Understanding Depression/Overdose with Psychosis: A Case Study of Jenna Taylor, 18 years old
Added on 2023-04-22
11 Pages2782 Words142 Views
© 2016 Keith Rischer/www.KeithRN.com
Depression/Overdose with Psychosis
UNFOLDING Reasoning
Jenna Taylor, 18 years old
Primary Concept
Mood and Affect
Interrelated Concepts (In order of emphasis)
1. Safety
2. Psychosis
3. Clinical Judgment
4. Communication
5. Collaboration
Depression/Overdose with Psychosis
UNFOLDING Reasoning
Jenna Taylor, 18 years old
Primary Concept
Mood and Affect
Interrelated Concepts (In order of emphasis)
1. Safety
2. Psychosis
3. Clinical Judgment
4. Communication
5. Collaboration
© 2016 Keith Rischer/www.KeithRN.com
Depression/Overdose with Psychosis
PART 1:
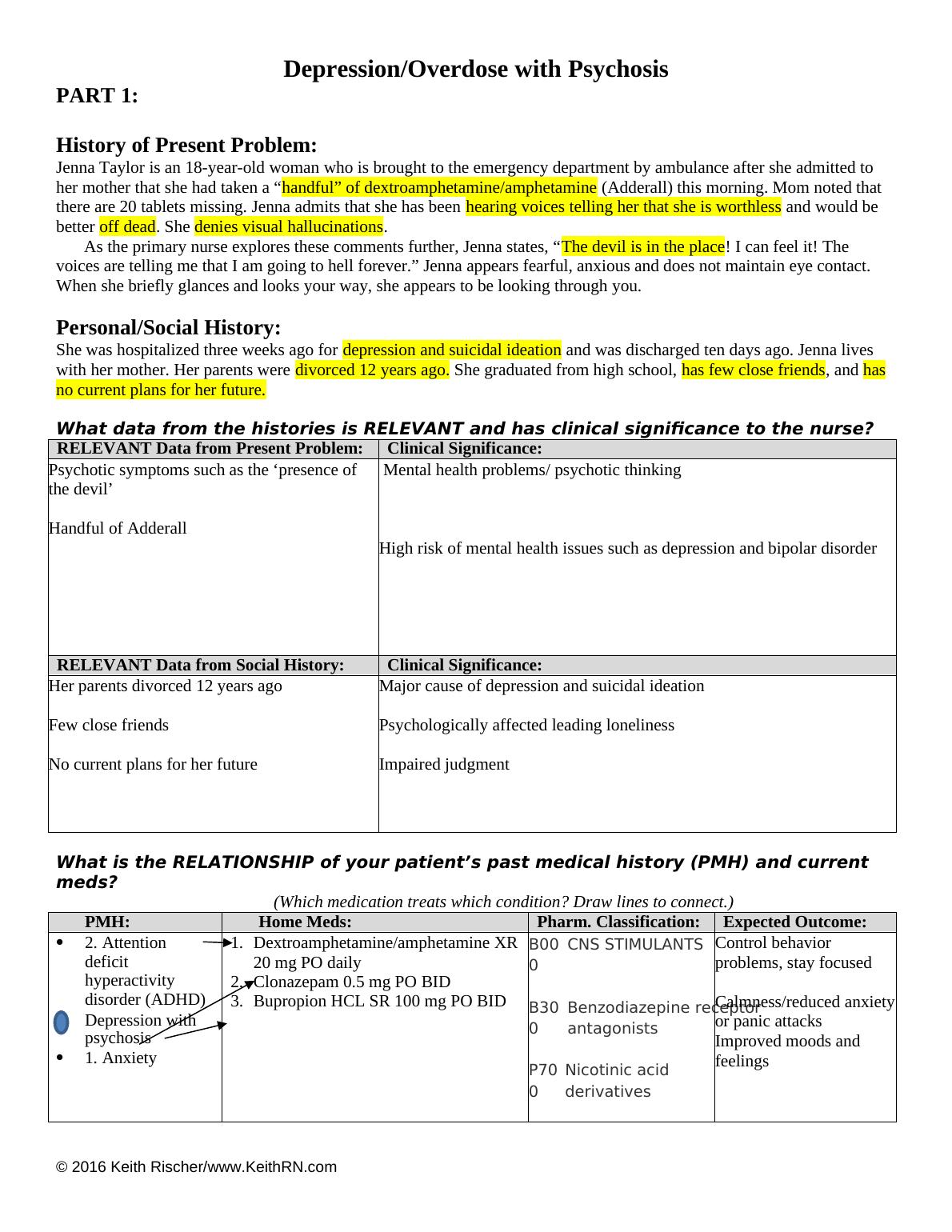
History of Present Problem:
Jenna Taylor is an 18-year-old woman who is brought to the emergency department by ambulance after she admitted to
her mother that she had taken a “handful” of dextroamphetamine/amphetamine (Adderall) this morning. Mom noted that
there are 20 tablets missing. Jenna admits that she has been hearing voices telling her that she is worthless and would be
better off dead. She denies visual hallucinations.
As the primary nurse explores these comments further, Jenna states, “The devil is in the place! I can feel it! The
voices are telling me that I am going to hell forever.” Jenna appears fearful, anxious and does not maintain eye contact.
When she briefly glances and looks your way, she appears to be looking through you.
Personal/Social History:
She was hospitalized three weeks ago for depression and suicidal ideation and was discharged ten days ago. Jenna lives
with her mother. Her parents were divorced 12 years ago. She graduated from high school, has few close friends, and has
no current plans for her future.
What data from the histories is RELEVANT and has clinical significance to the nurse?
RELEVANT Data from Present Problem: Clinical Significance:
Psychotic symptoms such as the ‘presence of
the devil’
Handful of Adderall
Mental health problems/ psychotic thinking
High risk of mental health issues such as depression and bipolar disorder
RELEVANT Data from Social History: Clinical Significance:
Her parents divorced 12 years ago
Few close friends
No current plans for her future
Major cause of depression and suicidal ideation
Psychologically affected leading loneliness
Impaired judgment
What is the RELATIONSHIP of your patient’s past medical history (PMH) and current
meds?
(Which medication treats which condition? Draw lines to connect.)
PMH: Home Meds: Pharm. Classification: Expected Outcome:
2. Attention
deficit
hyperactivity
disorder (ADHD)
Depression with
psychosis
1. Anxiety
1. Dextroamphetamine/amphetamine XR
20 mg PO daily
2. Clonazepam 0.5 mg PO BID
3. Bupropion HCL SR 100 mg PO BID
B00
0
CNS STIMULANTS
B30
0
Benzodiazepine receptor
antagonists
P70
0
Nicotinic acid
derivatives
Control behavior
problems, stay focused
Calmness/reduced anxiety
or panic attacks
Improved moods and
feelings
Depression/Overdose with Psychosis
PART 1:
History of Present Problem:
Jenna Taylor is an 18-year-old woman who is brought to the emergency department by ambulance after she admitted to
her mother that she had taken a “handful” of dextroamphetamine/amphetamine (Adderall) this morning. Mom noted that
there are 20 tablets missing. Jenna admits that she has been hearing voices telling her that she is worthless and would be
better off dead. She denies visual hallucinations.
As the primary nurse explores these comments further, Jenna states, “The devil is in the place! I can feel it! The
voices are telling me that I am going to hell forever.” Jenna appears fearful, anxious and does not maintain eye contact.
When she briefly glances and looks your way, she appears to be looking through you.
Personal/Social History:
She was hospitalized three weeks ago for depression and suicidal ideation and was discharged ten days ago. Jenna lives
with her mother. Her parents were divorced 12 years ago. She graduated from high school, has few close friends, and has
no current plans for her future.
What data from the histories is RELEVANT and has clinical significance to the nurse?
RELEVANT Data from Present Problem: Clinical Significance:
Psychotic symptoms such as the ‘presence of
the devil’
Handful of Adderall
Mental health problems/ psychotic thinking
High risk of mental health issues such as depression and bipolar disorder
RELEVANT Data from Social History: Clinical Significance:
Her parents divorced 12 years ago
Few close friends
No current plans for her future
Major cause of depression and suicidal ideation
Psychologically affected leading loneliness
Impaired judgment
What is the RELATIONSHIP of your patient’s past medical history (PMH) and current
meds?
(Which medication treats which condition? Draw lines to connect.)
PMH: Home Meds: Pharm. Classification: Expected Outcome:
2. Attention
deficit
hyperactivity
disorder (ADHD)
Depression with
psychosis
1. Anxiety
1. Dextroamphetamine/amphetamine XR
20 mg PO daily
2. Clonazepam 0.5 mg PO BID
3. Bupropion HCL SR 100 mg PO BID
B00
0
CNS STIMULANTS
B30
0
Benzodiazepine receptor
antagonists
P70
0
Nicotinic acid
derivatives
Control behavior
problems, stay focused
Calmness/reduced anxiety
or panic attacks
Improved moods and
feelings
© 2016 Keith Rischer/www.KeithRN.com
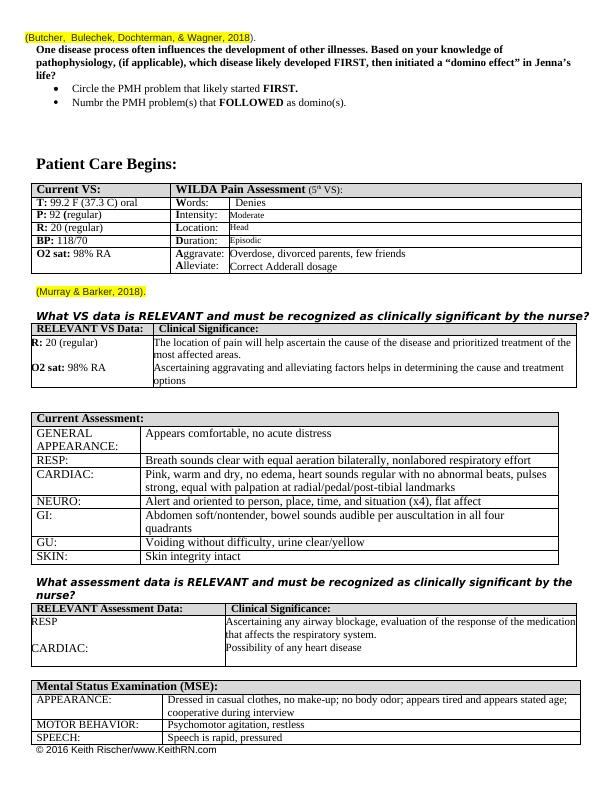
(Butcher, Bulechek, Dochterman, & Wagner, 2018).
One disease process often influences the development of other illnesses. Based on your knowledge of
pathophysiology, (if applicable), which disease likely developed FIRST, then initiated a “domino effect” in Jenna’s
life?
Circle the PMH problem that likely started FIRST.
Numbr the PMH problem(s) that FOLLOWED as domino(s).
Patient Care Begins:
Current VS: WILDA Pain Assessment (5th VS):
T: 99.2 F (37.3 C) oral Words: Denies
P: 92 (regular) Intensity: Moderate
R: 20 (regular) Location: Head
BP: 118/70 Duration: Episodic
O2 sat: 98% RA Aggravate:
Alleviate:
Overdose, divorced parents, few friends
Correct Adderall dosage
(Murray & Barker, 2018).
What VS data is RELEVANT and must be recognized as clinically significant by the nurse?
RELEVANT VS Data: Clinical Significance:
R: 20 (regular)
O2 sat: 98% RA
The location of pain will help ascertain the cause of the disease and prioritized treatment of the
most affected areas.
Ascertaining aggravating and alleviating factors helps in determining the cause and treatment
options
Current Assessment:
GENERAL
APPEARANCE:
Appears comfortable, no acute distress
RESP: Breath sounds clear with equal aeration bilaterally, nonlabored respiratory effort
CARDIAC: Pink, warm and dry, no edema, heart sounds regular with no abnormal beats, pulses
strong, equal with palpation at radial/pedal/post-tibial landmarks
NEURO: Alert and oriented to person, place, time, and situation (x4), flat affect
GI: Abdomen soft/nontender, bowel sounds audible per auscultation in all four
quadrants
GU: Voiding without difficulty, urine clear/yellow
SKIN: Skin integrity intact
What assessment data is RELEVANT and must be recognized as clinically significant by the
nurse?
RELEVANT Assessment Data: Clinical Significance:
RESP
CARDIAC:
Ascertaining any airway blockage, evaluation of the response of the medication
that affects the respiratory system.
Possibility of any heart disease
Mental Status Examination (MSE):
APPEARANCE: Dressed in casual clothes, no make-up; no body odor; appears tired and appears stated age;
cooperative during interview
MOTOR BEHAVIOR: Psychomotor agitation, restless
SPEECH: Speech is rapid, pressured
(Butcher, Bulechek, Dochterman, & Wagner, 2018).
One disease process often influences the development of other illnesses. Based on your knowledge of
pathophysiology, (if applicable), which disease likely developed FIRST, then initiated a “domino effect” in Jenna’s
life?
Circle the PMH problem that likely started FIRST.
Numbr the PMH problem(s) that FOLLOWED as domino(s).
Patient Care Begins:
Current VS: WILDA Pain Assessment (5th VS):
T: 99.2 F (37.3 C) oral Words: Denies
P: 92 (regular) Intensity: Moderate
R: 20 (regular) Location: Head
BP: 118/70 Duration: Episodic
O2 sat: 98% RA Aggravate:
Alleviate:
Overdose, divorced parents, few friends
Correct Adderall dosage
(Murray & Barker, 2018).
What VS data is RELEVANT and must be recognized as clinically significant by the nurse?
RELEVANT VS Data: Clinical Significance:
R: 20 (regular)
O2 sat: 98% RA
The location of pain will help ascertain the cause of the disease and prioritized treatment of the
most affected areas.
Ascertaining aggravating and alleviating factors helps in determining the cause and treatment
options
Current Assessment:
GENERAL
APPEARANCE:
Appears comfortable, no acute distress
RESP: Breath sounds clear with equal aeration bilaterally, nonlabored respiratory effort
CARDIAC: Pink, warm and dry, no edema, heart sounds regular with no abnormal beats, pulses
strong, equal with palpation at radial/pedal/post-tibial landmarks
NEURO: Alert and oriented to person, place, time, and situation (x4), flat affect
GI: Abdomen soft/nontender, bowel sounds audible per auscultation in all four
quadrants
GU: Voiding without difficulty, urine clear/yellow
SKIN: Skin integrity intact
What assessment data is RELEVANT and must be recognized as clinically significant by the
nurse?
RELEVANT Assessment Data: Clinical Significance:
RESP
CARDIAC:
Ascertaining any airway blockage, evaluation of the response of the medication
that affects the respiratory system.
Possibility of any heart disease
Mental Status Examination (MSE):
APPEARANCE: Dressed in casual clothes, no make-up; no body odor; appears tired and appears stated age;
cooperative during interview
MOTOR BEHAVIOR: Psychomotor agitation, restless
SPEECH: Speech is rapid, pressured
© 2016 Keith Rischer/www.KeithRN.com
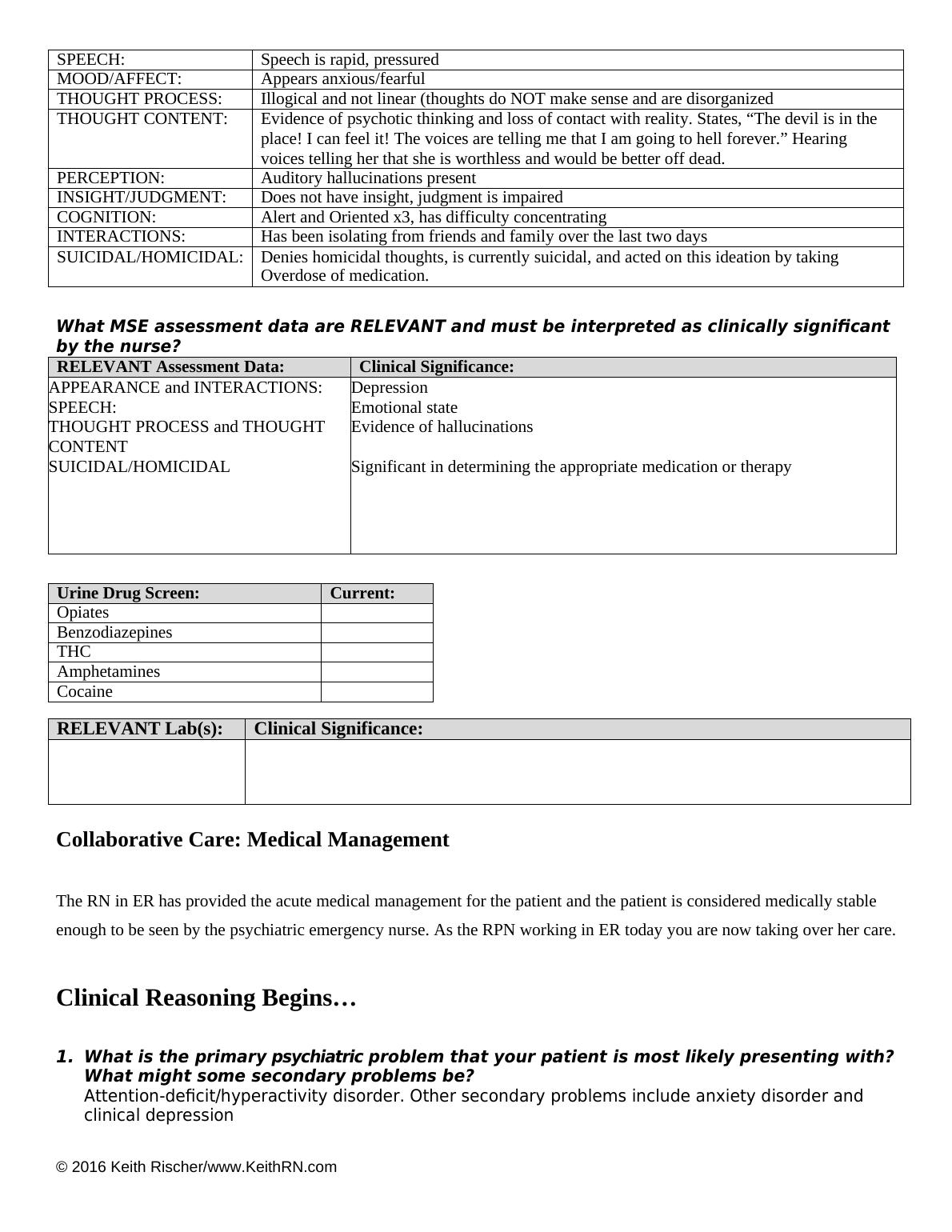
MOOD/AFFECT: Appears anxious/fearful
THOUGHT PROCESS: Illogical and not linear (thoughts do NOT make sense and are disorganized
THOUGHT CONTENT: Evidence of psychotic thinking and loss of contact with reality. States, “The devil is in the
place! I can feel it! The voices are telling me that I am going to hell forever.” Hearing
voices telling her that she is worthless and would be better off dead.
PERCEPTION: Auditory hallucinations present
INSIGHT/JUDGMENT: Does not have insight, judgment is impaired
COGNITION: Alert and Oriented x3, has difficulty concentrating
INTERACTIONS: Has been isolating from friends and family over the last two days
SUICIDAL/HOMICIDAL: Denies homicidal thoughts, is currently suicidal, and acted on this ideation by taking
Overdose of medication.
What MSE assessment data are RELEVANT and must be interpreted as clinically significant
by the nurse?
RELEVANT Assessment Data: Clinical Significance:
APPEARANCE and INTERACTIONS:
SPEECH:
THOUGHT PROCESS and THOUGHT
CONTENT
SUICIDAL/HOMICIDAL
Depression
Emotional state
Evidence of hallucinations
Significant in determining the appropriate medication or therapy
Urine Drug Screen: Current:
Opiates
Benzodiazepines
THC
Amphetamines
Cocaine
RELEVANT Lab(s): Clinical Significance:
Collaborative Care: Medical Management
The RN in ER has provided the acute medical management for the patient and the patient is considered medically stable
enough to be seen by the psychiatric emergency nurse. As the RPN working in ER today you are now taking over her care.
Clinical Reasoning Begins...
1. What is the primary psychiatric problem that your patient is most likely presenting with?
What might some secondary problems be?
Attention-deficit/hyperactivity disorder. Other secondary problems include anxiety disorder and
clinical depression
MOOD/AFFECT: Appears anxious/fearful
THOUGHT PROCESS: Illogical and not linear (thoughts do NOT make sense and are disorganized
THOUGHT CONTENT: Evidence of psychotic thinking and loss of contact with reality. States, “The devil is in the
place! I can feel it! The voices are telling me that I am going to hell forever.” Hearing
voices telling her that she is worthless and would be better off dead.
PERCEPTION: Auditory hallucinations present
INSIGHT/JUDGMENT: Does not have insight, judgment is impaired
COGNITION: Alert and Oriented x3, has difficulty concentrating
INTERACTIONS: Has been isolating from friends and family over the last two days
SUICIDAL/HOMICIDAL: Denies homicidal thoughts, is currently suicidal, and acted on this ideation by taking
Overdose of medication.
What MSE assessment data are RELEVANT and must be interpreted as clinically significant
by the nurse?
RELEVANT Assessment Data: Clinical Significance:
APPEARANCE and INTERACTIONS:
SPEECH:
THOUGHT PROCESS and THOUGHT
CONTENT
SUICIDAL/HOMICIDAL
Depression
Emotional state
Evidence of hallucinations
Significant in determining the appropriate medication or therapy
Urine Drug Screen: Current:
Opiates
Benzodiazepines
THC
Amphetamines
Cocaine
RELEVANT Lab(s): Clinical Significance:
Collaborative Care: Medical Management
The RN in ER has provided the acute medical management for the patient and the patient is considered medically stable
enough to be seen by the psychiatric emergency nurse. As the RPN working in ER today you are now taking over her care.
Clinical Reasoning Begins...
1. What is the primary psychiatric problem that your patient is most likely presenting with?
What might some secondary problems be?
Attention-deficit/hyperactivity disorder. Other secondary problems include anxiety disorder and
clinical depression
End of preview
Want to access all the pages? Upload your documents or become a member.