Sun Safety in Construction: Importance, Research, and Strategies
VerifiedAdded on 2023/06/10
|14
|8096
|129
AI Summary
This article discusses the importance of sun safety in construction, research on the topic, and different research strategies to tackle the issue. It includes a review of a published paper, literature review, analysis of qualitative and quantitative data, and types of research strategies. The article also provides initial research ideas and concludes with references and an appendix.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
SUN SAFETY IN CONSTRUCTION 1
Sun Safety in Construction
Sun Safety in Construction
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
SUN SAFETY IN CONSTRUCTION 2
Contents
Research on Sun Safety in construction.....................................................................................................................3
Review of Published paper........................................................................................................................................3
Literature Review......................................................................................................................................................3
Importance of literature review..................................................................................................................................3
Analysis of qualitative and quantitative data.............................................................................................................3
Qualitative data..........................................................................................................................................................3
Quantitative data........................................................................................................................................................4
Difference between Quantitative and Qualitative data...............................................................................................4
Types of research strategies.......................................................................................................................................4
Qualitative research strategy......................................................................................................................................4
Quantitative research strategy....................................................................................................................................4
Descriptive research strategy.....................................................................................................................................4
Analytic research strategy..........................................................................................................................................4
Applied research strategy..........................................................................................................................................4
Critical research strategy...........................................................................................................................................4
Initial research ideas..................................................................................................................................................4
Conclusion.................................................................................................................................................................5
References.................................................................................................................................................................6
Appendix................................................................................................................................................................... 7
Contents
Research on Sun Safety in construction.....................................................................................................................3
Review of Published paper........................................................................................................................................3
Literature Review......................................................................................................................................................3
Importance of literature review..................................................................................................................................3
Analysis of qualitative and quantitative data.............................................................................................................3
Qualitative data..........................................................................................................................................................3
Quantitative data........................................................................................................................................................4
Difference between Quantitative and Qualitative data...............................................................................................4
Types of research strategies.......................................................................................................................................4
Qualitative research strategy......................................................................................................................................4
Quantitative research strategy....................................................................................................................................4
Descriptive research strategy.....................................................................................................................................4
Analytic research strategy..........................................................................................................................................4
Applied research strategy..........................................................................................................................................4
Critical research strategy...........................................................................................................................................4
Initial research ideas..................................................................................................................................................4
Conclusion.................................................................................................................................................................5
References.................................................................................................................................................................6
Appendix................................................................................................................................................................... 7

SUN SAFETY IN CONSTRUCTION 3
Research on Sun Safety in construction
Review of Published paper
The title of this paper is Sun safety in construction: a UK intervention study was written by J. Houdmont, P. Madgwick, and
R. Randall. According to J. Houdmont, sun safety in UK construction has given skin cancer to sun exposure that is relative to
other occupational. The aim of this journal paper is to determine a change in sun safety knowledge and provide a proper
training to a construction worker. In which a number of intervention group that reported correct knowledge of sun safety was
not greater than to baseline. The biggest change in the intervention group is to use a shade when workers working in the sun
(Oxford academic, 2016).
Solar ultraviolet ray is the main reason to development of skin cancer problem. According to the data of 2010, solar ultraviolet
ray was responsible for around 90% of cases of melanoma in the UK. Skin cancer is a common problem in the UK, in
England around 56% increases in skin cancer between 2002 and 2011 (Parkin et al., 2011). The incidence rate of skin cancer
in the UK rising faster as compared to Europe. According to the THOR organization, industry workers in the UK whose age is
below 65 raised standardized ration as compared to all other industries. A total of 1279 workers completed baseline in which
around 71% of workers giving contact details. In the UK solar ultraviolet ray is main cause to raise skin cancer problem in
construction workers.
Literature Review
A literature review is a type of review article which includes knowledge, theoretical, and methodological of a particular topic.
A literature review is a type of scholarly paper which is used to give a review on a particular topic. It is also a part of a
graduate student, including in a journal article. A literature review is also provided research proposal of any journal paper.
There are four types of literature review used in research such as evaluative, instrumental, exploratory, and systematic review.
Importance of literature review
There are following importance of literature review-
Provide a brief summary of a research topic
Provide relationship of each work to other people
Identify a new path for prior research
Locate own research within the context
It creates a report with an audience
Identify data source of researched topic
Formulate research problem
Ultraviolet radiation is the main reason for skin cancer in the UK. It is calculated that UVR poses around 65% of skin cancer,
and around 99% of non-melanoma skin cancer (Armstrong, 2004). Scientists found links between MSC, NMSC, and sun
exposure, where MSC and BCC associated with sun and SSC is associated with chronic exposure (Berwick et al., 2009). In
UK skin cancer is a common type of problem, around 100,000 cases of non-melanoma cancer and around 12,818 cases of
melanoma cancer were found in 2010 (Cancer Research UK, 2012). In 2010, almost 2,749 people in the UK died from
melanoma skin cancer. According to cancer registration data, there were almost 5,440 skin cancer cases registered in England
(National Statistics, 2013).
Analysis of qualitative and quantitative data
Qualitative data
Qualitative data is defined as a data that approximates but it does not determine the properties, attributes, and characteristics
of a phenomenon. Qualitative data is used to determine where quantitative data defines. It is a type of information that is
unable to measure, and its analysis that which research performed last month. Qualitative data deals with an observation that
can be obtained through senses elements such as touch, taste, and hearing. There are many qualitative observations such as for
instance, textures, colors, and shape of an object. It cannot be expressed but generally considered on scales such as socieo
economic, religious preference, and gender.
Examples: Sight, touch, hearing, and taste.
Research on Sun Safety in construction
Review of Published paper
The title of this paper is Sun safety in construction: a UK intervention study was written by J. Houdmont, P. Madgwick, and
R. Randall. According to J. Houdmont, sun safety in UK construction has given skin cancer to sun exposure that is relative to
other occupational. The aim of this journal paper is to determine a change in sun safety knowledge and provide a proper
training to a construction worker. In which a number of intervention group that reported correct knowledge of sun safety was
not greater than to baseline. The biggest change in the intervention group is to use a shade when workers working in the sun
(Oxford academic, 2016).
Solar ultraviolet ray is the main reason to development of skin cancer problem. According to the data of 2010, solar ultraviolet
ray was responsible for around 90% of cases of melanoma in the UK. Skin cancer is a common problem in the UK, in
England around 56% increases in skin cancer between 2002 and 2011 (Parkin et al., 2011). The incidence rate of skin cancer
in the UK rising faster as compared to Europe. According to the THOR organization, industry workers in the UK whose age is
below 65 raised standardized ration as compared to all other industries. A total of 1279 workers completed baseline in which
around 71% of workers giving contact details. In the UK solar ultraviolet ray is main cause to raise skin cancer problem in
construction workers.
Literature Review
A literature review is a type of review article which includes knowledge, theoretical, and methodological of a particular topic.
A literature review is a type of scholarly paper which is used to give a review on a particular topic. It is also a part of a
graduate student, including in a journal article. A literature review is also provided research proposal of any journal paper.
There are four types of literature review used in research such as evaluative, instrumental, exploratory, and systematic review.
Importance of literature review
There are following importance of literature review-
Provide a brief summary of a research topic
Provide relationship of each work to other people
Identify a new path for prior research
Locate own research within the context
It creates a report with an audience
Identify data source of researched topic
Formulate research problem
Ultraviolet radiation is the main reason for skin cancer in the UK. It is calculated that UVR poses around 65% of skin cancer,
and around 99% of non-melanoma skin cancer (Armstrong, 2004). Scientists found links between MSC, NMSC, and sun
exposure, where MSC and BCC associated with sun and SSC is associated with chronic exposure (Berwick et al., 2009). In
UK skin cancer is a common type of problem, around 100,000 cases of non-melanoma cancer and around 12,818 cases of
melanoma cancer were found in 2010 (Cancer Research UK, 2012). In 2010, almost 2,749 people in the UK died from
melanoma skin cancer. According to cancer registration data, there were almost 5,440 skin cancer cases registered in England
(National Statistics, 2013).
Analysis of qualitative and quantitative data
Qualitative data
Qualitative data is defined as a data that approximates but it does not determine the properties, attributes, and characteristics
of a phenomenon. Qualitative data is used to determine where quantitative data defines. It is a type of information that is
unable to measure, and its analysis that which research performed last month. Qualitative data deals with an observation that
can be obtained through senses elements such as touch, taste, and hearing. There are many qualitative observations such as for
instance, textures, colors, and shape of an object. It cannot be expressed but generally considered on scales such as socieo
economic, religious preference, and gender.
Examples: Sight, touch, hearing, and taste.
SUN SAFETY IN CONSTRUCTION 4
Quantitative data
Quantitative data is defined as a data that can be verified and is responsible for statistical manipulation. It is used where
qualitative data describes. It can be expressed as a number; examples of quantitative data are a number of hours of study, and
scores archive in tests. It is used to verify any problem by producing numerical data which can be transforming into statistics
data. It includes different types of surveys such as online, paper, kiosk, and mobile surveys.
Examples: research on the percentage amount of elements on earth atmosphere, number of patients have to wait 2 hours in a
waiting room in a hospital, and research on the stock market of any company
Difference between Quantitative and Qualitative data
Quantitative data Qualitative data
It is used Exploratory method for
research
It is used Conclusive method for
research
Subjective approach Objective approach
Non-Statistical analysis Statistical analysis
Unstructured Structured
A small number of samples A large number of samples
There are many software’s through which qualitative data can be analyzed such as Atlas. ti, QDA Miner, SPSS, and
MAXQDA. There are three methods for qualitative data analysis such as thematic analysis, Statistical analysis, and text
analysis. For quantitative data there are two types of analysis can be used such as descriptive and inferential analysis.
Qualitative and quantitative data analysis is done in the above research. In this paper quantitative data like 56% increases in
the number of skin cancer patients were recorded in between 2001 and 2011. The person, whose age was under 65 years,
raised standardized ratio relative to other UK industries. The qualitative data like, skin cancer increased due to ultra violet rays
and it occurred more in case of workers, roofers, painter, and labourers in the building.
Types of research strategies
There are following types of strategies used in research-
Qualitative research strategy
It provides insights into a research problem and helps to achieve an objective of any research by different methods such as
observation, open-ended survey, focus group, an interview.
Quantitative research strategy
Examples of quantitative data are statistical, numeric, analysis of collected data, and mathematical.
Descriptive research strategy
It is used when any person wants to describe a situation, it observes the behavior of any community. It involves surveys, case
study, and observation. Example: the case study on the life of a cricketer.
Analytic research strategy
It involves the use of information and facts, for example, research on the condition of people in America after the 13 th
amendment.
Applied research strategy
The aim of any research strategy is to find a solution to a particular problem. It is applied by any organization or government
to determine the solution to a particular problem.
Critical research strategy
It is used to reveal any claim about the society. Using this research strategy, any person can pick conclusion of a particular
topic or culture. Example: A person researches and finds that Indian people are more racism than Nigerians in America.
Initial research ideas
In many organization or industries, some parts of EHS (environment, health, and safety) management are already placed such
as risk and policy assessment data’s. EHS management depends upon many factors such as a size of any organization, nature,
the condition of operation, and the hazards (Patel et al., 2010). There are many research ideas that are used for safety in
construction workers such as management responsibility for safety, clear roles, competence with responsibilities, balanced
priorities, proper training for safety in construction workers, operations authorization. According to above research, skin
cancer is a most common problem in the UK, the main cause of this problem is radiation generated by the sun. There are three
Quantitative data
Quantitative data is defined as a data that can be verified and is responsible for statistical manipulation. It is used where
qualitative data describes. It can be expressed as a number; examples of quantitative data are a number of hours of study, and
scores archive in tests. It is used to verify any problem by producing numerical data which can be transforming into statistics
data. It includes different types of surveys such as online, paper, kiosk, and mobile surveys.
Examples: research on the percentage amount of elements on earth atmosphere, number of patients have to wait 2 hours in a
waiting room in a hospital, and research on the stock market of any company
Difference between Quantitative and Qualitative data
Quantitative data Qualitative data
It is used Exploratory method for
research
It is used Conclusive method for
research
Subjective approach Objective approach
Non-Statistical analysis Statistical analysis
Unstructured Structured
A small number of samples A large number of samples
There are many software’s through which qualitative data can be analyzed such as Atlas. ti, QDA Miner, SPSS, and
MAXQDA. There are three methods for qualitative data analysis such as thematic analysis, Statistical analysis, and text
analysis. For quantitative data there are two types of analysis can be used such as descriptive and inferential analysis.
Qualitative and quantitative data analysis is done in the above research. In this paper quantitative data like 56% increases in
the number of skin cancer patients were recorded in between 2001 and 2011. The person, whose age was under 65 years,
raised standardized ratio relative to other UK industries. The qualitative data like, skin cancer increased due to ultra violet rays
and it occurred more in case of workers, roofers, painter, and labourers in the building.
Types of research strategies
There are following types of strategies used in research-
Qualitative research strategy
It provides insights into a research problem and helps to achieve an objective of any research by different methods such as
observation, open-ended survey, focus group, an interview.
Quantitative research strategy
Examples of quantitative data are statistical, numeric, analysis of collected data, and mathematical.
Descriptive research strategy
It is used when any person wants to describe a situation, it observes the behavior of any community. It involves surveys, case
study, and observation. Example: the case study on the life of a cricketer.
Analytic research strategy
It involves the use of information and facts, for example, research on the condition of people in America after the 13 th
amendment.
Applied research strategy
The aim of any research strategy is to find a solution to a particular problem. It is applied by any organization or government
to determine the solution to a particular problem.
Critical research strategy
It is used to reveal any claim about the society. Using this research strategy, any person can pick conclusion of a particular
topic or culture. Example: A person researches and finds that Indian people are more racism than Nigerians in America.
Initial research ideas
In many organization or industries, some parts of EHS (environment, health, and safety) management are already placed such
as risk and policy assessment data’s. EHS management depends upon many factors such as a size of any organization, nature,
the condition of operation, and the hazards (Patel et al., 2010). There are many research ideas that are used for safety in
construction workers such as management responsibility for safety, clear roles, competence with responsibilities, balanced
priorities, proper training for safety in construction workers, operations authorization. According to above research, skin
cancer is a most common problem in the UK, the main cause of this problem is radiation generated by the sun. There are three
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
SUN SAFETY IN CONSTRUCTION 5
types of radiation generated by the sun such as infra-red, visible light, and ultraviolet radiation. Ultraviolet radiation is the
main cause of skin cancer in the UK (Payne et al., 2013). There are many research ideas to avoid skin cancer in construction
workers such as using sunscreen, wear sunglasses, avoid mid-day, use policies and regulation, use EHS management and
policies to provide sun safety in construction workers, and wear long clothing (Safety and health practitioner, 2015).
Conclusion
A research proposal is a type of process which is used to propose a research idea, review of research, applying different types
of research strategies, and finding the result. In this research paper, one journal paper related to safety measures was discussed
and analyzed. Literature related to this paper was reviewed thoroughly. There are many types of research strategies are used
such as quantitative research, qualitative research, critical research, analytic research, and applied research. In this research
paper, two types of research strategies are analysed such as quantitative and qualitative research. Different types of research
idea related to safety, health, and environment were discussed.
types of radiation generated by the sun such as infra-red, visible light, and ultraviolet radiation. Ultraviolet radiation is the
main cause of skin cancer in the UK (Payne et al., 2013). There are many research ideas to avoid skin cancer in construction
workers such as using sunscreen, wear sunglasses, avoid mid-day, use policies and regulation, use EHS management and
policies to provide sun safety in construction workers, and wear long clothing (Safety and health practitioner, 2015).
Conclusion
A research proposal is a type of process which is used to propose a research idea, review of research, applying different types
of research strategies, and finding the result. In this research paper, one journal paper related to safety measures was discussed
and analyzed. Literature related to this paper was reviewed thoroughly. There are many types of research strategies are used
such as quantitative research, qualitative research, critical research, analytic research, and applied research. In this research
paper, two types of research strategies are analysed such as quantitative and qualitative research. Different types of research
idea related to safety, health, and environment were discussed.

SUN SAFETY IN CONSTRUCTION 6
References
Armstrong, B. (2004) how sun exposure causes skin cancer: an epidemiological perspective. Dordrecht: Kluwer Academic
Publishers.
Berwick, M., Lachiewicz, A., Pestak, C., and Thomas, N. (2009) Solar UV exposure and mortality from skin tumors. New
York: Landes Bioscience & Springer Science.
Cancer Research UK (2012) Skin cancer statistics [online]. Available from:
http://www.cancerresearchuk.org/cancer-info/cancerstats/types/skin/ [Accessed 21/06/18].
Culham centre fusion energy (2018) Safety, health & environment policy [online]. Available from:
http://www.ccfe.ac.uk/she.aspx [Accessed 21/06/18].
Office for National Statistics (2013) Cancer Registration Statistics [online]. Available from:
http://www.ons.gov.uk/ons/dcp171778_315795.pdf [Accessed 21/06/18].
Oxford academic (2016) Sun safety in construction: a UK intervention study [online]. Available from:
https://academic.oup.com/occmed/article/66/1/20/2750628 [Accessed 21/06/18].
Parkin, D., Mesher, D., and Sasieni, P. (2011) Cancers attributable to solar (ultraviolet) radiation exposure in the UK in 2010.
British Journal of Cancer, 105, pp. 566-569.
Patel, S., Nijhawan, R., Stechschulte, S., Parmet, Y., Rouhani, P., Kirsner, R., and Hu, S. (2010) Skin cancer awareness,
attitude, and sun protection behavior among medical students at the University of Miami Miller School of Medicine. Archives
of Dermatology, 146, pp. 797-800.
Payne, N., Jones, F., and Harris, P. (2013) Employees' perceptions of the impact of work on health behaviors. Journal of
Health Psychology, 17, pp. 887-899.
Safety and health practitioner (2015) Sun exposure and skin cancer health advice for outdoor workers [online]. Available
from: https://www.shponline.co.uk/sun-exposure-skin-cancer-health-advice-outdoor-workers/ [Accessed 21/06/18].
References
Armstrong, B. (2004) how sun exposure causes skin cancer: an epidemiological perspective. Dordrecht: Kluwer Academic
Publishers.
Berwick, M., Lachiewicz, A., Pestak, C., and Thomas, N. (2009) Solar UV exposure and mortality from skin tumors. New
York: Landes Bioscience & Springer Science.
Cancer Research UK (2012) Skin cancer statistics [online]. Available from:
http://www.cancerresearchuk.org/cancer-info/cancerstats/types/skin/ [Accessed 21/06/18].
Culham centre fusion energy (2018) Safety, health & environment policy [online]. Available from:
http://www.ccfe.ac.uk/she.aspx [Accessed 21/06/18].
Office for National Statistics (2013) Cancer Registration Statistics [online]. Available from:
http://www.ons.gov.uk/ons/dcp171778_315795.pdf [Accessed 21/06/18].
Oxford academic (2016) Sun safety in construction: a UK intervention study [online]. Available from:
https://academic.oup.com/occmed/article/66/1/20/2750628 [Accessed 21/06/18].
Parkin, D., Mesher, D., and Sasieni, P. (2011) Cancers attributable to solar (ultraviolet) radiation exposure in the UK in 2010.
British Journal of Cancer, 105, pp. 566-569.
Patel, S., Nijhawan, R., Stechschulte, S., Parmet, Y., Rouhani, P., Kirsner, R., and Hu, S. (2010) Skin cancer awareness,
attitude, and sun protection behavior among medical students at the University of Miami Miller School of Medicine. Archives
of Dermatology, 146, pp. 797-800.
Payne, N., Jones, F., and Harris, P. (2013) Employees' perceptions of the impact of work on health behaviors. Journal of
Health Psychology, 17, pp. 887-899.
Safety and health practitioner (2015) Sun exposure and skin cancer health advice for outdoor workers [online]. Available
from: https://www.shponline.co.uk/sun-exposure-skin-cancer-health-advice-outdoor-workers/ [Accessed 21/06/18].
SUN SAFETY IN CONSTRUCTION 7
Occupational Medicine 2016;66:20–26
Advance Access publication 26 September 2015 doi:10.1093/occmed/kqv140
Appendix
Sun safety in construction: a UK intervention study
J. Houdmont1, P. Madgwick1 and R. Randall2
1Division of Psychiatry and Applied Psychology, School of Medicine, University of Nottingham, Nottingham NG8 1BB, UK,
2School of Business and Economics, Loughborough University, Loughborough LE11 3TU, UK.
Correspondence to: J. Houdmont, Division of Psychiatry and Applied Psychology, School of Medicine, University of Nottingham,
B Floor, Yang Fujia Building, Jubilee Campus, Wollaton Road, Nottingham NG8 1BB, UK. Tel: +44 (0)7977 142860;
fax: +44 (0)11 5846 6625; e-mail: jonathan.houdmont@nottingham.ac.uk
Background Interventions to promote sun safety in the UK construction sector are warranted given the high incidence of
skin cancer attributable to sun exposure relative to other occupational groups.
Aims To evaluate change in sun safety knowledge and practices among construction workers in response
to an educational intervention.
Methods A baseline questionnaire was administered, followed by a bespoke sector-specific DVD-based inter-
vention. At 12-month follow-up, participants completed a further questionnaire.
Results Analyses were conducted on a sample of 120 workers (intervention group, n = 70; comparison
group, n = 50). At follow-up, the proportion of intervention group participants that reported correct
sun safety knowledge was not significantly greater than at baseline. However, the intervention group
demonstrated significant positive change on 9 out of 10 behavioural measures, the greatest change
being use of a shade/cover when working in the sun followed by regularly checking skin for moles or
unusual changes.
Conclusions Exposure to this intervention was linked to some specific positive changes in construction workers’ self-
reported sun safety practices. These findings highlight the potential for educational interven-tions to
contribute to tackling skin cancer in the UK construction sector. The findings support the development of
bespoke educational interventions for other high-risk outdoor worker groups.
Key words Construction; intervention; skin cancer; solar radiation; sun safety; transtheoretical model.
Introduction
Solar ultraviolet radiation (UVR) is a leading contributor to
the development of skin cancer [1,2], with data for 2010
indicating that solar UVR was responsible for an estimated
90% of cases of melanoma in men in the UK [3]. Skin
cancer is the most common type of cancer in the UK and on
the rise [4]. Registration data for England show a 56%
increase in melanoma skin cancer for men between 2002 and
2011 [5] and the incidence rate for non-melanoma skin
cancer appears to be rising faster in the UK than in the rest
of Europe [6]. Estimates for England for 2008 place the cost
of skin cancer to the NHS at £106–£112 million; on the basis
of the current trajectory, it is estimated that by 2020 the cost
to the NHS will exceed £180 million [7].
Outdoor workers are at significantly increased risk for
skin cancer attributable to solar UVR [8,9]. Data
reported by physicians between 2002 and 2008 to The
Health and Occupation Reporting Network (THOR) showed
that for skin neoplasia, male UK construction industry
workers aged under 65 had a significantly raised
standardized rate ratio (SRR) relative to all other UK
industries combined (SRR 4.2, 95% CI 3.3–5.3). Exposure
to solar UVR was the suspected causal factor in all but a
single reported case [10], with the risk being particularly
high among roofers, painters and decorators and labourers in
the building and woodwork trades [11]. On the basis of
incidence data from 2011 and mortality data from 2012, it
has been estimated that occupational exposure to solar UVR
results in 46 deaths and 239 new cases of malignant
melanoma in a typical year in Britain, with the construction
industry accounting for 44% of the deaths and 42% of the
registrations [12]. Sun safety knowledge and use of
protective and precautionary
© The Author 2015. Published by Oxford University Press on behalf of the Society of Occupational Medicine.
All rights reserved. For Permissions, please email: journals.permissions@oup.com
Occupational Medicine 2016;66:20–26
Advance Access publication 26 September 2015 doi:10.1093/occmed/kqv140
Appendix
Sun safety in construction: a UK intervention study
J. Houdmont1, P. Madgwick1 and R. Randall2
1Division of Psychiatry and Applied Psychology, School of Medicine, University of Nottingham, Nottingham NG8 1BB, UK,
2School of Business and Economics, Loughborough University, Loughborough LE11 3TU, UK.
Correspondence to: J. Houdmont, Division of Psychiatry and Applied Psychology, School of Medicine, University of Nottingham,
B Floor, Yang Fujia Building, Jubilee Campus, Wollaton Road, Nottingham NG8 1BB, UK. Tel: +44 (0)7977 142860;
fax: +44 (0)11 5846 6625; e-mail: jonathan.houdmont@nottingham.ac.uk
Background Interventions to promote sun safety in the UK construction sector are warranted given the high incidence of
skin cancer attributable to sun exposure relative to other occupational groups.
Aims To evaluate change in sun safety knowledge and practices among construction workers in response
to an educational intervention.
Methods A baseline questionnaire was administered, followed by a bespoke sector-specific DVD-based inter-
vention. At 12-month follow-up, participants completed a further questionnaire.
Results Analyses were conducted on a sample of 120 workers (intervention group, n = 70; comparison
group, n = 50). At follow-up, the proportion of intervention group participants that reported correct
sun safety knowledge was not significantly greater than at baseline. However, the intervention group
demonstrated significant positive change on 9 out of 10 behavioural measures, the greatest change
being use of a shade/cover when working in the sun followed by regularly checking skin for moles or
unusual changes.
Conclusions Exposure to this intervention was linked to some specific positive changes in construction workers’ self-
reported sun safety practices. These findings highlight the potential for educational interven-tions to
contribute to tackling skin cancer in the UK construction sector. The findings support the development of
bespoke educational interventions for other high-risk outdoor worker groups.
Key words Construction; intervention; skin cancer; solar radiation; sun safety; transtheoretical model.
Introduction
Solar ultraviolet radiation (UVR) is a leading contributor to
the development of skin cancer [1,2], with data for 2010
indicating that solar UVR was responsible for an estimated
90% of cases of melanoma in men in the UK [3]. Skin
cancer is the most common type of cancer in the UK and on
the rise [4]. Registration data for England show a 56%
increase in melanoma skin cancer for men between 2002 and
2011 [5] and the incidence rate for non-melanoma skin
cancer appears to be rising faster in the UK than in the rest
of Europe [6]. Estimates for England for 2008 place the cost
of skin cancer to the NHS at £106–£112 million; on the basis
of the current trajectory, it is estimated that by 2020 the cost
to the NHS will exceed £180 million [7].
Outdoor workers are at significantly increased risk for
skin cancer attributable to solar UVR [8,9]. Data
reported by physicians between 2002 and 2008 to The
Health and Occupation Reporting Network (THOR) showed
that for skin neoplasia, male UK construction industry
workers aged under 65 had a significantly raised
standardized rate ratio (SRR) relative to all other UK
industries combined (SRR 4.2, 95% CI 3.3–5.3). Exposure
to solar UVR was the suspected causal factor in all but a
single reported case [10], with the risk being particularly
high among roofers, painters and decorators and labourers in
the building and woodwork trades [11]. On the basis of
incidence data from 2011 and mortality data from 2012, it
has been estimated that occupational exposure to solar UVR
results in 46 deaths and 239 new cases of malignant
melanoma in a typical year in Britain, with the construction
industry accounting for 44% of the deaths and 42% of the
registrations [12]. Sun safety knowledge and use of
protective and precautionary
© The Author 2015. Published by Oxford University Press on behalf of the Society of Occupational Medicine.
All rights reserved. For Permissions, please email: journals.permissions@oup.com
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

SUN SAFETY IN CONSTRUCTION 8
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018

J. HOUDMONT ET AL.: SUN SAFETY IN THE UK CONSTRUCTION SECTOR 21
practices are low within the UK construction sector [13].
This indicates that relatively simple interventions could
result in significant positive health outcomes.
Sun safety interventions targeted at construction workers
and other manual outdoor worker groups (e.g. those laying
water pipes or electricity cables) have suc-cessfully
produced improvements in knowledge, attitudes and self-
reported behaviours [14–18]. However, no sun safety
intervention studies have been conducted in the UK
construction sector and it is not clear whether the existing
results can be generalized to this group. All pub-lished
intervention work has been conducted in Australia and
Israel, countries with more intense and prolonged periods of
sunshine than the UK, and findings therefore may not
transfer into the UK context. Furthermore, due to an
established sun safety culture in Australia [19], pre-
intervention attitudes towards sun protection might dif-fer
significantly from those held in the UK.
The high incidence of skin cancer attributable to solar
UVR among construction workers in the UK cou-pled with
their low levels of sun safety knowledge and associated risk-
reduction practices highlights a need for effective
interventions. The aim of this study there-fore was to
examine the effectiveness of a DVD-based sun safety
educational intervention designed specifi-cally for the UK
construction context. Several factors informed the decision
to focus on a film-based inter-vention. First, these have been
shown to be effective in promoting sunscreen knowledge
and usage and rated by study participants more positively
than alternative intervention media such as leaflets [20,21].
Second, film-based interventions can be created at relatively
little cost and delivered quickly in the workplace with little
disruption to work activities. Third, they can be administered
without expert knowledge on the part of the administrator.
Methods
The intervention was a 12-min DVD titled Sun Safety in
Construction: A Workplace Health Guidance Film. It was
developed as a low-cost educational intervention that could
be readily integrated into occupational safety and health
briefings on all types of construction sites. The intervention
is now freely available at http://www.notime-tolose.org.uk
as part of the Institution of Occupational Safety and Health’s
(IOSH) ‘No Time To Lose’ occu-pational cancer-reduction
campaign. The intervention addressed the risk of skin cancer
in the UK construc-tion sector, sun safety practices that
might be adopted on construction sites and self-checking of
skin for early signs of skin cancer.
Construction companies were contacted through the
personal contacts of the research team in addition to
advertisements in trade magazines and presenta-tions to
industry bodies. The baseline questionnaire
was administered in work time during health and safety
briefings in participating organizations (N = 22) between
May and August 2012. Questionnaire completion and return
was incentivized by a prize draw to win a sports car driving
experience. A stamped addressed envelope was provided
with each questionnaire for participants to return completed
questionnaires directly to the research team. The project
champion in each organization was provided with a copy of
the intervention and instructed to administer this only after
administration and comple-tion of the baseline
questionnaire; in most cases, these activities took place on
the same day or within a few days of one another.
Respondents who provided their contact details on the
baseline questionnaire were sent a follow-up questionnaire
along with a stamped addressed return envelope in the
summer of 2013. The mean lag between completion of
baseline and follow-up questionnaires was 12 months.
The study included an emergent comparison group,
comprising workers who completed the baseline ques-
tionnaire and follow-up questionnaire but who did not
receive the intervention [22]. Group membership was
established via an item on the follow-up question-naire that
assessed intervention exposure. Reasons for not having
received the intervention are unlikely to be related to self-
selection. Instead these included work scheduling
requirements, absence or working off-site at the time of
intervention administration, or staff turnover in the period
between baseline question-naire administration and
intervention administration. The emergent design was
adopted for three reasons. First, all participating companies
wanted to deliver the intervention as quickly as possible
ruling out the pos-sibility of populating a sizeable and
representative wait-list comparison group. Second, it was
thought unlikely that all employees who completed both the
baseline and follow-up questionnaires would be present on
the day of intervention administration for operational rea-
sons and due to the transitory nature of the workforce. These
reasons for participants being members of the comparison
group were unlikely to be related to inter-vention
effectiveness. Third, evidence from previous sun safety
intervention studies suggests that it is typi-cal that some
participating organizations fail to cor-rectly administer the
intervention [23]. Therefore, the design reduced the risk of a
type III error (erroneously concluding that an intervention
was unsuccessful when many participants had not received
the intervention as intended).
Respondents’ sun safety knowledge was assessed using
five items (Table 2) adapted from Patel et al. [24].
Respondents indicated whether they agreed or disa-greed
with each statement. We also examined respond-ents’ self-
reported use of a set of 10 sun safety practices (Table 3)
previously identified as the primary meas-ures typically
available to outdoor workers [25]. This
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
practices are low within the UK construction sector [13].
This indicates that relatively simple interventions could
result in significant positive health outcomes.
Sun safety interventions targeted at construction workers
and other manual outdoor worker groups (e.g. those laying
water pipes or electricity cables) have suc-cessfully
produced improvements in knowledge, attitudes and self-
reported behaviours [14–18]. However, no sun safety
intervention studies have been conducted in the UK
construction sector and it is not clear whether the existing
results can be generalized to this group. All pub-lished
intervention work has been conducted in Australia and
Israel, countries with more intense and prolonged periods of
sunshine than the UK, and findings therefore may not
transfer into the UK context. Furthermore, due to an
established sun safety culture in Australia [19], pre-
intervention attitudes towards sun protection might dif-fer
significantly from those held in the UK.
The high incidence of skin cancer attributable to solar
UVR among construction workers in the UK cou-pled with
their low levels of sun safety knowledge and associated risk-
reduction practices highlights a need for effective
interventions. The aim of this study there-fore was to
examine the effectiveness of a DVD-based sun safety
educational intervention designed specifi-cally for the UK
construction context. Several factors informed the decision
to focus on a film-based inter-vention. First, these have been
shown to be effective in promoting sunscreen knowledge
and usage and rated by study participants more positively
than alternative intervention media such as leaflets [20,21].
Second, film-based interventions can be created at relatively
little cost and delivered quickly in the workplace with little
disruption to work activities. Third, they can be administered
without expert knowledge on the part of the administrator.
Methods
The intervention was a 12-min DVD titled Sun Safety in
Construction: A Workplace Health Guidance Film. It was
developed as a low-cost educational intervention that could
be readily integrated into occupational safety and health
briefings on all types of construction sites. The intervention
is now freely available at http://www.notime-tolose.org.uk
as part of the Institution of Occupational Safety and Health’s
(IOSH) ‘No Time To Lose’ occu-pational cancer-reduction
campaign. The intervention addressed the risk of skin cancer
in the UK construc-tion sector, sun safety practices that
might be adopted on construction sites and self-checking of
skin for early signs of skin cancer.
Construction companies were contacted through the
personal contacts of the research team in addition to
advertisements in trade magazines and presenta-tions to
industry bodies. The baseline questionnaire
was administered in work time during health and safety
briefings in participating organizations (N = 22) between
May and August 2012. Questionnaire completion and return
was incentivized by a prize draw to win a sports car driving
experience. A stamped addressed envelope was provided
with each questionnaire for participants to return completed
questionnaires directly to the research team. The project
champion in each organization was provided with a copy of
the intervention and instructed to administer this only after
administration and comple-tion of the baseline
questionnaire; in most cases, these activities took place on
the same day or within a few days of one another.
Respondents who provided their contact details on the
baseline questionnaire were sent a follow-up questionnaire
along with a stamped addressed return envelope in the
summer of 2013. The mean lag between completion of
baseline and follow-up questionnaires was 12 months.
The study included an emergent comparison group,
comprising workers who completed the baseline ques-
tionnaire and follow-up questionnaire but who did not
receive the intervention [22]. Group membership was
established via an item on the follow-up question-naire that
assessed intervention exposure. Reasons for not having
received the intervention are unlikely to be related to self-
selection. Instead these included work scheduling
requirements, absence or working off-site at the time of
intervention administration, or staff turnover in the period
between baseline question-naire administration and
intervention administration. The emergent design was
adopted for three reasons. First, all participating companies
wanted to deliver the intervention as quickly as possible
ruling out the pos-sibility of populating a sizeable and
representative wait-list comparison group. Second, it was
thought unlikely that all employees who completed both the
baseline and follow-up questionnaires would be present on
the day of intervention administration for operational rea-
sons and due to the transitory nature of the workforce. These
reasons for participants being members of the comparison
group were unlikely to be related to inter-vention
effectiveness. Third, evidence from previous sun safety
intervention studies suggests that it is typi-cal that some
participating organizations fail to cor-rectly administer the
intervention [23]. Therefore, the design reduced the risk of a
type III error (erroneously concluding that an intervention
was unsuccessful when many participants had not received
the intervention as intended).
Respondents’ sun safety knowledge was assessed using
five items (Table 2) adapted from Patel et al. [24].
Respondents indicated whether they agreed or disa-greed
with each statement. We also examined respond-ents’ self-
reported use of a set of 10 sun safety practices (Table 3)
previously identified as the primary meas-ures typically
available to outdoor workers [25]. This
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
22 OCCUPATIONAL MEDICINE
behaviour was assessed in accordance with Prchaska and
DiClemente’s transtheoretical model of behaviour change
[26]. In this model, individuals pass through five stages of
change in relation to a particular behav-iour. Respondents
indicated which of five statements best described their usual
behaviour for each facet of sun safety. The five response
options were ‘I do not do this and I am not thinking about
starting’ (pre-contem-plation stage) (1), ‘I do not do this but
I am thinking about starting’ (contemplation stage) (2), ‘I do
not do this but am planning to start in the next month’ (pre-
paration stage) (3), ‘I do this but have only begun to do so
this year’ (action stage) (4), ‘I do this and have done so for
more than a year’ (maintenance stage) (5). The
questionnaire was also used to collect data on socio-
demographic and occupational factors (Table 1).
Pearson’s chi-square test was used to examine the
statistical significance of the link between self-reported
intervention exposure and changes in knowledge cor-
rectness. For each knowledge domain, we compared the
proportion of participants (intervention versus comparison)
that were incorrect at baseline and then correct at follow-up.
For each behavioural domain, the significance of change in
the mean score on the stage of change measure was
examined using a repeated meas-ures t-test in both the
intervention and comparison groups. The proportion of
respondents in the action or maintenance stage of change in
each group at follow-up was also examined to identify the
number of partici-pants crossing the thresholds from
inaction to action/ maintenance. This approach to reporting
is consistent with that employed in previous sun safety
intervention studies [16,17,27].
A research ethics committee at the University of
Nottingham granted ethical approval for the study and the
research adhered to the British Psychological Society’s
Code of Ethics and Conduct [28].
Results
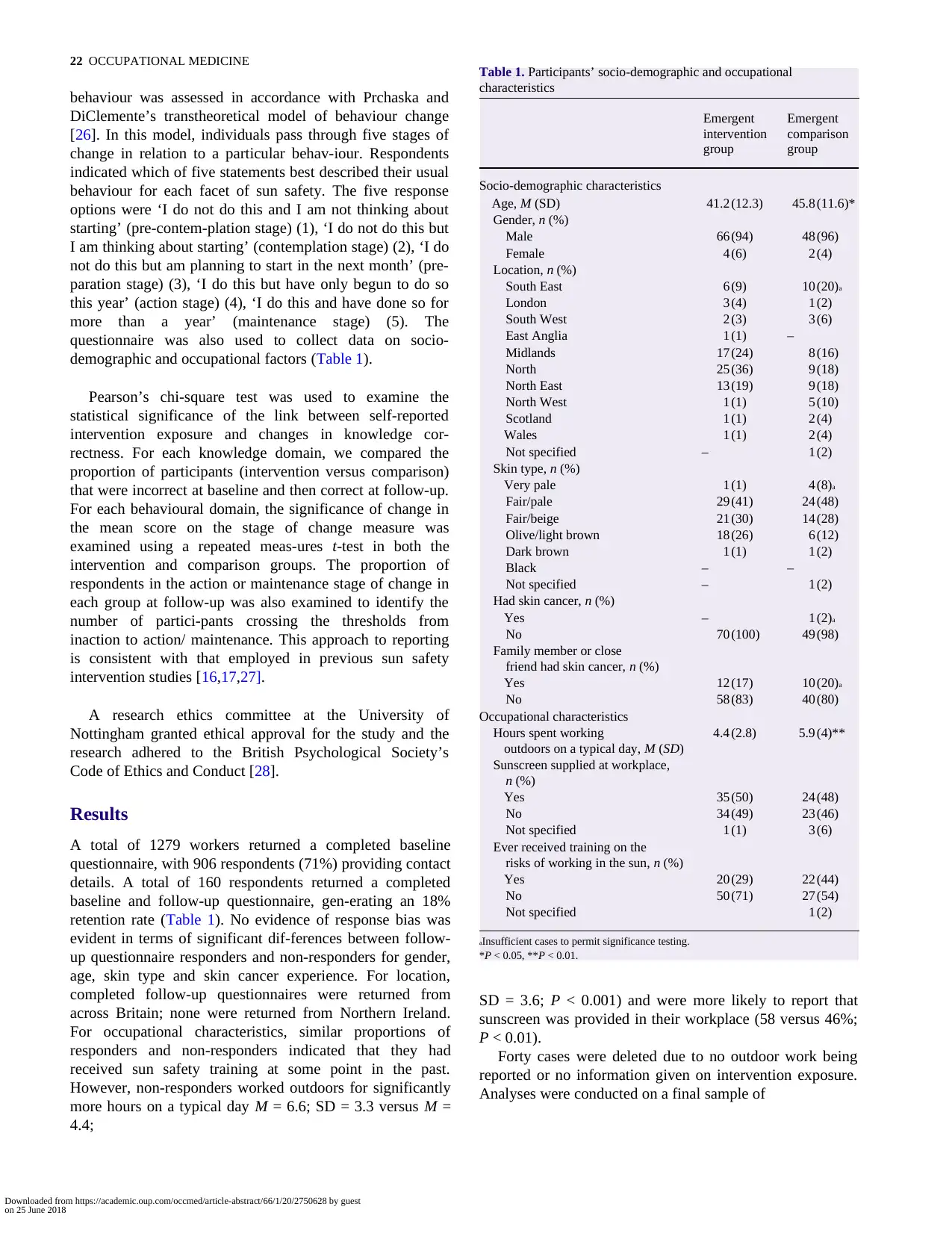
A total of 1279 workers returned a completed baseline
questionnaire, with 906 respondents (71%) providing contact
details. A total of 160 respondents returned a completed
baseline and follow-up questionnaire, gen-erating an 18%
retention rate (Table 1). No evidence of response bias was
evident in terms of significant dif-ferences between follow-
up questionnaire responders and non-responders for gender,
age, skin type and skin cancer experience. For location,
completed follow-up questionnaires were returned from
across Britain; none were returned from Northern Ireland.
For occupational characteristics, similar proportions of
responders and non-responders indicated that they had
received sun safety training at some point in the past.
However, non-responders worked outdoors for significantly
more hours on a typical day M = 6.6; SD = 3.3 versus M =
4.4;
Table 1. Participants’ socio-demographic and occupational
characteristics
Emergent Emergent
intervention comparison
group group
Socio-demographic characteristics
Age, M (SD) 41.2 (12.3) 45.8 (11.6)*
Gender, n (%)
Male 66 (94) 48 (96)
Female 4 (6) 2 (4)
Location, n (%)
South East 6 (9) 10 (20)a
London 3 (4) 1 (2)
South West 2 (3) 3 (6)
East Anglia 1 (1) –
Midlands 17 (24) 8 (16)
North 25 (36) 9 (18)
North East 13 (19) 9 (18)
North West 1 (1) 5 (10)
Scotland 1 (1) 2 (4)
Wales 1 (1) 2 (4)
Not specified – 1 (2)
Skin type, n (%)
Very pale 1 (1) 4 (8)a
Fair/pale 29 (41) 24 (48)
Fair/beige 21 (30) 14 (28)
Olive/light brown 18 (26) 6 (12)
Dark brown 1 (1) 1 (2)
Black – –
Not specified – 1 (2)
Had skin cancer, n (%)
Yes – 1 (2)a
No 70 (100) 49 (98)
Family member or close
friend had skin cancer, n (%)
Yes 12 (17) 10 (20)a
No 58 (83) 40 (80)
Occupational characteristics
Hours spent working 4.4 (2.8) 5.9 (4)**
outdoors on a typical day, M (SD)
Sunscreen supplied at workplace,
n (%)
Yes 35 (50) 24 (48)
No 34 (49) 23 (46)
Not specified 1 (1) 3 (6)
Ever received training on the
risks of working in the sun, n (%)
Yes 20 (29) 22 (44)
No 50 (71) 27 (54)
Not specified 1 (2)
aInsufficient cases to permit significance testing.
*P < 0.05, **P < 0.01.
SD = 3.6; P < 0.001) and were more likely to report that
sunscreen was provided in their workplace (58 versus 46%;
P < 0.01).
Forty cases were deleted due to no outdoor work being
reported or no information given on intervention exposure.
Analyses were conducted on a final sample of
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
behaviour was assessed in accordance with Prchaska and
DiClemente’s transtheoretical model of behaviour change
[26]. In this model, individuals pass through five stages of
change in relation to a particular behav-iour. Respondents
indicated which of five statements best described their usual
behaviour for each facet of sun safety. The five response
options were ‘I do not do this and I am not thinking about
starting’ (pre-contem-plation stage) (1), ‘I do not do this but
I am thinking about starting’ (contemplation stage) (2), ‘I do
not do this but am planning to start in the next month’ (pre-
paration stage) (3), ‘I do this but have only begun to do so
this year’ (action stage) (4), ‘I do this and have done so for
more than a year’ (maintenance stage) (5). The
questionnaire was also used to collect data on socio-
demographic and occupational factors (Table 1).
Pearson’s chi-square test was used to examine the
statistical significance of the link between self-reported
intervention exposure and changes in knowledge cor-
rectness. For each knowledge domain, we compared the
proportion of participants (intervention versus comparison)
that were incorrect at baseline and then correct at follow-up.
For each behavioural domain, the significance of change in
the mean score on the stage of change measure was
examined using a repeated meas-ures t-test in both the
intervention and comparison groups. The proportion of
respondents in the action or maintenance stage of change in
each group at follow-up was also examined to identify the
number of partici-pants crossing the thresholds from
inaction to action/ maintenance. This approach to reporting
is consistent with that employed in previous sun safety
intervention studies [16,17,27].
A research ethics committee at the University of
Nottingham granted ethical approval for the study and the
research adhered to the British Psychological Society’s
Code of Ethics and Conduct [28].
Results
A total of 1279 workers returned a completed baseline
questionnaire, with 906 respondents (71%) providing contact
details. A total of 160 respondents returned a completed
baseline and follow-up questionnaire, gen-erating an 18%
retention rate (Table 1). No evidence of response bias was
evident in terms of significant dif-ferences between follow-
up questionnaire responders and non-responders for gender,
age, skin type and skin cancer experience. For location,
completed follow-up questionnaires were returned from
across Britain; none were returned from Northern Ireland.
For occupational characteristics, similar proportions of
responders and non-responders indicated that they had
received sun safety training at some point in the past.
However, non-responders worked outdoors for significantly
more hours on a typical day M = 6.6; SD = 3.3 versus M =
4.4;
Table 1. Participants’ socio-demographic and occupational
characteristics
Emergent Emergent
intervention comparison
group group
Socio-demographic characteristics
Age, M (SD) 41.2 (12.3) 45.8 (11.6)*
Gender, n (%)
Male 66 (94) 48 (96)
Female 4 (6) 2 (4)
Location, n (%)
South East 6 (9) 10 (20)a
London 3 (4) 1 (2)
South West 2 (3) 3 (6)
East Anglia 1 (1) –
Midlands 17 (24) 8 (16)
North 25 (36) 9 (18)
North East 13 (19) 9 (18)
North West 1 (1) 5 (10)
Scotland 1 (1) 2 (4)
Wales 1 (1) 2 (4)
Not specified – 1 (2)
Skin type, n (%)
Very pale 1 (1) 4 (8)a
Fair/pale 29 (41) 24 (48)
Fair/beige 21 (30) 14 (28)
Olive/light brown 18 (26) 6 (12)
Dark brown 1 (1) 1 (2)
Black – –
Not specified – 1 (2)
Had skin cancer, n (%)
Yes – 1 (2)a
No 70 (100) 49 (98)
Family member or close
friend had skin cancer, n (%)
Yes 12 (17) 10 (20)a
No 58 (83) 40 (80)
Occupational characteristics
Hours spent working 4.4 (2.8) 5.9 (4)**
outdoors on a typical day, M (SD)
Sunscreen supplied at workplace,
n (%)
Yes 35 (50) 24 (48)
No 34 (49) 23 (46)
Not specified 1 (1) 3 (6)
Ever received training on the
risks of working in the sun, n (%)
Yes 20 (29) 22 (44)
No 50 (71) 27 (54)
Not specified 1 (2)
aInsufficient cases to permit significance testing.
*P < 0.05, **P < 0.01.
SD = 3.6; P < 0.001) and were more likely to report that
sunscreen was provided in their workplace (58 versus 46%;
P < 0.01).
Forty cases were deleted due to no outdoor work being
reported or no information given on intervention exposure.
Analyses were conducted on a final sample of
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
J. HOUDMONT ET AL.: SUN SAFETY IN THE UK CONSTRUCTION SECTOR 23
120 cases (emergent intervention group n = 70; emer-gent
comparison group n = 50). There were no signifi-cant pre-
intervention differences between the knowledge and
practices reported by the two groups.
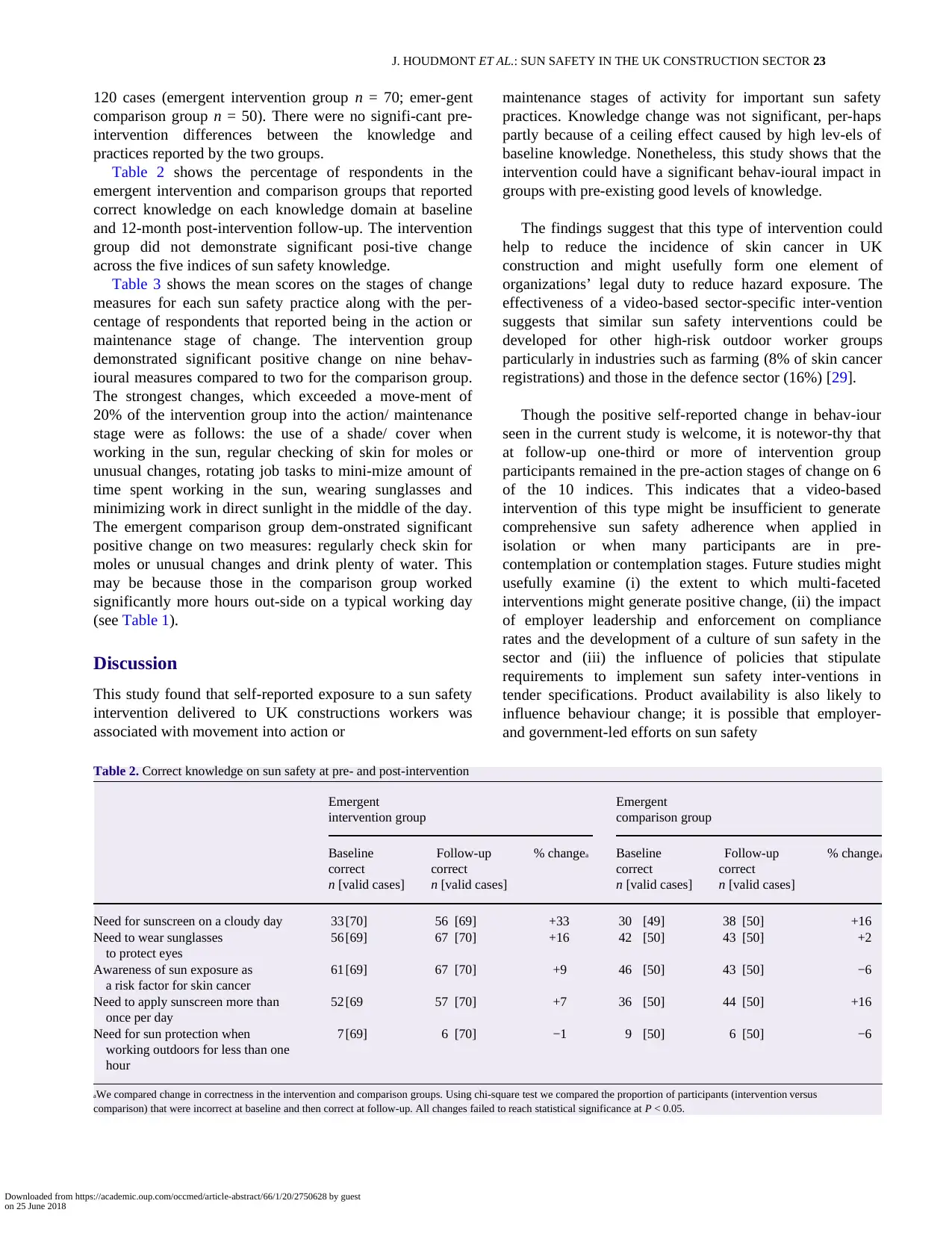
Table 2 shows the percentage of respondents in the
emergent intervention and comparison groups that reported
correct knowledge on each knowledge domain at baseline
and 12-month post-intervention follow-up. The intervention
group did not demonstrate significant posi-tive change
across the five indices of sun safety knowledge.
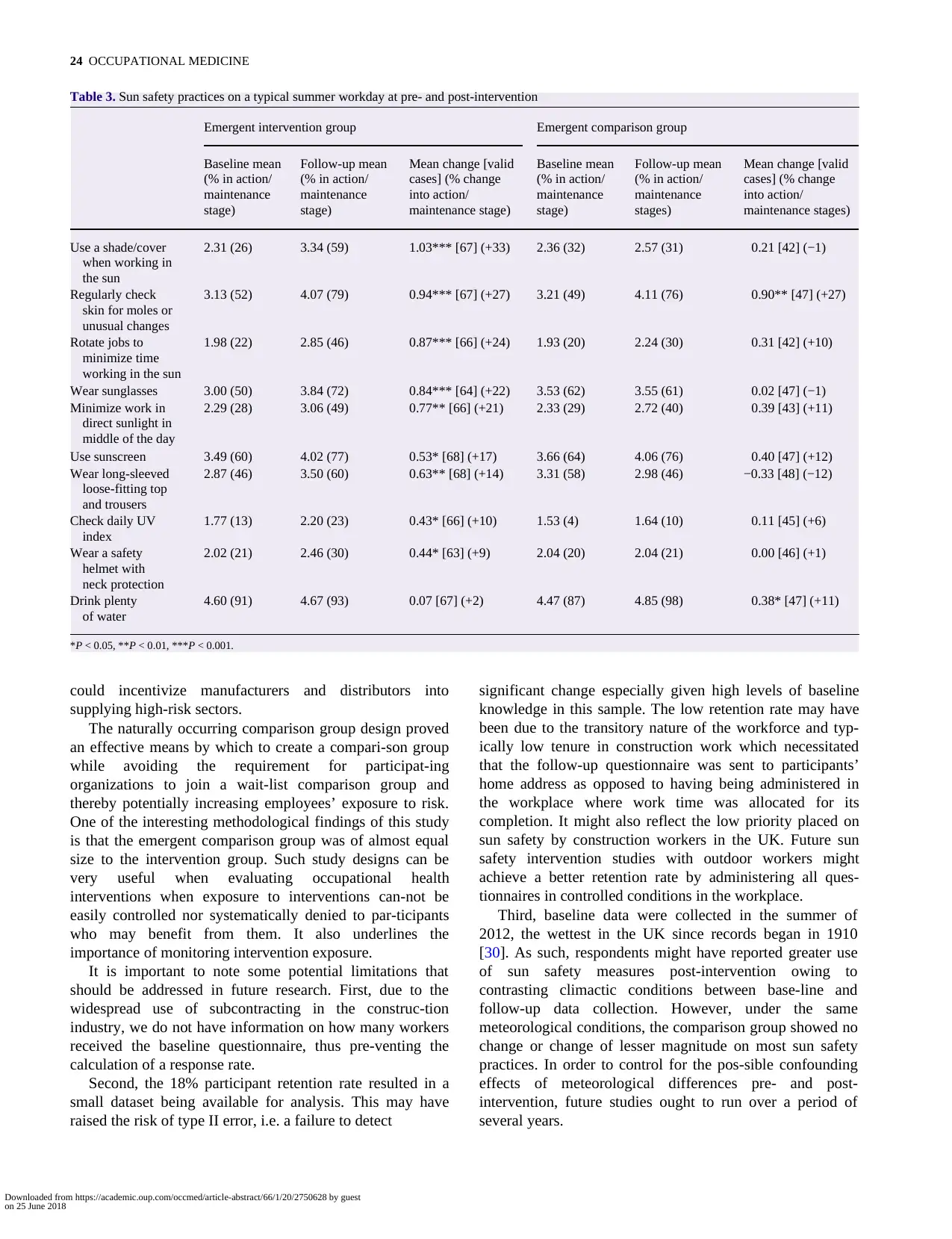
Table 3 shows the mean scores on the stages of change
measures for each sun safety practice along with the per-
centage of respondents that reported being in the action or
maintenance stage of change. The intervention group
demonstrated significant positive change on nine behav-
ioural measures compared to two for the comparison group.
The strongest changes, which exceeded a move-ment of
20% of the intervention group into the action/ maintenance
stage were as follows: the use of a shade/ cover when
working in the sun, regular checking of skin for moles or
unusual changes, rotating job tasks to mini-mize amount of
time spent working in the sun, wearing sunglasses and
minimizing work in direct sunlight in the middle of the day.
The emergent comparison group dem-onstrated significant
positive change on two measures: regularly check skin for
moles or unusual changes and drink plenty of water. This
may be because those in the comparison group worked
significantly more hours out-side on a typical working day
(see Table 1).
Discussion
This study found that self-reported exposure to a sun safety
intervention delivered to UK constructions workers was
associated with movement into action or
maintenance stages of activity for important sun safety
practices. Knowledge change was not significant, per-haps
partly because of a ceiling effect caused by high lev-els of
baseline knowledge. Nonetheless, this study shows that the
intervention could have a significant behav-ioural impact in
groups with pre-existing good levels of knowledge.
The findings suggest that this type of intervention could
help to reduce the incidence of skin cancer in UK
construction and might usefully form one element of
organizations’ legal duty to reduce hazard exposure. The
effectiveness of a video-based sector-specific inter-vention
suggests that similar sun safety interventions could be
developed for other high-risk outdoor worker groups
particularly in industries such as farming (8% of skin cancer
registrations) and those in the defence sector (16%) [29].
Though the positive self-reported change in behav-iour
seen in the current study is welcome, it is notewor-thy that
at follow-up one-third or more of intervention group
participants remained in the pre-action stages of change on 6
of the 10 indices. This indicates that a video-based
intervention of this type might be insufficient to generate
comprehensive sun safety adherence when applied in
isolation or when many participants are in pre-
contemplation or contemplation stages. Future studies might
usefully examine (i) the extent to which multi-faceted
interventions might generate positive change, (ii) the impact
of employer leadership and enforcement on compliance
rates and the development of a culture of sun safety in the
sector and (iii) the influence of policies that stipulate
requirements to implement sun safety inter-ventions in
tender specifications. Product availability is also likely to
influence behaviour change; it is possible that employer-
and government-led efforts on sun safety
Table 2. Correct knowledge on sun safety at pre- and post-intervention
Emergent Emergent
intervention group comparison group
Baseline Follow-up % changea Baseline Follow-up % changea
correct correct correct correct
n [valid cases] n [valid cases] n [valid cases] n [valid cases]
Need for sunscreen on a cloudy day 33 [70] 56 [69] +33 30 [49] 38 [50] +16
Need to wear sunglasses 56 [69] 67 [70] +16 42 [50] 43 [50] +2
to protect eyes
Awareness of sun exposure as 61 [69] 67 [70] +9 46 [50] 43 [50] −6
a risk factor for skin cancer
Need to apply sunscreen more than 52 [69 57 [70] +7 36 [50] 44 [50] +16
once per day
Need for sun protection when 7 [69] 6 [70] −1 9 [50] 6 [50] −6
working outdoors for less than one
hour
aWe compared change in correctness in the intervention and comparison groups. Using chi-square test we compared the proportion of participants (intervention versus
comparison) that were incorrect at baseline and then correct at follow-up. All changes failed to reach statistical significance at P < 0.05.
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
120 cases (emergent intervention group n = 70; emer-gent
comparison group n = 50). There were no signifi-cant pre-
intervention differences between the knowledge and
practices reported by the two groups.
Table 2 shows the percentage of respondents in the
emergent intervention and comparison groups that reported
correct knowledge on each knowledge domain at baseline
and 12-month post-intervention follow-up. The intervention
group did not demonstrate significant posi-tive change
across the five indices of sun safety knowledge.
Table 3 shows the mean scores on the stages of change
measures for each sun safety practice along with the per-
centage of respondents that reported being in the action or
maintenance stage of change. The intervention group
demonstrated significant positive change on nine behav-
ioural measures compared to two for the comparison group.
The strongest changes, which exceeded a move-ment of
20% of the intervention group into the action/ maintenance
stage were as follows: the use of a shade/ cover when
working in the sun, regular checking of skin for moles or
unusual changes, rotating job tasks to mini-mize amount of
time spent working in the sun, wearing sunglasses and
minimizing work in direct sunlight in the middle of the day.
The emergent comparison group dem-onstrated significant
positive change on two measures: regularly check skin for
moles or unusual changes and drink plenty of water. This
may be because those in the comparison group worked
significantly more hours out-side on a typical working day
(see Table 1).
Discussion
This study found that self-reported exposure to a sun safety
intervention delivered to UK constructions workers was
associated with movement into action or
maintenance stages of activity for important sun safety
practices. Knowledge change was not significant, per-haps
partly because of a ceiling effect caused by high lev-els of
baseline knowledge. Nonetheless, this study shows that the
intervention could have a significant behav-ioural impact in
groups with pre-existing good levels of knowledge.
The findings suggest that this type of intervention could
help to reduce the incidence of skin cancer in UK
construction and might usefully form one element of
organizations’ legal duty to reduce hazard exposure. The
effectiveness of a video-based sector-specific inter-vention
suggests that similar sun safety interventions could be
developed for other high-risk outdoor worker groups
particularly in industries such as farming (8% of skin cancer
registrations) and those in the defence sector (16%) [29].
Though the positive self-reported change in behav-iour
seen in the current study is welcome, it is notewor-thy that
at follow-up one-third or more of intervention group
participants remained in the pre-action stages of change on 6
of the 10 indices. This indicates that a video-based
intervention of this type might be insufficient to generate
comprehensive sun safety adherence when applied in
isolation or when many participants are in pre-
contemplation or contemplation stages. Future studies might
usefully examine (i) the extent to which multi-faceted
interventions might generate positive change, (ii) the impact
of employer leadership and enforcement on compliance
rates and the development of a culture of sun safety in the
sector and (iii) the influence of policies that stipulate
requirements to implement sun safety inter-ventions in
tender specifications. Product availability is also likely to
influence behaviour change; it is possible that employer-
and government-led efforts on sun safety
Table 2. Correct knowledge on sun safety at pre- and post-intervention
Emergent Emergent
intervention group comparison group
Baseline Follow-up % changea Baseline Follow-up % changea
correct correct correct correct
n [valid cases] n [valid cases] n [valid cases] n [valid cases]
Need for sunscreen on a cloudy day 33 [70] 56 [69] +33 30 [49] 38 [50] +16
Need to wear sunglasses 56 [69] 67 [70] +16 42 [50] 43 [50] +2
to protect eyes
Awareness of sun exposure as 61 [69] 67 [70] +9 46 [50] 43 [50] −6
a risk factor for skin cancer
Need to apply sunscreen more than 52 [69 57 [70] +7 36 [50] 44 [50] +16
once per day
Need for sun protection when 7 [69] 6 [70] −1 9 [50] 6 [50] −6
working outdoors for less than one
hour
aWe compared change in correctness in the intervention and comparison groups. Using chi-square test we compared the proportion of participants (intervention versus
comparison) that were incorrect at baseline and then correct at follow-up. All changes failed to reach statistical significance at P < 0.05.
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
24 OCCUPATIONAL MEDICINE
Table 3. Sun safety practices on a typical summer workday at pre- and post-intervention
Emergent intervention group Emergent comparison group
Baseline mean Follow-up mean Mean change [valid Baseline mean Follow-up mean Mean change [valid
(% in action/ (% in action/ cases] (% change (% in action/ (% in action/ cases] (% change
maintenance maintenance into action/ maintenance maintenance into action/
stage) stage) maintenance stage) stage) stages) maintenance stages)
Use a shade/cover 2.31 (26) 3.34 (59) 1.03*** [67] (+33) 2.36 (32) 2.57 (31) 0.21 [42] (−1)
when working in
the sun
Regularly check 3.13 (52) 4.07 (79) 0.94*** [67] (+27) 3.21 (49) 4.11 (76) 0.90** [47] (+27)
skin for moles or
unusual changes
Rotate jobs to 1.98 (22) 2.85 (46) 0.87*** [66] (+24) 1.93 (20) 2.24 (30) 0.31 [42] (+10)
minimize time
working in the sun
Wear sunglasses 3.00 (50) 3.84 (72) 0.84*** [64] (+22) 3.53 (62) 3.55 (61) 0.02 [47] (−1)
Minimize work in 2.29 (28) 3.06 (49) 0.77** [66] (+21) 2.33 (29) 2.72 (40) 0.39 [43] (+11)
direct sunlight in
middle of the day
Use sunscreen 3.49 (60) 4.02 (77) 0.53* [68] (+17) 3.66 (64) 4.06 (76) 0.40 [47] (+12)
Wear long-sleeved 2.87 (46) 3.50 (60) 0.63** [68] (+14) 3.31 (58) 2.98 (46) −0.33 [48] (−12)
loose-fitting top
and trousers
Check daily UV 1.77 (13) 2.20 (23) 0.43* [66] (+10) 1.53 (4) 1.64 (10) 0.11 [45] (+6)
index
Wear a safety 2.02 (21) 2.46 (30) 0.44* [63] (+9) 2.04 (20) 2.04 (21) 0.00 [46] (+1)
helmet with
neck protection
Drink plenty 4.60 (91) 4.67 (93) 0.07 [67] (+2) 4.47 (87) 4.85 (98) 0.38* [47] (+11)
of water
*P < 0.05, **P < 0.01, ***P < 0.001.
could incentivize manufacturers and distributors into
supplying high-risk sectors.
The naturally occurring comparison group design proved
an effective means by which to create a compari-son group
while avoiding the requirement for participat-ing
organizations to join a wait-list comparison group and
thereby potentially increasing employees’ exposure to risk.
One of the interesting methodological findings of this study
is that the emergent comparison group was of almost equal
size to the intervention group. Such study designs can be
very useful when evaluating occupational health
interventions when exposure to interventions can-not be
easily controlled nor systematically denied to par-ticipants
who may benefit from them. It also underlines the
importance of monitoring intervention exposure.
It is important to note some potential limitations that
should be addressed in future research. First, due to the
widespread use of subcontracting in the construc-tion
industry, we do not have information on how many workers
received the baseline questionnaire, thus pre-venting the
calculation of a response rate.
Second, the 18% participant retention rate resulted in a
small dataset being available for analysis. This may have
raised the risk of type II error, i.e. a failure to detect
significant change especially given high levels of baseline
knowledge in this sample. The low retention rate may have
been due to the transitory nature of the workforce and typ-
ically low tenure in construction work which necessitated
that the follow-up questionnaire was sent to participants’
home address as opposed to having being administered in
the workplace where work time was allocated for its
completion. It might also reflect the low priority placed on
sun safety by construction workers in the UK. Future sun
safety intervention studies with outdoor workers might
achieve a better retention rate by administering all ques-
tionnaires in controlled conditions in the workplace.
Third, baseline data were collected in the summer of
2012, the wettest in the UK since records began in 1910
[30]. As such, respondents might have reported greater use
of sun safety measures post-intervention owing to
contrasting climactic conditions between base-line and
follow-up data collection. However, under the same
meteorological conditions, the comparison group showed no
change or change of lesser magnitude on most sun safety
practices. In order to control for the pos-sible confounding
effects of meteorological differences pre- and post-
intervention, future studies ought to run over a period of
several years.
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
Table 3. Sun safety practices on a typical summer workday at pre- and post-intervention
Emergent intervention group Emergent comparison group
Baseline mean Follow-up mean Mean change [valid Baseline mean Follow-up mean Mean change [valid
(% in action/ (% in action/ cases] (% change (% in action/ (% in action/ cases] (% change
maintenance maintenance into action/ maintenance maintenance into action/
stage) stage) maintenance stage) stage) stages) maintenance stages)
Use a shade/cover 2.31 (26) 3.34 (59) 1.03*** [67] (+33) 2.36 (32) 2.57 (31) 0.21 [42] (−1)
when working in
the sun
Regularly check 3.13 (52) 4.07 (79) 0.94*** [67] (+27) 3.21 (49) 4.11 (76) 0.90** [47] (+27)
skin for moles or
unusual changes
Rotate jobs to 1.98 (22) 2.85 (46) 0.87*** [66] (+24) 1.93 (20) 2.24 (30) 0.31 [42] (+10)
minimize time
working in the sun
Wear sunglasses 3.00 (50) 3.84 (72) 0.84*** [64] (+22) 3.53 (62) 3.55 (61) 0.02 [47] (−1)
Minimize work in 2.29 (28) 3.06 (49) 0.77** [66] (+21) 2.33 (29) 2.72 (40) 0.39 [43] (+11)
direct sunlight in
middle of the day
Use sunscreen 3.49 (60) 4.02 (77) 0.53* [68] (+17) 3.66 (64) 4.06 (76) 0.40 [47] (+12)
Wear long-sleeved 2.87 (46) 3.50 (60) 0.63** [68] (+14) 3.31 (58) 2.98 (46) −0.33 [48] (−12)
loose-fitting top
and trousers
Check daily UV 1.77 (13) 2.20 (23) 0.43* [66] (+10) 1.53 (4) 1.64 (10) 0.11 [45] (+6)
index
Wear a safety 2.02 (21) 2.46 (30) 0.44* [63] (+9) 2.04 (20) 2.04 (21) 0.00 [46] (+1)
helmet with
neck protection
Drink plenty 4.60 (91) 4.67 (93) 0.07 [67] (+2) 4.47 (87) 4.85 (98) 0.38* [47] (+11)
of water
*P < 0.05, **P < 0.01, ***P < 0.001.
could incentivize manufacturers and distributors into
supplying high-risk sectors.
The naturally occurring comparison group design proved
an effective means by which to create a compari-son group
while avoiding the requirement for participat-ing
organizations to join a wait-list comparison group and
thereby potentially increasing employees’ exposure to risk.
One of the interesting methodological findings of this study
is that the emergent comparison group was of almost equal
size to the intervention group. Such study designs can be
very useful when evaluating occupational health
interventions when exposure to interventions can-not be
easily controlled nor systematically denied to par-ticipants
who may benefit from them. It also underlines the
importance of monitoring intervention exposure.
It is important to note some potential limitations that
should be addressed in future research. First, due to the
widespread use of subcontracting in the construc-tion
industry, we do not have information on how many workers
received the baseline questionnaire, thus pre-venting the
calculation of a response rate.
Second, the 18% participant retention rate resulted in a
small dataset being available for analysis. This may have
raised the risk of type II error, i.e. a failure to detect
significant change especially given high levels of baseline
knowledge in this sample. The low retention rate may have
been due to the transitory nature of the workforce and typ-
ically low tenure in construction work which necessitated
that the follow-up questionnaire was sent to participants’
home address as opposed to having being administered in
the workplace where work time was allocated for its
completion. It might also reflect the low priority placed on
sun safety by construction workers in the UK. Future sun
safety intervention studies with outdoor workers might
achieve a better retention rate by administering all ques-
tionnaires in controlled conditions in the workplace.
Third, baseline data were collected in the summer of
2012, the wettest in the UK since records began in 1910
[30]. As such, respondents might have reported greater use
of sun safety measures post-intervention owing to
contrasting climactic conditions between base-line and
follow-up data collection. However, under the same
meteorological conditions, the comparison group showed no
change or change of lesser magnitude on most sun safety
practices. In order to control for the pos-sible confounding
effects of meteorological differences pre- and post-
intervention, future studies ought to run over a period of
several years.
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018

J. HOUDMONT ET AL.: SUN SAFETY IN THE UK CONSTRUCTION SECTOR 25
Fourth, it is possible that respondents incorrectly recalled
whether or not they had been exposed to the intervention,
resulting in misclassification into the inter-vention group or
comparison group. We consider a large amount of
misclassification to be unlikely for two rea-sons: First,
video-based occupational health interven-tions are rare in
the UK construction sector. Second, the video contained
some humorous elements in order to engage the viewer.
Both of these factors are likely to have helped the film stick
in respondents’ minds suggesting that it would be unlikely
for a respondent to incorrectly recall whether or not they had
viewed the film.
Fifth, it is also possible that the behaviour of comparison
group participants was influenced by that of the interven-tion
group. For example, if a worker who viewed the DVD
subsequently used sunscreen when working outdoors, and that
individual worked alongside someone who had not viewed the
DVD, it is possible that the sun safety practices of the latter
individual might have been influenced by the for-mer. This
could help to explain improvements in sun safety practices
among emergent comparison group participants.
Finally, the intervention was of a one-size-fits-all type
rather than stage-matched and tailored to the needs of
participants in particular stages of change. Future studies
could usefully explore the development of stage-matched
interventions for construction workers.
This study provides an initial evidence base for the
efficacy of sun safety interventions for manual outdoor
workers in geographical contexts that experience rela-tively
few sunshine hours and high cloud levels during summer
months and where there exists an under-devel-oped sun
safety culture. The findings, considered in tandem with
statistical data on skin cancer attributable to occupational
solar UVR exposure [12], suggest that employers of outdoor
workers in such regions should administer sun safety
interventions within their provision for occupational health
protection and promotion.
Key points
• Interventions to promote sun safety in the UK
construction sector are warranted given the high
incidence of skin cancer attributable to solar ultra
violet radiation exposure.
• Exposure to an educational intervention was linked to
positive change in construction workers’ self-reported
sun safety practices at 12-month follow-up.
• This study highlights the potential for practical and
inexpensive sun safety interventions for high-risk
manual outdoor worker groups in geographi-cal
contexts that experience relatively few sunshine hours
and high cloud levels during summer months and
where there exists an under-developed sun safety
culture.
Funding
Institution of Occupational Safety and Health (IOSH).
Conflicts of interest
None declared.
References
1. Ichihashi M, Budiyanto A, Bito T et al. UV-induced skin
damage. Toxicol 2003;189:21–39.
2. Polefka T, Meyer T, Agin P et al. Effects of solar radiation on
the skin. J Cosmet Dermatol 2012;11:134–143.
3. Parkin D, Mesher D, Sasieni P. Cancers attributable to solar
(ultraviolet) radiation exposure in the UK in 2010. Br J Cancer
2011;105(Suppl. 2):S66–S69.
4. Cancer Research UK. Skin Cancer Statistics. 2014. http://
www.cancerresearchuk.org/cancer-info/cancerstats/types/ skin/
(11 December 2014, date last accessed).
5. Office for National Statistics. Cancer Registration Statistics,
England, 2011. Office for National Statistics, 2013.
http://www.ons.gov.uk/ons/dcp171778_315795.pdf (12
November 2014, date last accessed).
6. Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic
review of worldwide incidence of nonmelanoma skin can-cer.
Br J Dermatol 2012;166:1069–1080.
7. Vallejo-Torres L, Morris S, Kinge J et al. Measuring cur-rent
and future cost of skin cancer in England. J Public Health
2013;36:140–148.
8. Lucas R, McMichael A, Smith W et al. Solar Ultraviolet
Radiation. Environmental Burden of Disease Series No. 3.
Geneva, Switzerland: WHO, 2006.
9. Schmitt J, Seidler A, Diepgen T et al. Occupational UV-light
exposure increases the risk for the develop-ment of cutaneous
squamous cell carcinoma: a sys-
tematic review and meta-analysis. Br J Dermatol 2011;
164:291–307.
10. Stocks SJ, McNamee R, Carder M, Agius RM. The incidence
of medically reported work-related ill health in the UK
construction industry. Occup Environ Med 2010;67:574–576.
11. Stocks SJ, Turner S, McNamee R et al. Occupation and work-
related ill-health in UK construction workers. Occup Med
(Lond) 2011;61:407–415.
12. Rushton L, Hutchings S. The Burden of Occupational Cancer in
Great Britain: Cutaneous Malignant Melanoma and Occupational
Exposure to Solar Radiation. Institution of Occupational Safety
and Health, 2015. http://www.iosh.co.uk/~/media/
Documents/Books%20and%20resources/Skin%20
cancer/POL2756%20-%20Cutaneous%20Malignant%20
Melanoma%20Technical%20Full%20Report%20140415. ashx
(27 April 2015, date last accessed).
13. Madgwick P, Houdmont J, Randall R. Sun safety measures
among construction workers in Britain. Occup Med (Lond)
2011;61:430–433.
14. Azizi E, Flint P, Sadetzki S et al. A graded work site inter-
vention program to improve sun protection and skin can-cer
awareness in outdoor workers in Israel. Cancer Causes
Control 2000;11:513–521.
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
Fourth, it is possible that respondents incorrectly recalled
whether or not they had been exposed to the intervention,
resulting in misclassification into the inter-vention group or
comparison group. We consider a large amount of
misclassification to be unlikely for two rea-sons: First,
video-based occupational health interven-tions are rare in
the UK construction sector. Second, the video contained
some humorous elements in order to engage the viewer.
Both of these factors are likely to have helped the film stick
in respondents’ minds suggesting that it would be unlikely
for a respondent to incorrectly recall whether or not they had
viewed the film.
Fifth, it is also possible that the behaviour of comparison
group participants was influenced by that of the interven-tion
group. For example, if a worker who viewed the DVD
subsequently used sunscreen when working outdoors, and that
individual worked alongside someone who had not viewed the
DVD, it is possible that the sun safety practices of the latter
individual might have been influenced by the for-mer. This
could help to explain improvements in sun safety practices
among emergent comparison group participants.
Finally, the intervention was of a one-size-fits-all type
rather than stage-matched and tailored to the needs of
participants in particular stages of change. Future studies
could usefully explore the development of stage-matched
interventions for construction workers.
This study provides an initial evidence base for the
efficacy of sun safety interventions for manual outdoor
workers in geographical contexts that experience rela-tively
few sunshine hours and high cloud levels during summer
months and where there exists an under-devel-oped sun
safety culture. The findings, considered in tandem with
statistical data on skin cancer attributable to occupational
solar UVR exposure [12], suggest that employers of outdoor
workers in such regions should administer sun safety
interventions within their provision for occupational health
protection and promotion.
Key points
• Interventions to promote sun safety in the UK
construction sector are warranted given the high
incidence of skin cancer attributable to solar ultra
violet radiation exposure.
• Exposure to an educational intervention was linked to
positive change in construction workers’ self-reported
sun safety practices at 12-month follow-up.
• This study highlights the potential for practical and
inexpensive sun safety interventions for high-risk
manual outdoor worker groups in geographi-cal
contexts that experience relatively few sunshine hours
and high cloud levels during summer months and
where there exists an under-developed sun safety
culture.
Funding
Institution of Occupational Safety and Health (IOSH).
Conflicts of interest
None declared.
References
1. Ichihashi M, Budiyanto A, Bito T et al. UV-induced skin
damage. Toxicol 2003;189:21–39.
2. Polefka T, Meyer T, Agin P et al. Effects of solar radiation on
the skin. J Cosmet Dermatol 2012;11:134–143.
3. Parkin D, Mesher D, Sasieni P. Cancers attributable to solar
(ultraviolet) radiation exposure in the UK in 2010. Br J Cancer
2011;105(Suppl. 2):S66–S69.
4. Cancer Research UK. Skin Cancer Statistics. 2014. http://
www.cancerresearchuk.org/cancer-info/cancerstats/types/ skin/
(11 December 2014, date last accessed).
5. Office for National Statistics. Cancer Registration Statistics,
England, 2011. Office for National Statistics, 2013.
http://www.ons.gov.uk/ons/dcp171778_315795.pdf (12
November 2014, date last accessed).
6. Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic
review of worldwide incidence of nonmelanoma skin can-cer.
Br J Dermatol 2012;166:1069–1080.
7. Vallejo-Torres L, Morris S, Kinge J et al. Measuring cur-rent
and future cost of skin cancer in England. J Public Health
2013;36:140–148.
8. Lucas R, McMichael A, Smith W et al. Solar Ultraviolet
Radiation. Environmental Burden of Disease Series No. 3.
Geneva, Switzerland: WHO, 2006.
9. Schmitt J, Seidler A, Diepgen T et al. Occupational UV-light
exposure increases the risk for the develop-ment of cutaneous
squamous cell carcinoma: a sys-
tematic review and meta-analysis. Br J Dermatol 2011;
164:291–307.
10. Stocks SJ, McNamee R, Carder M, Agius RM. The incidence
of medically reported work-related ill health in the UK
construction industry. Occup Environ Med 2010;67:574–576.
11. Stocks SJ, Turner S, McNamee R et al. Occupation and work-
related ill-health in UK construction workers. Occup Med
(Lond) 2011;61:407–415.
12. Rushton L, Hutchings S. The Burden of Occupational Cancer in
Great Britain: Cutaneous Malignant Melanoma and Occupational
Exposure to Solar Radiation. Institution of Occupational Safety
and Health, 2015. http://www.iosh.co.uk/~/media/
Documents/Books%20and%20resources/Skin%20
cancer/POL2756%20-%20Cutaneous%20Malignant%20
Melanoma%20Technical%20Full%20Report%20140415. ashx
(27 April 2015, date last accessed).
13. Madgwick P, Houdmont J, Randall R. Sun safety measures
among construction workers in Britain. Occup Med (Lond)
2011;61:430–433.
14. Azizi E, Flint P, Sadetzki S et al. A graded work site inter-
vention program to improve sun protection and skin can-cer
awareness in outdoor workers in Israel. Cancer Causes
Control 2000;11:513–521.
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
26 OCCUPATIONAL MEDICINE
15. Borland RM, Hocking B, Godkin GA et al. The impact of a
skin cancer control education package for outdoor workers.
Med J Aust 1991;154:686–688.
16. Girgis A, Sanson-Fisher RW, Watson A. A workplace inter-
vention for increasing outdoor workers’ use of solar protec-
tion. Am J Public Health 1994;84:77–81.
17. Rye S, Janda M, Stoneham M et al. Changes in outdoor
workers’ sun-related attitudes, beliefs, and behaviors. J Occup
Environ Med 2014;56:e62–e72.
18. Woolley T, Lowe J, Raasch B et al. Workplace sun protec-tion
policies and employees’ sun-related skin damage. Am J Health
Behav 2008;32:201–208.
19. Garvin T, Eyles J. Public health responses for skin cancer
prevention: the policy framing of Sun Safety in Australia,
Canada and England. Soc Sci Med 2001;53:1175–1189.
20. Armstrong AW, Idriss NZ, Kim RH. Effects of video-based,
online education on behavioral and knowledge outcomes in
sunscreen use: a randomized controlled trial. Patient Educ
Couns 2011;83:273–277.
21. Tuong W, Larsen ER, Armstrong AW. Videos to influ-ence: a
systematic review of effectiveness of video-based education in
modifying health behaviors. J Behav Med 2014;37:218–233.
22. Randall R, Griffiths A, Cox T. Evaluating organizational stress-
management interventions using adapted study designs. Eur J
Work Organ Psy 2005;14:23–41.
23. McIver J, Rock V. Mystery shopping: A process evaluation of
an innovative skin cancer prevention campaign. Paper pre-
sented at the Second International Conference on UV and Skin
Cancer Prevention, Berlin, 10–13 September 2013.
24. Patel SS, Nijhawan RI, Stechschulte S et al. Skin cancer
awareness, attitude, and sun protection behavior among
medical students at the University of Miami Miller School of
Medicine. Arch Dermatol 2010;146:797–800.
25. Young C. Solar ultraviolet radiation and skin cancer. Occup
Med (Lond) 2009;59:82–88.
26. Prochaska J, DiClemente C. The Transtheoretical Approach:
Crossing the Traditional Boundaries of Change. Homewood,
IL: J. Irwin, 1984.
27. Weinstock M, Rossi J, Redding C et al. Randomized con-
trolled community trial of the efficacy of a multicompo-nent
stage-matched intervention to increase sun protection among
beach goers. Prev Med 2002;35:584–92.
28. British Psychological Society. Code of Ethics and Conduct.
London: British Psychological Society, 2009.
29. Rushton L, Bagga S, Bevan R et al. The Burden of
Occupational Cancer in Great Britain: Overview Report.
Research Report RR931. Health and Safety Executive. 2012.
http://www.hse.gov.uk/research/rrpdf/rr931.pdf (12 November
2014, date last accessed).
30. BBC. Rainy Weather Breaks UK Record for Three Months to
June. http://www.bbc.co.uk/news/uk-18653274 (14 May 2015,
date last accessed).
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
15. Borland RM, Hocking B, Godkin GA et al. The impact of a
skin cancer control education package for outdoor workers.
Med J Aust 1991;154:686–688.
16. Girgis A, Sanson-Fisher RW, Watson A. A workplace inter-
vention for increasing outdoor workers’ use of solar protec-
tion. Am J Public Health 1994;84:77–81.
17. Rye S, Janda M, Stoneham M et al. Changes in outdoor
workers’ sun-related attitudes, beliefs, and behaviors. J Occup
Environ Med 2014;56:e62–e72.
18. Woolley T, Lowe J, Raasch B et al. Workplace sun protec-tion
policies and employees’ sun-related skin damage. Am J Health
Behav 2008;32:201–208.
19. Garvin T, Eyles J. Public health responses for skin cancer
prevention: the policy framing of Sun Safety in Australia,
Canada and England. Soc Sci Med 2001;53:1175–1189.
20. Armstrong AW, Idriss NZ, Kim RH. Effects of video-based,
online education on behavioral and knowledge outcomes in
sunscreen use: a randomized controlled trial. Patient Educ
Couns 2011;83:273–277.
21. Tuong W, Larsen ER, Armstrong AW. Videos to influ-ence: a
systematic review of effectiveness of video-based education in
modifying health behaviors. J Behav Med 2014;37:218–233.
22. Randall R, Griffiths A, Cox T. Evaluating organizational stress-
management interventions using adapted study designs. Eur J
Work Organ Psy 2005;14:23–41.
23. McIver J, Rock V. Mystery shopping: A process evaluation of
an innovative skin cancer prevention campaign. Paper pre-
sented at the Second International Conference on UV and Skin
Cancer Prevention, Berlin, 10–13 September 2013.
24. Patel SS, Nijhawan RI, Stechschulte S et al. Skin cancer
awareness, attitude, and sun protection behavior among
medical students at the University of Miami Miller School of
Medicine. Arch Dermatol 2010;146:797–800.
25. Young C. Solar ultraviolet radiation and skin cancer. Occup
Med (Lond) 2009;59:82–88.
26. Prochaska J, DiClemente C. The Transtheoretical Approach:
Crossing the Traditional Boundaries of Change. Homewood,
IL: J. Irwin, 1984.
27. Weinstock M, Rossi J, Redding C et al. Randomized con-
trolled community trial of the efficacy of a multicompo-nent
stage-matched intervention to increase sun protection among
beach goers. Prev Med 2002;35:584–92.
28. British Psychological Society. Code of Ethics and Conduct.
London: British Psychological Society, 2009.
29. Rushton L, Bagga S, Bevan R et al. The Burden of
Occupational Cancer in Great Britain: Overview Report.
Research Report RR931. Health and Safety Executive. 2012.
http://www.hse.gov.uk/research/rrpdf/rr931.pdf (12 November
2014, date last accessed).
30. BBC. Rainy Weather Breaks UK Record for Three Months to
June. http://www.bbc.co.uk/news/uk-18653274 (14 May 2015,
date last accessed).
Downloaded from https://academic.oup.com/occmed/article-abstract/66/1/20/2750628 by guest
on 25 June 2018
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.