Nursing Case Study: Diagnosing Systolic Heart Failure Patient
VerifiedAdded on 2022/09/21
|10
|2149
|36
Case Study
AI Summary
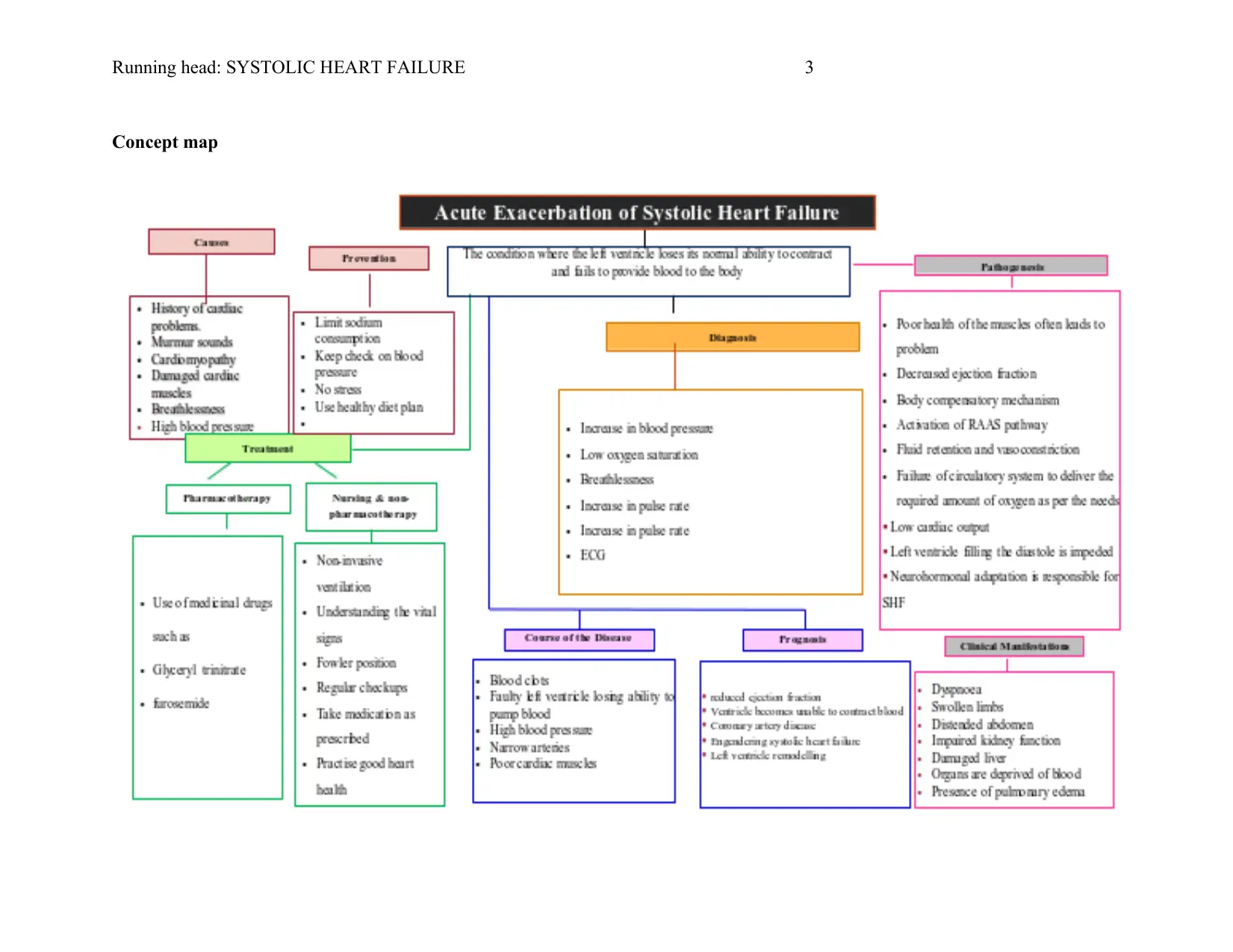
This case study focuses on a patient, Mrs. Brown, presenting with symptoms of systolic heart failure. The analysis begins with an overview of her medical history, including a previous cardiac complication and age-related factors, leading to her reported dyspnea and low oxygen saturation. The pathophysiology of dyspnea, high blood pressure, and atrial fibrillation are explored, along with the use of external oxygen administration, patient positioning, and vital sign monitoring as immediate interventions. The case then addresses the pharmacological management, specifically the use of Furosemide (Lasix) as a diuretic and Sublingual Glyceryl Trinitrate for vasodilation. The case study incorporates relevant research and guidelines to support the diagnosis and treatment strategies, including the NMBA Professional Code of Conduct, emphasizing the importance of nurses' role in patient care and safety. This case study provides a comprehensive understanding of the assessment, diagnosis, and management of systolic heart failure in an elderly patient.

1 out of 10
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.