Surgical Chart Data Retrieval Worksheet: Case 1 Analysis Report
VerifiedAdded on 2022/08/08
|2
|447
|4
Homework Assignment
AI Summary
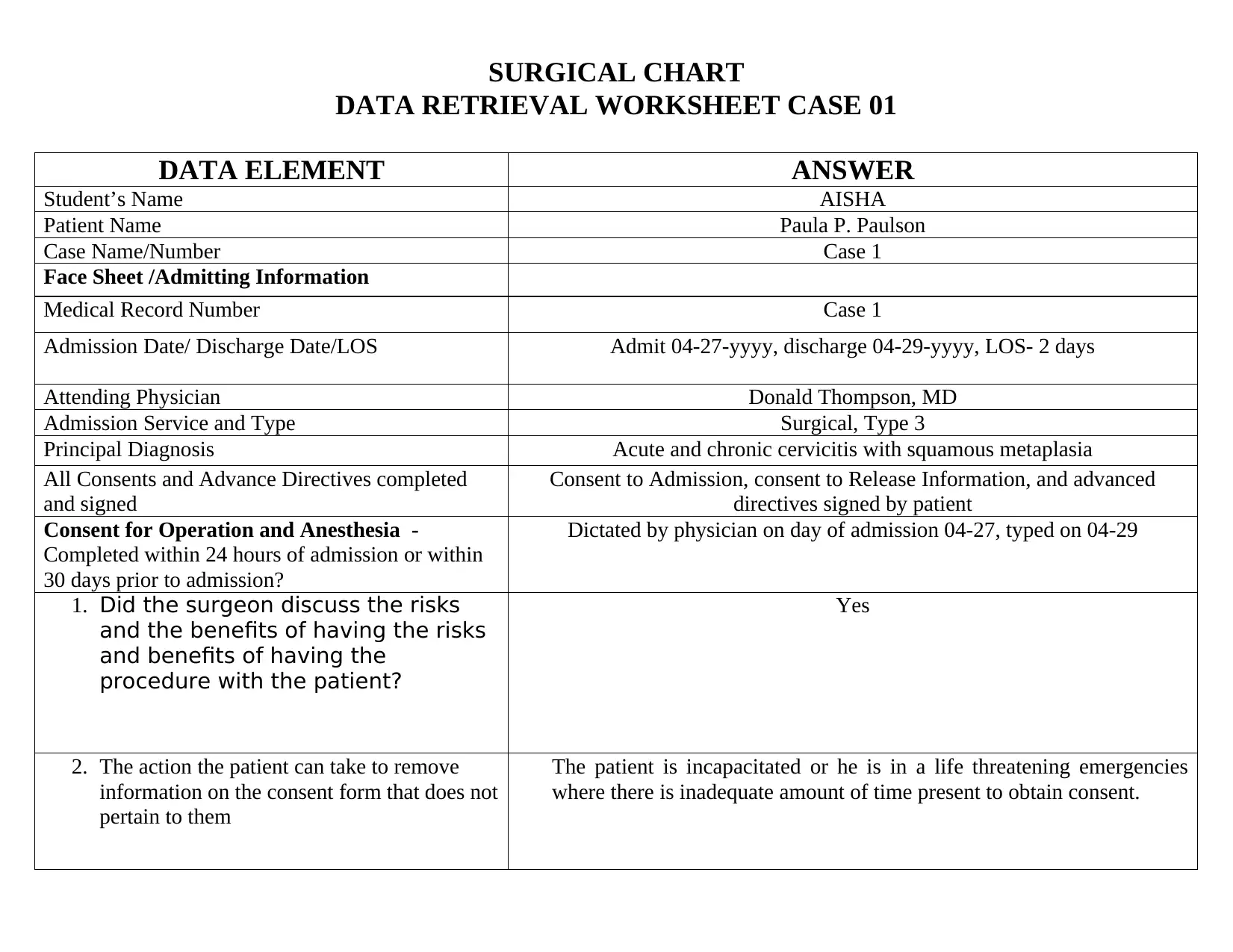
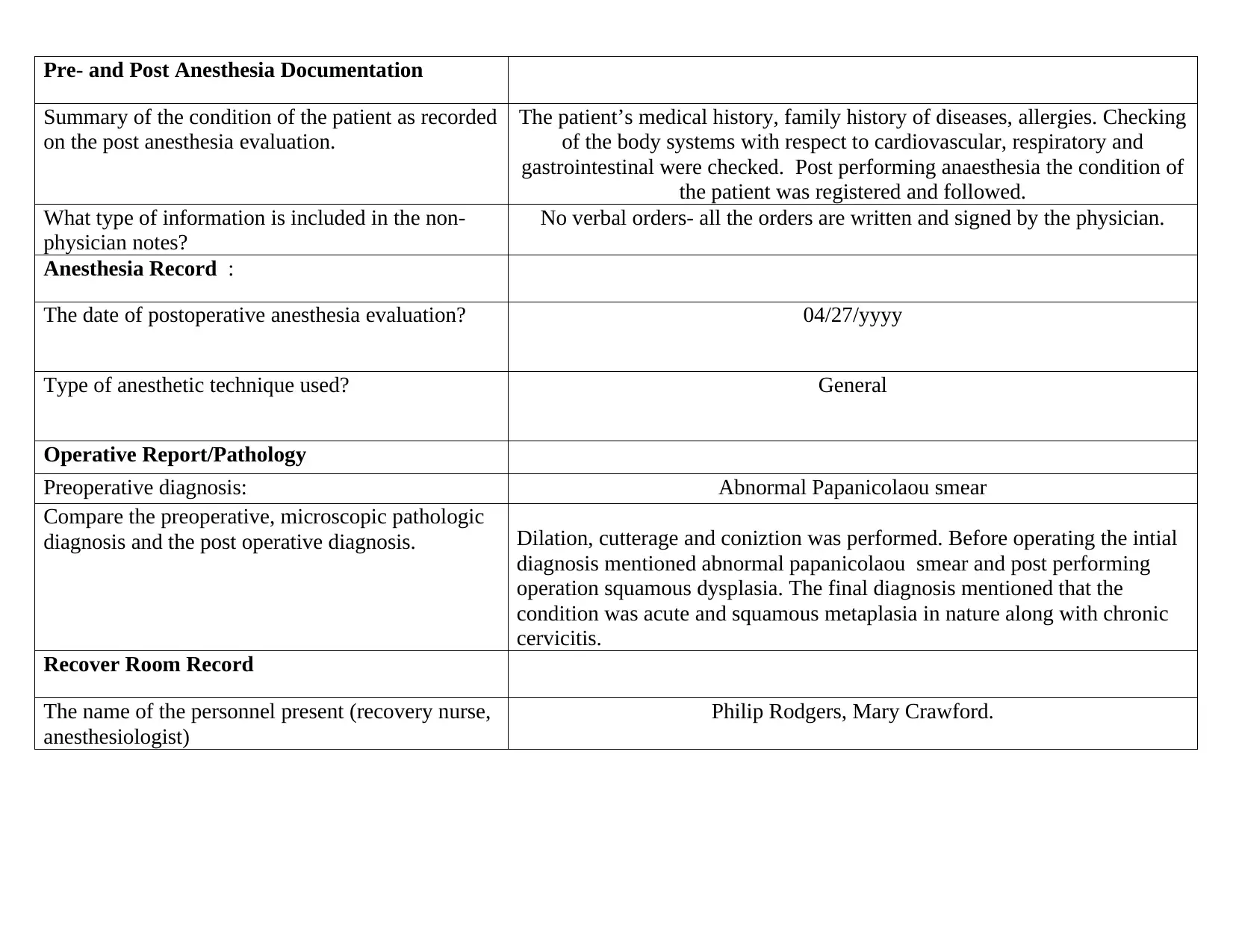
This assignment focuses on the analysis of surgical chart data for Case 1. It involves a detailed review of various sections of the medical record, including the face sheet, consent forms, anesthesia records, operative reports, and recovery room records. The student, Aisha, provides answers to specific data elements, such as patient and physician names, admission and discharge dates, diagnoses, and details related to the surgical procedure performed (dilation, curettage, and conization). The assignment follows a grading rubric that assesses the student's ability to identify areas of compliance and non-compliance with chart analysis guidelines, evaluate consent forms, examine pre- and post-anesthesia documentation, and assess the operative report and recovery room record. The analysis also covers aspects like the discussion of risks and benefits with the patient, the type of anesthetic technique used, and the personnel present in the recovery room. The student's responses demonstrate an understanding of medical record documentation and the ability to extract relevant information for chart analysis.
1 out of 2


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.