Economic Evaluation of BMI Screening Program in Schools: A Case Study
VerifiedAdded on 2023/06/11
|13
|3134
|150
Report
AI Summary
This report provides a comprehensive economic evaluation of a school-based Body Mass Index (BMI) screening program designed to identify and address obesity among students. It details the costs associated with the program, including material, training, communication, transport, and monitoring expenses, and compares them to the potential benefits, such as reduced prevalence of overweight and obesity, improved student health outcomes, and long-term cost savings. The report also discusses the intervention timeframe, analysis timeframe, and expected outcomes, emphasizing the importance of parental involvement and the integration of various intervention methods. Furthermore, the report highlights the need for continuous monitoring and evaluation to adapt the program for maximum effectiveness and cost-efficiency, while considering factors like student age, intervention intensity, and potential side effects. The analysis draws upon existing literature to support its findings and offers recommendations for optimizing the program's implementation and achieving its stated objectives. Desklib provides similar solved assignments and past papers for students.

Running head: HEALTH ECONOMICS 1
Health Economics
Name
Institution
Health Economics
Name
Institution
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 2
Cost of the Study
The study involves student screening for school programme. The screening programme is
supposed to focus on helping obese students. These are because the situation has caused to many
people especially young people from the age of 6 years and to the society. The screening process
is supposed to be positive according to the effectiveness of the type of therapy chosen. In this
case, the group has decided to use the BMI method. The screening is useful since a recent study
has shown that, obese individuals are likely to be infected with very chronic illnesses. These
chronic illnesses include; hypertension, diabetes, asthma, Tb, and headlice. For school going
children, such infections can be severe for them. The mass screening project has proved helpful
to many schools. Therefore it can be the best method of dealing with obese children in school.
Other health problems can be developed from obesity. Thus the screening process will be very
significant.
The process will also involve public health authorities that will give the professional help
in conducting the actual screening. The occupational health programme is supposed to determine
the health efficiency and procedure effectiveness. They are supposed to determine the
remediation ability to each of the students. The group will also determine the positive effect the
screening program will have for each student. The public health monitors will also determine the
level of information confidentiality that will be done during the screening program. The result of
the BMI program has to reach the parents of the students of the school as a way of implementing
the change of program for different children.
The school authority will help in providing choices for dietary interventions that can be
used for students that will be found suffering from obese conditions. The school authority is also
involved in defining a scope that will not interfere with the school routine and culture. The utility
Cost of the Study
The study involves student screening for school programme. The screening programme is
supposed to focus on helping obese students. These are because the situation has caused to many
people especially young people from the age of 6 years and to the society. The screening process
is supposed to be positive according to the effectiveness of the type of therapy chosen. In this
case, the group has decided to use the BMI method. The screening is useful since a recent study
has shown that, obese individuals are likely to be infected with very chronic illnesses. These
chronic illnesses include; hypertension, diabetes, asthma, Tb, and headlice. For school going
children, such infections can be severe for them. The mass screening project has proved helpful
to many schools. Therefore it can be the best method of dealing with obese children in school.
Other health problems can be developed from obesity. Thus the screening process will be very
significant.
The process will also involve public health authorities that will give the professional help
in conducting the actual screening. The occupational health programme is supposed to determine
the health efficiency and procedure effectiveness. They are supposed to determine the
remediation ability to each of the students. The group will also determine the positive effect the
screening program will have for each student. The public health monitors will also determine the
level of information confidentiality that will be done during the screening program. The result of
the BMI program has to reach the parents of the students of the school as a way of implementing
the change of program for different children.
The school authority will help in providing choices for dietary interventions that can be
used for students that will be found suffering from obese conditions. The school authority is also
involved in defining a scope that will not interfere with the school routine and culture. The utility
HEALTH ECONOMICS 3
of school items can also be monitored by the school authority. The inclusivity of staff members
that will provide an environment that is friendly and cool for the screening process to take place.
The implementation of this program is dependent on the mandate provided by the school
mandate program. The school mandate program under the children and the maternal program
focuses on various ways to help, the children who at risk of getting obese due dietary reasons.
The programme, therefore, focuses on ways that help detect and monitor childhood overweight.
The guidelines that will be used during the program are based on the Child Health Branch of the
countries department of Health and Human service. The screening although focuses on Obese
condition, will also detect other conditions that might be related to obesity. The group is hoping
to achieve the health goals through involving the parents. The parents will be involved in the
BMI health program. The BMI report will be submitted to parents during intervals. The parents
being important stakeholder might want to opt out their children out of the program after
sometimes.
Intervention time frame
The staff members of the group receive prior information about children in school for all
the students supposed to undergo screening. There should be a proper parental agreement and
consent within the first three months before the actual implementation since they form a more
significant part of the parental consciousness program. The parental consent is therefore done
before the measuring and weighing of the children. The school provides an environment that is
private. The school hall would probably be the best place. This is to help keep dignity, cultural
need, and confidentiality of the individual undertaking the test during those designated times for
the test.
of school items can also be monitored by the school authority. The inclusivity of staff members
that will provide an environment that is friendly and cool for the screening process to take place.
The implementation of this program is dependent on the mandate provided by the school
mandate program. The school mandate program under the children and the maternal program
focuses on various ways to help, the children who at risk of getting obese due dietary reasons.
The programme, therefore, focuses on ways that help detect and monitor childhood overweight.
The guidelines that will be used during the program are based on the Child Health Branch of the
countries department of Health and Human service. The screening although focuses on Obese
condition, will also detect other conditions that might be related to obesity. The group is hoping
to achieve the health goals through involving the parents. The parents will be involved in the
BMI health program. The BMI report will be submitted to parents during intervals. The parents
being important stakeholder might want to opt out their children out of the program after
sometimes.
Intervention time frame
The staff members of the group receive prior information about children in school for all
the students supposed to undergo screening. There should be a proper parental agreement and
consent within the first three months before the actual implementation since they form a more
significant part of the parental consciousness program. The parental consent is therefore done
before the measuring and weighing of the children. The school provides an environment that is
private. The school hall would probably be the best place. This is to help keep dignity, cultural
need, and confidentiality of the individual undertaking the test during those designated times for
the test.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH ECONOMICS 4
The test can be taken during the evenings so that it doesn’t interfere with the standard
learnings of the class schedules. All the equipment must be checked to ensure that they are error
free. They are also to be checked so that they don’t cause any injury to the students. Their
assembly must be done before the measurement so that they don’t scare the children off. Both
the weighing and the measuring scale should be hidden from the view of both the children and
other non-professionals. The child should be prepared psychological and be told of the test. Any
anxiety should be treated professionally and sensitively. The children should not be coerced into
the process. Any child under personal circumstances known by the school and the parents should
be treated with care. The child may feel excluded, but proper explanations for each circumstance
should make the child feel like the rest. At times measurement might be taken, but not recorded
as accurate or not reported either.
To attain competency, the observation for each staff member should be a minimum of 5
for both height and weight measurements. The observed should also carry a same minimum
number of both height and weight. For better results, the observation could be done annually
with mentors. Peer observed practice could be done annually, and useful feedback relayed to the
critical stakeholder.
Analysis Time Frame
Hours of intervention time frame depends on the ages of children found in the school.
The primarily obese children will require up 75 hours of contact with a period ranging from six
to twelve months depending on how they react to the behavioral intervention treatment. The
hours of contact are also part of the proxy used for treatment. Weight outcomes are limited to six
and twelve months since they are the beginning of the intervention unit, and the maintenance is
short and within the first interventions outcomes that are observed. Counseling of the weight
The test can be taken during the evenings so that it doesn’t interfere with the standard
learnings of the class schedules. All the equipment must be checked to ensure that they are error
free. They are also to be checked so that they don’t cause any injury to the students. Their
assembly must be done before the measurement so that they don’t scare the children off. Both
the weighing and the measuring scale should be hidden from the view of both the children and
other non-professionals. The child should be prepared psychological and be told of the test. Any
anxiety should be treated professionally and sensitively. The children should not be coerced into
the process. Any child under personal circumstances known by the school and the parents should
be treated with care. The child may feel excluded, but proper explanations for each circumstance
should make the child feel like the rest. At times measurement might be taken, but not recorded
as accurate or not reported either.
To attain competency, the observation for each staff member should be a minimum of 5
for both height and weight measurements. The observed should also carry a same minimum
number of both height and weight. For better results, the observation could be done annually
with mentors. Peer observed practice could be done annually, and useful feedback relayed to the
critical stakeholder.
Analysis Time Frame
Hours of intervention time frame depends on the ages of children found in the school.
The primarily obese children will require up 75 hours of contact with a period ranging from six
to twelve months depending on how they react to the behavioral intervention treatment. The
hours of contact are also part of the proxy used for treatment. Weight outcomes are limited to six
and twelve months since they are the beginning of the intervention unit, and the maintenance is
short and within the first interventions outcomes that are observed. Counseling of the weight
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 5
loss takes up to 12 months up to the end of the actual intervention of the obese problem, which is
the intervention method that takes the most extended period.
Low-intensity intervention methods are typically used for six months. The six months
involve up to 25 contact hours. The contact hours should reduce with the improvement of age.
Children aged up to 12 years and older will have reduced contact hours and short-term
intervention for up to 6 months. When submarine treatment is used as an intervention method
for a younger population, the group takes less than six months for older children of up to the age
of sixteen years. The intervention, however, has not been recommended for the younger children
below the age of 6 years. As much as these could be the fastest intervention method taking a
shorter time, it can’t be used in this case since there are younger children of that age within the
school environment. Screening intervals vary about the condition for each child that will be
tested for the first time. For extreme cases of overweight will require a shorter period of up to 3
months before undergoing another screening process. For those children of lesser weight will
involve up to six months for another screening to take place.
The incorporation of parents for counseling as suggested will lead to longer and much
time. The parents have to show commitment which will mean more time for the program.
Parental involvement is one of the vital components that might take up to six to twelve months
depending on the seriousness of the parent. The trajectory of the parent might help in the status
of the overall of the intentions of the child and the parent involved (Konnopka, Leichsenring,
Leibing & König, 2009). Interventions that involve combining two methods for one individual
have proven to take lesser times and longer accuracy depending on how they are combined. The
use of counseling and drug methods tend to work very fast, and effects are realized as early as
three months. Use of BMI method and counseling might take up to six months so that the effect
loss takes up to 12 months up to the end of the actual intervention of the obese problem, which is
the intervention method that takes the most extended period.
Low-intensity intervention methods are typically used for six months. The six months
involve up to 25 contact hours. The contact hours should reduce with the improvement of age.
Children aged up to 12 years and older will have reduced contact hours and short-term
intervention for up to 6 months. When submarine treatment is used as an intervention method
for a younger population, the group takes less than six months for older children of up to the age
of sixteen years. The intervention, however, has not been recommended for the younger children
below the age of 6 years. As much as these could be the fastest intervention method taking a
shorter time, it can’t be used in this case since there are younger children of that age within the
school environment. Screening intervals vary about the condition for each child that will be
tested for the first time. For extreme cases of overweight will require a shorter period of up to 3
months before undergoing another screening process. For those children of lesser weight will
involve up to six months for another screening to take place.
The incorporation of parents for counseling as suggested will lead to longer and much
time. The parents have to show commitment which will mean more time for the program.
Parental involvement is one of the vital components that might take up to six to twelve months
depending on the seriousness of the parent. The trajectory of the parent might help in the status
of the overall of the intentions of the child and the parent involved (Konnopka, Leichsenring,
Leibing & König, 2009). Interventions that involve combining two methods for one individual
have proven to take lesser times and longer accuracy depending on how they are combined. The
use of counseling and drug methods tend to work very fast, and effects are realized as early as
three months. Use of BMI method and counseling might take up to six months so that the effect
HEALTH ECONOMICS 6
is ready to be seen. The modest combination of pharmacological agents with behavioral dietary
intervention take shorter durations for children under the age of twelve. The problem only comes
after if the drug use is stopped or there is a discontinuation of the drug system. The healing
period, therefore, will be interfered with and might take a long time for up to 12 months, then the
expected three months. The combination, therefore, should be followed strictly for the short term
to be realized (Forman, Prokop, Keliher & Jacobs, 2008).
Cost collection and calculation
The estimated cost included the following critical areas. For the implementation of the
program, the cost is compared to an implementation of another school with the current one. This
implementation makes it easier to approximate what cost will be needed for ours. The first costs
will be material cost. Tools like handbooks, nutrition, and physical activities materials must be
included, dietary guideline materials and all the physical printing facilities that will be required
for the program.
The second cost is the training cost. This is a cost that includes meeting rooms, training
supplies for all the external trainers that shall have been invited to the program. These external
trainers include all the people that have been invited into the program, for example, the public
health group. Some of the trainers are also expected to participate in the preprogram training of
these individuals. The other cost is communication and transport cost. Communication includes
all the meetings that people and stakeholders of the program share their experience. These covers
for the venues and snacks that might be used during the process. The process even gets more
severe with the use and implementation of a future intervention that will require constant
communication between the members and the government stakeholders that will require constant
feedback. Transport cost is from the internal traveling tickets for experts. The tickets are required
is ready to be seen. The modest combination of pharmacological agents with behavioral dietary
intervention take shorter durations for children under the age of twelve. The problem only comes
after if the drug use is stopped or there is a discontinuation of the drug system. The healing
period, therefore, will be interfered with and might take a long time for up to 12 months, then the
expected three months. The combination, therefore, should be followed strictly for the short term
to be realized (Forman, Prokop, Keliher & Jacobs, 2008).
Cost collection and calculation
The estimated cost included the following critical areas. For the implementation of the
program, the cost is compared to an implementation of another school with the current one. This
implementation makes it easier to approximate what cost will be needed for ours. The first costs
will be material cost. Tools like handbooks, nutrition, and physical activities materials must be
included, dietary guideline materials and all the physical printing facilities that will be required
for the program.
The second cost is the training cost. This is a cost that includes meeting rooms, training
supplies for all the external trainers that shall have been invited to the program. These external
trainers include all the people that have been invited into the program, for example, the public
health group. Some of the trainers are also expected to participate in the preprogram training of
these individuals. The other cost is communication and transport cost. Communication includes
all the meetings that people and stakeholders of the program share their experience. These covers
for the venues and snacks that might be used during the process. The process even gets more
severe with the use and implementation of a future intervention that will require constant
communication between the members and the government stakeholders that will require constant
feedback. Transport cost is from the internal traveling tickets for experts. The tickets are required
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH ECONOMICS 7
both for the pre-training period and intervention period. The cost for transport administrators that
may require taxi and other transport expenses (Wright, Austin, LeAnn Noh, Jiang & Sonneville,
2014).
Monitoring cost includes all the cost related to observation at each level. Monitoring is
mostly done at the schools. Further monitoring might be required at the homes of the children
where the parents will be. The cost can be summarized into three essential divisions. Money,
labor and time investment cost. The evaluation of all this data can only be broken down during
the beginning of the actual intervention period. The evaluation must be done and frequently
revisited since it is difficult to predict the cost at their exact. Therefore, all this cost remains
estimates.
Expected outcomes
There should be the difference in change for the overweight and obese prevalence. The
achievement should hope to see an increment in BMI for the significant group and slightly lower
in the control group. This will prove to us that the intervention has worked successfully. There is
also expected outcome of the long-term study. After the 12 months, there should be a 1.8kg/m
reduction of BMI for the child that has reduced the least. The panel expects inconsistent results
these should be the least approximated result (Stuhldreher et al., 2012).
In results where the outcome will be the same. There would be a test for energy intake for
external physical activities. Such cases should consider the possibility of an individual using part
exercise for a short-term period of about two months. The average daily cost of energy will,
therefore, be more than the magnitude proposed for the BMI and the childhood obesity. Parental
intervention with high-intensity nutrition should also reflect. There should be a relation of the
parental intervention though it is challenging to determine this parental intervention. Previous
both for the pre-training period and intervention period. The cost for transport administrators that
may require taxi and other transport expenses (Wright, Austin, LeAnn Noh, Jiang & Sonneville,
2014).
Monitoring cost includes all the cost related to observation at each level. Monitoring is
mostly done at the schools. Further monitoring might be required at the homes of the children
where the parents will be. The cost can be summarized into three essential divisions. Money,
labor and time investment cost. The evaluation of all this data can only be broken down during
the beginning of the actual intervention period. The evaluation must be done and frequently
revisited since it is difficult to predict the cost at their exact. Therefore, all this cost remains
estimates.
Expected outcomes
There should be the difference in change for the overweight and obese prevalence. The
achievement should hope to see an increment in BMI for the significant group and slightly lower
in the control group. This will prove to us that the intervention has worked successfully. There is
also expected outcome of the long-term study. After the 12 months, there should be a 1.8kg/m
reduction of BMI for the child that has reduced the least. The panel expects inconsistent results
these should be the least approximated result (Stuhldreher et al., 2012).
In results where the outcome will be the same. There would be a test for energy intake for
external physical activities. Such cases should consider the possibility of an individual using part
exercise for a short-term period of about two months. The average daily cost of energy will,
therefore, be more than the magnitude proposed for the BMI and the childhood obesity. Parental
intervention with high-intensity nutrition should also reflect. There should be a relation of the
parental intervention though it is challenging to determine this parental intervention. Previous
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 8
cases have not shown any relation of the parental intervention to any BMI and any other
intervention though it has proven key to the intervention process (Nihiser et al., 2009).
The intervention should also reflect the cost outcome. The implemented solution should
give a much lower monetary feedback than the one that has been put in. This will reflect perfect
and accurate cost estimates. For combined intervention cases although they might reflect high
cost. They should also show high effectiveness as expected since a lot shall have been invested
in them regarding both labor and cost. Since it is difficult to convert BMI intervention measures
into monetary terms, there isn’t much expected of the cost analysis.
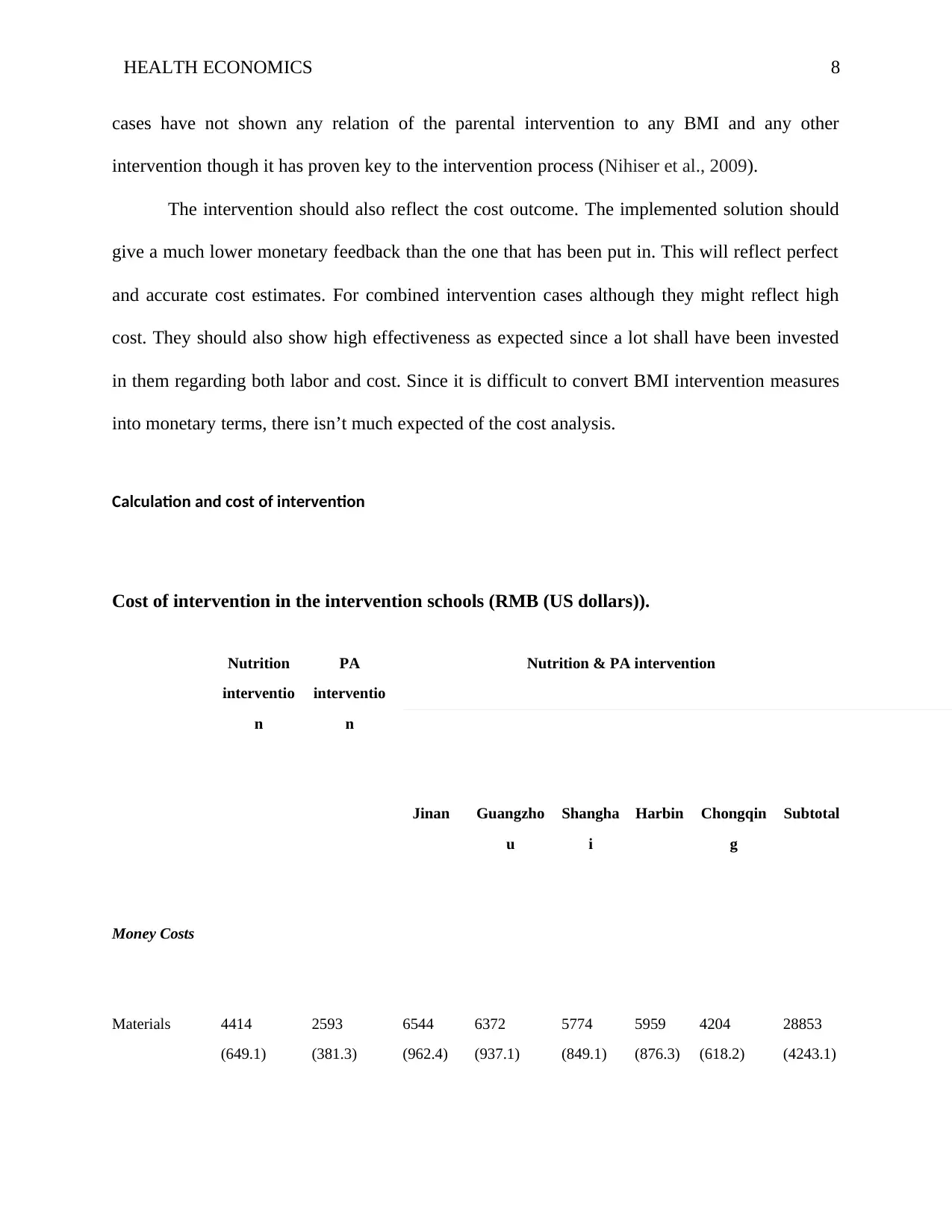
Calculation and cost of intervention
Cost of intervention in the intervention schools (RMB (US dollars)).
Nutrition
interventio
n
PA
interventio
n
Nutrition & PA intervention
Jinan Guangzho
u
Shangha
i
Harbin Chongqin
g
Subtotal
Money Costs
Materials 4414
(649.1)
2593
(381.3)
6544
(962.4)
6372
(937.1)
5774
(849.1)
5959
(876.3)
4204
(618.2)
28853
(4243.1)
cases have not shown any relation of the parental intervention to any BMI and any other
intervention though it has proven key to the intervention process (Nihiser et al., 2009).
The intervention should also reflect the cost outcome. The implemented solution should
give a much lower monetary feedback than the one that has been put in. This will reflect perfect
and accurate cost estimates. For combined intervention cases although they might reflect high
cost. They should also show high effectiveness as expected since a lot shall have been invested
in them regarding both labor and cost. Since it is difficult to convert BMI intervention measures
into monetary terms, there isn’t much expected of the cost analysis.
Calculation and cost of intervention
Cost of intervention in the intervention schools (RMB (US dollars)).
Nutrition
interventio
n
PA
interventio
n
Nutrition & PA intervention
Jinan Guangzho
u
Shangha
i
Harbin Chongqin
g
Subtotal
Money Costs
Materials 4414
(649.1)
2593
(381.3)
6544
(962.4)
6372
(937.1)
5774
(849.1)
5959
(876.3)
4204
(618.2)
28853
(4243.1)
HEALTH ECONOMICS 9
Nutrition
interventio
n
PA
interventio
n
Nutrition & PA intervention
Jinan Guangzho
u
Shangha
i
Harbin Chongqin
g
Subtotal
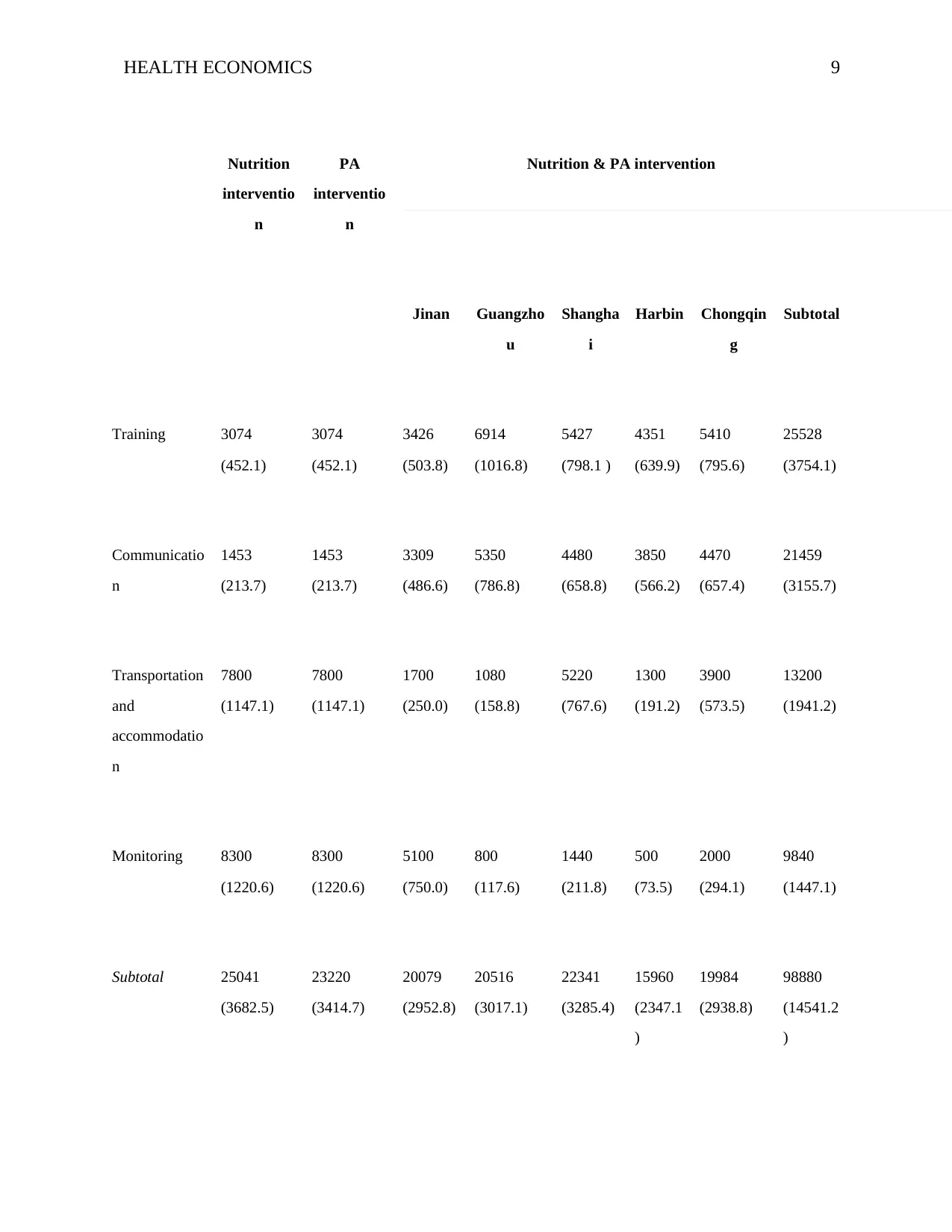
Training 3074
(452.1)
3074
(452.1)
3426
(503.8)
6914
(1016.8)
5427
(798.1 )
4351
(639.9)
5410
(795.6)
25528
(3754.1)
Communicatio
n
1453
(213.7)
1453
(213.7)
3309
(486.6)
5350
(786.8)
4480
(658.8)
3850
(566.2)
4470
(657.4)
21459
(3155.7)
Transportation
and
accommodatio
n
7800
(1147.1)
7800
(1147.1)
1700
(250.0)
1080
(158.8)
5220
(767.6)
1300
(191.2)
3900
(573.5)
13200
(1941.2)
Monitoring 8300
(1220.6)
8300
(1220.6)
5100
(750.0)
800
(117.6)
1440
(211.8)
500
(73.5)
2000
(294.1)
9840
(1447.1)
Subtotal 25041
(3682.5)
23220
(3414.7)
20079
(2952.8)
20516
(3017.1)
22341
(3285.4)
15960
(2347.1
)
19984
(2938.8)
98880
(14541.2
)
Nutrition
interventio
n
PA
interventio
n
Nutrition & PA intervention
Jinan Guangzho
u
Shangha
i
Harbin Chongqin
g
Subtotal
Training 3074
(452.1)
3074
(452.1)
3426
(503.8)
6914
(1016.8)
5427
(798.1 )
4351
(639.9)
5410
(795.6)
25528
(3754.1)
Communicatio
n
1453
(213.7)
1453
(213.7)
3309
(486.6)
5350
(786.8)
4480
(658.8)
3850
(566.2)
4470
(657.4)
21459
(3155.7)
Transportation
and
accommodatio
n
7800
(1147.1)
7800
(1147.1)
1700
(250.0)
1080
(158.8)
5220
(767.6)
1300
(191.2)
3900
(573.5)
13200
(1941.2)
Monitoring 8300
(1220.6)
8300
(1220.6)
5100
(750.0)
800
(117.6)
1440
(211.8)
500
(73.5)
2000
(294.1)
9840
(1447.1)
Subtotal 25041
(3682.5)
23220
(3414.7)
20079
(2952.8)
20516
(3017.1)
22341
(3285.4)
15960
(2347.1
)
19984
(2938.8)
98880
(14541.2
)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH ECONOMICS 10
Nutrition
interventio
n
PA
interventio
n
Nutrition & PA intervention
Jinan Guangzho
u
Shangha
i
Harbin Chongqin
g
Subtotal
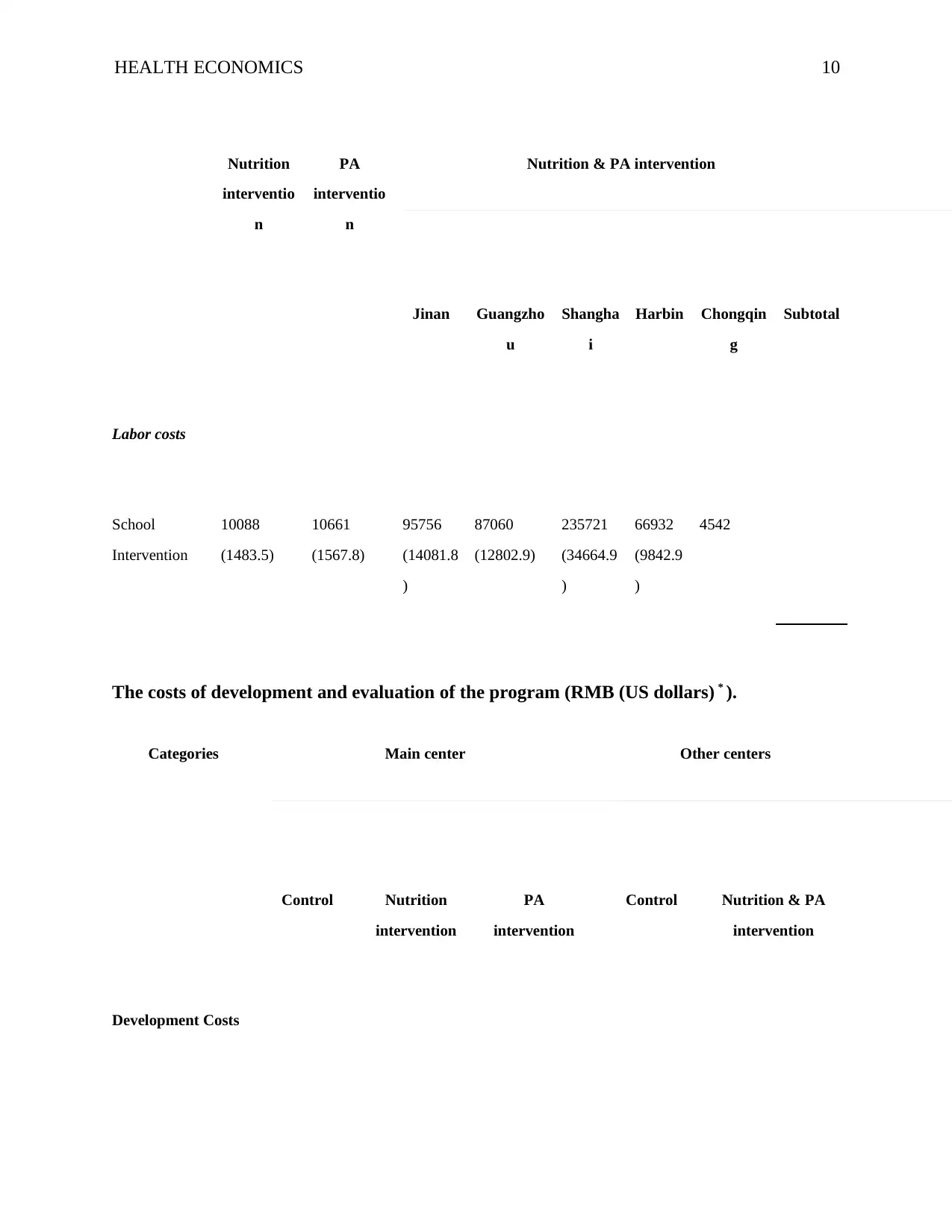
Labor costs
School
Intervention
10088
(1483.5)
10661
(1567.8)
95756
(14081.8
)
87060
(12802.9)
235721
(34664.9
)
66932
(9842.9
)
4542
The costs of development and evaluation of the program (RMB (US dollars) * ).
Categories Main center Other centers
Control Nutrition
intervention
PA
intervention
Control Nutrition & PA
intervention
Development Costs
Nutrition
interventio
n
PA
interventio
n
Nutrition & PA intervention
Jinan Guangzho
u
Shangha
i
Harbin Chongqin
g
Subtotal
Labor costs
School
Intervention
10088
(1483.5)
10661
(1567.8)
95756
(14081.8
)
87060
(12802.9)
235721
(34664.9
)
66932
(9842.9
)
4542
The costs of development and evaluation of the program (RMB (US dollars) * ).
Categories Main center Other centers
Control Nutrition
intervention
PA
intervention
Control Nutrition & PA
intervention
Development Costs
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 11
Categories Main center Other centers
Control Nutrition
intervention
PA
intervention
Control Nutrition & PA
intervention
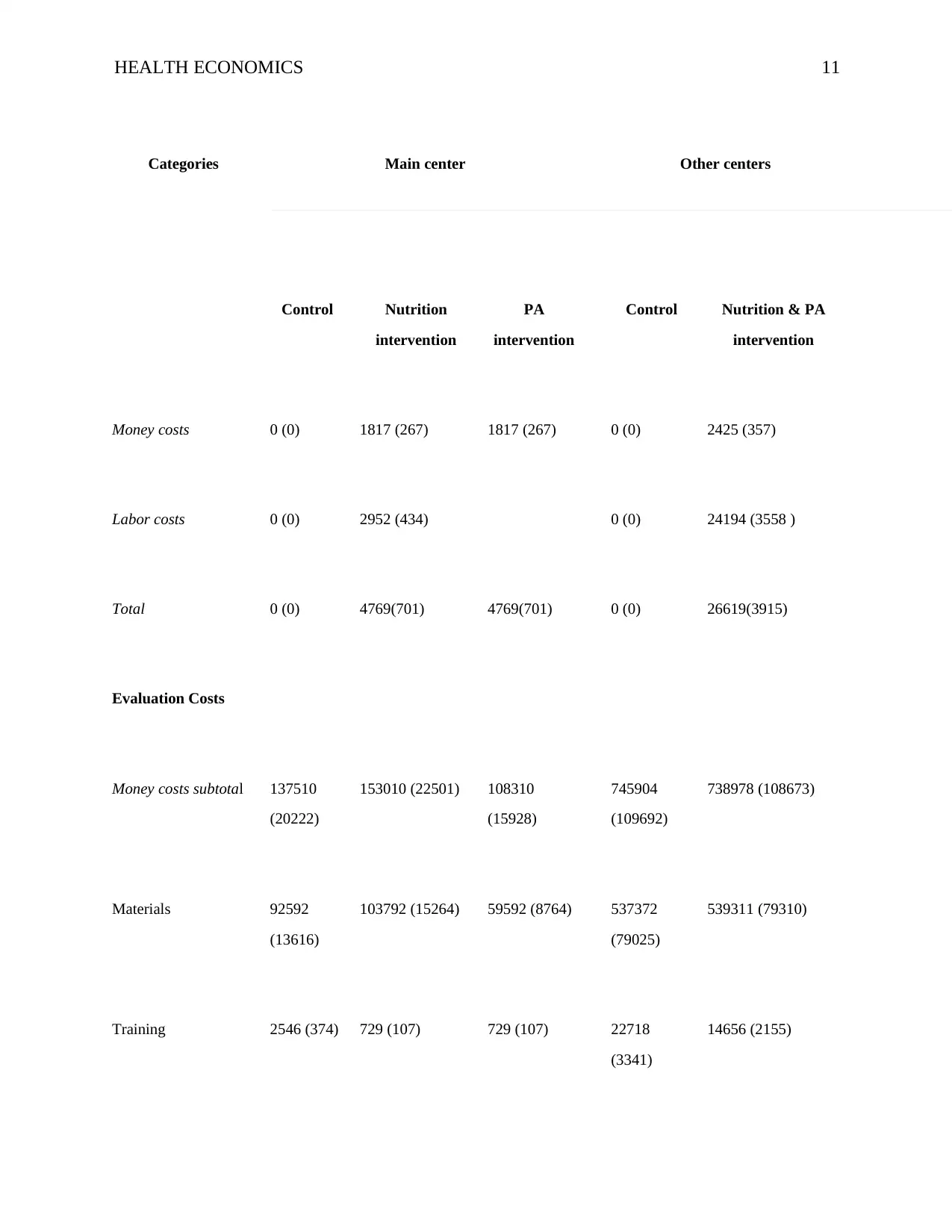
Money costs 0 (0) 1817 (267) 1817 (267) 0 (0) 2425 (357)
Labor costs 0 (0) 2952 (434) 0 (0) 24194 (3558 )
Total 0 (0) 4769(701) 4769(701) 0 (0) 26619(3915)
Evaluation Costs
Money costs subtotal 137510
(20222)
153010 (22501) 108310
(15928)
745904
(109692)
738978 (108673)
Materials 92592
(13616)
103792 (15264) 59592 (8764) 537372
(79025)
539311 (79310)
Training 2546 (374) 729 (107) 729 (107) 22718
(3341)
14656 (2155)
Categories Main center Other centers
Control Nutrition
intervention
PA
intervention
Control Nutrition & PA
intervention
Money costs 0 (0) 1817 (267) 1817 (267) 0 (0) 2425 (357)
Labor costs 0 (0) 2952 (434) 0 (0) 24194 (3558 )
Total 0 (0) 4769(701) 4769(701) 0 (0) 26619(3915)
Evaluation Costs
Money costs subtotal 137510
(20222)
153010 (22501) 108310
(15928)
745904
(109692)
738978 (108673)
Materials 92592
(13616)
103792 (15264) 59592 (8764) 537372
(79025)
539311 (79310)
Training 2546 (374) 729 (107) 729 (107) 22718
(3341)
14656 (2155)
HEALTH ECONOMICS 12
Categories Main center Other centers
Control Nutrition
intervention
PA
intervention
Control Nutrition & PA
intervention
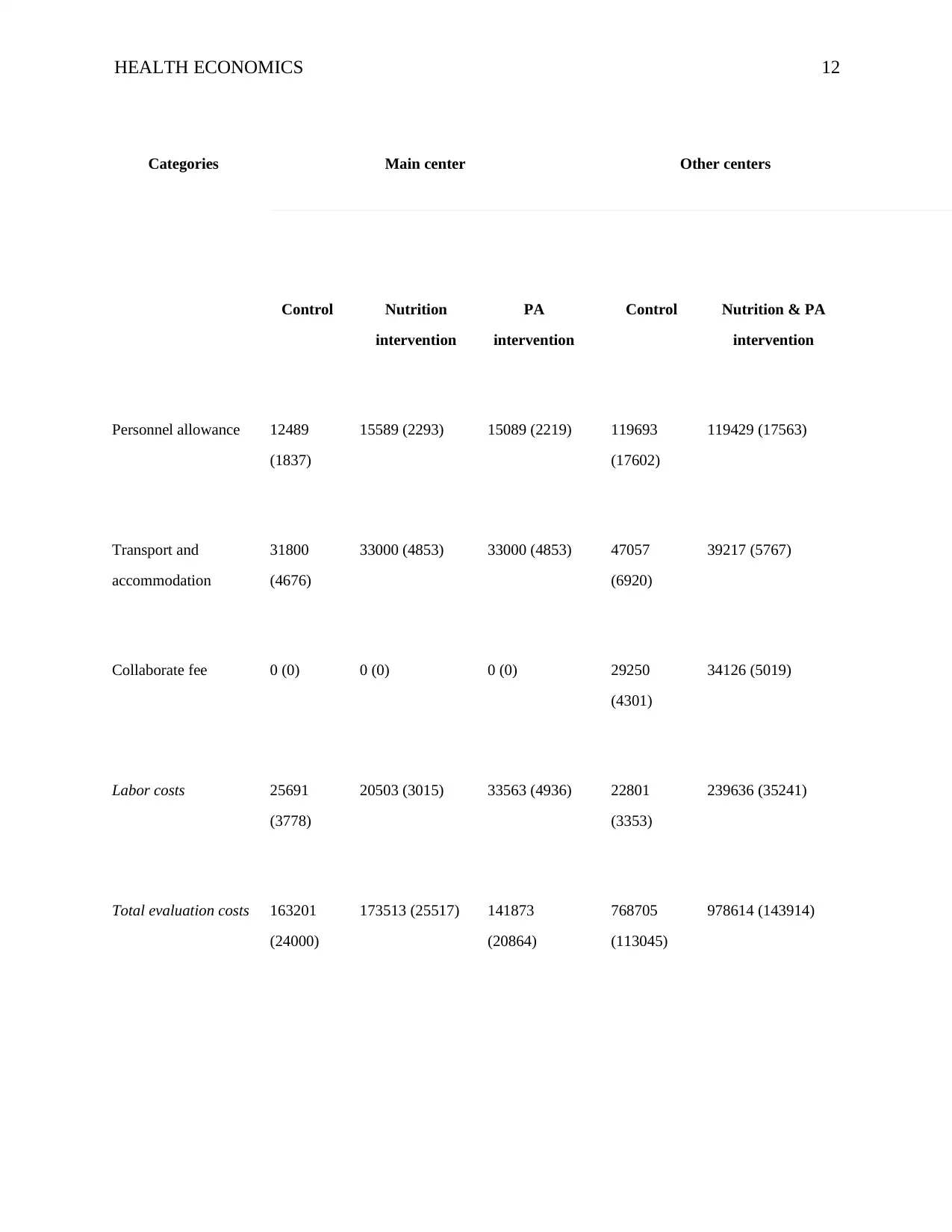
Personnel allowance 12489
(1837)
15589 (2293) 15089 (2219) 119693
(17602)
119429 (17563)
Transport and
accommodation
31800
(4676)
33000 (4853) 33000 (4853) 47057
(6920)
39217 (5767)
Collaborate fee 0 (0) 0 (0) 0 (0) 29250
(4301)
34126 (5019)
Labor costs 25691
(3778)
20503 (3015) 33563 (4936) 22801
(3353)
239636 (35241)
Total evaluation costs 163201
(24000)
173513 (25517) 141873
(20864)
768705
(113045)
978614 (143914)
Categories Main center Other centers
Control Nutrition
intervention
PA
intervention
Control Nutrition & PA
intervention
Personnel allowance 12489
(1837)
15589 (2293) 15089 (2219) 119693
(17602)
119429 (17563)
Transport and
accommodation
31800
(4676)
33000 (4853) 33000 (4853) 47057
(6920)
39217 (5767)
Collaborate fee 0 (0) 0 (0) 0 (0) 29250
(4301)
34126 (5019)
Labor costs 25691
(3778)
20503 (3015) 33563 (4936) 22801
(3353)
239636 (35241)
Total evaluation costs 163201
(24000)
173513 (25517) 141873
(20864)
768705
(113045)
978614 (143914)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.