PUBH610 Health Equity Audit for Stormlands Zone, Australia: Report
VerifiedAdded on 2023/04/08
|11
|2452
|100
Report
AI Summary
This report presents a health equity audit of the Stormlands Zone in Australia, focusing on cancer trends, health risk factors, and causes of death across five subzones. The audit analyzes population demographics, socio-economic disadvantages, and cancer screening program utilization. It highlights disparities in screening participation, particularly for bowel cancer, and examines mortality rates related to various cancers, including lung and breast cancer. The report discusses the role of public health in addressing health inequalities, emphasizing the need for comprehensive assessments of social determinants and equitable resource allocation to improve health outcomes in the Stormlands Zone. This document is available on Desklib, a platform offering a wide range of study resources for students.

Task
Health Equity Audit assessment for Stormlands Zone, Australia
UNIVERSITY
Unit
Student name
Date
Health Equity Audit assessment for Stormlands Zone, Australia
UNIVERSITY
Unit
Student name
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Health Equity Audit assessment for Stormlands Zone, Australia
Introduction
Health equity is essential in the public health arena. According to WHO, equity refers
to the absence of avoidable and unfair differences among different groups. The different
groups can be defined in terms of social standards, economic, parameters, demographics or
geographical locations or any other stratification. Health equity generally implies to
population getting fair access to full health and no segregation on this factor.
Culture enhances the overall responsibility of living a healthy life. Across the nation,
health gaps do exist and tend to show an increasing curve. Health equity assumes the
population to be having fair and just opportunities for positive outcomes, thus the need for
concerted efforts to increase healthy growth opportunities.
Health equity audit is a review of procedures on how key health determinants affect
the population in accessing the relevant health services and outcomes distributed across the
population. Further, it is essential as a decision-making tool for all levels of governance in
prioritizing resources (Vallgårda, 2010).
This health audit focuses on Stormland Region Australia. This audit focuses on cancer
trends, health risks factors and causes of deaths affecting Stomrland, 5 territorial states.
Cancer represents a broad variety of diseases which depict an increased number of different
diseases. Cancer is the leading cause of mortality hence the vital focus for this audit analysis.
The report seeks to assess equity and inequality available for Stormland region comparing 5
subzones and how different actors can play a significant role in any established health
inequity is key.
Health data analysis
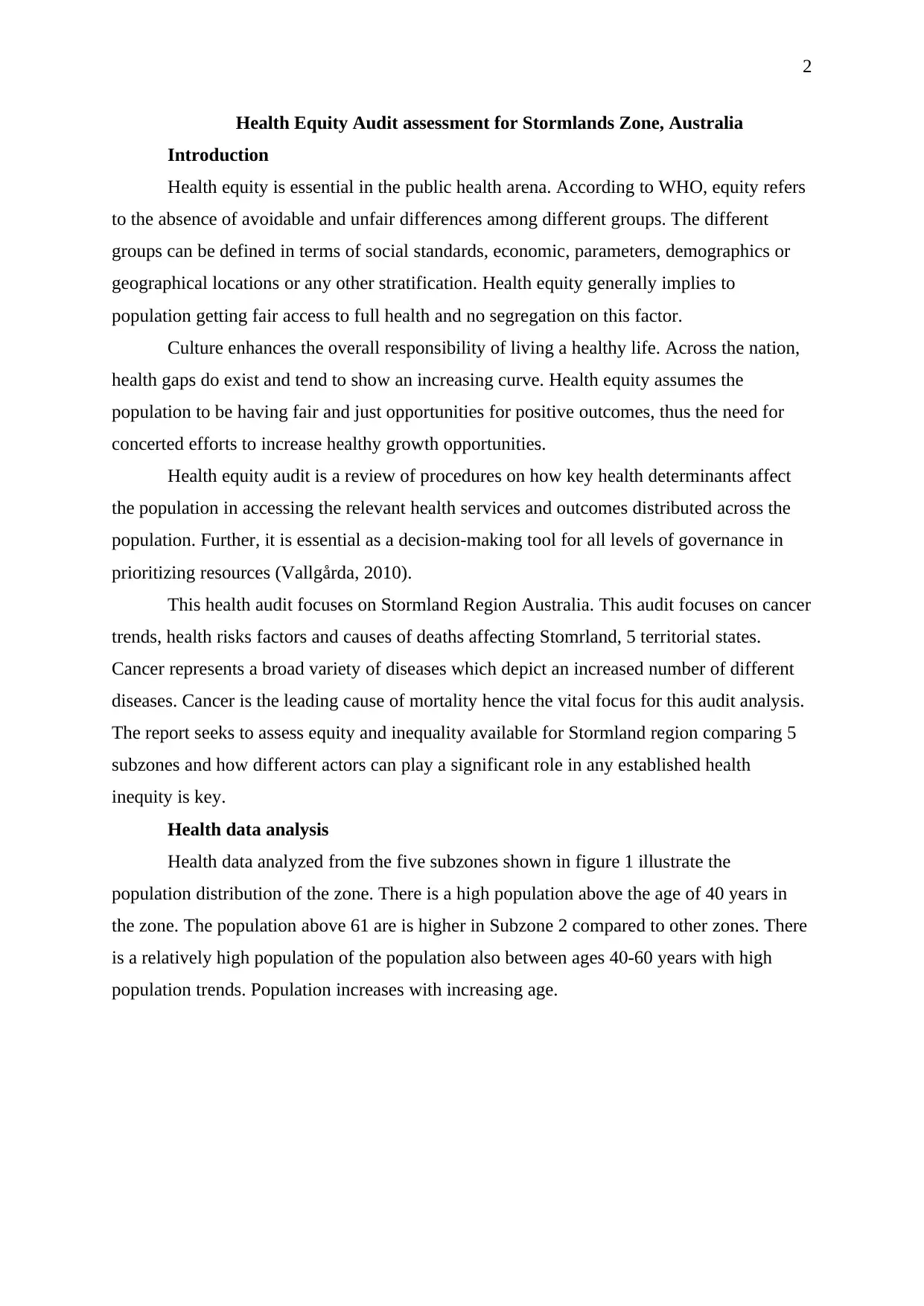
Health data analyzed from the five subzones shown in figure 1 illustrate the
population distribution of the zone. There is a high population above the age of 40 years in
the zone. The population above 61 are is higher in Subzone 2 compared to other zones. There
is a relatively high population of the population also between ages 40-60 years with high
population trends. Population increases with increasing age.
Health Equity Audit assessment for Stormlands Zone, Australia
Introduction
Health equity is essential in the public health arena. According to WHO, equity refers
to the absence of avoidable and unfair differences among different groups. The different
groups can be defined in terms of social standards, economic, parameters, demographics or
geographical locations or any other stratification. Health equity generally implies to
population getting fair access to full health and no segregation on this factor.
Culture enhances the overall responsibility of living a healthy life. Across the nation,
health gaps do exist and tend to show an increasing curve. Health equity assumes the
population to be having fair and just opportunities for positive outcomes, thus the need for
concerted efforts to increase healthy growth opportunities.
Health equity audit is a review of procedures on how key health determinants affect
the population in accessing the relevant health services and outcomes distributed across the
population. Further, it is essential as a decision-making tool for all levels of governance in
prioritizing resources (Vallgårda, 2010).
This health audit focuses on Stormland Region Australia. This audit focuses on cancer
trends, health risks factors and causes of deaths affecting Stomrland, 5 territorial states.
Cancer represents a broad variety of diseases which depict an increased number of different
diseases. Cancer is the leading cause of mortality hence the vital focus for this audit analysis.
The report seeks to assess equity and inequality available for Stormland region comparing 5
subzones and how different actors can play a significant role in any established health
inequity is key.
Health data analysis
Health data analyzed from the five subzones shown in figure 1 illustrate the
population distribution of the zone. There is a high population above the age of 40 years in
the zone. The population above 61 are is higher in Subzone 2 compared to other zones. There
is a relatively high population of the population also between ages 40-60 years with high
population trends. Population increases with increasing age.
3
Persons, below 18
years % Persons, 18-40
years % Persons, 41-60
years % Persons, 61 years
and over %
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
Age distribution of the population
Subzone 15
Subzone 07
Subzone 10
Subzone 14
Subzone 02
Figure 1 Population by age categories
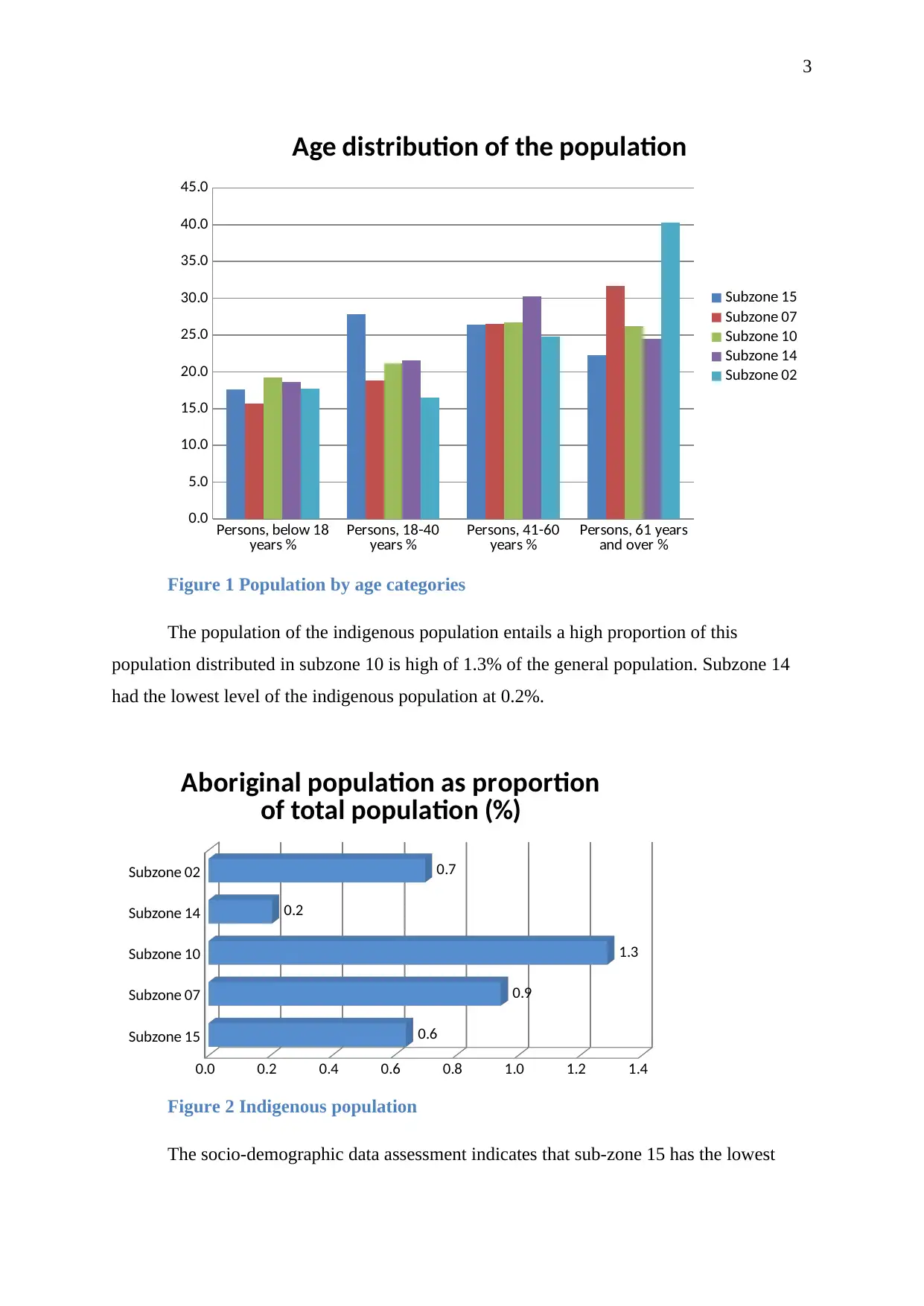
The population of the indigenous population entails a high proportion of this
population distributed in subzone 10 is high of 1.3% of the general population. Subzone 14
had the lowest level of the indigenous population at 0.2%.
Subzone 15
Subzone 07
Subzone 10
Subzone 14
Subzone 02
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4
0.6
0.9
1.3
0.2
0.7
Aboriginal population as proportion
of total population (%)
Figure 2 Indigenous population
The socio-demographic data assessment indicates that sub-zone 15 has the lowest
Persons, below 18
years % Persons, 18-40
years % Persons, 41-60
years % Persons, 61 years
and over %
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
Age distribution of the population
Subzone 15
Subzone 07
Subzone 10
Subzone 14
Subzone 02
Figure 1 Population by age categories
The population of the indigenous population entails a high proportion of this
population distributed in subzone 10 is high of 1.3% of the general population. Subzone 14
had the lowest level of the indigenous population at 0.2%.
Subzone 15
Subzone 07
Subzone 10
Subzone 14
Subzone 02
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4
0.6
0.9
1.3
0.2
0.7
Aboriginal population as proportion
of total population (%)
Figure 2 Indigenous population
The socio-demographic data assessment indicates that sub-zone 15 has the lowest
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
score while subzone based on the general average score of the population. There is a variation
on the socio-economic disadvantaged status of the population.
Table 1Socio economic disadvantage population status
SEIFA Index of Relative Socio-economic
Disadvantage
2011
Name
Index
score
(based on
Australian
score of
1000)
The
minimum
score for
SA1s in
area
The
maximum
score for
SA1s in
area
Aust
rank
(highest
to
lowest
out of
564)
Usual
resident
population
(Census
2011)
Subzone 02 968 901 1061 322 6,372
Subzone 10 998 749 1115 184 42,902
Subzone 14 1091 751 1155 18 91,855
Subzone 15 1047 733 1157 63
118,28
2
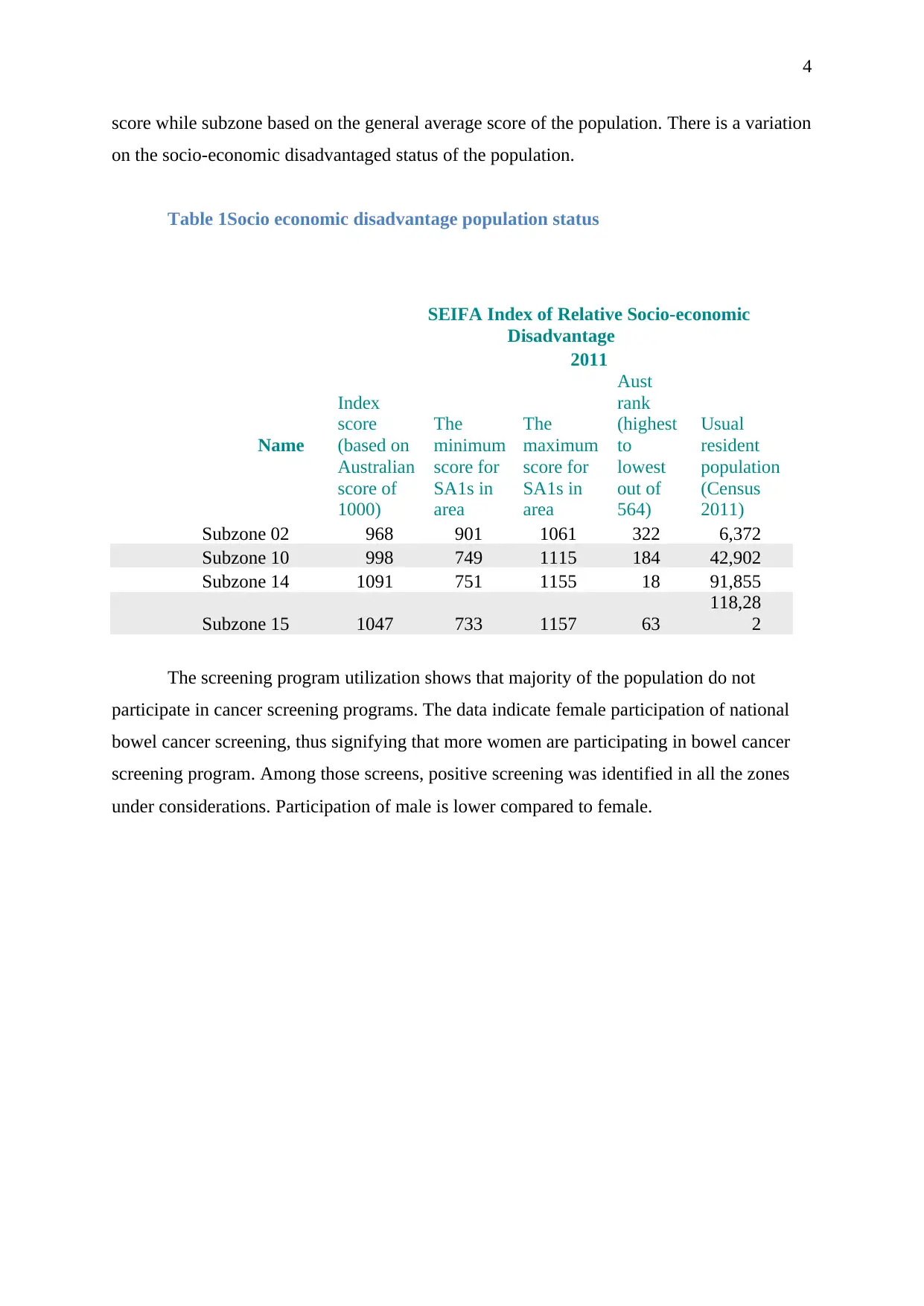
The screening program utilization shows that majority of the population do not
participate in cancer screening programs. The data indicate female participation of national
bowel cancer screening, thus signifying that more women are participating in bowel cancer
screening program. Among those screens, positive screening was identified in all the zones
under considerations. Participation of male is lower compared to female.
score while subzone based on the general average score of the population. There is a variation
on the socio-economic disadvantaged status of the population.
Table 1Socio economic disadvantage population status
SEIFA Index of Relative Socio-economic
Disadvantage
2011
Name
Index
score
(based on
Australian
score of
1000)
The
minimum
score for
SA1s in
area
The
maximum
score for
SA1s in
area
Aust
rank
(highest
to
lowest
out of
564)
Usual
resident
population
(Census
2011)
Subzone 02 968 901 1061 322 6,372
Subzone 10 998 749 1115 184 42,902
Subzone 14 1091 751 1155 18 91,855
Subzone 15 1047 733 1157 63
118,28
2
The screening program utilization shows that majority of the population do not
participate in cancer screening programs. The data indicate female participation of national
bowel cancer screening, thus signifying that more women are participating in bowel cancer
screening program. Among those screens, positive screening was identified in all the zones
under considerations. Participation of male is lower compared to female.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
Subzone 15
Subzone 07
Subzone 10
Subzone 02
Subzone 04
0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 40.0 45.0 50.0
Users of the National Bowel Cancer
Screening Program (NBCSP)
Positive Screening Females %
Positive Screening Males %
Participation in the
NBCSP,Females %
Participation of males %
Figure 3 National Screening program for bowel cancer
Subzone
15 Subzone
07 Subzone
10 Subzone
14 Subzone
02
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
55.4
59.2 61.6 55.4
65.165.7
60.3 63.6
73.6
61.6
Breast and Cervical cancer screening
Breast screening participation,
females aged 50 to 69 years
Cervical screening
participation, females aged 20
to 69 years
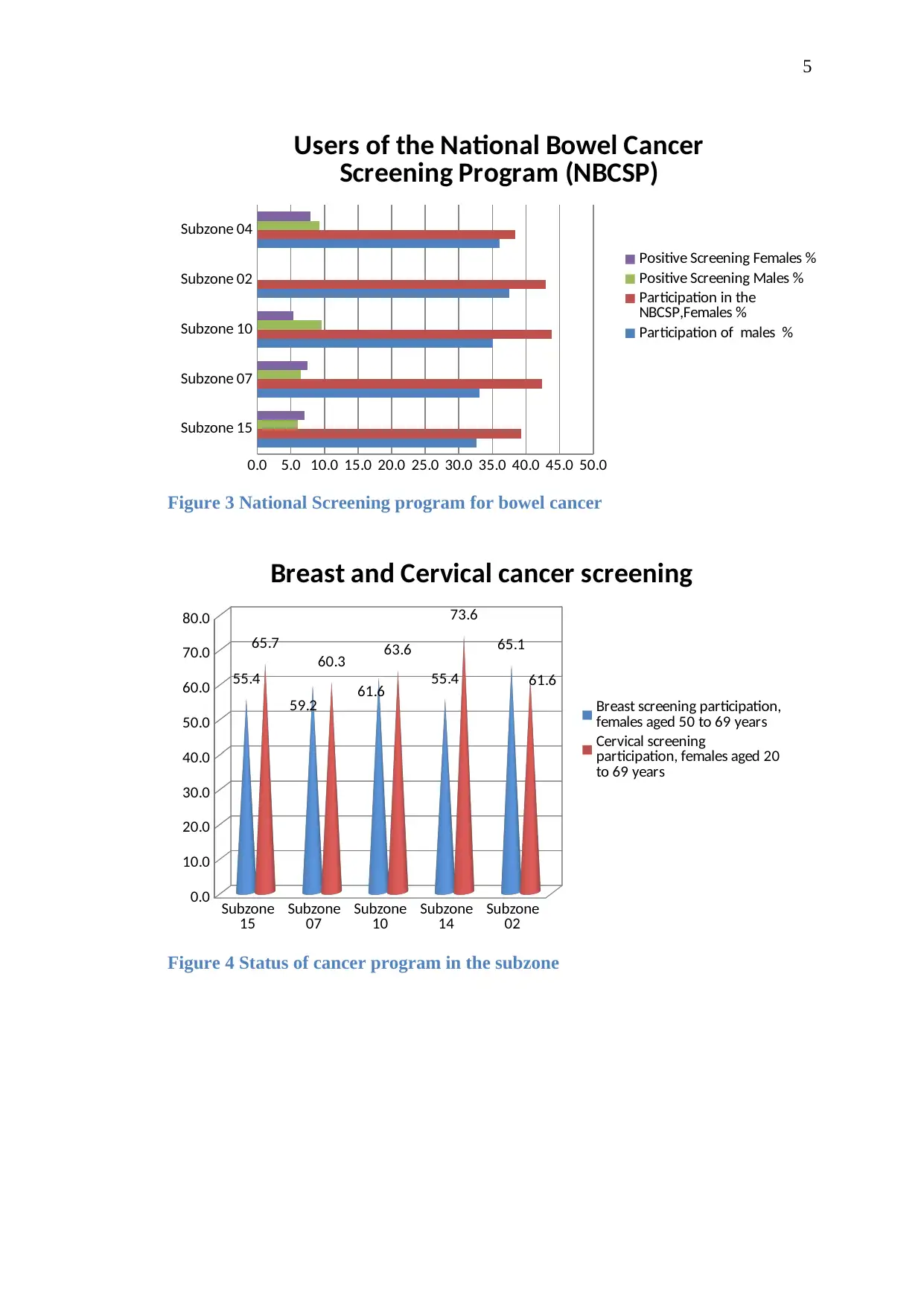
Figure 4 Status of cancer program in the subzone
Subzone 15
Subzone 07
Subzone 10
Subzone 02
Subzone 04
0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 40.0 45.0 50.0
Users of the National Bowel Cancer
Screening Program (NBCSP)
Positive Screening Females %
Positive Screening Males %
Participation in the
NBCSP,Females %
Participation of males %
Figure 3 National Screening program for bowel cancer
Subzone
15 Subzone
07 Subzone
10 Subzone
14 Subzone
02
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
55.4
59.2 61.6 55.4
65.165.7
60.3 63.6
73.6
61.6
Breast and Cervical cancer screening
Breast screening participation,
females aged 50 to 69 years
Cervical screening
participation, females aged 20
to 69 years
Figure 4 Status of cancer program in the subzone
6
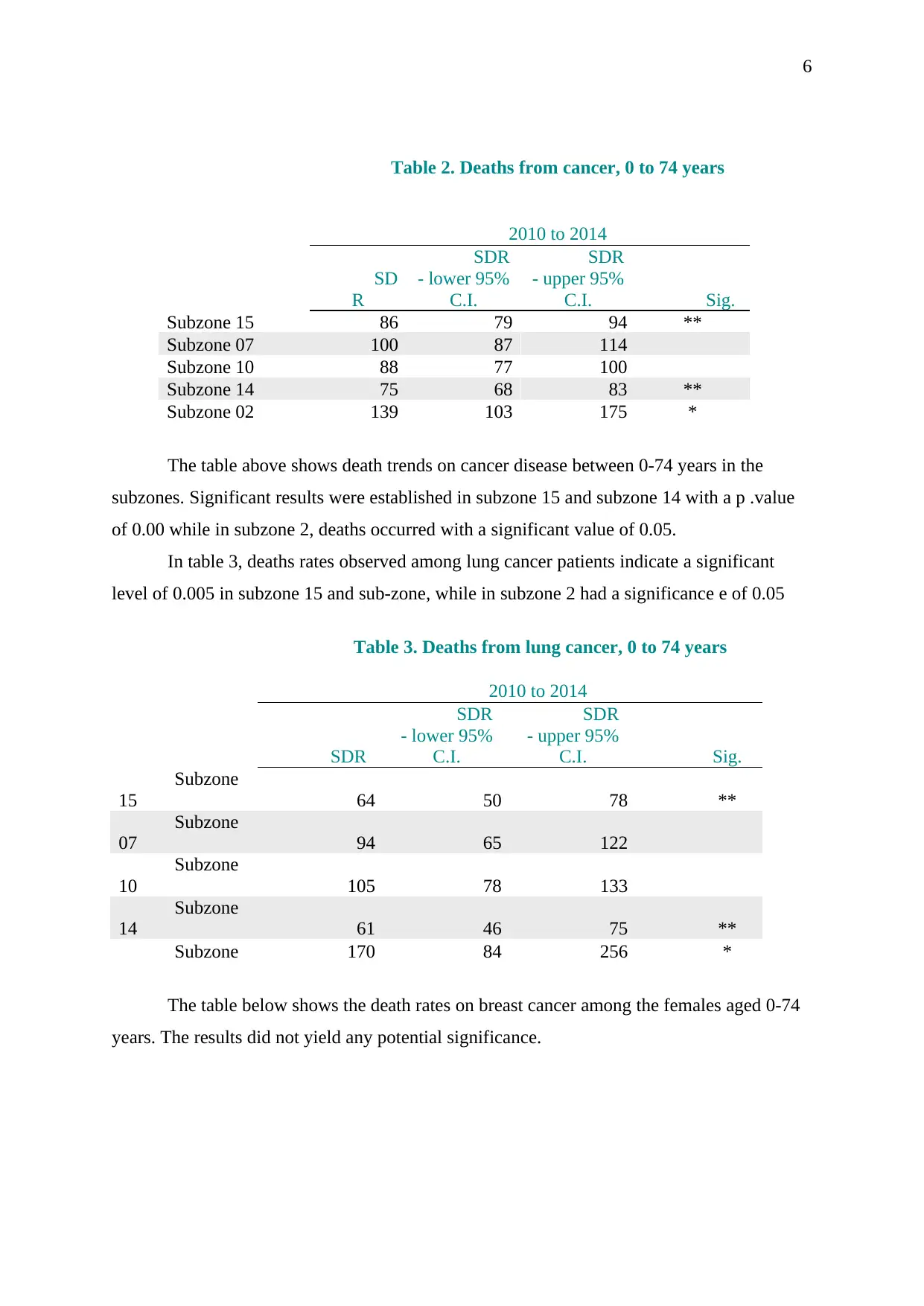
Table 2. Deaths from cancer, 0 to 74 years
2010 to 2014
SD
R
SDR
- lower 95%
C.I.
SDR
- upper 95%
C.I. Sig.
Subzone 15 86 79 94 **
Subzone 07 100 87 114
Subzone 10 88 77 100
Subzone 14 75 68 83 **
Subzone 02 139 103 175 *
The table above shows death trends on cancer disease between 0-74 years in the
subzones. Significant results were established in subzone 15 and subzone 14 with a p .value
of 0.00 while in subzone 2, deaths occurred with a significant value of 0.05.
In table 3, deaths rates observed among lung cancer patients indicate a significant
level of 0.005 in subzone 15 and sub-zone, while in subzone 2 had a significance e of 0.05
Table 3. Deaths from lung cancer, 0 to 74 years
2010 to 2014
SDR
SDR
- lower 95%
C.I.
SDR
- upper 95%
C.I. Sig.
Subzone
15 64 50 78 **
Subzone
07 94 65 122
Subzone
10 105 78 133
Subzone
14 61 46 75 **
Subzone 170 84 256 *
The table below shows the death rates on breast cancer among the females aged 0-74
years. The results did not yield any potential significance.
Table 2. Deaths from cancer, 0 to 74 years
2010 to 2014
SD
R
SDR
- lower 95%
C.I.
SDR
- upper 95%
C.I. Sig.
Subzone 15 86 79 94 **
Subzone 07 100 87 114
Subzone 10 88 77 100
Subzone 14 75 68 83 **
Subzone 02 139 103 175 *
The table above shows death trends on cancer disease between 0-74 years in the
subzones. Significant results were established in subzone 15 and subzone 14 with a p .value
of 0.00 while in subzone 2, deaths occurred with a significant value of 0.05.
In table 3, deaths rates observed among lung cancer patients indicate a significant
level of 0.005 in subzone 15 and sub-zone, while in subzone 2 had a significance e of 0.05
Table 3. Deaths from lung cancer, 0 to 74 years
2010 to 2014
SDR
SDR
- lower 95%
C.I.
SDR
- upper 95%
C.I. Sig.
Subzone
15 64 50 78 **
Subzone
07 94 65 122
Subzone
10 105 78 133
Subzone
14 61 46 75 **
Subzone 170 84 256 *
The table below shows the death rates on breast cancer among the females aged 0-74
years. The results did not yield any potential significance.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
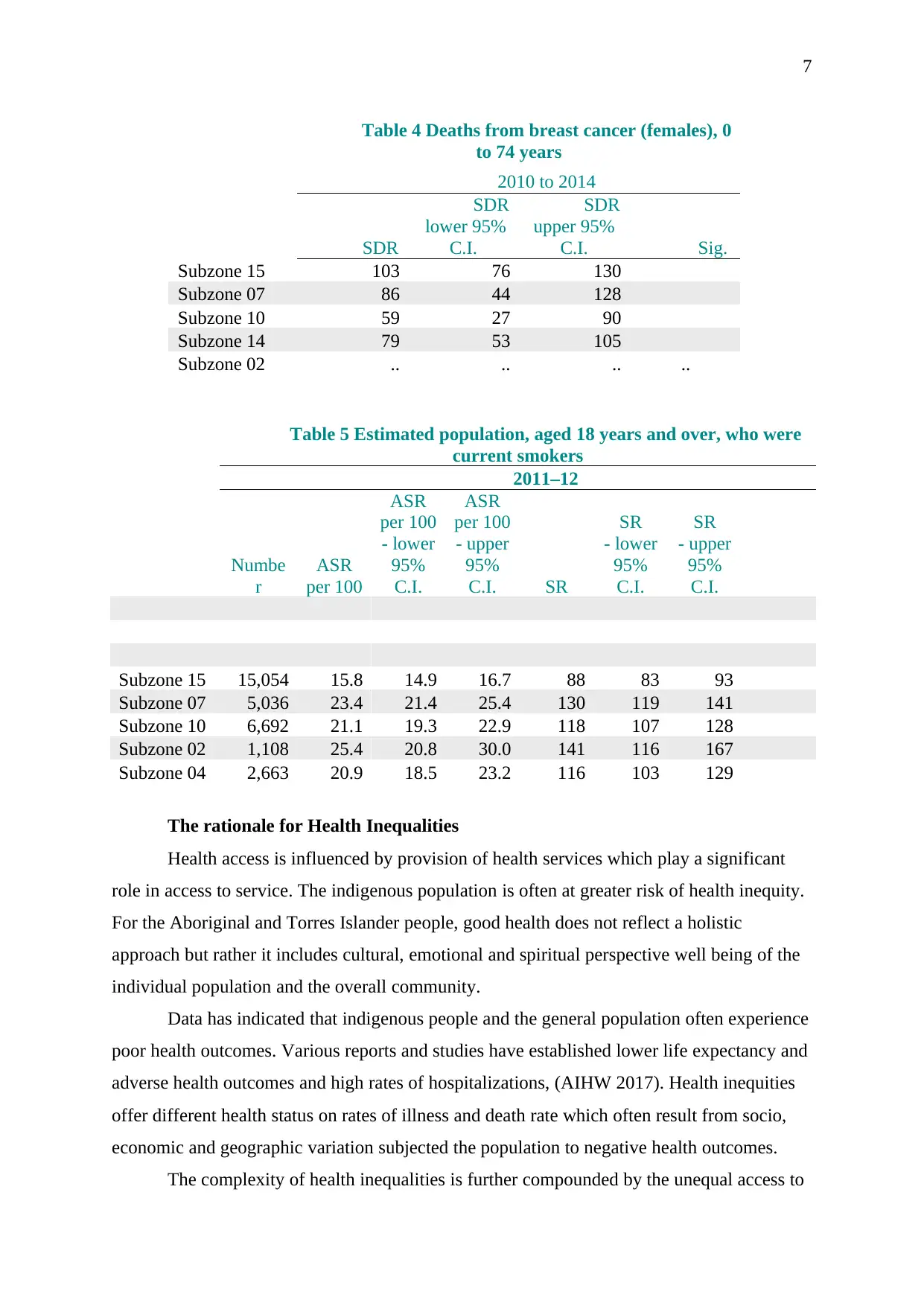
Table 4 Deaths from breast cancer (females), 0
to 74 years
2010 to 2014
SDR
SDR
lower 95%
C.I.
SDR
upper 95%
C.I. Sig.
Subzone 15 103 76 130
Subzone 07 86 44 128
Subzone 10 59 27 90
Subzone 14 79 53 105
Subzone 02 .. .. .. ..
Table 5 Estimated population, aged 18 years and over, who were
current smokers
2011–12
Numbe
r
ASR
per 100
ASR
per 100
- lower
95%
C.I.
ASR
per 100
- upper
95%
C.I. SR
SR
- lower
95%
C.I.
SR
- upper
95%
C.I.
Subzone 15 15,054 15.8 14.9 16.7 88 83 93
Subzone 07 5,036 23.4 21.4 25.4 130 119 141
Subzone 10 6,692 21.1 19.3 22.9 118 107 128
Subzone 02 1,108 25.4 20.8 30.0 141 116 167
Subzone 04 2,663 20.9 18.5 23.2 116 103 129
The rationale for Health Inequalities
Health access is influenced by provision of health services which play a significant
role in access to service. The indigenous population is often at greater risk of health inequity.
For the Aboriginal and Torres Islander people, good health does not reflect a holistic
approach but rather it includes cultural, emotional and spiritual perspective well being of the
individual population and the overall community.
Data has indicated that indigenous people and the general population often experience
poor health outcomes. Various reports and studies have established lower life expectancy and
adverse health outcomes and high rates of hospitalizations, (AIHW 2017). Health inequities
offer different health status on rates of illness and death rate which often result from socio,
economic and geographic variation subjected the population to negative health outcomes.
The complexity of health inequalities is further compounded by the unequal access to
Table 4 Deaths from breast cancer (females), 0
to 74 years
2010 to 2014
SDR
SDR
lower 95%
C.I.
SDR
upper 95%
C.I. Sig.
Subzone 15 103 76 130
Subzone 07 86 44 128
Subzone 10 59 27 90
Subzone 14 79 53 105
Subzone 02 .. .. .. ..
Table 5 Estimated population, aged 18 years and over, who were
current smokers
2011–12
Numbe
r
ASR
per 100
ASR
per 100
- lower
95%
C.I.
ASR
per 100
- upper
95%
C.I. SR
SR
- lower
95%
C.I.
SR
- upper
95%
C.I.
Subzone 15 15,054 15.8 14.9 16.7 88 83 93
Subzone 07 5,036 23.4 21.4 25.4 130 119 141
Subzone 10 6,692 21.1 19.3 22.9 118 107 128
Subzone 02 1,108 25.4 20.8 30.0 141 116 167
Subzone 04 2,663 20.9 18.5 23.2 116 103 129
The rationale for Health Inequalities
Health access is influenced by provision of health services which play a significant
role in access to service. The indigenous population is often at greater risk of health inequity.
For the Aboriginal and Torres Islander people, good health does not reflect a holistic
approach but rather it includes cultural, emotional and spiritual perspective well being of the
individual population and the overall community.
Data has indicated that indigenous people and the general population often experience
poor health outcomes. Various reports and studies have established lower life expectancy and
adverse health outcomes and high rates of hospitalizations, (AIHW 2017). Health inequities
offer different health status on rates of illness and death rate which often result from socio,
economic and geographic variation subjected the population to negative health outcomes.
The complexity of health inequalities is further compounded by the unequal access to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
a resource which facilitates health positive outcomes. These inequalities have a direct impact
on the health status of the population which results in social and psychological problems. An
illustration is an importance of how low income can lead to deprived access to health care
services such as screening and public health initiatives are critical.
Cancer continues to be among the leading causes of death. The number of cancer
cases being diagnosed in Australia is estimated to be 1237,887 new cases. Recent data have
shown a rise in new cases to about 138,321 new cases. The occurrence of death accounted for
about 45,782 deaths with risks increasing with an increase in age.
The associated standardized mortality trends have shown that there an estimate of 484
new cases per 100,000. In recent data, the age-standardized incidence rate accounts for 472
cases per 100,000. The age-standardized mortality rates per 100,000 are estimated to be
around 159 cases with the numbers estimated to increase.
Analysis
The current population of the Stormland zone is estimated to be over 200,000 people.
Majority of this population are those below the age of 18 years. The indigenous population in
subzone 10 account for a higher proportion with 1.3% of the general population.
The economic potential of the subzones is lower compared to the National average
estimates. The population of the disadvantaged among the zones shows a relatively lower
index compared to national scores, as shown in figure 3.
Cancer screening program under the National Bowel Cancer screening program being
implemented by the government has shown slow uptake engagement among the population.
The low participation of screening exercise across the state zones is lower hence low
coverage rate. Males and females participation account for an average of 40% engaging in
bowel cancer screening. Compared to the general population status, the figures are still low
thus there are health challenges in accessing the overall population.
Among the screened population in both sexes, there was a positive screening of bowel
cancer population. Thus, this depicts the significance of cancer problem among the
population. Lack of effective participation leads to low detection of cancer rates.
Breast and cancer screening program shows that, across the zones, there are varied
rates of participation among the four zones. In subzone 15, cervical cancer screening
participation and females aged between 50-69 years had the participation of about 55.4%
while in subzone 2, had a screening rate of 65.1% depicting high rate. Among the cervical
cancer screening conducted for ages 20-69 years, subzone 15 has high rates of 65.7% and a
low of 55.4% in subzone 14. Over ally, subzone 07 had the lowest rates of screening for both
a resource which facilitates health positive outcomes. These inequalities have a direct impact
on the health status of the population which results in social and psychological problems. An
illustration is an importance of how low income can lead to deprived access to health care
services such as screening and public health initiatives are critical.
Cancer continues to be among the leading causes of death. The number of cancer
cases being diagnosed in Australia is estimated to be 1237,887 new cases. Recent data have
shown a rise in new cases to about 138,321 new cases. The occurrence of death accounted for
about 45,782 deaths with risks increasing with an increase in age.
The associated standardized mortality trends have shown that there an estimate of 484
new cases per 100,000. In recent data, the age-standardized incidence rate accounts for 472
cases per 100,000. The age-standardized mortality rates per 100,000 are estimated to be
around 159 cases with the numbers estimated to increase.
Analysis
The current population of the Stormland zone is estimated to be over 200,000 people.
Majority of this population are those below the age of 18 years. The indigenous population in
subzone 10 account for a higher proportion with 1.3% of the general population.
The economic potential of the subzones is lower compared to the National average
estimates. The population of the disadvantaged among the zones shows a relatively lower
index compared to national scores, as shown in figure 3.
Cancer screening program under the National Bowel Cancer screening program being
implemented by the government has shown slow uptake engagement among the population.
The low participation of screening exercise across the state zones is lower hence low
coverage rate. Males and females participation account for an average of 40% engaging in
bowel cancer screening. Compared to the general population status, the figures are still low
thus there are health challenges in accessing the overall population.
Among the screened population in both sexes, there was a positive screening of bowel
cancer population. Thus, this depicts the significance of cancer problem among the
population. Lack of effective participation leads to low detection of cancer rates.
Breast and cancer screening program shows that, across the zones, there are varied
rates of participation among the four zones. In subzone 15, cervical cancer screening
participation and females aged between 50-69 years had the participation of about 55.4%
while in subzone 2, had a screening rate of 65.1% depicting high rate. Among the cervical
cancer screening conducted for ages 20-69 years, subzone 15 has high rates of 65.7% and a
low of 55.4% in subzone 14. Over ally, subzone 07 had the lowest rates of screening for both
9
breast and cervical cancer.
The causes of death among the population indicate that cancer still remains the largest
cause of death among the population of the zone. Among 0-74 years, deaths attributed to
cancer had a significance level of 0.05 at subzone 15 and 14. More cancer-related deaths
were observed in these two zones on a 95% confidence level (79:94, 68:83) respectively.
Cancer is continuous to be the leading of cause mortality and thus screening plays a
fundamental role in ensuring that these deaths are minimized through identification of the
true positives having a disease. On cause-specific mortality, lung cancer remains to be
largely be seen as the specific cause mortality rate with a high significance level. Lung cancer
cases have high mortality in subzone 15 and 14.
Role of public health
The health concern related to cancer mortality trends across the population of the
Australian Stormaland Zone calls for urgent attention. There is a need for a comprehensive
assessment of determining the key aspects which control the inequities existing in the
population. The social determinants which hinder the population from participating in health
care screening assessments need to be focussed (Harris-Roxas et al., 2012).
The population participating in the screening process is small, hence the need for
more emphasis on cancer screening as observed, it is currently the leading cause of mortality.
In assessing the social determinants of health, there is a need in addressing the inequities
affecting the structural process of health awareness in the population. The differential
perspective occurring in the population reflects the social stratifications systems depicting
differences in the health care status of the population (Nansen et al., 2012).
More equity on health care resources should be implemented in the population, not all
healthy approaches could have a significant impact on the overall population status.
Addressing equity of the population can lead to disadvantaging other settings when dealing
with a larger proportion of people.
Addressing the questions of equity calls for leveling of the social gradient of
population health, so as the middle groups experience the health screening programs. Further
as illustrated by Killoran Ross & Craig, (2011) distinguishing the question of does it works is
essential in implementing cancer screening for ht population. The need for reduced health
inequities through 100% cancer screening coverage is crucial for this population. Addressing
cancer screening in order to achieve greater coverage is of significance in this nursing
practice. Addressing cancer screening issues through attainment of over 90% participation is
key in reducing the inequities existing in the Stomaland Zone.
breast and cervical cancer.
The causes of death among the population indicate that cancer still remains the largest
cause of death among the population of the zone. Among 0-74 years, deaths attributed to
cancer had a significance level of 0.05 at subzone 15 and 14. More cancer-related deaths
were observed in these two zones on a 95% confidence level (79:94, 68:83) respectively.
Cancer is continuous to be the leading of cause mortality and thus screening plays a
fundamental role in ensuring that these deaths are minimized through identification of the
true positives having a disease. On cause-specific mortality, lung cancer remains to be
largely be seen as the specific cause mortality rate with a high significance level. Lung cancer
cases have high mortality in subzone 15 and 14.
Role of public health
The health concern related to cancer mortality trends across the population of the
Australian Stormaland Zone calls for urgent attention. There is a need for a comprehensive
assessment of determining the key aspects which control the inequities existing in the
population. The social determinants which hinder the population from participating in health
care screening assessments need to be focussed (Harris-Roxas et al., 2012).
The population participating in the screening process is small, hence the need for
more emphasis on cancer screening as observed, it is currently the leading cause of mortality.
In assessing the social determinants of health, there is a need in addressing the inequities
affecting the structural process of health awareness in the population. The differential
perspective occurring in the population reflects the social stratifications systems depicting
differences in the health care status of the population (Nansen et al., 2012).
More equity on health care resources should be implemented in the population, not all
healthy approaches could have a significant impact on the overall population status.
Addressing equity of the population can lead to disadvantaging other settings when dealing
with a larger proportion of people.
Addressing the questions of equity calls for leveling of the social gradient of
population health, so as the middle groups experience the health screening programs. Further
as illustrated by Killoran Ross & Craig, (2011) distinguishing the question of does it works is
essential in implementing cancer screening for ht population. The need for reduced health
inequities through 100% cancer screening coverage is crucial for this population. Addressing
cancer screening in order to achieve greater coverage is of significance in this nursing
practice. Addressing cancer screening issues through attainment of over 90% participation is
key in reducing the inequities existing in the Stomaland Zone.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
Further cancer screening needs to consider the cultural perceptions and practices of
the indigenous population. Addressing the barriers towards participating in the national
promotion for screening is key so as to achieve improved rates of cancer and thus improving
the health outcomes of the population (Mundel & Chapman, 2010). Addressing factors such
as smoking is vital reducing lung cancer deaths.
Conclusion
The results of this analysis illustrate similar trends as those observed in other states,
which have shown increased incidences of smoking, leading to number two cause of deaths
across all age groups. Thus the public health initiatives need to engage in anti-smoking
campaigning needs to be rolled. Understanding the needs of the indigenous community is
essential so as to ensure targeted programs. Public health programs for screening need to be
rolled out to the general population. Cancer remains to be among the top causes of death in
Australia. Cancer screening rates are still low hence the need for public health initiatives to
enhance cancer awareness campaign to the general population to improve screening coverage
rates.
Further cancer screening needs to consider the cultural perceptions and practices of
the indigenous population. Addressing the barriers towards participating in the national
promotion for screening is key so as to achieve improved rates of cancer and thus improving
the health outcomes of the population (Mundel & Chapman, 2010). Addressing factors such
as smoking is vital reducing lung cancer deaths.
Conclusion
The results of this analysis illustrate similar trends as those observed in other states,
which have shown increased incidences of smoking, leading to number two cause of deaths
across all age groups. Thus the public health initiatives need to engage in anti-smoking
campaigning needs to be rolled. Understanding the needs of the indigenous community is
essential so as to ensure targeted programs. Public health programs for screening need to be
rolled out to the general population. Cancer remains to be among the top causes of death in
Australia. Cancer screening rates are still low hence the need for public health initiatives to
enhance cancer awareness campaign to the general population to improve screening coverage
rates.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
References
Harris-Roxas, B., Viliani, F., Bond, A., Cave, B., Divall, M., Furu, P., ... & Winkler, M.
(2012). Health impact assessment: the state of the art. Impact assessment and project
appraisal, 30(1), 43-52.
Killoran Ross, M., & Craig, P. (2011). Tackling inequalities in primary care mental health.
Journal of Public Mental Health, 10(2), 99-109.
Mundel, E., & Chapman, G. E. (2010). A decolonizing approach to health promotion in
Canada: the case of the Urban Aboriginal Community Kitchen Garden Project. Health
Promotion International, 25(2), 166-173.
Nansen, B., Chakraborty, K., Gibbs, L., MacDougall, C., & Vetere, F. (2012). Children and
Digital Wellbeing in Australia: Online regulation, conduct and competence. Journal Of
Children And Media, 6(2), 237-254. doi: 10.1080/17482798.2011.619548
Vallgårda, S. (2010). Tackling social inequalities in health in the Nordic countries: targeting a
residuum or the whole population?. Journal of Epidemiology & Community Health,
64(6), 495-496
Australian Institute of Health and Welfare (AIHW) 2017. All cancers combined. Canberra:
AIHW. [Accessed February 2019]. Retrieved from https://www.aihw.gov.au/
References
Harris-Roxas, B., Viliani, F., Bond, A., Cave, B., Divall, M., Furu, P., ... & Winkler, M.
(2012). Health impact assessment: the state of the art. Impact assessment and project
appraisal, 30(1), 43-52.
Killoran Ross, M., & Craig, P. (2011). Tackling inequalities in primary care mental health.
Journal of Public Mental Health, 10(2), 99-109.
Mundel, E., & Chapman, G. E. (2010). A decolonizing approach to health promotion in
Canada: the case of the Urban Aboriginal Community Kitchen Garden Project. Health
Promotion International, 25(2), 166-173.
Nansen, B., Chakraborty, K., Gibbs, L., MacDougall, C., & Vetere, F. (2012). Children and
Digital Wellbeing in Australia: Online regulation, conduct and competence. Journal Of
Children And Media, 6(2), 237-254. doi: 10.1080/17482798.2011.619548
Vallgårda, S. (2010). Tackling social inequalities in health in the Nordic countries: targeting a
residuum or the whole population?. Journal of Epidemiology & Community Health,
64(6), 495-496
Australian Institute of Health and Welfare (AIHW) 2017. All cancers combined. Canberra:
AIHW. [Accessed February 2019]. Retrieved from https://www.aihw.gov.au/
1 out of 11
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.