Research Proposal: Assessing Quality of Life in Hemodialysis Patients
VerifiedAdded on 2020/02/24
|49
|10503
|238
Report
AI Summary
This research proposal, titled "Assessment of factors affecting quality of life in hemodialysis patients in Saudi Arabia," aims to explore the multidimensional concept of Health-Related Quality of Life (HRQoL) as perceived by patients with end-stage renal failure undergoing hemodialysis. The study will define HRQoL, identify key domains (psychological, physical, environmental, and social), and investigate the influence of factors such as age, sex, education, income, disease duration, and treatment on patients' QoL. The research will address the question of how these factors, along with biological and socio-economic variables, impact QoL, with the goal of improving treatment and patient outcomes. The proposal includes a literature review, methodology, plan for data analysis, and discussion of probable findings, limitations, and potential implications for healthcare interventions. The study intends to contribute to the existing literature by providing a comprehensive understanding of the complex processes involved in HRQoL for hemodialysis patients.

Running head: QUALITY OF LIFE ASSESSMENT
Research Proposal- Assessment of factors affecting quality of life in hemodialysis
patients in Saudi Arabia
Name of the Student
Name of the University
Author Note
Research Proposal- Assessment of factors affecting quality of life in hemodialysis
patients in Saudi Arabia
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1QUALITY OF LIFE ASSESSMENT
Executive summary
The concept of quality of life (QoL) or health-related quality of life (HRQoL) is used as a patient
specific outcome measure in different healthcare settings. It has been measured and
conceptualised by using several validated instruments in the scientific community. However, in
most literature, the true meaning of this concept is still not clear. The aim of this research
proposal is to formulate a study that will explore the gap in present literature and will define the
concept of HRQoL, identify the key domains and eventually conceptualise it as perceived by
patients with end stage renal failure and those undergoing haemodialysis in a healthcare centre at
Saudi Arabia.
Executive summary
The concept of quality of life (QoL) or health-related quality of life (HRQoL) is used as a patient
specific outcome measure in different healthcare settings. It has been measured and
conceptualised by using several validated instruments in the scientific community. However, in
most literature, the true meaning of this concept is still not clear. The aim of this research
proposal is to formulate a study that will explore the gap in present literature and will define the
concept of HRQoL, identify the key domains and eventually conceptualise it as perceived by
patients with end stage renal failure and those undergoing haemodialysis in a healthcare centre at
Saudi Arabia.
2QUALITY OF LIFE ASSESSMENT
Table of Contents
Introduction..........................................................................................................................3
Literature review..................................................................................................................6
Methodology......................................................................................................................14
Plan for data analysis.........................................................................................................18
Probable findings...............................................................................................................19
Conclusions........................................................................................................................20
References..........................................................................................................................22
APPENDIX A....................................................................................................................28
APPENDIX B....................................................................................................................29
APPENDIX C....................................................................................................................30
APPENDIX D....................................................................................................................49
Table of Contents
Introduction..........................................................................................................................3
Literature review..................................................................................................................6
Methodology......................................................................................................................14
Plan for data analysis.........................................................................................................18
Probable findings...............................................................................................................19
Conclusions........................................................................................................................20
References..........................................................................................................................22
APPENDIX A....................................................................................................................28
APPENDIX B....................................................................................................................29
APPENDIX C....................................................................................................................30
APPENDIX D....................................................................................................................49
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3QUALITY OF LIFE ASSESSMENT
Introduction
The term quality of life (QoL) is a multidimensional concept that encompasses an array
of negative and positive indicators related to psychological, physical, environmental and social
domains (Fayers & Machin, 2013). Health related quality of life (HRQoL) assessment is not just
limited to the verification of the health status of any individual, it analyses the physical, social
and mental wellness and life satisfaction of the person as well. According to the The World
Health Organization Quality of Life Group, Quality of life is the perception of an individual of
positions in their life with respect to value and culture systems where they live and in accordance
to their expectations, goals, concerns and standards (Frisch, 2014). HRQoL is defined as the
functional consequence of a disease and its related therapy administered on the patient, as the
patient perceives. Over the last decade, research on quality of life has emerged as a valuable tool
to assess therapeutic intervention outcomes of several chronic diseases (Michalos, 2017).
End-stage renal failure/disease (ESRD) is one type of a chronic disease form of
irreversible decline in the functions of the kidneys, which require kidney transplantation or
dialysis to sustain our life (Coresh et al., 2014). The impacts of ESRD in human are severe. The
aggregate costs of dialysis, co-morbid conditions and recurrent hospitalizations overwhelm the
patients and affect their health plans. In 2011, the total Medicare cost for ESRD in 2011 was
$34.3 billion. PPPY health costs (per person per year) for patients on hemodialysis were $87,945
in the same year (Collins et al., 2015). The fifth stage of chronic kidney disease progression
manifests itself in the form of end stage renal disease. It is measured by the rate of glomerular
filtration (GFR).
Introduction
The term quality of life (QoL) is a multidimensional concept that encompasses an array
of negative and positive indicators related to psychological, physical, environmental and social
domains (Fayers & Machin, 2013). Health related quality of life (HRQoL) assessment is not just
limited to the verification of the health status of any individual, it analyses the physical, social
and mental wellness and life satisfaction of the person as well. According to the The World
Health Organization Quality of Life Group, Quality of life is the perception of an individual of
positions in their life with respect to value and culture systems where they live and in accordance
to their expectations, goals, concerns and standards (Frisch, 2014). HRQoL is defined as the
functional consequence of a disease and its related therapy administered on the patient, as the
patient perceives. Over the last decade, research on quality of life has emerged as a valuable tool
to assess therapeutic intervention outcomes of several chronic diseases (Michalos, 2017).
End-stage renal failure/disease (ESRD) is one type of a chronic disease form of
irreversible decline in the functions of the kidneys, which require kidney transplantation or
dialysis to sustain our life (Coresh et al., 2014). The impacts of ESRD in human are severe. The
aggregate costs of dialysis, co-morbid conditions and recurrent hospitalizations overwhelm the
patients and affect their health plans. In 2011, the total Medicare cost for ESRD in 2011 was
$34.3 billion. PPPY health costs (per person per year) for patients on hemodialysis were $87,945
in the same year (Collins et al., 2015). The fifth stage of chronic kidney disease progression
manifests itself in the form of end stage renal disease. It is measured by the rate of glomerular
filtration (GFR).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4QUALITY OF LIFE ASSESSMENT
Causes- Certain conditions or disease responsible for end stage renal disease are
hypertension, type 1 and type 2 diabetes, glomerulonephritis, polycystic kidneys, urinal tract
obstruction form kidney stones or enlarged prostate and interstitial nephritis.
Symptoms- The common symptoms observed as the disease progresses are vomiting,
nausea, loss of appetite, muscle twitch, swelling of ankles and feet, chest pain, hypoxia and
hypertension. Hemodialysis, peritoneal dialysis and kidney transplantation are the common
treatment methods.
ESRD patients are subjected to hemodialysis treatment that removes the salt, wastes and
extra water from their body to prevent waste accumulation in the blood (Robinson et al., 2014).
It also ensures a safe level of specific chemicals in the blood and regulates blood pressure. Renal
replacement therapy reduces symptom severity and increase survival rates of ESRD patients.
Hemodialysis is expensive, time intensive and restricts the amount of fluid and dietary intakes.
Prolonged therapy leads to dependence on healthcare givers, freedom loss and disruption of
social and family life. It also affects financial stability.
Objective- Frequent hospitalizations increase morbidity and mortality risks in patients
exacerbates social and emotional stress. This affects the patient HRQo (Kang et al., 2015)L.
Literature based evidence indicate association of low QoL scores with death in such patients.
HRQoL assessment will help in improving treatment and prognosis (Birren et al., 2014). The
main aim of this study is assessing QoL in hemodialysis patients with respect to their
psychological, physical, environmental and social health domains. Moreover, the study will
analyse effects of sex, age, education level, income, disease duration and treatment on the QoL
(Martinson et al., 2014).
Causes- Certain conditions or disease responsible for end stage renal disease are
hypertension, type 1 and type 2 diabetes, glomerulonephritis, polycystic kidneys, urinal tract
obstruction form kidney stones or enlarged prostate and interstitial nephritis.
Symptoms- The common symptoms observed as the disease progresses are vomiting,
nausea, loss of appetite, muscle twitch, swelling of ankles and feet, chest pain, hypoxia and
hypertension. Hemodialysis, peritoneal dialysis and kidney transplantation are the common
treatment methods.
ESRD patients are subjected to hemodialysis treatment that removes the salt, wastes and
extra water from their body to prevent waste accumulation in the blood (Robinson et al., 2014).
It also ensures a safe level of specific chemicals in the blood and regulates blood pressure. Renal
replacement therapy reduces symptom severity and increase survival rates of ESRD patients.
Hemodialysis is expensive, time intensive and restricts the amount of fluid and dietary intakes.
Prolonged therapy leads to dependence on healthcare givers, freedom loss and disruption of
social and family life. It also affects financial stability.
Objective- Frequent hospitalizations increase morbidity and mortality risks in patients
exacerbates social and emotional stress. This affects the patient HRQo (Kang et al., 2015)L.
Literature based evidence indicate association of low QoL scores with death in such patients.
HRQoL assessment will help in improving treatment and prognosis (Birren et al., 2014). The
main aim of this study is assessing QoL in hemodialysis patients with respect to their
psychological, physical, environmental and social health domains. Moreover, the study will
analyse effects of sex, age, education level, income, disease duration and treatment on the QoL
(Martinson et al., 2014).
5QUALITY OF LIFE ASSESSMENT
Research question- Quality of life is an essential issue for healthcare providers. The
research questions for this proposal are: 1) “What is the quality of life of hemodialysis patients at
healthcare facility in Saudi Arabia?”, 2) “Do symptoms (dialysis, fatigue, anxiety, depression),
general health perception, functional status, individual characteristics (gender, age, race),
biological function (serum albumin and hemoglobin) and socio-economic factors, marital status
and treatment time affect the quality of life?” (Lowney et al., 2015) and 3) “When individual
characteristics and environmental characteristics are controlled, do biological factors affect the
overall quality of life?” Little research has been conducted on the broad spectrum of QoL in
patients with ESRD. This research proposal thus aims to explain how factors of satisfaction,
dissatisfaction, physical quality, duration of hemodialysis treatment, standard of living and
psychological aspects that are important to a person affect his perception on the quality of life
(Bayoumi et al., 2013). Independent variables such as gain in weight, urea reduction ratio, years
of dialysis treatment and levels of phosphorus, calcium, albumin, parathyroid hormone and
serum hemoglobin were considered. The dependent variables were kidney disease burden,
symptoms, problems and their effects on daily life of the patients. These variables have been
selected because previous studies have reported lack of theoretical framework in selecting the
variables for the assessment. This failed to establish the relationship between HRQoL and its
physical and psychological determinants.
Scope- The study will help in improving financial and social and support of ESRD
patients. It will provide interventions for promoting physical activity and coping with
psychological distress in the patient population. This might prove effective in eventually
enhancing their HRQoL. The findings from the study will add to the literature, the underlying
complex psychological and biological processes of HRQoL. It will take knowledge acquired
Research question- Quality of life is an essential issue for healthcare providers. The
research questions for this proposal are: 1) “What is the quality of life of hemodialysis patients at
healthcare facility in Saudi Arabia?”, 2) “Do symptoms (dialysis, fatigue, anxiety, depression),
general health perception, functional status, individual characteristics (gender, age, race),
biological function (serum albumin and hemoglobin) and socio-economic factors, marital status
and treatment time affect the quality of life?” (Lowney et al., 2015) and 3) “When individual
characteristics and environmental characteristics are controlled, do biological factors affect the
overall quality of life?” Little research has been conducted on the broad spectrum of QoL in
patients with ESRD. This research proposal thus aims to explain how factors of satisfaction,
dissatisfaction, physical quality, duration of hemodialysis treatment, standard of living and
psychological aspects that are important to a person affect his perception on the quality of life
(Bayoumi et al., 2013). Independent variables such as gain in weight, urea reduction ratio, years
of dialysis treatment and levels of phosphorus, calcium, albumin, parathyroid hormone and
serum hemoglobin were considered. The dependent variables were kidney disease burden,
symptoms, problems and their effects on daily life of the patients. These variables have been
selected because previous studies have reported lack of theoretical framework in selecting the
variables for the assessment. This failed to establish the relationship between HRQoL and its
physical and psychological determinants.
Scope- The study will help in improving financial and social and support of ESRD
patients. It will provide interventions for promoting physical activity and coping with
psychological distress in the patient population. This might prove effective in eventually
enhancing their HRQoL. The findings from the study will add to the literature, the underlying
complex psychological and biological processes of HRQoL. It will take knowledge acquired
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6QUALITY OF LIFE ASSESSMENT
through statistical analysis in HRQoL of hemodialysis patients to a theoretical level and will
provide insight for the development of appropriate and effective strategies to optimize their
quality of life.
Limitations- Limitations of this research proposal include small caregiver sample size,
lack of random sampling and low reliability of independent variables. Recruiting samples from a
single institution is another limitation. This will prohibit any form of generalization beyond the
sample for this study.
Literature review
Quality of life is a matter of utmost concern in clinical research based on evaluation. All
healthcare policies expect improvement in the quality of life as a desired outcome. Though,
health related quality of life is extensively used for research studies, the term has not been
conceptualized yet and this creates confusion among researchers. Several studies developed
definitions for quality of life. However, these lacked consensus (Anees et al., 2014). Some
studies focused on the concept of patient reported toxicity to define quality of life. Some global
definitions incorporate and encompass the ideas of patient happiness, unhappiness, satisfaction
and dissatisfaction. Quality of life is also defined as a feeling of satisfaction and wellbeing that
indicates the way a patient perceives his life to be. Quality of life makes life worthwhile. Other
studies state that the value and meaning of life are expressed in terms of an individual’s view of
quality of life (Vasilopoulou et al., 2016). However, these definitions fail to provide information
on the components related to quality of life; therefore make it difficult for researchers to
operationalize. The ambiguous definitions can be made research specific if they focus on the
concept of QoL related to research area of interest. Multidimensional concepts that consist of
through statistical analysis in HRQoL of hemodialysis patients to a theoretical level and will
provide insight for the development of appropriate and effective strategies to optimize their
quality of life.
Limitations- Limitations of this research proposal include small caregiver sample size,
lack of random sampling and low reliability of independent variables. Recruiting samples from a
single institution is another limitation. This will prohibit any form of generalization beyond the
sample for this study.
Literature review
Quality of life is a matter of utmost concern in clinical research based on evaluation. All
healthcare policies expect improvement in the quality of life as a desired outcome. Though,
health related quality of life is extensively used for research studies, the term has not been
conceptualized yet and this creates confusion among researchers. Several studies developed
definitions for quality of life. However, these lacked consensus (Anees et al., 2014). Some
studies focused on the concept of patient reported toxicity to define quality of life. Some global
definitions incorporate and encompass the ideas of patient happiness, unhappiness, satisfaction
and dissatisfaction. Quality of life is also defined as a feeling of satisfaction and wellbeing that
indicates the way a patient perceives his life to be. Quality of life makes life worthwhile. Other
studies state that the value and meaning of life are expressed in terms of an individual’s view of
quality of life (Vasilopoulou et al., 2016). However, these definitions fail to provide information
on the components related to quality of life; therefore make it difficult for researchers to
operationalize. The ambiguous definitions can be made research specific if they focus on the
concept of QoL related to research area of interest. Multidimensional concepts that consist of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7QUALITY OF LIFE ASSESSMENT
four life domains such as social and economic, health and functioning, family and psychological
or spiritual, wellbeing can help in defining HRQoL in a comprehensive way (Rostami et al.,
2013). These definitions are generally found in research articles that focus on the term “health
related quality of life”. Several studies compared the HRQoL in end stage renal failure in nurses,
patients, and physicians. These studies utilized tools to determine the quality of life only related
to health items (Borzou et al., 2016). Some instruments used to assess HRQoL emphasize on the
use of a single domain like emotional functioning. On the other hand, other studies consider all
components to be equally important in affecting health outcomes and therefore include a
combination of different factors or components.
Moreover, many authors utilized a combination of all the definitions (Lopes et al., 2014).
Some research studies revealed health related quality of life as an essential cultural concept.
They evaluated the differences in association between clinical compliance of the patient, rates of
patient survival, health outcomes and the life quality (Cukor et al., 2014). For the purpose of this
proposed study, review of the literature will focus specifically on health realted quality of life in
hemodialysis patients who have been admitted to healthcare centres or hospital. Health related
quality of life evaluation and determination can be attempted by researchers and clinicians either
by designing objective assessments for the patients which are generally undertaken by an
interviewer or by designing subjective assessments which are done by the patients themselves.
Both these assessment methods report different findings. A particular study used more than 250
patients as sample and had collected data based on a reliable questionnaire. The questions in the
survey were framed based on the clinical history of the patients and several social and
demographic factors (Ayoub & Hijjazi, 2013). The health status of the patients was determined
by using the EQ-5D-5L dimensions. The obtained results suggested that low rates of HRQoL
four life domains such as social and economic, health and functioning, family and psychological
or spiritual, wellbeing can help in defining HRQoL in a comprehensive way (Rostami et al.,
2013). These definitions are generally found in research articles that focus on the term “health
related quality of life”. Several studies compared the HRQoL in end stage renal failure in nurses,
patients, and physicians. These studies utilized tools to determine the quality of life only related
to health items (Borzou et al., 2016). Some instruments used to assess HRQoL emphasize on the
use of a single domain like emotional functioning. On the other hand, other studies consider all
components to be equally important in affecting health outcomes and therefore include a
combination of different factors or components.
Moreover, many authors utilized a combination of all the definitions (Lopes et al., 2014).
Some research studies revealed health related quality of life as an essential cultural concept.
They evaluated the differences in association between clinical compliance of the patient, rates of
patient survival, health outcomes and the life quality (Cukor et al., 2014). For the purpose of this
proposed study, review of the literature will focus specifically on health realted quality of life in
hemodialysis patients who have been admitted to healthcare centres or hospital. Health related
quality of life evaluation and determination can be attempted by researchers and clinicians either
by designing objective assessments for the patients which are generally undertaken by an
interviewer or by designing subjective assessments which are done by the patients themselves.
Both these assessment methods report different findings. A particular study used more than 250
patients as sample and had collected data based on a reliable questionnaire. The questions in the
survey were framed based on the clinical history of the patients and several social and
demographic factors (Ayoub & Hijjazi, 2013). The health status of the patients was determined
by using the EQ-5D-5L dimensions. The obtained results suggested that low rates of HRQoL
8QUALITY OF LIFE ASSESSMENT
were associated with higher medication and more severity of the chronic disease. One particular
study designed a comparative to study dialysis patients. The participants were allowed to
complete the SF-36 (36-Item Short Form Health Survey) and the QoL index dialysis tool. A
thorough comparative analysis of the results was done for both the tools by using descriptive
statistical methods.
Results of multiple linear regression analysis determined the effect of different variables
on QoL scores (Sa’ed et al., 2016). In a study results of multiple regression analysis revealed that
prevalence of a chronic illness created the strongest impact on the scores obtained from both the
tools. A thorough comparison between the variables that were statistically significant for both the
samples revealed some contradictory results on using the two tools (D’Onofrio et al., 2017). This
meant that, the two tools had measured QoL differently. The participants who had been suffering
from ongoing chronic illness showed lower QoL scores. This finding was also supported by
evidence from other international studies. It was also found that ethnicity showed statistically
significant difference in the total score of QoL index in UAE nationals. The chronic illness
variables had a statistically significant implication on the total scores. In some studies age failed
to show statistically significant correlation with SF-36 scores.
Advanced age has also been linked with deterioration in physical activity. This resulted in
lower SF-36 scores in hemodialysis patients. In contrast, some study also reported that old
patients undergoing hemodialysis were more satisfied with their life. Older patients had accepted
their limitations better on comparison with younger patients. However, another study showed
absence of statistically significant age correlation with QoL index total scores. It had used the
same tool, but results depicted that with increase in age, some QoL index scores increased. This
suggested that chronically ill older patients had a tendency to show greater contentment level
were associated with higher medication and more severity of the chronic disease. One particular
study designed a comparative to study dialysis patients. The participants were allowed to
complete the SF-36 (36-Item Short Form Health Survey) and the QoL index dialysis tool. A
thorough comparative analysis of the results was done for both the tools by using descriptive
statistical methods.
Results of multiple linear regression analysis determined the effect of different variables
on QoL scores (Sa’ed et al., 2016). In a study results of multiple regression analysis revealed that
prevalence of a chronic illness created the strongest impact on the scores obtained from both the
tools. A thorough comparison between the variables that were statistically significant for both the
samples revealed some contradictory results on using the two tools (D’Onofrio et al., 2017). This
meant that, the two tools had measured QoL differently. The participants who had been suffering
from ongoing chronic illness showed lower QoL scores. This finding was also supported by
evidence from other international studies. It was also found that ethnicity showed statistically
significant difference in the total score of QoL index in UAE nationals. The chronic illness
variables had a statistically significant implication on the total scores. In some studies age failed
to show statistically significant correlation with SF-36 scores.
Advanced age has also been linked with deterioration in physical activity. This resulted in
lower SF-36 scores in hemodialysis patients. In contrast, some study also reported that old
patients undergoing hemodialysis were more satisfied with their life. Older patients had accepted
their limitations better on comparison with younger patients. However, another study showed
absence of statistically significant age correlation with QoL index total scores. It had used the
same tool, but results depicted that with increase in age, some QoL index scores increased. This
suggested that chronically ill older patients had a tendency to show greater contentment level
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9QUALITY OF LIFE ASSESSMENT
with respect to their health and social status (Brown et al., 2015). In some studies, iPTH was
found to be the only clinical parameter that correlated to a poor QoL (Villa-Bellosta et al., 2017).
Other parameters like phosphate levels or hemoglobin that are responsible for itching and fatigue
were not found to be associated with a poor QoL in some population.
To increase the statistical relevance, a larger population should always be assessed for
long term evaluation. Specific KDQoL-SF dimensions are associated with low mean scores of
PCS and MCS. MCS score were generally found to be higher than PCS. The difference between
the scores is generally small. In many studies, the average number of hemodialysis years is
small. It concludes reduction in MCS at the beginning of treatment. It gets subsequently
improved (Turkistani et al., 2014). According to multiple linear regression analysis results,
physical and mental health is improved when associated to normal iPTH values. The values are
linked with longer age of dialysis and living in a family. The fact that better QoL is linked with
longer dialysis age is surprising. Studies found that patients with ESRD in predialysis stage had a
poor QoL and suffered from impaired cognition than ESRD patients on regular dialysis. It has
been demonstrated that dialysis improves cognitive variables like attention, memory, information
processing and concentration. Furthermore, variables such as ethnicity and chronic health
problems were statistically significant determinants of QoL Index in people living in the UAE..
Conceptual framework- The framework used for this proposal will be loosely based on
Ferran’s model on quality of life. According to this model, several determinants are associated
with the quality of life of a particular person. The framework used for this study will deal with
the effects of health status, functioning status, social and economic status, family status and
psychological status to assess the health related quality of life in the respondents of the study. It
will evaluate concepts like, limitations in physical activities, limitations in social activities,
with respect to their health and social status (Brown et al., 2015). In some studies, iPTH was
found to be the only clinical parameter that correlated to a poor QoL (Villa-Bellosta et al., 2017).
Other parameters like phosphate levels or hemoglobin that are responsible for itching and fatigue
were not found to be associated with a poor QoL in some population.
To increase the statistical relevance, a larger population should always be assessed for
long term evaluation. Specific KDQoL-SF dimensions are associated with low mean scores of
PCS and MCS. MCS score were generally found to be higher than PCS. The difference between
the scores is generally small. In many studies, the average number of hemodialysis years is
small. It concludes reduction in MCS at the beginning of treatment. It gets subsequently
improved (Turkistani et al., 2014). According to multiple linear regression analysis results,
physical and mental health is improved when associated to normal iPTH values. The values are
linked with longer age of dialysis and living in a family. The fact that better QoL is linked with
longer dialysis age is surprising. Studies found that patients with ESRD in predialysis stage had a
poor QoL and suffered from impaired cognition than ESRD patients on regular dialysis. It has
been demonstrated that dialysis improves cognitive variables like attention, memory, information
processing and concentration. Furthermore, variables such as ethnicity and chronic health
problems were statistically significant determinants of QoL Index in people living in the UAE..
Conceptual framework- The framework used for this proposal will be loosely based on
Ferran’s model on quality of life. According to this model, several determinants are associated
with the quality of life of a particular person. The framework used for this study will deal with
the effects of health status, functioning status, social and economic status, family status and
psychological status to assess the health related quality of life in the respondents of the study. It
will evaluate concepts like, limitations in physical activities, limitations in social activities,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10QUALITY OF LIFE ASSESSMENT
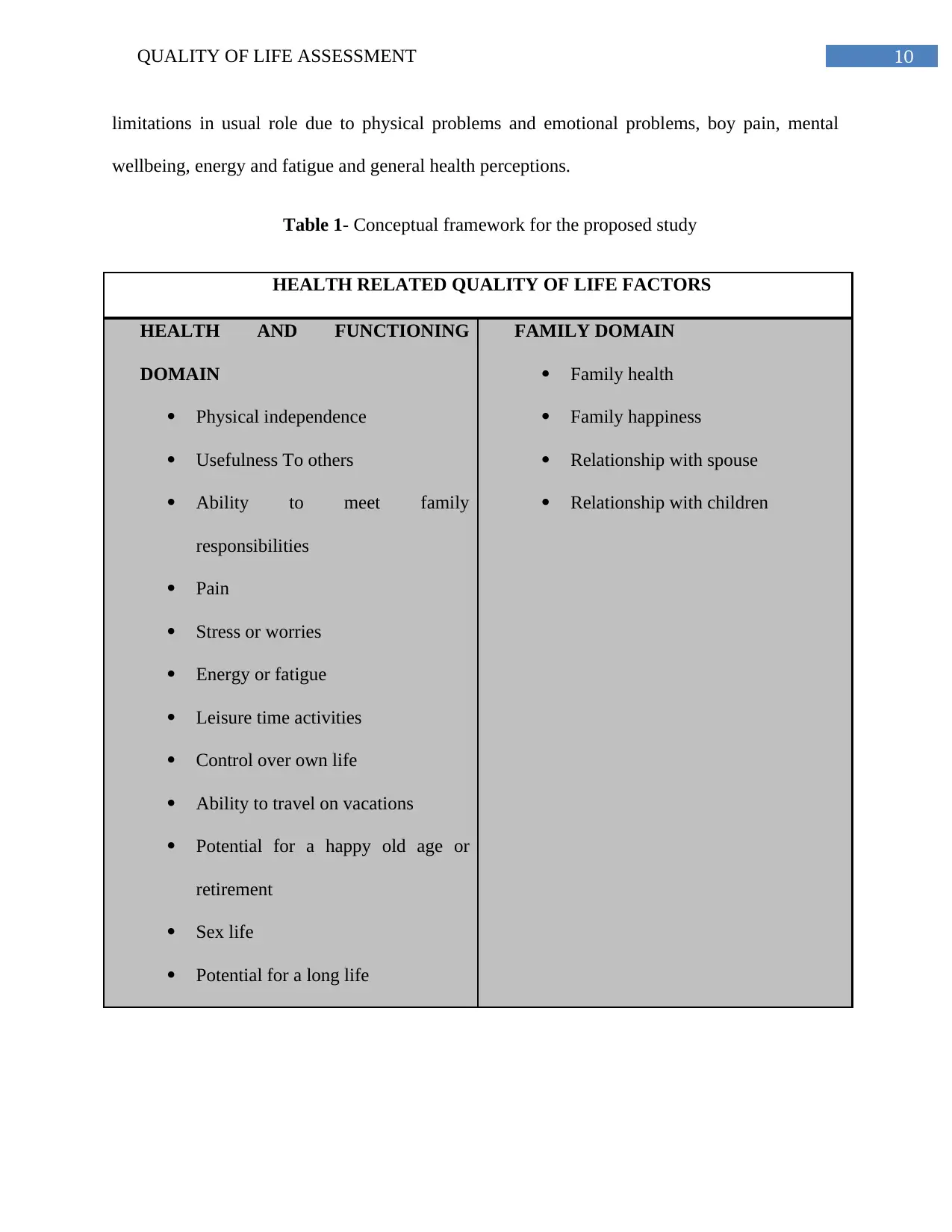
limitations in usual role due to physical problems and emotional problems, boy pain, mental
wellbeing, energy and fatigue and general health perceptions.
Table 1- Conceptual framework for the proposed study
HEALTH RELATED QUALITY OF LIFE FACTORS
HEALTH AND FUNCTIONING
DOMAIN
Physical independence
Usefulness To others
Ability to meet family
responsibilities
Pain
Stress or worries
Energy or fatigue
Leisure time activities
Control over own life
Ability to travel on vacations
Potential for a happy old age or
retirement
Sex life
Potential for a long life
FAMILY DOMAIN
Family health
Family happiness
Relationship with spouse
Relationship with children
limitations in usual role due to physical problems and emotional problems, boy pain, mental
wellbeing, energy and fatigue and general health perceptions.
Table 1- Conceptual framework for the proposed study
HEALTH RELATED QUALITY OF LIFE FACTORS
HEALTH AND FUNCTIONING
DOMAIN
Physical independence
Usefulness To others
Ability to meet family
responsibilities
Pain
Stress or worries
Energy or fatigue
Leisure time activities
Control over own life
Ability to travel on vacations
Potential for a happy old age or
retirement
Sex life
Potential for a long life
FAMILY DOMAIN
Family health
Family happiness
Relationship with spouse
Relationship with children
11QUALITY OF LIFE ASSESSMENT
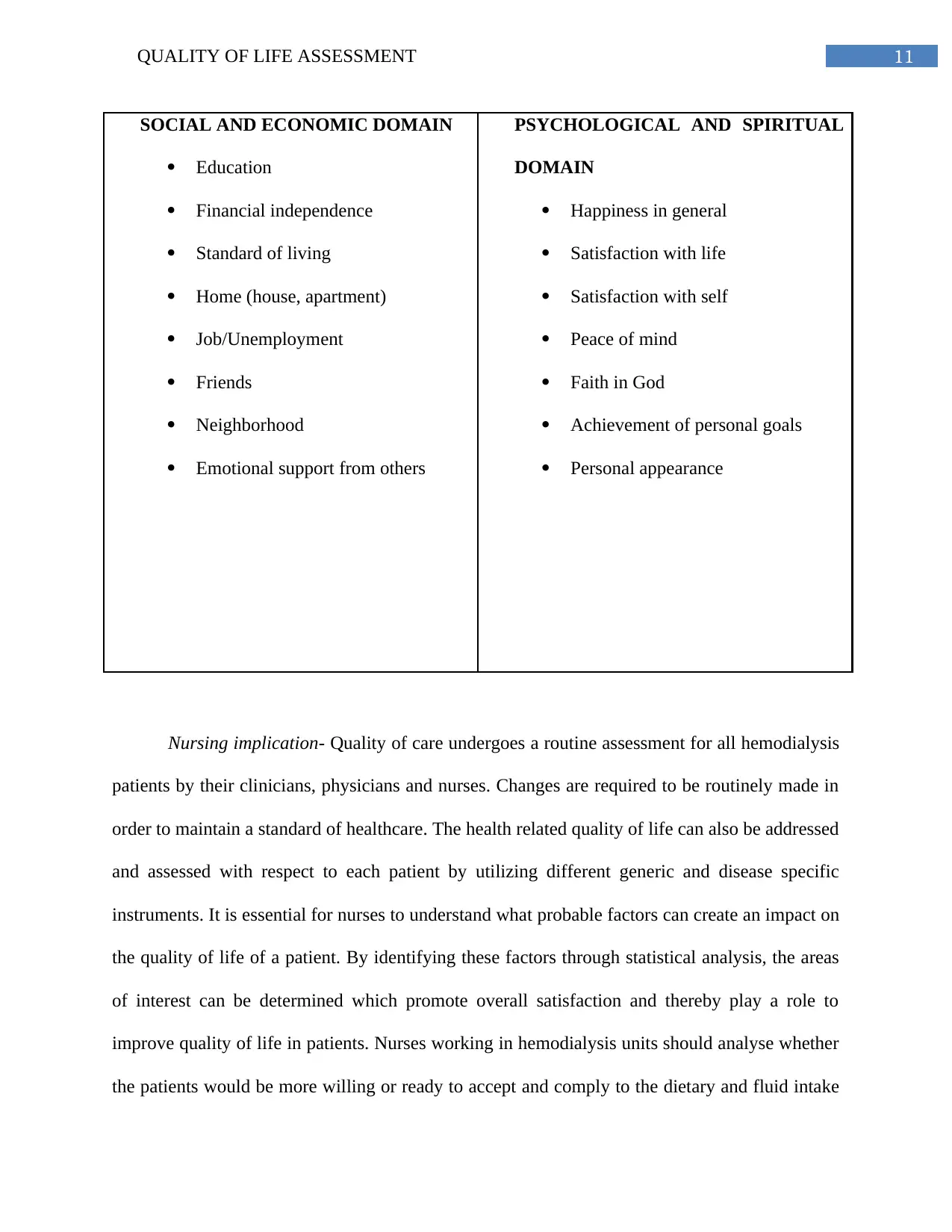
SOCIAL AND ECONOMIC DOMAIN
Education
Financial independence
Standard of living
Home (house, apartment)
Job/Unemployment
Friends
Neighborhood
Emotional support from others
PSYCHOLOGICAL AND SPIRITUAL
DOMAIN
Happiness in general
Satisfaction with life
Satisfaction with self
Peace of mind
Faith in God
Achievement of personal goals
Personal appearance
Nursing implication- Quality of care undergoes a routine assessment for all hemodialysis
patients by their clinicians, physicians and nurses. Changes are required to be routinely made in
order to maintain a standard of healthcare. The health related quality of life can also be addressed
and assessed with respect to each patient by utilizing different generic and disease specific
instruments. It is essential for nurses to understand what probable factors can create an impact on
the quality of life of a patient. By identifying these factors through statistical analysis, the areas
of interest can be determined which promote overall satisfaction and thereby play a role to
improve quality of life in patients. Nurses working in hemodialysis units should analyse whether
the patients would be more willing or ready to accept and comply to the dietary and fluid intake
SOCIAL AND ECONOMIC DOMAIN
Education
Financial independence
Standard of living
Home (house, apartment)
Job/Unemployment
Friends
Neighborhood
Emotional support from others
PSYCHOLOGICAL AND SPIRITUAL
DOMAIN
Happiness in general
Satisfaction with life
Satisfaction with self
Peace of mind
Faith in God
Achievement of personal goals
Personal appearance
Nursing implication- Quality of care undergoes a routine assessment for all hemodialysis
patients by their clinicians, physicians and nurses. Changes are required to be routinely made in
order to maintain a standard of healthcare. The health related quality of life can also be addressed
and assessed with respect to each patient by utilizing different generic and disease specific
instruments. It is essential for nurses to understand what probable factors can create an impact on
the quality of life of a patient. By identifying these factors through statistical analysis, the areas
of interest can be determined which promote overall satisfaction and thereby play a role to
improve quality of life in patients. Nurses working in hemodialysis units should analyse whether
the patients would be more willing or ready to accept and comply to the dietary and fluid intake
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 49
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.