Pharmacology Report: Adrenaline Receptors and Effects
VerifiedAdded on 2020/02/05
|8
|1991
|322
Report
AI Summary
This pharmacology report comprehensively examines adrenaline's actions within the body, focusing on its receptor interactions, therapeutic applications, and potential adverse effects. The report identifies the major receptors adrenaline binds to (alpha and beta receptors) and details the pathways through which it elicits various physiological responses, including its role in anaphylaxis treatment and improving cardiac output. It also includes a table outlining receptor subtypes and their locations. Furthermore, the report discusses potential adverse events associated with adrenaline use, such as disease interactions, allergic reactions, and metabolic acidosis. The report also explains why specific injection site warnings are given and why certain adverse responses like anxiety and tremors may occur. The document concludes with a list of references used to support the information provided.
Pharmacology Report
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENTS
PART C...........................................................................................................................................1
1. Identify the major receptors adrenaline binds to and describe for each the pathway by which
it causes an effect on the body.....................................................................................................1
2. Create a Table of receptor subtypes that includes their locations within the body.................1
3. Describe the manifestations of an allergic reaction with specific attention to the vascular
and respiratory effects..................................................................................................................2
4. Explain how adrenaline causes a therapeutic response in anaphylaxis...................................2
5. Explain how adrenaline improves cardiac output....................................................................3
PART D...........................................................................................................................................3
1. Explain why you think adrenaline can result in adverse events..............................................3
2. Adrenaline should not be injected into hands, feet, nose, ears, genitaliaor buttocks. Explain
why this warning is given............................................................................................................3
3. Anxiety, fear, tenseness, restlessness, irritability are potential adverse responses to
adrenaline. Explain why these responses may occur...................................................................4
4. Repeated dosing can lead to metabolic acidosis. Explain how metabolic acidosis can
eventuate......................................................................................................................................4
5. Explain why a caution is given with respect to using adrenaline in those with Parkinsonism5
REFERENCES................................................................................................................................6
PART C...........................................................................................................................................1
1. Identify the major receptors adrenaline binds to and describe for each the pathway by which
it causes an effect on the body.....................................................................................................1
2. Create a Table of receptor subtypes that includes their locations within the body.................1
3. Describe the manifestations of an allergic reaction with specific attention to the vascular
and respiratory effects..................................................................................................................2
4. Explain how adrenaline causes a therapeutic response in anaphylaxis...................................2
5. Explain how adrenaline improves cardiac output....................................................................3
PART D...........................................................................................................................................3
1. Explain why you think adrenaline can result in adverse events..............................................3
2. Adrenaline should not be injected into hands, feet, nose, ears, genitaliaor buttocks. Explain
why this warning is given............................................................................................................3
3. Anxiety, fear, tenseness, restlessness, irritability are potential adverse responses to
adrenaline. Explain why these responses may occur...................................................................4
4. Repeated dosing can lead to metabolic acidosis. Explain how metabolic acidosis can
eventuate......................................................................................................................................4
5. Explain why a caution is given with respect to using adrenaline in those with Parkinsonism5
REFERENCES................................................................................................................................6
PART C
1. Identify the major receptors adrenaline binds to and describe for each the pathway by which it
causes an effect on the body
The major receptors to which adrenaline binds are G- Protein coupled receptors. These
receptors act as targets of norepinephrine and epinephrine (Tripathi, 2013). The receptors of
adrenaline are divided into two categories, α receptors and β receptors.
α receptors
There receptors are further divided into α1 and α2 subtypes. Activation causes the
heterotrimeric G protein Gq to further activate phospholipase C (PLC). This PLC works to cause
cleavage of phosphatidylinositol 4, 5-bisphosphate (PIP2).as a result of this, diacylglycerol
(DAG) and inositol triphosphate (IP3) increases. Following this, interactions takes places
between calcium channels of sarcoplasmic and endoplasmic reticulum and IP3 (Schmidt and
Weinshenker, 2014). This leads to alterations in the chemical content of a cell. All the other
effects are triggered due to this. Coupling of α2 receptor takes place with Gi/o protein. This
receptor is precynaptic and causes initiation of negative feedback.
β receptors
These are further subdivided into β1, β2 and β3 receptors. β1 receptors are responsible for
increasing cardiac output. β2 receptor binds with epinephrine and leads to “flight or fight”
response (Jacobs and et.al., 2011). β3 receptors are involved in enhancement of lipolysis in
adipose tissue.
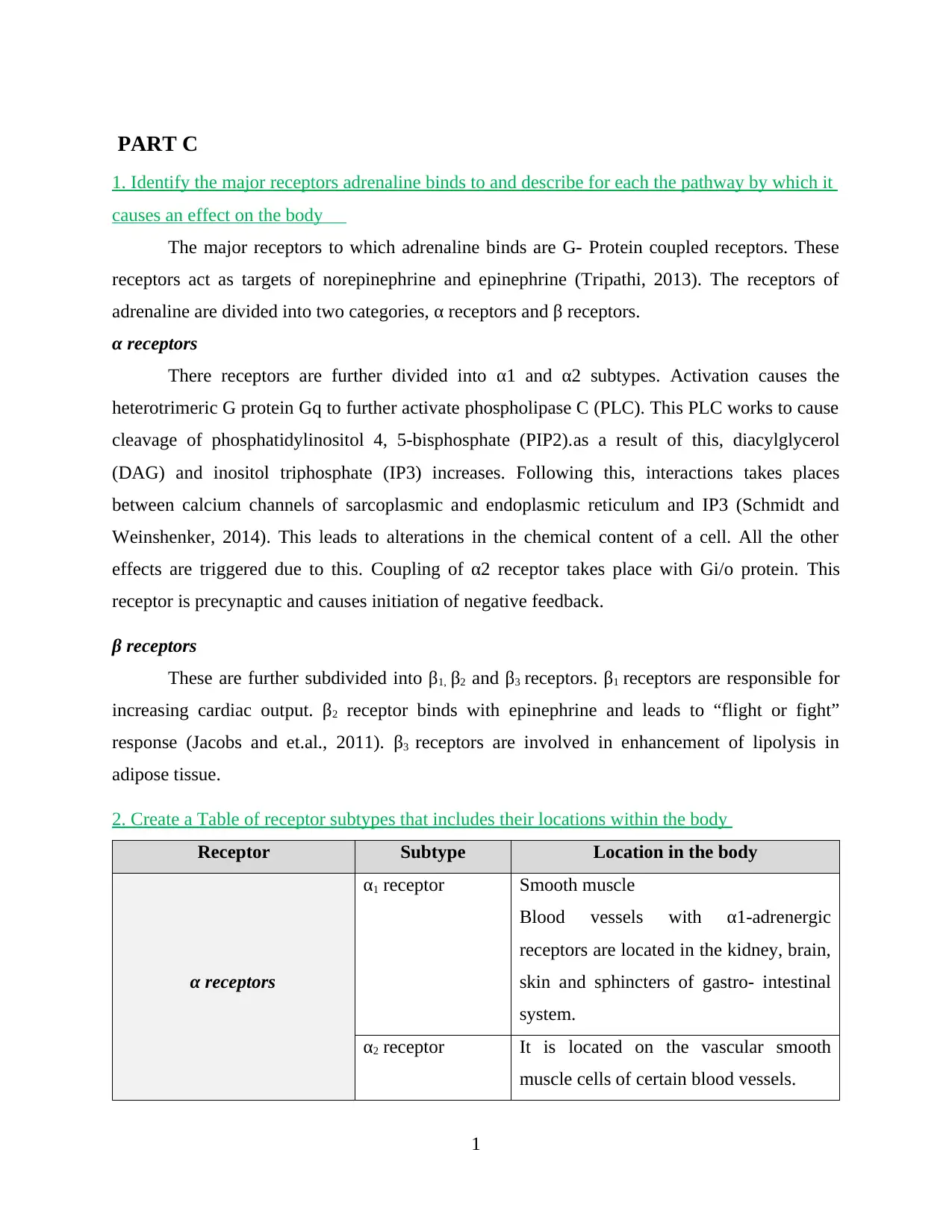
2. Create a Table of receptor subtypes that includes their locations within the body
Receptor Subtype Location in the body
α receptors
α1 receptor Smooth muscle
Blood vessels with α1-adrenergic
receptors are located in the kidney, brain,
skin and sphincters of gastro- intestinal
system.
α2 receptor It is located on the vascular smooth
muscle cells of certain blood vessels.
1
1. Identify the major receptors adrenaline binds to and describe for each the pathway by which it
causes an effect on the body
The major receptors to which adrenaline binds are G- Protein coupled receptors. These
receptors act as targets of norepinephrine and epinephrine (Tripathi, 2013). The receptors of
adrenaline are divided into two categories, α receptors and β receptors.
α receptors
There receptors are further divided into α1 and α2 subtypes. Activation causes the
heterotrimeric G protein Gq to further activate phospholipase C (PLC). This PLC works to cause
cleavage of phosphatidylinositol 4, 5-bisphosphate (PIP2).as a result of this, diacylglycerol
(DAG) and inositol triphosphate (IP3) increases. Following this, interactions takes places
between calcium channels of sarcoplasmic and endoplasmic reticulum and IP3 (Schmidt and
Weinshenker, 2014). This leads to alterations in the chemical content of a cell. All the other
effects are triggered due to this. Coupling of α2 receptor takes place with Gi/o protein. This
receptor is precynaptic and causes initiation of negative feedback.
β receptors
These are further subdivided into β1, β2 and β3 receptors. β1 receptors are responsible for
increasing cardiac output. β2 receptor binds with epinephrine and leads to “flight or fight”
response (Jacobs and et.al., 2011). β3 receptors are involved in enhancement of lipolysis in
adipose tissue.
2. Create a Table of receptor subtypes that includes their locations within the body
Receptor Subtype Location in the body
α receptors
α1 receptor Smooth muscle
Blood vessels with α1-adrenergic
receptors are located in the kidney, brain,
skin and sphincters of gastro- intestinal
system.
α2 receptor It is located on the vascular smooth
muscle cells of certain blood vessels.
1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
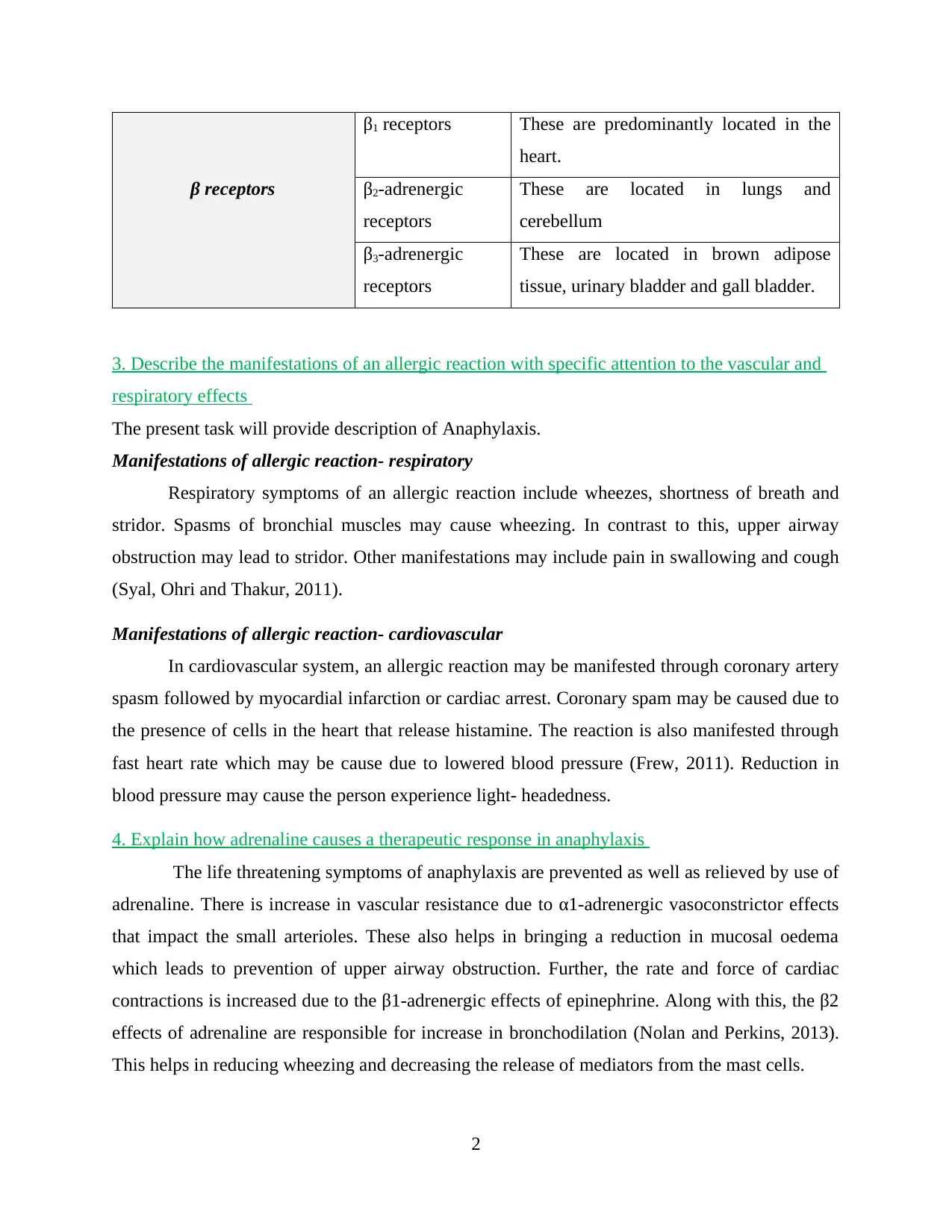
β receptors
β1 receptors These are predominantly located in the
heart.
β2-adrenergic
receptors
These are located in lungs and
cerebellum
β3-adrenergic
receptors
These are located in brown adipose
tissue, urinary bladder and gall bladder.
3. Describe the manifestations of an allergic reaction with specific attention to the vascular and
respiratory effects
The present task will provide description of Anaphylaxis.
Manifestations of allergic reaction- respiratory
Respiratory symptoms of an allergic reaction include wheezes, shortness of breath and
stridor. Spasms of bronchial muscles may cause wheezing. In contrast to this, upper airway
obstruction may lead to stridor. Other manifestations may include pain in swallowing and cough
(Syal, Ohri and Thakur, 2011).
Manifestations of allergic reaction- cardiovascular
In cardiovascular system, an allergic reaction may be manifested through coronary artery
spasm followed by myocardial infarction or cardiac arrest. Coronary spam may be caused due to
the presence of cells in the heart that release histamine. The reaction is also manifested through
fast heart rate which may be cause due to lowered blood pressure (Frew, 2011). Reduction in
blood pressure may cause the person experience light- headedness.
4. Explain how adrenaline causes a therapeutic response in anaphylaxis
The life threatening symptoms of anaphylaxis are prevented as well as relieved by use of
adrenaline. There is increase in vascular resistance due to α1-adrenergic vasoconstrictor effects
that impact the small arterioles. These also helps in bringing a reduction in mucosal oedema
which leads to prevention of upper airway obstruction. Further, the rate and force of cardiac
contractions is increased due to the β1-adrenergic effects of epinephrine. Along with this, the β2
effects of adrenaline are responsible for increase in bronchodilation (Nolan and Perkins, 2013).
This helps in reducing wheezing and decreasing the release of mediators from the mast cells.
2
β1 receptors These are predominantly located in the
heart.
β2-adrenergic
receptors
These are located in lungs and
cerebellum
β3-adrenergic
receptors
These are located in brown adipose
tissue, urinary bladder and gall bladder.
3. Describe the manifestations of an allergic reaction with specific attention to the vascular and
respiratory effects
The present task will provide description of Anaphylaxis.
Manifestations of allergic reaction- respiratory
Respiratory symptoms of an allergic reaction include wheezes, shortness of breath and
stridor. Spasms of bronchial muscles may cause wheezing. In contrast to this, upper airway
obstruction may lead to stridor. Other manifestations may include pain in swallowing and cough
(Syal, Ohri and Thakur, 2011).
Manifestations of allergic reaction- cardiovascular
In cardiovascular system, an allergic reaction may be manifested through coronary artery
spasm followed by myocardial infarction or cardiac arrest. Coronary spam may be caused due to
the presence of cells in the heart that release histamine. The reaction is also manifested through
fast heart rate which may be cause due to lowered blood pressure (Frew, 2011). Reduction in
blood pressure may cause the person experience light- headedness.
4. Explain how adrenaline causes a therapeutic response in anaphylaxis
The life threatening symptoms of anaphylaxis are prevented as well as relieved by use of
adrenaline. There is increase in vascular resistance due to α1-adrenergic vasoconstrictor effects
that impact the small arterioles. These also helps in bringing a reduction in mucosal oedema
which leads to prevention of upper airway obstruction. Further, the rate and force of cardiac
contractions is increased due to the β1-adrenergic effects of epinephrine. Along with this, the β2
effects of adrenaline are responsible for increase in bronchodilation (Nolan and Perkins, 2013).
This helps in reducing wheezing and decreasing the release of mediators from the mast cells.
2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5. Explain how adrenaline improves cardiac output
Adrenaline works to improve cardiac output through the following ways. The contractile
force and heart rate are increased due to activation of Beta 1 receptors. This myocardial
contraction is increased due to the activation of beta receptors that are associated with ventricles
and atria. The various electrophysiologic factors lead to an orderly and rhythmic electrical
activity (Robertson and et.al., 2011). As a result of this, the efficiency of the contractile ability of
heart is ensured. The response to this activation is provided an increase in these parameters
which make the heart beat at a faster rate.
PART D
1. Explain why you think adrenaline can result in adverse events
Adrenaline may result in adverse events due to the following reasons:
Disease interactions: Adrenaline carries a greater risk of developing adverse reactions in
some patients. These include patients with heart disease as well as those with Parkinson’s
disease, hypothyroidism, diabetes mellitus and elderly individuals (Tripathi, 2013).
Allergic reactions due to Sulfite: Adrenalin contains sodium bisulphite that may result
into allergic reactions which may be mild to severe.
Adverse reactions: Systematic administration of adrenalin causes adverse reactions such
as restlessness, weakness, sweating, anxiety, tremor, apprehensiveness, respiratory
difficulties etc.
Incorrect locations of injection: Incorrect location of adrenalin injections may also lad to
adverse effects (Jacobs and et.al., 2011). For example, if adrenalin injections
administered at the same site for second time, it leads to tissue necrosis.
Infections: Also, serious infections may be caused at the site of adrenalin injections.
2. Adrenaline should not be injected into hands, feet, nose, ears, genitaliaor buttocks. Explain
why this warning is given
The warning that adrenalin should not be injected in hands, feet, nose, ears, genitalia or buttocks
is given due to the following reasons:
Buttock: adrenalin should not be injected into buttock as it may lead to ineffective
treatment. Also, clostridial infections or gas gangrene may develop (Syal, Ohri and
3
Adrenaline works to improve cardiac output through the following ways. The contractile
force and heart rate are increased due to activation of Beta 1 receptors. This myocardial
contraction is increased due to the activation of beta receptors that are associated with ventricles
and atria. The various electrophysiologic factors lead to an orderly and rhythmic electrical
activity (Robertson and et.al., 2011). As a result of this, the efficiency of the contractile ability of
heart is ensured. The response to this activation is provided an increase in these parameters
which make the heart beat at a faster rate.
PART D
1. Explain why you think adrenaline can result in adverse events
Adrenaline may result in adverse events due to the following reasons:
Disease interactions: Adrenaline carries a greater risk of developing adverse reactions in
some patients. These include patients with heart disease as well as those with Parkinson’s
disease, hypothyroidism, diabetes mellitus and elderly individuals (Tripathi, 2013).
Allergic reactions due to Sulfite: Adrenalin contains sodium bisulphite that may result
into allergic reactions which may be mild to severe.
Adverse reactions: Systematic administration of adrenalin causes adverse reactions such
as restlessness, weakness, sweating, anxiety, tremor, apprehensiveness, respiratory
difficulties etc.
Incorrect locations of injection: Incorrect location of adrenalin injections may also lad to
adverse effects (Jacobs and et.al., 2011). For example, if adrenalin injections
administered at the same site for second time, it leads to tissue necrosis.
Infections: Also, serious infections may be caused at the site of adrenalin injections.
2. Adrenaline should not be injected into hands, feet, nose, ears, genitaliaor buttocks. Explain
why this warning is given
The warning that adrenalin should not be injected in hands, feet, nose, ears, genitalia or buttocks
is given due to the following reasons:
Buttock: adrenalin should not be injected into buttock as it may lead to ineffective
treatment. Also, clostridial infections or gas gangrene may develop (Syal, Ohri and
3
Thakur, 2011). Further, even cleaning of this site with alcohol does not lower the risk as
it fails to kill bacterial spores.
Digits, hands or feet: Warning is provided that adrenalin should not be injected to these
sites because epinephrine works as a strong vasoconstrictor. Therefore, if it is injected at
these sites, it results in loss of blood flow to the affected area. This can further result in
tissue necrosis.
Adrenalin is also not injected into nose, ears and genitalia as it leads to complications
(Schmidt and Weinshenker, 2014).
3. Anxiety, fear, tenseness, restlessness, irritability are potential adverse responses to adrenaline.
Explain why these responses may occur
There are various adverse response to adrenalin. These include anxiety, fear, restlessness,
tremors etc. Tremors are cause due to adrenalin because it feeds energy into the body and
prepares the body for to either run or fight. Further, it also leads to constriction of blood vessels.
This results in shaking of the body or tremors.
Adrenaline leads to release of glucose which is to be used during flight or fight response.
However, when no danger is present the excess energy generated as a result of glucose cannot be
used anywhere. This leads to the feeling of restlessness and irritability (Syal, Ohri and Thakur,
2011). This also leads to the feelings of nervousness.
4. Repeated dosing can lead to metabolic acidosis. Explain how metabolic acidosis can
eventuate.
Metabolic acidosis refers to a situation when there is excessive accumulation of non-
volatile acid. It is manifested in the form a primary reduction in the concentration of serum
bicarbonate which is related to low plasma pH (Nolan and Perkins, 2013). Overdose of adrenalin
results in metabolic acidosis sue to elevated concentrations of lactic acid in the blood.
Adrenaline leads to a prompt increase in blood glucose concentration in post absorptive
state. A transient increase in hepatic glucose production mediates this effect. It is also mediated
by inhibition of glucose disposal by tissues that are insulin dependent. Due to epinephrine, the
conversion of hepatic glycogenolysis and glycolysis to lactate is enhanced. This brings a
reduction in the utilization of pyruvate which results in lactic acidosis in massive doses
(Nandwani and et.al., 2010).
4
it fails to kill bacterial spores.
Digits, hands or feet: Warning is provided that adrenalin should not be injected to these
sites because epinephrine works as a strong vasoconstrictor. Therefore, if it is injected at
these sites, it results in loss of blood flow to the affected area. This can further result in
tissue necrosis.
Adrenalin is also not injected into nose, ears and genitalia as it leads to complications
(Schmidt and Weinshenker, 2014).
3. Anxiety, fear, tenseness, restlessness, irritability are potential adverse responses to adrenaline.
Explain why these responses may occur
There are various adverse response to adrenalin. These include anxiety, fear, restlessness,
tremors etc. Tremors are cause due to adrenalin because it feeds energy into the body and
prepares the body for to either run or fight. Further, it also leads to constriction of blood vessels.
This results in shaking of the body or tremors.
Adrenaline leads to release of glucose which is to be used during flight or fight response.
However, when no danger is present the excess energy generated as a result of glucose cannot be
used anywhere. This leads to the feeling of restlessness and irritability (Syal, Ohri and Thakur,
2011). This also leads to the feelings of nervousness.
4. Repeated dosing can lead to metabolic acidosis. Explain how metabolic acidosis can
eventuate.
Metabolic acidosis refers to a situation when there is excessive accumulation of non-
volatile acid. It is manifested in the form a primary reduction in the concentration of serum
bicarbonate which is related to low plasma pH (Nolan and Perkins, 2013). Overdose of adrenalin
results in metabolic acidosis sue to elevated concentrations of lactic acid in the blood.
Adrenaline leads to a prompt increase in blood glucose concentration in post absorptive
state. A transient increase in hepatic glucose production mediates this effect. It is also mediated
by inhibition of glucose disposal by tissues that are insulin dependent. Due to epinephrine, the
conversion of hepatic glycogenolysis and glycolysis to lactate is enhanced. This brings a
reduction in the utilization of pyruvate which results in lactic acidosis in massive doses
(Nandwani and et.al., 2010).
4
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
5. Explain why a caution is given with respect to using adrenaline in those with Parkinsonism
A caution is given for adrenalin use with patients suffering from Parkinson’s disease.
This is because a psychomotor agitation may be experienced by persons suffering with
Parkinson’s disease if they are administered adrenalin (Robertson and et.al., 2011). It may also
lead to worsening of symptoms.
5
A caution is given for adrenalin use with patients suffering from Parkinson’s disease.
This is because a psychomotor agitation may be experienced by persons suffering with
Parkinson’s disease if they are administered adrenalin (Robertson and et.al., 2011). It may also
lead to worsening of symptoms.
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

REFERENCES
Journals and books
Frew, A. J. (2011). What are the ‘ideal’features of an adrenaline (epinephrine) auto‐injector in
the treatment of anaphylaxis?. Allergy, 66(1), 15-24.
Jacobs, I. G. & et.al., (2011). Effect of adrenaline on survival in out-of-hospital cardiac arrest: a
randomised double-blind placebo-controlled trial. Resuscitation, 82(9), 1138-1143.
Nolan, J. P., & Perkins, G. D. (2013). Is there a role for adrenaline during cardiopulmonary
resuscitation?. Current opinion in critical care, 19(3), 169-174.
Robertson, N. & et.al., (2011). The properties of thermostabilised G protein-coupled receptors
(StaRs) and their use in drug discovery. Neuropharmacology, 60(1), 36-44.
Schmidt, K. T., & Weinshenker, D. (2014). Adrenaline rush: the role of adrenergic receptors in
stimulant-induced behaviors. Molecular pharmacology, 85(4), 640-650.
Syal, K., Ohri, A., & Thakur, J. R. (2011). Adrenaline induced pulmonary oedema. Journal of
anaesthesiology, clinical pharmacology, 27(1), 132.
Tripathi, K. D. (2013). Essentials of medical pharmacology. JP Medical Ltd.
Nandwani, S., & et.al., (2010). Lactic Acidosis In Critically Ill Patients. People’s Journal of
Scientific Research, 3(1),
6
Journals and books
Frew, A. J. (2011). What are the ‘ideal’features of an adrenaline (epinephrine) auto‐injector in
the treatment of anaphylaxis?. Allergy, 66(1), 15-24.
Jacobs, I. G. & et.al., (2011). Effect of adrenaline on survival in out-of-hospital cardiac arrest: a
randomised double-blind placebo-controlled trial. Resuscitation, 82(9), 1138-1143.
Nolan, J. P., & Perkins, G. D. (2013). Is there a role for adrenaline during cardiopulmonary
resuscitation?. Current opinion in critical care, 19(3), 169-174.
Robertson, N. & et.al., (2011). The properties of thermostabilised G protein-coupled receptors
(StaRs) and their use in drug discovery. Neuropharmacology, 60(1), 36-44.
Schmidt, K. T., & Weinshenker, D. (2014). Adrenaline rush: the role of adrenergic receptors in
stimulant-induced behaviors. Molecular pharmacology, 85(4), 640-650.
Syal, K., Ohri, A., & Thakur, J. R. (2011). Adrenaline induced pulmonary oedema. Journal of
anaesthesiology, clinical pharmacology, 27(1), 132.
Tripathi, K. D. (2013). Essentials of medical pharmacology. JP Medical Ltd.
Nandwani, S., & et.al., (2010). Lactic Acidosis In Critically Ill Patients. People’s Journal of
Scientific Research, 3(1),
6
1 out of 8


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.