SOAP Note Analysis: Abdominal Pain, Nausea, and Vomiting
VerifiedAdded on 2022/11/07
|6
|2290
|72
Homework Assignment
AI Summary
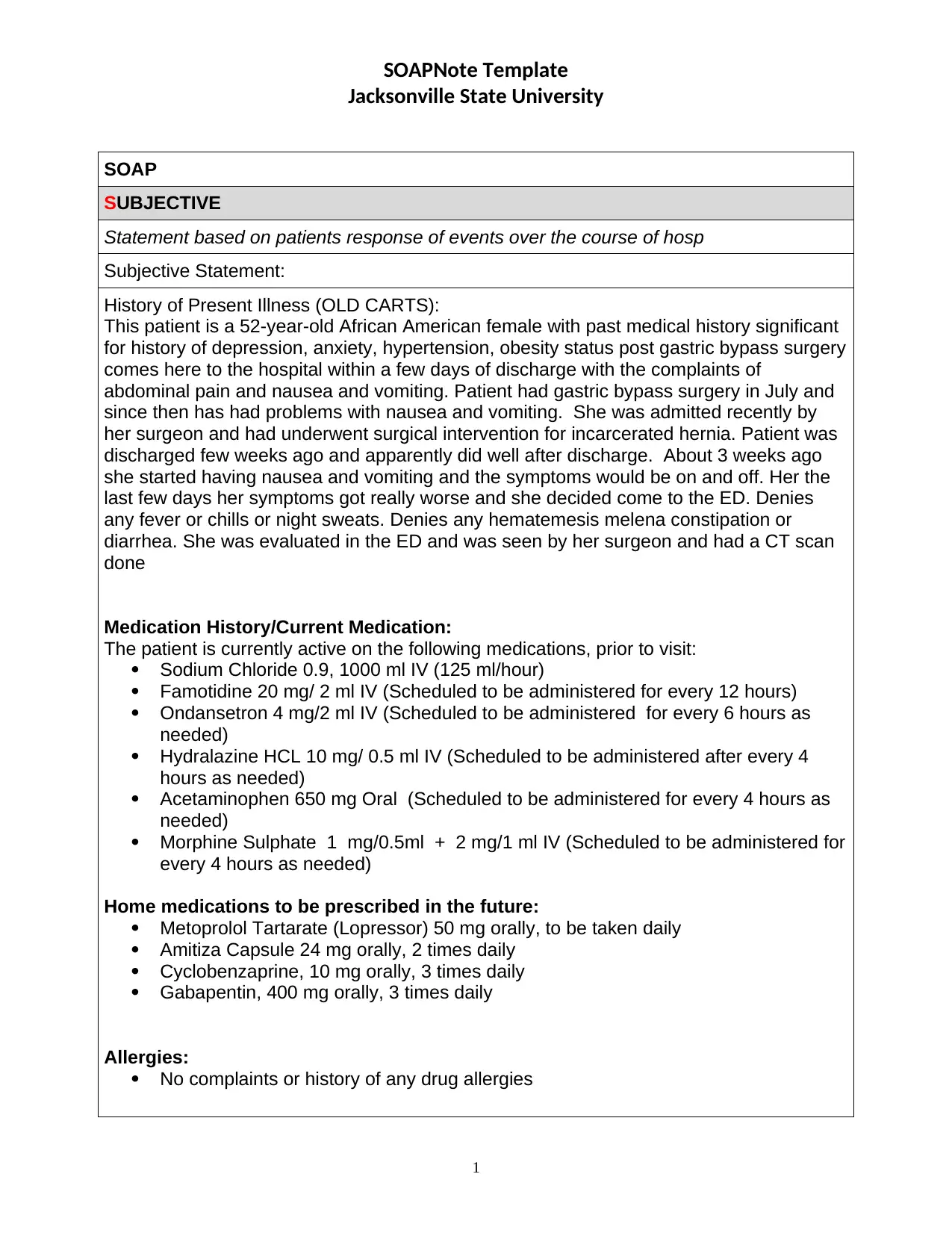
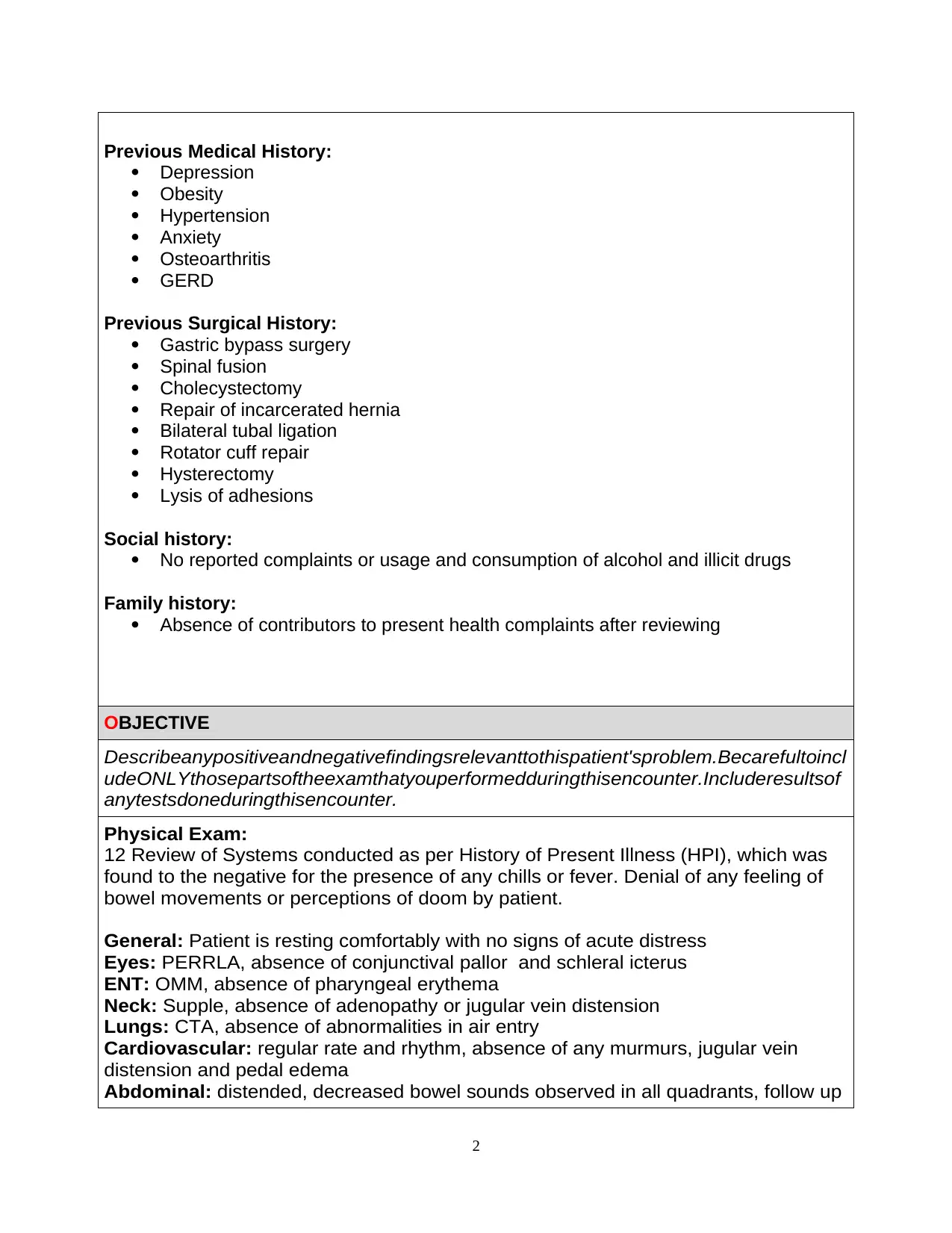
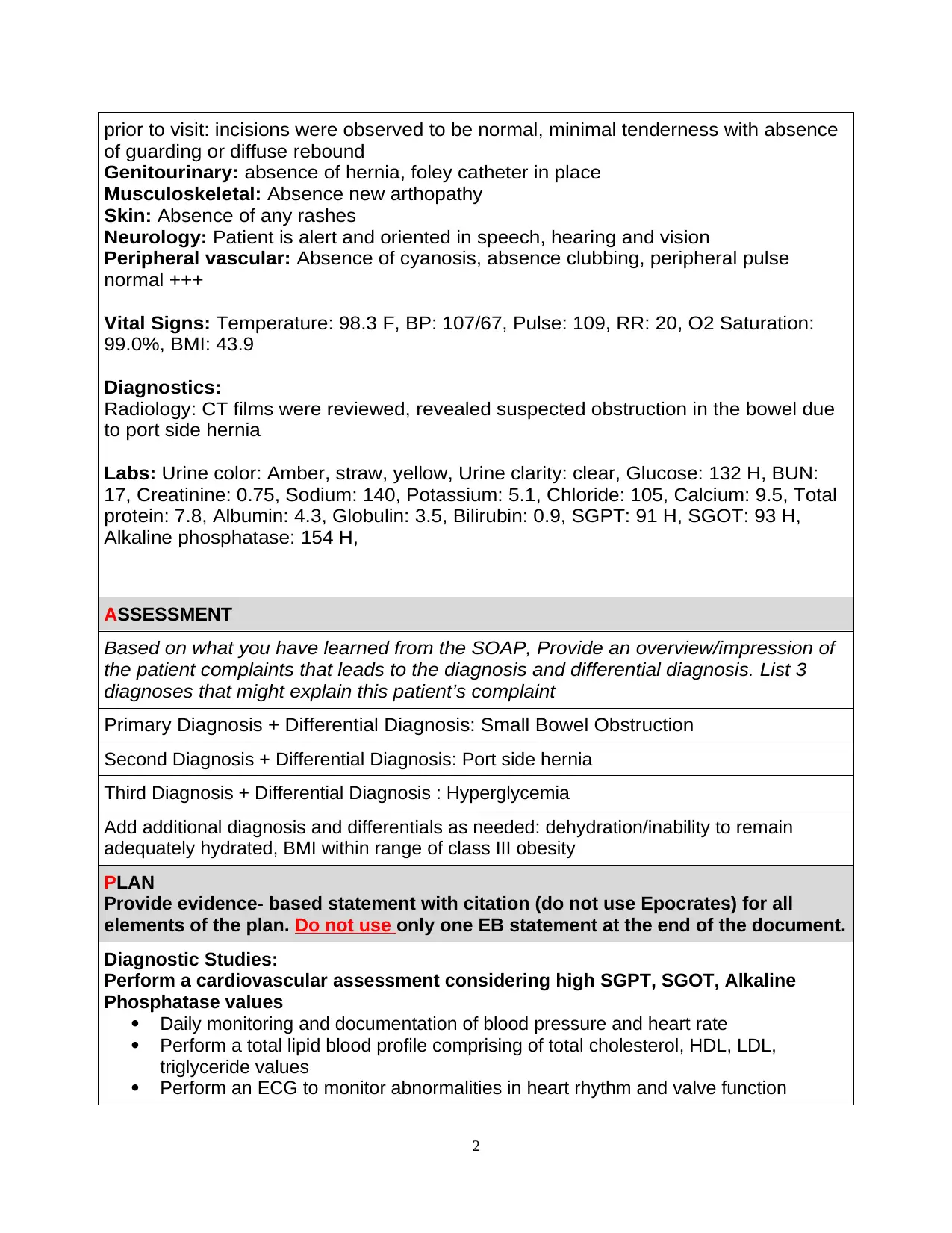
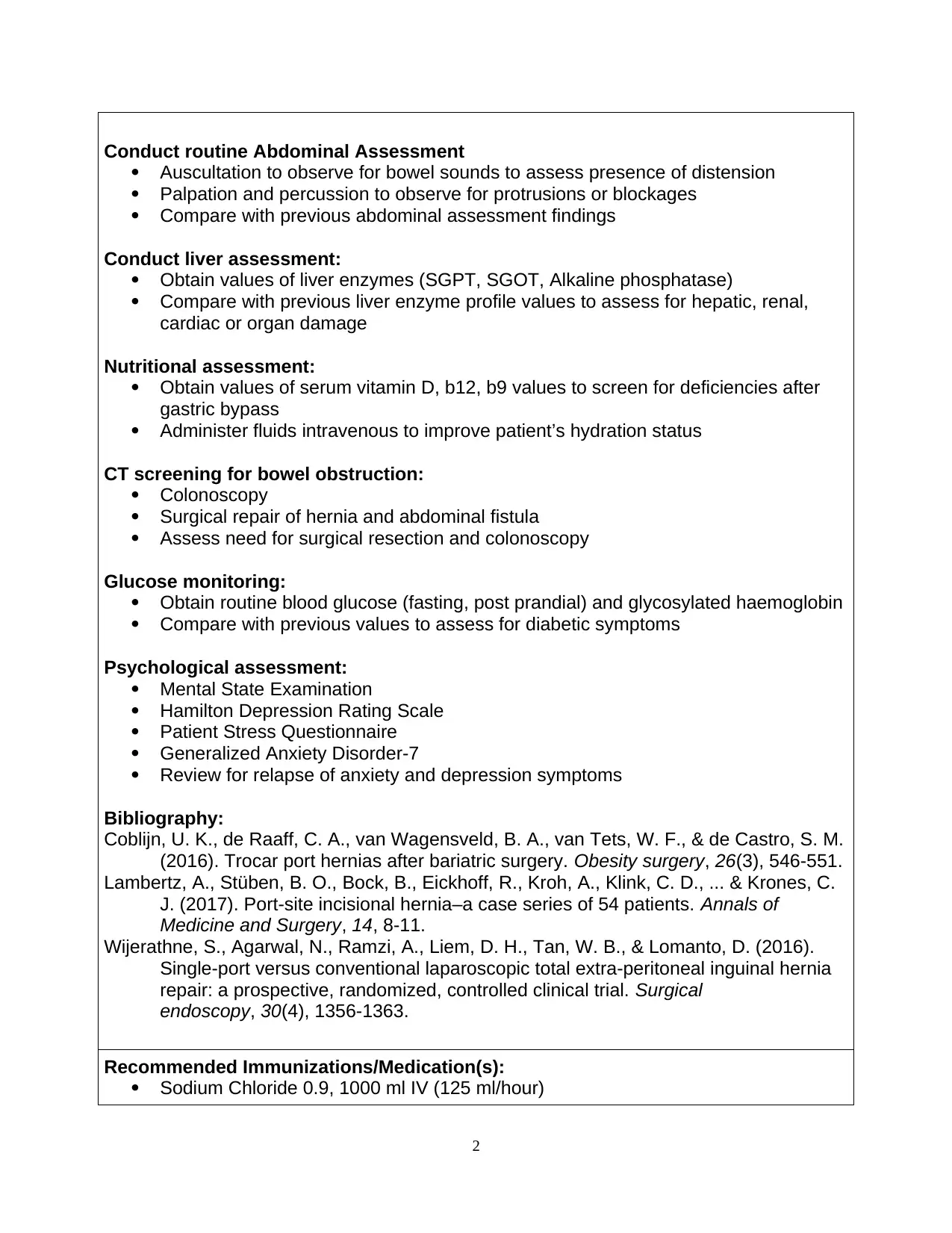
This SOAP note documents the case of a 52-year-old African American female presenting with abdominal pain, nausea, and vomiting following gastric bypass surgery and recent hernia repair. The subjective section details the patient's history of present illness, including the onset, characteristics, and alleviating factors of her symptoms, as well as her medication history, allergies, and past medical and surgical history. The objective section includes vital signs, physical exam findings (e.g., distended abdomen, decreased bowel sounds), and diagnostic results from a CT scan and lab tests (e.g., elevated liver enzymes and glucose). The assessment identifies primary diagnoses of small bowel obstruction, port side hernia, and hyperglycemia, along with differential diagnoses. The plan outlines evidence-based diagnostic studies (e.g., cardiovascular assessment, total lipid profile), nutritional and psychological assessments, and recommended immunizations/medications, including intravenous fluids, antiemetics, and analgesics. The plan also includes surgical considerations and patient instructions for follow-up care. The note concludes with a bibliography of cited sources and recommendations for follow-up with various specialists.
1 out of 6
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.