Understanding and Managing Low Back Pain
VerifiedAdded on 2020/05/04
|14
|3824
|80
AI Summary
This assignment delves into the complex issue of low back pain. It examines the various causes, including stress fractures, sports injuries, and osteoporosis. The assignment also explores diagnostic techniques used to identify the root cause of low back pain. Furthermore, it discusses various treatment options, ranging from conservative management strategies like physical therapy to surgical interventions in severe cases. The focus is on providing a comprehensive understanding of low back pain and effective approaches to its management.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: STRESS FRACTURE OF LUMBAR SPINE
STRESS FRACTURE OF LUMBAR SPINE
Name of the Student
Student number
Word Count - 2229
STRESS FRACTURE OF LUMBAR SPINE
Name of the Student
Student number
Word Count - 2229
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1STRESS FRACTURE OF LUMBAR SPINE
Executive Summary
Overexertion of the lumbar spine, particularly L5 can give rise to the generation of small
fractures. Large number of micro fractures, causes inability of the vertebrae to absorb shocks
resulting in pain of the lower back. It is associated with sports like football, gymnastics, among
others. Diagnosis generally involves X-rays, radiographs, MRI, CT scan, SPECT, among others.
Various treatments are available, which involve proper rest and consumption of NSAIDs, to
relieve pain. Back braces are also used. Surgical treatments involve the spinal fusion technique.
Following treatment, the athlete is advised to participate in a rehabilitation program, which
involves physical therapy under the guidance of an experienced physiotherapist. Sufficient rest
and nutritional supplementation help to prevent lumbar spine. Thus, stress fractures if severe and
not diagnosed on time can give rise to serious consequences and affect the athlete’s ability to
participate in games.
Executive Summary
Overexertion of the lumbar spine, particularly L5 can give rise to the generation of small
fractures. Large number of micro fractures, causes inability of the vertebrae to absorb shocks
resulting in pain of the lower back. It is associated with sports like football, gymnastics, among
others. Diagnosis generally involves X-rays, radiographs, MRI, CT scan, SPECT, among others.
Various treatments are available, which involve proper rest and consumption of NSAIDs, to
relieve pain. Back braces are also used. Surgical treatments involve the spinal fusion technique.
Following treatment, the athlete is advised to participate in a rehabilitation program, which
involves physical therapy under the guidance of an experienced physiotherapist. Sufficient rest
and nutritional supplementation help to prevent lumbar spine. Thus, stress fractures if severe and
not diagnosed on time can give rise to serious consequences and affect the athlete’s ability to
participate in games.
2STRESS FRACTURE OF LUMBAR SPINE
Table of Contents
Introduction......................................................................................................................................3
Classification and Diagnosis............................................................................................................4
Treatment and Rehabilitation..........................................................................................................7
Prevention measures........................................................................................................................8
Conclusion.....................................................................................................................................10
Reference List................................................................................................................................12
Table of Contents
Introduction......................................................................................................................................3
Classification and Diagnosis............................................................................................................4
Treatment and Rehabilitation..........................................................................................................7
Prevention measures........................................................................................................................8
Conclusion.....................................................................................................................................10
Reference List................................................................................................................................12
3STRESS FRACTURE OF LUMBAR SPINE
Introduction
This report is based on football-associated stress fracture of the lumbar spine. Football is
the world’s most loved game. It’s history dates back to more than a century. It began in the year
1863 when Football Association of England was first formed. It was the first body formed to
govern the sports (Walvin, 2014). The earliest form of the game dates back to the Han dynasty of
China. Another variation of the game originated in the Far East as well and this was named the
‘Kemari’, which originated in Japan. Moreover, the Greeks and the Romans also had other
variations to this game like the ‘Episkryos’ and the ‘Harpastum’, respectively (Ryynänen, 2015).
In 1882, the football related associations in England collaborated to create the International
Football Association Board (IFAB). FIFA was established in the year 1904 in Paris and it
became a part of IFAB in the year 1913. At that time, FIFA had only 7 countries as its members
but now it consists of 208 members. This game involves the participation of 11 players from
each team. The players need to maneuver the ball and hit it inside the opposition’s goal post.
This game involves the skillful use of one’s legs and feet and as a result, it is associated with a
number of injuries (Sorez, 2012).
Knee injuries are the most common form of injuries associated with football. Knee
injuries involve the anterior cruciate ligament and the medial collateral ligament injuries. Others
include ankle sprains, torn meniscus, torn hamstrings, muscle contusions, shoulder dislocation
and shoulder tendinitis (Whittaker et al., 2015). Stress fracture of the lumbar spine is another
type of injury associated with football. This is medically known as Spondylolysis. It is caused
due to overuse of one’s lower back. It is the most common form of injury to the lower back
associated with various games including football. It occurs in the lowermost lumbar vertebra
Introduction
This report is based on football-associated stress fracture of the lumbar spine. Football is
the world’s most loved game. It’s history dates back to more than a century. It began in the year
1863 when Football Association of England was first formed. It was the first body formed to
govern the sports (Walvin, 2014). The earliest form of the game dates back to the Han dynasty of
China. Another variation of the game originated in the Far East as well and this was named the
‘Kemari’, which originated in Japan. Moreover, the Greeks and the Romans also had other
variations to this game like the ‘Episkryos’ and the ‘Harpastum’, respectively (Ryynänen, 2015).
In 1882, the football related associations in England collaborated to create the International
Football Association Board (IFAB). FIFA was established in the year 1904 in Paris and it
became a part of IFAB in the year 1913. At that time, FIFA had only 7 countries as its members
but now it consists of 208 members. This game involves the participation of 11 players from
each team. The players need to maneuver the ball and hit it inside the opposition’s goal post.
This game involves the skillful use of one’s legs and feet and as a result, it is associated with a
number of injuries (Sorez, 2012).
Knee injuries are the most common form of injuries associated with football. Knee
injuries involve the anterior cruciate ligament and the medial collateral ligament injuries. Others
include ankle sprains, torn meniscus, torn hamstrings, muscle contusions, shoulder dislocation
and shoulder tendinitis (Whittaker et al., 2015). Stress fracture of the lumbar spine is another
type of injury associated with football. This is medically known as Spondylolysis. It is caused
due to overuse of one’s lower back. It is the most common form of injury to the lower back
associated with various games including football. It occurs in the lowermost lumbar vertebra
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4STRESS FRACTURE OF LUMBAR SPINE
named L5 (Kobayashi et al., 2013). The L5 is situated at the junction of the lumbar spine and the
pelvis. This part remains highly stresses during various physical activities, which involves
continuous moving and maneuvering. Heavy muscular forces can cause the micro fractures in the
lumbar spine. It involves severe pain in the lower back. This causes restrictions in the movement
of the player (Murthy, 2012).
This report describes the football-associated injury termed Spondylolysis or stress
fracture of lumbar spine. Firstly, it provides a classification of stress fractures, diagnosis and the
causes associated with this type of injury. Secondly, it provides treatment and rehabilitation
programs. Lastly, it provides a prevention measures associated with the injury.
Classification and Diagnosis
Lumbar spine provides support and stability to the upper part of the body. An injury to
this region changes the lumbar vertebral shape, thereby affecting the posture. Spondylolysis can
be classified as (1) dysplastic, which is usually congenital, (2) degenerative, which is generally
associated with old age, (3) isthmic, which is usually associated with sports, (4) traumatic, which
occurs following previous fractures and (5) pathologic, which involves either a localized or
generalized disease of the bone. Dysplastic spondylolysis occurs as a result of abnormalities
present in the pper scarum or it involves the arch present in the L5. Isthmic Spondylolysis occurs
because of lesion development, which can cause a lytic-fatige fracture of pars. Degenerative
spondylolysis involves instability of the pars segments (Long & Whang, 2015).
X-Rays are not useful to detect early stages of stress fractures of the lumbar spine. X-rays
can only detect them at the late stages when it is beyond treatment. A radiograph helps to
identify compression fracture of the vertebra (Cicala et al., 2013). It also helps to determine the
named L5 (Kobayashi et al., 2013). The L5 is situated at the junction of the lumbar spine and the
pelvis. This part remains highly stresses during various physical activities, which involves
continuous moving and maneuvering. Heavy muscular forces can cause the micro fractures in the
lumbar spine. It involves severe pain in the lower back. This causes restrictions in the movement
of the player (Murthy, 2012).
This report describes the football-associated injury termed Spondylolysis or stress
fracture of lumbar spine. Firstly, it provides a classification of stress fractures, diagnosis and the
causes associated with this type of injury. Secondly, it provides treatment and rehabilitation
programs. Lastly, it provides a prevention measures associated with the injury.
Classification and Diagnosis
Lumbar spine provides support and stability to the upper part of the body. An injury to
this region changes the lumbar vertebral shape, thereby affecting the posture. Spondylolysis can
be classified as (1) dysplastic, which is usually congenital, (2) degenerative, which is generally
associated with old age, (3) isthmic, which is usually associated with sports, (4) traumatic, which
occurs following previous fractures and (5) pathologic, which involves either a localized or
generalized disease of the bone. Dysplastic spondylolysis occurs as a result of abnormalities
present in the pper scarum or it involves the arch present in the L5. Isthmic Spondylolysis occurs
because of lesion development, which can cause a lytic-fatige fracture of pars. Degenerative
spondylolysis involves instability of the pars segments (Long & Whang, 2015).
X-Rays are not useful to detect early stages of stress fractures of the lumbar spine. X-rays
can only detect them at the late stages when it is beyond treatment. A radiograph helps to
identify compression fracture of the vertebra (Cicala et al., 2013). It also helps to determine the
5STRESS FRACTURE OF LUMBAR SPINE
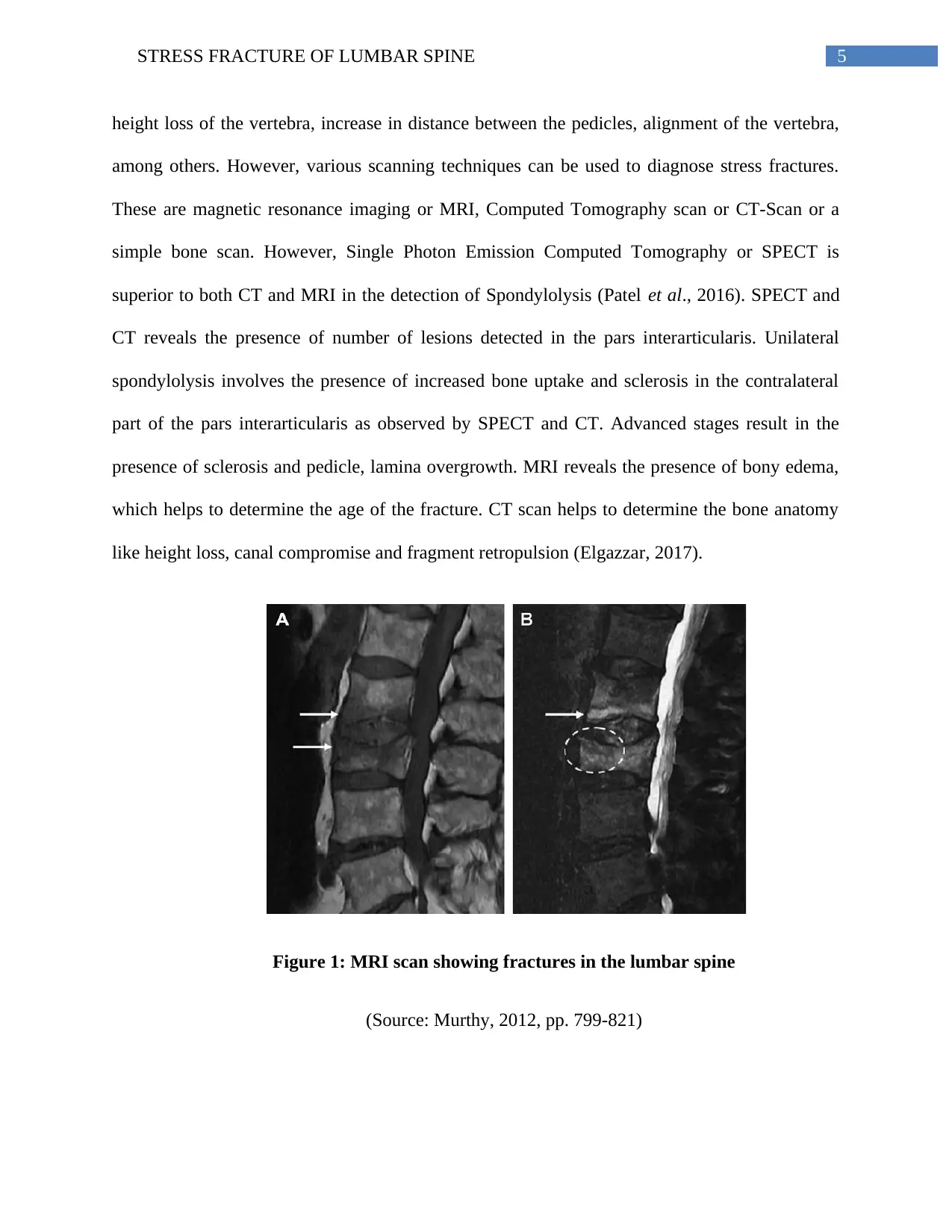
height loss of the vertebra, increase in distance between the pedicles, alignment of the vertebra,
among others. However, various scanning techniques can be used to diagnose stress fractures.
These are magnetic resonance imaging or MRI, Computed Tomography scan or CT-Scan or a
simple bone scan. However, Single Photon Emission Computed Tomography or SPECT is
superior to both CT and MRI in the detection of Spondylolysis (Patel et al., 2016). SPECT and
CT reveals the presence of number of lesions detected in the pars interarticularis. Unilateral
spondylolysis involves the presence of increased bone uptake and sclerosis in the contralateral
part of the pars interarticularis as observed by SPECT and CT. Advanced stages result in the
presence of sclerosis and pedicle, lamina overgrowth. MRI reveals the presence of bony edema,
which helps to determine the age of the fracture. CT scan helps to determine the bone anatomy
like height loss, canal compromise and fragment retropulsion (Elgazzar, 2017).
Figure 1: MRI scan showing fractures in the lumbar spine
(Source: Murthy, 2012, pp. 799-821)
height loss of the vertebra, increase in distance between the pedicles, alignment of the vertebra,
among others. However, various scanning techniques can be used to diagnose stress fractures.
These are magnetic resonance imaging or MRI, Computed Tomography scan or CT-Scan or a
simple bone scan. However, Single Photon Emission Computed Tomography or SPECT is
superior to both CT and MRI in the detection of Spondylolysis (Patel et al., 2016). SPECT and
CT reveals the presence of number of lesions detected in the pars interarticularis. Unilateral
spondylolysis involves the presence of increased bone uptake and sclerosis in the contralateral
part of the pars interarticularis as observed by SPECT and CT. Advanced stages result in the
presence of sclerosis and pedicle, lamina overgrowth. MRI reveals the presence of bony edema,
which helps to determine the age of the fracture. CT scan helps to determine the bone anatomy
like height loss, canal compromise and fragment retropulsion (Elgazzar, 2017).
Figure 1: MRI scan showing fractures in the lumbar spine
(Source: Murthy, 2012, pp. 799-821)
6STRESS FRACTURE OF LUMBAR SPINE
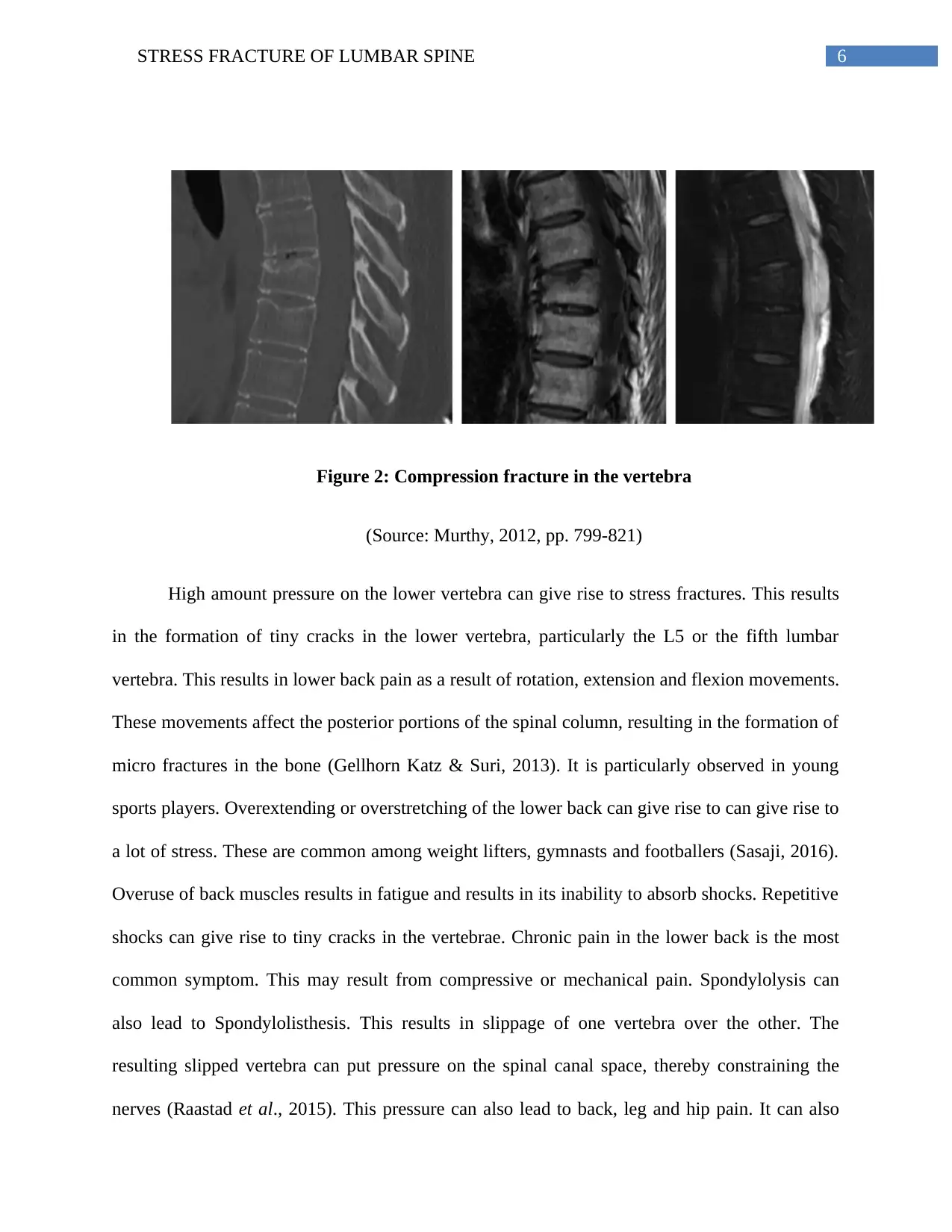
Figure 2: Compression fracture in the vertebra
(Source: Murthy, 2012, pp. 799-821)
High amount pressure on the lower vertebra can give rise to stress fractures. This results
in the formation of tiny cracks in the lower vertebra, particularly the L5 or the fifth lumbar
vertebra. This results in lower back pain as a result of rotation, extension and flexion movements.
These movements affect the posterior portions of the spinal column, resulting in the formation of
micro fractures in the bone (Gellhorn Katz & Suri, 2013). It is particularly observed in young
sports players. Overextending or overstretching of the lower back can give rise to can give rise to
a lot of stress. These are common among weight lifters, gymnasts and footballers (Sasaji, 2016).
Overuse of back muscles results in fatigue and results in its inability to absorb shocks. Repetitive
shocks can give rise to tiny cracks in the vertebrae. Chronic pain in the lower back is the most
common symptom. This may result from compressive or mechanical pain. Spondylolysis can
also lead to Spondylolisthesis. This results in slippage of one vertebra over the other. The
resulting slipped vertebra can put pressure on the spinal canal space, thereby constraining the
nerves (Raastad et al., 2015). This pressure can also lead to back, leg and hip pain. It can also
Figure 2: Compression fracture in the vertebra
(Source: Murthy, 2012, pp. 799-821)
High amount pressure on the lower vertebra can give rise to stress fractures. This results
in the formation of tiny cracks in the lower vertebra, particularly the L5 or the fifth lumbar
vertebra. This results in lower back pain as a result of rotation, extension and flexion movements.
These movements affect the posterior portions of the spinal column, resulting in the formation of
micro fractures in the bone (Gellhorn Katz & Suri, 2013). It is particularly observed in young
sports players. Overextending or overstretching of the lower back can give rise to can give rise to
a lot of stress. These are common among weight lifters, gymnasts and footballers (Sasaji, 2016).
Overuse of back muscles results in fatigue and results in its inability to absorb shocks. Repetitive
shocks can give rise to tiny cracks in the vertebrae. Chronic pain in the lower back is the most
common symptom. This may result from compressive or mechanical pain. Spondylolysis can
also lead to Spondylolisthesis. This results in slippage of one vertebra over the other. The
resulting slipped vertebra can put pressure on the spinal canal space, thereby constraining the
nerves (Raastad et al., 2015). This pressure can also lead to back, leg and hip pain. It can also
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7STRESS FRACTURE OF LUMBAR SPINE
result in numbness of the feet. Other factors that can cause stress fractures are the genetic
constitution of an individual and osteoporosis.
Treatment and Rehabilitation
An effective and acute treatment program is needed for players suffering from stress
fractures of the lumbar spine. The treatment usually begins after diagnosis and involves
advocating of complete rest to the athlete. The player is needed to stop the various routine
exercises and any movements that may cause in pain development. If the pain continues after 3
weeks, it means that the player in getting insufficient rest or may need the support of a back
brace. Back braces help to maintain the proper positioning of the back in order to speed up the
healing process (Lee et al., 2012). Periodic X-Rays are needed to determine if the back is in
proper position. If non-surgical treatment does not help to keep the back in proper position, a
spinal fusion is recommended. In this procedure, screws and rods are used which helps to keep
the vertebra in the proper position alongside the healing process. This in turn helps to stop the
motion of a a vertebral segment, thereby reducing the pain (Wu et al., 2012). However, there are
risks involved with this procedure, which involves infection, bleeding, blood vessel injury and
poor healing of wounds. Moreover, ibuprofen, which is an inhibitor of inflammation, can be used
to heal the pain. Apart from the use of various nonsteroidal anti-inflammatory drugs (NSAIDs),
muscle relaxants can also be used (Patrick, Emanski & Knaub, 2016). Medications directed
against narcotic pain and against neuropathic pain (like tricyclic antidepressants) can be used.
Other techniques for treatment of pain involve analgesic patches, which are localized and
intercostals nerve blocks or transcutaneous nerve stimulatory units (Wong & McGirt, 2013).
result in numbness of the feet. Other factors that can cause stress fractures are the genetic
constitution of an individual and osteoporosis.
Treatment and Rehabilitation
An effective and acute treatment program is needed for players suffering from stress
fractures of the lumbar spine. The treatment usually begins after diagnosis and involves
advocating of complete rest to the athlete. The player is needed to stop the various routine
exercises and any movements that may cause in pain development. If the pain continues after 3
weeks, it means that the player in getting insufficient rest or may need the support of a back
brace. Back braces help to maintain the proper positioning of the back in order to speed up the
healing process (Lee et al., 2012). Periodic X-Rays are needed to determine if the back is in
proper position. If non-surgical treatment does not help to keep the back in proper position, a
spinal fusion is recommended. In this procedure, screws and rods are used which helps to keep
the vertebra in the proper position alongside the healing process. This in turn helps to stop the
motion of a a vertebral segment, thereby reducing the pain (Wu et al., 2012). However, there are
risks involved with this procedure, which involves infection, bleeding, blood vessel injury and
poor healing of wounds. Moreover, ibuprofen, which is an inhibitor of inflammation, can be used
to heal the pain. Apart from the use of various nonsteroidal anti-inflammatory drugs (NSAIDs),
muscle relaxants can also be used (Patrick, Emanski & Knaub, 2016). Medications directed
against narcotic pain and against neuropathic pain (like tricyclic antidepressants) can be used.
Other techniques for treatment of pain involve analgesic patches, which are localized and
intercostals nerve blocks or transcutaneous nerve stimulatory units (Wong & McGirt, 2013).
8STRESS FRACTURE OF LUMBAR SPINE
The rehabilitation program begins after the treatment phase. If the pain subsides and the
player is able to perform daily activities, the athlete is allowed to progress to the rehabilitation
program. The rehabilitation program begins in the second month after diagnosis, since the first
month is associated with various surgical or non-surgical treatments. The rehabilitation program
is characterized by physical therapy with the help of an experienced physiotherapist (Peterson &
Renstrom, 2016). Physical therapy involves various exercises like the lumbar and core exercises
for stabilization, core exercises for generation of core stability, exercises that strengthen the legs
and the hips. Other exercises involve postural taping, soft tissue massaging and Spinal
Proprioceptive Extension Exercise Dynamic Program (SPEED) (Papa, 2012). Moreover, these
exercises also help to make the muscles flexible to allow proper movement. Exercise programs
can also be designed to enable the players to practice at home. Activities that provide lesser
amounts of stress can be introduced. However, activities that put a lot of pressure on the spine
like rotation or back arching is avoided. If the player is able to carry out the physical therapy and
the low stress activities, then they are allowed to progress to the third phase of the rehabilitation
program. The third phase involves continuation of the exercise programs both at home and at the
rehabilitation center. Physical therapy exercises are also increased. The players are allowed to
return to their sports, however, it is a gradual and progressive return, which involves a set of
parameters and guidelines set out by the medical practitioner or physiotherapist (Garet et al.,
2013). However, participation in the sport should not be carried out on consecutive days. On
reoccurrence of pain, the activities and exercises are needed to be reduced.
Prevention measures
Stress fracture of the lumbar spine usually causes lower back pain that occurs on one side
of the back rather than the center (Lotz, Fields & Liebenberg, 2013). It occurs as a mild pain in
The rehabilitation program begins after the treatment phase. If the pain subsides and the
player is able to perform daily activities, the athlete is allowed to progress to the rehabilitation
program. The rehabilitation program begins in the second month after diagnosis, since the first
month is associated with various surgical or non-surgical treatments. The rehabilitation program
is characterized by physical therapy with the help of an experienced physiotherapist (Peterson &
Renstrom, 2016). Physical therapy involves various exercises like the lumbar and core exercises
for stabilization, core exercises for generation of core stability, exercises that strengthen the legs
and the hips. Other exercises involve postural taping, soft tissue massaging and Spinal
Proprioceptive Extension Exercise Dynamic Program (SPEED) (Papa, 2012). Moreover, these
exercises also help to make the muscles flexible to allow proper movement. Exercise programs
can also be designed to enable the players to practice at home. Activities that provide lesser
amounts of stress can be introduced. However, activities that put a lot of pressure on the spine
like rotation or back arching is avoided. If the player is able to carry out the physical therapy and
the low stress activities, then they are allowed to progress to the third phase of the rehabilitation
program. The third phase involves continuation of the exercise programs both at home and at the
rehabilitation center. Physical therapy exercises are also increased. The players are allowed to
return to their sports, however, it is a gradual and progressive return, which involves a set of
parameters and guidelines set out by the medical practitioner or physiotherapist (Garet et al.,
2013). However, participation in the sport should not be carried out on consecutive days. On
reoccurrence of pain, the activities and exercises are needed to be reduced.
Prevention measures
Stress fracture of the lumbar spine usually causes lower back pain that occurs on one side
of the back rather than the center (Lotz, Fields & Liebenberg, 2013). It occurs as a mild pain in
9STRESS FRACTURE OF LUMBAR SPINE
the beginning and progresses to chronic pain following activities like jumping, running, kicking,
among others. This is mostly common among young athletes like footballers. However, various
preventative measures can be followed to avoid the development of stress fractures in the lumbar
spine. These are:
(1) Maintenance of good physical condition during off seasons and not overexerting oneself
during the peak seasons.
(2) Activities that require high impact like jumping, running, rotation and back arching
should be increased in a gradual manner.
(3) It is necessary to take day-offs in order to give rest to the back muscles and the body as a
whole.
(4) It is necessary to avoid participating in the sport throughout the year, as it puts a lot of
pressure on the muscles and the vertebra.
(5) Maintenance of good flexibility of the hip and hamstring flexors, strength of the core,
lumbar and abdominal muscles.
(6) Female athletes should be checked to determine their bone mass density (BMD), which
helps to understand the quality of their bone health (Chen, Tenforde & Fredericson,
2013).
(7) Calcium and Vitamin D supplementation can also help to prevent stress fracture.
(8) Orthotic devices can prevent lower back stress fractures by shock absorptions. Insoles
that absorb shocks are very effective in preventing stress fractures (Kendall, Bird &
Azari, 2014).
the beginning and progresses to chronic pain following activities like jumping, running, kicking,
among others. This is mostly common among young athletes like footballers. However, various
preventative measures can be followed to avoid the development of stress fractures in the lumbar
spine. These are:
(1) Maintenance of good physical condition during off seasons and not overexerting oneself
during the peak seasons.
(2) Activities that require high impact like jumping, running, rotation and back arching
should be increased in a gradual manner.
(3) It is necessary to take day-offs in order to give rest to the back muscles and the body as a
whole.
(4) It is necessary to avoid participating in the sport throughout the year, as it puts a lot of
pressure on the muscles and the vertebra.
(5) Maintenance of good flexibility of the hip and hamstring flexors, strength of the core,
lumbar and abdominal muscles.
(6) Female athletes should be checked to determine their bone mass density (BMD), which
helps to understand the quality of their bone health (Chen, Tenforde & Fredericson,
2013).
(7) Calcium and Vitamin D supplementation can also help to prevent stress fracture.
(8) Orthotic devices can prevent lower back stress fractures by shock absorptions. Insoles
that absorb shocks are very effective in preventing stress fractures (Kendall, Bird &
Azari, 2014).
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10STRESS FRACTURE OF LUMBAR SPINE
Other injuries like those in the ankle can be prevented by the use of balance boards and
proprioceptive training. Strengthening programs help to reduce hamstring, knee and groin
sprains.
Conclusion
Lumbar spine generally provides support to the entire upper part of the body. However,
continuous strains on the lower vertebra, particularly L5 can give rise to the generation of small
fractures. Continuous pressure through various exercises and continuous tournaments lead to the
development of a large number of these micro fractures, which eventually results in inability of
the vertebrae to absorb shocks causing pain of the lower back. Initially mild pain ensues, which
then progresses to severe and chronic pain. The player is unable to carry out normal movements
and carry on with their game. With the appearance of mild pain, it is essential for the player to
consult a medical practitioner for proper diagnosis. Diagnosis generally involves X-rays,
radiographs, MRI, CT scan, SPECT, among others. Such stress fractures of the lumbar spine are
generally observed among the athletes who perform gymnastics, weight lifting, footballers, and
cricketers, among others. Such athletes require rotation and arching of their backs continuously.
Various treatments that are available involve proper rest and consumption of NSAIDs, in order
to relieve the pain. However, back braces can also be used. Surgical treatments involve the spinal
fusion technique, which employs screws and rods to keep the vertebra in proper position,
preventing it from slipping. Following treatment, the athlete is advised to participate in a
rehabilitation program, which involves physical therapy under the guidance of an experienced
physiotherapist. Moreover, it involves various exercises that help to stabilize and strengthen the
core, lumbar, legs and hip muscles. Other techniques are postural taping, soft tissue massage and
SPEED programs. However, it is necessary for the athletes to prevent such occurrence of stress
Other injuries like those in the ankle can be prevented by the use of balance boards and
proprioceptive training. Strengthening programs help to reduce hamstring, knee and groin
sprains.
Conclusion
Lumbar spine generally provides support to the entire upper part of the body. However,
continuous strains on the lower vertebra, particularly L5 can give rise to the generation of small
fractures. Continuous pressure through various exercises and continuous tournaments lead to the
development of a large number of these micro fractures, which eventually results in inability of
the vertebrae to absorb shocks causing pain of the lower back. Initially mild pain ensues, which
then progresses to severe and chronic pain. The player is unable to carry out normal movements
and carry on with their game. With the appearance of mild pain, it is essential for the player to
consult a medical practitioner for proper diagnosis. Diagnosis generally involves X-rays,
radiographs, MRI, CT scan, SPECT, among others. Such stress fractures of the lumbar spine are
generally observed among the athletes who perform gymnastics, weight lifting, footballers, and
cricketers, among others. Such athletes require rotation and arching of their backs continuously.
Various treatments that are available involve proper rest and consumption of NSAIDs, in order
to relieve the pain. However, back braces can also be used. Surgical treatments involve the spinal
fusion technique, which employs screws and rods to keep the vertebra in proper position,
preventing it from slipping. Following treatment, the athlete is advised to participate in a
rehabilitation program, which involves physical therapy under the guidance of an experienced
physiotherapist. Moreover, it involves various exercises that help to stabilize and strengthen the
core, lumbar, legs and hip muscles. Other techniques are postural taping, soft tissue massage and
SPEED programs. However, it is necessary for the athletes to prevent such occurrence of stress
11STRESS FRACTURE OF LUMBAR SPINE
fractures in the future. The athlete needs to provide sufficient rest to his/her body in order to
prevent stress. Nutritional supplementations like calcium and vitamin D helps to prevent stress
fractures of the lumbar spine. Moreover, orthotic devices are also known to prevent development
of stress fractures in the future. Thus, from the above discussions it can be concluded that stress
fractures if severe and not diagnosed properly can give rise to serious consequences and affect
the ability of the athlete to participate in the game in the future.
fractures in the future. The athlete needs to provide sufficient rest to his/her body in order to
prevent stress. Nutritional supplementations like calcium and vitamin D helps to prevent stress
fractures of the lumbar spine. Moreover, orthotic devices are also known to prevent development
of stress fractures in the future. Thus, from the above discussions it can be concluded that stress
fractures if severe and not diagnosed properly can give rise to serious consequences and affect
the ability of the athlete to participate in the game in the future.
12STRESS FRACTURE OF LUMBAR SPINE
Reference List
Chen, Y. T., Tenforde, A. S., & Fredericson, M. (2013). Update on stress fractures in female
athletes: epidemiology, treatment, and prevention. Current reviews in musculoskeletal
medicine, 6(2), 173-181.
Cicala, D., Briganti, F., Casale, L., Rossi, C., Cagini, L., Cesarano, E., & Giganti, M. (2013).
Atraumatic vertebral compression fractures: differential diagnosis between benign
osteoporotic and malignant fractures by MRI. Musculoskeletal surgery, 97(2), 169-179.
Elgazzar, A. H. (2017). Diagnosis of Traumatic Disorders. In Orthopedic Nuclear Medicine (pp.
147-189). Springer, Cham.
Garet, M., Reiman, M. P., Mathers, J., & Sylvain, J. (2013). Nonoperative treatment in lumbar
spondylolysis and spondylolisthesis: a systematic review. Sports health, 5(3), 225-232.
Gellhorn, A. C., Katz, J. N., & Suri, P. (2013). Osteoarthritis of the spine: the facet joints. Nature
Reviews Rheumatology, 9(4), 216-224.
Kendall, J. C., Bird, A. R., & Azari, M. F. (2014). Foot posture, leg length discrepancy and low
back pain–Their relationship and clinical management using foot orthoses–An
overview. The Foot, 24(2), 75-80.
Kobayashi, A., Kobayashi, T., Kato, K., Higuchi, H., & Takagishi, K. (2013). Diagnosis of
radiographically occult lumbar spondylolysis in young athletes by magnetic resonance
imaging. The American journal of sports medicine, 41(1), 169-176.
Lee, H. M., Park, S. Y., Lee, S. H., Suh, S. W., & Hong, J. Y. (2012). Comparative analysis of
clinical outcomes in patients with osteoporotic vertebral compression fractures (OVCFs):
conservative treatment versus balloon kyphoplasty. The Spine Journal, 12(11), 998-1005.
Long III, W. D., & Whang, P. G. (2014). Adult Spondylolysis and Isthmic Spondylolisthesis.
In Spine Surgery Basics (pp. 229-238). Springer Berlin Heidelberg.
Lotz, J. C., Fields, A. J., & Liebenberg, E. C. (2013). The role of the vertebral end plate in low
back pain. Global spine journal, 3(03), 153-164.
Murthy, N. S. (2012). Imaging of stress fractures of the spine. Radiologic clinics of North
America, 50(4), 799-821.
Papa, J. A. (2012). Conservative management of a lumbar compression fracture in an
osteoporotic patient: a case report. The Journal of the Canadian Chiropractic
Association, 56(1), 29.
Patel, N. D., Broderick, D. F., Burns, J., Deshmukh, T. K., Fries, I. B., Harvey, H. B., &
O’Toole, J. E. (2016). ACR appropriateness criteria low back pain. Journal of the
American College of Radiology, 13(9), 1069-1078.
Reference List
Chen, Y. T., Tenforde, A. S., & Fredericson, M. (2013). Update on stress fractures in female
athletes: epidemiology, treatment, and prevention. Current reviews in musculoskeletal
medicine, 6(2), 173-181.
Cicala, D., Briganti, F., Casale, L., Rossi, C., Cagini, L., Cesarano, E., & Giganti, M. (2013).
Atraumatic vertebral compression fractures: differential diagnosis between benign
osteoporotic and malignant fractures by MRI. Musculoskeletal surgery, 97(2), 169-179.
Elgazzar, A. H. (2017). Diagnosis of Traumatic Disorders. In Orthopedic Nuclear Medicine (pp.
147-189). Springer, Cham.
Garet, M., Reiman, M. P., Mathers, J., & Sylvain, J. (2013). Nonoperative treatment in lumbar
spondylolysis and spondylolisthesis: a systematic review. Sports health, 5(3), 225-232.
Gellhorn, A. C., Katz, J. N., & Suri, P. (2013). Osteoarthritis of the spine: the facet joints. Nature
Reviews Rheumatology, 9(4), 216-224.
Kendall, J. C., Bird, A. R., & Azari, M. F. (2014). Foot posture, leg length discrepancy and low
back pain–Their relationship and clinical management using foot orthoses–An
overview. The Foot, 24(2), 75-80.
Kobayashi, A., Kobayashi, T., Kato, K., Higuchi, H., & Takagishi, K. (2013). Diagnosis of
radiographically occult lumbar spondylolysis in young athletes by magnetic resonance
imaging. The American journal of sports medicine, 41(1), 169-176.
Lee, H. M., Park, S. Y., Lee, S. H., Suh, S. W., & Hong, J. Y. (2012). Comparative analysis of
clinical outcomes in patients with osteoporotic vertebral compression fractures (OVCFs):
conservative treatment versus balloon kyphoplasty. The Spine Journal, 12(11), 998-1005.
Long III, W. D., & Whang, P. G. (2014). Adult Spondylolysis and Isthmic Spondylolisthesis.
In Spine Surgery Basics (pp. 229-238). Springer Berlin Heidelberg.
Lotz, J. C., Fields, A. J., & Liebenberg, E. C. (2013). The role of the vertebral end plate in low
back pain. Global spine journal, 3(03), 153-164.
Murthy, N. S. (2012). Imaging of stress fractures of the spine. Radiologic clinics of North
America, 50(4), 799-821.
Papa, J. A. (2012). Conservative management of a lumbar compression fracture in an
osteoporotic patient: a case report. The Journal of the Canadian Chiropractic
Association, 56(1), 29.
Patel, N. D., Broderick, D. F., Burns, J., Deshmukh, T. K., Fries, I. B., Harvey, H. B., &
O’Toole, J. E. (2016). ACR appropriateness criteria low back pain. Journal of the
American College of Radiology, 13(9), 1069-1078.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13STRESS FRACTURE OF LUMBAR SPINE
Patrick, N., Emanski, E., & Knaub, M. A. (2016). Acute and chronic low back pain. Medical
Clinics of North America, 100(1), 169-181.
Peterson, L., & Renstrom, P. A. (2016). Sports Injuries: Prevention, Treatment and
Rehabilitation. CRC Press.
Raastad, J., Reiman, M., Coeytaux, R., Ledbetter, L., & Goode, A. P. (2015, April). The
association between lumbar spine radiographic features and low back pain: A systematic
review and meta-analysis. In Seminars in arthritis and rheumatism (Vol. 44, No. 5, pp.
571-585). WB Saunders.
Ryynänen, J. (2015). The influence of match events on injury incidence during male World Cup
football-Epidemiological studies and video analysis of injuries.
Sasaji, T., Imaizumi, H., Takano, H., Saitoh, H., Murakami, T., Kanabuchi, R., & Sekiya, M.
(2016). Sacral Stress Fracture following the Bone Union of Lumbar Spondylolysis. Case
reports in medicine, 2016.
Sorez, J. (2012). A History of Football in Paris: Challenges Faced by Sport Practised within a
Capital City (1890–1940). The International Journal of the History of Sport, 29(8), 1125-
1140.
Walvin, J. (2014). The people's game: the history of football revisited. Random House.
Whittaker, J. L., Woodhouse, L. J., Nettel-Aguirre, A., & Emery, C. A. (2015). Outcomes
associated with early post-traumatic osteoarthritis and other negative health consequences
3–10 years following knee joint injury in youth sport. Osteoarthritis and cartilage, 23(7),
1122-1129.
Wong, C. C., & McGirt, M. J. (2013). Vertebral compression fractures: a review of current
management and multimodal therapy. Journal of multidisciplinary healthcare, 6, 205.
Wu, Z. X., Gong, F. T., Liu, L., Ma, Z. S., Zhang, Y., Zhao, X., & Sang, H. X. (2012). A
comparative study on screw loosening in osteoporotic lumbar spine fusion between
expandable and conventional pedicle screws. Archives of orthopaedic and trauma
surgery, 132(4), 471-476.
Patrick, N., Emanski, E., & Knaub, M. A. (2016). Acute and chronic low back pain. Medical
Clinics of North America, 100(1), 169-181.
Peterson, L., & Renstrom, P. A. (2016). Sports Injuries: Prevention, Treatment and
Rehabilitation. CRC Press.
Raastad, J., Reiman, M., Coeytaux, R., Ledbetter, L., & Goode, A. P. (2015, April). The
association between lumbar spine radiographic features and low back pain: A systematic
review and meta-analysis. In Seminars in arthritis and rheumatism (Vol. 44, No. 5, pp.
571-585). WB Saunders.
Ryynänen, J. (2015). The influence of match events on injury incidence during male World Cup
football-Epidemiological studies and video analysis of injuries.
Sasaji, T., Imaizumi, H., Takano, H., Saitoh, H., Murakami, T., Kanabuchi, R., & Sekiya, M.
(2016). Sacral Stress Fracture following the Bone Union of Lumbar Spondylolysis. Case
reports in medicine, 2016.
Sorez, J. (2012). A History of Football in Paris: Challenges Faced by Sport Practised within a
Capital City (1890–1940). The International Journal of the History of Sport, 29(8), 1125-
1140.
Walvin, J. (2014). The people's game: the history of football revisited. Random House.
Whittaker, J. L., Woodhouse, L. J., Nettel-Aguirre, A., & Emery, C. A. (2015). Outcomes
associated with early post-traumatic osteoarthritis and other negative health consequences
3–10 years following knee joint injury in youth sport. Osteoarthritis and cartilage, 23(7),
1122-1129.
Wong, C. C., & McGirt, M. J. (2013). Vertebral compression fractures: a review of current
management and multimodal therapy. Journal of multidisciplinary healthcare, 6, 205.
Wu, Z. X., Gong, F. T., Liu, L., Ma, Z. S., Zhang, Y., Zhao, X., & Sang, H. X. (2012). A
comparative study on screw loosening in osteoporotic lumbar spine fusion between
expandable and conventional pedicle screws. Archives of orthopaedic and trauma
surgery, 132(4), 471-476.
1 out of 14
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.