(PDF) Toward health and wellbeing for indigenous Australians
VerifiedAdded on 2021/02/20
|13
|3190
|94
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Aboriginal Health
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

Contents
INTRODUCTION...........................................................................................................................1
MAIN BODY..................................................................................................................................1
Health inequalities and inequities in Australia............................................................................1
Health Outcomes.........................................................................................................................3
Social Disparities and its impact on Aboriginal people...............................................................4
Health Disparities that impact on Aboriginal community...........................................................5
Practices for improvement of health outcomes of aboriginal people..........................................8
REFERENCES................................................................................................................................9
INTRODUCTION...........................................................................................................................1
MAIN BODY..................................................................................................................................1
Health inequalities and inequities in Australia............................................................................1
Health Outcomes.........................................................................................................................3
Social Disparities and its impact on Aboriginal people...............................................................4
Health Disparities that impact on Aboriginal community...........................................................5
Practices for improvement of health outcomes of aboriginal people..........................................8
REFERENCES................................................................................................................................9

INTRODUCTION
Health is considered as an important factor for enhancing life expectancy, which includes
well-being of people at physical, social, mental, ecological and emotional way. In context with
Australia, health of population has improved markedly after 20th century, due to reducing
inequalities between indigenous and non-indigenous people (Reading and Greenwood, 2018).
Despite such improvements, at the beginning of the 21st century, Australia is characterised
mainly by significant health inequalities. It includes morbidity, risk factors, health behaviours
and accessibility of service, for people living at both remote and non-remote areas (Howse and
Dwyer, 2016). This report is going make an investigation on different aspects of health
inequalities, especially for aboriginal people in Australia. Health inequalities are hereby,
measured in terms of mortality, difference in health status, affordability and health issues, that
impact on this community. The reason behind choosing this community is social disparities or
socio-economic disadvantages faced by it, that highly affect their health. Furthermore,
recommendations for improving health and life-expectancy of aboriginal people is also given.
MAIN BODY
Health inequalities and inequities in Australia
Indigenous culture within Australia is considered as most complex and diverse, that
counted as one of the oldest living community in the world. The reason behind long time
survival of this community is ability for adapting and change with time. Aboriginal people not
only keep cultural heritage of them rich and alive, but also passes their knowledge, rituals,
traditions, arts and performances from one generation to other (Ivers and et. al., (2016). Having
spiritual belief on wellbeing, community members were hunter-gathers who searched for wild
animals and uncultivated plant. Along with this, traditional diet of these people includes richness
in carbohydrates, nutrients, proteins and low in fat and sugars. However, with development of
modernisation, diet of aboriginal communities is heavily westernised i.e. not tend to be high in
sugar and fat and lower in nutritional and carbohydrate value. As to improve well-being of this
community and overall health, a number of interventions have been taken by Australia
Government. But still, there exists a number of factors or social difference that creates
longstanding challenges (Hatala, Desjardins & Bombay, 2016). It includes uneven employment,
education, socio-economic disadvantages and poorer healthcare accessibility. Therefore, in order
1
Health is considered as an important factor for enhancing life expectancy, which includes
well-being of people at physical, social, mental, ecological and emotional way. In context with
Australia, health of population has improved markedly after 20th century, due to reducing
inequalities between indigenous and non-indigenous people (Reading and Greenwood, 2018).
Despite such improvements, at the beginning of the 21st century, Australia is characterised
mainly by significant health inequalities. It includes morbidity, risk factors, health behaviours
and accessibility of service, for people living at both remote and non-remote areas (Howse and
Dwyer, 2016). This report is going make an investigation on different aspects of health
inequalities, especially for aboriginal people in Australia. Health inequalities are hereby,
measured in terms of mortality, difference in health status, affordability and health issues, that
impact on this community. The reason behind choosing this community is social disparities or
socio-economic disadvantages faced by it, that highly affect their health. Furthermore,
recommendations for improving health and life-expectancy of aboriginal people is also given.
MAIN BODY
Health inequalities and inequities in Australia
Indigenous culture within Australia is considered as most complex and diverse, that
counted as one of the oldest living community in the world. The reason behind long time
survival of this community is ability for adapting and change with time. Aboriginal people not
only keep cultural heritage of them rich and alive, but also passes their knowledge, rituals,
traditions, arts and performances from one generation to other (Ivers and et. al., (2016). Having
spiritual belief on wellbeing, community members were hunter-gathers who searched for wild
animals and uncultivated plant. Along with this, traditional diet of these people includes richness
in carbohydrates, nutrients, proteins and low in fat and sugars. However, with development of
modernisation, diet of aboriginal communities is heavily westernised i.e. not tend to be high in
sugar and fat and lower in nutritional and carbohydrate value. As to improve well-being of this
community and overall health, a number of interventions have been taken by Australia
Government. But still, there exists a number of factors or social difference that creates
longstanding challenges (Hatala, Desjardins & Bombay, 2016). It includes uneven employment,
education, socio-economic disadvantages and poorer healthcare accessibility. Therefore, in order
1
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
to cultivate an environment for improvement of health of original like, it is essential for
government and public health organisations to provide opportunities for personal growth to
aboriginal people, which is crucial for an extended as well as blissful life. As per statistical data,
life expectancy of aboriginal people in Australia is calculated as approximate 69.1 years for male
as compared to non-indigenous population of male, having 79.9 years (Hatala, Desjardins &
Bombay, 2016). While life-expectancy of female aboriginals is 79.7 where a normal female lives
up to 83.1 years, where leading causes of death of indigenous communities is occurred due to
circulatory disease system, respiratory issues, diabetes and cancer. These inequalities show the
major difference among indigenous and non-indigenous communities, due to lack of accessibility
of health services.
In context with social disparities, there are several factors present that highly affect the
health of people (Howell and et. al., 2016). It includes surrounding environment where they live
like housing facilities, education, economic condition and income level etc. As per survey, it has
been identified that gap of homelessness between aboriginal and non-aboriginal is much high,
where aboriginal holds 14.7% as single person households and non-aboriginal as 24.7%, where
near about 79% of total population of this vulnerable communities live in rural areas (Australia’s
Welfare: in brief, 2017). So, accessibility of health services, educational and employment
facilities in these areas are much less, that highly affect health of aboriginal people. Similarly,
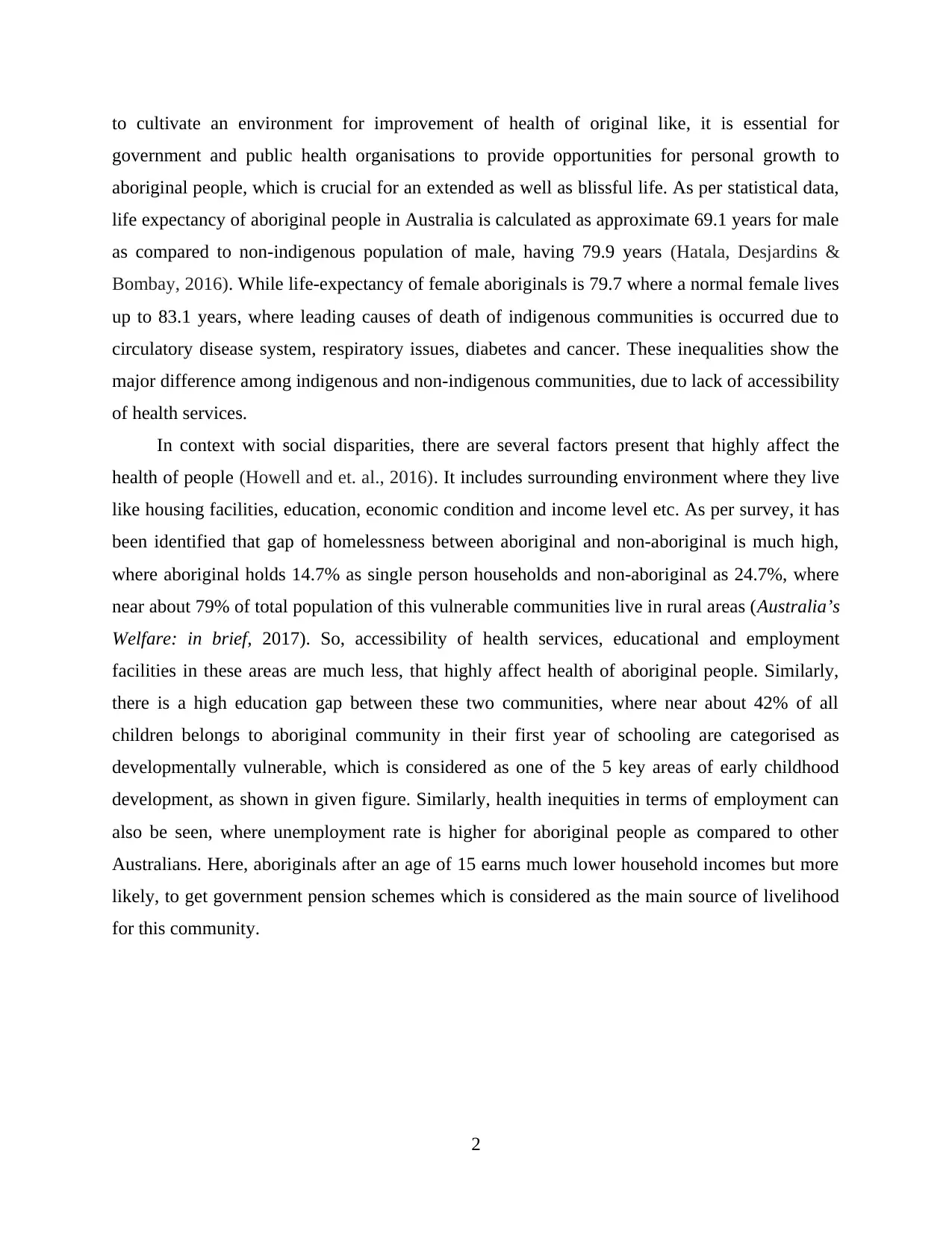
there is a high education gap between these two communities, where near about 42% of all
children belongs to aboriginal community in their first year of schooling are categorised as
developmentally vulnerable, which is considered as one of the 5 key areas of early childhood
development, as shown in given figure. Similarly, health inequities in terms of employment can
also be seen, where unemployment rate is higher for aboriginal people as compared to other
Australians. Here, aboriginals after an age of 15 earns much lower household incomes but more
likely, to get government pension schemes which is considered as the main source of livelihood
for this community.
2
government and public health organisations to provide opportunities for personal growth to
aboriginal people, which is crucial for an extended as well as blissful life. As per statistical data,
life expectancy of aboriginal people in Australia is calculated as approximate 69.1 years for male
as compared to non-indigenous population of male, having 79.9 years (Hatala, Desjardins &
Bombay, 2016). While life-expectancy of female aboriginals is 79.7 where a normal female lives
up to 83.1 years, where leading causes of death of indigenous communities is occurred due to
circulatory disease system, respiratory issues, diabetes and cancer. These inequalities show the
major difference among indigenous and non-indigenous communities, due to lack of accessibility
of health services.
In context with social disparities, there are several factors present that highly affect the
health of people (Howell and et. al., 2016). It includes surrounding environment where they live
like housing facilities, education, economic condition and income level etc. As per survey, it has
been identified that gap of homelessness between aboriginal and non-aboriginal is much high,
where aboriginal holds 14.7% as single person households and non-aboriginal as 24.7%, where
near about 79% of total population of this vulnerable communities live in rural areas (Australia’s
Welfare: in brief, 2017). So, accessibility of health services, educational and employment
facilities in these areas are much less, that highly affect health of aboriginal people. Similarly,
there is a high education gap between these two communities, where near about 42% of all
children belongs to aboriginal community in their first year of schooling are categorised as
developmentally vulnerable, which is considered as one of the 5 key areas of early childhood
development, as shown in given figure. Similarly, health inequities in terms of employment can
also be seen, where unemployment rate is higher for aboriginal people as compared to other
Australians. Here, aboriginals after an age of 15 earns much lower household incomes but more
likely, to get government pension schemes which is considered as the main source of livelihood
for this community.
2
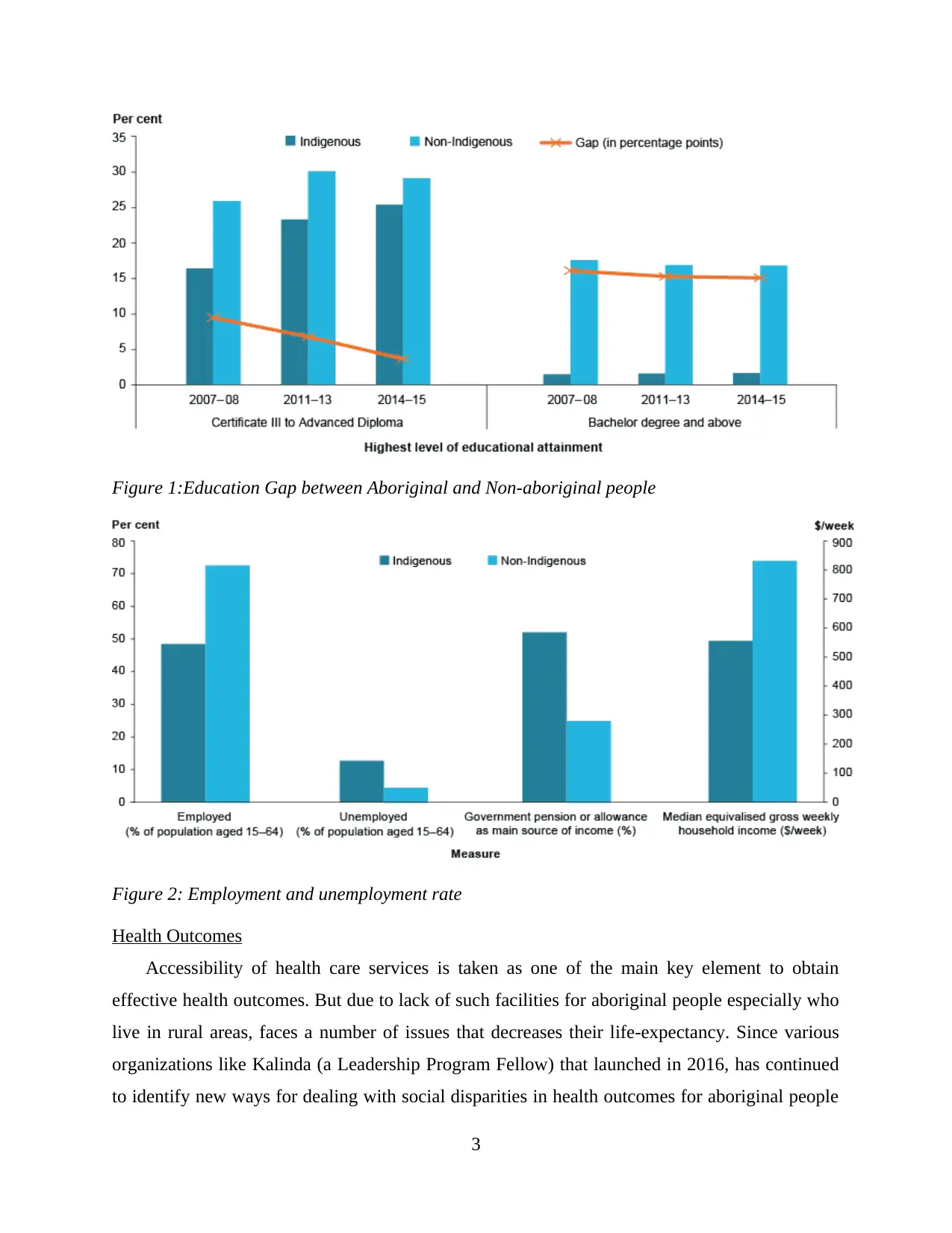
Figure 1:Education Gap between Aboriginal and Non-aboriginal people
Figure 2: Employment and unemployment rate
Health Outcomes
Accessibility of health care services is taken as one of the main key element to obtain
effective health outcomes. But due to lack of such facilities for aboriginal people especially who
live in rural areas, faces a number of issues that decreases their life-expectancy. Since various
organizations like Kalinda (a Leadership Program Fellow) that launched in 2016, has continued
to identify new ways for dealing with social disparities in health outcomes for aboriginal people
3
Figure 2: Employment and unemployment rate
Health Outcomes
Accessibility of health care services is taken as one of the main key element to obtain
effective health outcomes. But due to lack of such facilities for aboriginal people especially who
live in rural areas, faces a number of issues that decreases their life-expectancy. Since various
organizations like Kalinda (a Leadership Program Fellow) that launched in 2016, has continued
to identify new ways for dealing with social disparities in health outcomes for aboriginal people
3
of Australia. But there is not such improvements have been made yet. According to Melanie
Pescud and et.al. (2015), it has been analysed that disparities between Indigenous and non-
Indigenous populations’ health is one of the major issue that highly impacts on well-being of
people (Factors Influencing the Health Behaviour of Indigenous Australians: Perspectives from
Support People, 2015). Aboriginal people have shorter life-expectancy, where cardiovascular
disease is the major contributor of arising gap between positive health outcomes of indigenous
and non-indigenous communities, followed by mental issues, respiratory disease and diabetes.
Along with this, over 43.8% of aboriginal people are reported as chain smokers, as comparison
only 15.7% of non-indigenous are smokers (Anderson & Sanders, 2018). This vulnerable
community also engages in tobacco activities, drug and alcoholic addiction, that creates a large
gap with other communities in terms of health outcomes.
Social Disparities and its impact on Aboriginal people
So many elements are there such as biological factors, environmental elements, social
factors and behaviours which affect the life of aboriginal people. Social and cultural elements
consist economic development, education, homelessness, home ownership and various historical
elements such as discrimination and racism (Anderson & Brady, 2018). An investigation done in
2001 clear that average income for indigenous people in Australia is $364 per week while it is
$585 of non-indigenous people and the unemployment rate of aboriginal people was over 30%
which was three time more as compare to the non-indigenous of Australia. Ratio of indigenous
people was very less in almost every aspect and in education also. Due to poor education, the
capacity of these kind of individuals to access the health services and medicines was less. In
1989, indigenous people said that their overall status of health is directly linked with “control
over the physical environment of community, of dignity and of self-esteem”. Maintain the health
status of these kind of individuals is not the whole responsibility of doctors, medicines and
hospitals. Indigenous people expect development in social elements (Boyer, 2019). Due of lack
of effective medical te1ratment available for indigenous people there was high rate of mental
health problems among indigenous people further, hospitalisation rate of these were twice as
compare to non-indigenous people. Various elements are there that have negative impact on
health of indigenous people and this can be understood by following points:
4
Pescud and et.al. (2015), it has been analysed that disparities between Indigenous and non-
Indigenous populations’ health is one of the major issue that highly impacts on well-being of
people (Factors Influencing the Health Behaviour of Indigenous Australians: Perspectives from
Support People, 2015). Aboriginal people have shorter life-expectancy, where cardiovascular
disease is the major contributor of arising gap between positive health outcomes of indigenous
and non-indigenous communities, followed by mental issues, respiratory disease and diabetes.
Along with this, over 43.8% of aboriginal people are reported as chain smokers, as comparison
only 15.7% of non-indigenous are smokers (Anderson & Sanders, 2018). This vulnerable
community also engages in tobacco activities, drug and alcoholic addiction, that creates a large
gap with other communities in terms of health outcomes.
Social Disparities and its impact on Aboriginal people
So many elements are there such as biological factors, environmental elements, social
factors and behaviours which affect the life of aboriginal people. Social and cultural elements
consist economic development, education, homelessness, home ownership and various historical
elements such as discrimination and racism (Anderson & Brady, 2018). An investigation done in
2001 clear that average income for indigenous people in Australia is $364 per week while it is
$585 of non-indigenous people and the unemployment rate of aboriginal people was over 30%
which was three time more as compare to the non-indigenous of Australia. Ratio of indigenous
people was very less in almost every aspect and in education also. Due to poor education, the
capacity of these kind of individuals to access the health services and medicines was less. In
1989, indigenous people said that their overall status of health is directly linked with “control
over the physical environment of community, of dignity and of self-esteem”. Maintain the health
status of these kind of individuals is not the whole responsibility of doctors, medicines and
hospitals. Indigenous people expect development in social elements (Boyer, 2019). Due of lack
of effective medical te1ratment available for indigenous people there was high rate of mental
health problems among indigenous people further, hospitalisation rate of these were twice as
compare to non-indigenous people. Various elements are there that have negative impact on
health of indigenous people and this can be understood by following points:
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Racism: this is the element that affect both physical and mental health of an individual.
according to a survey, 21.5% indigenous children experienced racism in last 6 months. One of
the main reason of this was increased consumption of alcohol and smoking.
Children removed from their family: In an investigation, it was revealed that
approximate 38% respondents either removed them from their family or forcibly removed from
their natural family.
Other than this, various elements are there that affect the health of indigenous people of
Australia. It is very essential for Government to formulate an effective strategy in order to deal
with the gap between indigenous people and non-indigenous people (Lin, Green, & Bessarab,
2016). With help of this development of a better society and nation is possible. Government is
the one which can remove this gap and for this government can go for a partnership approach to
policy and a strength based approach could be used by government in order to deal with this gap.
Health Disparities that impact on Aboriginal community
Aboriginal health not only indicates the physical well-being of individuals within
Australia but it also tends towards cultural social and emotional state of whole community. It has
been determined from numerous facts and figures that Aboriginal and Torres strive to achieve
total well-being (Kotalik and Martin, 2016). In addition to this, it has been identified from
Indigenous Australian health and wellbeing statistics that there are very much less healthy
individuals in rest of Australian community. Major cause of hospital admissions of Aboriginal
individual is for kidney dialysis treatment, mental health problems, respiratory diseases, diabetes
cardiovascular, diseases and chronic kidney diseases. It has been seen that life expectancy of
Aboriginal within Australia is very less as they deprived from various Access for Healthcare
services which is essential to improve their life expectancy and health (Schembri and et. al.,
2016).
5
according to a survey, 21.5% indigenous children experienced racism in last 6 months. One of
the main reason of this was increased consumption of alcohol and smoking.
Children removed from their family: In an investigation, it was revealed that
approximate 38% respondents either removed them from their family or forcibly removed from
their natural family.
Other than this, various elements are there that affect the health of indigenous people of
Australia. It is very essential for Government to formulate an effective strategy in order to deal
with the gap between indigenous people and non-indigenous people (Lin, Green, & Bessarab,
2016). With help of this development of a better society and nation is possible. Government is
the one which can remove this gap and for this government can go for a partnership approach to
policy and a strength based approach could be used by government in order to deal with this gap.
Health Disparities that impact on Aboriginal community
Aboriginal health not only indicates the physical well-being of individuals within
Australia but it also tends towards cultural social and emotional state of whole community. It has
been determined from numerous facts and figures that Aboriginal and Torres strive to achieve
total well-being (Kotalik and Martin, 2016). In addition to this, it has been identified from
Indigenous Australian health and wellbeing statistics that there are very much less healthy
individuals in rest of Australian community. Major cause of hospital admissions of Aboriginal
individual is for kidney dialysis treatment, mental health problems, respiratory diseases, diabetes
cardiovascular, diseases and chronic kidney diseases. It has been seen that life expectancy of
Aboriginal within Australia is very less as they deprived from various Access for Healthcare
services which is essential to improve their life expectancy and health (Schembri and et. al.,
2016).
5
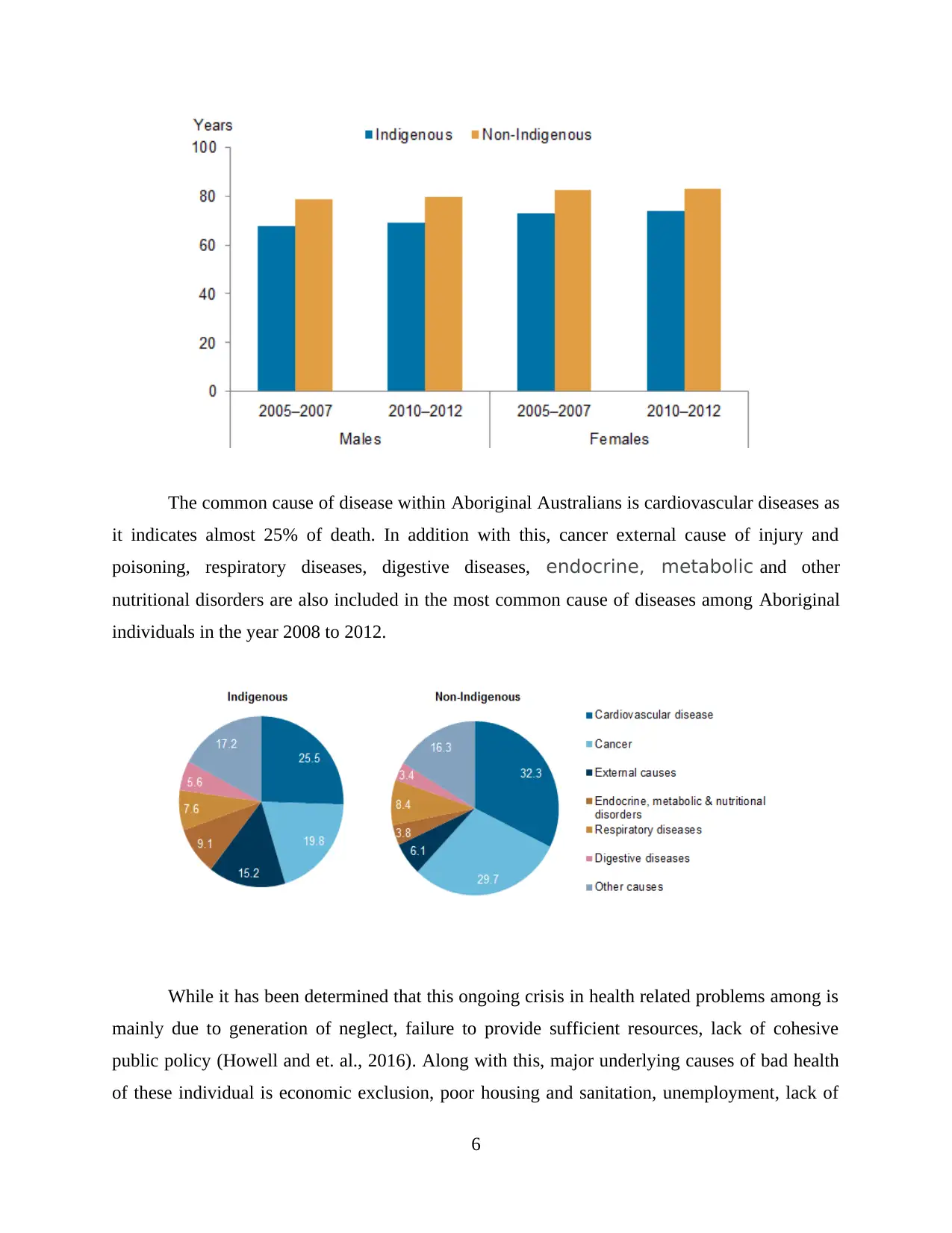
The common cause of disease within Aboriginal Australians is cardiovascular diseases as
it indicates almost 25% of death. In addition with this, cancer external cause of injury and
poisoning, respiratory diseases, digestive diseases, endocrine, metabolic and other
nutritional disorders are also included in the most common cause of diseases among Aboriginal
individuals in the year 2008 to 2012.
While it has been determined that this ongoing crisis in health related problems among is
mainly due to generation of neglect, failure to provide sufficient resources, lack of cohesive
public policy (Howell and et. al., 2016). Along with this, major underlying causes of bad health
of these individual is economic exclusion, poor housing and sanitation, unemployment, lack of
6
it indicates almost 25% of death. In addition with this, cancer external cause of injury and
poisoning, respiratory diseases, digestive diseases, endocrine, metabolic and other
nutritional disorders are also included in the most common cause of diseases among Aboriginal
individuals in the year 2008 to 2012.
While it has been determined that this ongoing crisis in health related problems among is
mainly due to generation of neglect, failure to provide sufficient resources, lack of cohesive
public policy (Howell and et. al., 2016). Along with this, major underlying causes of bad health
of these individual is economic exclusion, poor housing and sanitation, unemployment, lack of
6

adequate nutrition, poor education and social exclusion. It has been determined that these
individual suffer from much more health then other Australians. As they have been neglected
from various health facilities further it has been that Aboriginal individuals have little power to
effectively influence these factors that further affect their health and life (Hatala, Desjardins &
Bombay, 2016). The shortfall in life expectancy of Aboriginal in Australia reflects that there is
ongoing impact of health related factors on their life and health that continues to be widen in past
many years. As per the report of Australian Medical Association it has been identified that
Aboriginal health mainly determines lack of commitment to equal need based findings, failure to
address environmental health and housing and gaps in Primary Health Care coverage. In addition
to this, it has been identified that, improving the health status of Aboriginal individuals with
Australia is longstanding challenge for Australian government as the gap among health status
between non Aboriginal and aboriginals keeps on widening (Hatala, Desjardins and Bombay,
2016). It has been identified that the most important determinant factors that affect Aboriginal
and Torres health is inequalities in equal access to Primary Health Care along with low level
standard of health infrastructure among Aboriginal community these standards include healthy
housing, sanitation, food etc as compared to other Australians. It has also been identified that
there is lack of sexual health clinics in regional and rural areas along with this no after clinic
services delivers to these individuals at proper time. All these facts act as an major element that
affect health and further lower down the life expectancy of Aboriginal Australians.
7
individual suffer from much more health then other Australians. As they have been neglected
from various health facilities further it has been that Aboriginal individuals have little power to
effectively influence these factors that further affect their health and life (Hatala, Desjardins &
Bombay, 2016). The shortfall in life expectancy of Aboriginal in Australia reflects that there is
ongoing impact of health related factors on their life and health that continues to be widen in past
many years. As per the report of Australian Medical Association it has been identified that
Aboriginal health mainly determines lack of commitment to equal need based findings, failure to
address environmental health and housing and gaps in Primary Health Care coverage. In addition
to this, it has been identified that, improving the health status of Aboriginal individuals with
Australia is longstanding challenge for Australian government as the gap among health status
between non Aboriginal and aboriginals keeps on widening (Hatala, Desjardins and Bombay,
2016). It has been identified that the most important determinant factors that affect Aboriginal
and Torres health is inequalities in equal access to Primary Health Care along with low level
standard of health infrastructure among Aboriginal community these standards include healthy
housing, sanitation, food etc as compared to other Australians. It has also been identified that
there is lack of sexual health clinics in regional and rural areas along with this no after clinic
services delivers to these individuals at proper time. All these facts act as an major element that
affect health and further lower down the life expectancy of Aboriginal Australians.
7
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Thus, it has been determined from the above discussion that aboriginal individual do not
have equal opportunity to be as healthy as compared to aboriginal Australians. While there is
little progress to lower down this inequality gap among from past decades. These inequalities
among health status that has been experienced by these emotional individual is mainly related to
systematic discrimination, as they do not have same opportunities as compared to other normal
Australians (Ivers and et. al., (2016).. Further it has been identified that these inequalities
simultaneously lead towards increase in cervical cancer and other sexual related problems among
these individual that further decrease their life expectancy. It has been identified that chronic
disease is one of the major cause of potential avoidable that factor among Aboriginal individuals
in Western Australia. These diseases include kidney diseases, respiratory diseases, high blood
pleasure cancer heart and circulatory diseases.
Practices for improvement of health outcomes of aboriginal people
The current study has highlighted the complexities as well as challenges that are created due to
large difference in life-expectancy and health outcomes of Indigenous and non-Indigenous
communities. This dynamic is confounded due to discrimination, racism, lower income sources,
inaccessibility of health services and education etc. Therefore, it shows the necessity for
coalition driven efforts within Indigenous community to improve their health behaviour, that
helps in reducing inequities, inequalities and empower the communities to enhance life-
expectancy (Howse and Dwyer, 2016). For this purpose, prevention of chronic or non-
communicable disease considers as the largest contributor for reducing health differences
between Indigenous and non-Indigenous Australians. Hereby, targeting the aboriginal people,
recommendation of best-practice preventive care in Australia is not consistently provided for this
community (Improving preventive health care in Aboriginal and Torres Strait Islander primary
care settings, 2017). However, significant improvement in delivery of health care services could
be achieved by identifying as well as minimising the evidence-practice gaps. This would assist to
utilize clinical audit data, for creation of a framework of strategies to address and support the
healthcare system to increase their accessibility in rural areas, particularly for aboriginal people.
8
have equal opportunity to be as healthy as compared to aboriginal Australians. While there is
little progress to lower down this inequality gap among from past decades. These inequalities
among health status that has been experienced by these emotional individual is mainly related to
systematic discrimination, as they do not have same opportunities as compared to other normal
Australians (Ivers and et. al., (2016).. Further it has been identified that these inequalities
simultaneously lead towards increase in cervical cancer and other sexual related problems among
these individual that further decrease their life expectancy. It has been identified that chronic
disease is one of the major cause of potential avoidable that factor among Aboriginal individuals
in Western Australia. These diseases include kidney diseases, respiratory diseases, high blood
pleasure cancer heart and circulatory diseases.
Practices for improvement of health outcomes of aboriginal people
The current study has highlighted the complexities as well as challenges that are created due to
large difference in life-expectancy and health outcomes of Indigenous and non-Indigenous
communities. This dynamic is confounded due to discrimination, racism, lower income sources,
inaccessibility of health services and education etc. Therefore, it shows the necessity for
coalition driven efforts within Indigenous community to improve their health behaviour, that
helps in reducing inequities, inequalities and empower the communities to enhance life-
expectancy (Howse and Dwyer, 2016). For this purpose, prevention of chronic or non-
communicable disease considers as the largest contributor for reducing health differences
between Indigenous and non-Indigenous Australians. Hereby, targeting the aboriginal people,
recommendation of best-practice preventive care in Australia is not consistently provided for this
community (Improving preventive health care in Aboriginal and Torres Strait Islander primary
care settings, 2017). However, significant improvement in delivery of health care services could
be achieved by identifying as well as minimising the evidence-practice gaps. This would assist to
utilize clinical audit data, for creation of a framework of strategies to address and support the
healthcare system to increase their accessibility in rural areas, particularly for aboriginal people.
8
REFERENCES
Books and Journals
Anderson, I., & Brady, M. (2018). Performance indicators for Aboriginal health services.
Anderson, I., & Sanders, W. (2018). Aboriginal health and institutional reform within Australian
federalism.
Boyer, Y. (2019). Moving Aboriginal health forward: Discarding Canada’s legal barriers.
Purich Publishing.
Hatala, A. R., Desjardins, M., & Bombay, A. (2016). Reframing narratives of aboriginal health
inequity: Exploring Cree elder resilience and well-being in contexts of historical
trauma. Qualitative health research. 26(14). 1911-1927.
Hatala, A. R., Desjardins, M., & Bombay, A. (2016). Reframing narratives of aboriginal health
inequity: Exploring Cree elder resilience and well-being in contexts of historical
trauma. Qualitative health research. 26(14). 1911-1927.
Howell, T., and et. al., (2016). Sharing our wisdom: a holistic aboriginal health
initiative. International Journal of Indigenous Health. 11(1). 111-132.
Howse, G., & Dwyer, J. (2016). Legally invisible: stewardship for Aboriginal and Torres Strait
Islander health. Australian and New Zealand journal of public health. 40(S1). S14-S20.
Ivers, R. Q., and et. al., (2016). Driver licensing: descriptive epidemiology of a social
determinant of Aboriginal and Torres Strait Islander health. Australian and New Zealand
journal of public health. 40(4). 377-382.
Kotalik, J., & Martin, G. (2016). Aboriginal health care and bioethics: A reflection on the
teaching of the Seven Grandfathers. The American Journal of Bioethics. 16(5). 38-43.
Lin, I., Green, C., & Bessarab, D. (2016). ‘Yarn with me’: applying clinical yarning to improve
clinician–patient communication in Aboriginal health care. Australian Journal of
Primary Health. 22(5). 377-382.
Reading, C., & Greenwood, M. (2018). Structural determinants of Aboriginal peoples’
health. Determinants of Indigenous Peoples' Health: Beyond the Social, 1.
Schembri, L., and et. al., (2016). The effect of nutrition education on nutrition‐related health
outcomes of Aboriginal and Torres Strait Islander people: a systematic review. Australian
and New Zealand journal of public health. 40(S1). S42-S47.
Online
Australia Health 2018: in brief. (2018). [Online] Available through:<
https://www.aihw.gov.au/reports/australias-health/australias-health-2018-in-brief/
contents/all-is-not-equal>.
Australia’s Welfare: in brief. (2017). [Online] Available through:<
https://www.aihw.gov.au/reports/australias-welfare/australias-welfare-2017-in-brief/
contents/indigenous-australians>.
Factors Influencing the Health Behaviour of Indigenous Australians: Perspectives from Support
People. (2015) [Online] Available through:< https://journals.plos.org/plosone/article?
id=10.1371/journal.pone.0142323 >.
Improving preventive health care in Aboriginal and Torres Strait Islander primary care settings.
(2017). [Online] Available through:<
https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992-017-0267-z).
9
Books and Journals
Anderson, I., & Brady, M. (2018). Performance indicators for Aboriginal health services.
Anderson, I., & Sanders, W. (2018). Aboriginal health and institutional reform within Australian
federalism.
Boyer, Y. (2019). Moving Aboriginal health forward: Discarding Canada’s legal barriers.
Purich Publishing.
Hatala, A. R., Desjardins, M., & Bombay, A. (2016). Reframing narratives of aboriginal health
inequity: Exploring Cree elder resilience and well-being in contexts of historical
trauma. Qualitative health research. 26(14). 1911-1927.
Hatala, A. R., Desjardins, M., & Bombay, A. (2016). Reframing narratives of aboriginal health
inequity: Exploring Cree elder resilience and well-being in contexts of historical
trauma. Qualitative health research. 26(14). 1911-1927.
Howell, T., and et. al., (2016). Sharing our wisdom: a holistic aboriginal health
initiative. International Journal of Indigenous Health. 11(1). 111-132.
Howse, G., & Dwyer, J. (2016). Legally invisible: stewardship for Aboriginal and Torres Strait
Islander health. Australian and New Zealand journal of public health. 40(S1). S14-S20.
Ivers, R. Q., and et. al., (2016). Driver licensing: descriptive epidemiology of a social
determinant of Aboriginal and Torres Strait Islander health. Australian and New Zealand
journal of public health. 40(4). 377-382.
Kotalik, J., & Martin, G. (2016). Aboriginal health care and bioethics: A reflection on the
teaching of the Seven Grandfathers. The American Journal of Bioethics. 16(5). 38-43.
Lin, I., Green, C., & Bessarab, D. (2016). ‘Yarn with me’: applying clinical yarning to improve
clinician–patient communication in Aboriginal health care. Australian Journal of
Primary Health. 22(5). 377-382.
Reading, C., & Greenwood, M. (2018). Structural determinants of Aboriginal peoples’
health. Determinants of Indigenous Peoples' Health: Beyond the Social, 1.
Schembri, L., and et. al., (2016). The effect of nutrition education on nutrition‐related health
outcomes of Aboriginal and Torres Strait Islander people: a systematic review. Australian
and New Zealand journal of public health. 40(S1). S42-S47.
Online
Australia Health 2018: in brief. (2018). [Online] Available through:<
https://www.aihw.gov.au/reports/australias-health/australias-health-2018-in-brief/
contents/all-is-not-equal>.
Australia’s Welfare: in brief. (2017). [Online] Available through:<
https://www.aihw.gov.au/reports/australias-welfare/australias-welfare-2017-in-brief/
contents/indigenous-australians>.
Factors Influencing the Health Behaviour of Indigenous Australians: Perspectives from Support
People. (2015) [Online] Available through:< https://journals.plos.org/plosone/article?
id=10.1371/journal.pone.0142323 >.
Improving preventive health care in Aboriginal and Torres Strait Islander primary care settings.
(2017). [Online] Available through:<
https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992-017-0267-z).
9

10
1 out of 13






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.