Road Safety Policy Impact in Ethiopia: Interrupted Time Series Study
VerifiedAdded on 2023/05/29
|7
|5291
|286
Report
AI Summary
This research article, published in BMC Public Health, investigates the effectiveness of an improved road safety policy implemented in Ethiopia by the Oromia Regional State Transport Bureau in September 2007. Using an interrupted time series design, the study analyzes routine road traffic accident data from 2002 to 2011 to assess the impact of the new regulations, which included stricter enforcement of existing laws and the introduction of new ones such as the prohibition of cell phone use while driving and mandatory seat belt use. The findings reveal statistically significant reductions in non-injury crashes and fatalities following the policy implementation. Non-injury crashes decreased by 19%, and fatalities decreased by 12.4% in the first year. Despite these improvements, the overall incidence rate of crashes and fatalities remains high, indicating a need for further interventions to enhance road safety in Ethiopia. The study highlights the importance of well-designed and enforced road safety policies in reducing road traffic incidents and underscores the need for ongoing efforts to minimize the loss of lives.
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/262777017
Effectiveness of an improved road safety policy in Ethiopia: An interrupted
time series study
Article in BMC Public Health · May 2014
DOI: 10.1186/1471-2458-14-539 · Source: PubMed
CITATIONS
5
READS
919
4 authors, including:
Some of the authors of this publication are also working on these related projects:
Maternal and child health in south EthiopiaView project
Public HealthView project
Teferi Abegaz
Hawassa University
8 PUBLICATIONS63CITATIONS
SEE PROFILE
Yemane Berhane
Addis Continental Institute of Public Health
276PUBLICATIONS5,351CITATIONS
SEE PROFILE
Alemayehu Worku
Addis Ababa University
190PUBLICATIONS2,709CITATIONS
SEE PROFILE
Effectiveness of an improved road safety policy in Ethiopia: An interrupted
time series study
Article in BMC Public Health · May 2014
DOI: 10.1186/1471-2458-14-539 · Source: PubMed
CITATIONS
5
READS
919
4 authors, including:
Some of the authors of this publication are also working on these related projects:
Maternal and child health in south EthiopiaView project
Public HealthView project
Teferi Abegaz
Hawassa University
8 PUBLICATIONS63CITATIONS
SEE PROFILE
Yemane Berhane
Addis Continental Institute of Public Health
276PUBLICATIONS5,351CITATIONS
SEE PROFILE
Alemayehu Worku
Addis Ababa University
190PUBLICATIONS2,709CITATIONS
SEE PROFILE
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
R E S E A R C H A R T I C L E Open Access
Effectiveness of an improved road safety policy
Ethiopia:an interrupted time series study
TeferiAbegaz1*
, Yemane Berhane2
, Alemayehu Worku3 and Abebe Assrat4
Abstract
Background:In recent years,there has been an increasing interest in implementing road safety policy by differe
low income countries.However;the evidence is scarce on its success in the reduction of crashes,injuries and
deaths.This study was conducted to assess whether road crashes,injuries and fatalities was reduced following the
road safety regulation introduced as of September 2007 by Oromia RegionalState Transport Bureau.
Methods:Routine road traffic accident data for the year 2002-2011were collected from sixteen traffic police
Data on average daily vehicle flow was obtained from the Ethiopian Road Authority.Interrupted time series design
using segmented linear regression modelwas applied to estimate the effect of an improved road safety policy.
Results:A totalof 4,053 crashes occurred on Addis Ababa - Adama/Hawassa main road.Of these crashes,almost
half 46.4% (1,880) were property damage,29.4% (1,193) were fataland 24.2% (980) injury crashes,resulting 1,392
fatalities and 1,749 injuries.There were statistically significant reductions in non-injury crashes and deaths.Non-injury
crash was reduced by 19% and fatality by 12.4% in the first year of implementing the revised transport sa
regulation.
Conclusion: Although revised road safety policy helped in reducing motor vehicle crashes and associated
fatalities,the overallincidence rate is stillvery high.Further action is required to avoid unnecessary loss of lives.
Keywords: Road crash,Road injury,Road death,Road safety law effectiveness
Background
Road traffic crash isa growing public health threat,
being responsible for 1.2 million deaths and up to 50
million nonfatalinjuries globally.It is a big challenge
especially for low and middle income countries,90% of
the victims were found [1].Accidenttrends observed
in industrialized countries witnessed the rapid reduc-
tion over the last three to four decades,while a terrify-
ing incrementreported from a number ofdeveloping
countries including Ethiopia [2,3].The problem may
grow further in the coming decades;due to the rapid
rising ofvehicle ownership associated with their eco-
nomic growth [4].
Evidence from high income countries showed that im-
plementation of appropriately designed and well enforced
road safety policy contribute a lion share for their impres-
sive achievements ofthe declining trend in the number
and severity ofcrashes [5].According to the European
TransportSafety Councilestimation,if all existing road
safety laws in European Union are enforced up to 50% of
death and injuries could be averted [6].
Likewise in recentyears,many low income countries
are implementing improved road safety policy to deter
risky driving practices including:− exceeding the speed
limit, impaired driving by alcoholand drugs,phoning
and texting while driving,and not using seat belt [5,7].
Howeverthere islittle empiricalevidence asto their
effectiveness in reducing crashes,injuries and fatalities
[7].For example,Brazil,after implementing an improved
traffic code with stiff penalty and media coverage a 21%
and 25% reduction of injuries and fatalities,respectively,
was observed [8].A study conducted in Uganda follow-
ing,police enforcement using patrolcars equipped with
radar brings a 17% reduction of fatalities [9].In Rwanda
a 30% reduction in traffic death was observed following
an improved legislative change complimented with pub-
lic awareness campaign [10].
* Correspondence:tefabeg@yahoo.com
1Schoolof Public and EnvironmentalHealth,College of Medicine and Health
Sciences,Hawassa University,Hawassa,Ethiopia
Fulllist of author information is available at the end of the article
© 2014 Abegaz et al.;licensee BioMed CentralLtd.This is an Open Access article distributed under the terms of the Creative
Commons Attribution License (http://creativecommons.org/licenses/by/2.0),which permits unrestricted use,distribution,and
reproduction in any medium,provided the originalwork is properly credited.The Creative Commons Public Domain
Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,
unless otherwise stated.
Abegaz et al.BMC Public Health 2014,14:539
http://www.biomedcentral.com/1471-2458/14/539
Effectiveness of an improved road safety policy
Ethiopia:an interrupted time series study
TeferiAbegaz1*
, Yemane Berhane2
, Alemayehu Worku3 and Abebe Assrat4
Abstract
Background:In recent years,there has been an increasing interest in implementing road safety policy by differe
low income countries.However;the evidence is scarce on its success in the reduction of crashes,injuries and
deaths.This study was conducted to assess whether road crashes,injuries and fatalities was reduced following the
road safety regulation introduced as of September 2007 by Oromia RegionalState Transport Bureau.
Methods:Routine road traffic accident data for the year 2002-2011were collected from sixteen traffic police
Data on average daily vehicle flow was obtained from the Ethiopian Road Authority.Interrupted time series design
using segmented linear regression modelwas applied to estimate the effect of an improved road safety policy.
Results:A totalof 4,053 crashes occurred on Addis Ababa - Adama/Hawassa main road.Of these crashes,almost
half 46.4% (1,880) were property damage,29.4% (1,193) were fataland 24.2% (980) injury crashes,resulting 1,392
fatalities and 1,749 injuries.There were statistically significant reductions in non-injury crashes and deaths.Non-injury
crash was reduced by 19% and fatality by 12.4% in the first year of implementing the revised transport sa
regulation.
Conclusion: Although revised road safety policy helped in reducing motor vehicle crashes and associated
fatalities,the overallincidence rate is stillvery high.Further action is required to avoid unnecessary loss of lives.
Keywords: Road crash,Road injury,Road death,Road safety law effectiveness
Background
Road traffic crash isa growing public health threat,
being responsible for 1.2 million deaths and up to 50
million nonfatalinjuries globally.It is a big challenge
especially for low and middle income countries,90% of
the victims were found [1].Accidenttrends observed
in industrialized countries witnessed the rapid reduc-
tion over the last three to four decades,while a terrify-
ing incrementreported from a number ofdeveloping
countries including Ethiopia [2,3].The problem may
grow further in the coming decades;due to the rapid
rising ofvehicle ownership associated with their eco-
nomic growth [4].
Evidence from high income countries showed that im-
plementation of appropriately designed and well enforced
road safety policy contribute a lion share for their impres-
sive achievements ofthe declining trend in the number
and severity ofcrashes [5].According to the European
TransportSafety Councilestimation,if all existing road
safety laws in European Union are enforced up to 50% of
death and injuries could be averted [6].
Likewise in recentyears,many low income countries
are implementing improved road safety policy to deter
risky driving practices including:− exceeding the speed
limit, impaired driving by alcoholand drugs,phoning
and texting while driving,and not using seat belt [5,7].
Howeverthere islittle empiricalevidence asto their
effectiveness in reducing crashes,injuries and fatalities
[7].For example,Brazil,after implementing an improved
traffic code with stiff penalty and media coverage a 21%
and 25% reduction of injuries and fatalities,respectively,
was observed [8].A study conducted in Uganda follow-
ing,police enforcement using patrolcars equipped with
radar brings a 17% reduction of fatalities [9].In Rwanda
a 30% reduction in traffic death was observed following
an improved legislative change complimented with pub-
lic awareness campaign [10].
* Correspondence:tefabeg@yahoo.com
1Schoolof Public and EnvironmentalHealth,College of Medicine and Health
Sciences,Hawassa University,Hawassa,Ethiopia
Fulllist of author information is available at the end of the article
© 2014 Abegaz et al.;licensee BioMed CentralLtd.This is an Open Access article distributed under the terms of the Creative
Commons Attribution License (http://creativecommons.org/licenses/by/2.0),which permits unrestricted use,distribution,and
reproduction in any medium,provided the originalwork is properly credited.The Creative Commons Public Domain
Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,
unless otherwise stated.
Abegaz et al.BMC Public Health 2014,14:539
http://www.biomedcentral.com/1471-2458/14/539

This studywas conducted to measurethe levelof
effectiveness ofan improved road safety policy (Oromia
RegionalState Road Transport Regulation No;96/2007)
enforced as ofSeptember2007.The Oromia Regional
stateis one of the largeststatesin Ethiopia. This
improved road safety policy include the new road safety
laws (prohibition of cell phone conversation while behind
the wheel,driving without using a seat belt and not using
motorcycle helmet)and the amendmentof the existing
road safety laws (excessive speeding,impaired driving
with alcohol and Khat and unsafe loading) by introducing
higher penalty rate including suspension ofthe drivers’
licens.Seat balt wearing,healmet use and phoning while
driving were enforced by using a roadside random check
up on a regular bases;however speed and alcoholwere
not well enforced due to lack of radar and breath analyzer.
Methods
Study design
Interrupted time series design was utilized to evaluate
the effectivenessof an improved road safetypolicy
implemented by Oromia Regional State Transport Bureau.
Interrupted time series design is an alternative approach
used to evaluate the effects ofany intervention,when
randomized control trials are infeasible or identification
of a control group impractical[11].This design was
utilized by various researchers to assess the effectiveness
of health care intervention [11,12].
Study setting
The study was conducted on one of the main and busi-
est roads ofEthiopia,which extends south from the
capital Addis Ababa to Adama/Hawassa.This two-way
and two-lane road has an average width of8 meters
and covers a totaldistance of 264 Km.It is part of the
main route of the country’s import and export corridor
from the port of Djibouti and part of the Trans-African
Highway (an international road that stretched from Cairo
to Cape Town).Moreover,the road hasa significant
economic importance since many ofthe cash crops,
floriculture farms,recreational areas and tourist centers
are located across the stretches ofthe road.According
to the Ethiopian Road Authority report more than 20,
000 vehicles used the road daily.
Data sources
We reviewed traffic crash records,routinely collected by
the police officers from 16 district traffic offices for the
period 2002 through 2011. Additional data on daily vehicle
flow wasobtained from the Ethiopian Road Authority.
Only crashes happened on Addis Ababa- Adama/Hawassa
highway was considered for this study.A data retrieving
form was developed and used to record information from
the crash registration (CR)book.A total of 16 traffic
officers,who are assigned as an expert in documentation
and reporting ofcrash related cases were recruited from
each of the 16 traffic offices and provide training.Further-
more,two senior police officers and the principal investi-
gator were involved in the data collection process as a
supervisor.Relevant information on the type and severity
of the crash, type of vehicles and road users involved in the
crash and the time and place of the crash was retrieved.
Data management and quality assurance
Those crashes lacked some ofthe relevantinformation
needed were excluded.Among the total46 casesthat
excluded from the analysis,27 of them were reported
before the intervention and 19 ofthem reported after
the intervention.The main reason for the exclusion is
due to lack ofinformation on injury severity and num-
ber of victims involved.The collected data was double
entered by two differentdata clerk,using the EpiData
3.1 statisticalsoftware.Once the data entry completed,
we run the frequency and printout the outputof the
two datasets.Consistency was checked by comparing the
frequency and the difference was corrected accordingly
by using the original data retrieving form.
Statistical analysis
The revised road safety policy include the new road
safety laws (banning of cellphone conversation,unbelted
driving and not using motorcycle helmet) and the amend-
ment of the existing road safety laws (excessive speeding,
impaired driving with alcoholand Khat and unsafe
loading) which was implemented as of September 2007.
Prior to September2007,road safety enforcementin
Oromia RegionalState implemented by police officer
using less strict enforcement with low penalty.On the
other hand,the existing and the newly enacted road
safetylaws were implemented in acoordinated way
(traffic police and transport expert) using a stricter law
enforcement to the extent of drivers’licence suspension.
Seat belt wearing,helmet use and unsafe loading were
enforced by using a roadside random check up on a
regular basis;however,lack ofroad safety instruments
like;radar and breath analyzer hinder the implementa-
tion of speeding and alcohol intoxication.
In this study three different dependent variables were
considered in the statisticalanalysis:monthly rates of
non-injury crashes,fatalitiesand injuriesper 10,000
vehicles.The explanatory variables were intervention
dummy variable coded 0 before the intervention and
coded 1 after the intervention.A time trend was used
to control the confounding effectof the underlying
trend on the actual intervention coded as 1 at the starting
month ofthe first observation and continued to the last
observation.To estimate the trend change we introduced
a scaled interaction term (the number of months counted
Abegaz et al.BMC Public Health 2014,14:539 Page 2 of 6
http://www.biomedcentral.com/1471-2458/14/539
effectiveness ofan improved road safety policy (Oromia
RegionalState Road Transport Regulation No;96/2007)
enforced as ofSeptember2007.The Oromia Regional
stateis one of the largeststatesin Ethiopia. This
improved road safety policy include the new road safety
laws (prohibition of cell phone conversation while behind
the wheel,driving without using a seat belt and not using
motorcycle helmet)and the amendmentof the existing
road safety laws (excessive speeding,impaired driving
with alcohol and Khat and unsafe loading) by introducing
higher penalty rate including suspension ofthe drivers’
licens.Seat balt wearing,healmet use and phoning while
driving were enforced by using a roadside random check
up on a regular bases;however speed and alcoholwere
not well enforced due to lack of radar and breath analyzer.
Methods
Study design
Interrupted time series design was utilized to evaluate
the effectivenessof an improved road safetypolicy
implemented by Oromia Regional State Transport Bureau.
Interrupted time series design is an alternative approach
used to evaluate the effects ofany intervention,when
randomized control trials are infeasible or identification
of a control group impractical[11].This design was
utilized by various researchers to assess the effectiveness
of health care intervention [11,12].
Study setting
The study was conducted on one of the main and busi-
est roads ofEthiopia,which extends south from the
capital Addis Ababa to Adama/Hawassa.This two-way
and two-lane road has an average width of8 meters
and covers a totaldistance of 264 Km.It is part of the
main route of the country’s import and export corridor
from the port of Djibouti and part of the Trans-African
Highway (an international road that stretched from Cairo
to Cape Town).Moreover,the road hasa significant
economic importance since many ofthe cash crops,
floriculture farms,recreational areas and tourist centers
are located across the stretches ofthe road.According
to the Ethiopian Road Authority report more than 20,
000 vehicles used the road daily.
Data sources
We reviewed traffic crash records,routinely collected by
the police officers from 16 district traffic offices for the
period 2002 through 2011. Additional data on daily vehicle
flow wasobtained from the Ethiopian Road Authority.
Only crashes happened on Addis Ababa- Adama/Hawassa
highway was considered for this study.A data retrieving
form was developed and used to record information from
the crash registration (CR)book.A total of 16 traffic
officers,who are assigned as an expert in documentation
and reporting ofcrash related cases were recruited from
each of the 16 traffic offices and provide training.Further-
more,two senior police officers and the principal investi-
gator were involved in the data collection process as a
supervisor.Relevant information on the type and severity
of the crash, type of vehicles and road users involved in the
crash and the time and place of the crash was retrieved.
Data management and quality assurance
Those crashes lacked some ofthe relevantinformation
needed were excluded.Among the total46 casesthat
excluded from the analysis,27 of them were reported
before the intervention and 19 ofthem reported after
the intervention.The main reason for the exclusion is
due to lack ofinformation on injury severity and num-
ber of victims involved.The collected data was double
entered by two differentdata clerk,using the EpiData
3.1 statisticalsoftware.Once the data entry completed,
we run the frequency and printout the outputof the
two datasets.Consistency was checked by comparing the
frequency and the difference was corrected accordingly
by using the original data retrieving form.
Statistical analysis
The revised road safety policy include the new road
safety laws (banning of cellphone conversation,unbelted
driving and not using motorcycle helmet) and the amend-
ment of the existing road safety laws (excessive speeding,
impaired driving with alcoholand Khat and unsafe
loading) which was implemented as of September 2007.
Prior to September2007,road safety enforcementin
Oromia RegionalState implemented by police officer
using less strict enforcement with low penalty.On the
other hand,the existing and the newly enacted road
safetylaws were implemented in acoordinated way
(traffic police and transport expert) using a stricter law
enforcement to the extent of drivers’licence suspension.
Seat belt wearing,helmet use and unsafe loading were
enforced by using a roadside random check up on a
regular basis;however,lack ofroad safety instruments
like;radar and breath analyzer hinder the implementa-
tion of speeding and alcohol intoxication.
In this study three different dependent variables were
considered in the statisticalanalysis:monthly rates of
non-injury crashes,fatalitiesand injuriesper 10,000
vehicles.The explanatory variables were intervention
dummy variable coded 0 before the intervention and
coded 1 after the intervention.A time trend was used
to control the confounding effectof the underlying
trend on the actual intervention coded as 1 at the starting
month ofthe first observation and continued to the last
observation.To estimate the trend change we introduced
a scaled interaction term (the number of months counted
Abegaz et al.BMC Public Health 2014,14:539 Page 2 of 6
http://www.biomedcentral.com/1471-2458/14/539
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
starting from the new policy intervention) time coded 1 at
the start month and continued through the last month.
The monthly rate ofnon-injury crashes,fatalities and
injuries were plotted over time and visually inspected to
assess the trends or the non-stationarity of the data.We
also used autocorrelation function (ACF)and partial
autocorrelation function (PACF) and Dickey-Fuller unit
root test to determine the nature of the trend.Both tests
showed the trend wasdeterministic,hence segmented
regression model(fit a least-squares regression line to
each segmentof the explanatory variables)was the
recommended approach formodel building process
[13].Autocorrelation wasassessed by using Durbin-
Watson statistics (for serialcorrelation)and Breusch
and Godfrey (forhigherorder correlation).Durbin-
Watson statistics showed serialcorrelation in one of
the dependentvariable (non-injury crashes).So fitting a
least-squares regression line provide a biased estimate and
hence adjustmentwas done by applying feasible GLS
estimator (generalized least squares),using Prais-Winston
method [14].
Model diagnosticswere carried outusing variance
inflation factors and visual observation of the line graph
to investigate the existence ofcollinearity and influen-
tial or outliers.Model fitnesswas checked by using
change in percentile rank (CPR) statistics.Hence,only
the trend change shows the statisticalsignificant effect.
Applying - R2 as modelfitness was notapplicable be-
cause itindependently predicted by levelchange only
(immediate effect after intervention) which is insignifi-
cant in all of the three models in our case.
This intervention study was performed using STATA
12 software package.Prais-Winston regression approach
(model 1) was fitted for non-injury crashes and segmented
regression using an ordinary least square approach (model
2 & 3) for both fatalitiesand injuries.Both models
included 120 monthly observations.The effectiveness of
the improved road safety intervention wasassessed by
using the formula indicated by equation (1) reference [11].
yt ¼ β0 þ β1 time þ β2 inetervention
þ β3 postslope þ εt ð1Þ
Where yt is the outcome variable attime,time is a
continuous variable indicating time (in months) at time
t from the start (t = 0 month) until the end (t = 120 months)
of the observation period (January 2002 to December 2011),
intervention is an indicatorvariable for time toccurring
before (t = 0 month) or after (t = 1 month) (September
2007)the change to an improved road safety policy;
post-slope is coded 0 up to the lastpoint before the
intervention phase (January 2002 to August 2007) and
(time 1–52) after the intervention of an improved road
safety (September 2007 to December 2011) and et is the
error term attime t. Similarly β0 value attime zero,
β1 change over time before the intervention was imple-
mented,β2 is change in the outcome measure from the
last time point before the intervention to the first time
point afterthe intervention and β3 difference in the
slope of the time period before the intervention and the
slope of the time period after the intervention.
In the absence ofthe improved road safety interven-
tion the modelpredictthe non-injury crashes,injuries
and deaths given by equation (2) reference [11].
ytNo ¼ β0 þ β1 time ð2Þ
Results
The result showed that,a totalof 4,053 crashes occurred
on the Addis Ababa - Adama/Hawassa main road during
the study period. Almost half, 46.4% (1,880) were property
damage only crashes;29.4% (1,193) fatalcrashes and the
rest 24.2% (980) injury crashes.From 1,193 fatalcrashes
1,392 people were dying,on average 1.2 deaths per fatal
crashes.Of these deaths,more than half 57.5% (800) were
pedestrian,32% (445) vehicle occupants and 10.5% (147)
drivers.During the 980 injury crashes 1,749 people were
injured,on average,1.8 injuries per crash,over half,55.2%
(965)were vehicleoccupants,followed bypedestrian
35.1% (614) and the rest 9.7% (170) were drivers (Table 1)
Regarding the type ofcrashesreported in the study
area,40.6% (1,645)were crashing with othervehicles,
followed by pedestrian collision 32.9% (1,335),rollover
crashes accounted 16% (651) and the rest 6% (238),4.5%
(184) crash with fixed objectand others including
animalvehicle crash respectively.Day time collision
accounted 69% (2,795) of total crashes (Table 1).
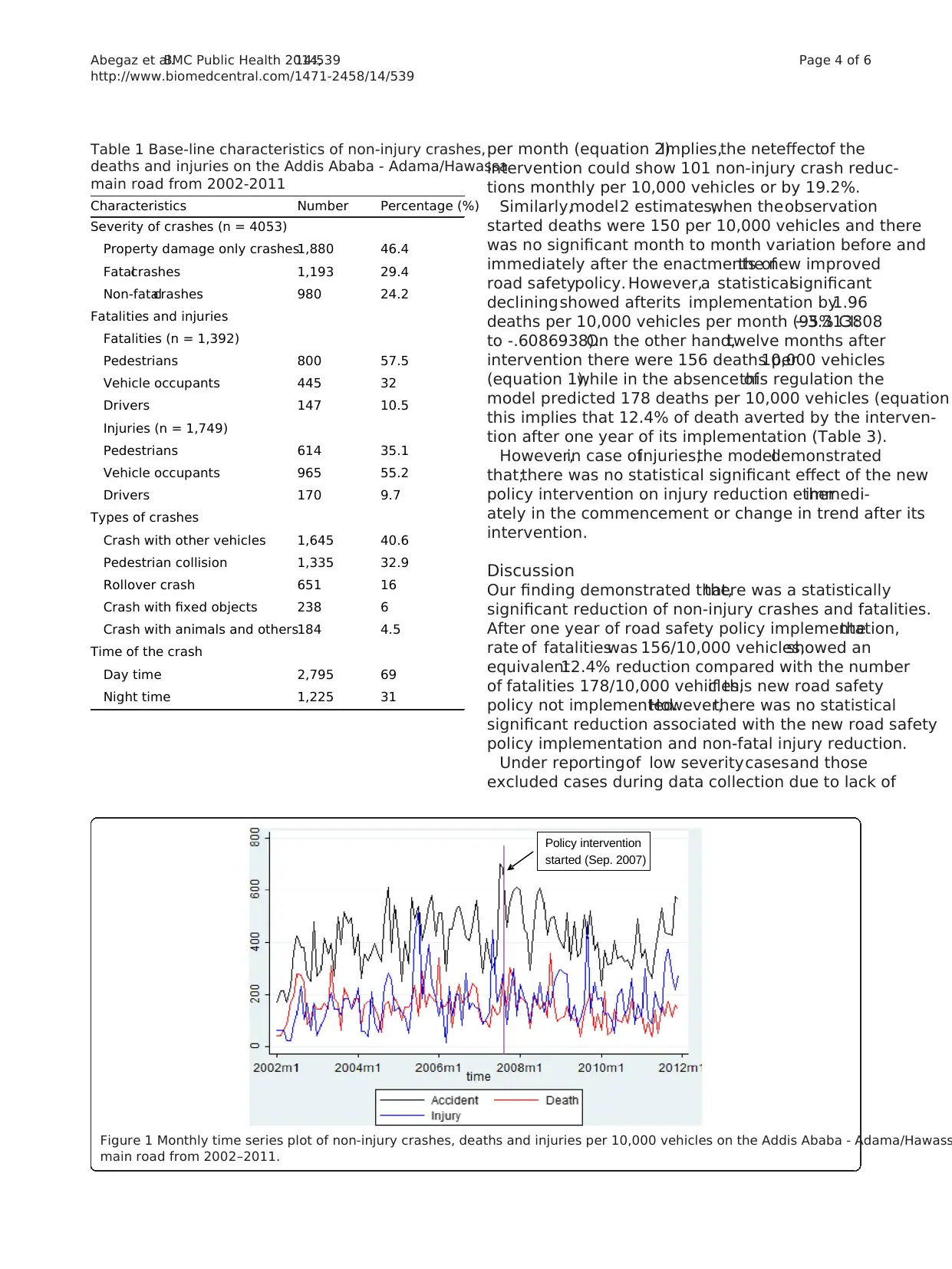
Figure 1 indicatesthe monthly time seriestrend of
non-injury crashes,deaths and injuries before and after
the intervention.The plot shows no observed seasonality
and time trend before intervention.The monthly rates
of non-injury crashes,deathsand injuriesper 10,000
vehiclesbeforeand after the implementation ofan
improved road safety policy were illustrated in Table 2.
Table 3 summarizesthe effectof the new improved
road safety in non-injury crashes,injuriesand deaths.
According to a model1 estimate,there were 295 non-
injury crashes per 10,000 vehicles atthe beginning of
observation.Before and afterintervention,the trend
showed statically significant variation;increased by 3.2
(95% CI: 1.57 to 4.92)before and decreased by 5.1
(95% CI:−8.143365 to −2.04914) after intervention per
10,000 vehicles per month respectively.The estimated
coefficients of the Model 1 showed that,after one year of
intervention,we observed 451 crashes/10,000 vehicles
(equation 1),however;in the absence of this intervention
the model predicted an average of 558 per 10,000 vehicles
Abegaz et al.BMC Public Health 2014,14:539 Page 3 of 6
http://www.biomedcentral.com/1471-2458/14/539
the start month and continued through the last month.
The monthly rate ofnon-injury crashes,fatalities and
injuries were plotted over time and visually inspected to
assess the trends or the non-stationarity of the data.We
also used autocorrelation function (ACF)and partial
autocorrelation function (PACF) and Dickey-Fuller unit
root test to determine the nature of the trend.Both tests
showed the trend wasdeterministic,hence segmented
regression model(fit a least-squares regression line to
each segmentof the explanatory variables)was the
recommended approach formodel building process
[13].Autocorrelation wasassessed by using Durbin-
Watson statistics (for serialcorrelation)and Breusch
and Godfrey (forhigherorder correlation).Durbin-
Watson statistics showed serialcorrelation in one of
the dependentvariable (non-injury crashes).So fitting a
least-squares regression line provide a biased estimate and
hence adjustmentwas done by applying feasible GLS
estimator (generalized least squares),using Prais-Winston
method [14].
Model diagnosticswere carried outusing variance
inflation factors and visual observation of the line graph
to investigate the existence ofcollinearity and influen-
tial or outliers.Model fitnesswas checked by using
change in percentile rank (CPR) statistics.Hence,only
the trend change shows the statisticalsignificant effect.
Applying - R2 as modelfitness was notapplicable be-
cause itindependently predicted by levelchange only
(immediate effect after intervention) which is insignifi-
cant in all of the three models in our case.
This intervention study was performed using STATA
12 software package.Prais-Winston regression approach
(model 1) was fitted for non-injury crashes and segmented
regression using an ordinary least square approach (model
2 & 3) for both fatalitiesand injuries.Both models
included 120 monthly observations.The effectiveness of
the improved road safety intervention wasassessed by
using the formula indicated by equation (1) reference [11].
yt ¼ β0 þ β1 time þ β2 inetervention
þ β3 postslope þ εt ð1Þ
Where yt is the outcome variable attime,time is a
continuous variable indicating time (in months) at time
t from the start (t = 0 month) until the end (t = 120 months)
of the observation period (January 2002 to December 2011),
intervention is an indicatorvariable for time toccurring
before (t = 0 month) or after (t = 1 month) (September
2007)the change to an improved road safety policy;
post-slope is coded 0 up to the lastpoint before the
intervention phase (January 2002 to August 2007) and
(time 1–52) after the intervention of an improved road
safety (September 2007 to December 2011) and et is the
error term attime t. Similarly β0 value attime zero,
β1 change over time before the intervention was imple-
mented,β2 is change in the outcome measure from the
last time point before the intervention to the first time
point afterthe intervention and β3 difference in the
slope of the time period before the intervention and the
slope of the time period after the intervention.
In the absence ofthe improved road safety interven-
tion the modelpredictthe non-injury crashes,injuries
and deaths given by equation (2) reference [11].
ytNo ¼ β0 þ β1 time ð2Þ
Results
The result showed that,a totalof 4,053 crashes occurred
on the Addis Ababa - Adama/Hawassa main road during
the study period. Almost half, 46.4% (1,880) were property
damage only crashes;29.4% (1,193) fatalcrashes and the
rest 24.2% (980) injury crashes.From 1,193 fatalcrashes
1,392 people were dying,on average 1.2 deaths per fatal
crashes.Of these deaths,more than half 57.5% (800) were
pedestrian,32% (445) vehicle occupants and 10.5% (147)
drivers.During the 980 injury crashes 1,749 people were
injured,on average,1.8 injuries per crash,over half,55.2%
(965)were vehicleoccupants,followed bypedestrian
35.1% (614) and the rest 9.7% (170) were drivers (Table 1)
Regarding the type ofcrashesreported in the study
area,40.6% (1,645)were crashing with othervehicles,
followed by pedestrian collision 32.9% (1,335),rollover
crashes accounted 16% (651) and the rest 6% (238),4.5%
(184) crash with fixed objectand others including
animalvehicle crash respectively.Day time collision
accounted 69% (2,795) of total crashes (Table 1).
Figure 1 indicatesthe monthly time seriestrend of
non-injury crashes,deaths and injuries before and after
the intervention.The plot shows no observed seasonality
and time trend before intervention.The monthly rates
of non-injury crashes,deathsand injuriesper 10,000
vehiclesbeforeand after the implementation ofan
improved road safety policy were illustrated in Table 2.
Table 3 summarizesthe effectof the new improved
road safety in non-injury crashes,injuriesand deaths.
According to a model1 estimate,there were 295 non-
injury crashes per 10,000 vehicles atthe beginning of
observation.Before and afterintervention,the trend
showed statically significant variation;increased by 3.2
(95% CI: 1.57 to 4.92)before and decreased by 5.1
(95% CI:−8.143365 to −2.04914) after intervention per
10,000 vehicles per month respectively.The estimated
coefficients of the Model 1 showed that,after one year of
intervention,we observed 451 crashes/10,000 vehicles
(equation 1),however;in the absence of this intervention
the model predicted an average of 558 per 10,000 vehicles
Abegaz et al.BMC Public Health 2014,14:539 Page 3 of 6
http://www.biomedcentral.com/1471-2458/14/539
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
per month (equation 2).Implies,the neteffectof the
intervention could show 101 non-injury crash reduc-
tions monthly per 10,000 vehicles or by 19.2%.
Similarly,model2 estimates,when theobservation
started deaths were 150 per 10,000 vehicles and there
was no significant month to month variation before and
immediately after the enactments ofthe new improved
road safetypolicy. However,a statisticalsignificant
decliningshowed afterits implementation by1.96
deaths per 10,000 vehicles per month (95% CI:−3.313808
to -.6086938).On the other hand,twelve months after
intervention there were 156 deaths per10,000 vehicles
(equation 1),while in the absence ofthis regulation the
model predicted 178 deaths per 10,000 vehicles (equation
this implies that 12.4% of death averted by the interven-
tion after one year of its implementation (Table 3).
However,in case ofinjuries,the modeldemonstrated
that;there was no statistical significant effect of the new
policy intervention on injury reduction etherimmedi-
ately in the commencement or change in trend after its
intervention.
Discussion
Our finding demonstrated that,there was a statistically
significant reduction of non-injury crashes and fatalities.
After one year of road safety policy implementation,the
rate of fatalitieswas 156/10,000 vehicles,showed an
equivalent12.4% reduction compared with the number
of fatalities 178/10,000 vehicles,if this new road safety
policy not implemented.However,there was no statistical
significant reduction associated with the new road safety
policy implementation and non-fatal injury reduction.
Under reportingof low severitycasesand those
excluded cases during data collection due to lack of
Table 1 Base-line characteristics of non-injury crashes,
deaths and injuries on the Addis Ababa - Adama/Hawassa
main road from 2002-2011
Characteristics Number Percentage (%)
Severity of crashes (n = 4053)
Property damage only crashes1,880 46.4
Fatalcrashes 1,193 29.4
Non-fatalcrashes 980 24.2
Fatalities and injuries
Fatalities (n = 1,392)
Pedestrians 800 57.5
Vehicle occupants 445 32
Drivers 147 10.5
Injuries (n = 1,749)
Pedestrians 614 35.1
Vehicle occupants 965 55.2
Drivers 170 9.7
Types of crashes
Crash with other vehicles 1,645 40.6
Pedestrian collision 1,335 32.9
Rollover crash 651 16
Crash with fixed objects 238 6
Crash with animals and others184 4.5
Time of the crash
Day time 2,795 69
Night time 1,225 31
Policy intervention
started (Sep. 2007)
Figure 1 Monthly time series plot of non-injury crashes, deaths and injuries per 10,000 vehicles on the Addis Ababa - Adama/Hawass
main road from 2002–2011.
Abegaz et al.BMC Public Health 2014,14:539 Page 4 of 6
http://www.biomedcentral.com/1471-2458/14/539
intervention could show 101 non-injury crash reduc-
tions monthly per 10,000 vehicles or by 19.2%.
Similarly,model2 estimates,when theobservation
started deaths were 150 per 10,000 vehicles and there
was no significant month to month variation before and
immediately after the enactments ofthe new improved
road safetypolicy. However,a statisticalsignificant
decliningshowed afterits implementation by1.96
deaths per 10,000 vehicles per month (95% CI:−3.313808
to -.6086938).On the other hand,twelve months after
intervention there were 156 deaths per10,000 vehicles
(equation 1),while in the absence ofthis regulation the
model predicted 178 deaths per 10,000 vehicles (equation
this implies that 12.4% of death averted by the interven-
tion after one year of its implementation (Table 3).
However,in case ofinjuries,the modeldemonstrated
that;there was no statistical significant effect of the new
policy intervention on injury reduction etherimmedi-
ately in the commencement or change in trend after its
intervention.
Discussion
Our finding demonstrated that,there was a statistically
significant reduction of non-injury crashes and fatalities.
After one year of road safety policy implementation,the
rate of fatalitieswas 156/10,000 vehicles,showed an
equivalent12.4% reduction compared with the number
of fatalities 178/10,000 vehicles,if this new road safety
policy not implemented.However,there was no statistical
significant reduction associated with the new road safety
policy implementation and non-fatal injury reduction.
Under reportingof low severitycasesand those
excluded cases during data collection due to lack of
Table 1 Base-line characteristics of non-injury crashes,
deaths and injuries on the Addis Ababa - Adama/Hawassa
main road from 2002-2011
Characteristics Number Percentage (%)
Severity of crashes (n = 4053)
Property damage only crashes1,880 46.4
Fatalcrashes 1,193 29.4
Non-fatalcrashes 980 24.2
Fatalities and injuries
Fatalities (n = 1,392)
Pedestrians 800 57.5
Vehicle occupants 445 32
Drivers 147 10.5
Injuries (n = 1,749)
Pedestrians 614 35.1
Vehicle occupants 965 55.2
Drivers 170 9.7
Types of crashes
Crash with other vehicles 1,645 40.6
Pedestrian collision 1,335 32.9
Rollover crash 651 16
Crash with fixed objects 238 6
Crash with animals and others184 4.5
Time of the crash
Day time 2,795 69
Night time 1,225 31
Policy intervention
started (Sep. 2007)
Figure 1 Monthly time series plot of non-injury crashes, deaths and injuries per 10,000 vehicles on the Addis Ababa - Adama/Hawass
main road from 2002–2011.
Abegaz et al.BMC Public Health 2014,14:539 Page 4 of 6
http://www.biomedcentral.com/1471-2458/14/539
necessary information,might have an effect on the overall
trend.But we are not expecting similar consequences on
the effectiveness ofthe new improved road safety policy,
since the reporting system is similar before and after the
intervention.In this study,we could notalso take into
accountthe potentialimpactof otherroad safety ini-
tiatives,like mass media intervention atthe federaland
regionallevel.Hence,the mass media intervention was
started before the implementation ofthe new improved
road safety policy.So we are notexpecting assuch a
significant effect on the result.Moreover,we have consid-
ered longer pre and post-intervention period 68 months
and 52 months respectively.This larger number ofdata
points prior to the intervention helps to obtain a stable
estimate of the underlying trend [12,15]. With this, we can
avoid the shortcoming related to regression towards the
mean and over fitting.
Abnormally high fatality rate,156 per 10,000 vehicles
was observed in this study compared with the national
average,95 death per 10,000 vehicles as reported by UN
Economic Commission for Africa 2007–2008 [16].This
might be due to the high traffic volume of the road seg-
ment,as it is one of the countries import export corridor
from the port Djibouti.The diverse traffic mix,including
animaldrawn carts frequently shares the road with high
speed vehicles.
The effectivenessof policy intervention achieved by
low and high income countries couldn’t be comparable
for a number of reasons;in the first place the difference
of road user categories frequently affected.While vehicle
occupantsare the mostcommon fatally injured road
users in high income countries,more than half 45–75% of
all road fatalities were pedestrian in low income countries
[17].The other reason might be the levelof enforcement
by police officers,the availability of to date logistic supply,
the safety equipment inside the vehicles and the levelof
police officers’ commitment.
Nineteen percentof non-injurycrashesand twelve
percent ofdeaths averted by the implementation ofthe
new road safety policy in the study area might be due to
the integration of police and transport sector at different
administrative level and the establishment of a road safety
committee in some parts of the region. However, 11 .2% of
fatality reduction obtained in this study area after one year
of intervention,still lower than the achievements of other
similarlow income countries,for example 30% fatality
reduction in Burundiand 17% in Uganda [9,10].The
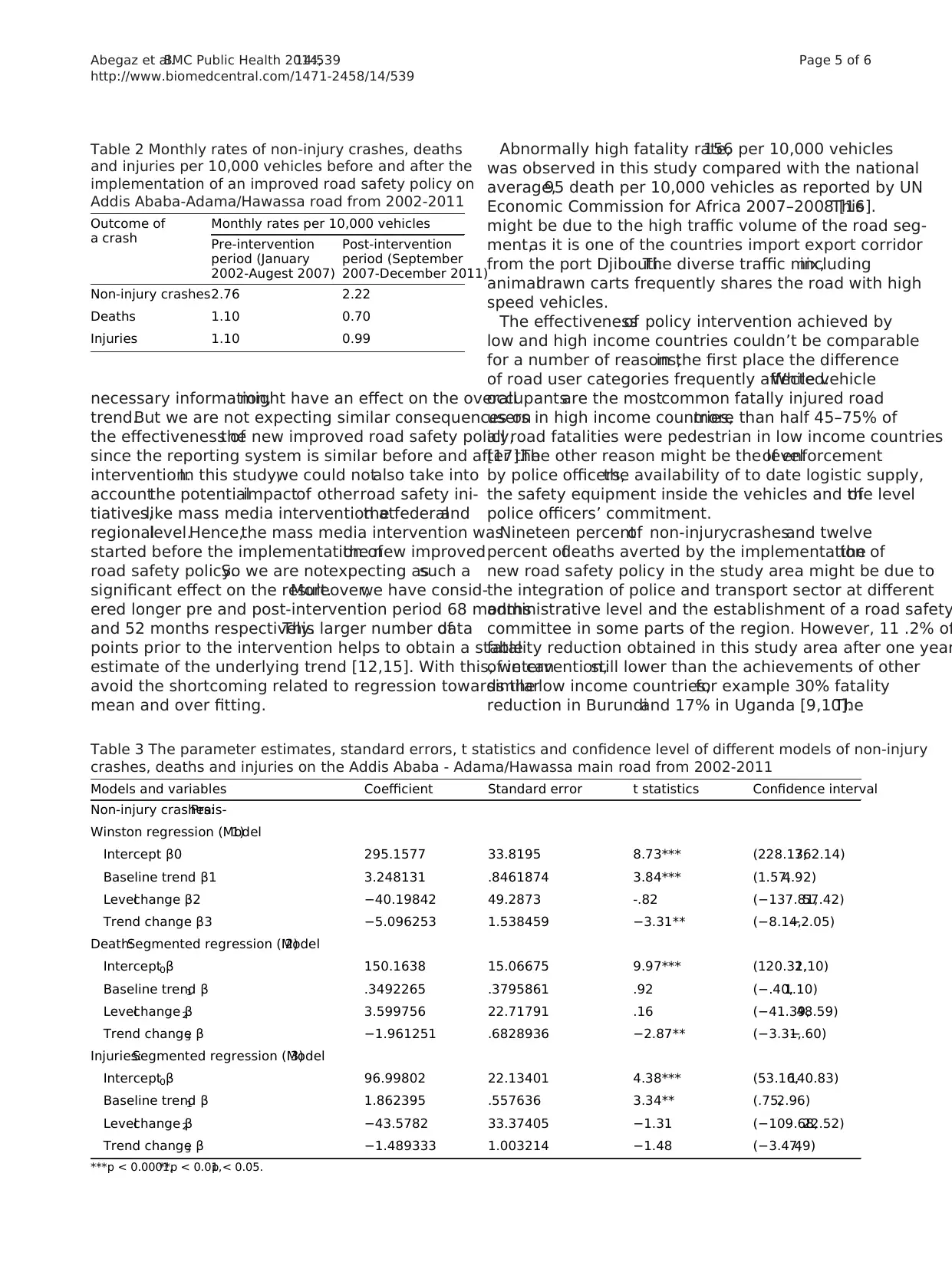
Table 2 Monthly rates of non-injury crashes, deaths
and injuries per 10,000 vehicles before and after the
implementation of an improved road safety policy on
Addis Ababa-Adama/Hawassa road from 2002-2011
Outcome of
a crash
Monthly rates per 10,000 vehicles
Pre-intervention
period (January
2002-Augest 2007)
Post-intervention
period (September
2007-December 2011)
Non-injury crashes2.76 2.22
Deaths 1.10 0.70
Injuries 1.10 0.99
Table 3 The parameter estimates, standard errors, t statistics and confidence level of different models of non-injury
crashes, deaths and injuries on the Addis Ababa - Adama/Hawassa main road from 2002-2011
Models and variables Coefficient Standard error t statistics Confidence interval
Non-injury crashes:Prais-
Winston regression (Model1)
Intercept β0 295.1577 33.8195 8.73*** (228.17,362.14)
Baseline trend β1 3.248131 .8461874 3.84*** (1.57,4.92)
Levelchange β2 −40.19842 49.2873 -.82 (−137.81,57.42)
Trend change β3 −5.096253 1.538459 −3.31** (−8.14,−2.05)
Death:Segmented regression (Model2)
Intercept β0 150.1638 15.06675 9.97*** (120.32,1.10)
Baseline trend β1 .3492265 .3795861 .92 (−.40,1.10)
Levelchange β2 3.599756 22.71791 .16 (−41.39,48.59)
Trend change β3 −1.961251 .6828936 −2.87** (−3.31,−.60)
Injuries:Segmented regression (Model3)
Intercept β0 96.99802 22.13401 4.38*** (53.16,140.83)
Baseline trend β1 1.862395 .557636 3.34** (.75,2.96)
Levelchange β2 −43.5782 33.37405 −1.31 (−109.68,22.52)
Trend change β3 −1.489333 1.003214 −1.48 (−3.47,.49)
***p < 0.0001,**p < 0.01,p < 0.05.
Abegaz et al.BMC Public Health 2014,14:539 Page 5 of 6
http://www.biomedcentral.com/1471-2458/14/539
trend.But we are not expecting similar consequences on
the effectiveness ofthe new improved road safety policy,
since the reporting system is similar before and after the
intervention.In this study,we could notalso take into
accountthe potentialimpactof otherroad safety ini-
tiatives,like mass media intervention atthe federaland
regionallevel.Hence,the mass media intervention was
started before the implementation ofthe new improved
road safety policy.So we are notexpecting assuch a
significant effect on the result.Moreover,we have consid-
ered longer pre and post-intervention period 68 months
and 52 months respectively.This larger number ofdata
points prior to the intervention helps to obtain a stable
estimate of the underlying trend [12,15]. With this, we can
avoid the shortcoming related to regression towards the
mean and over fitting.
Abnormally high fatality rate,156 per 10,000 vehicles
was observed in this study compared with the national
average,95 death per 10,000 vehicles as reported by UN
Economic Commission for Africa 2007–2008 [16].This
might be due to the high traffic volume of the road seg-
ment,as it is one of the countries import export corridor
from the port Djibouti.The diverse traffic mix,including
animaldrawn carts frequently shares the road with high
speed vehicles.
The effectivenessof policy intervention achieved by
low and high income countries couldn’t be comparable
for a number of reasons;in the first place the difference
of road user categories frequently affected.While vehicle
occupantsare the mostcommon fatally injured road
users in high income countries,more than half 45–75% of
all road fatalities were pedestrian in low income countries
[17].The other reason might be the levelof enforcement
by police officers,the availability of to date logistic supply,
the safety equipment inside the vehicles and the levelof
police officers’ commitment.
Nineteen percentof non-injurycrashesand twelve
percent ofdeaths averted by the implementation ofthe
new road safety policy in the study area might be due to
the integration of police and transport sector at different
administrative level and the establishment of a road safety
committee in some parts of the region. However, 11 .2% of
fatality reduction obtained in this study area after one year
of intervention,still lower than the achievements of other
similarlow income countries,for example 30% fatality
reduction in Burundiand 17% in Uganda [9,10].The
Table 2 Monthly rates of non-injury crashes, deaths
and injuries per 10,000 vehicles before and after the
implementation of an improved road safety policy on
Addis Ababa-Adama/Hawassa road from 2002-2011
Outcome of
a crash
Monthly rates per 10,000 vehicles
Pre-intervention
period (January
2002-Augest 2007)
Post-intervention
period (September
2007-December 2011)
Non-injury crashes2.76 2.22
Deaths 1.10 0.70
Injuries 1.10 0.99
Table 3 The parameter estimates, standard errors, t statistics and confidence level of different models of non-injury
crashes, deaths and injuries on the Addis Ababa - Adama/Hawassa main road from 2002-2011
Models and variables Coefficient Standard error t statistics Confidence interval
Non-injury crashes:Prais-
Winston regression (Model1)
Intercept β0 295.1577 33.8195 8.73*** (228.17,362.14)
Baseline trend β1 3.248131 .8461874 3.84*** (1.57,4.92)
Levelchange β2 −40.19842 49.2873 -.82 (−137.81,57.42)
Trend change β3 −5.096253 1.538459 −3.31** (−8.14,−2.05)
Death:Segmented regression (Model2)
Intercept β0 150.1638 15.06675 9.97*** (120.32,1.10)
Baseline trend β1 .3492265 .3795861 .92 (−.40,1.10)
Levelchange β2 3.599756 22.71791 .16 (−41.39,48.59)
Trend change β3 −1.961251 .6828936 −2.87** (−3.31,−.60)
Injuries:Segmented regression (Model3)
Intercept β0 96.99802 22.13401 4.38*** (53.16,140.83)
Baseline trend β1 1.862395 .557636 3.34** (.75,2.96)
Levelchange β2 −43.5782 33.37405 −1.31 (−109.68,22.52)
Trend change β3 −1.489333 1.003214 −1.48 (−3.47,.49)
***p < 0.0001,**p < 0.01,p < 0.05.
Abegaz et al.BMC Public Health 2014,14:539 Page 5 of 6
http://www.biomedcentral.com/1471-2458/14/539
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
smaller effect observed in this study might be explained
by,poor enforcement by traffic officers,especially related
to excessive speeding.The speed limit is not respected by
many ofthe drivers and even police officers not consid-
ered as a serious offense.Lack of speed control devices is
an impediment to enforcing the law (Personalcommuni-
cation with traffic officers).Lack of effective enforcement
for speed violators and absence ofspeed controldevices
was one ofthe main reason for low income countries’
poor achievementin the area ofroad safety [18].In
addition,there was weak enforcementon impaired
driver by alcoholand khatdue to the absence ofa
breath test and the lack ofstated legalalcohollimit in
the new road safety regulation.
Conclusion
This study has shown a statistically significant reduction
of non-injury crashes and fatalities after the implemen-
tation of the improved road safety regulation in the
regionalstate.However,the problem is stillgrave and
needsfurthereffortsto make our road safe.Crash,
injury and fatality reduction can be more promising if
it is complemented by public awareness campaign,inter-
sectoralcollaboration and furtherenforcementusing
appropriate control devices.
Competing interests
The authors declare that they have no competing interests.
Authors'contributions
TA is the principalinvestigator and contributed to the development of
research protocols,implementation of the study,and drafted the manuscript.
YB and AW contributed from protocoldevelopment through writing up and
assisted during data collection and commented on the draft manuscript.All
authors read and approved the finalmanuscript.
Acknowledgements
This study was sponsored and financed by Hawassa University and the WHO
country office.Specialthanks to Addis ContinentalInstitute of Public Health
for this research opportunity.The authors also would like to appreciate
management bodies and police officers involved in the data collection
process.
Author details
1Schoolof Public and EnvironmentalHealth,College of Medicine and Health
Sciences,Hawassa University,Hawassa,Ethiopia.2Addis ContinentalInstitute
of Public Health,Addis Ababa,Ethiopia.3Schoolof Public Health,College of
Health Sciences,Addis Ababa University,Addis Ababa,Ethiopia.4Ministry of
Transport,Addis Ababa,Ethiopia.
Received:9 September 2013 Accepted:23 May 2014
Published:31 May 2014
References
1. Peden M,Sleet D,Mohan D,Hyder AA,Jarawan E,Mathers C:World report
on road traffic injury prevention.Geneva:World Health Organization;2004.
2. Elvik R:The stability of long-term trends in the number of traffic fatalities
in a sample of highly motorised countries.Accid AnalPrev 2010,
42:245–260.
3. Mohan D:Road safety in less motorized environments:future concerns.
Int J Epidemiol2002,31:527–532.
4. Kopits E,Cropper M:Traffic fatalities and economic growth (Policy Research
Working Paper No 3035).Washington,DC:The World Bank;2003.
5. World Health Organization:Globalstatus report on road safety:time for
action.In Geneva:World Health Organization;2009.
6. European Transport Safety Council:Police enforcement strategies to
reduce traffic casualties in Europe.In Brussels:European Transport Safety
Council;1999.
7. Ameratunga S,Hijar M,Norton R:Road-traffic injuries:confronting
disparities to address a global-health problem.Lancet 2006,367:1533–1540.
8. Figueiredo LP,Rasslan S,Bruscagin V:Increases in fines and driver license
withdrawalhave effectively reduced immediate deaths from trauma on
Brazilian roads:first year report on the new traffic code.Injury 2001,
32:91–94.
9. BishaiD,Asiimwe B,Abbas S,Hyder A,Bazeyo W:Cost-effectiveness of
traffic enforcement:case study from Uganda.InjPrev 2008,14:223–227.
10. World Health Organization:Rwanda’s road-safety transformation.Bull
World Health Organ 2007,85:421.
11. Mylene L:How to do (or not to do) .. . Assessing the impact of a policy
change with routine longitudinaldata.Health Policy Plan 2011,1–8.
12. Ramsay CR,Matowe L,GrilliR,Grimshaw JM,Ruth E:Thomas Interrupted
time series designs in health technology assessment:lessons from two
systematic reviews of behavior change strategies.Int J TechnolAssess
Health Care 2003,19(4):613–623.
13. Wagner A,SoumeraiS,Zhang F,Ross-Degnan D:Segmented regression
analysis of interrupted time series studies in medication use research.
J Clin Pharm Ther 2002,27:299–309.
14. Judge G,Griffiths W,HillR,LutkepohlH,Lee T:The Theory and Practice of
Econometrics.New York:John Wiley & Sons;1985.
15. AnsariF,Gray K,NathwaniD,Phillips G,Ogston S,Ramsay C,Davey P:
Outcomes of an intervention to improve hospitalantibiotic prescribing:
interrupted time series with segmented regression analysis.J Antimicrob
Chemother 2003,52:842–848.
16. United Nation Economic Commission for Africa:Case study:road safety in
Ethiopia.In United Nation Economic Commission for Africa;2009.
17. NaciH,Chisholm D,Baker TD:Distribution of road traffic deaths by road
user group:a global comparison.InjPrev 2009,15:55–59.
18. Afukaar F:Speed controlin developing countries:issues,challenges and
opportunities in reducing road traffic injuries.InjControlSaf Promot 2003,
10:77–81.
doi:10.1186/1471-2458-14-539
Cite this article as:Abegaz et al.:Effectiveness of an improved road
safety policy in Ethiopia:an interrupted time series study.BMC Public
Health 2014 14:539.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Abegaz et al.BMC Public Health 2014,14:539 Page 6 of 6
http://www.biomedcentral.com/1471-2458/14/539
View publication statsView publication stats
by,poor enforcement by traffic officers,especially related
to excessive speeding.The speed limit is not respected by
many ofthe drivers and even police officers not consid-
ered as a serious offense.Lack of speed control devices is
an impediment to enforcing the law (Personalcommuni-
cation with traffic officers).Lack of effective enforcement
for speed violators and absence ofspeed controldevices
was one ofthe main reason for low income countries’
poor achievementin the area ofroad safety [18].In
addition,there was weak enforcementon impaired
driver by alcoholand khatdue to the absence ofa
breath test and the lack ofstated legalalcohollimit in
the new road safety regulation.
Conclusion
This study has shown a statistically significant reduction
of non-injury crashes and fatalities after the implemen-
tation of the improved road safety regulation in the
regionalstate.However,the problem is stillgrave and
needsfurthereffortsto make our road safe.Crash,
injury and fatality reduction can be more promising if
it is complemented by public awareness campaign,inter-
sectoralcollaboration and furtherenforcementusing
appropriate control devices.
Competing interests
The authors declare that they have no competing interests.
Authors'contributions
TA is the principalinvestigator and contributed to the development of
research protocols,implementation of the study,and drafted the manuscript.
YB and AW contributed from protocoldevelopment through writing up and
assisted during data collection and commented on the draft manuscript.All
authors read and approved the finalmanuscript.
Acknowledgements
This study was sponsored and financed by Hawassa University and the WHO
country office.Specialthanks to Addis ContinentalInstitute of Public Health
for this research opportunity.The authors also would like to appreciate
management bodies and police officers involved in the data collection
process.
Author details
1Schoolof Public and EnvironmentalHealth,College of Medicine and Health
Sciences,Hawassa University,Hawassa,Ethiopia.2Addis ContinentalInstitute
of Public Health,Addis Ababa,Ethiopia.3Schoolof Public Health,College of
Health Sciences,Addis Ababa University,Addis Ababa,Ethiopia.4Ministry of
Transport,Addis Ababa,Ethiopia.
Received:9 September 2013 Accepted:23 May 2014
Published:31 May 2014
References
1. Peden M,Sleet D,Mohan D,Hyder AA,Jarawan E,Mathers C:World report
on road traffic injury prevention.Geneva:World Health Organization;2004.
2. Elvik R:The stability of long-term trends in the number of traffic fatalities
in a sample of highly motorised countries.Accid AnalPrev 2010,
42:245–260.
3. Mohan D:Road safety in less motorized environments:future concerns.
Int J Epidemiol2002,31:527–532.
4. Kopits E,Cropper M:Traffic fatalities and economic growth (Policy Research
Working Paper No 3035).Washington,DC:The World Bank;2003.
5. World Health Organization:Globalstatus report on road safety:time for
action.In Geneva:World Health Organization;2009.
6. European Transport Safety Council:Police enforcement strategies to
reduce traffic casualties in Europe.In Brussels:European Transport Safety
Council;1999.
7. Ameratunga S,Hijar M,Norton R:Road-traffic injuries:confronting
disparities to address a global-health problem.Lancet 2006,367:1533–1540.
8. Figueiredo LP,Rasslan S,Bruscagin V:Increases in fines and driver license
withdrawalhave effectively reduced immediate deaths from trauma on
Brazilian roads:first year report on the new traffic code.Injury 2001,
32:91–94.
9. BishaiD,Asiimwe B,Abbas S,Hyder A,Bazeyo W:Cost-effectiveness of
traffic enforcement:case study from Uganda.InjPrev 2008,14:223–227.
10. World Health Organization:Rwanda’s road-safety transformation.Bull
World Health Organ 2007,85:421.
11. Mylene L:How to do (or not to do) .. . Assessing the impact of a policy
change with routine longitudinaldata.Health Policy Plan 2011,1–8.
12. Ramsay CR,Matowe L,GrilliR,Grimshaw JM,Ruth E:Thomas Interrupted
time series designs in health technology assessment:lessons from two
systematic reviews of behavior change strategies.Int J TechnolAssess
Health Care 2003,19(4):613–623.
13. Wagner A,SoumeraiS,Zhang F,Ross-Degnan D:Segmented regression
analysis of interrupted time series studies in medication use research.
J Clin Pharm Ther 2002,27:299–309.
14. Judge G,Griffiths W,HillR,LutkepohlH,Lee T:The Theory and Practice of
Econometrics.New York:John Wiley & Sons;1985.
15. AnsariF,Gray K,NathwaniD,Phillips G,Ogston S,Ramsay C,Davey P:
Outcomes of an intervention to improve hospitalantibiotic prescribing:
interrupted time series with segmented regression analysis.J Antimicrob
Chemother 2003,52:842–848.
16. United Nation Economic Commission for Africa:Case study:road safety in
Ethiopia.In United Nation Economic Commission for Africa;2009.
17. NaciH,Chisholm D,Baker TD:Distribution of road traffic deaths by road
user group:a global comparison.InjPrev 2009,15:55–59.
18. Afukaar F:Speed controlin developing countries:issues,challenges and
opportunities in reducing road traffic injuries.InjControlSaf Promot 2003,
10:77–81.
doi:10.1186/1471-2458-14-539
Cite this article as:Abegaz et al.:Effectiveness of an improved road
safety policy in Ethiopia:an interrupted time series study.BMC Public
Health 2014 14:539.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Abegaz et al.BMC Public Health 2014,14:539 Page 6 of 6
http://www.biomedcentral.com/1471-2458/14/539
View publication statsView publication stats
1 out of 7
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.