Clinical Analysis and Management of Systolic Heart Failure: A Report
VerifiedAdded on 2022/10/13
|11
|2894
|19
Report
AI Summary
This report provides a detailed analysis of a case involving a 78-year-old patient, Mrs. Brown, admitted to the hospital with severe shortness of breath and a history of heart failure. The report explores the pathophysiology of systolic heart failure, including the reduced cardiac output due to enlarged left ventricles, leading to decreased oxygen supply, kidney dysfunction, atrial fibrillation, and increased heart rate. It examines the patient's clinical presentation, including high blood pressure, rapid respiratory rate, and low oxygen saturation, which confirmed the diagnosis of systolic heart failure. The report then outlines nursing strategies, such as monitoring vital signs and implementing effective medication and oxygen therapy, including Furosemide and Sublingual Glyceryl Trinitrite (GTN), to manage the patient's condition. References to relevant research papers are included to support the analysis and treatment approaches.
Running head: SYSTOLIC HEART FAILURE
SYSTOLIC HEART FAILURE
Name of Student
Name of University
SYSTOLIC HEART FAILURE
Name of Student
Name of University
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1SYSTOLIC HEART FAILURE
Author’s Note
Author’s Note
2SYSTOLIC HEART FAILURE
Acute Exacerbation of Heart
Failure
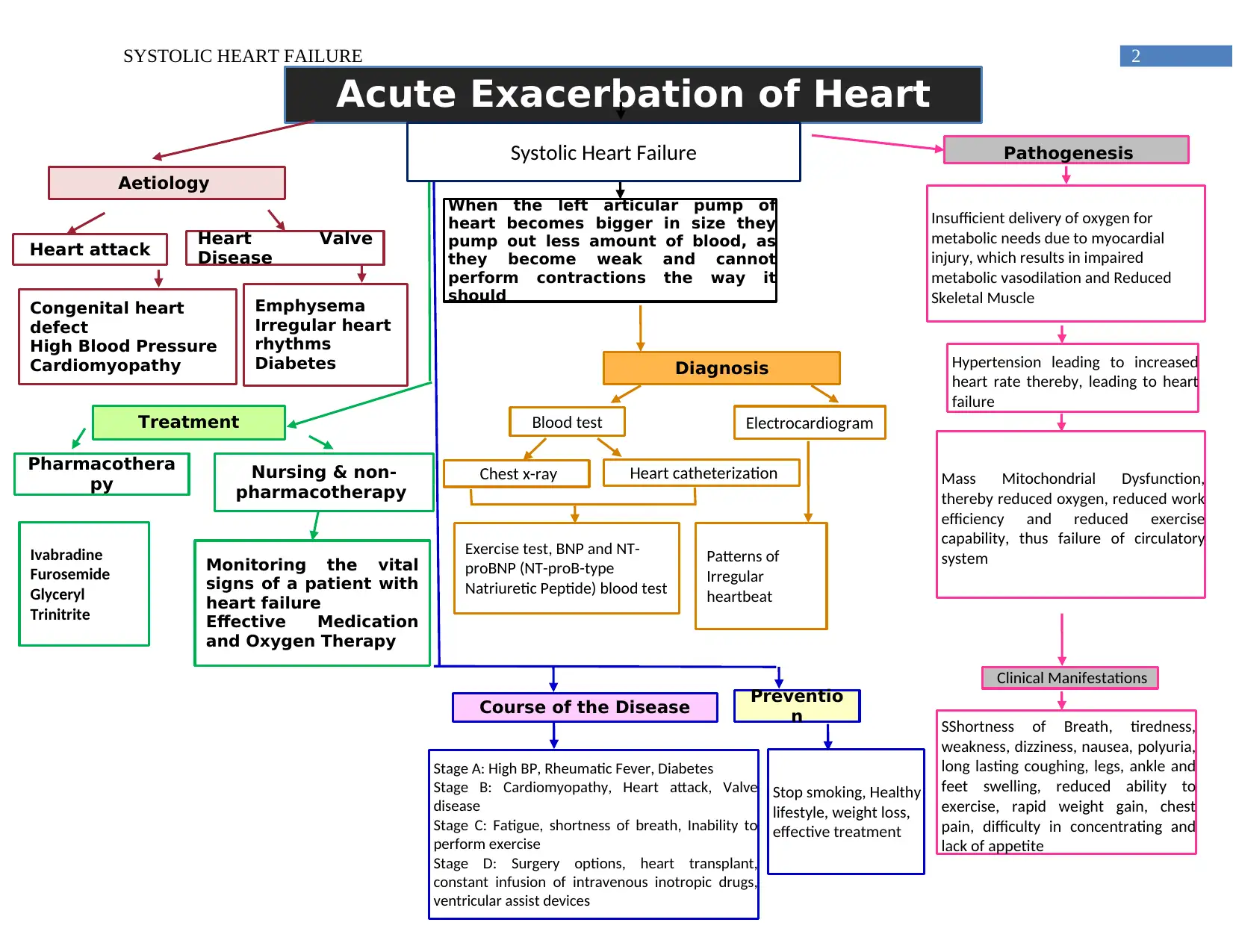
Aetiology
Congenital heart
defect
High Blood Pressure
Cardiomyopathy
Heart attack Heart Valve
Disease
Emphysema
Irregular heart
rhythms
Diabetes
Pathogenesis
Hypertension leading to increased
heart rate thereby, leading to heart
failure
Mass Mitochondrial Dysfunction,
thereby reduced oxygen, reduced work
efficiency and reduced exercise
capability, thus failure of circulatory
system
Clinical Manifestations
SShortness of Breath, tiredness,
weakness, dizziness, nausea, polyuria,
long lasting coughing, legs, ankle and
feet swelling, reduced ability to
exercise, rapid weight gain, chest
pain, difficulty in concentrating and
lack of appetite
Insufficient delivery of oxygen for
metabolic needs due to myocardial
injury, which results in impaired
metabolic vasodilation and Reduced
Skeletal Muscle
Treatment
Ivabradine
Furosemide
Glyceryl
Trinitrite
Pharmacothera
py Nursing & non-
pharmacotherapy
Monitoring the vital
signs of a patient with
heart failure
Effective Medication
and Oxygen Therapy
Diagnosis
Exercise test, BNP and NT-
proBNP (NT-proB-type
Natriuretic Peptide) blood test
Chest x-ray Heart catheterization
Patterns of
Irregular
heartbeat
Blood test Electrocardiogram
Course of the Disease Preventio
n
Stage A: High BP, Rheumatic Fever, Diabetes
Stage B: Cardiomyopathy, Heart attack, Valve
disease
Stage C: Fatigue, shortness of breath, Inability to
perform exercise
Stage D: Surgery options, heart transplant,
constant infusion of intravenous inotropic drugs,
ventricular assist devices
Stop smoking, Healthy
lifestyle, weight loss,
effective treatment
Systolic Heart Failure
When the left articular pump of
heart becomes bigger in size they
pump out less amount of blood, as
they become weak and cannot
perform contractions the way it
should
Acute Exacerbation of Heart
Failure
Aetiology
Congenital heart
defect
High Blood Pressure
Cardiomyopathy
Heart attack Heart Valve
Disease
Emphysema
Irregular heart
rhythms
Diabetes
Pathogenesis
Hypertension leading to increased
heart rate thereby, leading to heart
failure
Mass Mitochondrial Dysfunction,
thereby reduced oxygen, reduced work
efficiency and reduced exercise
capability, thus failure of circulatory
system
Clinical Manifestations
SShortness of Breath, tiredness,
weakness, dizziness, nausea, polyuria,
long lasting coughing, legs, ankle and
feet swelling, reduced ability to
exercise, rapid weight gain, chest
pain, difficulty in concentrating and
lack of appetite
Insufficient delivery of oxygen for
metabolic needs due to myocardial
injury, which results in impaired
metabolic vasodilation and Reduced
Skeletal Muscle
Treatment
Ivabradine
Furosemide
Glyceryl
Trinitrite
Pharmacothera
py Nursing & non-
pharmacotherapy
Monitoring the vital
signs of a patient with
heart failure
Effective Medication
and Oxygen Therapy
Diagnosis
Exercise test, BNP and NT-
proBNP (NT-proB-type
Natriuretic Peptide) blood test
Chest x-ray Heart catheterization
Patterns of
Irregular
heartbeat
Blood test Electrocardiogram
Course of the Disease Preventio
n
Stage A: High BP, Rheumatic Fever, Diabetes
Stage B: Cardiomyopathy, Heart attack, Valve
disease
Stage C: Fatigue, shortness of breath, Inability to
perform exercise
Stage D: Surgery options, heart transplant,
constant infusion of intravenous inotropic drugs,
ventricular assist devices
Stop smoking, Healthy
lifestyle, weight loss,
effective treatment
Systolic Heart Failure
When the left articular pump of
heart becomes bigger in size they
pump out less amount of blood, as
they become weak and cannot
perform contractions the way it
should
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3SYSTOLIC HEART FAILURE
Question 1
Mrs. Brown (78 year old) was admitted to the hospital because of severe shortness of breath and the doctors were told about
her medical history of heart failure. In the case of a systolic heart failure, cardiac output is reduced as the size of the left ventricles
muscles increases and thereby loses the capability to pump adequate amount of blood efficiently (Alpert et al., 2014), leading to low
amount of oxygen, inability of the kidney to remove excess fluids, atrial fibrillation and increased heart rate. This oxygen loss further
results in various dysfunctions of the body, as oxygen is the primary source for the efficient metabolism and functioning of the body
and the reduced levels of oxygen results in the increased blood pressure, decreased oxygen saturation, increased heart rate and
increased respiration rate (Harjola et al., 2017). Due to the inactivity of the kidneys to remove excess fluids, the renin (also termed as
angiotensinogenase) release converts the Angiotensin 1 to Angiotensin 2 (Sayer & Bhat, 2014) by effectively participating in the
body's renin–angiotensin–aldosterone system, which is responsible for resolving the amount of excess fluid and vasoconstriction of
arteries (Clark, Krum & Hopper, 2014). Thereby increasing the blood pressure and increased aldosterone biosynthesis, thereby
increasing the reabsorption of salt and water and increased volume of extracellular fluid. Angiotensin 2 further leads the pituitary
gland to secrete huge amount of antidiuretic hormones. Antidiuretic hormones are responsible for maintaining the water balance in the
blood, thus increased amount of the hormone results in increased concentration of water in blood (Ter Maaten et al., 2015), which
thereby causes increase in volume and blood pressure. With the reduced amount of blood flow from heart, the carotid baroreceptor
starts responding to the changes of the pressure and blood flow amount of the heart (Ponikowski et al., 2014). The response of carotid
Question 1
Mrs. Brown (78 year old) was admitted to the hospital because of severe shortness of breath and the doctors were told about
her medical history of heart failure. In the case of a systolic heart failure, cardiac output is reduced as the size of the left ventricles
muscles increases and thereby loses the capability to pump adequate amount of blood efficiently (Alpert et al., 2014), leading to low
amount of oxygen, inability of the kidney to remove excess fluids, atrial fibrillation and increased heart rate. This oxygen loss further
results in various dysfunctions of the body, as oxygen is the primary source for the efficient metabolism and functioning of the body
and the reduced levels of oxygen results in the increased blood pressure, decreased oxygen saturation, increased heart rate and
increased respiration rate (Harjola et al., 2017). Due to the inactivity of the kidneys to remove excess fluids, the renin (also termed as
angiotensinogenase) release converts the Angiotensin 1 to Angiotensin 2 (Sayer & Bhat, 2014) by effectively participating in the
body's renin–angiotensin–aldosterone system, which is responsible for resolving the amount of excess fluid and vasoconstriction of
arteries (Clark, Krum & Hopper, 2014). Thereby increasing the blood pressure and increased aldosterone biosynthesis, thereby
increasing the reabsorption of salt and water and increased volume of extracellular fluid. Angiotensin 2 further leads the pituitary
gland to secrete huge amount of antidiuretic hormones. Antidiuretic hormones are responsible for maintaining the water balance in the
blood, thus increased amount of the hormone results in increased concentration of water in blood (Ter Maaten et al., 2015), which
thereby causes increase in volume and blood pressure. With the reduced amount of blood flow from heart, the carotid baroreceptor
starts responding to the changes of the pressure and blood flow amount of the heart (Ponikowski et al., 2014). The response of carotid
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4SYSTOLIC HEART FAILURE
bio receptor results in the increased activities of sympathetic nervous system. This increased activity causes rapid regulation of
homeostasis, leading to increased pressure and respiration rate. With the increased respiration rate the heartbeats increases to supply
the required amount of Oxygen, but due to increased size of ventricular muscles, the supply of oxygen is very low, causing decreased
rate of saturation oxygen. Due to the failure of the enough supply of oxygen, the chances of myocardial infarction (inotropy) are
elevated (Johnson, 2014). These risk levels leads to the possibility of vasoconstriction or systolic heart failure because of the
narrowing of the blood vessels because of the contraction of muscles and arteries both large and small (van Riet et al., 2016).
All these symptoms were primarily observed in the patient, Mrs. Brown. After the admission procedure, several tests were
performed to have an overall body checkup. Her blood pressure was found to be extremely high (170/95mmHg), and for which
indicated the chances of myocardial infarction, as the she already had a history of heart failure. Her respiratory rate was found to be
24 breaths per minute, which further indicated low amount of oxygen in her body. After checking her percentage of oxygen
saturation, it was found to be 85% in room air, which is extremely low and proved that the levels of oxygen were very low in her
body. This low level of oxygen further indicated the rick of systolic heart failure. For an individual to have heart failure the heart rate
will be increased and in the case of Mrs. Brown, her heart beat rate was found to be 120 beats/minute, clearly indicating that she was
suffering from a systolic heart failure. Her shortness of breath and less amount of oxygen resulted in bilateral basal crackles identified
because of her auscultation of lungs. All the clinical manifestations lead to the confirmation of systolic heart failure. An ECG monitor
was connected to monitor her heart rate, which further showed atrial fibrillation, which occurs when the heart rate is irregular and
causes reduced blood flow from the heart. The patient was also suffering from severe dysponea in the morning before she was
bio receptor results in the increased activities of sympathetic nervous system. This increased activity causes rapid regulation of
homeostasis, leading to increased pressure and respiration rate. With the increased respiration rate the heartbeats increases to supply
the required amount of Oxygen, but due to increased size of ventricular muscles, the supply of oxygen is very low, causing decreased
rate of saturation oxygen. Due to the failure of the enough supply of oxygen, the chances of myocardial infarction (inotropy) are
elevated (Johnson, 2014). These risk levels leads to the possibility of vasoconstriction or systolic heart failure because of the
narrowing of the blood vessels because of the contraction of muscles and arteries both large and small (van Riet et al., 2016).
All these symptoms were primarily observed in the patient, Mrs. Brown. After the admission procedure, several tests were
performed to have an overall body checkup. Her blood pressure was found to be extremely high (170/95mmHg), and for which
indicated the chances of myocardial infarction, as the she already had a history of heart failure. Her respiratory rate was found to be
24 breaths per minute, which further indicated low amount of oxygen in her body. After checking her percentage of oxygen
saturation, it was found to be 85% in room air, which is extremely low and proved that the levels of oxygen were very low in her
body. This low level of oxygen further indicated the rick of systolic heart failure. For an individual to have heart failure the heart rate
will be increased and in the case of Mrs. Brown, her heart beat rate was found to be 120 beats/minute, clearly indicating that she was
suffering from a systolic heart failure. Her shortness of breath and less amount of oxygen resulted in bilateral basal crackles identified
because of her auscultation of lungs. All the clinical manifestations lead to the confirmation of systolic heart failure. An ECG monitor
was connected to monitor her heart rate, which further showed atrial fibrillation, which occurs when the heart rate is irregular and
causes reduced blood flow from the heart. The patient was also suffering from severe dysponea in the morning before she was
5SYSTOLIC HEART FAILURE
admitted to the hospital, this usually happens when the patient is suffering from acute asthma, heart failure, interstitial lung disease or
chronic obstructive pulmonary disease. In the case, Mrs. Brown’s severe dysponea might be because of her medical history of heart
failure and as per her symptoms, it can be deduced that she is again suffering from systolic heart failure.
Nursing Strategies:
Monitoring the vital signs of a patient with heart failure
Patient with systolic heart failure have a very low cardiac output because of the increase in size of the left ventricles, which
then is not capable of pumping blood out of the heart, resulting in increased heart beat and eventually heart failure. In the given case
the patient, Mrs. Brown, when admitted to the hospital had a heart rate of 120 beats per minute, which is double than the normal rate
of an individual, which is 72 beats per minute. In order to closely monitor the heart rates and other vital signs, the nurses prioritize the
monitoring, as these monitoring further helps the physicians and nurses in designing the healthcare plan (Ekström, Abernethy &
Currow, 2015). The nurses check pulse patterns, blood pressure, patient’s saturation, respiration rate and the body temperature,
because of the low amount of oxygen in the body, the functioning of the organs are hampered severely (Park, 2014). The patient in the
case study had a blood pressure of 170/95mmHg, which is very high for a normal and healthy individual, apart from the blood
pressure, the patient’s respiratory rate was 24breath/minute, which is also very high for a normal and healthy individual. Lastly, the
patient’s oxygen saturation rate was found to be very low i.e. 85% on room air, all these symptoms comprises of the systolic heart
admitted to the hospital, this usually happens when the patient is suffering from acute asthma, heart failure, interstitial lung disease or
chronic obstructive pulmonary disease. In the case, Mrs. Brown’s severe dysponea might be because of her medical history of heart
failure and as per her symptoms, it can be deduced that she is again suffering from systolic heart failure.
Nursing Strategies:
Monitoring the vital signs of a patient with heart failure
Patient with systolic heart failure have a very low cardiac output because of the increase in size of the left ventricles, which
then is not capable of pumping blood out of the heart, resulting in increased heart beat and eventually heart failure. In the given case
the patient, Mrs. Brown, when admitted to the hospital had a heart rate of 120 beats per minute, which is double than the normal rate
of an individual, which is 72 beats per minute. In order to closely monitor the heart rates and other vital signs, the nurses prioritize the
monitoring, as these monitoring further helps the physicians and nurses in designing the healthcare plan (Ekström, Abernethy &
Currow, 2015). The nurses check pulse patterns, blood pressure, patient’s saturation, respiration rate and the body temperature,
because of the low amount of oxygen in the body, the functioning of the organs are hampered severely (Park, 2014). The patient in the
case study had a blood pressure of 170/95mmHg, which is very high for a normal and healthy individual, apart from the blood
pressure, the patient’s respiratory rate was 24breath/minute, which is also very high for a normal and healthy individual. Lastly, the
patient’s oxygen saturation rate was found to be very low i.e. 85% on room air, all these symptoms comprises of the systolic heart
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6SYSTOLIC HEART FAILURE
failure and thus nurses choses to prioritize to monitor these readings first, because it was important to reduce and increase the
respective levels, so that the patient remains out of danger.
Effective Medication and Oxygen Therapy
The second strategy, which the nurses prioritize, is the implementation of effective medications and oxygen therapy. The
medications were necessary to bring the body back to normal and healthy state. With the extreme low amount of oxygen, the body was
in extreme danger, thus oxygen therapy was a must, to increase the levels of oxygen and reduce the chances of ultimate heart failure.
The nurses with efficient pharmacological knowledge are appointed for providing medications to the patients with heart failure, as
accurate amount of medications are required to reduce the size of left ventricular pumps (Ekström, Abernethy & Currow, 2015). The
medicines like digitalis (to enhance the heart contractions), furosemide (to improve the elimination rate of extra fluids from the body),
ACE inhibitors (to prohibit the transformation of Angiotensin1 to 2, hence prohibiting the reabsorption of fluid and salt) and oxygen
supply (efficient saturation), requires pharmacological knowledge and a slight mistake can lead to the death of the patient. With the
help of these medications the patient’s body boosts the treatment procedure and thereby the nurses prioritize it.
Furosemide
This drug is used to eliminate the excess amount of fluid from the body by means of urination and helps in the improvisation
of the functions of kidney, as kidneys also helps in flushing out the excess fluid. The only side effect of this particular medication is
failure and thus nurses choses to prioritize to monitor these readings first, because it was important to reduce and increase the
respective levels, so that the patient remains out of danger.
Effective Medication and Oxygen Therapy
The second strategy, which the nurses prioritize, is the implementation of effective medications and oxygen therapy. The
medications were necessary to bring the body back to normal and healthy state. With the extreme low amount of oxygen, the body was
in extreme danger, thus oxygen therapy was a must, to increase the levels of oxygen and reduce the chances of ultimate heart failure.
The nurses with efficient pharmacological knowledge are appointed for providing medications to the patients with heart failure, as
accurate amount of medications are required to reduce the size of left ventricular pumps (Ekström, Abernethy & Currow, 2015). The
medicines like digitalis (to enhance the heart contractions), furosemide (to improve the elimination rate of extra fluids from the body),
ACE inhibitors (to prohibit the transformation of Angiotensin1 to 2, hence prohibiting the reabsorption of fluid and salt) and oxygen
supply (efficient saturation), requires pharmacological knowledge and a slight mistake can lead to the death of the patient. With the
help of these medications the patient’s body boosts the treatment procedure and thereby the nurses prioritize it.
Furosemide
This drug is used to eliminate the excess amount of fluid from the body by means of urination and helps in the improvisation
of the functions of kidney, as kidneys also helps in flushing out the excess fluid. The only side effect of this particular medication is
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7SYSTOLIC HEART FAILURE
the risk of dehydration, because with the elimination of the excess fluid, the amount of salt in the body is also reduced, thereby
causing dehydration (De Vecchis et al., 2015). Therefore, in this case the patient, Mrs. Brown, is provided with this medicine, in order
to lower down the patient’s blood pressure which is extremely high (170/95mmHg).
Sublingual Glyceryl Trinitrite (GTN)
GTN is vasodilating agent and assists in lowering of pulmonary vascular resistance. It helps in the relaxation of the smooth
heart muscles (Hope et al., 2014). In the given case study, the patient, Mrs. Brown, has a heartbeat of 120 beats per minute which is
almost double than the heartbeats of a healthy individual. The reason behind increased heart rate is the increase in size of the left
ventricular pumps of the heart, leading to low output of oxygen. This medication helps in the smoothening of the muscles and helps in
regulation of oxygen transport, by helping the muscles to pump out adequate amount of oxygen from the heart, so that the organs
functions properly.
the risk of dehydration, because with the elimination of the excess fluid, the amount of salt in the body is also reduced, thereby
causing dehydration (De Vecchis et al., 2015). Therefore, in this case the patient, Mrs. Brown, is provided with this medicine, in order
to lower down the patient’s blood pressure which is extremely high (170/95mmHg).
Sublingual Glyceryl Trinitrite (GTN)
GTN is vasodilating agent and assists in lowering of pulmonary vascular resistance. It helps in the relaxation of the smooth
heart muscles (Hope et al., 2014). In the given case study, the patient, Mrs. Brown, has a heartbeat of 120 beats per minute which is
almost double than the heartbeats of a healthy individual. The reason behind increased heart rate is the increase in size of the left
ventricular pumps of the heart, leading to low output of oxygen. This medication helps in the smoothening of the muscles and helps in
regulation of oxygen transport, by helping the muscles to pump out adequate amount of oxygen from the heart, so that the organs
functions properly.
8SYSTOLIC HEART FAILURE
References
Alpert, M. A., Lavie, C. J., Agrawal, H., Aggarwal, K. B., & Kumar, S. A. (2014). Obesity and heart failure: epidemiology,
pathophysiology, clinical manifestations, and management. Translational Research, 164(4), 345-356.
https://doi.org/10.1016/j.trsl.2014.04.010
Clark, H., Krum, H., & Hopper, I. (2014). Worsening renal function during renin–angiotensin–aldosterone system inhibitor initiation
and long‐term outcomes in patients with left ventricular systolic dysfunction. European journal of heart failure, 16(1), 41-48.
doi:10.1002/ejhf.13
De Vecchis, R., Esposito, C., Ariano, C., & Cantatrione, S. (2015). Hypertonic saline plus iv furosemide improve renal safety profile
and clinical outcomes in acute decompensated heart failure. Herz, 40(3), 423-435.
https://link.springer.com/article/10.1007/s00059-013-4041-6
Ekström, M. P., Abernethy, A. P., & Currow, D. C. (2015). The management of chronic breathlessness in patients with advanced and
terminal illness. Bmj, 349, g7617. doi: 10.1136/bmj.g7617
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P., Chioncel, O., ... & Fuhrmann, V. (2017).
Organ dysfunction, injury and failure in acute heart failure: from pathophysiology to diagnosis and management. A review on
References
Alpert, M. A., Lavie, C. J., Agrawal, H., Aggarwal, K. B., & Kumar, S. A. (2014). Obesity and heart failure: epidemiology,
pathophysiology, clinical manifestations, and management. Translational Research, 164(4), 345-356.
https://doi.org/10.1016/j.trsl.2014.04.010
Clark, H., Krum, H., & Hopper, I. (2014). Worsening renal function during renin–angiotensin–aldosterone system inhibitor initiation
and long‐term outcomes in patients with left ventricular systolic dysfunction. European journal of heart failure, 16(1), 41-48.
doi:10.1002/ejhf.13
De Vecchis, R., Esposito, C., Ariano, C., & Cantatrione, S. (2015). Hypertonic saline plus iv furosemide improve renal safety profile
and clinical outcomes in acute decompensated heart failure. Herz, 40(3), 423-435.
https://link.springer.com/article/10.1007/s00059-013-4041-6
Ekström, M. P., Abernethy, A. P., & Currow, D. C. (2015). The management of chronic breathlessness in patients with advanced and
terminal illness. Bmj, 349, g7617. doi: 10.1136/bmj.g7617
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P., Chioncel, O., ... & Fuhrmann, V. (2017).
Organ dysfunction, injury and failure in acute heart failure: from pathophysiology to diagnosis and management. A review on
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9SYSTOLIC HEART FAILURE
behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology
(ESC). European journal of heart failure, 19(7), 821-836. https://doi.org/10.1002/ejhf.872
Hope, K., Eglin, C., Golden, F., & Tipton, M. (2014). Sublingual glyceryl trinitrate and the peripheral thermal responses in normal and
cold-sensitive individuals. Microvascular research, 91, 84-89.
https://www.researchgate.net/profile/Katrina_Hope/publication/259092828_Peripheral_thermal_responses_in_normal_and_col
d-sensitive_individuals_to_sublingual_Glyceryl_Trinitrate_GTN/links/5513dcef0cf2eda0df302f3a/Peripheral-thermal-
responses-in-normal-and-cold-sensitive-individuals-to-sublingual-Glyceryl-Trinitrate-GTN.pdf
Johnson, F. L. (2014). Pathophysiology and etiology of heart failure. Cardiol Clin, 32(1), 9-19. https://books.google.co.in/books?
hl=en&lr=&id=28vaAgAAQBAJ&oi=fnd&pg=PA9&dq=systolic+heart+failure+pathophysiology&ots=V0T8_q8KbS&sig=0a
XeAS1iJ00jiRqy-R11T8gB9L8#v=onepage&q=systolic%20heart%20failure%20pathophysiology&f=false
Park, H. (2014). Identifying core NANDA‐I nursing diagnoses, NIC interventions, NOC outcomes, and NNN linkages for heart
failure. International journal of nursing knowledge, 25(1), 30-38. https://doi.org/10.1111/2047-3095.12010
Ponikowski, P., Anker, S. D., AlHabib, K. F., Cowie, M. R., Force, T. L., Hu, S., ... & Samal, U. C. (2014). Heart failure: preventing
disease and death worldwide. ESC heart failure, 1(1), 4-25. DOI:10.1002/ehf2.12005
behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology
(ESC). European journal of heart failure, 19(7), 821-836. https://doi.org/10.1002/ejhf.872
Hope, K., Eglin, C., Golden, F., & Tipton, M. (2014). Sublingual glyceryl trinitrate and the peripheral thermal responses in normal and
cold-sensitive individuals. Microvascular research, 91, 84-89.
https://www.researchgate.net/profile/Katrina_Hope/publication/259092828_Peripheral_thermal_responses_in_normal_and_col
d-sensitive_individuals_to_sublingual_Glyceryl_Trinitrate_GTN/links/5513dcef0cf2eda0df302f3a/Peripheral-thermal-
responses-in-normal-and-cold-sensitive-individuals-to-sublingual-Glyceryl-Trinitrate-GTN.pdf
Johnson, F. L. (2014). Pathophysiology and etiology of heart failure. Cardiol Clin, 32(1), 9-19. https://books.google.co.in/books?
hl=en&lr=&id=28vaAgAAQBAJ&oi=fnd&pg=PA9&dq=systolic+heart+failure+pathophysiology&ots=V0T8_q8KbS&sig=0a
XeAS1iJ00jiRqy-R11T8gB9L8#v=onepage&q=systolic%20heart%20failure%20pathophysiology&f=false
Park, H. (2014). Identifying core NANDA‐I nursing diagnoses, NIC interventions, NOC outcomes, and NNN linkages for heart
failure. International journal of nursing knowledge, 25(1), 30-38. https://doi.org/10.1111/2047-3095.12010
Ponikowski, P., Anker, S. D., AlHabib, K. F., Cowie, M. R., Force, T. L., Hu, S., ... & Samal, U. C. (2014). Heart failure: preventing
disease and death worldwide. ESC heart failure, 1(1), 4-25. DOI:10.1002/ehf2.12005
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10SYSTOLIC HEART FAILURE
Sayer, G., & Bhat, G. (2014). The renin-angiotensin-aldosterone system and heart failure. Cardiology clinics, 32(1), 21-32.
https://doi.org/10.1016/j.ccl.2013.09.002
Suzuki, T., Heaney, L. M., Bhandari, S. S., Jones, D. J., & Ng, L. L. (2016). Trimethylamine N-oxide and prognosis in acute heart
failure. Heart, 102(11), 841-848. https://lra.le.ac.uk/bitstream/2381/36371/2/TMAO%20Heart%20-%20Accepted
%20Version.pdf
Ter Maaten, J. M., Valente, M. A., Damman, K., Hillege, H. L., Navis, G., & Voors, A. A. (2015). Diuretic response in acute heart
failure—pathophysiology, evaluation, and therapy. Nature Reviews Cardiology, 12(3), 184.
https://www.rug.nl/research/portal/files/32723614/Complete_thesis.pdf#page=20
van Riet, E. E., Hoes, A. W., Wagenaar, K. P., Limburg, A., Landman, M. A., & Rutten, F. H. (2016). Epidemiology of heart failure:
the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. European journal of
heart failure, 18(3), 242-252. https://doi.org/10.1002/ejhf.483
Sayer, G., & Bhat, G. (2014). The renin-angiotensin-aldosterone system and heart failure. Cardiology clinics, 32(1), 21-32.
https://doi.org/10.1016/j.ccl.2013.09.002
Suzuki, T., Heaney, L. M., Bhandari, S. S., Jones, D. J., & Ng, L. L. (2016). Trimethylamine N-oxide and prognosis in acute heart
failure. Heart, 102(11), 841-848. https://lra.le.ac.uk/bitstream/2381/36371/2/TMAO%20Heart%20-%20Accepted
%20Version.pdf
Ter Maaten, J. M., Valente, M. A., Damman, K., Hillege, H. L., Navis, G., & Voors, A. A. (2015). Diuretic response in acute heart
failure—pathophysiology, evaluation, and therapy. Nature Reviews Cardiology, 12(3), 184.
https://www.rug.nl/research/portal/files/32723614/Complete_thesis.pdf#page=20
van Riet, E. E., Hoes, A. W., Wagenaar, K. P., Limburg, A., Landman, M. A., & Rutten, F. H. (2016). Epidemiology of heart failure:
the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. European journal of
heart failure, 18(3), 242-252. https://doi.org/10.1002/ejhf.483
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.