Charles Sturt University ITC571: Telemedicine in COPD - A Review
VerifiedAdded on 2024/07/12
|15
|3439
|271
Report
AI Summary
This report reviews the application of telemedicine in managing Chronic Obstructive Pulmonary Disease (COPD). It begins with an introduction to telemedicine, its phenomenology, methods, and applications, followed by background information on COPD. The report details an approach encompassing architecture, cooperation, intervention strategies such as telephone counseling and forced spirometry, data acquisition methods using sensors and signal conditioning, and data analysis. Results are presented concerning body structure, living with COPD including physical and mental limitations, and the benefits of telemedicine in terms of accessibility, support, and analytical insights. The discussion highlights telemedicine's potential in overcoming disease limitations, concluding with abbreviations and references. The study uses figures to depict telemedicine application and redundancy between different application systems focusing on chronic diseases.
Charles Sturt University
ITC571: Emerging Technologies and
Innovation
Project Type: Review
Chronic Obstructive Pulmonary Disease with
the help of telemedicine
1
ITC571: Emerging Technologies and
Innovation
Project Type: Review
Chronic Obstructive Pulmonary Disease with
the help of telemedicine
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of content
1. Introduction to Telemedicine
1.1. Phenomenology
1.2. Methods
1.3. Applications available
2. Background of Chronic Obstructive Pulmonary Disease
3. Approach
3.1. Architecture
3.2. Cooperation
3.3. Intervention
3.4. Data acquisition
3.5. Data analysis
4. Results
4.1. Body structure
4.2. Living with Chronic Operative Pulmonary Disease
4.2.1. Physical limitations
4.2.2. Mental limitations
4.3. Getting care through Telemedicine
4.3.1. Accessibility
4.3.2. Support
4.3.3. Analytical insights
5. Discussion
5.1. Unlocking the limitations of disease through telemedicine
6. Conclusion
7. Abbreviation
8. Table of content
9. References
2
1. Introduction to Telemedicine
1.1. Phenomenology
1.2. Methods
1.3. Applications available
2. Background of Chronic Obstructive Pulmonary Disease
3. Approach
3.1. Architecture
3.2. Cooperation
3.3. Intervention
3.4. Data acquisition
3.5. Data analysis
4. Results
4.1. Body structure
4.2. Living with Chronic Operative Pulmonary Disease
4.2.1. Physical limitations
4.2.2. Mental limitations
4.3. Getting care through Telemedicine
4.3.1. Accessibility
4.3.2. Support
4.3.3. Analytical insights
5. Discussion
5.1. Unlocking the limitations of disease through telemedicine
6. Conclusion
7. Abbreviation
8. Table of content
9. References
2

1. Introduction to Telemedicine
Telecommunication and medicine are brought together to cater for health services remotely
known as telemedicine. It was first introduced in the early 1970s. Through telemedicine patients
can get consistent access to the preferred services, decreases the cost and increase the quality of
productivity and care and also disregard the distance barriers. Patients use telemedicine when
needed urgent access to the medical services and cannot travel to the specialist. It also provides
immense opportunities to the medical students from the expertise specialists. Telemedicine is
accessible and evolving constantly as it comes with new advancements in technology, and adapts
the rapids changes in health needs of the societies (Edoh, Pawar, & Kora, 2018). Telemedicine is
completely distinguished from telehealth, telehealth is restricted to the physicians only and
telemedicine services are open to health professionals from different fields including
pharmacists, nursing, and others. Telemedicine applications provoke types of transmissions like
text, audio, video, and image with varying Quality of Services requirements. In order to deliver
high quality of services, QoS requirements are accomplished by network providers. As per the
QoS, telemedicine services are required to have reliability, availability and low delay (Edoh et
al., 2018). The prevalence of chronic neurological disorder increases with the old age people,
access to the neurologist care is likely to worsen in various regions. The telemedicine is defined
as the use of real-time and also the video conferencing for the delivery of medical care. It can
also be used for improving the access to neurologist care for patients who are suffering a range
of chronic disorders as cancer, dementia, and others. Many of the previous studies show the
advantage of telemedicine in the delivery of healthcare facility for the customer.
Telemedicine can be categorized in two terms: Store and forward, and real-time
interactive.(Grogan et al., 2017)Gathering medical data and transmitting it to a practitioner or a
medical specialist for assessment is defined as store and forward. In this category of
telemedicine, the patient’s assessments are recorded in actual time and practitioner reviews at the
later time, based on this patients is recommended further care. This method of telemedicine
would be acceptable for providers and patient and gives an alternate path that increases the
number of patients available to assess by telemedicine. (Pulley et al., 2018) This method has
been rated high because of its mobility feature, severe mobility patients can get treated by
staying back home. In spite of being so many benefits, store and forward has some difficulty in
some areas where telemedicine has included with the video file. Size of the video file might
3
Telecommunication and medicine are brought together to cater for health services remotely
known as telemedicine. It was first introduced in the early 1970s. Through telemedicine patients
can get consistent access to the preferred services, decreases the cost and increase the quality of
productivity and care and also disregard the distance barriers. Patients use telemedicine when
needed urgent access to the medical services and cannot travel to the specialist. It also provides
immense opportunities to the medical students from the expertise specialists. Telemedicine is
accessible and evolving constantly as it comes with new advancements in technology, and adapts
the rapids changes in health needs of the societies (Edoh, Pawar, & Kora, 2018). Telemedicine is
completely distinguished from telehealth, telehealth is restricted to the physicians only and
telemedicine services are open to health professionals from different fields including
pharmacists, nursing, and others. Telemedicine applications provoke types of transmissions like
text, audio, video, and image with varying Quality of Services requirements. In order to deliver
high quality of services, QoS requirements are accomplished by network providers. As per the
QoS, telemedicine services are required to have reliability, availability and low delay (Edoh et
al., 2018). The prevalence of chronic neurological disorder increases with the old age people,
access to the neurologist care is likely to worsen in various regions. The telemedicine is defined
as the use of real-time and also the video conferencing for the delivery of medical care. It can
also be used for improving the access to neurologist care for patients who are suffering a range
of chronic disorders as cancer, dementia, and others. Many of the previous studies show the
advantage of telemedicine in the delivery of healthcare facility for the customer.
Telemedicine can be categorized in two terms: Store and forward, and real-time
interactive.(Grogan et al., 2017)Gathering medical data and transmitting it to a practitioner or a
medical specialist for assessment is defined as store and forward. In this category of
telemedicine, the patient’s assessments are recorded in actual time and practitioner reviews at the
later time, based on this patients is recommended further care. This method of telemedicine
would be acceptable for providers and patient and gives an alternate path that increases the
number of patients available to assess by telemedicine. (Pulley et al., 2018) This method has
been rated high because of its mobility feature, severe mobility patients can get treated by
staying back home. In spite of being so many benefits, store and forward has some difficulty in
some areas where telemedicine has included with the video file. Size of the video file might
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
sometimes big enough that there's no adequate capacity of storage is not available to store.
(Pulley et al., 2018) The second category is real-time interactive telemedicine where there’s an
interaction between doctors and patients parted with distance. (Sasikala, Indhira, &
Chandrasekaran, 2018)
4
(Pulley et al., 2018) The second category is real-time interactive telemedicine where there’s an
interaction between doctors and patients parted with distance. (Sasikala, Indhira, &
Chandrasekaran, 2018)
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1.2 Phenomenology
Phenomenology is a generalized analysis of the appearance of things which is related with an
appearance anything that conscious for individual. The presumption of phenomenology is that
everything that comes to our consciousness has the certain value and is legitimate for
investigation. COPD patients assume that there is no healing for this disease and it will only get
worse, phenomenology helps in finding and confront their experiences and emotions got during
the exacerbation. It is monitored especially right after the exacerbation- as this might only time
nurses can read the state of mind and have a chance to intervene positively. (Rosa et al., 2017)
5
Phenomenology is a generalized analysis of the appearance of things which is related with an
appearance anything that conscious for individual. The presumption of phenomenology is that
everything that comes to our consciousness has the certain value and is legitimate for
investigation. COPD patients assume that there is no healing for this disease and it will only get
worse, phenomenology helps in finding and confront their experiences and emotions got during
the exacerbation. It is monitored especially right after the exacerbation- as this might only time
nurses can read the state of mind and have a chance to intervene positively. (Rosa et al., 2017)
5
2. Background of Chronic Obstructive Pulmonary Disease
Chronic Obstructive Pulmonary Disease has basically affected the people aged above 25. COPD
has effecting symptoms of burden and very less controlled symptoms that needed to have the
greater level of care. This is characterized under intermittent worsening of symptoms which
leads to acute exacerbations.(Central, 2016) As per the several pieces of evidence, more or less
half of all exacerbations are caused by bacteria. Respiratory tract bacteriology exacerbations,
immune's responses to bacterial pathogens, relations of airways tenderness with outcomes of
sputum ability during exacerbations are included in the evidence. Haemophilus influenzae,
Chlamydia pneumoniae, Moraxella catarrhalis, and Streptococcus pneumoniae are the most
important exacerbations of this disease caused by the bacteria. (Murphy & Sethi, 2002)
The factors that define the severity of COPD (simple or complicated) are how severe the
lung disease is, how frequently the patient have the exacerbation or does a patient have comorbid
conditions. If it is a simple COPD, patients get treated with the macrolide, or a spectrum oral
cephalosporin; if it is diagnosed as complicated COPD, it is treated with clavulanate/amoxicillin
or fluoroquinolone. (Barken, Thygesen, & Söderhamn, 2018)
6
Chronic Obstructive Pulmonary Disease has basically affected the people aged above 25. COPD
has effecting symptoms of burden and very less controlled symptoms that needed to have the
greater level of care. This is characterized under intermittent worsening of symptoms which
leads to acute exacerbations.(Central, 2016) As per the several pieces of evidence, more or less
half of all exacerbations are caused by bacteria. Respiratory tract bacteriology exacerbations,
immune's responses to bacterial pathogens, relations of airways tenderness with outcomes of
sputum ability during exacerbations are included in the evidence. Haemophilus influenzae,
Chlamydia pneumoniae, Moraxella catarrhalis, and Streptococcus pneumoniae are the most
important exacerbations of this disease caused by the bacteria. (Murphy & Sethi, 2002)
The factors that define the severity of COPD (simple or complicated) are how severe the
lung disease is, how frequently the patient have the exacerbation or does a patient have comorbid
conditions. If it is a simple COPD, patients get treated with the macrolide, or a spectrum oral
cephalosporin; if it is diagnosed as complicated COPD, it is treated with clavulanate/amoxicillin
or fluoroquinolone. (Barken, Thygesen, & Söderhamn, 2018)
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3. Approach
3.1 Architecture
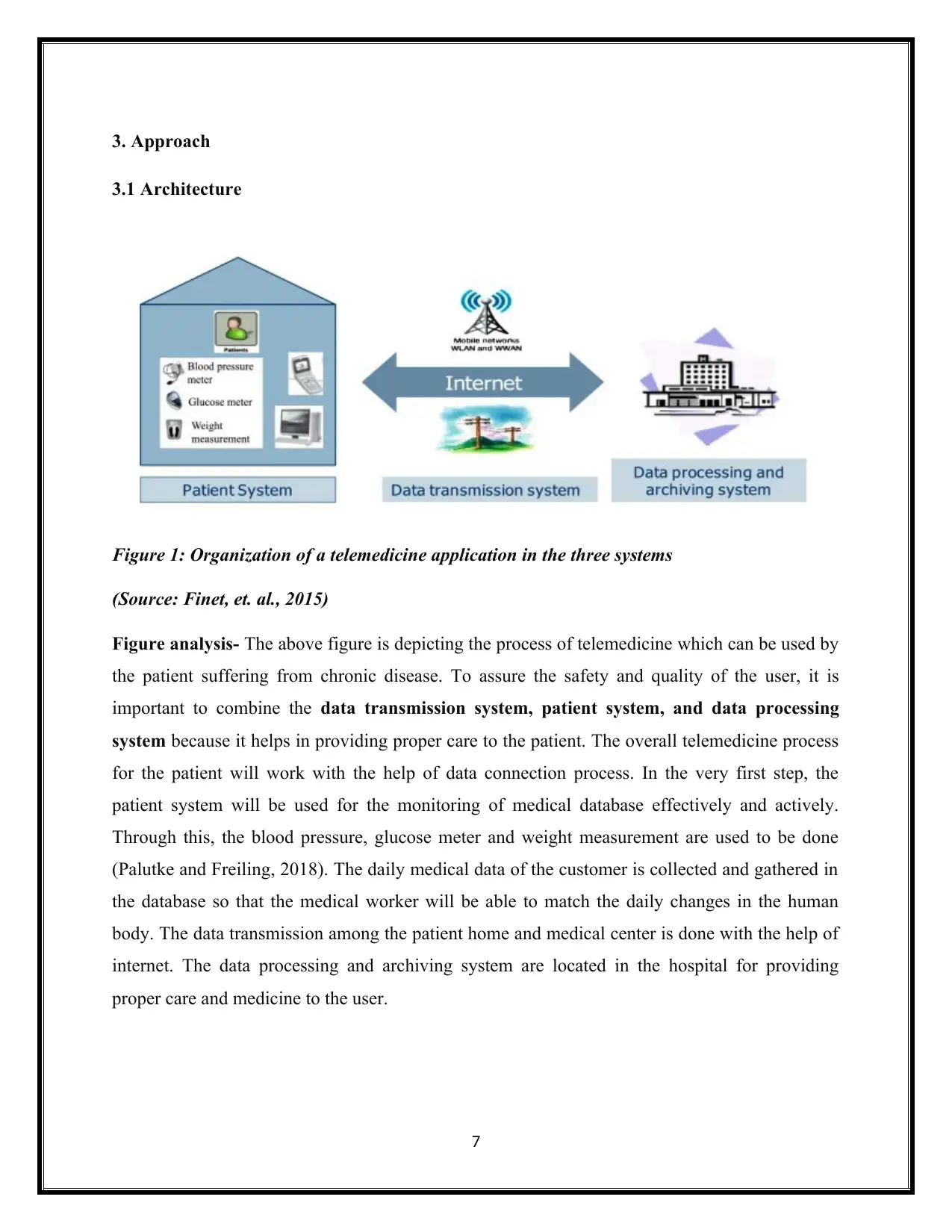
Figure 1: Organization of a telemedicine application in the three systems
(Source: Finet, et. al., 2015)
Figure analysis- The above figure is depicting the process of telemedicine which can be used by
the patient suffering from chronic disease. To assure the safety and quality of the user, it is
important to combine the data transmission system, patient system, and data processing
system because it helps in providing proper care to the patient. The overall telemedicine process
for the patient will work with the help of data connection process. In the very first step, the
patient system will be used for the monitoring of medical database effectively and actively.
Through this, the blood pressure, glucose meter and weight measurement are used to be done
(Palutke and Freiling, 2018). The daily medical data of the customer is collected and gathered in
the database so that the medical worker will be able to match the daily changes in the human
body. The data transmission among the patient home and medical center is done with the help of
internet. The data processing and archiving system are located in the hospital for providing
proper care and medicine to the user.
7
3.1 Architecture
Figure 1: Organization of a telemedicine application in the three systems
(Source: Finet, et. al., 2015)
Figure analysis- The above figure is depicting the process of telemedicine which can be used by
the patient suffering from chronic disease. To assure the safety and quality of the user, it is
important to combine the data transmission system, patient system, and data processing
system because it helps in providing proper care to the patient. The overall telemedicine process
for the patient will work with the help of data connection process. In the very first step, the
patient system will be used for the monitoring of medical database effectively and actively.
Through this, the blood pressure, glucose meter and weight measurement are used to be done
(Palutke and Freiling, 2018). The daily medical data of the customer is collected and gathered in
the database so that the medical worker will be able to match the daily changes in the human
body. The data transmission among the patient home and medical center is done with the help of
internet. The data processing and archiving system are located in the hospital for providing
proper care and medicine to the user.
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
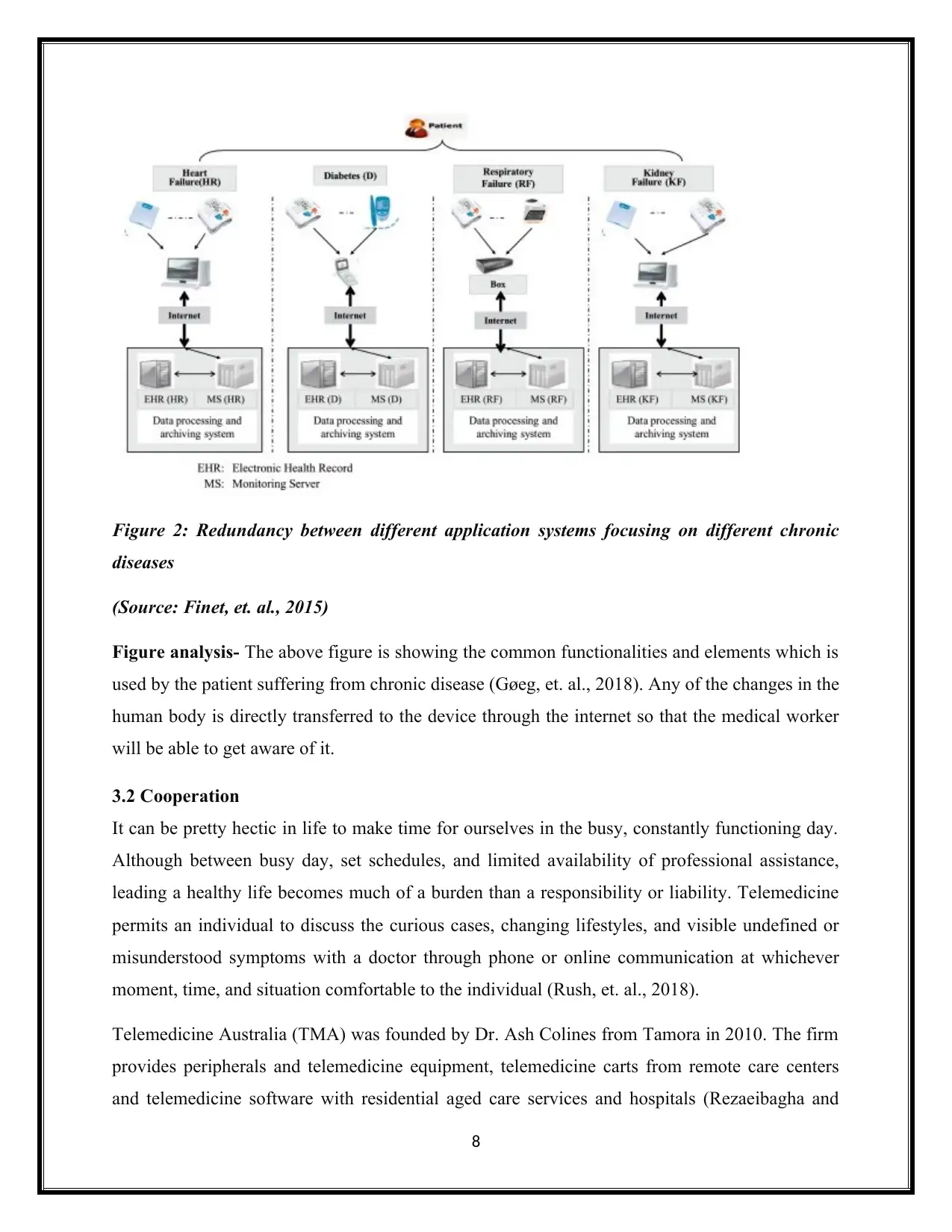
Figure 2: Redundancy between different application systems focusing on different chronic
diseases
(Source: Finet, et. al., 2015)
Figure analysis- The above figure is showing the common functionalities and elements which is
used by the patient suffering from chronic disease (Gøeg, et. al., 2018). Any of the changes in the
human body is directly transferred to the device through the internet so that the medical worker
will be able to get aware of it.
3.2 Cooperation
It can be pretty hectic in life to make time for ourselves in the busy, constantly functioning day.
Although between busy day, set schedules, and limited availability of professional assistance,
leading a healthy life becomes much of a burden than a responsibility or liability. Telemedicine
permits an individual to discuss the curious cases, changing lifestyles, and visible undefined or
misunderstood symptoms with a doctor through phone or online communication at whichever
moment, time, and situation comfortable to the individual (Rush, et. al., 2018).
Telemedicine Australia (TMA) was founded by Dr. Ash Colines from Tamora in 2010. The firm
provides peripherals and telemedicine equipment, telemedicine carts from remote care centers
and telemedicine software with residential aged care services and hospitals (Rezaeibagha and
8
diseases
(Source: Finet, et. al., 2015)
Figure analysis- The above figure is showing the common functionalities and elements which is
used by the patient suffering from chronic disease (Gøeg, et. al., 2018). Any of the changes in the
human body is directly transferred to the device through the internet so that the medical worker
will be able to get aware of it.
3.2 Cooperation
It can be pretty hectic in life to make time for ourselves in the busy, constantly functioning day.
Although between busy day, set schedules, and limited availability of professional assistance,
leading a healthy life becomes much of a burden than a responsibility or liability. Telemedicine
permits an individual to discuss the curious cases, changing lifestyles, and visible undefined or
misunderstood symptoms with a doctor through phone or online communication at whichever
moment, time, and situation comfortable to the individual (Rush, et. al., 2018).
Telemedicine Australia (TMA) was founded by Dr. Ash Colines from Tamora in 2010. The firm
provides peripherals and telemedicine equipment, telemedicine carts from remote care centers
and telemedicine software with residential aged care services and hospitals (Rezaeibagha and
8
Mu, 2018). The HQ of TMA has an active functioning training center that provides hands-on
telemedicine training sessions and experience with ways for trainees to join actual telemedicine
consultation during such training sessions. The clinic of TMA includes telemedicine consultation
for individuals habituating in Riverina area (Harting, et. al., 2018). On the basis of the latest
survey, the telemedicine clinic has crossed more than 800 telemed consultations regard people of
Temora, and the communities living around it.
3.3 Intervention
Telephone counseling
Telephone counselling is not one of the most admired methods of smoking cessation. Telephone
counselling has been one of the earliest interventions reviewed by Cochrane Collaboration.
Although the review concludes that telephone counselling does help smoke addicts who often
look for an escape or change to lead them out of the consistent lifestyle (Lesher and Shah, 2018).
Telephone ‘quitliness' refers to access support for smokers, the process of call-back counselling
which makes it even more useful. However, there are barricades on the number of a call made
and acceptable other than smoking cessation, to analyze and observe the benefits and outcomes
of the proactive telephonic counselling.
Forced spirometry
The issues that turn up with early diagnosis of CRD and management are seen in higher
prevalence, such as COPD (Chronic obstructive pulmonary Disease) and as well of Asthma.
For diagnosis and management of respiratory diseases, some forced spirometry is expected and
required. According to a survey conducted online that stated that there are about three main
functional web-based applications set up for primary care:
1. Educational material accessibility for CPD (Continued Professional Development)
2. Aid and support for experts conducted quality tests
3. Assistance for interpretation of lung function
Computed tomography and diagnostic support
A CT scan, a non invasive test which precisely is painless, is used to monitor chest radiography
to check respiratory issues and to identify the cause of change in lung function, the analyses and
9
telemedicine training sessions and experience with ways for trainees to join actual telemedicine
consultation during such training sessions. The clinic of TMA includes telemedicine consultation
for individuals habituating in Riverina area (Harting, et. al., 2018). On the basis of the latest
survey, the telemedicine clinic has crossed more than 800 telemed consultations regard people of
Temora, and the communities living around it.
3.3 Intervention
Telephone counseling
Telephone counselling is not one of the most admired methods of smoking cessation. Telephone
counselling has been one of the earliest interventions reviewed by Cochrane Collaboration.
Although the review concludes that telephone counselling does help smoke addicts who often
look for an escape or change to lead them out of the consistent lifestyle (Lesher and Shah, 2018).
Telephone ‘quitliness' refers to access support for smokers, the process of call-back counselling
which makes it even more useful. However, there are barricades on the number of a call made
and acceptable other than smoking cessation, to analyze and observe the benefits and outcomes
of the proactive telephonic counselling.
Forced spirometry
The issues that turn up with early diagnosis of CRD and management are seen in higher
prevalence, such as COPD (Chronic obstructive pulmonary Disease) and as well of Asthma.
For diagnosis and management of respiratory diseases, some forced spirometry is expected and
required. According to a survey conducted online that stated that there are about three main
functional web-based applications set up for primary care:
1. Educational material accessibility for CPD (Continued Professional Development)
2. Aid and support for experts conducted quality tests
3. Assistance for interpretation of lung function
Computed tomography and diagnostic support
A CT scan, a non invasive test which precisely is painless, is used to monitor chest radiography
to check respiratory issues and to identify the cause of change in lung function, the analyses and
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
deciphering of the symptoms visible in an individual, such as shot and quick breathing (Fortis, et.
al., 2018). The understanding and ability to analyze a CT scan requires the wide knowledge of
the subject, ability to understand the medical terminology, specialized training, the transferring
movement of CT images to one professional to the other. In order to study CT review on the
borderline three things are required:
1. CT Scan Machine
2. A functioning transmission network to send the file from one place to another
3. A high-quality system to observe the displayed image on its screen (Michel-Macarty, et.
al., 2018).
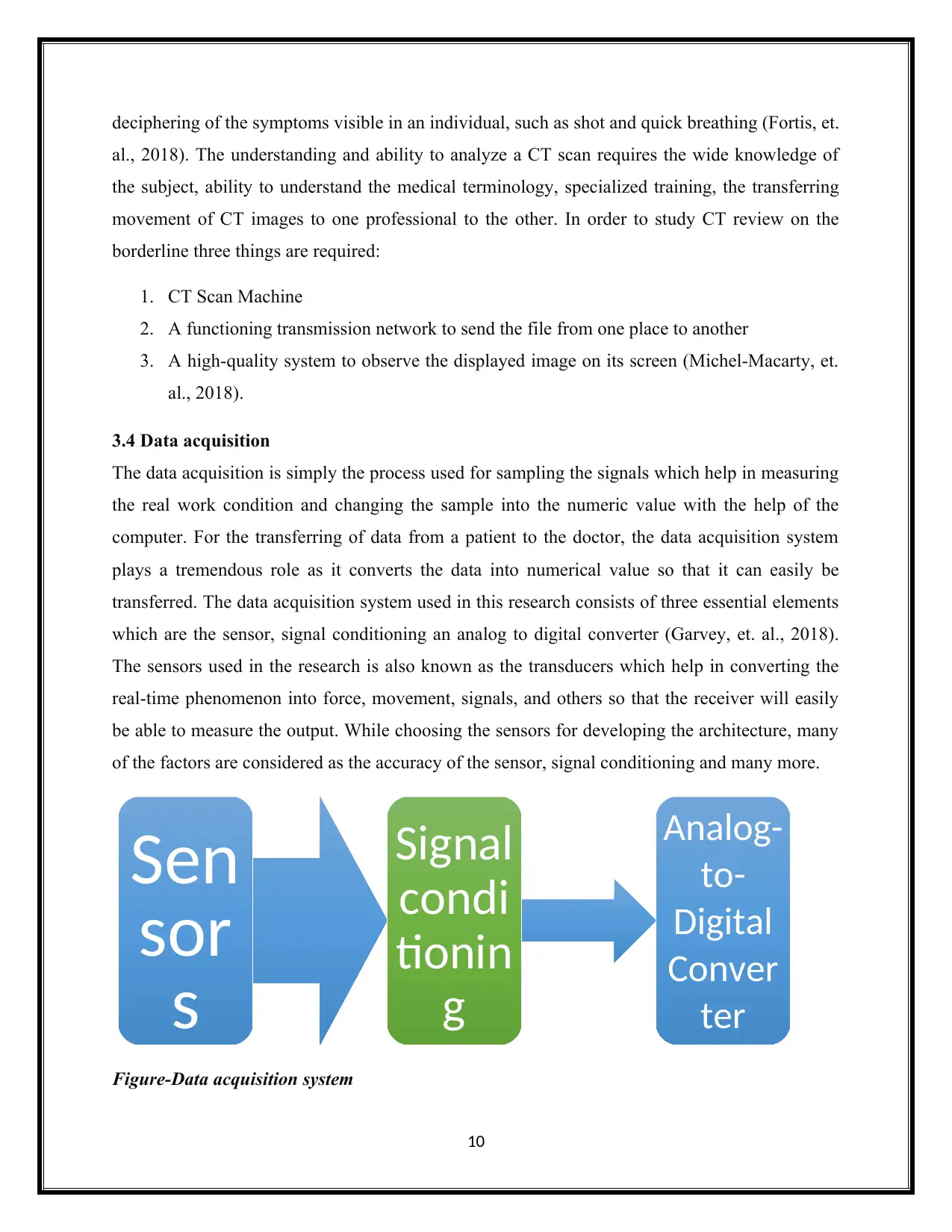
3.4 Data acquisition
The data acquisition is simply the process used for sampling the signals which help in measuring
the real work condition and changing the sample into the numeric value with the help of the
computer. For the transferring of data from a patient to the doctor, the data acquisition system
plays a tremendous role as it converts the data into numerical value so that it can easily be
transferred. The data acquisition system used in this research consists of three essential elements
which are the sensor, signal conditioning an analog to digital converter (Garvey, et. al., 2018).
The sensors used in the research is also known as the transducers which help in converting the
real-time phenomenon into force, movement, signals, and others so that the receiver will easily
be able to measure the output. While choosing the sensors for developing the architecture, many
of the factors are considered as the accuracy of the sensor, signal conditioning and many more.
Figure-Data acquisition system
10
Sen
sor
s
Signal
condi
tionin
g
Analog-
to-
Digital
Conver
ter
al., 2018). The understanding and ability to analyze a CT scan requires the wide knowledge of
the subject, ability to understand the medical terminology, specialized training, the transferring
movement of CT images to one professional to the other. In order to study CT review on the
borderline three things are required:
1. CT Scan Machine
2. A functioning transmission network to send the file from one place to another
3. A high-quality system to observe the displayed image on its screen (Michel-Macarty, et.
al., 2018).
3.4 Data acquisition
The data acquisition is simply the process used for sampling the signals which help in measuring
the real work condition and changing the sample into the numeric value with the help of the
computer. For the transferring of data from a patient to the doctor, the data acquisition system
plays a tremendous role as it converts the data into numerical value so that it can easily be
transferred. The data acquisition system used in this research consists of three essential elements
which are the sensor, signal conditioning an analog to digital converter (Garvey, et. al., 2018).
The sensors used in the research is also known as the transducers which help in converting the
real-time phenomenon into force, movement, signals, and others so that the receiver will easily
be able to measure the output. While choosing the sensors for developing the architecture, many
of the factors are considered as the accuracy of the sensor, signal conditioning and many more.
Figure-Data acquisition system
10
Sen
sor
s
Signal
condi
tionin
g
Analog-
to-
Digital
Conver
ter
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Signal conditioning is vital because it helps in making quality measurement over the signal. The
signal conditioning used in the research architecture includes the Wheatstone bridge completion
and cold junction compensation. While converting analog to digital, the chip takes data directly
from the environment and convert into the discrete level so that it can easily be interpreted. The
conversion is important because it helps in enabling the computer to store the signals for the
future work.
In general, the data acquisition system starts with the physical property which needs to be
measured as light intensity, gas pressure, and others. The sensor used in the system simply
changes the physical property into the electric signal so that it can easily be transferred to the
system. The signal conditioning is important because it helps in providing suitability to the
hardware which is being used in the system. Once the data is digitalized then it cannot be
encoded to correct the transmission error.
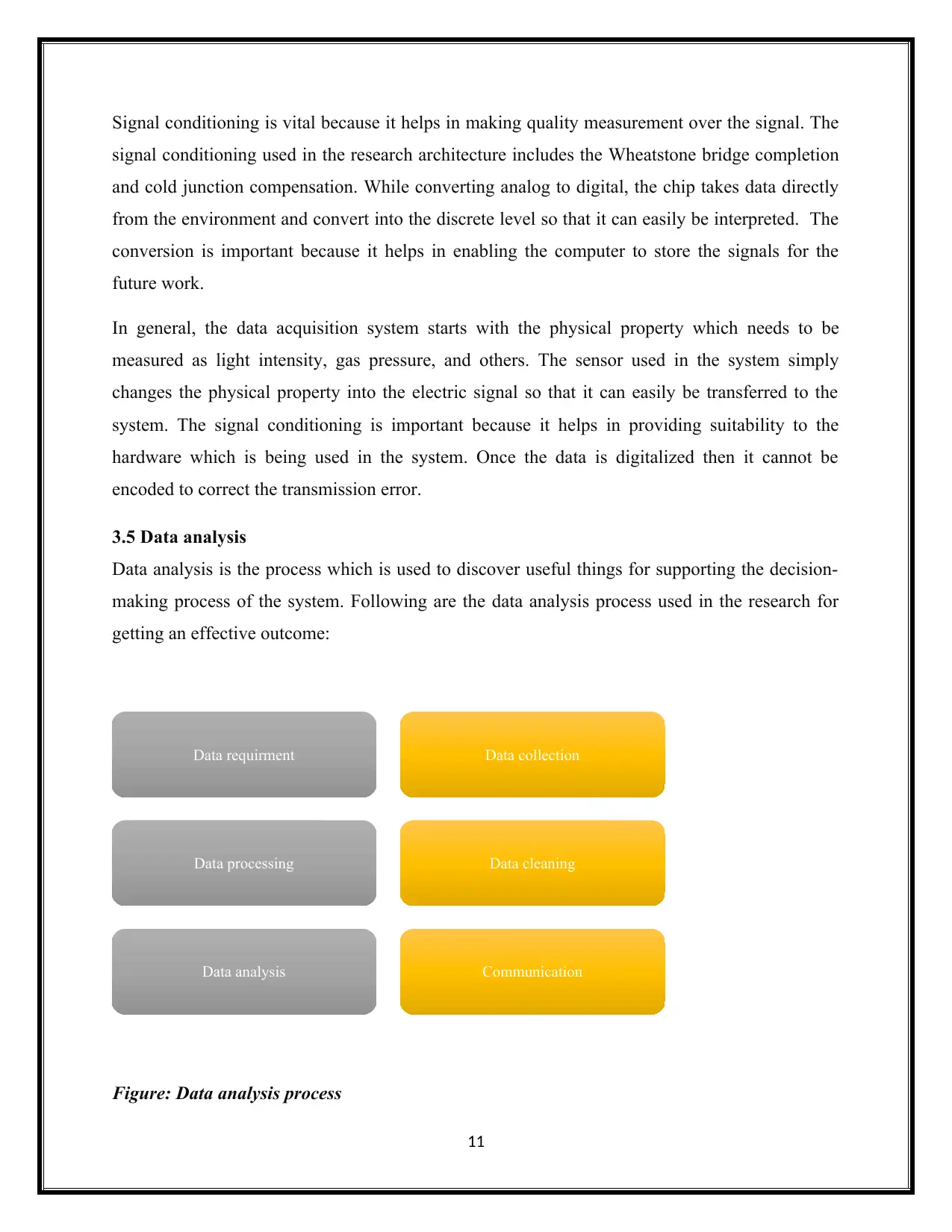
3.5 Data analysis
Data analysis is the process which is used to discover useful things for supporting the decision-
making process of the system. Following are the data analysis process used in the research for
getting an effective outcome:
Figure: Data analysis process
11
Data requirment Data collection
Data processing Data cleaning
Data analysis Communication
signal conditioning used in the research architecture includes the Wheatstone bridge completion
and cold junction compensation. While converting analog to digital, the chip takes data directly
from the environment and convert into the discrete level so that it can easily be interpreted. The
conversion is important because it helps in enabling the computer to store the signals for the
future work.
In general, the data acquisition system starts with the physical property which needs to be
measured as light intensity, gas pressure, and others. The sensor used in the system simply
changes the physical property into the electric signal so that it can easily be transferred to the
system. The signal conditioning is important because it helps in providing suitability to the
hardware which is being used in the system. Once the data is digitalized then it cannot be
encoded to correct the transmission error.
3.5 Data analysis
Data analysis is the process which is used to discover useful things for supporting the decision-
making process of the system. Following are the data analysis process used in the research for
getting an effective outcome:
Figure: Data analysis process
11
Data requirment Data collection
Data processing Data cleaning
Data analysis Communication
Figure analysis- in the above image, the data analysis process are discussed which are used in
the research project. The first step is linked to the specification of data requirement which is
done by secondary data collection. The data requirement analysis is made as per the issue rise in
the solution. In the second step, the required data and information are collected from books,
blogs, journals and others in a specified form (Peters and Weber, 2018). The data which are
collected through secondary data collection process will be processed and organized with the
help of relevant analysis tool. The error and issue in the solution will be cleaned for prevention
the issue which can be responsible in affecting the outcome of the research. The data which are
processed, organized and cleaned are ready for analysis. This helps in making an effective
decision regarding the outcome of the research. The result of the data analysis process will be
communicated to the end user of the system.
12
the research project. The first step is linked to the specification of data requirement which is
done by secondary data collection. The data requirement analysis is made as per the issue rise in
the solution. In the second step, the required data and information are collected from books,
blogs, journals and others in a specified form (Peters and Weber, 2018). The data which are
collected through secondary data collection process will be processed and organized with the
help of relevant analysis tool. The error and issue in the solution will be cleaned for prevention
the issue which can be responsible in affecting the outcome of the research. The data which are
processed, organized and cleaned are ready for analysis. This helps in making an effective
decision regarding the outcome of the research. The result of the data analysis process will be
communicated to the end user of the system.
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.