A Comprehensive Report on Sleep Apnea: Diagnosis and Treatment
VerifiedAdded on 2023/06/11
|10
|3543
|447
Report
AI Summary
This report provides a detailed overview of sleep apnea, a condition characterized by repeated upper airway collapse during sleep. It differentiates between central and obstructive sleep apnea, focusing primarily on the latter. The report identifies key risk factors such as loud snoring, obesity, and large neck circumference, and discusses diagnostic methods including history and physical examination, polysomnography, and portable monitoring. Various treatment options are explored, including CPAP therapy, oral appliances, surgical interventions, behavioral changes, and over-the-counter remedies. The importance of quality sleep and the potential impact of sleep deprivation on productivity are also highlighted.

Running head: SLEEP APNEA
Sleep Apnea
Name of the Student
Name of the University
Author note
Sleep Apnea
Name of the Student
Name of the University
Author note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1SLEEP APNEA
Table of Contents
Introduction...........................................................................................................................................2
Discussion..............................................................................................................................................2
Identification of risk factors of the patients of Sleep Apnea..................................................................2
Diagnosis:..............................................................................................................................................3
History and physical examination..........................................................................................................3
Objective testing....................................................................................................................................4
Polysomngraphy....................................................................................................................................4
Testing with potable monitors...............................................................................................................4
Other sleep procedures.........................................................................................................................4
Treatment..............................................................................................................................................5
BEHAVIORAL APPROACHES...................................................................................................................6
Conclusion.............................................................................................................................................7
References.............................................................................................................................................8
Table of Contents
Introduction...........................................................................................................................................2
Discussion..............................................................................................................................................2
Identification of risk factors of the patients of Sleep Apnea..................................................................2
Diagnosis:..............................................................................................................................................3
History and physical examination..........................................................................................................3
Objective testing....................................................................................................................................4
Polysomngraphy....................................................................................................................................4
Testing with potable monitors...............................................................................................................4
Other sleep procedures.........................................................................................................................4
Treatment..............................................................................................................................................5
BEHAVIORAL APPROACHES...................................................................................................................6
Conclusion.............................................................................................................................................7
References.............................................................................................................................................8
2SLEEP APNEA
Introduction
Sleep apnea is a genuine, possibly perilous condition. It is a breathing issue portrayed by
rehashed fall of the upper airway route while taking sleep, with subsequent suspension of relaxing.
For all intents and purposes all sleep apnea patients have a background marked by noisy wheezing.
They may likewise unconsciously encounter visit feelings of excitement amid the night, bringing
about interminable daytime tiredness or on the other hand weakness. Focal and obstructive sleep
apnea are the two discrete sorts. Focal sleep apnea, portrayed by an absence of wind current in the
nonappearance of ventilatory exertion, is uncommon. Obstructive sleep apnea is considerably more
typical and is alluded to as sleep apnea from this point forward. It is described by conclusion of the
upper aviation route, bringing about the discontinuance of wind current in spite of relentless
ventilator exertion (16). Apnea is characterized as discontinuance of wind current for over 10
seconds. A related occasion, hypopnea, is described by a diminishment in wind current related with
an abatement in oxygen immersion. The normal number of apnea, hypopnea occasions every hour
of sleep is known as the apnea-hypopnea file (AHI). Grown-ups may encounter up to five occasions
for every hour without indications. By and large, as AHI expands, so does the seriousness of
indications, an AHI of five or more noteworthy in blend with self-revealed hypersomnolenceis
demonstrative of the sleep apnea syndrome (11).
1 Sleep apnea has all the earmarks of being as normal as a few better known sicknesses. It is
evaluated that 4 percent of moderately aged men and 2 percent of moderately aged ladies meet
negligible criteria for sleep apnea syndrome.
1 this thinks about to a 4.5 percent commonness of asthma in moderately aged adults.
2 Sleep apnea is more common among the hefty, in guys, and in more seasoned individuals.
3 There likewise is by all accounts a higher pervasiveness of sleep apnea in the hypertensive
populace
The purpose of this essay is to highlight the identification, diagonosis and numerous types of
treatments of the disease.
Discussion
Identification of risk factors of the patients of Sleep Apnea
The individuals who exhibit frequent signs of sleep apnea exhibit loud and frequent snoring
while sleeping. In this context it can be said that when people do not snore frequently they might be
under no risk of having sleep apnea (10). On the contrary, people who have been observed to
experience apneic events which are characterized by gasping or choking while sleeping can definitely
be marked as people who are at risk of sleep apnea. In most occasions the family members identify
the people who are at risk of this disease. In many cases obesity plays a major role and particularly
Introduction
Sleep apnea is a genuine, possibly perilous condition. It is a breathing issue portrayed by
rehashed fall of the upper airway route while taking sleep, with subsequent suspension of relaxing.
For all intents and purposes all sleep apnea patients have a background marked by noisy wheezing.
They may likewise unconsciously encounter visit feelings of excitement amid the night, bringing
about interminable daytime tiredness or on the other hand weakness. Focal and obstructive sleep
apnea are the two discrete sorts. Focal sleep apnea, portrayed by an absence of wind current in the
nonappearance of ventilatory exertion, is uncommon. Obstructive sleep apnea is considerably more
typical and is alluded to as sleep apnea from this point forward. It is described by conclusion of the
upper aviation route, bringing about the discontinuance of wind current in spite of relentless
ventilator exertion (16). Apnea is characterized as discontinuance of wind current for over 10
seconds. A related occasion, hypopnea, is described by a diminishment in wind current related with
an abatement in oxygen immersion. The normal number of apnea, hypopnea occasions every hour
of sleep is known as the apnea-hypopnea file (AHI). Grown-ups may encounter up to five occasions
for every hour without indications. By and large, as AHI expands, so does the seriousness of
indications, an AHI of five or more noteworthy in blend with self-revealed hypersomnolenceis
demonstrative of the sleep apnea syndrome (11).
1 Sleep apnea has all the earmarks of being as normal as a few better known sicknesses. It is
evaluated that 4 percent of moderately aged men and 2 percent of moderately aged ladies meet
negligible criteria for sleep apnea syndrome.
1 this thinks about to a 4.5 percent commonness of asthma in moderately aged adults.
2 Sleep apnea is more common among the hefty, in guys, and in more seasoned individuals.
3 There likewise is by all accounts a higher pervasiveness of sleep apnea in the hypertensive
populace
The purpose of this essay is to highlight the identification, diagonosis and numerous types of
treatments of the disease.
Discussion
Identification of risk factors of the patients of Sleep Apnea
The individuals who exhibit frequent signs of sleep apnea exhibit loud and frequent snoring
while sleeping. In this context it can be said that when people do not snore frequently they might be
under no risk of having sleep apnea (10). On the contrary, people who have been observed to
experience apneic events which are characterized by gasping or choking while sleeping can definitely
be marked as people who are at risk of sleep apnea. In most occasions the family members identify
the people who are at risk of this disease. In many cases obesity plays a major role and particularly
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3SLEEP APNEA
obesity in the upper body section of individuals play a significant role to make the individual fall prey
of sleep apnea. It has been observed that majority of the sleep apnea patients are obese and the
people having more than 120% of the ideal body are seen to have experienced sleep apnea. In many
occasions large neck girth in both female and male snorers can be majorly predictive of sleep apnea
and in most cases males with circumference of neck of 17 inches or greater than that and females
with the next circumference of 15 to 16 inches or more can be tagged as individuals who are at
higher risk for experiencing sleep apnea (11).
There are many other Symptoms and Signs that can help the individuals to identify the
patients who are at higher risk for sleep apnea and those are frequent daytime sleepiness
hypertension automobile or workplace accidents are having unexplained pulmonary hypertension in
individuals that may call in diseases like sleep apnea in a frequent manner. When an individual
complaints regarding sleepiness in the times but does not experience are the symptoms and science
of sleep apnea A thorough observation of the Sleeping habits audit individual should be useful in
that particular scenario (13). For an example the individuals related to the person who complained
regarding the sleepiness can check up on the average hours of sleep of that person or the frequently
changing sleeping schedules of that person or recent change in the lifestyle of that individual. Not
only for the adults but sleep apnea can affect children also and tonsillar hypertrophy is one of the
major reason behind that. Children experiencing sleep apnea may show various Symptoms and Signs
then the adults exhibit (8).
Diagnosis:
The existence or the absence of OSA should be determined before the initiation of the
treatment. This should be done in order to figure out the failures of those patients who are suffering
from the risk of sleep apnea (14). This would act as the first step of guidance for the patients. This is
the first steep of developing the baseline to establish the presence of the disease in the patients. The
diagnostic criteria for OSA are completely based on the clinical signs and the symptoms that are
observed during the sleep of a particular person (3). These are based on the clinical signs and
symbols. This is related to the history of the sleep and the physical examination.
History and physical examination
Knowing the history of the sleep is the first step toward knowing the disease well that might
help in the diagnosis process of the disease. This is divided into three different parts. The first part is
the evaluation of the of the routine health checkup (7). The second part is the assessment of the
symptoms that forms the major cause of the sleep apnea and that disturbs the sleep. The third part
is the wide-ranging evaluation of the patients at high risk for OSA. The patients who have the high
risk of having the disease are those who have high risk of heart failure, atrial fibrillation,
hypertension, stroke, diabetes nocturnal dysrhythmias and the ones who are evaluated for bariatric
surgery. In order to know about the history of the disease certain questions should be asked to the
patient regarding the history of snoring and daytime sleepiness and on the existence of obesity or
hypertension.
obesity in the upper body section of individuals play a significant role to make the individual fall prey
of sleep apnea. It has been observed that majority of the sleep apnea patients are obese and the
people having more than 120% of the ideal body are seen to have experienced sleep apnea. In many
occasions large neck girth in both female and male snorers can be majorly predictive of sleep apnea
and in most cases males with circumference of neck of 17 inches or greater than that and females
with the next circumference of 15 to 16 inches or more can be tagged as individuals who are at
higher risk for experiencing sleep apnea (11).
There are many other Symptoms and Signs that can help the individuals to identify the
patients who are at higher risk for sleep apnea and those are frequent daytime sleepiness
hypertension automobile or workplace accidents are having unexplained pulmonary hypertension in
individuals that may call in diseases like sleep apnea in a frequent manner. When an individual
complaints regarding sleepiness in the times but does not experience are the symptoms and science
of sleep apnea A thorough observation of the Sleeping habits audit individual should be useful in
that particular scenario (13). For an example the individuals related to the person who complained
regarding the sleepiness can check up on the average hours of sleep of that person or the frequently
changing sleeping schedules of that person or recent change in the lifestyle of that individual. Not
only for the adults but sleep apnea can affect children also and tonsillar hypertrophy is one of the
major reason behind that. Children experiencing sleep apnea may show various Symptoms and Signs
then the adults exhibit (8).
Diagnosis:
The existence or the absence of OSA should be determined before the initiation of the
treatment. This should be done in order to figure out the failures of those patients who are suffering
from the risk of sleep apnea (14). This would act as the first step of guidance for the patients. This is
the first steep of developing the baseline to establish the presence of the disease in the patients. The
diagnostic criteria for OSA are completely based on the clinical signs and the symptoms that are
observed during the sleep of a particular person (3). These are based on the clinical signs and
symbols. This is related to the history of the sleep and the physical examination.
History and physical examination
Knowing the history of the sleep is the first step toward knowing the disease well that might
help in the diagnosis process of the disease. This is divided into three different parts. The first part is
the evaluation of the of the routine health checkup (7). The second part is the assessment of the
symptoms that forms the major cause of the sleep apnea and that disturbs the sleep. The third part
is the wide-ranging evaluation of the patients at high risk for OSA. The patients who have the high
risk of having the disease are those who have high risk of heart failure, atrial fibrillation,
hypertension, stroke, diabetes nocturnal dysrhythmias and the ones who are evaluated for bariatric
surgery. In order to know about the history of the disease certain questions should be asked to the
patient regarding the history of snoring and daytime sleepiness and on the existence of obesity or
hypertension.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4SLEEP APNEA
Objective testing
In order to deal with this a serious treatment process should be designed. There are no
specific treatment model that can be recommended in order to predict the severity of OSP. In order
to fix this objective testing is essential (14). The diagnosis can be recognized by an satisfactory
method. The most common method of objective testing are in-laboratory polysomnography and
home testing with portable monitors. The particulars on the parameters should be considered with
PSG and PM. The patients who have high risk with some amount of nocturnal symptoms of OSA
should go through the sleep testing that includes who are obese, the ones who are having diastolic
heart failure and the coronary artery disease (16).
Polysomngraphy
This is an effective process that can be used to evaluate OSA that requires the recording the
signals that are related to the electroencephalogram, electrooculogram, chin electromyogram,
airflow, oxygen saturation, respiratory effort and electrocardiogram or heart rate (5).
Testing with potable monitors
Portable Monitors for diagnosis of OSA should be performed only in the conjunction with a
complete sleep evaluation. The clinical sleep evaluations that use PM must be evaluated and
supervised by the practitioner with the broad certification in sleep medicine or an individual who
fulfils the eligibility criteria for the sleep medicine certification examination (15).
Other sleep procedures
In many instances the multiple sleep latency test is not routinely indicated in the initial
evaluation and the diagnosis of OSA or in an assessment of change that is followed by the treatment
with nasal CPAP.
Objective testing
In order to deal with this a serious treatment process should be designed. There are no
specific treatment model that can be recommended in order to predict the severity of OSP. In order
to fix this objective testing is essential (14). The diagnosis can be recognized by an satisfactory
method. The most common method of objective testing are in-laboratory polysomnography and
home testing with portable monitors. The particulars on the parameters should be considered with
PSG and PM. The patients who have high risk with some amount of nocturnal symptoms of OSA
should go through the sleep testing that includes who are obese, the ones who are having diastolic
heart failure and the coronary artery disease (16).
Polysomngraphy
This is an effective process that can be used to evaluate OSA that requires the recording the
signals that are related to the electroencephalogram, electrooculogram, chin electromyogram,
airflow, oxygen saturation, respiratory effort and electrocardiogram or heart rate (5).
Testing with potable monitors
Portable Monitors for diagnosis of OSA should be performed only in the conjunction with a
complete sleep evaluation. The clinical sleep evaluations that use PM must be evaluated and
supervised by the practitioner with the broad certification in sleep medicine or an individual who
fulfils the eligibility criteria for the sleep medicine certification examination (15).
Other sleep procedures
In many instances the multiple sleep latency test is not routinely indicated in the initial
evaluation and the diagnosis of OSA or in an assessment of change that is followed by the treatment
with nasal CPAP.
5SLEEP APNEA
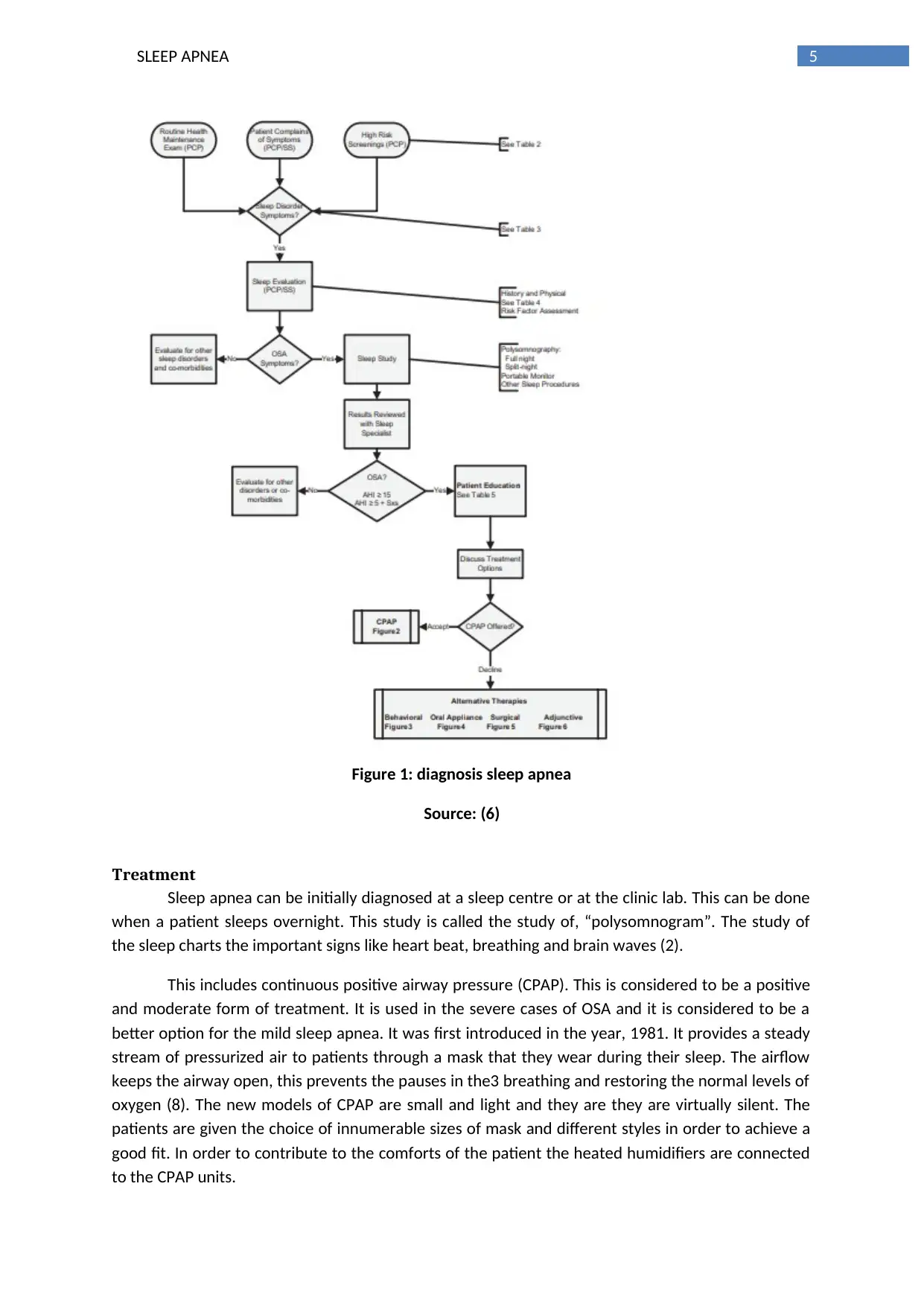
Figure 1: diagnosis sleep apnea
Source: (6)
Treatment
Sleep apnea can be initially diagnosed at a sleep centre or at the clinic lab. This can be done
when a patient sleeps overnight. This study is called the study of, “polysomnogram”. The study of
the sleep charts the important signs like heart beat, breathing and brain waves (2).
This includes continuous positive airway pressure (CPAP). This is considered to be a positive
and moderate form of treatment. It is used in the severe cases of OSA and it is considered to be a
better option for the mild sleep apnea. It was first introduced in the year, 1981. It provides a steady
stream of pressurized air to patients through a mask that they wear during their sleep. The airflow
keeps the airway open, this prevents the pauses in the3 breathing and restoring the normal levels of
oxygen (8). The new models of CPAP are small and light and they are they are virtually silent. The
patients are given the choice of innumerable sizes of mask and different styles in order to achieve a
good fit. In order to contribute to the comforts of the patient the heated humidifiers are connected
to the CPAP units.
Figure 1: diagnosis sleep apnea
Source: (6)
Treatment
Sleep apnea can be initially diagnosed at a sleep centre or at the clinic lab. This can be done
when a patient sleeps overnight. This study is called the study of, “polysomnogram”. The study of
the sleep charts the important signs like heart beat, breathing and brain waves (2).
This includes continuous positive airway pressure (CPAP). This is considered to be a positive
and moderate form of treatment. It is used in the severe cases of OSA and it is considered to be a
better option for the mild sleep apnea. It was first introduced in the year, 1981. It provides a steady
stream of pressurized air to patients through a mask that they wear during their sleep. The airflow
keeps the airway open, this prevents the pauses in the3 breathing and restoring the normal levels of
oxygen (8). The new models of CPAP are small and light and they are they are virtually silent. The
patients are given the choice of innumerable sizes of mask and different styles in order to achieve a
good fit. In order to contribute to the comforts of the patient the heated humidifiers are connected
to the CPAP units.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6SLEEP APNEA
The other form is the oral appliances. The oral appliance is a useful option of treatment for
the people having mild issues, in order to reasonable OSA to the ones who actually prefer CPAP or
they are not able to successfully comply with the therapy of CPAP. The oral appliances appear as
sports mouth guards, which assist in maintaining an unobstructed and open airway by stabilizing or
repositioning the lower jaw, the soft palate, the tongue and the uvula. Some of them are designed
mostly for the purpose of snoring and the sleep apnea. However, they need to be fitted by those
dentists who should be trained in giving sleep medicines.
The other process is the process of surgery. This option can be applied when the problem
involves anatomic deformity. This can be corrected in order to alleviate the breathing problem. On
the other hand this has a severe risk. The surgical option most often addresses the issue by removing
or reducing the tissue from soft palate, tonsils, uvula, adenoids and the tongue. The surgical method
can be performed only with the help of an operation (7). The biggest risk is that it contains is the fact
that it is not certain that the result will be positive. The surgical removal of the tonsil and adenoids is
treated as the most common option for treating the children.
The other includes the behavioural changes. It has been observed in many cases that the
persons who are overweight suffer from sleep apnea. In such case weight loss is the best option.99
This option might be effective one for those who might develop the habit of changing from back-
sleeping to side-sleeping. This might bring results for those who are suffering from the mild cases of
OSA (9).
Apart from this the other treatments include the over-the-counter remedies. There are
certain sprays that might reduce the snoring like internal nasal dilators, external dilator strips and
lubricant sprays (4). However it has been proved that there is no such evidence that these remedies
might even reduce the problems of loud snoring. The snoring created loud sound that is regarded as
the warning sign for this disorder. The most common treatment that is used for the snoring patients
is the change of the position of the sleep. The patients are generally advised to stay off the back
during sleeping and raise their heads of the bed in order to reduce these symptoms.
BEHAVIORAL APPROACHES
It is a matter of fact that quality sleep for a long period of time helps to maintain a good
balance in life and if an individual gets deprived of sound sleep that can potentially affect the
productivity and can bring in numerous troubles for that particular person. It has been seen that the
lack of sleep aggravates anxiety, reduced quality of daily life, increases stress level and harms the
daily course of life of that individual (10). First and foremost lack of sleep destroys the patterns of
electric inside human brain and reorganizes cognitive functions. Continuous lack of sleep can cause
various disorders with cognitive impairments (3). Not only that, it can definitely be said that sleep
apnea results in a major negative impact on the individual alertness, attention, learning ability and
significantly harms the productivity of that person (12). One should not only look for the physical
factors of sleep apnea but also look for the associated psychological factors of the disease. It is a
matter of fact that the psychological roots can be found based on emotional factors, attitudes that
concerns sleep and some dysfunctional beliefs along with many other behavioural factors like
inadequate sleep hygiene (13).
The other form is the oral appliances. The oral appliance is a useful option of treatment for
the people having mild issues, in order to reasonable OSA to the ones who actually prefer CPAP or
they are not able to successfully comply with the therapy of CPAP. The oral appliances appear as
sports mouth guards, which assist in maintaining an unobstructed and open airway by stabilizing or
repositioning the lower jaw, the soft palate, the tongue and the uvula. Some of them are designed
mostly for the purpose of snoring and the sleep apnea. However, they need to be fitted by those
dentists who should be trained in giving sleep medicines.
The other process is the process of surgery. This option can be applied when the problem
involves anatomic deformity. This can be corrected in order to alleviate the breathing problem. On
the other hand this has a severe risk. The surgical option most often addresses the issue by removing
or reducing the tissue from soft palate, tonsils, uvula, adenoids and the tongue. The surgical method
can be performed only with the help of an operation (7). The biggest risk is that it contains is the fact
that it is not certain that the result will be positive. The surgical removal of the tonsil and adenoids is
treated as the most common option for treating the children.
The other includes the behavioural changes. It has been observed in many cases that the
persons who are overweight suffer from sleep apnea. In such case weight loss is the best option.99
This option might be effective one for those who might develop the habit of changing from back-
sleeping to side-sleeping. This might bring results for those who are suffering from the mild cases of
OSA (9).
Apart from this the other treatments include the over-the-counter remedies. There are
certain sprays that might reduce the snoring like internal nasal dilators, external dilator strips and
lubricant sprays (4). However it has been proved that there is no such evidence that these remedies
might even reduce the problems of loud snoring. The snoring created loud sound that is regarded as
the warning sign for this disorder. The most common treatment that is used for the snoring patients
is the change of the position of the sleep. The patients are generally advised to stay off the back
during sleeping and raise their heads of the bed in order to reduce these symptoms.
BEHAVIORAL APPROACHES
It is a matter of fact that quality sleep for a long period of time helps to maintain a good
balance in life and if an individual gets deprived of sound sleep that can potentially affect the
productivity and can bring in numerous troubles for that particular person. It has been seen that the
lack of sleep aggravates anxiety, reduced quality of daily life, increases stress level and harms the
daily course of life of that individual (10). First and foremost lack of sleep destroys the patterns of
electric inside human brain and reorganizes cognitive functions. Continuous lack of sleep can cause
various disorders with cognitive impairments (3). Not only that, it can definitely be said that sleep
apnea results in a major negative impact on the individual alertness, attention, learning ability and
significantly harms the productivity of that person (12). One should not only look for the physical
factors of sleep apnea but also look for the associated psychological factors of the disease. It is a
matter of fact that the psychological roots can be found based on emotional factors, attitudes that
concerns sleep and some dysfunctional beliefs along with many other behavioural factors like
inadequate sleep hygiene (13).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

7SLEEP APNEA
It has been seen that when a person who is fighting with sleep apnea after getting professional help
gets out of the trauma they exhibited sorts of depression and fatigue while performing daily
activities(3). It is a matter of fact that the patients of sleep apnea should be handled with proper
care and under professional supervision in order to eradicate these issues (14).
Conclusion
Thus to coclude, it can surely be said that the diseases like sleep apnea can surely be treated
with proper care and by utilizing cognitive behavioural therapy in order to enhance the sleep quality,
disorders of sleep and many more. It Is a matter of fact that diseases like sleep apnea initially may
look simple and easy to get rid of but negligence can cost a lot as with lesser productivity and
increased stress and depression of the patients, the matter becomes pretty serious and the patients
who are fighting with this odd, may find themselves cornered.
It has been seen that when a person who is fighting with sleep apnea after getting professional help
gets out of the trauma they exhibited sorts of depression and fatigue while performing daily
activities(3). It is a matter of fact that the patients of sleep apnea should be handled with proper
care and under professional supervision in order to eradicate these issues (14).
Conclusion
Thus to coclude, it can surely be said that the diseases like sleep apnea can surely be treated
with proper care and by utilizing cognitive behavioural therapy in order to enhance the sleep quality,
disorders of sleep and many more. It Is a matter of fact that diseases like sleep apnea initially may
look simple and easy to get rid of but negligence can cost a lot as with lesser productivity and
increased stress and depression of the patients, the matter becomes pretty serious and the patients
who are fighting with this odd, may find themselves cornered.
8SLEEP APNEA
References
1. Alonso-Álvarez, M.L., Terán-Santos, J., Carbajo, E.O., Cordero-Guevara, J.A., Navazo-Egüia,
A.I., Kheirandish-Gozal, L. and Gozal, D., 2015. Reliability of home respiratory polygraphy for
the diagnosis of sleep apnea in children. Chest, 147(4), pp.1020-1028.
2. Qaseem, A., Dallas, P., Owens, D.K., Starkey, M., Holty, J.E.C. and Shekelle, P., 2014.
Diagnosis of obstructive sleep apnea in adults: a clinical practice guideline from the
American College of Physicians. Annals of internal medicine, 161(3), pp.210-220.
3. Kapur, V.K., Auckley, D.H., Chowdhuri, S., Kuhlmann, D.C., Mehra, R., Ramar, K. and Harrod,
C.G., 2017. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea:
an American Academy of Sleep Medicine clinical practice guideline. Journal of clinical sleep
medicine: JCSM: official publication of the American Academy of Sleep Medicine, 13(3),
pp.479-504.
4. Alshaer, H., Fernie, G.R., Tseng, W.H. and Bradley, T.D., 2016. Comparison of in-laboratory
and home diagnosis of sleep apnea using a cordless portable acoustic device. Sleep
medicine, 22, pp.91-96.
5. Chiu, H.Y., Chen, P.Y., Chuang, L.P., Chen, N.H., Tu, Y.K., Hsieh, Y.J., Wang, Y.C. and
Guilleminault, C., 2017. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP,
and Epworth sleepiness scale in detecting obstructive sleep apnea: a bivariate meta-
analysis. Sleep medicine reviews, 36, pp.57-70.
6. Brill, A.K., Horvath, T., Seiler, A., Camilo, M., Haynes, A.G., Ott, S.R., Egger, M. and Bassetti,
C.L., 2018. CPAP as treatment of sleep apnea after stroke: A meta-analysis of randomized
trials. Neurology, 90(14), pp.e1222-e1230.
7. Friedman, M., Irwin, J.J., Gorman, W.J., Garibotto, J.T. and Flaherty, J.C., Lumen Devices LLC,
2015. Devices, systems and methods for the treatment of sleep apnea. U.S. Patent 9,132,028.
8. Hetzenecker, A., Escourrou, P., Kuna, S.T., Series, F., Lewis, K., Birner, C., Pfeifer, M. and Arzt,
M., 2016. Treatment of sleep apnea in chronic heart failure patients with auto-servo
ventilation improves sleep fragmentation: a randomized controlled trial. Sleep medicine, 17,
pp.25-31.
9. Masa, J.F., Duran-Cantolla, J., Capote, F., Cabello, M., Abad, J., Garcia-Rio, F., Ferrer, A.,
Fortuna, A.M., Gonzalez-Mangado, N., de la Peña, M. and Aizpuru, F., 2015. Efficacy of home
single-channel nasal pressure for recommending continuous positive airway pressure
treatment in sleep apnea. Sleep, 38(1), pp.13-21.
10. Kendzerska, T., Gershon, A.S., Tomlinson, G. and Leung, R.S., 2016. The Effect of patient
neighborhood income level on the purchase of continuous positive airway pressure
treatment among patients with sleep apnea. Annals of the American Thoracic Society, 13(1),
pp.93-100.
11. Chung, F., Abdullah, H.R. and Liao, P., 2016. STOP-Bang questionnaire: a practical approach
to screen for obstructive sleep apnea. Chest, 149(3), pp.631-638.
12. Peker, Y., Glantz, H., Eulenburg, C., Wegscheider, K., Herlitz, J. and Thunström, E., 2016.
Effect of positive airway pressure on cardiovascular outcomes in coronary artery disease
References
1. Alonso-Álvarez, M.L., Terán-Santos, J., Carbajo, E.O., Cordero-Guevara, J.A., Navazo-Egüia,
A.I., Kheirandish-Gozal, L. and Gozal, D., 2015. Reliability of home respiratory polygraphy for
the diagnosis of sleep apnea in children. Chest, 147(4), pp.1020-1028.
2. Qaseem, A., Dallas, P., Owens, D.K., Starkey, M., Holty, J.E.C. and Shekelle, P., 2014.
Diagnosis of obstructive sleep apnea in adults: a clinical practice guideline from the
American College of Physicians. Annals of internal medicine, 161(3), pp.210-220.
3. Kapur, V.K., Auckley, D.H., Chowdhuri, S., Kuhlmann, D.C., Mehra, R., Ramar, K. and Harrod,
C.G., 2017. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea:
an American Academy of Sleep Medicine clinical practice guideline. Journal of clinical sleep
medicine: JCSM: official publication of the American Academy of Sleep Medicine, 13(3),
pp.479-504.
4. Alshaer, H., Fernie, G.R., Tseng, W.H. and Bradley, T.D., 2016. Comparison of in-laboratory
and home diagnosis of sleep apnea using a cordless portable acoustic device. Sleep
medicine, 22, pp.91-96.
5. Chiu, H.Y., Chen, P.Y., Chuang, L.P., Chen, N.H., Tu, Y.K., Hsieh, Y.J., Wang, Y.C. and
Guilleminault, C., 2017. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP,
and Epworth sleepiness scale in detecting obstructive sleep apnea: a bivariate meta-
analysis. Sleep medicine reviews, 36, pp.57-70.
6. Brill, A.K., Horvath, T., Seiler, A., Camilo, M., Haynes, A.G., Ott, S.R., Egger, M. and Bassetti,
C.L., 2018. CPAP as treatment of sleep apnea after stroke: A meta-analysis of randomized
trials. Neurology, 90(14), pp.e1222-e1230.
7. Friedman, M., Irwin, J.J., Gorman, W.J., Garibotto, J.T. and Flaherty, J.C., Lumen Devices LLC,
2015. Devices, systems and methods for the treatment of sleep apnea. U.S. Patent 9,132,028.
8. Hetzenecker, A., Escourrou, P., Kuna, S.T., Series, F., Lewis, K., Birner, C., Pfeifer, M. and Arzt,
M., 2016. Treatment of sleep apnea in chronic heart failure patients with auto-servo
ventilation improves sleep fragmentation: a randomized controlled trial. Sleep medicine, 17,
pp.25-31.
9. Masa, J.F., Duran-Cantolla, J., Capote, F., Cabello, M., Abad, J., Garcia-Rio, F., Ferrer, A.,
Fortuna, A.M., Gonzalez-Mangado, N., de la Peña, M. and Aizpuru, F., 2015. Efficacy of home
single-channel nasal pressure for recommending continuous positive airway pressure
treatment in sleep apnea. Sleep, 38(1), pp.13-21.
10. Kendzerska, T., Gershon, A.S., Tomlinson, G. and Leung, R.S., 2016. The Effect of patient
neighborhood income level on the purchase of continuous positive airway pressure
treatment among patients with sleep apnea. Annals of the American Thoracic Society, 13(1),
pp.93-100.
11. Chung, F., Abdullah, H.R. and Liao, P., 2016. STOP-Bang questionnaire: a practical approach
to screen for obstructive sleep apnea. Chest, 149(3), pp.631-638.
12. Peker, Y., Glantz, H., Eulenburg, C., Wegscheider, K., Herlitz, J. and Thunström, E., 2016.
Effect of positive airway pressure on cardiovascular outcomes in coronary artery disease
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9SLEEP APNEA
patients with nonsleepy obstructive sleep apnea. The RICCADSA randomized controlled trial.
American journal of respiratory and critical care medicine, 194(5), pp.613-620.
13. Sabato, R., Guido, P., Salerno, F.G., Resta, O., Spanevello, A. and Barbaro, M.F., 2016. Airway
inflammation in patients affected by obstructive sleep apnea. Monaldi Archives for Chest
Disease, 65(2).
14. Gottlieb, D.J., Punjabi, N.M., Mehra, R., Patel, S.R., Quan, S.F., Babineau, D.C., Tracy, R.P.,
Rueschman, M., Blumenthal, R.S., Lewis, E.F. and Bhatt, D.L., 2014. CPAP versus oxygen in
obstructive sleep apnea. New England Journal of Medicine, 370(24), pp.2276-2285.
15. Burks, S.V., Anderson, J.E., Bombyk, M., Haider, R., Ganzhorn, D., Jiao, X., Lewis, C., Lexvold,
A., Liu, H., Ning, J. and Toll, A., 2016. Nonadherence with employer-mandated sleep apnea
treatment and increased risk of serious truck crashes. Sleep, 39(5), pp.967-975.
16. Pepin, J.L., Joyeux-Faure, M., Naegele, B., Tamisier, R., Levy, P. and Launois, S., 2016.
Evaluation Of Cpap Treatment On Memory Processes In Obstructive Sleep Apnea Patients
Through a randomized Controlled Trial. In A110. THE SLEEPY AND AGING BRAIN: OSA AND
COGNITION IN THE ELDERLY (pp. A2847-A2847). American Thoracic Society.
patients with nonsleepy obstructive sleep apnea. The RICCADSA randomized controlled trial.
American journal of respiratory and critical care medicine, 194(5), pp.613-620.
13. Sabato, R., Guido, P., Salerno, F.G., Resta, O., Spanevello, A. and Barbaro, M.F., 2016. Airway
inflammation in patients affected by obstructive sleep apnea. Monaldi Archives for Chest
Disease, 65(2).
14. Gottlieb, D.J., Punjabi, N.M., Mehra, R., Patel, S.R., Quan, S.F., Babineau, D.C., Tracy, R.P.,
Rueschman, M., Blumenthal, R.S., Lewis, E.F. and Bhatt, D.L., 2014. CPAP versus oxygen in
obstructive sleep apnea. New England Journal of Medicine, 370(24), pp.2276-2285.
15. Burks, S.V., Anderson, J.E., Bombyk, M., Haider, R., Ganzhorn, D., Jiao, X., Lewis, C., Lexvold,
A., Liu, H., Ning, J. and Toll, A., 2016. Nonadherence with employer-mandated sleep apnea
treatment and increased risk of serious truck crashes. Sleep, 39(5), pp.967-975.
16. Pepin, J.L., Joyeux-Faure, M., Naegele, B., Tamisier, R., Levy, P. and Launois, S., 2016.
Evaluation Of Cpap Treatment On Memory Processes In Obstructive Sleep Apnea Patients
Through a randomized Controlled Trial. In A110. THE SLEEPY AND AGING BRAIN: OSA AND
COGNITION IN THE ELDERLY (pp. A2847-A2847). American Thoracic Society.
1 out of 10
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.