: 10.3109/13561820.2014.939744 A realist synthesis of interprofessional teamwork505
Declaration of interest
This projectwas funded by the NationalInstitute for Health Research
(NIHR) Health Services and Delivery Research (HS&DR)programme
(project number 08/1819/219). The views and opinions expressed therein
are those ofthe authorsand do notnecessarily reflectthose ofthe
HS&DR programme,NIHR, NHS or the Departmentof Health.The
authors report no conflicts of interest. The authors are responsible for the
writing and content of this paper.
References
Apker,J., Propp,K.M., & Ford, W.S.Z.(2005).Negotiating status and
identity tensions in healthcare team interactions:An exploration of
nurse role dialectics. Journal of Applied Communication Research, 33,
93–115.
Apker, J., Propp, K.M., Ford, W.S.Z., & Hofmeister,N. (2006).
Collaboration,credibility,compassion,and coordination: Professional
nursecommunication skillsets in health careteam interactions.
Journal of Professional Nursing,22,180–189.
Atwal, A. (2002). A world apart: How occupational therapists, nurses and
care managers perceive each otherin acute health care.The British
Journal of Occupational Therapy,65,446–452.
Byng, R., Norman, I., & Redfern, S. (2005). Using realistic evaluation to
evaluate a practice-level intervention to improve primary healthcare for
patients with long-term mental illness.Evaluation, 11,69–94.
Coombs, M. (2003). Power and conflict in intensive care clinical decision
making.Intensive & Critical Care Nursing, 19,125–135.
Coombs,M., & Ersser, S.J. (2004).Medicalhegemony in decision-
making – A barrierto interdisciplinary working in intensive care?
Journal of Advanced Nursing,46,245–252.
Craigie Jr F.C., & Hobbs, R.F. (2004).Exploring the organizational
cultureof exemplarycommunityhealthcenterpractices.Family
Medicine,36,733–738.
Fear,T., & de Renzie-Brett,H. (2007).Developing interprofessional
working in primary care.Practice Developmentin Health Care,6,
107–118.
Field, R., & West, M. (1995).Teamwork in primary health care.2.
Perspectivesfrom practices.Journal of InterprofessionalCare, 9,
123–30.
Gantert,T.W., & McWilliam, C.L. (2004).Interdisciplinaryteam
processeswithin an in-homeservicedelivery organization.Home
Health Care Services Quarterly,23,1–17.
Hammick,M., Freeth,D., Koppel,I., Reeves,S., & Barr,H. (2007).A
best evidence systematic review of interprofessional education: BEME
guide no.9. Medical Teacher,29,735–751.
Harris, R., Sims, S., Hewitt, G., Joy, M., Brearley, S., Cloud, G., Drennan,
V., et al. (2013).Interprofessionalteamworkacrossstrokecare
pathways: Outcomes and patientand carer experience.Final report,
NIHR Service Delivery and Organisation Programme.
Hewitt, G., Sims, S., & Harris, R. (in press). Evidence of communication,
influence and behavioural norms in interprofessional teams: A realist
synthesis.Journal of Interprofessional Care.
Kvarnstrom,S., & Cedersund,E. (2006).Discursive patterns in multi-
professionalhealthcareteams.Journal of Advanced Nursing,53,
244–253.
Lingard,L., Espin,S., Evans,C., & Hawryluck,L. (2004).The rules of
the game:Interprofessionalcollaboration on the intensive care unit
team.Critical Care,8, R403–R408.
Molleman,E., Broekhuis,M., Stoffels,R., & Jaspers,F. (2008).How
health care complexity leads to cooperation and affects the autonomy
of health care professionals.Health Care Analysis, 16, 329–341.
Morris,R., Payne,O., & Lambert,A. (2007).Patient,carerand staff
experience of a hospital-based stroke service. International Journal for
Quality in Health Care, 19,105–112.
Pawson,R. (2006).Digging for nuggets:How ‘bad’ research can yield
‘good’ evidence. International Journal of Social Research
Methodology,9, 127–142.
Pawson,R., Greenhalgh,T., Harvey,G., & Walshe,K. (2004).Realist
Synthesis:An introduction.ESRC Research MethodsProgramme
Working Paper Series,University of Manchester.
Pawson,R., Greenhalgh,T., Harvey,G., & Walshe,K. (2005).Realist
review – A new method of systematic review designed for complex
policy interventions. Journal of Health Services Research & Policy, 10,
21–34.
Pawson,R., & Tilley, N. (1997).Realistic evaluation.London:Sage
Publications.
Pethybridge, J. (2004). How team working influences discharge planning
from hospital:A study offour multi-disciplinary teams in an acute
hospital in England.Journal of Interprofessional Care, 18,29–41.
Piquette,D., Reeves,S., & Leblanc, V.R. (2009).Interprofessional
intensive care unit team interactions and medical crises: A qualitative
study.Journal of Interprofessional Care,23,273–285.
Reeves,S., & Lewin, S. (2004).Interprofessionalcollaboration in the
hospital: Strategies and meanings. Journal of Health Services Researc
and Policy,9, 218–225.
Reeves,S., Lewin, S., Espin, S., & Zwarenstein, M. (2010).
Interprofessionalteamwork forhealth and socialcare.Chichester:
Wiley-Blackwell.
Rice Simpson, K., James, D. C., & Knox, G. E. (2006). Nurse-physician
communication during labor and birth: Implications for patient safety.
Journal of Obstetric,Gynecologic,and NeonatalNursing, 35,
547–556.
Salhani,D., & Coulter, I. (2009).The politicsof interprofessional
working and the struggle for professional autonomy in nursing. Social
Science & Medicine,68,1221–1228.
Sargeant, J., Loney, E., & Murphy, G. (2008). Effective interprofessional
teams: ‘‘Contact is not enough’’ to build a team. Journal of Continuing
Education in the Health Professions,28,228–234.
Shaw,L., Walker,R., & Hogue, A. (2008).The art and science of
teamwork: enacting a transdisciplinary approach in work rehabilitatio
Work (Reading,MA), 30,297–306.
Silen-Lipponen, M., Tossavainen, K., Turunen, H., Smith, A., & Burdett,
K. (2004).Teamwork in operating room nursing as experienced by
Finnish,British and American nurses.Diversity in Health & Social
Care, 1,127–137.
Sims, S., Hewitt, G., & Harris, R. (in press a). Evidence of collaboration,
pooling ofresources,learning and role blurring in interprofessional
healthcare teams: A realist synthesis. Journal of Interprofessional Car
Sims, S., Hewitt, G., & Harris, R. (in press b). Evidence of a shared sense
of purpose,criticalreflection,innovation and leadership in inter-
professionalhealthcareteams:A realist synthesis.Journal of
Interprofessional Care.
Wilson,V.J., McCormack,B.G., & Ives, G. (2005).Understanding the
workplace culture ofa specialcare nursery.Journal of Advanced
Nursing,50, 27–38.
Wittenberg-Lyles,E.M., & Parker-Oliver,D. (2007).The powerof
interdisciplinary collaboration in hospice. Progress in Palliative Care,
15,6–12.
Appendix: Data extraction form
Reviewer: EndNote library number:
Reference:
Objective of study:
Description of paper (include location,setting,field of health,partici-
pants,brief methods):
Mechanisms discussed:
Shared sense of purpose Support and value
Pooling of resources Critically reviewing performance
& decisions
Collaboration and coordination Generating and implementing
new ideas
Efficient,open & equitable
communication
Individual learning
Shared responsibility and influenceLeadership
Role blurring Team behavioural norms
Tactical communication
Summary of main findings related to original mechanisms (including
page nos.for reference); highlight which mechanisms findings relate to,
any important context factors and whether outcomes relate to staff, tea
patients or organization:
Summary of main findings related to alternativemechanisms
(including page nos.for reference); as above:
Study quality issues:
Any other comments (including reasons for exclusion,if applicable):
Other references identified from paper:
506 G. Hewitt et al. J Interprof Care,2014; 28(6): 501–506
This projectwas funded by the NationalInstitute for Health Research
(NIHR) Health Services and Delivery Research (HS&DR)programme
(project number 08/1819/219). The views and opinions expressed therein
are those ofthe authorsand do notnecessarily reflectthose ofthe
HS&DR programme,NIHR, NHS or the Departmentof Health.The
authors report no conflicts of interest. The authors are responsible for the
writing and content of this paper.
References
Apker,J., Propp,K.M., & Ford, W.S.Z.(2005).Negotiating status and
identity tensions in healthcare team interactions:An exploration of
nurse role dialectics. Journal of Applied Communication Research, 33,
93–115.
Apker, J., Propp, K.M., Ford, W.S.Z., & Hofmeister,N. (2006).
Collaboration,credibility,compassion,and coordination: Professional
nursecommunication skillsets in health careteam interactions.
Journal of Professional Nursing,22,180–189.
Atwal, A. (2002). A world apart: How occupational therapists, nurses and
care managers perceive each otherin acute health care.The British
Journal of Occupational Therapy,65,446–452.
Byng, R., Norman, I., & Redfern, S. (2005). Using realistic evaluation to
evaluate a practice-level intervention to improve primary healthcare for
patients with long-term mental illness.Evaluation, 11,69–94.
Coombs, M. (2003). Power and conflict in intensive care clinical decision
making.Intensive & Critical Care Nursing, 19,125–135.
Coombs,M., & Ersser, S.J. (2004).Medicalhegemony in decision-
making – A barrierto interdisciplinary working in intensive care?
Journal of Advanced Nursing,46,245–252.
Craigie Jr F.C., & Hobbs, R.F. (2004).Exploring the organizational
cultureof exemplarycommunityhealthcenterpractices.Family
Medicine,36,733–738.
Fear,T., & de Renzie-Brett,H. (2007).Developing interprofessional
working in primary care.Practice Developmentin Health Care,6,
107–118.
Field, R., & West, M. (1995).Teamwork in primary health care.2.
Perspectivesfrom practices.Journal of InterprofessionalCare, 9,
123–30.
Gantert,T.W., & McWilliam, C.L. (2004).Interdisciplinaryteam
processeswithin an in-homeservicedelivery organization.Home
Health Care Services Quarterly,23,1–17.
Hammick,M., Freeth,D., Koppel,I., Reeves,S., & Barr,H. (2007).A
best evidence systematic review of interprofessional education: BEME
guide no.9. Medical Teacher,29,735–751.
Harris, R., Sims, S., Hewitt, G., Joy, M., Brearley, S., Cloud, G., Drennan,
V., et al. (2013).Interprofessionalteamworkacrossstrokecare
pathways: Outcomes and patientand carer experience.Final report,
NIHR Service Delivery and Organisation Programme.
Hewitt, G., Sims, S., & Harris, R. (in press). Evidence of communication,
influence and behavioural norms in interprofessional teams: A realist
synthesis.Journal of Interprofessional Care.
Kvarnstrom,S., & Cedersund,E. (2006).Discursive patterns in multi-
professionalhealthcareteams.Journal of Advanced Nursing,53,
244–253.
Lingard,L., Espin,S., Evans,C., & Hawryluck,L. (2004).The rules of
the game:Interprofessionalcollaboration on the intensive care unit
team.Critical Care,8, R403–R408.
Molleman,E., Broekhuis,M., Stoffels,R., & Jaspers,F. (2008).How
health care complexity leads to cooperation and affects the autonomy
of health care professionals.Health Care Analysis, 16, 329–341.
Morris,R., Payne,O., & Lambert,A. (2007).Patient,carerand staff
experience of a hospital-based stroke service. International Journal for
Quality in Health Care, 19,105–112.
Pawson,R. (2006).Digging for nuggets:How ‘bad’ research can yield
‘good’ evidence. International Journal of Social Research
Methodology,9, 127–142.
Pawson,R., Greenhalgh,T., Harvey,G., & Walshe,K. (2004).Realist
Synthesis:An introduction.ESRC Research MethodsProgramme
Working Paper Series,University of Manchester.
Pawson,R., Greenhalgh,T., Harvey,G., & Walshe,K. (2005).Realist
review – A new method of systematic review designed for complex
policy interventions. Journal of Health Services Research & Policy, 10,
21–34.
Pawson,R., & Tilley, N. (1997).Realistic evaluation.London:Sage
Publications.
Pethybridge, J. (2004). How team working influences discharge planning
from hospital:A study offour multi-disciplinary teams in an acute
hospital in England.Journal of Interprofessional Care, 18,29–41.
Piquette,D., Reeves,S., & Leblanc, V.R. (2009).Interprofessional
intensive care unit team interactions and medical crises: A qualitative
study.Journal of Interprofessional Care,23,273–285.
Reeves,S., & Lewin, S. (2004).Interprofessionalcollaboration in the
hospital: Strategies and meanings. Journal of Health Services Researc
and Policy,9, 218–225.
Reeves,S., Lewin, S., Espin, S., & Zwarenstein, M. (2010).
Interprofessionalteamwork forhealth and socialcare.Chichester:
Wiley-Blackwell.
Rice Simpson, K., James, D. C., & Knox, G. E. (2006). Nurse-physician
communication during labor and birth: Implications for patient safety.
Journal of Obstetric,Gynecologic,and NeonatalNursing, 35,
547–556.
Salhani,D., & Coulter, I. (2009).The politicsof interprofessional
working and the struggle for professional autonomy in nursing. Social
Science & Medicine,68,1221–1228.
Sargeant, J., Loney, E., & Murphy, G. (2008). Effective interprofessional
teams: ‘‘Contact is not enough’’ to build a team. Journal of Continuing
Education in the Health Professions,28,228–234.
Shaw,L., Walker,R., & Hogue, A. (2008).The art and science of
teamwork: enacting a transdisciplinary approach in work rehabilitatio
Work (Reading,MA), 30,297–306.
Silen-Lipponen, M., Tossavainen, K., Turunen, H., Smith, A., & Burdett,
K. (2004).Teamwork in operating room nursing as experienced by
Finnish,British and American nurses.Diversity in Health & Social
Care, 1,127–137.
Sims, S., Hewitt, G., & Harris, R. (in press a). Evidence of collaboration,
pooling ofresources,learning and role blurring in interprofessional
healthcare teams: A realist synthesis. Journal of Interprofessional Car
Sims, S., Hewitt, G., & Harris, R. (in press b). Evidence of a shared sense
of purpose,criticalreflection,innovation and leadership in inter-
professionalhealthcareteams:A realist synthesis.Journal of
Interprofessional Care.
Wilson,V.J., McCormack,B.G., & Ives, G. (2005).Understanding the
workplace culture ofa specialcare nursery.Journal of Advanced
Nursing,50, 27–38.
Wittenberg-Lyles,E.M., & Parker-Oliver,D. (2007).The powerof
interdisciplinary collaboration in hospice. Progress in Palliative Care,
15,6–12.
Appendix: Data extraction form
Reviewer: EndNote library number:
Reference:
Objective of study:
Description of paper (include location,setting,field of health,partici-
pants,brief methods):
Mechanisms discussed:
Shared sense of purpose Support and value
Pooling of resources Critically reviewing performance
& decisions
Collaboration and coordination Generating and implementing
new ideas
Efficient,open & equitable
communication
Individual learning
Shared responsibility and influenceLeadership
Role blurring Team behavioural norms
Tactical communication
Summary of main findings related to original mechanisms (including
page nos.for reference); highlight which mechanisms findings relate to,
any important context factors and whether outcomes relate to staff, tea
patients or organization:
Summary of main findings related to alternativemechanisms
(including page nos.for reference); as above:
Study quality issues:
Any other comments (including reasons for exclusion,if applicable):
Other references identified from paper:
506 G. Hewitt et al. J Interprof Care,2014; 28(6): 501–506

Copyright of Journal of Interprofessional Care is the property of Taylor & Francis Ltd and its
content may not be copied or emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission. However, users may print, download, or email
articles for individual use.
content may not be copied or emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission. However, users may print, download, or email
articles for individual use.
1 out of 7

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.