Comparison of Skin Closure Methods in Laparoscopic Surgery
VerifiedAdded on 2023/06/15
|56
|16858
|167
AI Summary
This study compares the effectiveness of skin closure methods in laparoscopic surgery using glue, clips, and sutures. The study aims to determine the most effective method based on factors such as patient satisfaction, wound healing time, and cosmetic appearance.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

A Comparison of the Effectiveness of Skin Closure by Glue, Clips and Skin Sutures Methods
for Patients Undergoing Laparoscopic Surgery
By (Student’s Name)
Professor’s Name
College
Course
Date
for Patients Undergoing Laparoscopic Surgery
By (Student’s Name)
Professor’s Name
College
Course
Date
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ABSTRACT
Surgical practitioners are faced with challenges when deciding the best wound closure
method to be used in closing the laparoscopic port sites after the surgery, especially for child
or female. An effective method should be one that: saves time in operating room; has better
cosmetic; leads to patient satisfaction; saves time and costs of removal; cost-effective;
simple; bactericidal; painless and with less complications. All these variables must be
considered by a surgeon before settling on a particular method of wound closure. Whereas
traditional skin sutures (TSS) and metal skin clips (SC) have been commonly used before,
they have had their share of shortcomings when weighed against the above-mentioned factors
for consideration. It is upon this backdrop that the current assignment is designed to compare
sutures, clips and glue methods using in laparoscopic surgeries to determine the best method
based on the metrics indicated above. To do this, this project uses an extended literature
review to review only Randomized Control Trials studies. Thematic and content analysis is
then made using the data from these RCTs to determine the best method to be recommended
for laparoscopic surgery port site’s closure. From the review and subsequent analysis, it is
evident that whereas TSS and SC are safe and effective holding other factors constant, their
applications further need instruments; they are time consuming; create an additional staff and
cost burden for the staples/sutures removal. For this reason, glues (adhesives) is
recommended to be the ideal method for laparoscopic surgery port sites’ closure. Glue is thus
the ideal incision, which, ideally, remains simple, effective, rapid, safe, inexpensive,
cosmetic, painless and bactericidal.
Keywords: Laparoscopic surgery; wound healing; surgery; skin suture; skin staple; skin
adhesive; patient satisfaction; cosmetic appearance, surgery wound; and healing time
2
Surgical practitioners are faced with challenges when deciding the best wound closure
method to be used in closing the laparoscopic port sites after the surgery, especially for child
or female. An effective method should be one that: saves time in operating room; has better
cosmetic; leads to patient satisfaction; saves time and costs of removal; cost-effective;
simple; bactericidal; painless and with less complications. All these variables must be
considered by a surgeon before settling on a particular method of wound closure. Whereas
traditional skin sutures (TSS) and metal skin clips (SC) have been commonly used before,
they have had their share of shortcomings when weighed against the above-mentioned factors
for consideration. It is upon this backdrop that the current assignment is designed to compare
sutures, clips and glue methods using in laparoscopic surgeries to determine the best method
based on the metrics indicated above. To do this, this project uses an extended literature
review to review only Randomized Control Trials studies. Thematic and content analysis is
then made using the data from these RCTs to determine the best method to be recommended
for laparoscopic surgery port site’s closure. From the review and subsequent analysis, it is
evident that whereas TSS and SC are safe and effective holding other factors constant, their
applications further need instruments; they are time consuming; create an additional staff and
cost burden for the staples/sutures removal. For this reason, glues (adhesives) is
recommended to be the ideal method for laparoscopic surgery port sites’ closure. Glue is thus
the ideal incision, which, ideally, remains simple, effective, rapid, safe, inexpensive,
cosmetic, painless and bactericidal.
Keywords: Laparoscopic surgery; wound healing; surgery; skin suture; skin staple; skin
adhesive; patient satisfaction; cosmetic appearance, surgery wound; and healing time
2
Table of Contents
ABSTRACT..........................................................................................................................................2
CHAPTER 1: INTRODUCTION.........................................................................................................5
1.0 Introduction.....................................................................................................................................5
Research Question:...........................................................................................................................6
CHAPTER 2: REVIEW OF LITERATURE.........................................................................................7
Method 1: Tissue Adhesives:.............................................................................................................7
Uses, pros, and cons of tissue adhesives (glue).................................................................................8
Uses...............................................................................................................................................8
Pros:..............................................................................................................................................9
Cons:.............................................................................................................................................9
Contraindication:.........................................................................................................................10
Comparison:................................................................................................................................10
Adhesive Tapes:...............................................................................................................................11
Uses, Pros and Cons.........................................................................................................................12
Uses.............................................................................................................................................12
Cons:...........................................................................................................................................12
Method 2: Sutures:..........................................................................................................................13
Types of Suture:..........................................................................................................................14
Method 3: Clips:..............................................................................................................................18
CHAPTER THREE: METHODOLOGY............................................................................................20
Introduction.....................................................................................................................................20
Searching Techniques:.....................................................................................................................20
Subject Identification:......................................................................................................................20
Limiting the Search..........................................................................................................................21
3
ABSTRACT..........................................................................................................................................2
CHAPTER 1: INTRODUCTION.........................................................................................................5
1.0 Introduction.....................................................................................................................................5
Research Question:...........................................................................................................................6
CHAPTER 2: REVIEW OF LITERATURE.........................................................................................7
Method 1: Tissue Adhesives:.............................................................................................................7
Uses, pros, and cons of tissue adhesives (glue).................................................................................8
Uses...............................................................................................................................................8
Pros:..............................................................................................................................................9
Cons:.............................................................................................................................................9
Contraindication:.........................................................................................................................10
Comparison:................................................................................................................................10
Adhesive Tapes:...............................................................................................................................11
Uses, Pros and Cons.........................................................................................................................12
Uses.............................................................................................................................................12
Cons:...........................................................................................................................................12
Method 2: Sutures:..........................................................................................................................13
Types of Suture:..........................................................................................................................14
Method 3: Clips:..............................................................................................................................18
CHAPTER THREE: METHODOLOGY............................................................................................20
Introduction.....................................................................................................................................20
Searching Techniques:.....................................................................................................................20
Subject Identification:......................................................................................................................20
Limiting the Search..........................................................................................................................21
3
Literature Type:...............................................................................................................................22
Prisma Chart....................................................................................................................................23
Identification...................................................................................................................................23
Screening.........................................................................................................................................23
Eligibility..........................................................................................................................................23
Included...........................................................................................................................................23
Framework for Critique...................................................................................................................24
CHAPTER 4: STUDY FINDINGS.....................................................................................................24
Category Two: Results of Wound Cosmetic Appearance.................................................................26
Category Three: Patients’ Satisfaction Results................................................................................26
CHAPTER 5: DISCUSSION:.............................................................................................................27
CHAPTER 6: CONCLUSION............................................................................................................38
REFERENCES:……………………………………………………………………………………………………………………………………42
APPENDICES.....................................................................................................................................53
Appendix 1:.....................................................................................................................................53
4
Prisma Chart....................................................................................................................................23
Identification...................................................................................................................................23
Screening.........................................................................................................................................23
Eligibility..........................................................................................................................................23
Included...........................................................................................................................................23
Framework for Critique...................................................................................................................24
CHAPTER 4: STUDY FINDINGS.....................................................................................................24
Category Two: Results of Wound Cosmetic Appearance.................................................................26
Category Three: Patients’ Satisfaction Results................................................................................26
CHAPTER 5: DISCUSSION:.............................................................................................................27
CHAPTER 6: CONCLUSION............................................................................................................38
REFERENCES:……………………………………………………………………………………………………………………………………42
APPENDICES.....................................................................................................................................53
Appendix 1:.....................................................................................................................................53
4
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER 1: INTRODUCTION
1.0 Introduction
Laparoscopic surgery is a form of surgery which is minimally invasive; the surgeon uses a
key hole to assess the desired body organ (Robinson et al 2004). It is a modern surgical
method whereby operations are undertaken via small incisions (normally 0.5 to 1.5
centimeter) elsewhere in the body. Laparoscopic surgery an advantage over common, open
procedure, because both hemorrhaging and pain are decreased as a result of smaller incisions
alongside shorter recovery time (Rosen et al 2005). The use laparoscope is the key element in
this laparoscopic surgery together with a long fiber optic cable system that allows the affected
area to be viewed through a snaking cable from a distant, yet more effortlessly accessible
destination. The laparoscopic surgery entails operations within pelvic and abdominal cavities
while the keyhole surgery undertaken on chest and thoracic cavity is known as thoracoscopic
surgery. The laparoscopic surgical surgery wound closure can be done using glues, clips and
sutures (Singer et al 2004). The glue is never put in wound but on a wound (outside the
wound) whereby the surgeon pinches the skin edges together when they are dry and placing a
drop of glue on the top of the wound (Chow et al 2010). This glue has tiny threads that make
it stronger as fiberglass therefore it prevents gaping and eliminates bandaging. A suture is a
threadlike substance used by surgeons to hold tissues together following the surgery. Suturing
entails use of a needle with attached length thread. There are both absorbable and non-
absorbable sutures based on the degradeability of the materials used to make the suture by the
body. Examples of absorbable sutures are original catgut and newer synthetics polylactic
acid, polyglycolic acid, caprolactone and polydioxane. Examples of non-absorbable sutures
5
1.0 Introduction
Laparoscopic surgery is a form of surgery which is minimally invasive; the surgeon uses a
key hole to assess the desired body organ (Robinson et al 2004). It is a modern surgical
method whereby operations are undertaken via small incisions (normally 0.5 to 1.5
centimeter) elsewhere in the body. Laparoscopic surgery an advantage over common, open
procedure, because both hemorrhaging and pain are decreased as a result of smaller incisions
alongside shorter recovery time (Rosen et al 2005). The use laparoscope is the key element in
this laparoscopic surgery together with a long fiber optic cable system that allows the affected
area to be viewed through a snaking cable from a distant, yet more effortlessly accessible
destination. The laparoscopic surgery entails operations within pelvic and abdominal cavities
while the keyhole surgery undertaken on chest and thoracic cavity is known as thoracoscopic
surgery. The laparoscopic surgical surgery wound closure can be done using glues, clips and
sutures (Singer et al 2004). The glue is never put in wound but on a wound (outside the
wound) whereby the surgeon pinches the skin edges together when they are dry and placing a
drop of glue on the top of the wound (Chow et al 2010). This glue has tiny threads that make
it stronger as fiberglass therefore it prevents gaping and eliminates bandaging. A suture is a
threadlike substance used by surgeons to hold tissues together following the surgery. Suturing
entails use of a needle with attached length thread. There are both absorbable and non-
absorbable sutures based on the degradeability of the materials used to make the suture by the
body. Examples of absorbable sutures are original catgut and newer synthetics polylactic
acid, polyglycolic acid, caprolactone and polydioxane. Examples of non-absorbable sutures
5
are made of silk or synthetic polyester, nylon or polypropylene. Clips have “teeth’ that offer
better clamping and wound closure of skin. The clips are also easy to remove following
recovery and have less trauma and usable with existing 9mm removers and applies. They are
perfect for swiftly closing wounds as they provide maximum holding force with fewer
traumas, and remain much easier and swifter to use as opposed to traditional sutures.
This extended literature review is designed to critically review the existing literature and
compare the use of skin closure by glue, clip, and suture in laparoscopic surgery to determine
the safety as well as the efficacy of the three materials. A review of ten RCT studies is done
to compare all these wound closure substances.
In essence, a surgical incision closure method has to be economical, time saving, simple to
perform, as well as provide an optimal cosmetic outcome. Albeit sutures are frequently used
in surgery, unlimited number of reviews are available in the field which compares or even
assessment the qualities and attributes of the sutures. Over the decades, the study on critical
wound healing has culminated in the technological advamncement of staples and tissues
adhesive methods. Scientist and medical researchers have conducted studies to analyze the
different types materials used for wound closure including laser assisted tissue bonding
(Simohon, Gabay and Shpolyansky et al,,, 2015).
Research Question:
Which are the most effective wound closure methods (glue, clip, or sutures) in laparoscopic
surgery?
Aim and objectives of the study:
This study is aimed at investigating which wound closure technique is most effective during
laparoscopic surgery
Specific objectives:
6
better clamping and wound closure of skin. The clips are also easy to remove following
recovery and have less trauma and usable with existing 9mm removers and applies. They are
perfect for swiftly closing wounds as they provide maximum holding force with fewer
traumas, and remain much easier and swifter to use as opposed to traditional sutures.
This extended literature review is designed to critically review the existing literature and
compare the use of skin closure by glue, clip, and suture in laparoscopic surgery to determine
the safety as well as the efficacy of the three materials. A review of ten RCT studies is done
to compare all these wound closure substances.
In essence, a surgical incision closure method has to be economical, time saving, simple to
perform, as well as provide an optimal cosmetic outcome. Albeit sutures are frequently used
in surgery, unlimited number of reviews are available in the field which compares or even
assessment the qualities and attributes of the sutures. Over the decades, the study on critical
wound healing has culminated in the technological advamncement of staples and tissues
adhesive methods. Scientist and medical researchers have conducted studies to analyze the
different types materials used for wound closure including laser assisted tissue bonding
(Simohon, Gabay and Shpolyansky et al,,, 2015).
Research Question:
Which are the most effective wound closure methods (glue, clip, or sutures) in laparoscopic
surgery?
Aim and objectives of the study:
This study is aimed at investigating which wound closure technique is most effective during
laparoscopic surgery
Specific objectives:
6
To determine which closure technique leads to optimal cosmetic appearance and less
wound complications.
Identifying which wound closure technique (suture, glue or clip) provide the most
patient satisfaction after laparoscopic surgery.
Investigating which wound closure technique leads to the quickest wound healing
duration
CHAPTER 2: REVIEW OF LITERATURE
Method 1: Tissue Adhesives:
Many methods are available for wound closures like glues, clips and sutures (Ebersole and
Choudhury 2018). However, the most commonly used material is sutured(Norton and Ischy
2017). Nevertheless, new techniques have been introduced such as tissue adhesives and
adhesive paper tape. In the year 1949, a cyanoacrylate tissue adhesive was developed by a
German chemist which was utilized for the first time in 1959 by a British plastic surgeon
(Buchweitz et al. 2016). In 1998, Food and Drug Association (FDA) approved Octyl-2-
cyanoacrylate or OCA for use in wound closure. It often begins to work upon being applied
within ten seconds. The stabilizer gets neutralized by partly ionized water molecules on the
surface of the skin that eventually trigger polymerization of molecules (Antoniou et al. 2016).
The OCA, interestingly, breaking strength is almost 5-times that of monofilament nylon
sutures. The HVOCA (high-viscosity octyl-2-cyanoacrylate) is a newer formulation which is
thicker as opposed to the initial OCA (Buchweitz et al. 2016). The high-viscosity has an
7
wound complications.
Identifying which wound closure technique (suture, glue or clip) provide the most
patient satisfaction after laparoscopic surgery.
Investigating which wound closure technique leads to the quickest wound healing
duration
CHAPTER 2: REVIEW OF LITERATURE
Method 1: Tissue Adhesives:
Many methods are available for wound closures like glues, clips and sutures (Ebersole and
Choudhury 2018). However, the most commonly used material is sutured(Norton and Ischy
2017). Nevertheless, new techniques have been introduced such as tissue adhesives and
adhesive paper tape. In the year 1949, a cyanoacrylate tissue adhesive was developed by a
German chemist which was utilized for the first time in 1959 by a British plastic surgeon
(Buchweitz et al. 2016). In 1998, Food and Drug Association (FDA) approved Octyl-2-
cyanoacrylate or OCA for use in wound closure. It often begins to work upon being applied
within ten seconds. The stabilizer gets neutralized by partly ionized water molecules on the
surface of the skin that eventually trigger polymerization of molecules (Antoniou et al. 2016).
The OCA, interestingly, breaking strength is almost 5-times that of monofilament nylon
sutures. The HVOCA (high-viscosity octyl-2-cyanoacrylate) is a newer formulation which is
thicker as opposed to the initial OCA (Buchweitz et al. 2016). The high-viscosity has an
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

advantage of risk reduction; the adhesive is applied away from the wound, there-by
enhancing the cosmetics of the skin. Under five-ten days, the adhesive sloughs of generally as
the wound re-epithelialize (Chen et al. 2010). Premature sloughing of the adhesive could
arise from topical ointment alongside frequent wound cleansing when it is treated with OCA.
Many new reports have illustrated the OCA effectiveness of skin closure in a broad range of
clinical context as well as surgical subspecialists (Park et al. 2015). The wound has to be
evaluated before the application of the adhesive for the subcutaneous sutures placement to
reduce the tension of the wound, elimination of subcutaneous dead space as well as
maximization of skin edge eversion (Buchweitz et al. 2016).
Uses, pros, and cons of tissue adhesives (glue)
( Al-mubarak and Al-Haddab 2013)
Uses
Tissues adhesives have already been utilized for decades in both major and minor skin
closure procedures. These materials have widespread applications and indications and have
been utilized for tissue adhesion, implants fixation, cerebrospinal fluid leaks closure as well
as blood vessels’ embolization (Buchweitz et al. 2016). Besides, these materials are currently
being utilized for groin wounds, facial wounds, laparoscopic surgical wounds,
blepharoplasty, hand surgery, and lacrimal punctum closure as well as hair transplantation.
8
enhancing the cosmetics of the skin. Under five-ten days, the adhesive sloughs of generally as
the wound re-epithelialize (Chen et al. 2010). Premature sloughing of the adhesive could
arise from topical ointment alongside frequent wound cleansing when it is treated with OCA.
Many new reports have illustrated the OCA effectiveness of skin closure in a broad range of
clinical context as well as surgical subspecialists (Park et al. 2015). The wound has to be
evaluated before the application of the adhesive for the subcutaneous sutures placement to
reduce the tension of the wound, elimination of subcutaneous dead space as well as
maximization of skin edge eversion (Buchweitz et al. 2016).
Uses, pros, and cons of tissue adhesives (glue)
( Al-mubarak and Al-Haddab 2013)
Uses
Tissues adhesives have already been utilized for decades in both major and minor skin
closure procedures. These materials have widespread applications and indications and have
been utilized for tissue adhesion, implants fixation, cerebrospinal fluid leaks closure as well
as blood vessels’ embolization (Buchweitz et al. 2016). Besides, these materials are currently
being utilized for groin wounds, facial wounds, laparoscopic surgical wounds,
blepharoplasty, hand surgery, and lacrimal punctum closure as well as hair transplantation.
8
Pros:
Many pros of tissue adhesives have been identified in comparison to skin sutures and other
techniques of closure of wounds, like reduced rate of infection, minimal time in operation
room, better cosmetic outcomes, cost-effectiveness, easy to use, instant sealing of wound,
swifter return to work and athletic activities, needle-stick injuries elimination alongside
removal of the need for post-operative suture removal (Kane et al. 2018). These tissue
adhesives are further easier as well as more friendly when children are the subjects
(Buchweitz et al. 2016). Furthermore, OCA has an undoubted safety record; as no report of
adverse effects or even carcinogenicity has been reported. Recent studies have interestingly
demonstrated that OCA utilization bars growth of bacteria and further preventing the Gram-
positive bacterial wound infections (Dowson et al. 2006). Moreover, the OCA remains a good
technique for closure of wound for patients at high risk of hypertrophic or keloid scar
formation. Hence, surgical doctors could consider tissue adhesive as the substitute technique
to sutures.
Cons:
Some limitations have been discovered on the use of OCA notwithstanding its costs that
might be more than 4 times as costly as sutures. Besides, OCA requires effective patient
selection as well as is solely for the exterior use (Matin 2003). Furthermore, OCA utilization
calls for a meticulous method, because there is a need for no gap between the margins of skin
and the bleeding. Even in the presence of small gaps, the adhesives could seep through and
hence preventing the epithelialization, eventually disrupting the healing of the wound (Matin
2003)
.
9
Many pros of tissue adhesives have been identified in comparison to skin sutures and other
techniques of closure of wounds, like reduced rate of infection, minimal time in operation
room, better cosmetic outcomes, cost-effectiveness, easy to use, instant sealing of wound,
swifter return to work and athletic activities, needle-stick injuries elimination alongside
removal of the need for post-operative suture removal (Kane et al. 2018). These tissue
adhesives are further easier as well as more friendly when children are the subjects
(Buchweitz et al. 2016). Furthermore, OCA has an undoubted safety record; as no report of
adverse effects or even carcinogenicity has been reported. Recent studies have interestingly
demonstrated that OCA utilization bars growth of bacteria and further preventing the Gram-
positive bacterial wound infections (Dowson et al. 2006). Moreover, the OCA remains a good
technique for closure of wound for patients at high risk of hypertrophic or keloid scar
formation. Hence, surgical doctors could consider tissue adhesive as the substitute technique
to sutures.
Cons:
Some limitations have been discovered on the use of OCA notwithstanding its costs that
might be more than 4 times as costly as sutures. Besides, OCA requires effective patient
selection as well as is solely for the exterior use (Matin 2003). Furthermore, OCA utilization
calls for a meticulous method, because there is a need for no gap between the margins of skin
and the bleeding. Even in the presence of small gaps, the adhesives could seep through and
hence preventing the epithelialization, eventually disrupting the healing of the wound (Matin
2003)
.
9
Contraindication:
The tissue adhesives complications are the increased susceptibility to infections,
ulceration/gangrene, oozing or bleeding from incision (Chen et al. 2010). Others include
incision under massive tension calling for sutured approximation or even edematous wound
edges, burns, partly-thickness skin loss, animal bites, across muco-cutaneous junction or
mucosal surfaces, high moisture area or dense hair, as well as high tension areas like joints
(Chen et al. 2010). Tissue adhesives remain contraindicated further in patients at high risk of
delayed healing of wound including diabetic and collagen vascular illness and also among the
OCA-allergic patients.
Comparison:
The initial prospective RCT was undertaken by Maartense et al. that compared the techniques
of closure by use of OCA, adhesive paper tape/poliglecaprone in the elective laparoscopic
surgery (Maartense et al. 2002). This study discovered that laparoscopic trocar wounds
closure with OCA reduces the duration of the surgical procedure however; it was the most
costly of the three techniques. Adhesive paper tape stood the fastest, cheapest as well as most
cost-effective technique. The cosmetic outcome stood significant better for OCA as opposed
to adhesive paper tape (Mueller, Kenton, and Anger, et al 2016). Moreover, OCA was
attributed to fewer infections of the wound compared to sutures. Additional subsequent
studies have further demonstrated the antimicrobial influences of tissue adhesives. A recent
research/Cochrane review indicated that no variation in the wound infections rates or wound
dehiscence between the sutures and HVOCAs (Barto 2003).
A RCT undertaken by (Zempsky et al 2014) accomplished similar cosmetic outcomes with
decreased cost utilizing adhesive tape closure as opposed to tissue glue in facial lacerations
amongst children. The study conducted by (Brown et al 2009) shown that an enhanced
10
The tissue adhesives complications are the increased susceptibility to infections,
ulceration/gangrene, oozing or bleeding from incision (Chen et al. 2010). Others include
incision under massive tension calling for sutured approximation or even edematous wound
edges, burns, partly-thickness skin loss, animal bites, across muco-cutaneous junction or
mucosal surfaces, high moisture area or dense hair, as well as high tension areas like joints
(Chen et al. 2010). Tissue adhesives remain contraindicated further in patients at high risk of
delayed healing of wound including diabetic and collagen vascular illness and also among the
OCA-allergic patients.
Comparison:
The initial prospective RCT was undertaken by Maartense et al. that compared the techniques
of closure by use of OCA, adhesive paper tape/poliglecaprone in the elective laparoscopic
surgery (Maartense et al. 2002). This study discovered that laparoscopic trocar wounds
closure with OCA reduces the duration of the surgical procedure however; it was the most
costly of the three techniques. Adhesive paper tape stood the fastest, cheapest as well as most
cost-effective technique. The cosmetic outcome stood significant better for OCA as opposed
to adhesive paper tape (Mueller, Kenton, and Anger, et al 2016). Moreover, OCA was
attributed to fewer infections of the wound compared to sutures. Additional subsequent
studies have further demonstrated the antimicrobial influences of tissue adhesives. A recent
research/Cochrane review indicated that no variation in the wound infections rates or wound
dehiscence between the sutures and HVOCAs (Barto 2003).
A RCT undertaken by (Zempsky et al 2014) accomplished similar cosmetic outcomes with
decreased cost utilizing adhesive tape closure as opposed to tissue glue in facial lacerations
amongst children. The study conducted by (Brown et al 2009) shown that an enhanced
10
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

cosmetic result when suturing was utilized to close wounds engaging tissue excision, leading
to higher tension of wound. The corresponding cosmetic outcome with OCA alongside
sutured closure utilization was satisfactory. A prospective RCT indicated that skin closure in
the traumatic wounds utilizing 2-OCA produced outcomes that were comparable to those of
the standard sutured closure in respect of rates of infection, long-term cosmetic outcome and
dehiscence (Maartense et al. 2002).
Adhesive Tapes:
The surgical adhesive tapes often entail an adhesive backing entailing iso-octo-acrylate
together with n-vinyl-pryolidone. The ideal surgical adhesive tape needs to be non-allergic,
water-resistant, non-irritating, vapor permeable as well as have to be strictly adhered to skin
(Buchweitz et al. 2016). Adhesive tapes are utilized most often as adjunctive wound
assistance/support following staples or even sutures removal, together with buried dermal
sutures, or even with absorbable running subcuticular sutures in the less-tension wounds
(Buchweitz et al. 2016). The application of surgical adhesive tapes in the parallel, non-
overlapping fashion following coating the whole area of application with the adjuvant
adhesive remains the optimal application method which showed the best adherence over a
period of time, as well as several significant variables in tape application have been noted
encompassing dry skin acute edges’ apposition, strict homeostasis as well as utilization of an
adhesive adjunct; besides, tension has to be disseminated along the whole tape to bar blisters
(Maartense et al. 2002).
11
to higher tension of wound. The corresponding cosmetic outcome with OCA alongside
sutured closure utilization was satisfactory. A prospective RCT indicated that skin closure in
the traumatic wounds utilizing 2-OCA produced outcomes that were comparable to those of
the standard sutured closure in respect of rates of infection, long-term cosmetic outcome and
dehiscence (Maartense et al. 2002).
Adhesive Tapes:
The surgical adhesive tapes often entail an adhesive backing entailing iso-octo-acrylate
together with n-vinyl-pryolidone. The ideal surgical adhesive tape needs to be non-allergic,
water-resistant, non-irritating, vapor permeable as well as have to be strictly adhered to skin
(Buchweitz et al. 2016). Adhesive tapes are utilized most often as adjunctive wound
assistance/support following staples or even sutures removal, together with buried dermal
sutures, or even with absorbable running subcuticular sutures in the less-tension wounds
(Buchweitz et al. 2016). The application of surgical adhesive tapes in the parallel, non-
overlapping fashion following coating the whole area of application with the adjuvant
adhesive remains the optimal application method which showed the best adherence over a
period of time, as well as several significant variables in tape application have been noted
encompassing dry skin acute edges’ apposition, strict homeostasis as well as utilization of an
adhesive adjunct; besides, tension has to be disseminated along the whole tape to bar blisters
(Maartense et al. 2002).
11

Uses, Pros and Cons
(Al-mubarak and Al-Haddab 2013)
Uses
Suture-less skin closure using adhesive tape is able to bar local skin tension, reduce overall
cost as well as decrease time consumed in operating room. (Maartense et al 2002).
Furthermore, this method permits swifter tensile strength equal restoration or eve superior at
ten days as opposed to sutured wounds. Tension of skin equal in the entire length of incision
as well as this technique helps evade post-operative “railroad track” scaring for the sutures
(Chen et al. 2010). The micro porous strips permits passage of water and gas from the surface
of skin that makes environment unfavorable for the proliferation of bacteria and hence
leading to lower infection of the wound (Chen et al. 2010). The study conducted by (Gohil,
Lakhawala and Patel 2018) study showed that wounds sealed with skin tapes stood resistant
to infection. Moreover there is reduced infection rate of the taped wounds at 3.8% against
14.0% for the wounds closed by skin sutures in those patients with clean adulterated wounds
(Matin 2003)
.
Cons:
The use of tapes is not highly recommended because of the poor reliability in their adhesive
features (Dowson et al. 2006). They are prone to losing their adhesiveness as time passes by
12
(Al-mubarak and Al-Haddab 2013)
Uses
Suture-less skin closure using adhesive tape is able to bar local skin tension, reduce overall
cost as well as decrease time consumed in operating room. (Maartense et al 2002).
Furthermore, this method permits swifter tensile strength equal restoration or eve superior at
ten days as opposed to sutured wounds. Tension of skin equal in the entire length of incision
as well as this technique helps evade post-operative “railroad track” scaring for the sutures
(Chen et al. 2010). The micro porous strips permits passage of water and gas from the surface
of skin that makes environment unfavorable for the proliferation of bacteria and hence
leading to lower infection of the wound (Chen et al. 2010). The study conducted by (Gohil,
Lakhawala and Patel 2018) study showed that wounds sealed with skin tapes stood resistant
to infection. Moreover there is reduced infection rate of the taped wounds at 3.8% against
14.0% for the wounds closed by skin sutures in those patients with clean adulterated wounds
(Matin 2003)
.
Cons:
The use of tapes is not highly recommended because of the poor reliability in their adhesive
features (Dowson et al. 2006). They are prone to losing their adhesiveness as time passes by
12
hence culminating in wound dehiscence. The adhesiveness variability is linked to the
variation in knowledge and skills of operator utilizing the tape (Kane et al. 2018). The main
cons of the tape ae the difficulties in ensuring accurate skin edge apposition as well as skin
edge eversion. Moreover, the operating room time-saving pros is in increased doubt (Gibson
et al 2011). Furthermore, it has been discovered that skin edges stood usually challenging to
accurately estimate (Park et al. 2015). In order to guarantee tape adhesiveness, skin edges
have to remain dry and strict hemostasis has to stay absolute (Siu et al. 2002). These tapes
can as well trigger injury to epidermis in the course of placement as well as removal. A
research undertaken by Sarifakioglu et al., undertook the comparison between the adhesive
strength of tincture of benzoin as well as transparent film dressing spray, and the authors
visibly illustrated that tincture of benzoin surges the adhesiveness of these tapes by nearly
seven times, while merely two-fold surge was recorded with transparent film dressing spray
(Park et al. 2015)
.
Method 2: Sutures:
Suturing has been classified as the oldest method of suturing. Wound closure by sutures is
described by the Egyptian Scroll that traces back to 3500 BC (Chen et al. 2010). The use
tendons of animals, strips of leather, horsehair, vegetable fibers, strips as well as human hair
are the oldest forms of suture materials that were used in the medieval age.
In the new age sutures were made from silk which is a biologic material for example catgut.
Today sutures are made synthetically they can be absorbable or non-absorbable (Chen et al
2010). In surgical literature, debates have existed relating to the “ideal suture substance”. For
the repair of skin, the ideal substance needs to be unreactive in tissue, inject no foreign
reaction to the body, have a fine caliber alongside smooth surface, as well as remain strong
alongside easy to handle(Chen et al. 2010). Moreover, it has to have secure knotting
13
variation in knowledge and skills of operator utilizing the tape (Kane et al. 2018). The main
cons of the tape ae the difficulties in ensuring accurate skin edge apposition as well as skin
edge eversion. Moreover, the operating room time-saving pros is in increased doubt (Gibson
et al 2011). Furthermore, it has been discovered that skin edges stood usually challenging to
accurately estimate (Park et al. 2015). In order to guarantee tape adhesiveness, skin edges
have to remain dry and strict hemostasis has to stay absolute (Siu et al. 2002). These tapes
can as well trigger injury to epidermis in the course of placement as well as removal. A
research undertaken by Sarifakioglu et al., undertook the comparison between the adhesive
strength of tincture of benzoin as well as transparent film dressing spray, and the authors
visibly illustrated that tincture of benzoin surges the adhesiveness of these tapes by nearly
seven times, while merely two-fold surge was recorded with transparent film dressing spray
(Park et al. 2015)
.
Method 2: Sutures:
Suturing has been classified as the oldest method of suturing. Wound closure by sutures is
described by the Egyptian Scroll that traces back to 3500 BC (Chen et al. 2010). The use
tendons of animals, strips of leather, horsehair, vegetable fibers, strips as well as human hair
are the oldest forms of suture materials that were used in the medieval age.
In the new age sutures were made from silk which is a biologic material for example catgut.
Today sutures are made synthetically they can be absorbable or non-absorbable (Chen et al
2010). In surgical literature, debates have existed relating to the “ideal suture substance”. For
the repair of skin, the ideal substance needs to be unreactive in tissue, inject no foreign
reaction to the body, have a fine caliber alongside smooth surface, as well as remain strong
alongside easy to handle(Chen et al. 2010). Moreover, it has to have secure knotting
13
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
attributes alongside minimum trauma must arise from its insertion. Moreover, suturing
substance has to contain some qualities of handling to be used effectively. Suture infection
risk, strength, power of tissue-holding, type of incision alongside suturing method remain
significant variables for making a decision on what particular suture type for closure of
wound(Buchweitz et al. 2016). Staples/sutures are commonly used since they avail the
desired mechanical support. A broad range of suture substances stay accessible to the present-
day surgeons (Buchweitz et al. 2016). The suture choice of a given procedure must be
anchored on known biological alongside physical attributes of suture substance, technique as
well as sutured tissues’ healing properties (Buchweitz et al. 2016). Nevertheless, the suture
materials’ availability alongside the surgeon personal preferences has key roles to play.
Types of Suture:
Suture are categorized as absorbable or permanent, natural or synthetic as well as multi-
filament or monofilament. The multi-filament suture as the easiest to handle and have
preferable knot-tying attributes (Buchweitz et al. 2016). Nevertheless, bacteria are able to
make their way in the braided interstices and thus escaping phagocytosis culminating in
suture infection, sinuses and granulomas. Conversely, monofilament sutures trigger
substantially less tissue reactions and remain easily glided via the tissue (Buchweitz et al.
2016). Their cons encompass high package shape retention, hard to handle, insecurity in
knotting, and cutting via the tissue.
14
substance has to contain some qualities of handling to be used effectively. Suture infection
risk, strength, power of tissue-holding, type of incision alongside suturing method remain
significant variables for making a decision on what particular suture type for closure of
wound(Buchweitz et al. 2016). Staples/sutures are commonly used since they avail the
desired mechanical support. A broad range of suture substances stay accessible to the present-
day surgeons (Buchweitz et al. 2016). The suture choice of a given procedure must be
anchored on known biological alongside physical attributes of suture substance, technique as
well as sutured tissues’ healing properties (Buchweitz et al. 2016). Nevertheless, the suture
materials’ availability alongside the surgeon personal preferences has key roles to play.
Types of Suture:
Suture are categorized as absorbable or permanent, natural or synthetic as well as multi-
filament or monofilament. The multi-filament suture as the easiest to handle and have
preferable knot-tying attributes (Buchweitz et al. 2016). Nevertheless, bacteria are able to
make their way in the braided interstices and thus escaping phagocytosis culminating in
suture infection, sinuses and granulomas. Conversely, monofilament sutures trigger
substantially less tissue reactions and remain easily glided via the tissue (Buchweitz et al.
2016). Their cons encompass high package shape retention, hard to handle, insecurity in
knotting, and cutting via the tissue.
14

(Al-mubarak and Al-haddad 2013)
Absorbable Suture Materials
The main characteristic of absorbable sutures is the reduction of elasticity within 60 days
after placement (Al-mubarak and Al-haddad 2013). They need to be absorbed with little or
even no tissue reaction at an anticipated rate suitable for the period of the desired tissue
support. They are utilized mainly as buried sutures for closing dermis as well as subcutaneous
tissue alongside in the reduction of wound tension (Antoniou et al. 2016). These absorbable
sutures conventionally have never been recommended for closure of skin, mainly because of
unsightly formation of railroad track. The solely natural absorbable suture recommendable is
surgical gut/catgut sutures. The synthetic multi-filament substances encompass polyglycolic
acid (Antoniou et al. 2016). On the other hand, the monofilaments forms encompass
polydioxanone (Buchweitz et al. 2016). The table below summarizes the types of the sutures
and absorbable sutures:
15
Absorbable Suture Materials
The main characteristic of absorbable sutures is the reduction of elasticity within 60 days
after placement (Al-mubarak and Al-haddad 2013). They need to be absorbed with little or
even no tissue reaction at an anticipated rate suitable for the period of the desired tissue
support. They are utilized mainly as buried sutures for closing dermis as well as subcutaneous
tissue alongside in the reduction of wound tension (Antoniou et al. 2016). These absorbable
sutures conventionally have never been recommended for closure of skin, mainly because of
unsightly formation of railroad track. The solely natural absorbable suture recommendable is
surgical gut/catgut sutures. The synthetic multi-filament substances encompass polyglycolic
acid (Antoniou et al. 2016). On the other hand, the monofilaments forms encompass
polydioxanone (Buchweitz et al. 2016). The table below summarizes the types of the sutures
and absorbable sutures:
15
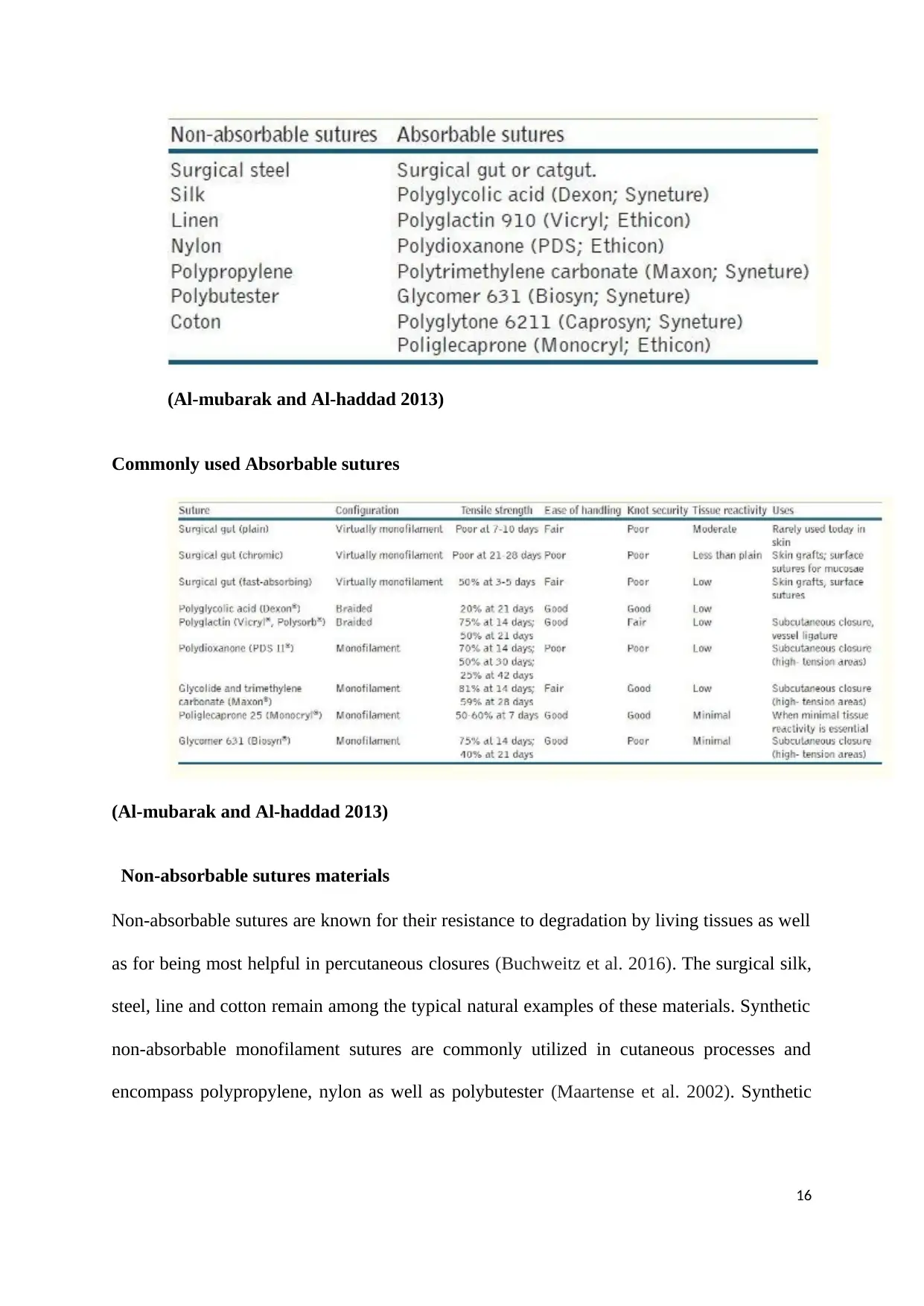
(Al-mubarak and Al-haddad 2013)
Commonly used Absorbable sutures
(Al-mubarak and Al-haddad 2013)
Non-absorbable sutures materials
Non-absorbable sutures are known for their resistance to degradation by living tissues as well
as for being most helpful in percutaneous closures (Buchweitz et al. 2016). The surgical silk,
steel, line and cotton remain among the typical natural examples of these materials. Synthetic
non-absorbable monofilament sutures are commonly utilized in cutaneous processes and
encompass polypropylene, nylon as well as polybutester (Maartense et al. 2002). Synthetic
16
Commonly used Absorbable sutures
(Al-mubarak and Al-haddad 2013)
Non-absorbable sutures materials
Non-absorbable sutures are known for their resistance to degradation by living tissues as well
as for being most helpful in percutaneous closures (Buchweitz et al. 2016). The surgical silk,
steel, line and cotton remain among the typical natural examples of these materials. Synthetic
non-absorbable monofilament sutures are commonly utilized in cutaneous processes and
encompass polypropylene, nylon as well as polybutester (Maartense et al. 2002). Synthetic
16
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
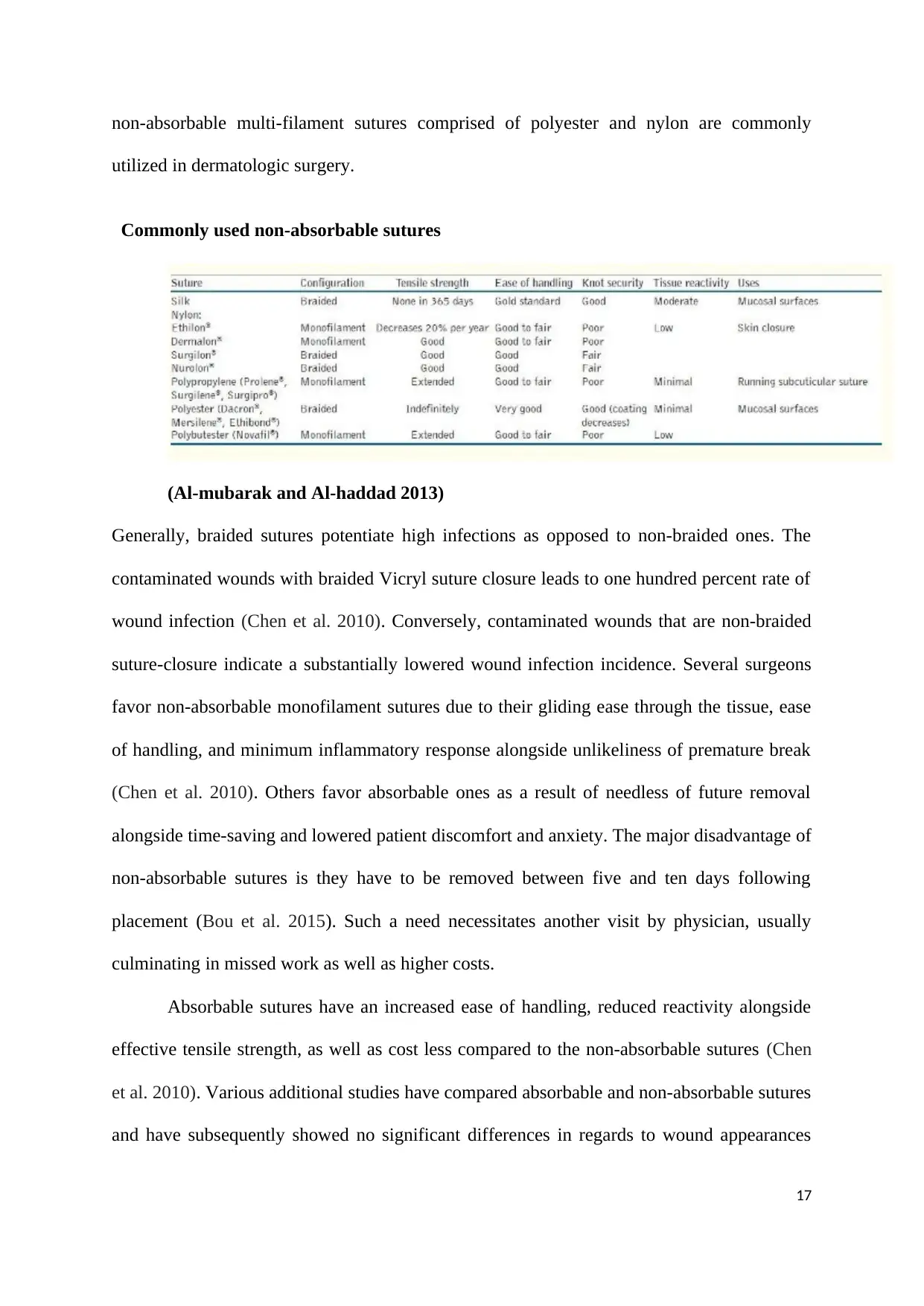
non-absorbable multi-filament sutures comprised of polyester and nylon are commonly
utilized in dermatologic surgery.
Commonly used non-absorbable sutures
(Al-mubarak and Al-haddad 2013)
Generally, braided sutures potentiate high infections as opposed to non-braided ones. The
contaminated wounds with braided Vicryl suture closure leads to one hundred percent rate of
wound infection (Chen et al. 2010). Conversely, contaminated wounds that are non-braided
suture-closure indicate a substantially lowered wound infection incidence. Several surgeons
favor non-absorbable monofilament sutures due to their gliding ease through the tissue, ease
of handling, and minimum inflammatory response alongside unlikeliness of premature break
(Chen et al. 2010). Others favor absorbable ones as a result of needless of future removal
alongside time-saving and lowered patient discomfort and anxiety. The major disadvantage of
non-absorbable sutures is they have to be removed between five and ten days following
placement (Bou et al. 2015). Such a need necessitates another visit by physician, usually
culminating in missed work as well as higher costs.
Absorbable sutures have an increased ease of handling, reduced reactivity alongside
effective tensile strength, as well as cost less compared to the non-absorbable sutures (Chen
et al. 2010). Various additional studies have compared absorbable and non-absorbable sutures
and have subsequently showed no significant differences in regards to wound appearances
17
utilized in dermatologic surgery.
Commonly used non-absorbable sutures
(Al-mubarak and Al-haddad 2013)
Generally, braided sutures potentiate high infections as opposed to non-braided ones. The
contaminated wounds with braided Vicryl suture closure leads to one hundred percent rate of
wound infection (Chen et al. 2010). Conversely, contaminated wounds that are non-braided
suture-closure indicate a substantially lowered wound infection incidence. Several surgeons
favor non-absorbable monofilament sutures due to their gliding ease through the tissue, ease
of handling, and minimum inflammatory response alongside unlikeliness of premature break
(Chen et al. 2010). Others favor absorbable ones as a result of needless of future removal
alongside time-saving and lowered patient discomfort and anxiety. The major disadvantage of
non-absorbable sutures is they have to be removed between five and ten days following
placement (Bou et al. 2015). Such a need necessitates another visit by physician, usually
culminating in missed work as well as higher costs.
Absorbable sutures have an increased ease of handling, reduced reactivity alongside
effective tensile strength, as well as cost less compared to the non-absorbable sutures (Chen
et al. 2010). Various additional studies have compared absorbable and non-absorbable sutures
and have subsequently showed no significant differences in regards to wound appearances
17
alongside rates of infection and hence concluded that clean facial wounds were linked to low
rates of infections irrespective of the technique of repair (Matin 2003).
Studies conducted indicate that no clinical significant variations in cosmetic appearance
between non-absorbable and absorbable sutures following 90 days after placement (Dowson
et al. 2006). It is reported that there is no clinical difference in scores of cosmetics between
plain catgut against nylon sutures within pediatric lacerations following four to five months
of placement (Chow et al. 2010). It was revealed that 3-point corner stich had the greatest
capillary blood flow at tip in the initial post-operative time (Kane et al. 2018). When
compared to absorbable sutures, monofilament nylon type decreased the risk of hypertonic
scaring primarily in the sternotomy scars. 3 out of 5 RCT trials that compared staples with
sutures unraveled that the rate of complication was much lower with sutures (Kane et al.
2018). Excitedly, 2/5 of studies noted that sutures were superior cosmetically. Higher
complication rates were experienced in superficial wounds that were closed using metallic
staple as opposed to the ones closed with subcuticular vicryl (Kane et al. 2018). No
difference in long-run cosmetics outcomes of repair using absorbable or non-absorbable
suture substances in adults patients that had clean wound on neck or face (Dumville et al.
2014). This new formulation’s tensile strength is decreased by fifty percent following five
days as opposed to initial Vicryl that has thirty-five reduction at fourteen days; moreover, no
traction is left following the fourteen days ( Sarifakioglu and Sarifakioglu 2006).
Method 3: Clips:
In long skin incision, skin staples are an effective method for wound closure compared to
staples because they are cost effective and time effective during closure (Shetty et al 2004).
Staples require more time during removal (Tajirian and Goldberg 2010). Studies show that
metal staples lead to a faster healing compared to other forms of wound closure, but they
increase the risk of developing infection (Shetty et al., 2004; Joshi et al., 2007; Cross et al.,
18
rates of infections irrespective of the technique of repair (Matin 2003).
Studies conducted indicate that no clinical significant variations in cosmetic appearance
between non-absorbable and absorbable sutures following 90 days after placement (Dowson
et al. 2006). It is reported that there is no clinical difference in scores of cosmetics between
plain catgut against nylon sutures within pediatric lacerations following four to five months
of placement (Chow et al. 2010). It was revealed that 3-point corner stich had the greatest
capillary blood flow at tip in the initial post-operative time (Kane et al. 2018). When
compared to absorbable sutures, monofilament nylon type decreased the risk of hypertonic
scaring primarily in the sternotomy scars. 3 out of 5 RCT trials that compared staples with
sutures unraveled that the rate of complication was much lower with sutures (Kane et al.
2018). Excitedly, 2/5 of studies noted that sutures were superior cosmetically. Higher
complication rates were experienced in superficial wounds that were closed using metallic
staple as opposed to the ones closed with subcuticular vicryl (Kane et al. 2018). No
difference in long-run cosmetics outcomes of repair using absorbable or non-absorbable
suture substances in adults patients that had clean wound on neck or face (Dumville et al.
2014). This new formulation’s tensile strength is decreased by fifty percent following five
days as opposed to initial Vicryl that has thirty-five reduction at fourteen days; moreover, no
traction is left following the fourteen days ( Sarifakioglu and Sarifakioglu 2006).
Method 3: Clips:
In long skin incision, skin staples are an effective method for wound closure compared to
staples because they are cost effective and time effective during closure (Shetty et al 2004).
Staples require more time during removal (Tajirian and Goldberg 2010). Studies show that
metal staples lead to a faster healing compared to other forms of wound closure, but they
increase the risk of developing infection (Shetty et al., 2004; Joshi et al., 2007; Cross et al.,
18
2009). Staples are associated with cosmetic dissatisfaction because they are not accepted as
suture (Singh et al., 2006).
Clips have also been successfully used in wound closure. However, they have a challenge of
failure due slippage or cellophane breakage long after the clip has been inserted (Kane et al.
2018). Albeit surface area contact has been discoursed as a variable in the study of metallic
clips, it seems as though the much larger influence in clip strength is the flexibility
(Buchweitz et al 2016). This probably further combines with Hemo clip having the greater
coefficient of the friction as opposed to the Hem-o-lok clip, although further test could be
required to have the eventual conclusion in this area (Park et al. 2015). Slippage has been
discussed in various studies as being the major method of failure of the hemo clip, the
manner they might slip has never been discussed in any previous studies.
In a wide array of instances, the clips slipped one after another in the cellophane branding
tensile tests (Park et al. 2015) which is probably a result of the vertical extension of circular
jaw stretching out cellophane, hitting each clip independently (Chen et al. 2010). In many
samples, the clips were never originally touching one another when applied, thus, when one
clip slipping, it would then join with the adjacent one, surging the slip force of each
subsequent number of clips (Chen et al. 2010). In a single slip case, the clips are often put
closer together, culminating in a slip of all the clips at a go (Chen et al. 2010). Occasionally,
this has been of higher value as opposed to multiple slip instances, however, they have just
been as often lower as the multiple slips, and remain far less common (Chen, Klapper, and
Voige et al 2008).
It remains likely that the clip type has no general effect on the load which ligation clips are
able to bear. The stainless steel Hemoclip has been found to remain stronger than the polymer
Hem-o-lok clips (Chen et al. 2010). This has shown to be statistically significant. The clips
19
suture (Singh et al., 2006).
Clips have also been successfully used in wound closure. However, they have a challenge of
failure due slippage or cellophane breakage long after the clip has been inserted (Kane et al.
2018). Albeit surface area contact has been discoursed as a variable in the study of metallic
clips, it seems as though the much larger influence in clip strength is the flexibility
(Buchweitz et al 2016). This probably further combines with Hemo clip having the greater
coefficient of the friction as opposed to the Hem-o-lok clip, although further test could be
required to have the eventual conclusion in this area (Park et al. 2015). Slippage has been
discussed in various studies as being the major method of failure of the hemo clip, the
manner they might slip has never been discussed in any previous studies.
In a wide array of instances, the clips slipped one after another in the cellophane branding
tensile tests (Park et al. 2015) which is probably a result of the vertical extension of circular
jaw stretching out cellophane, hitting each clip independently (Chen et al. 2010). In many
samples, the clips were never originally touching one another when applied, thus, when one
clip slipping, it would then join with the adjacent one, surging the slip force of each
subsequent number of clips (Chen et al. 2010). In a single slip case, the clips are often put
closer together, culminating in a slip of all the clips at a go (Chen et al. 2010). Occasionally,
this has been of higher value as opposed to multiple slip instances, however, they have just
been as often lower as the multiple slips, and remain far less common (Chen, Klapper, and
Voige et al 2008).
It remains likely that the clip type has no general effect on the load which ligation clips are
able to bear. The stainless steel Hemoclip has been found to remain stronger than the polymer
Hem-o-lok clips (Chen et al. 2010). This has shown to be statistically significant. The clips
19
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
did not break, and cellophane solely broke following clips had already slipped, hence it is not
likely that there was a failure of material itself, but instead the interactions between the
cellophane and the clips (Buchweitz et al. 2016). This interaction is attributable to coefficient
of friction between the material of the clip and the cellophane alongside the grip mode on the
cellophane (Antoniou et al. 2016). The Hemoclip depends wholly on the surface area
alongside its stiffness to usher a frictional grip. Since it makes full contact with band and is
able undergo comprehension into the thick triple layer of cellophane, it is able to maintain the
loading to the tune of 11.5 Newton for bigger clips (Antoniou et al. 2016)
.
CHAPTER THREE: METHODOLOGY
Introduction
The present study uses the systematic critical review of literature design. The literature
review permits the researchers to systematically retrieve and subsequently analyze the
existing literature on the particular topic in healthcare. The literature review used in this study
remains consistent with the Evidence-Based Care (Crochet, Aggarwal and Knight et al 2017).
This is because it enables the healthcare providers to utilize information drawn from
published research when selecting the kinds of closure techniques and materials for the
patient who under surgical procedures and process in the operation room.
Searching Techniques:
The Randomized Control Trial studies for this present study were drawn from PubMed
database(Greco, Carpreeti and Beretta et al 2014).It is a credible database to retrieve the
healthcare or medical sources. It contains nursing and allied health journals with million
health-linked literature citations.
20
likely that there was a failure of material itself, but instead the interactions between the
cellophane and the clips (Buchweitz et al. 2016). This interaction is attributable to coefficient
of friction between the material of the clip and the cellophane alongside the grip mode on the
cellophane (Antoniou et al. 2016). The Hemoclip depends wholly on the surface area
alongside its stiffness to usher a frictional grip. Since it makes full contact with band and is
able undergo comprehension into the thick triple layer of cellophane, it is able to maintain the
loading to the tune of 11.5 Newton for bigger clips (Antoniou et al. 2016)
.
CHAPTER THREE: METHODOLOGY
Introduction
The present study uses the systematic critical review of literature design. The literature
review permits the researchers to systematically retrieve and subsequently analyze the
existing literature on the particular topic in healthcare. The literature review used in this study
remains consistent with the Evidence-Based Care (Crochet, Aggarwal and Knight et al 2017).
This is because it enables the healthcare providers to utilize information drawn from
published research when selecting the kinds of closure techniques and materials for the
patient who under surgical procedures and process in the operation room.
Searching Techniques:
The Randomized Control Trial studies for this present study were drawn from PubMed
database(Greco, Carpreeti and Beretta et al 2014).It is a credible database to retrieve the
healthcare or medical sources. It contains nursing and allied health journals with million
health-linked literature citations.
20
Subject Identification:
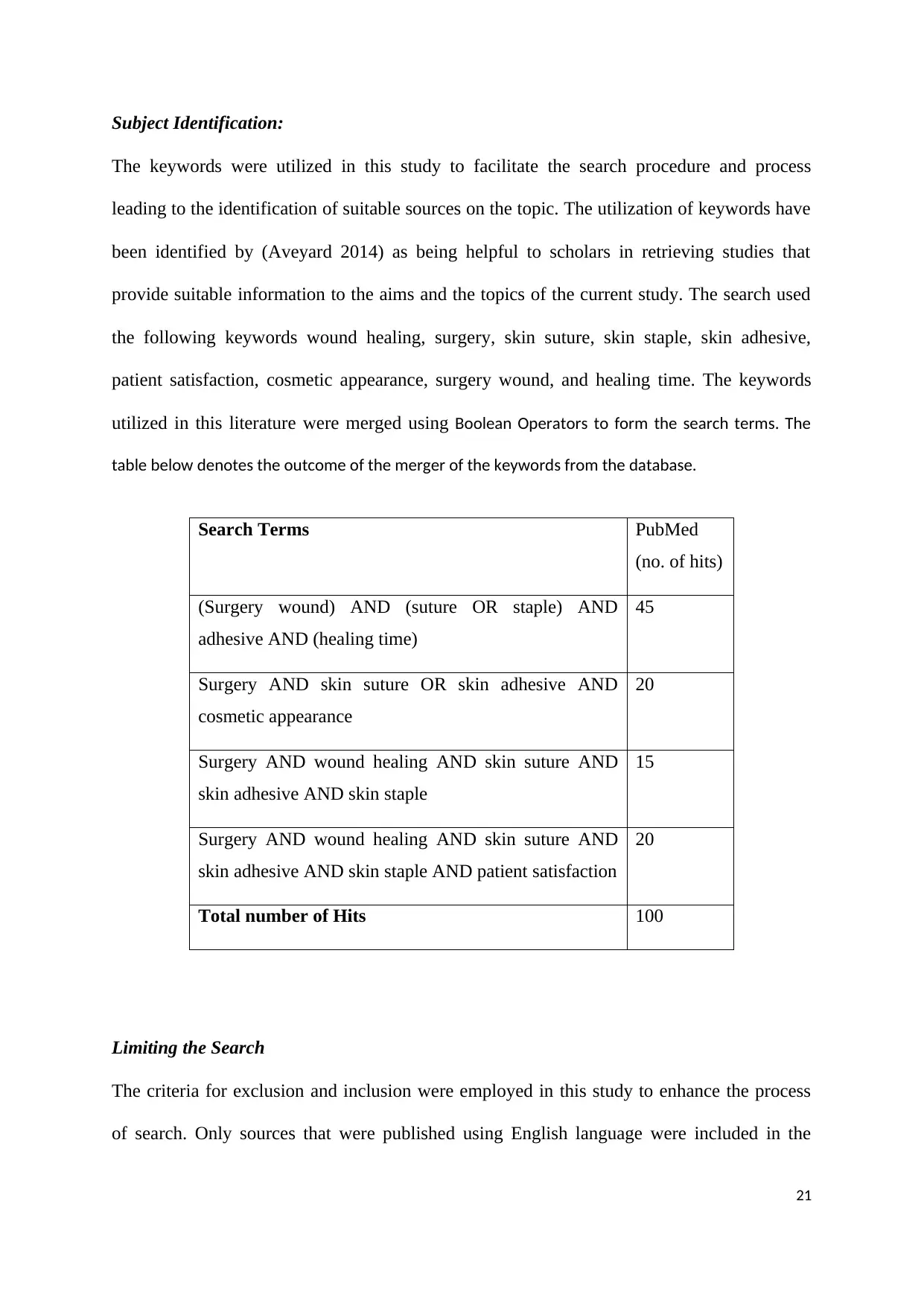
The keywords were utilized in this study to facilitate the search procedure and process
leading to the identification of suitable sources on the topic. The utilization of keywords have
been identified by (Aveyard 2014) as being helpful to scholars in retrieving studies that
provide suitable information to the aims and the topics of the current study. The search used
the following keywords wound healing, surgery, skin suture, skin staple, skin adhesive,
patient satisfaction, cosmetic appearance, surgery wound, and healing time. The keywords
utilized in this literature were merged using Boolean Operators to form the search terms. The
table below denotes the outcome of the merger of the keywords from the database.
Search Terms PubMed
(no. of hits)
(Surgery wound) AND (suture OR staple) AND
adhesive AND (healing time)
45
Surgery AND skin suture OR skin adhesive AND
cosmetic appearance
20
Surgery AND wound healing AND skin suture AND
skin adhesive AND skin staple
15
Surgery AND wound healing AND skin suture AND
skin adhesive AND skin staple AND patient satisfaction
20
Total number of Hits 100
Limiting the Search
The criteria for exclusion and inclusion were employed in this study to enhance the process
of search. Only sources that were published using English language were included in the
21
The keywords were utilized in this study to facilitate the search procedure and process
leading to the identification of suitable sources on the topic. The utilization of keywords have
been identified by (Aveyard 2014) as being helpful to scholars in retrieving studies that
provide suitable information to the aims and the topics of the current study. The search used
the following keywords wound healing, surgery, skin suture, skin staple, skin adhesive,
patient satisfaction, cosmetic appearance, surgery wound, and healing time. The keywords
utilized in this literature were merged using Boolean Operators to form the search terms. The
table below denotes the outcome of the merger of the keywords from the database.
Search Terms PubMed
(no. of hits)
(Surgery wound) AND (suture OR staple) AND
adhesive AND (healing time)
45
Surgery AND skin suture OR skin adhesive AND
cosmetic appearance
20
Surgery AND wound healing AND skin suture AND
skin adhesive AND skin staple
15
Surgery AND wound healing AND skin suture AND
skin adhesive AND skin staple AND patient satisfaction
20
Total number of Hits 100
Limiting the Search
The criteria for exclusion and inclusion were employed in this study to enhance the process
of search. Only sources that were published using English language were included in the
21
review in the period between 2000 and 2018. This timeframe is long enough for retrieving
required information on in order to effectively compare how each method has been use in
laparoscopic surgery to determine the best method. The articles that examined any or all of
the primary wound closure outcomes for the patients undergoing the laparoscopic surgery
were include for review. The inclusion criteria also allowed the studies examining patients
that were undergoing different surgical procedures. Studies carried out in the United
Kingdom and overseas were further allowed in the literature review. The inclusion criteria
made sure that a broad array of quality studies was included. The expert opinion sources were
also excluded because they rank least in the evidential hierarchy. The restrictions were
further made in the age group of patients recruited in the RCT. The review of the literature
solely included the RCTs. This is because RCTs are more valid, credible, reliable and
trustworthy sources and rates high in the evidence hierarchy only when the literature review
is well conducted (Greenhalgh, 2010). The studies published in foreign language were further
excluded in the literature review this is because, the review team was only conversant with
English and hence inclusion of foreign language is expensive to translate.
Literature Type:
The literature type for this extended literature review was from Randomized Controlled Trial
sources. This is because they provide more vigorous findings as opposed to other kinds of
quantitative studies (Polit et al., 2013). Both random selection and allocation of subjects to
the RCTs experimental group enhance the RCTs’ robustness where by all clients have an
equal chance of being allocated to either control or experimental cohort (Polit et al., 2013).
Moreover, the RCTs probed the effectiveness of intervention on a cohort of patients.
Therefore, this literature review remains restricted to RCTs because the purpose of the
current review is to determine the most effective closure technique amongst glue, clip and
suture during the laparoscopic surgery procedure.
22
required information on in order to effectively compare how each method has been use in
laparoscopic surgery to determine the best method. The articles that examined any or all of
the primary wound closure outcomes for the patients undergoing the laparoscopic surgery
were include for review. The inclusion criteria also allowed the studies examining patients
that were undergoing different surgical procedures. Studies carried out in the United
Kingdom and overseas were further allowed in the literature review. The inclusion criteria
made sure that a broad array of quality studies was included. The expert opinion sources were
also excluded because they rank least in the evidential hierarchy. The restrictions were
further made in the age group of patients recruited in the RCT. The review of the literature
solely included the RCTs. This is because RCTs are more valid, credible, reliable and
trustworthy sources and rates high in the evidence hierarchy only when the literature review
is well conducted (Greenhalgh, 2010). The studies published in foreign language were further
excluded in the literature review this is because, the review team was only conversant with
English and hence inclusion of foreign language is expensive to translate.
Literature Type:
The literature type for this extended literature review was from Randomized Controlled Trial
sources. This is because they provide more vigorous findings as opposed to other kinds of
quantitative studies (Polit et al., 2013). Both random selection and allocation of subjects to
the RCTs experimental group enhance the RCTs’ robustness where by all clients have an
equal chance of being allocated to either control or experimental cohort (Polit et al., 2013).
Moreover, the RCTs probed the effectiveness of intervention on a cohort of patients.
Therefore, this literature review remains restricted to RCTs because the purpose of the
current review is to determine the most effective closure technique amongst glue, clip and
suture during the laparoscopic surgery procedure.
22
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
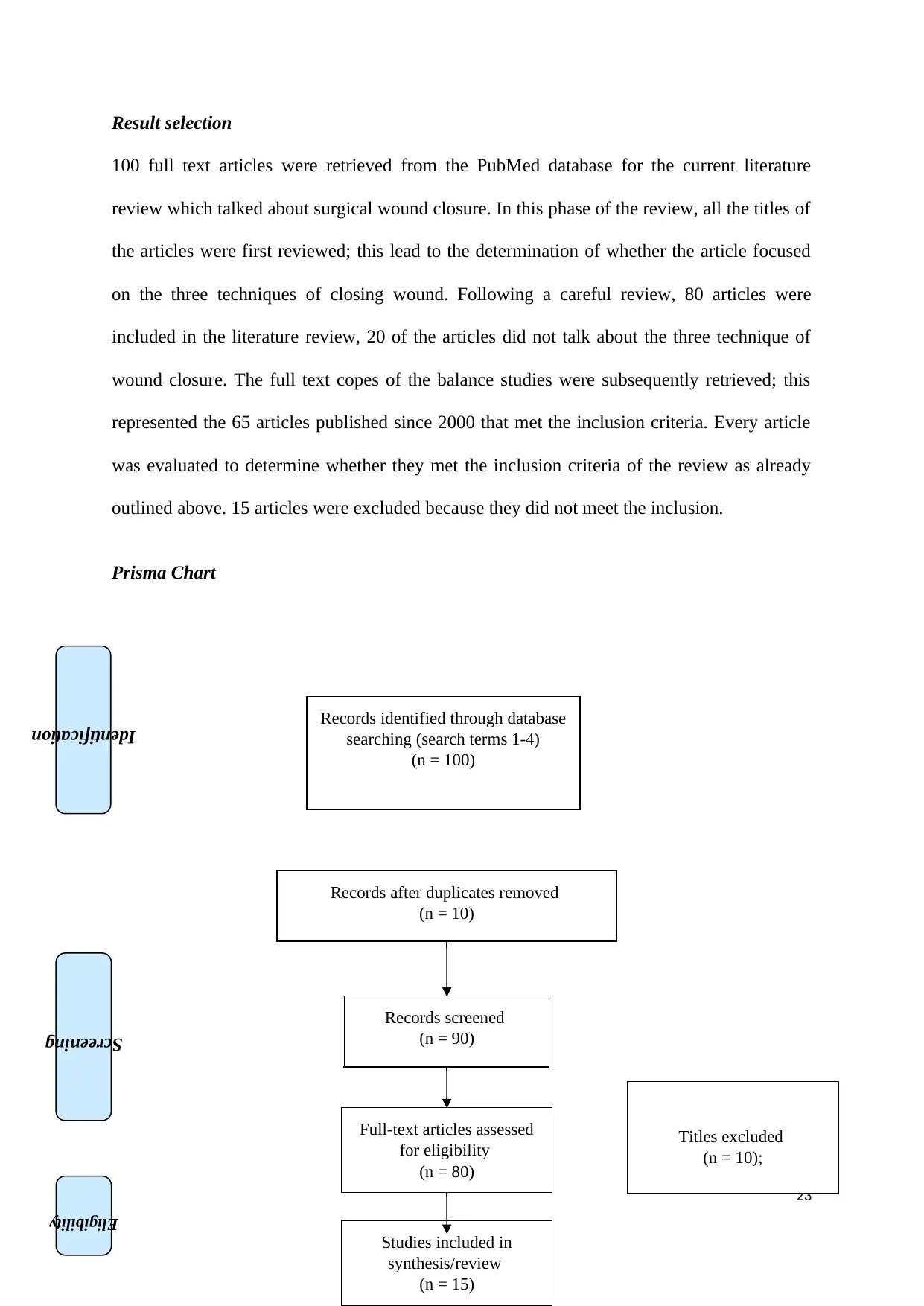
Result selection
100 full text articles were retrieved from the PubMed database for the current literature
review which talked about surgical wound closure. In this phase of the review, all the titles of
the articles were first reviewed; this lead to the determination of whether the article focused
on the three techniques of closing wound. Following a careful review, 80 articles were
included in the literature review, 20 of the articles did not talk about the three technique of
wound closure. The full text copes of the balance studies were subsequently retrieved; this
represented the 65 articles published since 2000 that met the inclusion criteria. Every article
was evaluated to determine whether they met the inclusion criteria of the review as already
outlined above. 15 articles were excluded because they did not meet the inclusion.
Prisma Chart
23
Records identified through database
searching (search terms 1-4)
(n = 100)
Screening
Eligibility
Identification
Records after duplicates removed
(n = 10)
Records screened
(n = 90)
Titles excluded
(n = 10);
Full-text articles assessed
for eligibility
(n = 80)
Studies included in
synthesis/review
(n = 15)
100 full text articles were retrieved from the PubMed database for the current literature
review which talked about surgical wound closure. In this phase of the review, all the titles of
the articles were first reviewed; this lead to the determination of whether the article focused
on the three techniques of closing wound. Following a careful review, 80 articles were
included in the literature review, 20 of the articles did not talk about the three technique of
wound closure. The full text copes of the balance studies were subsequently retrieved; this
represented the 65 articles published since 2000 that met the inclusion criteria. Every article
was evaluated to determine whether they met the inclusion criteria of the review as already
outlined above. 15 articles were excluded because they did not meet the inclusion.
Prisma Chart
23
Records identified through database
searching (search terms 1-4)
(n = 100)
Screening
Eligibility
Identification
Records after duplicates removed
(n = 10)
Records screened
(n = 90)
Titles excluded
(n = 10);
Full-text articles assessed
for eligibility
(n = 80)
Studies included in
synthesis/review
(n = 15)
Framework for Critique
The RCTs were reviewed critically utilizing the CASP, Critical Appraisal Skills Programme
(2013) tool for the RCTs. The CASP tool been validated in the previous studies and are
broadly utilized in the determination of the qualitative and quantitative studies. The CASP
tool has eleven questions that aid the scholars to appraise their corresponding articles in terms
of quality of evidence that RCTs present. The CASP tool has questions on reliability and
validity of the methods utilized in the study alongside the study outcomes. It is further helpful
for healthcare providers in determining whether the RCT has offered a precisely focused
question. The CASP help the researchers to determine whether adequate rigor has been
accomplished in the selection of the subjects.
CHAPTER 4: RESULTS
The results and findings of the literature review were classified in three key areas based on
what was being tested or reviewed. The first category of was in relation to the wound closure
time and complication (Al-mubarak and Al-haddad 2013). The second category was in
relation to cosmetic appearance and the third category was based on the surgical patients’
satisfaction. The current study review finding in relation to time was based on the mean
24
Included
Full-text articles (n=15)
excluded since they did not
meet the inclusion criteria
The RCTs were reviewed critically utilizing the CASP, Critical Appraisal Skills Programme
(2013) tool for the RCTs. The CASP tool been validated in the previous studies and are
broadly utilized in the determination of the qualitative and quantitative studies. The CASP
tool has eleven questions that aid the scholars to appraise their corresponding articles in terms
of quality of evidence that RCTs present. The CASP tool has questions on reliability and
validity of the methods utilized in the study alongside the study outcomes. It is further helpful
for healthcare providers in determining whether the RCT has offered a precisely focused
question. The CASP help the researchers to determine whether adequate rigor has been
accomplished in the selection of the subjects.
CHAPTER 4: RESULTS
The results and findings of the literature review were classified in three key areas based on
what was being tested or reviewed. The first category of was in relation to the wound closure
time and complication (Al-mubarak and Al-haddad 2013). The second category was in
relation to cosmetic appearance and the third category was based on the surgical patients’
satisfaction. The current study review finding in relation to time was based on the mean
24
Included
Full-text articles (n=15)
excluded since they did not
meet the inclusion criteria
closure time between tissue adhesive, clips and skin sutures (Al-mubarak and Al-haddad
2013). The investigators of the previous studies came to findings that, tissues adhesive wound
closure was perfect compared to clip closure and skin sutures at the initial stages of wound
closing by surgeons and nurses. Findings for these were derived from a search of 100 which
talked about surgical wound closure, 80 of these articles were included in the study and 20
were excluded because they were not about laparoscopy. Of the 80 included 65 of the articles
meet the inclusion criteria and they were published since 2000.
Moreover, the investigators conducted a three months patient’s follow up where they came
realize that there were close similarities in terms of complications and cosmetic wound
appearances within the selected three months for both skin closure using glue, clip and
adhesive (Maartense et al. 2002). Significantly, the previous study investigators found that
there were more dressings required by clip and suture groups compared to tissues adhesive
patients groups. This meant that clips and sutures needed more time to complete the closure
compared to skin closure by glue or tissue adhesive wound closer which required very
minimal dressings immediately after the laparoscopic port surgeries (Maartense et al. 2002).
The findings of the study shows that in only 21% of the patient with skin closure using glue
required immediate wound dressing while approximately 88% of the patient who went
through clip closure and skin sutures (Chen et al. 2010). According the previous findings, the
current study review suggested that, tissue adhesive wound closer method required less
wound dressings immediately after surgery compared to clip closure and tissue sutures
require several dressings immediately after surgery.
Category One: Wound Closure Time and Wound Complication Results
In relation to wound closure complications, previous study investigators found that, time
taken while using tissues adhesive wound closer method was less compared to clip and skin
25
2013). The investigators of the previous studies came to findings that, tissues adhesive wound
closure was perfect compared to clip closure and skin sutures at the initial stages of wound
closing by surgeons and nurses. Findings for these were derived from a search of 100 which
talked about surgical wound closure, 80 of these articles were included in the study and 20
were excluded because they were not about laparoscopy. Of the 80 included 65 of the articles
meet the inclusion criteria and they were published since 2000.
Moreover, the investigators conducted a three months patient’s follow up where they came
realize that there were close similarities in terms of complications and cosmetic wound
appearances within the selected three months for both skin closure using glue, clip and
adhesive (Maartense et al. 2002). Significantly, the previous study investigators found that
there were more dressings required by clip and suture groups compared to tissues adhesive
patients groups. This meant that clips and sutures needed more time to complete the closure
compared to skin closure by glue or tissue adhesive wound closer which required very
minimal dressings immediately after the laparoscopic port surgeries (Maartense et al. 2002).
The findings of the study shows that in only 21% of the patient with skin closure using glue
required immediate wound dressing while approximately 88% of the patient who went
through clip closure and skin sutures (Chen et al. 2010). According the previous findings, the
current study review suggested that, tissue adhesive wound closer method required less
wound dressings immediately after surgery compared to clip closure and tissue sutures
require several dressings immediately after surgery.
Category One: Wound Closure Time and Wound Complication Results
In relation to wound closure complications, previous study investigators found that, time
taken while using tissues adhesive wound closer method was less compared to clip and skin
25
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
sutures thus minimum complications (Chen et al. 2010). This study review based on the
previous study findings suggested that wound infection risks and complication are always
high when operation time is long than when it is short. This meant that there were minimum
wound infection risks and complications while using tissues adhesive wound closure method
compared to clips and skin sutures (Matin 2003). It was concluded by the investigators that,
wound closure time is directly related to wound complications and infections. The current
study review in relation to previous study findings concluded that the shorter the closure time
the lesser the complication and wound infections (Dowson et al. 2006). Hence, skin adhesive
proved to me more appropriate surgical wound closer method compared to clip closure
method and skin sutures.
Category Two: Results of Wound Cosmetic Appearance
The cosmetic satisfaction was assessed by previous investigators where they came to find no
statistically significant difference found between tissue adhesive closure method and clips as
well as skin sutures (Bisgaard, Klarskov, Kehlet and Rosenberg 2003). The current study
based on previous studies suggested that surgical doctors and nurses could use either of the
wound closure methods to achieve optimal cosmetics of a surgical wound. However, previous
studies proved that the cost of wound closure by tissue adhesive closure method is higher
compared to clips and skin sutures (Dowson et al. 2006). Current studies suggest that the
issue of wound closure should be reviewed as both methods have no significant different
when it comes to cosmetic wound appearances.
Majority of the reviewed articles indicated that wound cosmetic appearances are similar for
both tissue adhesive method, clips closure method and skin suture methods (Kane et al.
2018). However, one of the studies indicated small difference between wound cosmetic
appearances scars close using two different methods of wound closer methods. The surgeon
in the study who used tissues adhesive method was given a score of 45.1 %while the other
26
previous study findings suggested that wound infection risks and complication are always
high when operation time is long than when it is short. This meant that there were minimum
wound infection risks and complications while using tissues adhesive wound closure method
compared to clips and skin sutures (Matin 2003). It was concluded by the investigators that,
wound closure time is directly related to wound complications and infections. The current
study review in relation to previous study findings concluded that the shorter the closure time
the lesser the complication and wound infections (Dowson et al. 2006). Hence, skin adhesive
proved to me more appropriate surgical wound closer method compared to clip closure
method and skin sutures.
Category Two: Results of Wound Cosmetic Appearance
The cosmetic satisfaction was assessed by previous investigators where they came to find no
statistically significant difference found between tissue adhesive closure method and clips as
well as skin sutures (Bisgaard, Klarskov, Kehlet and Rosenberg 2003). The current study
based on previous studies suggested that surgical doctors and nurses could use either of the
wound closure methods to achieve optimal cosmetics of a surgical wound. However, previous
studies proved that the cost of wound closure by tissue adhesive closure method is higher
compared to clips and skin sutures (Dowson et al. 2006). Current studies suggest that the
issue of wound closure should be reviewed as both methods have no significant different
when it comes to cosmetic wound appearances.
Majority of the reviewed articles indicated that wound cosmetic appearances are similar for
both tissue adhesive method, clips closure method and skin suture methods (Kane et al.
2018). However, one of the studies indicated small difference between wound cosmetic
appearances scars close using two different methods of wound closer methods. The surgeon
in the study who used tissues adhesive method was given a score of 45.1 %while the other
26
doctor who used skin suture method was given a score of 22.45% after observing pictures of
the wounds after seven (Park et al. 2015) this was however regarded as biased observation as
majority of other studies found no significant differences in when either of the wound closer
methods is used. The current study found some contradicting opinions regarding wound
cosmetic appearance, thereby recommending future studies to be focused on the wound
cosmetics (Park et al. 2015).
Category Three: Patients’ Satisfaction Results
The study results regarding patients’ satisfaction were found after reviewing findings in the
selected previous studies. The reviewed findings from the articles revealed that at the time of
discharge, there was no difference in the wound cosmetic and scar appearance thus nor does
significant patient satisfaction among the three group (Park et al. 2015). However, the study
results changed after six weeks follow up of the three patients groups. After six weeks
recovery, the current study review based on the previous findings found that there was high
patient satisfaction among the skin closure by glue compared to clips group and skin suture
group (Chen et al. 2010). This study suggested that high patients’ satisfaction among the
tissue adhesive group was a result of shorter wound healing period, optimal wound
appearance after surgery and working scars. One of the study review investigators also found
that there was a close match between the skin colour and the surgical wound scars in tissue
adhesive group with reduced wound visibility (Chen et al. 2010). The study concluded that in
terms of healing and wound appearance skin closure by glue resulted in to increased patient
compared to the other two wound closer methods.
CHAPTER 5: DISCUSSION:
The creation of the topical skin adhesives including the monomer 2-ocytylcyanoacrylate,
surgical staples alongside tapes to replace sutures has supplemented the wound closure
27
the wounds after seven (Park et al. 2015) this was however regarded as biased observation as
majority of other studies found no significant differences in when either of the wound closer
methods is used. The current study found some contradicting opinions regarding wound
cosmetic appearance, thereby recommending future studies to be focused on the wound
cosmetics (Park et al. 2015).
Category Three: Patients’ Satisfaction Results
The study results regarding patients’ satisfaction were found after reviewing findings in the
selected previous studies. The reviewed findings from the articles revealed that at the time of
discharge, there was no difference in the wound cosmetic and scar appearance thus nor does
significant patient satisfaction among the three group (Park et al. 2015). However, the study
results changed after six weeks follow up of the three patients groups. After six weeks
recovery, the current study review based on the previous findings found that there was high
patient satisfaction among the skin closure by glue compared to clips group and skin suture
group (Chen et al. 2010). This study suggested that high patients’ satisfaction among the
tissue adhesive group was a result of shorter wound healing period, optimal wound
appearance after surgery and working scars. One of the study review investigators also found
that there was a close match between the skin colour and the surgical wound scars in tissue
adhesive group with reduced wound visibility (Chen et al. 2010). The study concluded that in
terms of healing and wound appearance skin closure by glue resulted in to increased patient
compared to the other two wound closer methods.
CHAPTER 5: DISCUSSION:
The creation of the topical skin adhesives including the monomer 2-ocytylcyanoacrylate,
surgical staples alongside tapes to replace sutures has supplemented the wound closure
27
method armamentarium. Aesthetic closure of laparoscopic surgery wound closure, if
traumatic/surgically induced, is anchored on the knowledge of healing mechanism as well as
skin anatomy alongside the appreciation of suture substances besides closure technique.
Selecting the proper material for wound closure guarantees optimal healing after the
laparoscopic surgery (Buchweitz et al. 2016).
The efficacy of the OCA tissue adhesive has been investigated in the previous studies and
compared with the non-absorbable monofilament sutures in the laparoscopic port sites’
closure (Dowson et al. 2006). The prospective, RCT design was used whereby 78 patients
were included in the study. All the subjects were taken through elective laparoscopic
procedures. The patients were assigned to the wound closure with suture or tissue adhesives
groups at random. The wound dressing requirements, wound complications, cosmetics and
skin closure time were used as the study endpoints (Buchweitz et al. 2016). The result of the
study were then measures at weeks 4; 6; and at 3 months following the discharge. A critical
review of this study demonstrate that suitable sample of (n=78) in suture group and (n=76) in
the tissue adhesive cohort stood included for the comparison of the effectiveness between
adhesives and sutures (Buchweitz et al. 2016).
Significantly, the authors highlighted that they carried out power calculations in
determining the effects of treatment in the study. It has been reported that the pilot data
presented in this study was useful in the computation of sample size. The authors managed to
detect the a fifty percent decrease in the wound closure time at 2 minutes when tissues
adhesive was used and 4 minutes when sutures were employed using a two-tailed
significance level of 0.05 and the CF of 95% (Maartense et al. 2002). This indicates the
effectiveness of tissue adhesives (glues) over sutures based on assumption of having eighty-
four patients in every arm of treatment. The utilization of the a prospective RCT design in
this study further made sure that there was a reduction in allocation bias because all patients
28
traumatic/surgically induced, is anchored on the knowledge of healing mechanism as well as
skin anatomy alongside the appreciation of suture substances besides closure technique.
Selecting the proper material for wound closure guarantees optimal healing after the
laparoscopic surgery (Buchweitz et al. 2016).
The efficacy of the OCA tissue adhesive has been investigated in the previous studies and
compared with the non-absorbable monofilament sutures in the laparoscopic port sites’
closure (Dowson et al. 2006). The prospective, RCT design was used whereby 78 patients
were included in the study. All the subjects were taken through elective laparoscopic
procedures. The patients were assigned to the wound closure with suture or tissue adhesives
groups at random. The wound dressing requirements, wound complications, cosmetics and
skin closure time were used as the study endpoints (Buchweitz et al. 2016). The result of the
study were then measures at weeks 4; 6; and at 3 months following the discharge. A critical
review of this study demonstrate that suitable sample of (n=78) in suture group and (n=76) in
the tissue adhesive cohort stood included for the comparison of the effectiveness between
adhesives and sutures (Buchweitz et al. 2016).
Significantly, the authors highlighted that they carried out power calculations in
determining the effects of treatment in the study. It has been reported that the pilot data
presented in this study was useful in the computation of sample size. The authors managed to
detect the a fifty percent decrease in the wound closure time at 2 minutes when tissues
adhesive was used and 4 minutes when sutures were employed using a two-tailed
significance level of 0.05 and the CF of 95% (Maartense et al. 2002). This indicates the
effectiveness of tissue adhesives (glues) over sutures based on assumption of having eighty-
four patients in every arm of treatment. The utilization of the a prospective RCT design in
this study further made sure that there was a reduction in allocation bias because all patients
28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
were assigned at random in skin adhesive or suture cohorts (Maartense et al. 2002). This
randomization should effective as it provided every patient an equal opportunity of being
allocated to control or intervention cohort.
A prospective study design was thus helpful in this study in allowing comparison of
endpoints across the time. Because the primary aim of this current study by Dowson above
was to compare the comparative effective of tissue adhesive or skin suture as methods of
wound closure, the authors would have assessed improvement over a period when measuring
endpoints. However, the study design selected in this study stays consistent with both
objectives and aims of the present study (Maartense et al. 2002). The randomization of
patients ensured that allocation bias is minimized and the use of patients with identical
baseline features was effective in aiding the comparison. The outcome of the study was thus
related to the interventions that the subjects were recceing and they were never influenced by
the variation in the features of the patients.
The findings are thus generalizable with a guaranteed credibility and reliability since
the study used a RCT design which ranks highest in terms hierarchy of evidence purely
because the generalizability as well as transferability of study is surged (Chen et al. 2010).
The outcome from this review clearly showed that average closure time varied between
adhesives and skin sutures. It was noted that the average time was extensive in sutures than it
was in tissue adhesive hence a confirmation of the effectiveness of adhesives over sutures
(Maartense et al. 2002). For example, the average time for closure was 220 seconds with
suture against 125 seconds in tissue adhesive with a p-value less than 0.0001. This implies
that where laparoscopic surgeon uses tissues adhesives, it will be more effective in earlier
closure of wound relative to sutures (Chen et al. 2010). Significantly, no significant variation
in cosmetics or even wound complications at weeks 4 and 6 noted following the laparoscopic
surgery or at the third month when the follow-up was done.
29
randomization should effective as it provided every patient an equal opportunity of being
allocated to control or intervention cohort.
A prospective study design was thus helpful in this study in allowing comparison of
endpoints across the time. Because the primary aim of this current study by Dowson above
was to compare the comparative effective of tissue adhesive or skin suture as methods of
wound closure, the authors would have assessed improvement over a period when measuring
endpoints. However, the study design selected in this study stays consistent with both
objectives and aims of the present study (Maartense et al. 2002). The randomization of
patients ensured that allocation bias is minimized and the use of patients with identical
baseline features was effective in aiding the comparison. The outcome of the study was thus
related to the interventions that the subjects were recceing and they were never influenced by
the variation in the features of the patients.
The findings are thus generalizable with a guaranteed credibility and reliability since
the study used a RCT design which ranks highest in terms hierarchy of evidence purely
because the generalizability as well as transferability of study is surged (Chen et al. 2010).
The outcome from this review clearly showed that average closure time varied between
adhesives and skin sutures. It was noted that the average time was extensive in sutures than it
was in tissue adhesive hence a confirmation of the effectiveness of adhesives over sutures
(Maartense et al. 2002). For example, the average time for closure was 220 seconds with
suture against 125 seconds in tissue adhesive with a p-value less than 0.0001. This implies
that where laparoscopic surgeon uses tissues adhesives, it will be more effective in earlier
closure of wound relative to sutures (Chen et al. 2010). Significantly, no significant variation
in cosmetics or even wound complications at weeks 4 and 6 noted following the laparoscopic
surgery or at the third month when the follow-up was done.
29
Significantly, the authors discovered that fewer dressings were needed when tissue
adhesive was used at twenty-one percent immediately following the laparoscopic surgery,
relative to suture that stood at 97 percent. The variation in the number of required dressing by
the suture and adhesive cohort stood significant at a p-value less than 0.001 (Chen et al.
2010). In the course of the discharge, statistical test showed a significant variations in
dressings needed by each group with twenty-four percent being noted in tissue adhesive
cohort against the 84 percent in the suture cohort at a p-value of less than 0.001(Dowson et
al. 2006). The outcome of this study by Dowson presents a precise suggestion that tissue
adhesive led to fewer dressing as opposed to sutures following the laparoscopic port site
closure thus confirming its effectiveness against the sutures (Dowson et al. 2006). Moreover,
the outcome of Dowson study recommends potential savings from the utilization of OCA
tissue adhesives because wound closure time stood shorter while wound complication is
shortened as well. On the basis of these outcomes, potential saving might be produced by the
requirements for fewer dressings when the surgeon uses tissue adhesive in laparoscopic port
site closure.
The review of the Dowson study indicates that patients stood blinded to the
intervention applied in wound closure. Nevertheless, the authors were never blinded to the
study. Authors who do not understand the intervention utilized in a research might interpret
the outcome subjectively (Kane et al. 2018). A review of the methodology of the study
indicates that taking photographs of wounds and permitting assessor’s independently in
determination of the wound cosmetics might have blinded the authors to wound closure
technique applied in the study. Therefore, when the subjects or researchers are blinded in the
study, the risk of bias reporting is curtailed.
Moreover, the data interpretations as well as statistics utilized were presented thus
giving a transparency which minimizes the interpretation bias. Seventy-eight patients were
30
adhesive was used at twenty-one percent immediately following the laparoscopic surgery,
relative to suture that stood at 97 percent. The variation in the number of required dressing by
the suture and adhesive cohort stood significant at a p-value less than 0.001 (Chen et al.
2010). In the course of the discharge, statistical test showed a significant variations in
dressings needed by each group with twenty-four percent being noted in tissue adhesive
cohort against the 84 percent in the suture cohort at a p-value of less than 0.001(Dowson et
al. 2006). The outcome of this study by Dowson presents a precise suggestion that tissue
adhesive led to fewer dressing as opposed to sutures following the laparoscopic port site
closure thus confirming its effectiveness against the sutures (Dowson et al. 2006). Moreover,
the outcome of Dowson study recommends potential savings from the utilization of OCA
tissue adhesives because wound closure time stood shorter while wound complication is
shortened as well. On the basis of these outcomes, potential saving might be produced by the
requirements for fewer dressings when the surgeon uses tissue adhesive in laparoscopic port
site closure.
The review of the Dowson study indicates that patients stood blinded to the
intervention applied in wound closure. Nevertheless, the authors were never blinded to the
study. Authors who do not understand the intervention utilized in a research might interpret
the outcome subjectively (Kane et al. 2018). A review of the methodology of the study
indicates that taking photographs of wounds and permitting assessor’s independently in
determination of the wound cosmetics might have blinded the authors to wound closure
technique applied in the study. Therefore, when the subjects or researchers are blinded in the
study, the risk of bias reporting is curtailed.
Moreover, the data interpretations as well as statistics utilized were presented thus
giving a transparency which minimizes the interpretation bias. Seventy-eight patients were
30
recruited in the suture cohort and 76 patients recruited in the tissue adhesive cohort. This
never contributed to the selection bias of the patient because the dropout rate was never high.
Moreover, the both cohorts had identical features at baseline thus reducing the bias in
selecting patients (Kane et al. 2018). A suitable sample size is necessary in the establishment
of rigor and making sure that the outcome is generalizable to a bigger and more heterogonous
cohort of patients. It is worth noting that tissue skin adhesive showed comparable outcome
based on cosmetics appearance as well as wound cosmetic besides rates of complication. The
primary advantage of tissue skin adhesive seems to be lower cost of utilizing tissue skin
adhesives as opposed to costly sutures. The application of tissue adhesives in laparoscopic
surgery leads to potential savings whereas still enhancing the cosmetic of the wounds (Kane
et al. 2018). The strength of this study depends on the number of recruited patents because an
adequately powered sample size implies that its outcome is generalizable to the bigger
population of patients who undergo laparoscopic port site closure. Nevertheless, the outcome
of this study is restricted to patients who are undergoing other surgical processes or
procedures. Skin adhesive, for example, is never suitable for gangrenous wound.
The study by (Krishnamoorthy et al. 2009) also gives useful comparison between
wound closure time and tissues adhesives Dermabond and the conventional subcuticular
sutures after the saphenous vein harvesting in the patients who underwent CABG (coronary
artery bypass grafting). The outcomes of this research shows that wound closure time stood
shorter in Dermabond cohort relative to suture group at a p-value equals to 0.017 (Park et al.
2015). In suture cohort, the media closure time stood at thirteen minutes and 20 seconds. In
comparison, the median wound closure time in Dermabond cohort stayed at merely ten
minutes and 45 seconds. This shows that Dermabond stays effective in the reduction of time
of wound as opposed to the conventional subcuticular sutures when used in the laparoscopic
surgery (Park et al. 2015).
31
never contributed to the selection bias of the patient because the dropout rate was never high.
Moreover, the both cohorts had identical features at baseline thus reducing the bias in
selecting patients (Kane et al. 2018). A suitable sample size is necessary in the establishment
of rigor and making sure that the outcome is generalizable to a bigger and more heterogonous
cohort of patients. It is worth noting that tissue skin adhesive showed comparable outcome
based on cosmetics appearance as well as wound cosmetic besides rates of complication. The
primary advantage of tissue skin adhesive seems to be lower cost of utilizing tissue skin
adhesives as opposed to costly sutures. The application of tissue adhesives in laparoscopic
surgery leads to potential savings whereas still enhancing the cosmetic of the wounds (Kane
et al. 2018). The strength of this study depends on the number of recruited patents because an
adequately powered sample size implies that its outcome is generalizable to the bigger
population of patients who undergo laparoscopic port site closure. Nevertheless, the outcome
of this study is restricted to patients who are undergoing other surgical processes or
procedures. Skin adhesive, for example, is never suitable for gangrenous wound.
The study by (Krishnamoorthy et al. 2009) also gives useful comparison between
wound closure time and tissues adhesives Dermabond and the conventional subcuticular
sutures after the saphenous vein harvesting in the patients who underwent CABG (coronary
artery bypass grafting). The outcomes of this research shows that wound closure time stood
shorter in Dermabond cohort relative to suture group at a p-value equals to 0.017 (Park et al.
2015). In suture cohort, the media closure time stood at thirteen minutes and 20 seconds. In
comparison, the median wound closure time in Dermabond cohort stayed at merely ten
minutes and 45 seconds. This shows that Dermabond stays effective in the reduction of time
of wound as opposed to the conventional subcuticular sutures when used in the laparoscopic
surgery (Park et al. 2015).
31
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
(Basha et al 2009) and (Figueroa et al 2013) studies have showed that wound
complications rates stood higher in surgical clip cohort as opposed to subcuticular suture
cohort. It is worth noting that none of the above studies unearthed that any significant
variations in patient cosmetic satisfaction at 4 to 6 weeks following the laparoscopic surgery.
Nevertheless, higher rates of complications were recognized in surgical clips cohort at
discharge in both articles (Park et al. 2015). The incidence of wound disruption or even
infection during discharge in 3 to 4 days stood at 7.1 percent in surgical clip cohort in
(Figueroa et al 2013) as opposed to 0.5 percent in suture cohort. The variations in wound
disruption or even infection rate between the cohorts stood significant with p-value less than
0.001, comparative risk stayed at 14.1 CF: 95% of 1.9 t 106 (Chen et al. 2010). In the course
of follow-up, at 4 to 6 weeks, the cumulative risk for wound disruption stayed higher in clip
at 14.5 percent as opposed to suture cohort being 5.9 percent.
The variations in wound disruptions rates stood further significant at a p-value equals
to 0.008, relative risk being 2.5 percent and 95% CI, 1.2-5.0. The statistical tests stood
utilized in establishing significant differences in results of two cohorts. (Basha et al 2015)
examined the correlation between laparoscopic surgery using clip and a 4-fold surges risk of
wound separation stood noted (adjusted odds ratio being 4.65; 95% CI of 2.070-10.52, p-
value less than 0.001) when contrasted with subcuticular suture. Therefore, from the
outcomes of (Figueroa et al 2013), together with (Basha et al 2010), it is clear that
subcuticular suture is suitable than clip sine the risk of wound complication is substantially
decreased as opposed to surgical clip. Conversely, wound complication rates are identical
when skin adhesive (glue) or surgical clip are utilized for the surgery. No significant
variations in rates of complication of wound at the third months of follow-up after the
surgery. Nevertheless, skin clips were discovered to be highly convenient in wound closure
and swifter to apply as compared to adhesives (Chen et al. 2010). Moreover, cost of skin clips
32
complications rates stood higher in surgical clip cohort as opposed to subcuticular suture
cohort. It is worth noting that none of the above studies unearthed that any significant
variations in patient cosmetic satisfaction at 4 to 6 weeks following the laparoscopic surgery.
Nevertheless, higher rates of complications were recognized in surgical clips cohort at
discharge in both articles (Park et al. 2015). The incidence of wound disruption or even
infection during discharge in 3 to 4 days stood at 7.1 percent in surgical clip cohort in
(Figueroa et al 2013) as opposed to 0.5 percent in suture cohort. The variations in wound
disruption or even infection rate between the cohorts stood significant with p-value less than
0.001, comparative risk stayed at 14.1 CF: 95% of 1.9 t 106 (Chen et al. 2010). In the course
of follow-up, at 4 to 6 weeks, the cumulative risk for wound disruption stayed higher in clip
at 14.5 percent as opposed to suture cohort being 5.9 percent.
The variations in wound disruptions rates stood further significant at a p-value equals
to 0.008, relative risk being 2.5 percent and 95% CI, 1.2-5.0. The statistical tests stood
utilized in establishing significant differences in results of two cohorts. (Basha et al 2015)
examined the correlation between laparoscopic surgery using clip and a 4-fold surges risk of
wound separation stood noted (adjusted odds ratio being 4.65; 95% CI of 2.070-10.52, p-
value less than 0.001) when contrasted with subcuticular suture. Therefore, from the
outcomes of (Figueroa et al 2013), together with (Basha et al 2010), it is clear that
subcuticular suture is suitable than clip sine the risk of wound complication is substantially
decreased as opposed to surgical clip. Conversely, wound complication rates are identical
when skin adhesive (glue) or surgical clip are utilized for the surgery. No significant
variations in rates of complication of wound at the third months of follow-up after the
surgery. Nevertheless, skin clips were discovered to be highly convenient in wound closure
and swifter to apply as compared to adhesives (Chen et al. 2010). Moreover, cost of skin clips
32
stood lower, albeit, the investigators explicated that the cost of skin clips stood lower as
opposed to costly skin adhesives.
To sum up, these studies have compared effectiveness of tissues adhesive to clips with
subcuticular sutures, in the reduction of wound complications and increasing would closure
time in diverse cohorts of patients. The effectiveness of tissue adhesive specifically
LiquiBand was compared with non-absorbable monofilament suture in laparoscopic port sites
closure (Park et al. 2015). The outcome of this study presents a suggestion that the utilization
of tissue adhesives culminated in swifter wound closure time alongside lower rates of
complications as opposed to monofilament suture.
The discussion can also be understood based on the cosmetic appearance. Dowson et al.
(2006) study indicated that cosmetic result of utilizing tissue adhesives stood relative to the
use of non-absorbable monofilament sutures for laparoscopic surgery closure of port sites.
When employed in nursing practice, the healthcare providers might either utilize tissue
adhesive or even suture for optimal cosmetic of the skin (Dowson et al. 2006). Nevertheless,
when the closure method’s cost is taken into account, the healthcare providers could favor
OCA tissue adhesive or LiquiBand rather than sutures. This finding has been bolstered by the
outcomes of the Krishnamoorthy et al. (2009) that compared the tissue adhesive
(Dermabond) effectiveness with conventional subcuticular suture for patients in the
improvement of closure of wound time, cosmetic appearance alongside satisfaction of
patients (Dowson et al. 2006) . It is imperative to highlight that the 2 independent researchers
examined the patients wound’s photographs taken 1.5 weeks following the surgery. They
were blinded to the wound closure technique displayed in the photographs.
These photographs allowed them to form the view on the cosmetics appearances of
scars following six weeks. Blinding of these surgeon researchers increased the credibility and
reliability of the findings of study. It further decreased the reporting of bias risk which is
33
opposed to costly skin adhesives.
To sum up, these studies have compared effectiveness of tissues adhesive to clips with
subcuticular sutures, in the reduction of wound complications and increasing would closure
time in diverse cohorts of patients. The effectiveness of tissue adhesive specifically
LiquiBand was compared with non-absorbable monofilament suture in laparoscopic port sites
closure (Park et al. 2015). The outcome of this study presents a suggestion that the utilization
of tissue adhesives culminated in swifter wound closure time alongside lower rates of
complications as opposed to monofilament suture.
The discussion can also be understood based on the cosmetic appearance. Dowson et al.
(2006) study indicated that cosmetic result of utilizing tissue adhesives stood relative to the
use of non-absorbable monofilament sutures for laparoscopic surgery closure of port sites.
When employed in nursing practice, the healthcare providers might either utilize tissue
adhesive or even suture for optimal cosmetic of the skin (Dowson et al. 2006). Nevertheless,
when the closure method’s cost is taken into account, the healthcare providers could favor
OCA tissue adhesive or LiquiBand rather than sutures. This finding has been bolstered by the
outcomes of the Krishnamoorthy et al. (2009) that compared the tissue adhesive
(Dermabond) effectiveness with conventional subcuticular suture for patients in the
improvement of closure of wound time, cosmetic appearance alongside satisfaction of
patients (Dowson et al. 2006) . It is imperative to highlight that the 2 independent researchers
examined the patients wound’s photographs taken 1.5 weeks following the surgery. They
were blinded to the wound closure technique displayed in the photographs.
These photographs allowed them to form the view on the cosmetics appearances of
scars following six weeks. Blinding of these surgeon researchers increased the credibility and
reliability of the findings of study. It further decreased the reporting of bias risk which is
33
common when investigators are unblended to the intervention. The wound cosmetic
appearance was thus rated by these two authors using the visual analogue scale (Dowson et
al. 2006). There were statistical tests that revealed substantial differences between scores in
Dermabond cohort and in conventional subcuticular suture cohort with p-values less than
0.001. It is also imperative to recognize that none of the wounds of the patients in suture
cohort had a score of zero denoting optimal cosmetic satisfaction. Because the two standalone
surgeons scored the wounds using distinct scenarios, it is essential to probe the inter-observer
variations.
The outcomes of statistical tests demonstrated that there were no significant with p-value
equals to 0.045 inter-observer variations between two standalone surgeons. This indicated
that the outcome stood valid as well as reliable. At follow-up in week six, the cosmetic
appearance of wounds in the Dermabond group and suture cohort stood were compared by
use of Vancouver Scale. The authors used the Fisher exact test in the analysis of the
variations in cosmetic appearance of wounds in both cohorts. Such a test is employed in
examining when the sample size is comparatively small (Dowson et al. 2006). The test is
useful in the examination of the non-random relationships between two categorical factors
like cosmetic appearance. The outcomes of Fisher exact test showed that cosmetic
appearance or wound scores in Dermabond cohort was higher significantly with a p-value
equals to 0.001 as opposed to those in the suture cohort.
After performing the postoperative examination, the pigmentation of skin of scar area stood
less visible in the Dermabond cohort, as opposed to suture cohort. In comparison, the
hyperpigmentation stood noticed in all patients’ wounds in subcuticular suture cohort. The
standalone surgeons as well as nurses were further included in this study, blindly to enable
the comparison between hyperpigmentation of scars in both suture and Derma bond cohorts
(Dowson et al. 2006). The inter-observer differences were never significant at a p-value
34
appearance was thus rated by these two authors using the visual analogue scale (Dowson et
al. 2006). There were statistical tests that revealed substantial differences between scores in
Dermabond cohort and in conventional subcuticular suture cohort with p-values less than
0.001. It is also imperative to recognize that none of the wounds of the patients in suture
cohort had a score of zero denoting optimal cosmetic satisfaction. Because the two standalone
surgeons scored the wounds using distinct scenarios, it is essential to probe the inter-observer
variations.
The outcomes of statistical tests demonstrated that there were no significant with p-value
equals to 0.045 inter-observer variations between two standalone surgeons. This indicated
that the outcome stood valid as well as reliable. At follow-up in week six, the cosmetic
appearance of wounds in the Dermabond group and suture cohort stood were compared by
use of Vancouver Scale. The authors used the Fisher exact test in the analysis of the
variations in cosmetic appearance of wounds in both cohorts. Such a test is employed in
examining when the sample size is comparatively small (Dowson et al. 2006). The test is
useful in the examination of the non-random relationships between two categorical factors
like cosmetic appearance. The outcomes of Fisher exact test showed that cosmetic
appearance or wound scores in Dermabond cohort was higher significantly with a p-value
equals to 0.001 as opposed to those in the suture cohort.
After performing the postoperative examination, the pigmentation of skin of scar area stood
less visible in the Dermabond cohort, as opposed to suture cohort. In comparison, the
hyperpigmentation stood noticed in all patients’ wounds in subcuticular suture cohort. The
standalone surgeons as well as nurses were further included in this study, blindly to enable
the comparison between hyperpigmentation of scars in both suture and Derma bond cohorts
(Dowson et al. 2006). The inter-observer differences were never significant at a p-value
34
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
equals to 0.130. This indicated that observations of nurses alongside surgeons tool not only
valid but also reliable. These studies have compared skin clip to subcuticular suture for
closure of wound following laparoscopic surgery but did not find any variations in cosmetic
of the wounds in both cohorts (Dowson et al. 2006). This indicates that either skin clip or
subcuticular sutures based on cosmetic appearance might be utilized after laparoscopic
surgery port sites. Moreover, (Liversey et al. 2009) probed the skin adhesive effectiveness
against the clips for skin closure after the laparoscopic surgery (Buchweitz et al. 2016). This
study regarded cosmetic appearance of scar of patients at 3 months following surgery. The
authors used visual analogue scale to assess cosmetic appearance of wounds. Significantly,
power computations were undertaken to determine the size of the sample. The use of power
calculations guarantees suitable sample size in the RCT (Buchweitz et al. 2016). Patients of
seventy-four were needed to detect a variation between the effectiveness of skin clips and
adhesives for closure after the surgery. A p-value of 0.05 alongside eighty percent power
stood observed in study.
The (Ridgway et al. 2007) study probed the skin clip and tissue glue for skin closure in
patients that needed collar line incision. The authors recruited 29 patients in the study using
random allocation to tissue glue with n=14 or skin clip of n=15. 14 of the patients had
hemithyroidectomies whereas six had sub-total thyroidectomies (Buchweitz et al. 2016). Five
patients had complete thyroidectomies while four patients were taken through
parathyroidectomies. The outcome of this study suggested that closure of wound utilizing
tissue glue took extended period as opposed to when clips were used with mean time closure
of 95 seconds in tissue glue cohort as opposed to twenty-eight seconds in clip cohort
(Buchweitz et al. 2016). The variations in closure between the two cohorts stood significant
with a p-value greater than 0.001. The outcome of the study indicated that cosmetic
appearance at 6 weeks after surgery stood comparable at the p-value equals to 0.898 in both
35
valid but also reliable. These studies have compared skin clip to subcuticular suture for
closure of wound following laparoscopic surgery but did not find any variations in cosmetic
of the wounds in both cohorts (Dowson et al. 2006). This indicates that either skin clip or
subcuticular sutures based on cosmetic appearance might be utilized after laparoscopic
surgery port sites. Moreover, (Liversey et al. 2009) probed the skin adhesive effectiveness
against the clips for skin closure after the laparoscopic surgery (Buchweitz et al. 2016). This
study regarded cosmetic appearance of scar of patients at 3 months following surgery. The
authors used visual analogue scale to assess cosmetic appearance of wounds. Significantly,
power computations were undertaken to determine the size of the sample. The use of power
calculations guarantees suitable sample size in the RCT (Buchweitz et al. 2016). Patients of
seventy-four were needed to detect a variation between the effectiveness of skin clips and
adhesives for closure after the surgery. A p-value of 0.05 alongside eighty percent power
stood observed in study.
The (Ridgway et al. 2007) study probed the skin clip and tissue glue for skin closure in
patients that needed collar line incision. The authors recruited 29 patients in the study using
random allocation to tissue glue with n=14 or skin clip of n=15. 14 of the patients had
hemithyroidectomies whereas six had sub-total thyroidectomies (Buchweitz et al. 2016). Five
patients had complete thyroidectomies while four patients were taken through
parathyroidectomies. The outcome of this study suggested that closure of wound utilizing
tissue glue took extended period as opposed to when clips were used with mean time closure
of 95 seconds in tissue glue cohort as opposed to twenty-eight seconds in clip cohort
(Buchweitz et al. 2016). The variations in closure between the two cohorts stood significant
with a p-value greater than 0.001. The outcome of the study indicated that cosmetic
appearance at 6 weeks after surgery stood comparable at the p-value equals to 0.898 in both
35
groups. The patient indicated levels of satisfaction at the appearance of their wound that was
identical in each group at the mean of 1.70 in tissue glue cohort and 1.80 in click cohort. The
standalone assessment of appearance of the wound demonstrated that mean cosmetics scores
in tissue glue cohort was 1.140 and click cohort with mean of 1.90 were never significantly
different with p-value of 0.365 (Buchweitz et al. 2016). The mean scores in tissue glue cohort
stood at 2.60 against 2.3 in clip cohort following the rating of appearance of wounds by
surgeons. The variations were never significant a p-value of 0.898. This study clearly
indicates that wound evaluation methods presented and outcome responded to the aims and
objectives of the study. The study conducted by (Gray 2009) stress that the objectives and
aims must be stated clearly to minimize the study ambiguity.
Patient satisfaction metric can also be used to compare the methods of wound closure. For
instance the study conducted by (Krishnamoorthy et al 2009) included patient satisfaction
amongst the health results being measured. This study compared the Dermabond
effectiveness as topical skin adhesive, with the traditional sutures for the closure of surgical
wound. A total of 106 patients that underwent CABG, stood included as well as randomized
to skin glue of n=53 alongside subcuticular sutures of n=53 cohorts after the harvesting of the
saphenous vein. There major outcomes measured in the research. Cosmetic appearance,
wound closure time as well as complications alongside patient satisfaction.
Krishnamoorthy study demonstrated no significant variations between two cohorts at
discharge based on the satisfaction of the patient with a p-value of greater than 0.990,
however at the 6-week follow-up; satisfaction of patients was significantly higher than the
suture cohort. Such a level of satisfaction could be attached to shorter duration of healing of
wound following the utilization of tissue adhesive alongside optimal cosmetic purpose. It was
also noted that the color of the scar closely matched skin color of patients in tissue adhesive
cohort whereas visibility o scar was decreased (Buchweitz et al. 2016). Nevertheless, the
36
identical in each group at the mean of 1.70 in tissue glue cohort and 1.80 in click cohort. The
standalone assessment of appearance of the wound demonstrated that mean cosmetics scores
in tissue glue cohort was 1.140 and click cohort with mean of 1.90 were never significantly
different with p-value of 0.365 (Buchweitz et al. 2016). The mean scores in tissue glue cohort
stood at 2.60 against 2.3 in clip cohort following the rating of appearance of wounds by
surgeons. The variations were never significant a p-value of 0.898. This study clearly
indicates that wound evaluation methods presented and outcome responded to the aims and
objectives of the study. The study conducted by (Gray 2009) stress that the objectives and
aims must be stated clearly to minimize the study ambiguity.
Patient satisfaction metric can also be used to compare the methods of wound closure. For
instance the study conducted by (Krishnamoorthy et al 2009) included patient satisfaction
amongst the health results being measured. This study compared the Dermabond
effectiveness as topical skin adhesive, with the traditional sutures for the closure of surgical
wound. A total of 106 patients that underwent CABG, stood included as well as randomized
to skin glue of n=53 alongside subcuticular sutures of n=53 cohorts after the harvesting of the
saphenous vein. There major outcomes measured in the research. Cosmetic appearance,
wound closure time as well as complications alongside patient satisfaction.
Krishnamoorthy study demonstrated no significant variations between two cohorts at
discharge based on the satisfaction of the patient with a p-value of greater than 0.990,
however at the 6-week follow-up; satisfaction of patients was significantly higher than the
suture cohort. Such a level of satisfaction could be attached to shorter duration of healing of
wound following the utilization of tissue adhesive alongside optimal cosmetic purpose. It was
also noted that the color of the scar closely matched skin color of patients in tissue adhesive
cohort whereas visibility o scar was decreased (Buchweitz et al. 2016). Nevertheless, the
36
satisfaction of the patient with scar size never differed significantly at a p-value of 0.067
between the two cohorts. It is worth noting that Dermabond has always been utilized for
different kinds of surgery, like pediatric surgery alongside neck surgery because it was easy
to use. (Krishnamoorthy et al 2009) was among the first studies to probe the cosmetic
satisfaction of the client, complication of wound and closure time of the wound after the
utilization of conventional subcuticular suture group.
CHAPTER 6: CONCLUSION
The most ultimate objective of surgical wound closure is to ensure that the patient scar is
cosmetically acceptable, functional and infection free. There are various ways of skin closure
methods as discussed within the content; however, the effectiveness of each wound closure
method depends on the kind of surgical operation performed on the patient (Al-Mubarak and
Al-Haddab 2013). The study reveals that use of tissue adhesive or skin closure by glue for
patients laparoscopic port surgery results into a quick wound healing compared to clips as
well as surgical suture methods. There were a lot of benefits wound closure by skin glue in
the study compared to clips and sutures.
Use of glue for skin closure proved to be taking minimum and time and less technically
challenging as clips and suture. The study also indicted that skin closure using tissues
adhesive is simple and easy to re-approximate, cost effective as well as rapid. Skin closure
using glue is increasingly being used as in the study results compared to clips and sutures
since it seals laparoscopic surgical wounds immediately reducing infection risks (Aveyard
2014). Laparoscopic surgeries take longer time compared to other open surgeries and this
makes various surgeons and nurses to increasingly use tissues adhesive wound closure which
reduces operating room time. Thus, the content of this current review recommends skin
closure by glue for patients undergoing laparoscopic surgery based on its benefits.
37
between the two cohorts. It is worth noting that Dermabond has always been utilized for
different kinds of surgery, like pediatric surgery alongside neck surgery because it was easy
to use. (Krishnamoorthy et al 2009) was among the first studies to probe the cosmetic
satisfaction of the client, complication of wound and closure time of the wound after the
utilization of conventional subcuticular suture group.
CHAPTER 6: CONCLUSION
The most ultimate objective of surgical wound closure is to ensure that the patient scar is
cosmetically acceptable, functional and infection free. There are various ways of skin closure
methods as discussed within the content; however, the effectiveness of each wound closure
method depends on the kind of surgical operation performed on the patient (Al-Mubarak and
Al-Haddab 2013). The study reveals that use of tissue adhesive or skin closure by glue for
patients laparoscopic port surgery results into a quick wound healing compared to clips as
well as surgical suture methods. There were a lot of benefits wound closure by skin glue in
the study compared to clips and sutures.
Use of glue for skin closure proved to be taking minimum and time and less technically
challenging as clips and suture. The study also indicted that skin closure using tissues
adhesive is simple and easy to re-approximate, cost effective as well as rapid. Skin closure
using glue is increasingly being used as in the study results compared to clips and sutures
since it seals laparoscopic surgical wounds immediately reducing infection risks (Aveyard
2014). Laparoscopic surgeries take longer time compared to other open surgeries and this
makes various surgeons and nurses to increasingly use tissues adhesive wound closure which
reduces operating room time. Thus, the content of this current review recommends skin
closure by glue for patients undergoing laparoscopic surgery based on its benefits.
37
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
As evident within the content of the current study review, laparoscopic wound closure using
clips and sutures takes a longer time compared to tissues adhesion method (Buchweitz et al.
2016). Increased time during surgical operations may account for increased rate of wound
infection risks as well as complications with the use of other closure methods such as clips
and sutures in laparoscopic surgeries. However, both clips and sutures proved to be easy to
use and cost effective even though take the same time for patients undergoing hip surgery
(Basha, Rochon, and Quiñones, et al 2010). In addition, both clips and suture wound closure
methods also shown to us less skins compare to tissues adhesive which costs as high as four
times the cost of sutures in caesarean surgery. However patients undergoing caesarean
delivery show high satisfaction rate when treated using tissues adhesive method (Buchweitz
et al. 2016). According to the current review, skin closure by glue is crucial and
recommended for patients undergoing laparoscopic and caesarean based time and minimum
wound infections but not recommended for patients with financial constrains based on its
high cost (Beam 2008). Clips and sutures are cost effective and affordable thus different to
tissue adhesive which is charged so high as a result of the reduced risks of infections.
Apart from operating time and minimal infection risks involves with tissue adhesive wound
closer method, the current review also shows advantages of skin closure by glue in relation to
patients satisfaction. As seen within the content of the review, skin closure by resulted into
high patients’ satisfaction rate for patients who underwent laparoscopic surgeries (Brown et
al. 2009). However, almost similar satisfaction response was evident for caesarean patients
who undergone wound closure by use of clips and sutures. However, tissue adhesive wound
closure method approved to be more satisfying when it comes to laparoscopic surgeries
compared to clip and sutures (Quinn, Coran and Hirsch 2009). The benefits of skin adhesive
resulted in many patients’ acceptance and satisfaction. The current study review found that
38
clips and sutures takes a longer time compared to tissues adhesion method (Buchweitz et al.
2016). Increased time during surgical operations may account for increased rate of wound
infection risks as well as complications with the use of other closure methods such as clips
and sutures in laparoscopic surgeries. However, both clips and sutures proved to be easy to
use and cost effective even though take the same time for patients undergoing hip surgery
(Basha, Rochon, and Quiñones, et al 2010). In addition, both clips and suture wound closure
methods also shown to us less skins compare to tissues adhesive which costs as high as four
times the cost of sutures in caesarean surgery. However patients undergoing caesarean
delivery show high satisfaction rate when treated using tissues adhesive method (Buchweitz
et al. 2016). According to the current review, skin closure by glue is crucial and
recommended for patients undergoing laparoscopic and caesarean based time and minimum
wound infections but not recommended for patients with financial constrains based on its
high cost (Beam 2008). Clips and sutures are cost effective and affordable thus different to
tissue adhesive which is charged so high as a result of the reduced risks of infections.
Apart from operating time and minimal infection risks involves with tissue adhesive wound
closer method, the current review also shows advantages of skin closure by glue in relation to
patients satisfaction. As seen within the content of the review, skin closure by resulted into
high patients’ satisfaction rate for patients who underwent laparoscopic surgeries (Brown et
al. 2009). However, almost similar satisfaction response was evident for caesarean patients
who undergone wound closure by use of clips and sutures. However, tissue adhesive wound
closure method approved to be more satisfying when it comes to laparoscopic surgeries
compared to clip and sutures (Quinn, Coran and Hirsch 2009). The benefits of skin adhesive
resulted in many patients’ acceptance and satisfaction. The current study review found that
38
high patient acceptance and satisfaction comes and increases when laparoscopic patients heal
faster.
The current review findings further suggest that patient’s satisfaction rate increased as a
result of optimal cosmetic appearance after surgery and working scars. In addition, skin by
glue resulted into optimal cosmetic wound appearance compared to other skin tissue adhesive
method of wound closure (Charters 2000). According to cosmetic appearance results, it
concluded be concluded that tissue adhesive wound closure is better than clips and sutures for
patients undergoing laparoscopic surgeries. Hence, tissue adhesive wound closure method is
suggested by this review the most recommended method of wound closer for patients
undergoing laparoscopic surgeries.
Moreover, considering the general benefits of the three closure methods, the current review
suggests that tissues adhesive can be used by patients undergoing various types of surgeries
laparoscopic surgeries, caesarean delivery and coronary artery bypass grafting (CABG)
(Buchweitz et al. 2016). In addition, previous review studies show that, even though there is a
closer rate of patient’s satisfaction with regards to hip replacements surgeries, patients’
satisfaction is the same for patients undergoing complete hip replacement surgeries when
surgeons use either surgical clips or skin closure by glue (Carbajo 2009). In relation to
similarities when it comes to adhesive and clips wound closure methods for patients
undergoing hip replacement, the study suggests that medical doctors can advise patients on
either of the methods. However, the findings of the study show that tissue adhesive wound
closure method is the most preferable method for patients undergoing laparoscopic surgeries
based on its benefits. Health practitioners should therefore advice patients undergoing
laparoscopic surgery to consider tissue adhesive instead of clips and sutures.
Finally, literature reviews as well as previous studies show that use of adhesive method for
patients undergoing laparoscopic surgery, leads to quick healing and faster wound closure
39
faster.
The current review findings further suggest that patient’s satisfaction rate increased as a
result of optimal cosmetic appearance after surgery and working scars. In addition, skin by
glue resulted into optimal cosmetic wound appearance compared to other skin tissue adhesive
method of wound closure (Charters 2000). According to cosmetic appearance results, it
concluded be concluded that tissue adhesive wound closure is better than clips and sutures for
patients undergoing laparoscopic surgeries. Hence, tissue adhesive wound closure method is
suggested by this review the most recommended method of wound closer for patients
undergoing laparoscopic surgeries.
Moreover, considering the general benefits of the three closure methods, the current review
suggests that tissues adhesive can be used by patients undergoing various types of surgeries
laparoscopic surgeries, caesarean delivery and coronary artery bypass grafting (CABG)
(Buchweitz et al. 2016). In addition, previous review studies show that, even though there is a
closer rate of patient’s satisfaction with regards to hip replacements surgeries, patients’
satisfaction is the same for patients undergoing complete hip replacement surgeries when
surgeons use either surgical clips or skin closure by glue (Carbajo 2009). In relation to
similarities when it comes to adhesive and clips wound closure methods for patients
undergoing hip replacement, the study suggests that medical doctors can advise patients on
either of the methods. However, the findings of the study show that tissue adhesive wound
closure method is the most preferable method for patients undergoing laparoscopic surgeries
based on its benefits. Health practitioners should therefore advice patients undergoing
laparoscopic surgery to consider tissue adhesive instead of clips and sutures.
Finally, literature reviews as well as previous studies show that use of adhesive method for
patients undergoing laparoscopic surgery, leads to quick healing and faster wound closure
39
which also results into a working scar, optimal cosmetic wound appearance, minimum wound
infection risk and patient satisfaction (Chow, Marshall, and Zacharakis, et al 2010). The
tissue adhesive method of skin closure can be suggested for patients undergoing various types
of surgeries like caesarean, CABGs and hip replacement, however, this method is method is
most suggested for patients undertaking laparoscopic port surgeries (Buchweitz et al. 2016).
Tissue adhesive has various benefits which will make it more accepted by majority of
patients, surgical doctors and nurses (Antoniou et al. 2016). Although tissue adhesive wound
closure method has various benefits over clip closure method and skin sutures, this method is
not for very surgical wound closure. Tissue adhesive is more expensive compared to clips
and skin sutures thus not affordable for every patient (Chow, Marshall, Zacharakis, Paraskeva
and Purkayastha 2010). This review therefore suggests that the cost of skin closer by glue
should be reviewed as patents’ satisfaction for both methods are almost similar. The
effectiveness of surgical wound closure methods vary in relation to type of surgery
undertaken by a patient. However, skin closure by glue of tissue adhesive remains the most
appropriate wound closure method for patients undertaking laparoscopic surgery.
In summary, tissue adhesive results into optimal wound appearance, minimal wound
infection risks and high patient satisfaction. Even though, tissue adhesive wound closure
method has several benefits for patients undergoing laparoscopic surgery, clips and skin
sutures have also proved to be effective for patients undertaking other types of surgeries
(Jones, Samy, and Boom et al 2017). This current study suggests and recommends for a
randomized controlled trial for future studies in order to examine the benefits of the three
surgical wound closure methods. This will ascertain the benefits of clips closure method,
tissue adhesive wound closer method and skin sutures in relation to surgical patients’
satisfaction, cosmetic wound appearance and wound healing period (Coughlan, Cronin and
Ryan 2007). Lastly, the study review recommends for future primary studies or systematic
40
infection risk and patient satisfaction (Chow, Marshall, and Zacharakis, et al 2010). The
tissue adhesive method of skin closure can be suggested for patients undergoing various types
of surgeries like caesarean, CABGs and hip replacement, however, this method is method is
most suggested for patients undertaking laparoscopic port surgeries (Buchweitz et al. 2016).
Tissue adhesive has various benefits which will make it more accepted by majority of
patients, surgical doctors and nurses (Antoniou et al. 2016). Although tissue adhesive wound
closure method has various benefits over clip closure method and skin sutures, this method is
not for very surgical wound closure. Tissue adhesive is more expensive compared to clips
and skin sutures thus not affordable for every patient (Chow, Marshall, Zacharakis, Paraskeva
and Purkayastha 2010). This review therefore suggests that the cost of skin closer by glue
should be reviewed as patents’ satisfaction for both methods are almost similar. The
effectiveness of surgical wound closure methods vary in relation to type of surgery
undertaken by a patient. However, skin closure by glue of tissue adhesive remains the most
appropriate wound closure method for patients undertaking laparoscopic surgery.
In summary, tissue adhesive results into optimal wound appearance, minimal wound
infection risks and high patient satisfaction. Even though, tissue adhesive wound closure
method has several benefits for patients undergoing laparoscopic surgery, clips and skin
sutures have also proved to be effective for patients undertaking other types of surgeries
(Jones, Samy, and Boom et al 2017). This current study suggests and recommends for a
randomized controlled trial for future studies in order to examine the benefits of the three
surgical wound closure methods. This will ascertain the benefits of clips closure method,
tissue adhesive wound closer method and skin sutures in relation to surgical patients’
satisfaction, cosmetic wound appearance and wound healing period (Coughlan, Cronin and
Ryan 2007). Lastly, the study review recommends for future primary studies or systematic
40
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
study reviews should be performed in order to look into healthcare costs of tissue adhesive as
a method of wound closure.
REFERENCES
Al-Mubarak, L. and Al-Haddab, M., 2013. Cutaneous wound closure materials: an overview
and update. Journal of cutaneous and aesthetic surgery, 6(4), p.178.
Antoniou, S.A., Köhler, G., Antoniou, G.A., Muysoms, F.E., Pointner, R. and Granderath,
F.A., 2016. Meta-analysis of randomized trials comparing nonpenetrating vs mechanical
mesh fixation in laparoscopic inguinal hernia repair. The American Journal of
Surgery, 211(1), pp.239-249.
Aveyard, H. 2014. Doing a literature review in health and social care: a practical guide. 3rd
ed. Maidenhead: McGraw Hill/Open University Press/.
Aveyard, H., 2014. Doing a literature review in health and social care: A practical guide.
McGraw-Hill Education (UK).
Barto, W., 2003. Randomized study of the effectiveness of closing laparoscopic trocar
wounds with octylcyanoacrylate, adhesive paper tape or poliglecaprone (Br J Surg 2002; 89:
1370–1375). British journal of surgery, 90(3), pp.369-369.
Basha, S.L., Rochon, M.L., Quiñones, J.N., Coassolo, K.M., Rust, O.A., and Smulian, J.C.,
2010. The randomized controlled trial of wound complication rates of subcuticular suture vs.
staples for skin closure at cesarean delivery. American Journal of Obstetrics &
Gynecology, 203(3), pp.285-e1.
Beam, J.W., 2008. Tissue adhesives for simple traumatic lacerations. Journal of Athletic
Training, 43(2), pp.222-224.
41
a method of wound closure.
REFERENCES
Al-Mubarak, L. and Al-Haddab, M., 2013. Cutaneous wound closure materials: an overview
and update. Journal of cutaneous and aesthetic surgery, 6(4), p.178.
Antoniou, S.A., Köhler, G., Antoniou, G.A., Muysoms, F.E., Pointner, R. and Granderath,
F.A., 2016. Meta-analysis of randomized trials comparing nonpenetrating vs mechanical
mesh fixation in laparoscopic inguinal hernia repair. The American Journal of
Surgery, 211(1), pp.239-249.
Aveyard, H. 2014. Doing a literature review in health and social care: a practical guide. 3rd
ed. Maidenhead: McGraw Hill/Open University Press/.
Aveyard, H., 2014. Doing a literature review in health and social care: A practical guide.
McGraw-Hill Education (UK).
Barto, W., 2003. Randomized study of the effectiveness of closing laparoscopic trocar
wounds with octylcyanoacrylate, adhesive paper tape or poliglecaprone (Br J Surg 2002; 89:
1370–1375). British journal of surgery, 90(3), pp.369-369.
Basha, S.L., Rochon, M.L., Quiñones, J.N., Coassolo, K.M., Rust, O.A., and Smulian, J.C.,
2010. The randomized controlled trial of wound complication rates of subcuticular suture vs.
staples for skin closure at cesarean delivery. American Journal of Obstetrics &
Gynecology, 203(3), pp.285-e1.
Beam, J.W., 2008. Tissue adhesives for simple traumatic lacerations. Journal of Athletic
Training, 43(2), pp.222-224.
41
Bisgaard, T., Klarskov, B., Kehlet, H. and Rosenberg, J., 2003. Preoperative dexamethasone
improves surgical outcome after laparoscopic cholecystectomy: a randomized double-blind
placebo-controlled trial. Annals of surgery, 238(5), p.651.
Blaxter, L. et al 2010. How to Research. 4th ed. Maidenhead: Open University Press.
Bou, H., Suzuki, H., Maejima, K., Uchida, E. and Tokunaga, A., 2015. Prevention of
incisional surgical site infection using a subcuticular absorbable suture in elective surgery for
gastrointestinal cancer. International surgery, 100(6), pp.999-1003.
Brown, J.K., Campbell, B.T., Drongowski, R.A., Alderman, A.K., Geiger, J.D., Teitelbaum,
D.H., Quinn, J., Coran, A.G. and Hirschl, R.B., 2009. A prospective, randomized comparison
of skin adhesive and subcuticular suture for closure of pediatric hernia incisions: cost and
cosmetic considerations. Journal of pediatric surgery, 44(7), pp.1418-1422.
Buchweitz, O., Frye, C., Moeller, C.P., Nugent, W., Krueger, E., Nugent, A., Biel, P. and
Juergens, S., 2016. Cosmetic outcome of skin adhesives versus transcutaneous sutures in
laparoscopic port-site wounds: a prospective randomized controlled trial. Surgical
endoscopy, 30(6), pp.2326-2331.
Carbajo, M.A., Del Olmo, J.M., Blanco, J.I., De la Cuesta, C., Toledano, M., Martin, F.,
Vaquero, C. and Inglada, L., 2009. Laparoscopic treatment vs open surgery in the solution of
major incisional and abdominal wall hernias with mesh. Surgical endoscopy, 13(3), pp.250-
252.
Charters, A., 2000. Wound glue: a comparative study of tissue adhesives. Accident and
emergency nursing, 8(4), pp.223-227.
Chen, K., Klapper, A., Voige, H. and Del Priore, G., 2008. A randomized controlled study
comparing two standardized closure methods of laparoscopic port sites. Fertility and
Sterility, 90, p.S40.
42
improves surgical outcome after laparoscopic cholecystectomy: a randomized double-blind
placebo-controlled trial. Annals of surgery, 238(5), p.651.
Blaxter, L. et al 2010. How to Research. 4th ed. Maidenhead: Open University Press.
Bou, H., Suzuki, H., Maejima, K., Uchida, E. and Tokunaga, A., 2015. Prevention of
incisional surgical site infection using a subcuticular absorbable suture in elective surgery for
gastrointestinal cancer. International surgery, 100(6), pp.999-1003.
Brown, J.K., Campbell, B.T., Drongowski, R.A., Alderman, A.K., Geiger, J.D., Teitelbaum,
D.H., Quinn, J., Coran, A.G. and Hirschl, R.B., 2009. A prospective, randomized comparison
of skin adhesive and subcuticular suture for closure of pediatric hernia incisions: cost and
cosmetic considerations. Journal of pediatric surgery, 44(7), pp.1418-1422.
Buchweitz, O., Frye, C., Moeller, C.P., Nugent, W., Krueger, E., Nugent, A., Biel, P. and
Juergens, S., 2016. Cosmetic outcome of skin adhesives versus transcutaneous sutures in
laparoscopic port-site wounds: a prospective randomized controlled trial. Surgical
endoscopy, 30(6), pp.2326-2331.
Carbajo, M.A., Del Olmo, J.M., Blanco, J.I., De la Cuesta, C., Toledano, M., Martin, F.,
Vaquero, C. and Inglada, L., 2009. Laparoscopic treatment vs open surgery in the solution of
major incisional and abdominal wall hernias with mesh. Surgical endoscopy, 13(3), pp.250-
252.
Charters, A., 2000. Wound glue: a comparative study of tissue adhesives. Accident and
emergency nursing, 8(4), pp.223-227.
Chen, K., Klapper, A., Voige, H. and Del Priore, G., 2008. A randomized controlled study
comparing two standardized closure methods of laparoscopic port sites. Fertility and
Sterility, 90, p.S40.
42
Chen, K., Klapper, A.S., Voige, H. and Del Priore, G., 2010. A randomized, controlled study
comparing two standardized closure methods of laparoscopic port sites. JSLS: Journal of the
Society of Laparoendoscopic Surgeons, 14(3), p.391.
Chibbaro, S. and Tacconi, L., 2009. Use of skin glue versus traditional wound closure
methods in brain surgery: A prospective, randomized, controlled study. Journal of Clinical
Neuroscience, 16(4), pp.535-539.
Chibbaro, S. and Tacconi, L., 2009. Use of skin glue versus traditional wound closure
methods in brain surgery: A prospective, randomized, controlled study. Journal of Clinical
Neuroscience, 16(4), pp.535-539.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Purkayastha, S., Aziz, O. and Paraskeva, P., 2010. Single-incision laparoscopic
surgery for cholecystectomy: an evolving technique. Surgical endoscopy, 24(3), pp.709-714.
Chow, A., Purkayastha, S., Aziz, O. and Paraskeva, P., 2010. Single-incision laparoscopic
surgery for cholecystectomy: an evolving technique. Surgical endoscopy, 24(3), pp.709-714.
43
comparing two standardized closure methods of laparoscopic port sites. JSLS: Journal of the
Society of Laparoendoscopic Surgeons, 14(3), p.391.
Chibbaro, S. and Tacconi, L., 2009. Use of skin glue versus traditional wound closure
methods in brain surgery: A prospective, randomized, controlled study. Journal of Clinical
Neuroscience, 16(4), pp.535-539.
Chibbaro, S. and Tacconi, L., 2009. Use of skin glue versus traditional wound closure
methods in brain surgery: A prospective, randomized, controlled study. Journal of Clinical
Neuroscience, 16(4), pp.535-539.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Marshall, H., Zacharakis, E., Paraskeva, P. and Purkayastha, S., 2010. Use of
tissue glue for surgical incision closure: a systematic review and meta-analysis of randomized
controlled trials. Journal of the American College of Surgeons, 211(1), pp.114-125.
Chow, A., Purkayastha, S., Aziz, O. and Paraskeva, P., 2010. Single-incision laparoscopic
surgery for cholecystectomy: an evolving technique. Surgical endoscopy, 24(3), pp.709-714.
Chow, A., Purkayastha, S., Aziz, O. and Paraskeva, P., 2010. Single-incision laparoscopic
surgery for cholecystectomy: an evolving technique. Surgical endoscopy, 24(3), pp.709-714.
43
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Conolly, W.B., Hunt, T.K., Zederfeldt, B., Cafferata, H.T. and Dunphy, J.E., 1969. Clinical
comparison of surgical wounds closed by suture and adhesive tapes. The American Journal of
Surgery, 117(3), pp.318-322.
Cooper, J.M. and Paige, K.T., 2006. Primary and revision cleft lip repairs using octyl-2-
cyanoacrylate. Journal of Craniofacial Surgery, 17(2), pp.340-343.
Coughlan, M., Cronin, P. and Ryan, F., 2007. Step-by-step guide to critiquing research. Part
1: quantitative research. British journal of nursing, 16(11), pp.658-663.
Crochet, P., Aggarwal, R., Knight, S., Berdah, S., Boubli, L. and Agostini, A., 2017.
Development of an evidence-based training program for laparoscopic hysterectomy on a
virtual reality simulator. Surgical endoscopy, 31(6), pp.2474-2482.
Cross, K.J., Teo, E.H., Wong, S.L., Lambe, J.S., Rohde, C.H., Grant, R.T. and Ascherman,
J.A., 2009. The absorbable dermal staple device: A faster, more cost-effective method for
incisional closure. Plastic and reconstructive surgery, 124(1), pp.156-162.
Dawson, C. 2009. Introduction to Research Methods: a practical guide for anyone
undertaking a research project. 4th ed. Oxford: How to Books.
Dowson, C.C., Gilliam, A.D., Speake, W.J., Lobo, D.N. and Beckingham, I.J., 2006. A
prospective, randomized controlled trial comparing n-butyl cyanoacrylate tissue adhesive
(LiquiBand) with sutures for skin closure after laparoscopic general surgical
procedures. Surgical Laparoscopy Endoscopy & Percutaneous Techniques, 16(3), pp.146-
150.
Draaijers, L.J., Tempelman, F.R., Botman, Y.A., Tuinebreijer, W.E., Middelkoop, E., Kreis,
R.W. and van Zuijlen, P.P., 2004. The patient and observer scar assessment scale: a reliable
and feasible tool for scar evaluation. Plastic and reconstructive Surgery, 113(7), pp.1960-
1965.
44
comparison of surgical wounds closed by suture and adhesive tapes. The American Journal of
Surgery, 117(3), pp.318-322.
Cooper, J.M. and Paige, K.T., 2006. Primary and revision cleft lip repairs using octyl-2-
cyanoacrylate. Journal of Craniofacial Surgery, 17(2), pp.340-343.
Coughlan, M., Cronin, P. and Ryan, F., 2007. Step-by-step guide to critiquing research. Part
1: quantitative research. British journal of nursing, 16(11), pp.658-663.
Crochet, P., Aggarwal, R., Knight, S., Berdah, S., Boubli, L. and Agostini, A., 2017.
Development of an evidence-based training program for laparoscopic hysterectomy on a
virtual reality simulator. Surgical endoscopy, 31(6), pp.2474-2482.
Cross, K.J., Teo, E.H., Wong, S.L., Lambe, J.S., Rohde, C.H., Grant, R.T. and Ascherman,
J.A., 2009. The absorbable dermal staple device: A faster, more cost-effective method for
incisional closure. Plastic and reconstructive surgery, 124(1), pp.156-162.
Dawson, C. 2009. Introduction to Research Methods: a practical guide for anyone
undertaking a research project. 4th ed. Oxford: How to Books.
Dowson, C.C., Gilliam, A.D., Speake, W.J., Lobo, D.N. and Beckingham, I.J., 2006. A
prospective, randomized controlled trial comparing n-butyl cyanoacrylate tissue adhesive
(LiquiBand) with sutures for skin closure after laparoscopic general surgical
procedures. Surgical Laparoscopy Endoscopy & Percutaneous Techniques, 16(3), pp.146-
150.
Draaijers, L.J., Tempelman, F.R., Botman, Y.A., Tuinebreijer, W.E., Middelkoop, E., Kreis,
R.W. and van Zuijlen, P.P., 2004. The patient and observer scar assessment scale: a reliable
and feasible tool for scar evaluation. Plastic and reconstructive Surgery, 113(7), pp.1960-
1965.
44
Dumville, J.C., Coulthard, P., Worthington, H.V., Riley, P., Patel, N., Darcey, J., Esposito,
M., van der Elst, M. and van Waes, O.J., 2014. Tissue adhesives for closure of surgical
incisions. The Cochrane Library.
Ebersole, G., Choudhury, M., Ostapoff, R., Nentwick, B. and Stevenson, R.P., Covidien LP,
2018. Wound closure material. U.S. Patent 9,888,924.
Elashry, O.M., Nakada, S.Y., Wolf, J.J., Figenshau, R.S., McDougall, E.M. and Clayman,
R.V., 2016. Comparative clinical study of port-closure techniques following laparoscopic
surgery. Journal of the American College of Surgeons, 183(4), pp.335-344.
Ferdman, A., Kuo, J.W., Miller, D., Pinsky, V., Richards, W.D. and Swann, D., MEDCHEM
PRODUCTS Inc A Corp OF, 2012. Method and device for wound closure. U.S. Patent
5,149,331.
Garcia-Ruiz, A., Gagner, M., Miller, J.H., Steiner, C.P. and Hahn, J.F., 2008. Manual vs
robotically assisted laparoscopic surgery in the performance of basic manipulation and
suturing tasks. Archives of surgery, 133(9), pp.957-961.
Gennari, R., Rotmensz, N., Ballardini, B., Scevola, S., Perego, E., Zanini, V. and Costa, A.,
2004. A prospective, randomized, controlled clinical trial of tissue adhesive (2-
octylcyanoacrylate) versus standard wound closure in breast surgery. Surgery, 136(3),
pp.593-599.
Gohil, K.S., Lakhawala, S.A. and Patel, V.P., 2018. Current Surgical Patches and Novel
Wound Closure Techniques. drugs, 3, p.4.
Goto, S., Hida, K., Furukawa, T.A. and Sakai, Y., 2016. Subcuticular sutures for skin closure
in non‐obstetric surgery. The Cochrane Library.
Greco, M., Capretti, G., Beretta, L., Gemma, M., Pecorelli, N. and Braga, M., 2014.
Enhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled
trials. World journal of surgery, 38(6), pp.1531-1541.
45
M., van der Elst, M. and van Waes, O.J., 2014. Tissue adhesives for closure of surgical
incisions. The Cochrane Library.
Ebersole, G., Choudhury, M., Ostapoff, R., Nentwick, B. and Stevenson, R.P., Covidien LP,
2018. Wound closure material. U.S. Patent 9,888,924.
Elashry, O.M., Nakada, S.Y., Wolf, J.J., Figenshau, R.S., McDougall, E.M. and Clayman,
R.V., 2016. Comparative clinical study of port-closure techniques following laparoscopic
surgery. Journal of the American College of Surgeons, 183(4), pp.335-344.
Ferdman, A., Kuo, J.W., Miller, D., Pinsky, V., Richards, W.D. and Swann, D., MEDCHEM
PRODUCTS Inc A Corp OF, 2012. Method and device for wound closure. U.S. Patent
5,149,331.
Garcia-Ruiz, A., Gagner, M., Miller, J.H., Steiner, C.P. and Hahn, J.F., 2008. Manual vs
robotically assisted laparoscopic surgery in the performance of basic manipulation and
suturing tasks. Archives of surgery, 133(9), pp.957-961.
Gennari, R., Rotmensz, N., Ballardini, B., Scevola, S., Perego, E., Zanini, V. and Costa, A.,
2004. A prospective, randomized, controlled clinical trial of tissue adhesive (2-
octylcyanoacrylate) versus standard wound closure in breast surgery. Surgery, 136(3),
pp.593-599.
Gohil, K.S., Lakhawala, S.A. and Patel, V.P., 2018. Current Surgical Patches and Novel
Wound Closure Techniques. drugs, 3, p.4.
Goto, S., Hida, K., Furukawa, T.A. and Sakai, Y., 2016. Subcuticular sutures for skin closure
in non‐obstetric surgery. The Cochrane Library.
Greco, M., Capretti, G., Beretta, L., Gemma, M., Pecorelli, N. and Braga, M., 2014.
Enhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled
trials. World journal of surgery, 38(6), pp.1531-1541.
45
Green, D.T., Bolanos, H., Young, W.P., McGarry, R.A., Heaton, L.W. and Ratcliff, K.,
United States Surgical Corp, 2002. Apparatus and method for applying surgical clips in
laparoscopic or endoscopic procedures. U.S. Patent 5,100,420.
Harold, K.L., Pollinger, H., Matthews, B.D., Kercher, K.W., Sing, R.F. and Heniford, B.T.,
2003. Comparison of ultrasonic energy, bipolar thermal energy, and vascular clips for the
hemostasis of small-, medium-, and large-sized arteries. Surgical Endoscopy And Other
Interventional Techniques, 17(8), pp.1228-1230.
Hart, A.M., Duggal, C., Pinell-White, X. and Losken, A., 2017. A prospective randomized
trial of the efficacy of fibrin glue, triamcinolone acetonide, and quilting sutures in seroma
prevention after latissimus dorsi breast reconstruction. Plastic and reconstructive
surgery, 139(4), pp.854e-863e.
Ibrahim, M.I., Riad, A.A.M. and Ahmed, S.R., 2017. Skin Adhesive Tape versus Non-
Absorbable Sutures in Repair of Laparoscopic Incision. Egyptian Journal of Hospital
Medicine, 68(2).
Jones, C.D., Ho, W., Samy, M., Boom, S. and Lam, W.L., 2017. Comparison of glues,
sutures, and other commercially available methods of skin closure: A review of
literature. Medical Research Archives, 5(7).
Kane, E.D., Leduc, M., Schlosser, K., Parentela, N., Wilson, D. and Romanelli, J.R., 2018.
Comparison of peritoneal closure versus non-closure in laparoscopic trans-abdominal
preperitoneal inguinal hernia repair with coated mesh. Surgical endoscopy, 32(2), pp.627-
637.
Kaouk, J.H., Haber, G.P., Goel, R.K., Desai, M.M., Aron, M., Rackley, R.R., Moore, C. and
Gill, I.S., 2008. Single-port laparoscopic surgery in urology: initial
experience. Urology, 71(1), pp.3-6.
46
United States Surgical Corp, 2002. Apparatus and method for applying surgical clips in
laparoscopic or endoscopic procedures. U.S. Patent 5,100,420.
Harold, K.L., Pollinger, H., Matthews, B.D., Kercher, K.W., Sing, R.F. and Heniford, B.T.,
2003. Comparison of ultrasonic energy, bipolar thermal energy, and vascular clips for the
hemostasis of small-, medium-, and large-sized arteries. Surgical Endoscopy And Other
Interventional Techniques, 17(8), pp.1228-1230.
Hart, A.M., Duggal, C., Pinell-White, X. and Losken, A., 2017. A prospective randomized
trial of the efficacy of fibrin glue, triamcinolone acetonide, and quilting sutures in seroma
prevention after latissimus dorsi breast reconstruction. Plastic and reconstructive
surgery, 139(4), pp.854e-863e.
Ibrahim, M.I., Riad, A.A.M. and Ahmed, S.R., 2017. Skin Adhesive Tape versus Non-
Absorbable Sutures in Repair of Laparoscopic Incision. Egyptian Journal of Hospital
Medicine, 68(2).
Jones, C.D., Ho, W., Samy, M., Boom, S. and Lam, W.L., 2017. Comparison of glues,
sutures, and other commercially available methods of skin closure: A review of
literature. Medical Research Archives, 5(7).
Kane, E.D., Leduc, M., Schlosser, K., Parentela, N., Wilson, D. and Romanelli, J.R., 2018.
Comparison of peritoneal closure versus non-closure in laparoscopic trans-abdominal
preperitoneal inguinal hernia repair with coated mesh. Surgical endoscopy, 32(2), pp.627-
637.
Kaouk, J.H., Haber, G.P., Goel, R.K., Desai, M.M., Aron, M., Rackley, R.R., Moore, C. and
Gill, I.S., 2008. Single-port laparoscopic surgery in urology: initial
experience. Urology, 71(1), pp.3-6.
46
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Karounis, H., Gouin, S., Eisman, H., Chalut, D., Pelletier, H. and Williams, B., 2004. A
Randomized, Controlled Trial Comparing Long‐term Cosmetic Outcomes of Traumatic
Pediatric Lacerations Repaired with Absorbable Plain Gut versus Nonabsorbable Nylon
Sutures. Academic Emergency Medicine, 11(7), pp.730-735.
Knott, P.D., Zins, J.E., Banbury, J., Djohan, R., Yetman, R.J. and Papay, F., 2007. A
comparison of dermabond tissue adhesive and sutures in the primary repair of the congenital
cleft lip. Annals of plastic surgery, 58(2), pp.121-125.
Köhler, G., Mayer, F., Lechner, M. and Bittner, R., 2015. Small bowel obstruction after
TAPP repair caused by a self-anchoring barbed suture device for peritoneal closure: case
report and review of the literature. Hernia, 19(3), pp.389-394.
LaBagnara, J.J., 1995. A review of absorbable suture materials in head & neck surgery and
introduction of monocryl: a new absorbable suture. Ear, nose, & throat journal, 74(6),
pp.409-415.
Landman, J., Kerbl, K., Rehman, J., Andreoni, C., Humphrey, P.A., Collyer, W., Olweny, E.,
Sundaram, C. and Clayman, R.V., 2003. Evaluation of a vessel sealing system, bipolar
electrosurgery, harmonic scalpel, titanium clips, endoscopic gastrointestinal anastomosis
vascular staples and sutures for arterial and venous ligation in a porcine model. The Journal
of urology, 169(2), pp.697-700.
Liebmann, P., Vorstandlechner, V. and Radtke, C., 2018. A Prospective Randomized Trial of
the Efficacy of Fibrin Glue, Triamcinolone Acetonide, and Quilting Sutures in Seroma
Prevention after Latissimus Dorsi Breast Reconstruction. Plastic and reconstructive
surgery, 141(2), pp.310e-311e.
Lloris‐Carsí, J.M., Ballester‐Álvaro, J., Barrios, C., Zaragozá‐Fernández, C., González‐
Cuartero, C., Prieto‐Moure, B. and Cejalvo‐Lapeña, D., 2016. Randomized clinical trial of a
47
Randomized, Controlled Trial Comparing Long‐term Cosmetic Outcomes of Traumatic
Pediatric Lacerations Repaired with Absorbable Plain Gut versus Nonabsorbable Nylon
Sutures. Academic Emergency Medicine, 11(7), pp.730-735.
Knott, P.D., Zins, J.E., Banbury, J., Djohan, R., Yetman, R.J. and Papay, F., 2007. A
comparison of dermabond tissue adhesive and sutures in the primary repair of the congenital
cleft lip. Annals of plastic surgery, 58(2), pp.121-125.
Köhler, G., Mayer, F., Lechner, M. and Bittner, R., 2015. Small bowel obstruction after
TAPP repair caused by a self-anchoring barbed suture device for peritoneal closure: case
report and review of the literature. Hernia, 19(3), pp.389-394.
LaBagnara, J.J., 1995. A review of absorbable suture materials in head & neck surgery and
introduction of monocryl: a new absorbable suture. Ear, nose, & throat journal, 74(6),
pp.409-415.
Landman, J., Kerbl, K., Rehman, J., Andreoni, C., Humphrey, P.A., Collyer, W., Olweny, E.,
Sundaram, C. and Clayman, R.V., 2003. Evaluation of a vessel sealing system, bipolar
electrosurgery, harmonic scalpel, titanium clips, endoscopic gastrointestinal anastomosis
vascular staples and sutures for arterial and venous ligation in a porcine model. The Journal
of urology, 169(2), pp.697-700.
Liebmann, P., Vorstandlechner, V. and Radtke, C., 2018. A Prospective Randomized Trial of
the Efficacy of Fibrin Glue, Triamcinolone Acetonide, and Quilting Sutures in Seroma
Prevention after Latissimus Dorsi Breast Reconstruction. Plastic and reconstructive
surgery, 141(2), pp.310e-311e.
Lloris‐Carsí, J.M., Ballester‐Álvaro, J., Barrios, C., Zaragozá‐Fernández, C., González‐
Cuartero, C., Prieto‐Moure, B. and Cejalvo‐Lapeña, D., 2016. Randomized clinical trial of a
47
new cyanoacrylate flexible tissue adhesive (Adhflex) for repairing surgical wounds. Wound
Repair and Regeneration, 24(3), pp.568-580.
Maartense, S., Bemelman, W.A., Dunker, M.S., De Lint, C., Pierik, E.G.J.M., Busch, O.R.C.
and Gouma, D.J., 2002. Randomized study of the effectiveness of closing laparoscopic trocar
wounds with octylcyanoacrylate, adhesive papertape or poliglecaprone. British journal of
surgery, 89(11), pp.1370-1375.
Magdeburg, R. and Kaehler, G., 2016. Natural orifice transluminal endoscopic surgery in
humans: feasibility and safety of transgastric closure using the OTSC system. Surgical
endoscopy, 30(1), pp.73-77.
Maloney, J., Rogers, G.S. and Kapadia, M., 2013. Surgical corner: a prospective randomized
evaluation of cyanoacrylate glue devices in the closure of surgical wounds. Journal of drugs
in dermatology: JDD, 12(7), pp.810-814.
Mangano, A., Albertin, A. and LaColla, L., 2009. Use of 2-octyl-cyanoacrylate skin adhesive
(Dermabond) for wound closure following reduction mammaplasty: a prospective,
randomized intervention study.“Tips and tricks” to improve statistical analysis and
significance of results. Plastic and reconstructive surgery, 124(2), p.669.
Marcovich, R., Williams, A.L., Rubin, M.A. and Wolf, J.S., 2011. Comparison of 2-octyl
cyanoacrylate adhesive, fibrin glue, and suturing for wound closure in the porcine urinary
tract. Urology, 57(4), pp.806-810.
Matin, S.F., 2003. Prospective randomized trial of skin adhesive versus sutures for closure of
217 laparoscopic port-site incisions. Journal of the American College of Surgeons, 196(6),
pp.845-853.
Mayhew, P.D. and Brown, D.C., 2007. Comparison of three techniques for ovarian pedicle
hemostasis during laparoscopic‐assisted ovariohysterectomy. Veterinary Surgery, 36(6),
pp.541-547.
48
Repair and Regeneration, 24(3), pp.568-580.
Maartense, S., Bemelman, W.A., Dunker, M.S., De Lint, C., Pierik, E.G.J.M., Busch, O.R.C.
and Gouma, D.J., 2002. Randomized study of the effectiveness of closing laparoscopic trocar
wounds with octylcyanoacrylate, adhesive papertape or poliglecaprone. British journal of
surgery, 89(11), pp.1370-1375.
Magdeburg, R. and Kaehler, G., 2016. Natural orifice transluminal endoscopic surgery in
humans: feasibility and safety of transgastric closure using the OTSC system. Surgical
endoscopy, 30(1), pp.73-77.
Maloney, J., Rogers, G.S. and Kapadia, M., 2013. Surgical corner: a prospective randomized
evaluation of cyanoacrylate glue devices in the closure of surgical wounds. Journal of drugs
in dermatology: JDD, 12(7), pp.810-814.
Mangano, A., Albertin, A. and LaColla, L., 2009. Use of 2-octyl-cyanoacrylate skin adhesive
(Dermabond) for wound closure following reduction mammaplasty: a prospective,
randomized intervention study.“Tips and tricks” to improve statistical analysis and
significance of results. Plastic and reconstructive surgery, 124(2), p.669.
Marcovich, R., Williams, A.L., Rubin, M.A. and Wolf, J.S., 2011. Comparison of 2-octyl
cyanoacrylate adhesive, fibrin glue, and suturing for wound closure in the porcine urinary
tract. Urology, 57(4), pp.806-810.
Matin, S.F., 2003. Prospective randomized trial of skin adhesive versus sutures for closure of
217 laparoscopic port-site incisions. Journal of the American College of Surgeons, 196(6),
pp.845-853.
Mayhew, P.D. and Brown, D.C., 2007. Comparison of three techniques for ovarian pedicle
hemostasis during laparoscopic‐assisted ovariohysterectomy. Veterinary Surgery, 36(6),
pp.541-547.
48
McCallum, I.J., King, P.M. and Bruce, J., 2008. Healing by primary closure versus open
healing after surgery for pilonidal sinus: systematic review and meta-
analysis. bmj, 336(7649), pp.868-871.
McCallum, I.J., King, P.M. and Bruce, J., 2008. Healing by primary closure versus open
healing after surgery for pilonidal sinus: systematic review and meta-
analysis. bmj, 336(7649), pp.868-871.
Mueller, E.R., Kenton, K., Anger, J.T., Bresee, C. and Tarnay, C., 2016. Cosmetic
appearance of port-site scars 1 year after laparoscopic versus robotic sacrocolpopexy: a
supplementary study of the ACCESS Clinical Trial. Journal of minimally invasive
gynecology, 23(6), pp.917-921.
Nho, S.J., Helfet, D.L. and Rozbruch, S.R., 2006. Temporary intentional leg shortening and
deformation to facilitate wound closure using the Ilizarov/Taylor spatial frame. Journal of
orthopaedic trauma, 20(6), pp.419-424.
Nipshagen, M.D., Hage, J.J. and Beekman, W.H., 2008. Use of 2-octyl-cyanoacrylate skin
adhesive (Dermabond) for wound closure following reduction mammaplasty: a prospective,
randomized intervention study. Plastic and reconstructive surgery, 122(1), pp.10-18.
Norton, M.J. and Ischy, N.D., Axcess Instruments Inc, 2017. Apparatus and method for
minimally invasive surgery. U.S. Patent 9,820,771.
Parell, G.J. and Becker, G.D., 2003. Comparison of absorbable with nonabsorbable sutures in
closure of facial skin wounds. Archives of facial plastic surgery, 5(6), pp.488-490.
Park, S.Y., Kim, K.H., Yuk, J.S., Ji, H.Y. and Lee, J.H., 2015. Skin closure methods after
single port laparoscopic surgery: a randomized clinical trial. European Journal of Obstetrics
and Gynecology and Reproductive Biology, 189, pp.8-12.
Pham, C., Greenwood, J., Cleland, H., Woodruff, P. and Maddern, G., 2007. Bioengineered
skin substitutes for the management of burns: a systematic review. Burns, 33(8), pp.946-957.
49
healing after surgery for pilonidal sinus: systematic review and meta-
analysis. bmj, 336(7649), pp.868-871.
McCallum, I.J., King, P.M. and Bruce, J., 2008. Healing by primary closure versus open
healing after surgery for pilonidal sinus: systematic review and meta-
analysis. bmj, 336(7649), pp.868-871.
Mueller, E.R., Kenton, K., Anger, J.T., Bresee, C. and Tarnay, C., 2016. Cosmetic
appearance of port-site scars 1 year after laparoscopic versus robotic sacrocolpopexy: a
supplementary study of the ACCESS Clinical Trial. Journal of minimally invasive
gynecology, 23(6), pp.917-921.
Nho, S.J., Helfet, D.L. and Rozbruch, S.R., 2006. Temporary intentional leg shortening and
deformation to facilitate wound closure using the Ilizarov/Taylor spatial frame. Journal of
orthopaedic trauma, 20(6), pp.419-424.
Nipshagen, M.D., Hage, J.J. and Beekman, W.H., 2008. Use of 2-octyl-cyanoacrylate skin
adhesive (Dermabond) for wound closure following reduction mammaplasty: a prospective,
randomized intervention study. Plastic and reconstructive surgery, 122(1), pp.10-18.
Norton, M.J. and Ischy, N.D., Axcess Instruments Inc, 2017. Apparatus and method for
minimally invasive surgery. U.S. Patent 9,820,771.
Parell, G.J. and Becker, G.D., 2003. Comparison of absorbable with nonabsorbable sutures in
closure of facial skin wounds. Archives of facial plastic surgery, 5(6), pp.488-490.
Park, S.Y., Kim, K.H., Yuk, J.S., Ji, H.Y. and Lee, J.H., 2015. Skin closure methods after
single port laparoscopic surgery: a randomized clinical trial. European Journal of Obstetrics
and Gynecology and Reproductive Biology, 189, pp.8-12.
Pham, C., Greenwood, J., Cleland, H., Woodruff, P. and Maddern, G., 2007. Bioengineered
skin substitutes for the management of burns: a systematic review. Burns, 33(8), pp.946-957.
49
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Qureshi, A., Drew, P.J., Duthie, G.S., Roberts, A.C. and Monson, J.R., 2007. n-Butyl
cyanoacrylate adhesive for skin closure of abdominal wounds: preliminary results. Annals of
the Royal College of Surgeons of England, 79(6), p.414.
Ridgway, D.M., Mahmood, F., Moore, L., Bramley, D. and Moore, P.J., 2007. A blinded,
randomised, controlled trial of stapled versus tissue glue closure of neck surgery
incisions. The Annals of The Royal College of Surgeons of England, 89(3), pp.242-246.
Ritter, E.M. and Scott, D.J., 2007. Design of a proficiency-based skills training curriculum
for the fundamentals of laparoscopic surgery. Surgical innovation, 14(2), pp.107-112.
Robertson, B.L., 2017. Technological Improvements in Ligation and Suturing Techniques: A
Comparison in the Material Strength of Ligating Clips and Suturing Devices.
Rosser, J.C., Rosser, L.E. and Savalgi, R.S., 200 Kanner, G., Angiolink Corp, 2001. Wound
site management and wound closure device. U.S. Patent 6,322,580.7. Skill acquisition and
assessment for laparoscopic surgery. Archives of Surgery, 132(2), pp.200-204.
Ryan, F., Coughlan, M. and Cronin, P., 2007. Step-by-step guide to critiquing research. Part
2: Qualitative research. British journal of nursing, 16(12), pp.738-744.
Sarifakioglu, E. and Sarifakioglu, N., 2006. Dressing spray enhances the adhesive strength of
surgical dressing tapes. Indian Journal of Dermatology, Venereology, and Leprology, 72(5),
p.353.
Shetty, A.A., Kumar, V.S., Morgan-Hough, C., Georgeu, G.A., James, K.D. and Nicholl,
J.E., 2004. Comparing wound complication rates following closure of hip wounds with
metallic skin staples or subcuticular vicryl suture: a prospective randomised trial. Journal of
Orthopaedic Surgery, 12(2), pp.191-193.
Simhon, D., Gabay, I., Shpolyansky, G., Vasilyev, T., Nur, I., Meidler, R., Hatoum, O.A.,
Katzir, A., Hashmonai, M. and Kopelman, D., 2015. Temperature-controlled laser-soldering
50
cyanoacrylate adhesive for skin closure of abdominal wounds: preliminary results. Annals of
the Royal College of Surgeons of England, 79(6), p.414.
Ridgway, D.M., Mahmood, F., Moore, L., Bramley, D. and Moore, P.J., 2007. A blinded,
randomised, controlled trial of stapled versus tissue glue closure of neck surgery
incisions. The Annals of The Royal College of Surgeons of England, 89(3), pp.242-246.
Ritter, E.M. and Scott, D.J., 2007. Design of a proficiency-based skills training curriculum
for the fundamentals of laparoscopic surgery. Surgical innovation, 14(2), pp.107-112.
Robertson, B.L., 2017. Technological Improvements in Ligation and Suturing Techniques: A
Comparison in the Material Strength of Ligating Clips and Suturing Devices.
Rosser, J.C., Rosser, L.E. and Savalgi, R.S., 200 Kanner, G., Angiolink Corp, 2001. Wound
site management and wound closure device. U.S. Patent 6,322,580.7. Skill acquisition and
assessment for laparoscopic surgery. Archives of Surgery, 132(2), pp.200-204.
Ryan, F., Coughlan, M. and Cronin, P., 2007. Step-by-step guide to critiquing research. Part
2: Qualitative research. British journal of nursing, 16(12), pp.738-744.
Sarifakioglu, E. and Sarifakioglu, N., 2006. Dressing spray enhances the adhesive strength of
surgical dressing tapes. Indian Journal of Dermatology, Venereology, and Leprology, 72(5),
p.353.
Shetty, A.A., Kumar, V.S., Morgan-Hough, C., Georgeu, G.A., James, K.D. and Nicholl,
J.E., 2004. Comparing wound complication rates following closure of hip wounds with
metallic skin staples or subcuticular vicryl suture: a prospective randomised trial. Journal of
Orthopaedic Surgery, 12(2), pp.191-193.
Simhon, D., Gabay, I., Shpolyansky, G., Vasilyev, T., Nur, I., Meidler, R., Hatoum, O.A.,
Katzir, A., Hashmonai, M. and Kopelman, D., 2015. Temperature-controlled laser-soldering
50
system and its clinical application for bonding skin incisions. Journal of Biomedical
Optics, 20(12), p.128002.
Singer, A.J. and Thode, H.C., 2014. A review of the literature on octylcyanoacrylate tissue
adhesive. The American journal of surgery, 187(2), pp.238-248.
Singer, A.J., Hollander, J.E., Valentine, S.M., Turque, T.W., McCuskey, C.F. and Quinn,
J.V., 1998. Prospective, Randomized, Controlled Trial of Tissue Adhesive (2‐
Octylcyanoacrylate) vs Standard Wound Closure Techniques for Laceration
Repair. Academic Emergency Medicine, 5(2), pp.94-99.
Singer, A.J., Quinn, J.V. and Hollander, J.E., 2008. The cyanoacrylate topical skin
adhesives. The American journal of emergency medicine, 26(4), pp.490-496.
Siu, W.T., Leong, H.T., Law, B.K., Chau, C.H., Li, A.C., Fung, K.H., Tai, Y.P. and Li, M.K.,
2002. Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial. Annals of
surgery, 235(3), p.313.
Smulian, M.D. and John, C., 2010. Randomized Controlled Trial of Wound Complication
Rates of Subcuticular Suture vs Staples for Skin Closure at Cesarean Delivery.
Sung, G.T. and Gill, I.S., 2001. Robotic laparoscopic surgery: a comparison of the da Vinci
and Zeus systems. Urology, 58(6), pp.893-898.
Tacchino, R., Greco, F. and Matera, D., 2009. Single-incision laparoscopic cholecystectomy:
surgery without a visible scar. Surgical endoscopy, 23(4), pp.896-899.
Tajirian, A.L. and Goldberg, D.J., 2010. A review of sutures and other skin closure
materials. Journal of Cosmetic and Laser Therapy, 12(6), pp.296-302.
Testini, M., Lissidini, G., Poli, E., Gurrado, A., Lardo, D. and Piccinni, G., 2010. A single-
surgeon randomized trial comparing sutures, N-butyl-2-cyanoacrylate and human fibrin glue
for mesh fixation during primary inguinal hernia repair. Canadian Journal of Surgery, 53(3),
p.155.
51
Optics, 20(12), p.128002.
Singer, A.J. and Thode, H.C., 2014. A review of the literature on octylcyanoacrylate tissue
adhesive. The American journal of surgery, 187(2), pp.238-248.
Singer, A.J., Hollander, J.E., Valentine, S.M., Turque, T.W., McCuskey, C.F. and Quinn,
J.V., 1998. Prospective, Randomized, Controlled Trial of Tissue Adhesive (2‐
Octylcyanoacrylate) vs Standard Wound Closure Techniques for Laceration
Repair. Academic Emergency Medicine, 5(2), pp.94-99.
Singer, A.J., Quinn, J.V. and Hollander, J.E., 2008. The cyanoacrylate topical skin
adhesives. The American journal of emergency medicine, 26(4), pp.490-496.
Siu, W.T., Leong, H.T., Law, B.K., Chau, C.H., Li, A.C., Fung, K.H., Tai, Y.P. and Li, M.K.,
2002. Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial. Annals of
surgery, 235(3), p.313.
Smulian, M.D. and John, C., 2010. Randomized Controlled Trial of Wound Complication
Rates of Subcuticular Suture vs Staples for Skin Closure at Cesarean Delivery.
Sung, G.T. and Gill, I.S., 2001. Robotic laparoscopic surgery: a comparison of the da Vinci
and Zeus systems. Urology, 58(6), pp.893-898.
Tacchino, R., Greco, F. and Matera, D., 2009. Single-incision laparoscopic cholecystectomy:
surgery without a visible scar. Surgical endoscopy, 23(4), pp.896-899.
Tajirian, A.L. and Goldberg, D.J., 2010. A review of sutures and other skin closure
materials. Journal of Cosmetic and Laser Therapy, 12(6), pp.296-302.
Testini, M., Lissidini, G., Poli, E., Gurrado, A., Lardo, D. and Piccinni, G., 2010. A single-
surgeon randomized trial comparing sutures, N-butyl-2-cyanoacrylate and human fibrin glue
for mesh fixation during primary inguinal hernia repair. Canadian Journal of Surgery, 53(3),
p.155.
51
Toriumi, D.M., O'grady, K., Desai, D. and Bagal, A., 1998. Use of octyl-2-cyanoacrylate for
skin closure in facial plastic surgery. Plastic and reconstructive surgery, 102(6), pp.2209-
2219.
Umranikar, S.A., Ubee, S.S., Selvan, M. and Cooke, P., 2017. Barbed suture tissue closure
device in urological surgery–a comprehensive review. Journal of Clinical Urology, 10(5),
pp.476-484.
Weiland, D.E., Bay, R.C. and Del Sordi, S., 1998. Choosing the best abdominal closure by
meta-analysis. The American journal of surgery, 176(6), pp.666-670.
Wolf, J.S., Tchetgen, M.B. and Merion, R.M., 1998. Hand-assisted laparoscopic live donor
nephrectomy. Urology, 52(5), pp.885-887.
Wolf, S.J., Soble, J.J., Nakada, S.Y., Rayala, H.J., Humphrey, P.A., Clayman, R.V. and
Poppas, D.P., 1997. Comparison of fibrin glue, laser weld, and mechanical suturing device
for the laparoscopic closure of ureterotomy in a porcine model. The Journal of
urology, 157(4), pp.1487-1492.
Wong, S.L., Cross, K.J., Teo, E.H., Rohde, C.H. and Ascherman, J., 2008. The absorbable
dermal staple device: A faster, more cost-effective method for incisional closure. Journal of
the American College of Surgeons, 207(3), p.S66.
Zempsky, W.T., Parrotti, D., Grem, C. and Nichols, J., 2004. Randomized controlled
comparison of cosmetic outcomes of simple facial lacerations closed with Steri Strip™ skin
Closures or Dermabond™ tissue adhesive. Pediatric emergency care, 20(8), pp.519-524.
52
skin closure in facial plastic surgery. Plastic and reconstructive surgery, 102(6), pp.2209-
2219.
Umranikar, S.A., Ubee, S.S., Selvan, M. and Cooke, P., 2017. Barbed suture tissue closure
device in urological surgery–a comprehensive review. Journal of Clinical Urology, 10(5),
pp.476-484.
Weiland, D.E., Bay, R.C. and Del Sordi, S., 1998. Choosing the best abdominal closure by
meta-analysis. The American journal of surgery, 176(6), pp.666-670.
Wolf, J.S., Tchetgen, M.B. and Merion, R.M., 1998. Hand-assisted laparoscopic live donor
nephrectomy. Urology, 52(5), pp.885-887.
Wolf, S.J., Soble, J.J., Nakada, S.Y., Rayala, H.J., Humphrey, P.A., Clayman, R.V. and
Poppas, D.P., 1997. Comparison of fibrin glue, laser weld, and mechanical suturing device
for the laparoscopic closure of ureterotomy in a porcine model. The Journal of
urology, 157(4), pp.1487-1492.
Wong, S.L., Cross, K.J., Teo, E.H., Rohde, C.H. and Ascherman, J., 2008. The absorbable
dermal staple device: A faster, more cost-effective method for incisional closure. Journal of
the American College of Surgeons, 207(3), p.S66.
Zempsky, W.T., Parrotti, D., Grem, C. and Nichols, J., 2004. Randomized controlled
comparison of cosmetic outcomes of simple facial lacerations closed with Steri Strip™ skin
Closures or Dermabond™ tissue adhesive. Pediatric emergency care, 20(8), pp.519-524.
52
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
APPENDICES
Appendix 1:
53
Appendix 1:
53
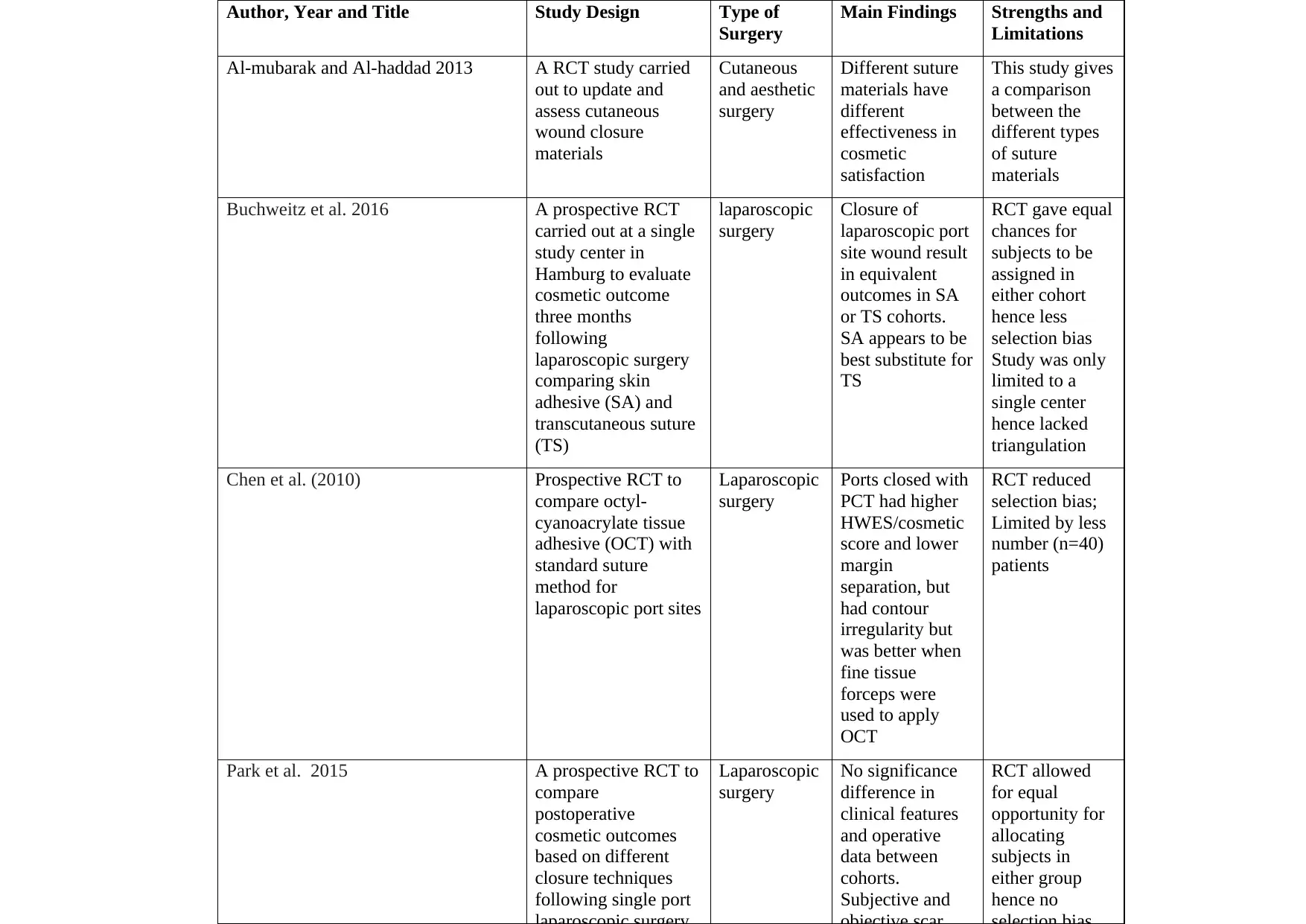
Author, Year and Title Study Design Type of
Surgery
Main Findings Strengths and
Limitations
Al-mubarak and Al-haddad 2013 A RCT study carried
out to update and
assess cutaneous
wound closure
materials
Cutaneous
and aesthetic
surgery
Different suture
materials have
different
effectiveness in
cosmetic
satisfaction
This study gives
a comparison
between the
different types
of suture
materials
Buchweitz et al. 2016 A prospective RCT
carried out at a single
study center in
Hamburg to evaluate
cosmetic outcome
three months
following
laparoscopic surgery
comparing skin
adhesive (SA) and
transcutaneous suture
(TS)
laparoscopic
surgery
Closure of
laparoscopic port
site wound result
in equivalent
outcomes in SA
or TS cohorts.
SA appears to be
best substitute for
TS
RCT gave equal
chances for
subjects to be
assigned in
either cohort
hence less
selection bias
Study was only
limited to a
single center
hence lacked
triangulation
Chen et al. (2010) Prospective RCT to
compare octyl-
cyanoacrylate tissue
adhesive (OCT) with
standard suture
method for
laparoscopic port sites
Laparoscopic
surgery
Ports closed with
PCT had higher
HWES/cosmetic
score and lower
margin
separation, but
had contour
irregularity but
was better when
fine tissue
forceps were
used to apply
OCT
RCT reduced
selection bias;
Limited by less
number (n=40)
patients
Park et al. 2015 A prospective RCT to
compare
postoperative
cosmetic outcomes
based on different
closure techniques
following single port
Laparoscopic
surgery
No significance
difference in
clinical features
and operative
data between
cohorts.
Subjective and
RCT allowed
for equal
opportunity for
allocating
subjects in
either group
hence no
Surgery
Main Findings Strengths and
Limitations
Al-mubarak and Al-haddad 2013 A RCT study carried
out to update and
assess cutaneous
wound closure
materials
Cutaneous
and aesthetic
surgery
Different suture
materials have
different
effectiveness in
cosmetic
satisfaction
This study gives
a comparison
between the
different types
of suture
materials
Buchweitz et al. 2016 A prospective RCT
carried out at a single
study center in
Hamburg to evaluate
cosmetic outcome
three months
following
laparoscopic surgery
comparing skin
adhesive (SA) and
transcutaneous suture
(TS)
laparoscopic
surgery
Closure of
laparoscopic port
site wound result
in equivalent
outcomes in SA
or TS cohorts.
SA appears to be
best substitute for
TS
RCT gave equal
chances for
subjects to be
assigned in
either cohort
hence less
selection bias
Study was only
limited to a
single center
hence lacked
triangulation
Chen et al. (2010) Prospective RCT to
compare octyl-
cyanoacrylate tissue
adhesive (OCT) with
standard suture
method for
laparoscopic port sites
Laparoscopic
surgery
Ports closed with
PCT had higher
HWES/cosmetic
score and lower
margin
separation, but
had contour
irregularity but
was better when
fine tissue
forceps were
used to apply
OCT
RCT reduced
selection bias;
Limited by less
number (n=40)
patients
Park et al. 2015 A prospective RCT to
compare
postoperative
cosmetic outcomes
based on different
closure techniques
following single port
Laparoscopic
surgery
No significance
difference in
clinical features
and operative
data between
cohorts.
Subjective and
RCT allowed
for equal
opportunity for
allocating
subjects in
either group
hence no

55
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

56
1 out of 56
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.