University Mental Health MSE Assessment Report for Leroy
VerifiedAdded on 2022/10/10
|10
|2566
|10
Report
AI Summary
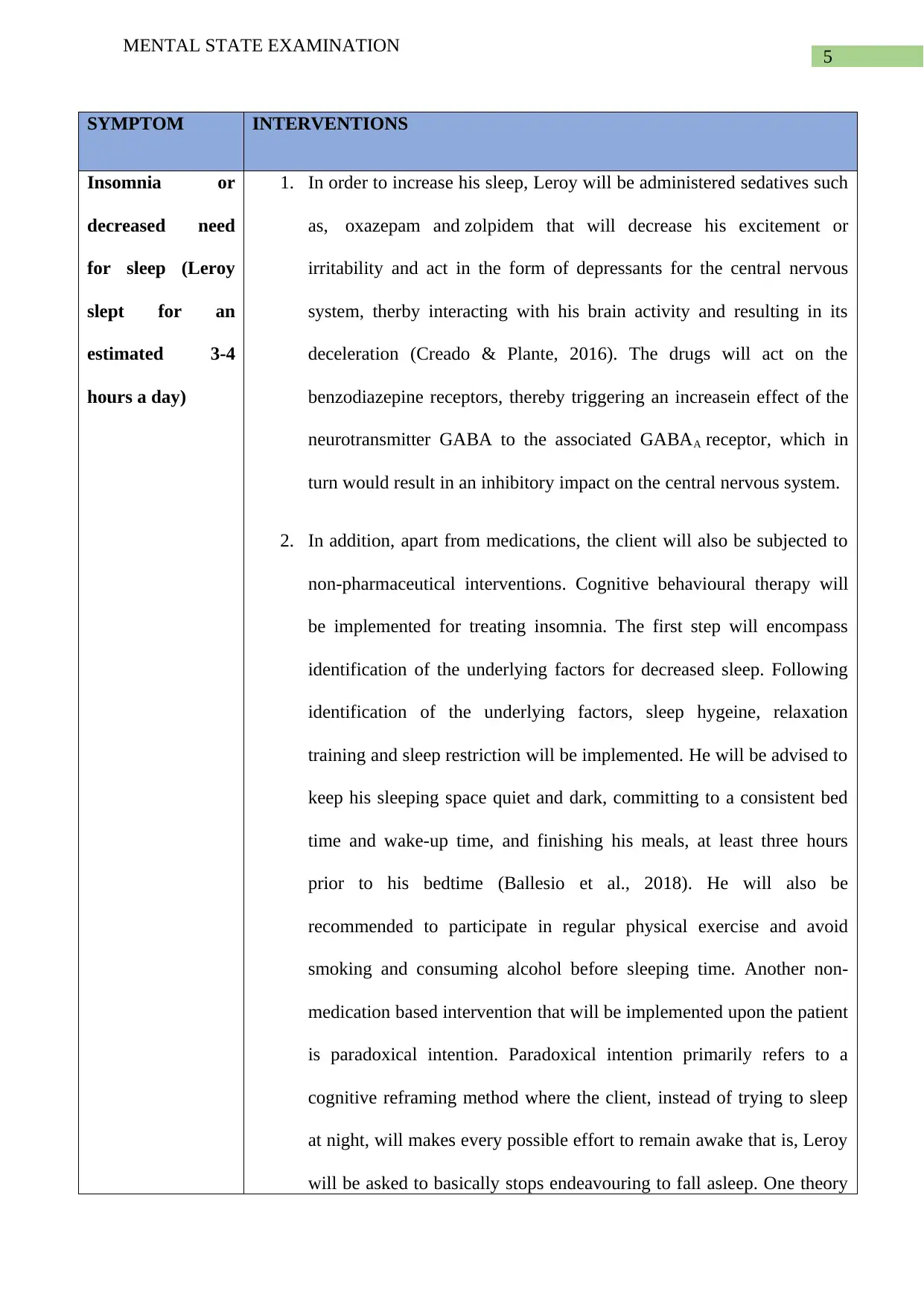
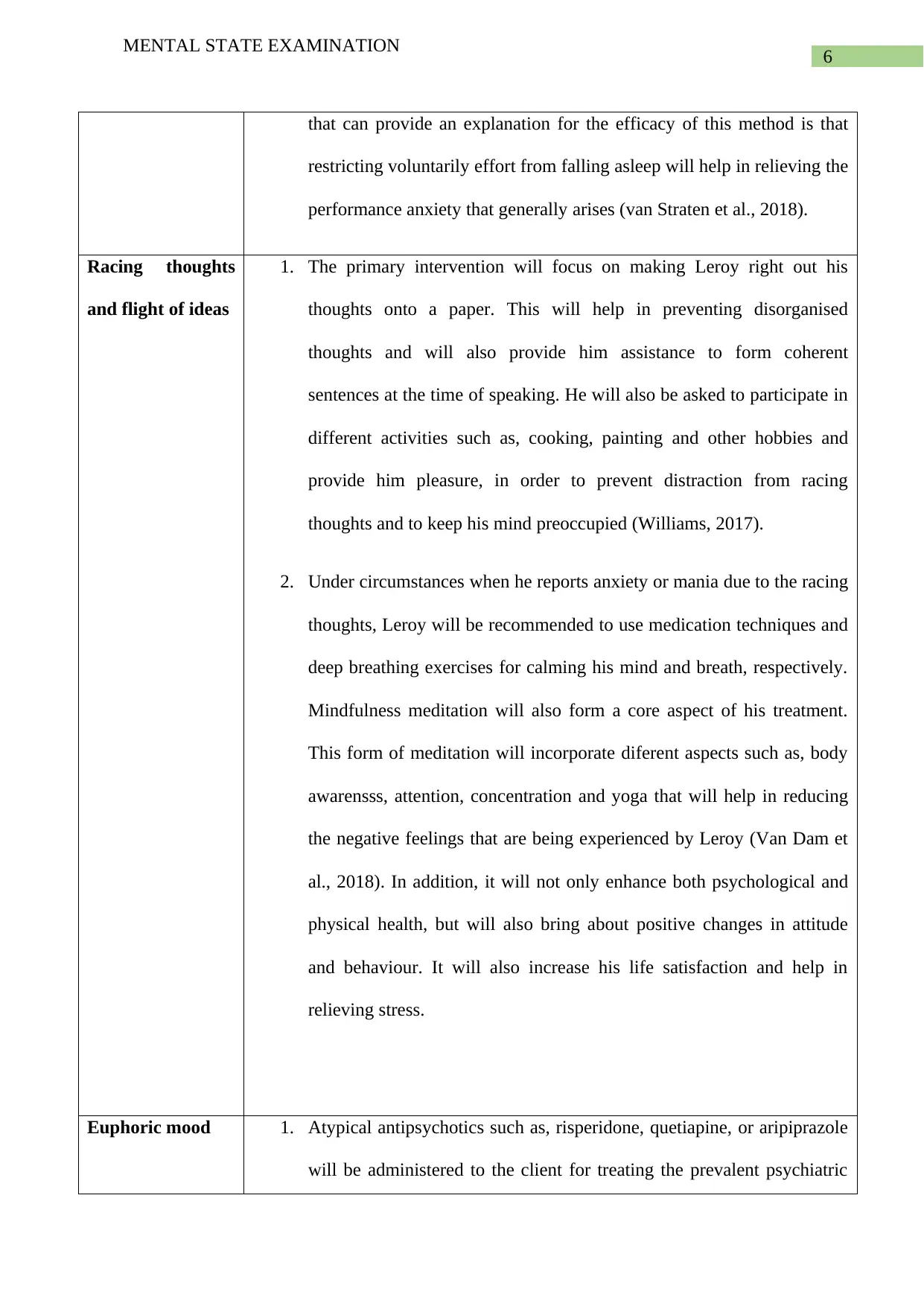
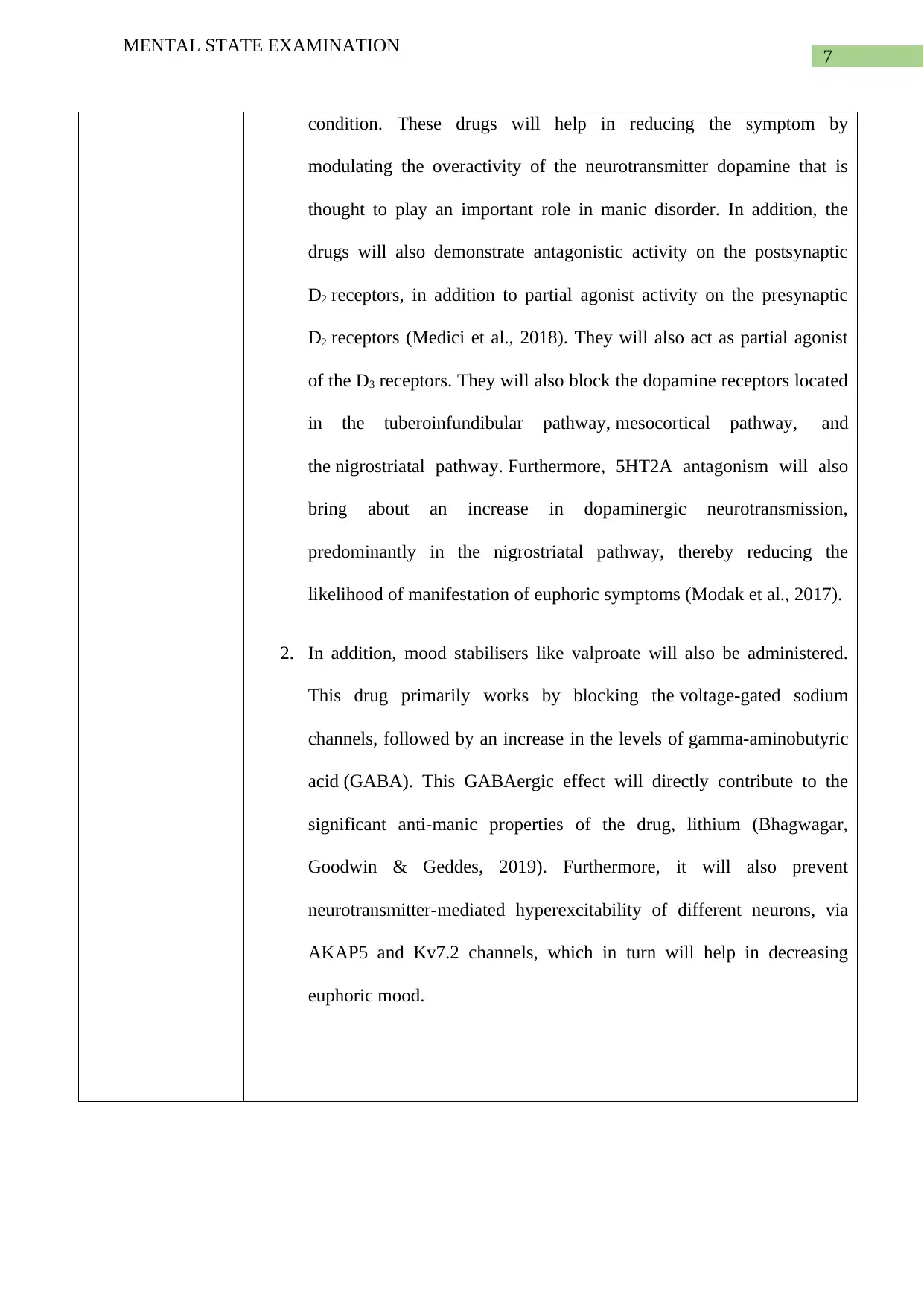
This report presents a mental state examination (MSE) assessment of a 35-year-old Caucasian male named Leroy, conducted as part of a nursing assignment. The assessment meticulously details various aspects of Leroy's mental state, including his general appearance, behavior, speech patterns, mood and affect, thought processes, thought content, perception, cognition, and judgment & insight. Leroy's presentation exhibited signs of potential mania, including a euphoric mood, rapid speech, and flight of ideas. The report further analyzes specific symptoms such as insomnia, racing thoughts, and a euphoric mood, offering detailed intervention strategies. These interventions include both pharmacological approaches, such as sedatives and atypical antipsychotics, and non-pharmacological techniques like cognitive behavioral therapy, paradoxical intention, mindfulness meditation, and recommending medication techniques. The assessment aims to provide a comprehensive overview of Leroy's mental state and propose appropriate interventions to address his symptoms.


1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.