Pregnancy Anemia in India: Epidemiology, Strategies, and Outcomes
VerifiedAdded on 2022/08/12
|6
|2281
|34
Presentation
AI Summary
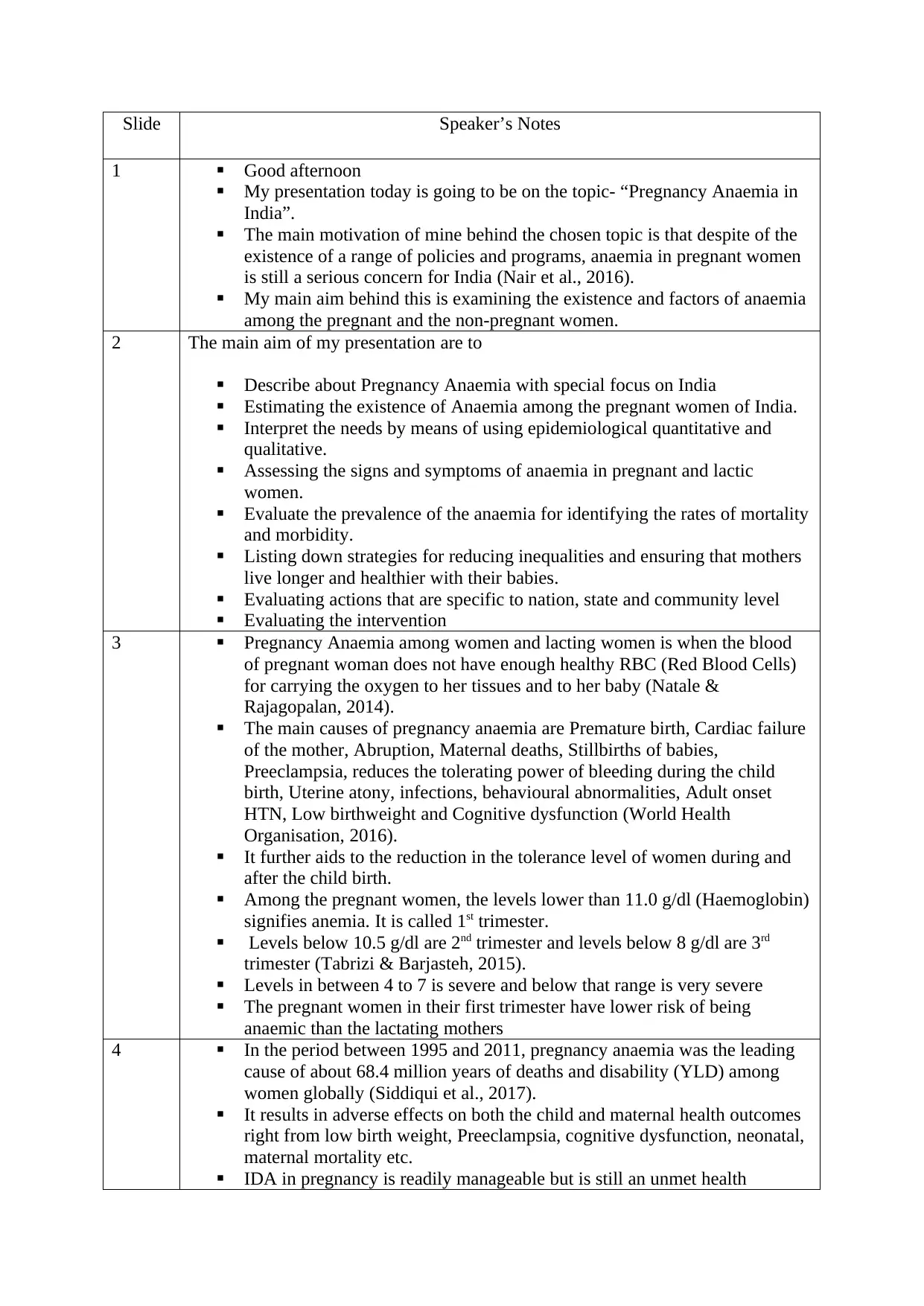
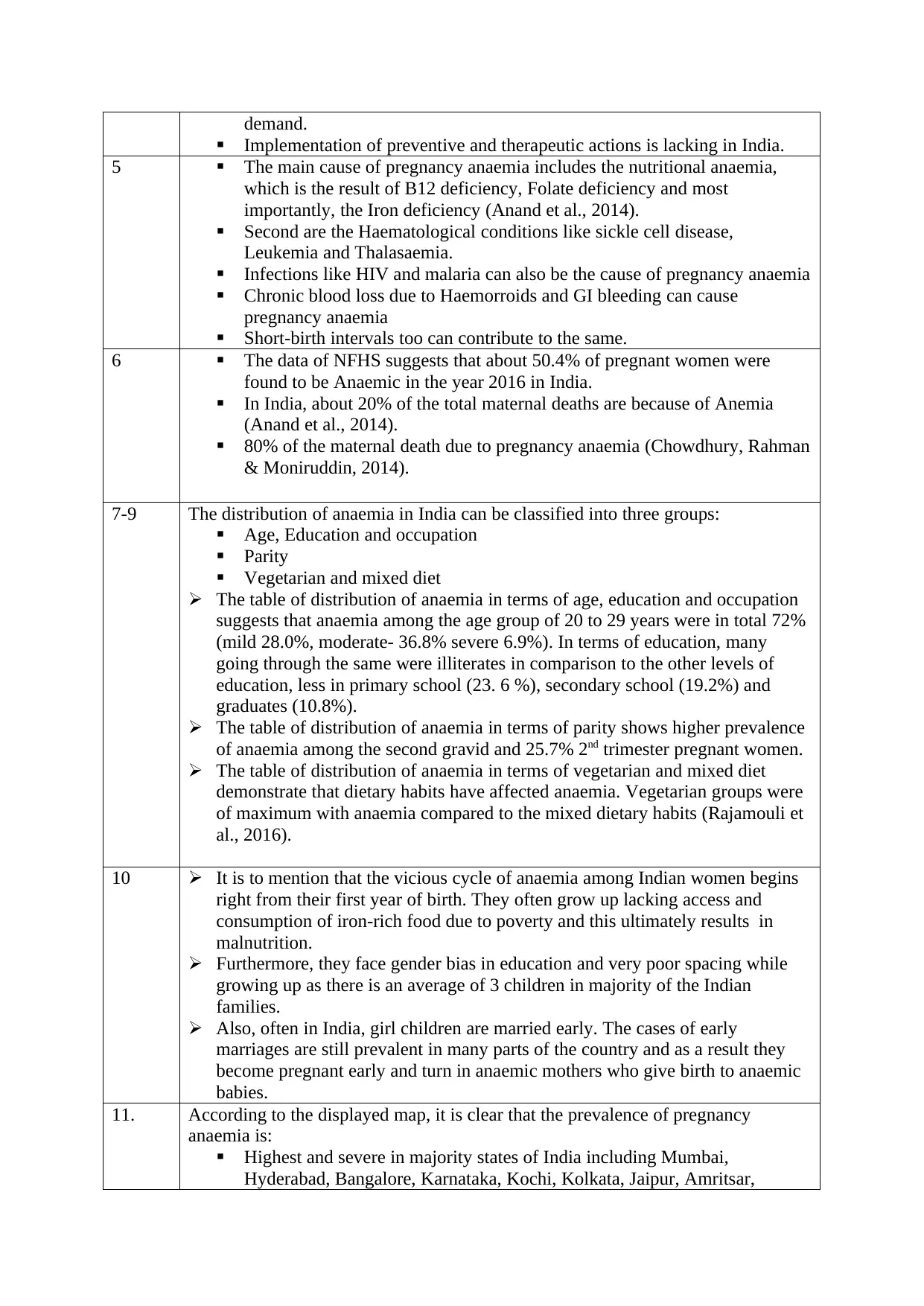
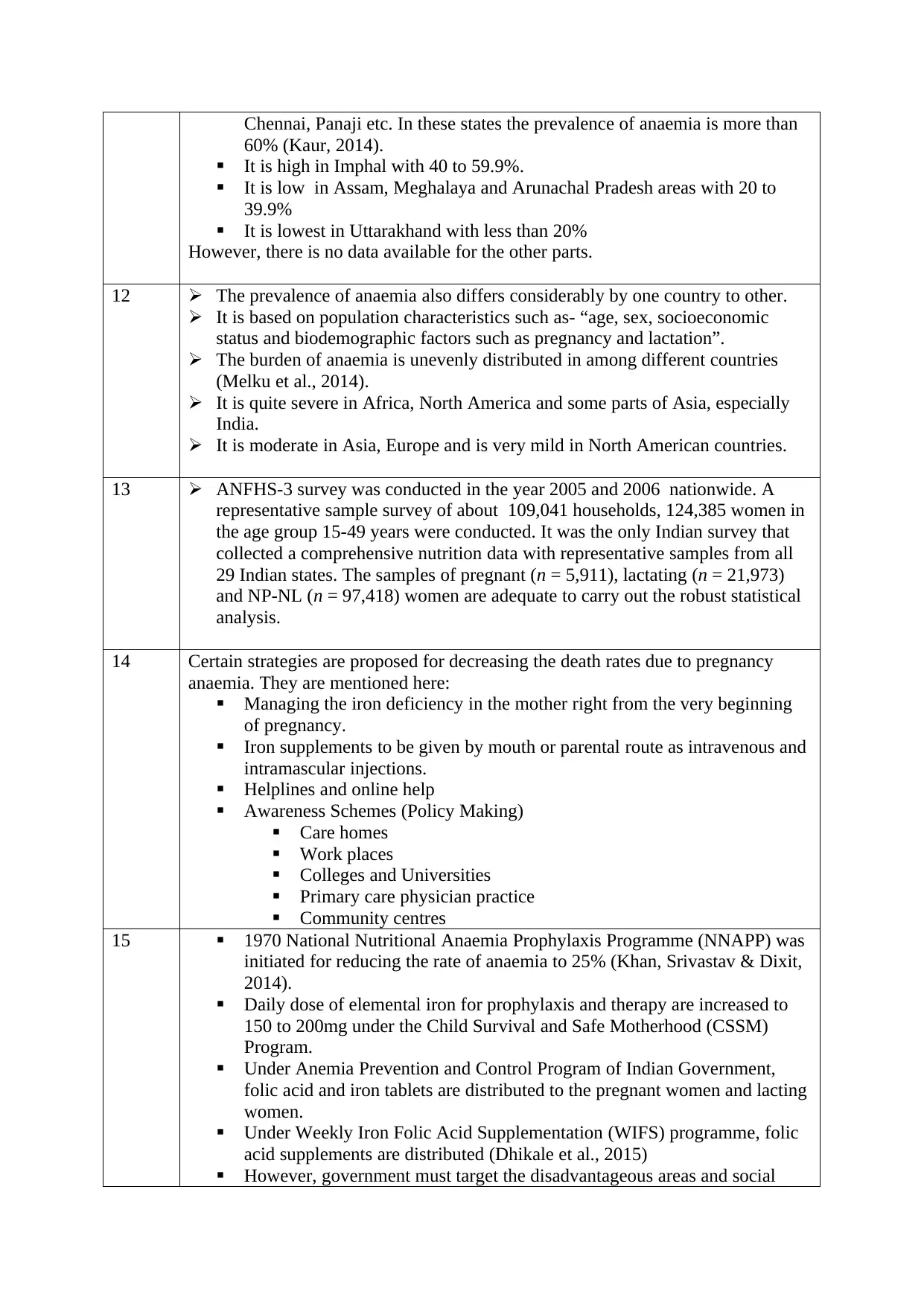
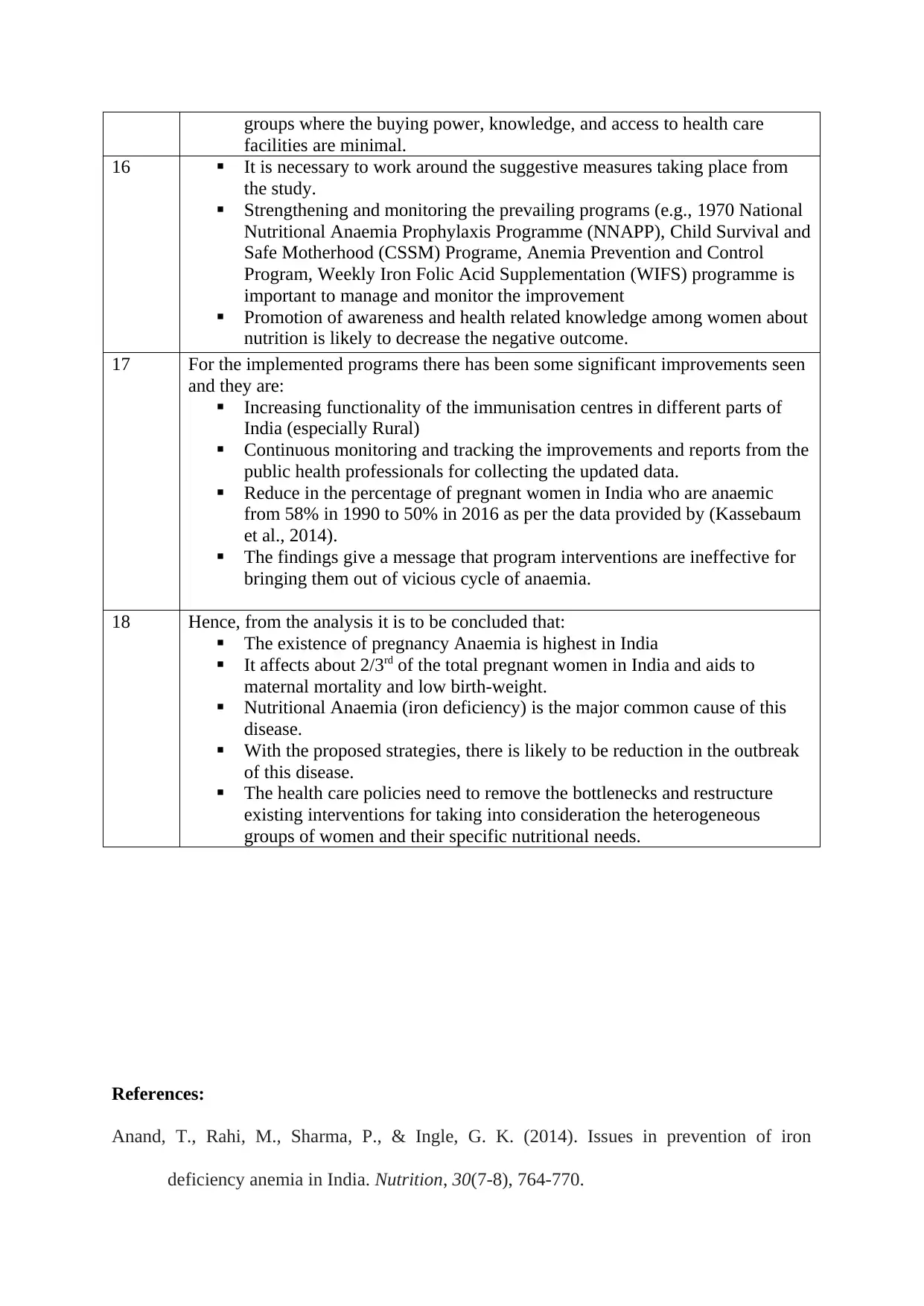
This presentation addresses the significant public health issue of pregnancy anemia in India. It begins by defining pregnancy anemia, emphasizing its impact on maternal and child health. The presentation explores the causes, including nutritional deficiencies (particularly iron, folate, and B12) and other contributing factors. It delves into epidemiological data, highlighting prevalence rates across different regions and demographic groups within India. The presentation analyzes the distribution of anemia based on age, education, occupation, and dietary habits. It also examines the vicious cycle of anemia, starting from early childhood and the impact of socio-economic factors. The presentation further discusses the global and regional burden of anemia, along with the existing strategies and programs implemented to combat the issue. It proposes specific interventions, including iron supplementation, awareness campaigns, and strengthening existing programs. The presentation concludes by summarizing the key findings, emphasizing the need for tailored interventions and policy adjustments to address the specific needs of vulnerable populations, ultimately aiming to reduce maternal mortality and improve birth outcomes.
1 out of 6
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.