Violence Risk Assessment Report Assignment
VerifiedAdded on 2022/09/05
|27
|9229
|33
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
VIOLENCE RISK ASSESSMENT REPORT
Name: Peter Brown Client ID no: 123456
Date of Birth: 07/07/1993 Age: 27 years
Report Date: 20/04/2020 Assessor:
1. PURPOSE OF ASSESSMENT
1.1 Mr Brown was referred to the Rehabilitation Forensic Service (RFS) by the
Health High Secure Inpatient Service (HHSIS) for an assessment of risk of
physical violence and identification of appropriate risk management strategies
for an inpatient setting.
1.2 The referral to RFS was made in the context of Mr Brown engaging in
concerning behaviours towards staff and other residents at the Healthy High
Secure Inpatient Service (HHSIS). The triggering behaviours include Mr
Brown both verbally and physically threatening staff.
1.3 Mr Brown was assessed in the Healthy High Secure Inpatient Service
(HHSIS) on the 9th April 2020 and the 14th April 2020 at the time he had
served 1 year 9 months of his 4 years 6 months full time sentence for the
following offences:
● 1 x Assault Occasioning Bodily Harm
● 1 x Breach of Order – Domestic Violence
● 1 x Deprivation of Liberty
● 1 x Escape Legal Custody
● 1 x Common Assault
● 2 x Willful Damage Property
Peter Brown DOB: 07/07/1993
Page 1 of 28
Name: Peter Brown Client ID no: 123456
Date of Birth: 07/07/1993 Age: 27 years
Report Date: 20/04/2020 Assessor:
1. PURPOSE OF ASSESSMENT
1.1 Mr Brown was referred to the Rehabilitation Forensic Service (RFS) by the
Health High Secure Inpatient Service (HHSIS) for an assessment of risk of
physical violence and identification of appropriate risk management strategies
for an inpatient setting.
1.2 The referral to RFS was made in the context of Mr Brown engaging in
concerning behaviours towards staff and other residents at the Healthy High
Secure Inpatient Service (HHSIS). The triggering behaviours include Mr
Brown both verbally and physically threatening staff.
1.3 Mr Brown was assessed in the Healthy High Secure Inpatient Service
(HHSIS) on the 9th April 2020 and the 14th April 2020 at the time he had
served 1 year 9 months of his 4 years 6 months full time sentence for the
following offences:
● 1 x Assault Occasioning Bodily Harm
● 1 x Breach of Order – Domestic Violence
● 1 x Deprivation of Liberty
● 1 x Escape Legal Custody
● 1 x Common Assault
● 2 x Willful Damage Property
Peter Brown DOB: 07/07/1993
Page 1 of 28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1.4 Please note that the two counts of willful damage (24/01/2020) and one count
of common assault (24/01/2020) occurred whilst incarcerated and relate to
damage of centre property and an assault on a nurse within the Healthy
Correctional Centre (13/11/2019).
2. SOURCES OF INFORMATION
2.1 The details contained in this report are based upon information gathered from
the following sources:
● Individual interviews with Mr Brown (2 x 2-hour interviews at the Healthy
High Secure Inpatient Service (09/04/2020 and 14/04/2020)
● Healthy Integrated Mental Health Database (HIMHD) file review (records
23/03/2012 to 08/05/2020).
● Healthy Offender Health Services File Review (08/07/2018 to 09/04/2020).
● HCC Offender Files Part 1 of 2 (04/09/2013 to 27/02/2018) and Part 2 of 2
(08/07/2018 to 09/04/2020).
● Psychometric Assessment of Mr Brown - Historical, Clinical and Risk
Management Scales – 20 version 3 (HCR-20v3).
3. ACKNOWLEDGMENT OF RIGHTS
3.1 The purpose of the assessment interviews was explained to Mr Brown as
were the limits of confidentiality and he agreed to participate. Mr Brown was
also made aware that a report outlining information reported during the
interviews and recommendations in relation to management of his risk of
violent behaviour would be provided to HCC Health Services and Healthy
Prison Mental Health Services. The purpose of this report is to assist in the
management of his institutional behaviour and support Mr Brown’s eventual
transition back to the community (fulltime release date 08/01/2023; and
eligible for parole 22/11/2021).
Peter Brown DOB: 07/07/1993
Page 2 of 28
of common assault (24/01/2020) occurred whilst incarcerated and relate to
damage of centre property and an assault on a nurse within the Healthy
Correctional Centre (13/11/2019).
2. SOURCES OF INFORMATION
2.1 The details contained in this report are based upon information gathered from
the following sources:
● Individual interviews with Mr Brown (2 x 2-hour interviews at the Healthy
High Secure Inpatient Service (09/04/2020 and 14/04/2020)
● Healthy Integrated Mental Health Database (HIMHD) file review (records
23/03/2012 to 08/05/2020).
● Healthy Offender Health Services File Review (08/07/2018 to 09/04/2020).
● HCC Offender Files Part 1 of 2 (04/09/2013 to 27/02/2018) and Part 2 of 2
(08/07/2018 to 09/04/2020).
● Psychometric Assessment of Mr Brown - Historical, Clinical and Risk
Management Scales – 20 version 3 (HCR-20v3).
3. ACKNOWLEDGMENT OF RIGHTS
3.1 The purpose of the assessment interviews was explained to Mr Brown as
were the limits of confidentiality and he agreed to participate. Mr Brown was
also made aware that a report outlining information reported during the
interviews and recommendations in relation to management of his risk of
violent behaviour would be provided to HCC Health Services and Healthy
Prison Mental Health Services. The purpose of this report is to assist in the
management of his institutional behaviour and support Mr Brown’s eventual
transition back to the community (fulltime release date 08/01/2023; and
eligible for parole 22/11/2021).
Peter Brown DOB: 07/07/1993
Page 2 of 28
4. BACKGROUND SUMMARY
4.1 Psychiatric History
Mr Brown depicts a considerable psychiatric history, which is briefed in the
`Psychometric Assessment of his reports of the doctors who have analyzed him
before he was an adjudication of his case. As his reports are present in the court, Mr
Brown’s psychiatric history would be summarized here:
The defendant Mr Brown denied any type of contact with the services of community
mental health however, he had some history of having contact with some of the
mental health services or psychiatric hospitalizations which also includes the
treatments of psychotropic medications in Queensland through his repeated
imprisonment. He also accepts that he had a history of suicide attempts or suicidal
thinking before he was transfered to the HHSIS (i.e., Health High Secure Inpatient
Service). His reported suggeted he had a history of attempting suicide in 2019, by
using a razor to cut his throats specifically the safety razors which were given to him
to shave. His effort also caused an injury which needed hospitalization and was
recognized to be a threat to life. However, Mr Brown denied any periods of
depression and he has never participated in any outpatient counselling earlier. The
defendant has also described the use of significant polysubstance and had a history
of substance abuse, and of which with the exception of his tobacco use that has
included stimulants, cannabis, and alcohol, marijuana, amphetamines, and solvents,
However, it is reported that he had stopped utilizing chroming in his adolescence
’20s i.e., dating back to his mid-adolescence but, he regularly kept abusing others at
the time of his short periods within the community (even when he was not in custody
or in prison) in which he had used every substance (except solvents) during the
presented offences against his second partner. He also referred to his major goal
during his time in the community (among incarcerations) is for utilizing drugs. Mr
Brown was found to be within the effect of the drug amphetamines as well as alcohol
during the time of his present offence while he met the criteria to use it heavily when
present inside the community.
Peter Brown DOB: 07/07/1993
Page 3 of 28
4.1 Psychiatric History
Mr Brown depicts a considerable psychiatric history, which is briefed in the
`Psychometric Assessment of his reports of the doctors who have analyzed him
before he was an adjudication of his case. As his reports are present in the court, Mr
Brown’s psychiatric history would be summarized here:
The defendant Mr Brown denied any type of contact with the services of community
mental health however, he had some history of having contact with some of the
mental health services or psychiatric hospitalizations which also includes the
treatments of psychotropic medications in Queensland through his repeated
imprisonment. He also accepts that he had a history of suicide attempts or suicidal
thinking before he was transfered to the HHSIS (i.e., Health High Secure Inpatient
Service). His reported suggeted he had a history of attempting suicide in 2019, by
using a razor to cut his throats specifically the safety razors which were given to him
to shave. His effort also caused an injury which needed hospitalization and was
recognized to be a threat to life. However, Mr Brown denied any periods of
depression and he has never participated in any outpatient counselling earlier. The
defendant has also described the use of significant polysubstance and had a history
of substance abuse, and of which with the exception of his tobacco use that has
included stimulants, cannabis, and alcohol, marijuana, amphetamines, and solvents,
However, it is reported that he had stopped utilizing chroming in his adolescence
’20s i.e., dating back to his mid-adolescence but, he regularly kept abusing others at
the time of his short periods within the community (even when he was not in custody
or in prison) in which he had used every substance (except solvents) during the
presented offences against his second partner. He also referred to his major goal
during his time in the community (among incarcerations) is for utilizing drugs. Mr
Brown was found to be within the effect of the drug amphetamines as well as alcohol
during the time of his present offence while he met the criteria to use it heavily when
present inside the community.
Peter Brown DOB: 07/07/1993
Page 3 of 28
However, during the time Mr Brown gave his last interview, his overall mental
condition started to be stabilized and he was also agreed on participating in the
intervention while being compliant with his regime of taking the medication. But, he
still depicted a lack of insight considering the MD symptoms he is currently facing as
well as the results that it had on him considering the impact of polysubstance abuse
on his life. However, he was also presented with a limited insight of factors such as
contextual or personal that might have added to his violent behaviour. Even the
factors which might have aggravated or mitigated his likelihood of violence in the
coming future. The defendant has also reported years of daily alcohol use.
4.2 Forensic and Problem Behaviour History
However, almost all the following information provided is already documented within
the earlier forensic reports that were available to the Court and hence, a summary is
provided herein a summarized form. From the start of the defendant’s mental illness,
Mr Brown has been involved in problem behaviour regularly at the community level
resulting in his offences such as assault resulting in any type of harm to body,
breaching of the order associated with domestic violence, depriving the liberty, and
even to try escaping from the custody, a basic assault, as well as twice of wilful
damage in 24/01/2020 which had occurred during the time he was incarcerated and
associated with the damage of the property of centre as well as an assault within the
inpatient centre on a nurse in 2019, which had led to his arrest as well as other types
of psychiatric commitments. However, on a regular basis, his behaviours have
included offences like verbal and physical threatening and harassing other
individuals, from individuals to staff and other residents within his community within
which Mr Brown was fixated.
A few of the defendant’s behaviour moreover, in his early years consist of extensive
serious behaviour along with a higher potential of causing injuries towards others. In
17.02.2012, Mr Brown was arrested on the grounds of making false complaints
towards the police, to drive a motor vehicle whilst being within the effect of alcohol,
possessing a severe drug as well as utilizing a service for menacing, and harassing
and causing offence to others. In 2013, he was charged with an assault causing
bodily harm to an individual, breached the probation order, and multiple charges of
breaking and entering inside a dwelling house with an intention during night,
Peter Brown DOB: 07/07/1993
Page 4 of 28
condition started to be stabilized and he was also agreed on participating in the
intervention while being compliant with his regime of taking the medication. But, he
still depicted a lack of insight considering the MD symptoms he is currently facing as
well as the results that it had on him considering the impact of polysubstance abuse
on his life. However, he was also presented with a limited insight of factors such as
contextual or personal that might have added to his violent behaviour. Even the
factors which might have aggravated or mitigated his likelihood of violence in the
coming future. The defendant has also reported years of daily alcohol use.
4.2 Forensic and Problem Behaviour History
However, almost all the following information provided is already documented within
the earlier forensic reports that were available to the Court and hence, a summary is
provided herein a summarized form. From the start of the defendant’s mental illness,
Mr Brown has been involved in problem behaviour regularly at the community level
resulting in his offences such as assault resulting in any type of harm to body,
breaching of the order associated with domestic violence, depriving the liberty, and
even to try escaping from the custody, a basic assault, as well as twice of wilful
damage in 24/01/2020 which had occurred during the time he was incarcerated and
associated with the damage of the property of centre as well as an assault within the
inpatient centre on a nurse in 2019, which had led to his arrest as well as other types
of psychiatric commitments. However, on a regular basis, his behaviours have
included offences like verbal and physical threatening and harassing other
individuals, from individuals to staff and other residents within his community within
which Mr Brown was fixated.
A few of the defendant’s behaviour moreover, in his early years consist of extensive
serious behaviour along with a higher potential of causing injuries towards others. In
17.02.2012, Mr Brown was arrested on the grounds of making false complaints
towards the police, to drive a motor vehicle whilst being within the effect of alcohol,
possessing a severe drug as well as utilizing a service for menacing, and harassing
and causing offence to others. In 2013, he was charged with an assault causing
bodily harm to an individual, breached the probation order, and multiple charges of
breaking and entering inside a dwelling house with an intention during night,
Peter Brown DOB: 07/07/1993
Page 4 of 28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
breaching of bail act twice, stealing, willful and unlawful property damage. In 2018,
again he was charged with the similar orders above and else for deprivation of
liberty. Various types of 'Offender on Offender' breaches, and even the breach of
being involved in fighting others when he was in the prison. However, out of it none
of such breaches have caused any legal compensation.
Mr Brown has recognized a no history of antisocial behaviour before he was of age
12 and there is no record data or security to revoke this. Moreover, there was no
approach to his official adolescent criminal history, in any case, he reports
involvement in the minor crime. In addition, reasonably reliably over his mid to late
youth, he has an official adult criminal history which starts at age 19 years with
punishments for driving, polysubstance and threat offences. His adult criminal history
incorporates driving offences, property offences, severe offences and breaches of
parole and abusive behaviour at domestic requests. Mr Brown also presents a brief
idea of antisocial behaviour.
4.3 Family/Developmental History
The available documents available on files related to family and developmental
history are still consistent with each other. Several inconsistencies considering the
information of file as well as self-report have been observed such as the defendant's
parents were living together till the death of his father in the year 2013. He was born
on 07.07.1993. He shared his childhood with his 2 younger brothers of age 25 and
23 years. He shared a very close relationship with his younger siblings and his
brothers are involved in violent acts, incarceration as well as polysubstance abuse,
however, no history of victimization. His history doesn’t state the presence of a legal
spouse, and children. However, he had two ex-de facto partners having Intimate live-
in relationships with both (Ms Susan Creat and, Anne Smith). The second partner
being the victim of his present major offences. He had a causal relationship with both
of them. He revealed no problem with his first relationship and also reported that his
first partner moved interstate once he was detained in 2013. The respondent's first
relationship went on for 1 year 5 months (April 2012 to September 2013). Moreover,
he depicted his second relationship as not stable and within conflicts. He
externalized all the fault to his ex-accomplice's psychological state (with no affirming
Peter Brown DOB: 07/07/1993
Page 5 of 28
again he was charged with the similar orders above and else for deprivation of
liberty. Various types of 'Offender on Offender' breaches, and even the breach of
being involved in fighting others when he was in the prison. However, out of it none
of such breaches have caused any legal compensation.
Mr Brown has recognized a no history of antisocial behaviour before he was of age
12 and there is no record data or security to revoke this. Moreover, there was no
approach to his official adolescent criminal history, in any case, he reports
involvement in the minor crime. In addition, reasonably reliably over his mid to late
youth, he has an official adult criminal history which starts at age 19 years with
punishments for driving, polysubstance and threat offences. His adult criminal history
incorporates driving offences, property offences, severe offences and breaches of
parole and abusive behaviour at domestic requests. Mr Brown also presents a brief
idea of antisocial behaviour.
4.3 Family/Developmental History
The available documents available on files related to family and developmental
history are still consistent with each other. Several inconsistencies considering the
information of file as well as self-report have been observed such as the defendant's
parents were living together till the death of his father in the year 2013. He was born
on 07.07.1993. He shared his childhood with his 2 younger brothers of age 25 and
23 years. He shared a very close relationship with his younger siblings and his
brothers are involved in violent acts, incarceration as well as polysubstance abuse,
however, no history of victimization. His history doesn’t state the presence of a legal
spouse, and children. However, he had two ex-de facto partners having Intimate live-
in relationships with both (Ms Susan Creat and, Anne Smith). The second partner
being the victim of his present major offences. He had a causal relationship with both
of them. He revealed no problem with his first relationship and also reported that his
first partner moved interstate once he was detained in 2013. The respondent's first
relationship went on for 1 year 5 months (April 2012 to September 2013). Moreover,
he depicted his second relationship as not stable and within conflicts. He
externalized all the fault to his ex-accomplice's psychological state (with no affirming
Peter Brown DOB: 07/07/1993
Page 5 of 28
data) and clarified that she was"setting him up". Mr Brown never developed this
issue yet it was important that he had an authentic record of twice the breach of
order in the event of abusive behaviour at home.
In addition, Mr Brown has no history of sexual violence. He remained socially
secluded in jail due to a limited extent to his forceful behaviour towards different
guilty offenders and furthermore because of his unpredictable behaviour with the
service units. He likewise had restrained any history from claiming exploitation or
injury and there was no document data to decline this part.
4.4 Educational/Occupational History
Mr Brown represents a significant no history of education and never finished
secondary school nor some other type of education or training as he had a disturbed
tutoring experience or truancy in his pre-adulthood for as long as 16 years.
Moreover, he was very occupied with day by day chroming, a minor crime, (for
example, non-violent, explicitly property and medication possession) before he left
the school which was because of the social gathering he had connected himself to.
In any case, the past hazard evaluation report (dated 11/12/2016) suggested that
adolescent offending history expressed that in his pre-adulthood he was removed
from the school after he was physically assaulted by a fellow cohort when he was 14.
He had a past filled with scholastical challenges as he failed in the entirety of his
courses which brought about his development in Toowoomba with his Aunt to
attempt TAFE preparation. He told in the report that he left his home at 16 years old
in the wake of leaving school to finish an electrical apprenticeship however he
couldn't finish it. Moreover, he neglected to furnish detail on who he remained with or
how he upheld himself during this period.
Mr Brown has recognized a no history of work in community or care except for
kitchen turn in his past imprisonment where he was sacked for returning food to the
detainee settlement units (against jail rules). It merits considering the impact Mr
Brown's psychological well-being has had upon his inspiration and capacity to
achieve and keep up profitable work.
Peter Brown DOB: 07/07/1993
Page 6 of 28
issue yet it was important that he had an authentic record of twice the breach of
order in the event of abusive behaviour at home.
In addition, Mr Brown has no history of sexual violence. He remained socially
secluded in jail due to a limited extent to his forceful behaviour towards different
guilty offenders and furthermore because of his unpredictable behaviour with the
service units. He likewise had restrained any history from claiming exploitation or
injury and there was no document data to decline this part.
4.4 Educational/Occupational History
Mr Brown represents a significant no history of education and never finished
secondary school nor some other type of education or training as he had a disturbed
tutoring experience or truancy in his pre-adulthood for as long as 16 years.
Moreover, he was very occupied with day by day chroming, a minor crime, (for
example, non-violent, explicitly property and medication possession) before he left
the school which was because of the social gathering he had connected himself to.
In any case, the past hazard evaluation report (dated 11/12/2016) suggested that
adolescent offending history expressed that in his pre-adulthood he was removed
from the school after he was physically assaulted by a fellow cohort when he was 14.
He had a past filled with scholastical challenges as he failed in the entirety of his
courses which brought about his development in Toowoomba with his Aunt to
attempt TAFE preparation. He told in the report that he left his home at 16 years old
in the wake of leaving school to finish an electrical apprenticeship however he
couldn't finish it. Moreover, he neglected to furnish detail on who he remained with or
how he upheld himself during this period.
Mr Brown has recognized a no history of work in community or care except for
kitchen turn in his past imprisonment where he was sacked for returning food to the
detainee settlement units (against jail rules). It merits considering the impact Mr
Brown's psychological well-being has had upon his inspiration and capacity to
achieve and keep up profitable work.
Peter Brown DOB: 07/07/1993
Page 6 of 28
5. PRESENTATION AT INTERVIEW
5.1 Mr Brown presented polite and co-operative to both interviews for this report.
He presented as generally euphoric, not overtly elevated, however quite
animated when discussing certain events (e.g., circumstances of his last
arrest). Mr Brown’s thought form was not disordered, however his thought
content included ongoing paranoid and persecutory beliefs. Some beliefs
appeared to be reality based, however ongoing delusional beliefs with regards
to his ex-partner were reported. There was no evidence (self-report or
observed) of perceptual disturbance. Mr Brown had some insight into the
morbid degree of his paranoia and his need for mental health treatment
however this was limited when it came to his substance use and violence risk.
He presented as motivated to change his life, however he holds unrealistic
expectations with regards to mental health intervention. At the time of the
interviews he denied suicidal and/or violent ideation, intent or plan. However,
it was reported post interview period (and prior to completion of this report)
that Mr Brown had made some vague intimidating statements in the context of
his frustration with the mental health processes.
6. VIOLENCE RISK ASSESSMENT
The defendant Mr Brown also denied having any history of violence before the
age of 12 years and there is no record data or support to decline this.
Notwithstanding, he had a past filled with being suspended from school at age
14 years for a physical assault on a fellow classmate at the same time, he
denied some other physical violence during his adolescence. He additionally
revealed that his Juvenile criminal history included minor property, driving and
medication offences, while he was never detained in an adolescent
confinement place. Additionally, his adult criminal history and custodial
occurrences have included various events of both undermined and
acknowledged physical violence. The reports additionally proposed that his
dangers of violence are under the criteria for violence in item 1 as they
expressly convey the plan to cause physical damage and incorporate
threatening behaviour that imparts an aim to cause physical damage (Dickens
and O'Shea, 2017). He had additionally gotten impositions of both lawful
Peter Brown DOB: 07/07/1993
Page 7 of 28
5.1 Mr Brown presented polite and co-operative to both interviews for this report.
He presented as generally euphoric, not overtly elevated, however quite
animated when discussing certain events (e.g., circumstances of his last
arrest). Mr Brown’s thought form was not disordered, however his thought
content included ongoing paranoid and persecutory beliefs. Some beliefs
appeared to be reality based, however ongoing delusional beliefs with regards
to his ex-partner were reported. There was no evidence (self-report or
observed) of perceptual disturbance. Mr Brown had some insight into the
morbid degree of his paranoia and his need for mental health treatment
however this was limited when it came to his substance use and violence risk.
He presented as motivated to change his life, however he holds unrealistic
expectations with regards to mental health intervention. At the time of the
interviews he denied suicidal and/or violent ideation, intent or plan. However,
it was reported post interview period (and prior to completion of this report)
that Mr Brown had made some vague intimidating statements in the context of
his frustration with the mental health processes.
6. VIOLENCE RISK ASSESSMENT
The defendant Mr Brown also denied having any history of violence before the
age of 12 years and there is no record data or support to decline this.
Notwithstanding, he had a past filled with being suspended from school at age
14 years for a physical assault on a fellow classmate at the same time, he
denied some other physical violence during his adolescence. He additionally
revealed that his Juvenile criminal history included minor property, driving and
medication offences, while he was never detained in an adolescent
confinement place. Additionally, his adult criminal history and custodial
occurrences have included various events of both undermined and
acknowledged physical violence. The reports additionally proposed that his
dangers of violence are under the criteria for violence in item 1 as they
expressly convey the plan to cause physical damage and incorporate
threatening behaviour that imparts an aim to cause physical damage (Dickens
and O'Shea, 2017). He had additionally gotten impositions of both lawful
Peter Brown DOB: 07/07/1993
Page 7 of 28
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
(criminal feelings), custodial (jailbreaks) and schooling (suspension) outcomes
for his violent conduct. He had a clear pattern of violence in his history as he
met the criteria for at any rate at least three particular events of violence.
Likewise, his willful damage offence that happened while in imprisonment can
be considered right now the damage of property and expectation to utilize the
property as projectiles to hurt others and cause fear. Indeed, even the
defendant's conviction for the hardship of freedom meets the criteria for the
meaning of violence as indicated by the HCR-20v3 (Douglas, 2014).
He tended to externalize the fault frequently to the people in question. He
additionally had an example of a relationship with antisocial peers and was
given pro-criminal behaviour and exceptionally dismissive of the criminal
justice framework. Moreover, it was not obvious that he delighted in the
enduring of others but instead have considered the to be of violence as an
adequate method to accomplish his objective.
The obtained descriptions of Mr Brown inside his document data mirrored the
utilization of violence to address his issues, antagonistic communications,
careless and rash behaviour. He additionally made some questionable
intimidating articulations with regards to his dissatisfaction with the mental
health forms after the interview. It is, in any case, significant that his
psychological state, specifically, his suspicious delusions bring about him
wrongly deciphering other's practices and have prompted physical arguments
in custody.
7. RISK FORMULATION
Mr Brown had various historical factors that might place him at risk for the
case of future violence. The risk involved a history of earlier cases of violence
initiating at an extensively young age (which is documented within the file
information as well as in earlier assessment reports), his abusive relationship
with his second partner Ms Anne Smith, along with his history of educational
and occupational issues, his history of untreated polysubstance use, as well
as his records while no record of juvenile offences has been recorded. The
defendant has caused the breach of parole on three events and abusive
behaviour at home request on two events. He has broken jail rules on 15
Peter Brown DOB: 07/07/1993
Page 8 of 28
for his violent conduct. He had a clear pattern of violence in his history as he
met the criteria for at any rate at least three particular events of violence.
Likewise, his willful damage offence that happened while in imprisonment can
be considered right now the damage of property and expectation to utilize the
property as projectiles to hurt others and cause fear. Indeed, even the
defendant's conviction for the hardship of freedom meets the criteria for the
meaning of violence as indicated by the HCR-20v3 (Douglas, 2014).
He tended to externalize the fault frequently to the people in question. He
additionally had an example of a relationship with antisocial peers and was
given pro-criminal behaviour and exceptionally dismissive of the criminal
justice framework. Moreover, it was not obvious that he delighted in the
enduring of others but instead have considered the to be of violence as an
adequate method to accomplish his objective.
The obtained descriptions of Mr Brown inside his document data mirrored the
utilization of violence to address his issues, antagonistic communications,
careless and rash behaviour. He additionally made some questionable
intimidating articulations with regards to his dissatisfaction with the mental
health forms after the interview. It is, in any case, significant that his
psychological state, specifically, his suspicious delusions bring about him
wrongly deciphering other's practices and have prompted physical arguments
in custody.
7. RISK FORMULATION
Mr Brown had various historical factors that might place him at risk for the
case of future violence. The risk involved a history of earlier cases of violence
initiating at an extensively young age (which is documented within the file
information as well as in earlier assessment reports), his abusive relationship
with his second partner Ms Anne Smith, along with his history of educational
and occupational issues, his history of untreated polysubstance use, as well
as his records while no record of juvenile offences has been recorded. The
defendant has caused the breach of parole on three events and abusive
behaviour at home request on two events. He has broken jail rules on 15
Peter Brown DOB: 07/07/1993
Page 8 of 28
events over his present detainment of which 12 included offenders on guilty
incidents (physical battles between two guilty parties). He likewise had a past
filled with dysphoric mood and neurovegetative unsettling influence. He
revealed a background marked by discontinuous perceptual difficulty in the
course of recent years including a male voice that he speaks with, portraying
him as a devil. He further gave distrustful considering delusional intensity e.g.,
accepted that his ex-accomplice had been both taping his discussions at the
hour of his file offence and remotely now while in confinement by means of
satellite. He likewise talked about his capacity to foresee significant occasions
that he can't examine with anybody until they are accounted for day by day in
the paper. Impression was that of an antisocial personality issue, emotional
dysregulation, and likely psychotic side effects. Moreover, he was opened to
the service for a mental evaluation. Furthermore, there are several historical
factors that might help in protecting Mr Brown against the future risk which
included his absence of a diagnosable personality disorder, as well as his
evident success considering an earlier period of release under supervision.
However, the clinical scales suggested the evidence of risk as well as
protective factors that may affect Mr Brown’s risk for his offences and re-
offence in future. The initial protective factor is considered to be the present
compliance of the inmate along with the present substance compliance and
the effect of substance abuse on the defendant’s mental illness. Moreover,
there is a remarkable presence of his thinking which tends to be more
impulsive with little planning (Fazel et al., 2016).
Mr Brown's violent conduct doesn't communicate powerful urges or desires to
hurt others later on. In any case, he presents with threatening attribution bias
in that he qualities violent aim with respect to others without a genuine plan.
Mr Brown limits his duty in his utilization of violence against others. There had
been an acceleration in his utilization of violence however, this has
additionally resembled the disintegration of his psychological well-being. The
defendant also depicts improved hostile attribution bias skills. However, his
records suggested that Mr Brown had depicted the skills to be callous and
violent, he denied any current suicidal or homicidal intent or ideation at the
time of both interviews. He has made no particular plans for his mental health
Peter Brown DOB: 07/07/1993
Page 9 of 28
incidents (physical battles between two guilty parties). He likewise had a past
filled with dysphoric mood and neurovegetative unsettling influence. He
revealed a background marked by discontinuous perceptual difficulty in the
course of recent years including a male voice that he speaks with, portraying
him as a devil. He further gave distrustful considering delusional intensity e.g.,
accepted that his ex-accomplice had been both taping his discussions at the
hour of his file offence and remotely now while in confinement by means of
satellite. He likewise talked about his capacity to foresee significant occasions
that he can't examine with anybody until they are accounted for day by day in
the paper. Impression was that of an antisocial personality issue, emotional
dysregulation, and likely psychotic side effects. Moreover, he was opened to
the service for a mental evaluation. Furthermore, there are several historical
factors that might help in protecting Mr Brown against the future risk which
included his absence of a diagnosable personality disorder, as well as his
evident success considering an earlier period of release under supervision.
However, the clinical scales suggested the evidence of risk as well as
protective factors that may affect Mr Brown’s risk for his offences and re-
offence in future. The initial protective factor is considered to be the present
compliance of the inmate along with the present substance compliance and
the effect of substance abuse on the defendant’s mental illness. Moreover,
there is a remarkable presence of his thinking which tends to be more
impulsive with little planning (Fazel et al., 2016).
Mr Brown's violent conduct doesn't communicate powerful urges or desires to
hurt others later on. In any case, he presents with threatening attribution bias
in that he qualities violent aim with respect to others without a genuine plan.
Mr Brown limits his duty in his utilization of violence against others. There had
been an acceleration in his utilization of violence however, this has
additionally resembled the disintegration of his psychological well-being. The
defendant also depicts improved hostile attribution bias skills. However, his
records suggested that Mr Brown had depicted the skills to be callous and
violent, he denied any current suicidal or homicidal intent or ideation at the
time of both interviews. He has made no particular plans for his mental health
Peter Brown DOB: 07/07/1993
Page 9 of 28
aftercare which also depicts having a normal relationship with the peers at the
facility. Mr Brown also claims his understanding of the underlying appraisals
post-arrival in HHSIS identified with a degree of confusion with conspicuous
pretentiousness, an illogical and over-well-known air and a level of woolliness
to his reasoning. He additionally has some successive idiotic upheavals of
singing and boasting were very incongruent to his conditions. He additionally
portrayed the state of mind fluctuation with various persecutory convictions
that were unmistakable while, some are no uncertainty reality-based (and
identified with his contentions with different guilty parties and solitary friends in
the community) however many are unusual in source. While his character
pathology was clear there was proof of a potential psychotic ailment with
beginning in any event a year sooner. It was recognized that his unlawful
substances use may have added to a worsening of his psychotic side effects
notwithstanding, there was a history that proposed that his psychotic
manifestations continued for quite a while even without illegal medications. It
was noticed that he experienced issues resting the first night and was seen to
be individualized boxing, whistling and talking noisily until 0015. The first
evening he was seen to just have three hours of irregular sleep (Iozzino et al.,
2015).
It is additionally noticed that Mr Brown exhibited an agreeable, pleasant,
helpful, aware, and cheerful behaviour to be in the medical clinic. Moreover,
his psychological state was evaluated as raised temperament, with affected
mood, psychosis, anxiety, and fear about security and police. His reports
likewise portray that he detests individuals in power, clarifying that he had
been attacked in the past by the police whom he accepts don't care for him.
Despite the fact that he is apologetic with respect to an occurrence in which
he threatened to "crush" staff if they gave him an injection and expressed that
the evil spirit disclosed to him that individuals were out to get him. While at
HHSIS there has been some adjustment in Mr Brown's psychological state.
He presents euphoric, not unmistakably raised with substitute times of
dysphoria. His idea structure can't, however, his idea content incorporates
suspicious and persecutory convictions. Out of which a few convictions are
reality-based, moreover, he keeps on holding continuous delusional
Peter Brown DOB: 07/07/1993
Page 10 of 28
facility. Mr Brown also claims his understanding of the underlying appraisals
post-arrival in HHSIS identified with a degree of confusion with conspicuous
pretentiousness, an illogical and over-well-known air and a level of woolliness
to his reasoning. He additionally has some successive idiotic upheavals of
singing and boasting were very incongruent to his conditions. He additionally
portrayed the state of mind fluctuation with various persecutory convictions
that were unmistakable while, some are no uncertainty reality-based (and
identified with his contentions with different guilty parties and solitary friends in
the community) however many are unusual in source. While his character
pathology was clear there was proof of a potential psychotic ailment with
beginning in any event a year sooner. It was recognized that his unlawful
substances use may have added to a worsening of his psychotic side effects
notwithstanding, there was a history that proposed that his psychotic
manifestations continued for quite a while even without illegal medications. It
was noticed that he experienced issues resting the first night and was seen to
be individualized boxing, whistling and talking noisily until 0015. The first
evening he was seen to just have three hours of irregular sleep (Iozzino et al.,
2015).
It is additionally noticed that Mr Brown exhibited an agreeable, pleasant,
helpful, aware, and cheerful behaviour to be in the medical clinic. Moreover,
his psychological state was evaluated as raised temperament, with affected
mood, psychosis, anxiety, and fear about security and police. His reports
likewise portray that he detests individuals in power, clarifying that he had
been attacked in the past by the police whom he accepts don't care for him.
Despite the fact that he is apologetic with respect to an occurrence in which
he threatened to "crush" staff if they gave him an injection and expressed that
the evil spirit disclosed to him that individuals were out to get him. While at
HHSIS there has been some adjustment in Mr Brown's psychological state.
He presents euphoric, not unmistakably raised with substitute times of
dysphoria. His idea structure can't, however, his idea content incorporates
suspicious and persecutory convictions. Out of which a few convictions are
reality-based, moreover, he keeps on holding continuous delusional
Peter Brown DOB: 07/07/1993
Page 10 of 28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
convictions, especially with respect to his ex-accomplice. There is right now
no proof (self-report or watched) of perceptual unsettling influence. Mr Brown
has some knowledge into the morbid level of his suspicion and communicates
a longing to change, in any case, he holds ridiculous desires with respect to
psychological wellness intervention. Taking into account that, Mr Brown
despite everything reports the capacity to anticipate significant occasions (Neil
et al., 2019).
He has a background marked by discontinuous consistency with medication.
At the hour of his last meeting, he was happy to take an interest in
interventions and stay agreeable with his medicine. Moreover, it requires
checking given his history of progress right now. The staff member further has
communicated worries concerning Mr Brown having the option to deal with his
own risk, while his arrangements are not reliable with that of the treating team.
Although Mr Brown medications helped him to remain stable, however, real
commitment towards taking medication within the less supervised is still not
clear. While he had promised to be on medications earlier however, he had
some history to stop taking medications. Mr Brown has some understanding
into the morbid level of his fear and communicates a longing to change,
however, he holds unreasonable desires with respect to mental health
intervention and substance use. He has no express plans for his potential
capacity discharge either at his parole qualification date or full-time discharge.
He has no aim of joining in with proficient services upon discharge. He is
eager to take part in interventions at HHSIS comparable to his mental health
as long as they don't target substance misuse or violence. While surveying
the risk management items Mr Brown has additionally raised worries about
other patients' conduct in the ward and he never got any genuine community
support as he has no contact with his family while he has restricted prosocial
peers.
However, if he returns back to the community, Mr Brown would likely be
exposed to various kinds of destabilizers as well as stressors. He has a
history of untreated polysubstance abuse issues and then he might again be
accessible with polysubstance use due to limited coping strategies and poor
Peter Brown DOB: 07/07/1993
Page 11 of 28
no proof (self-report or watched) of perceptual unsettling influence. Mr Brown
has some knowledge into the morbid level of his suspicion and communicates
a longing to change, in any case, he holds ridiculous desires with respect to
psychological wellness intervention. Taking into account that, Mr Brown
despite everything reports the capacity to anticipate significant occasions (Neil
et al., 2019).
He has a background marked by discontinuous consistency with medication.
At the hour of his last meeting, he was happy to take an interest in
interventions and stay agreeable with his medicine. Moreover, it requires
checking given his history of progress right now. The staff member further has
communicated worries concerning Mr Brown having the option to deal with his
own risk, while his arrangements are not reliable with that of the treating team.
Although Mr Brown medications helped him to remain stable, however, real
commitment towards taking medication within the less supervised is still not
clear. While he had promised to be on medications earlier however, he had
some history to stop taking medications. Mr Brown has some understanding
into the morbid level of his fear and communicates a longing to change,
however, he holds unreasonable desires with respect to mental health
intervention and substance use. He has no express plans for his potential
capacity discharge either at his parole qualification date or full-time discharge.
He has no aim of joining in with proficient services upon discharge. He is
eager to take part in interventions at HHSIS comparable to his mental health
as long as they don't target substance misuse or violence. While surveying
the risk management items Mr Brown has additionally raised worries about
other patients' conduct in the ward and he never got any genuine community
support as he has no contact with his family while he has restricted prosocial
peers.
However, if he returns back to the community, Mr Brown would likely be
exposed to various kinds of destabilizers as well as stressors. He has a
history of untreated polysubstance abuse issues and then he might again be
accessible with polysubstance use due to limited coping strategies and poor
Peter Brown DOB: 07/07/1993
Page 11 of 28
frustration tolerance. Therefore, it is unlikely for him to engage in adaptive
coping in the context of stressors (Persson et al., 2017).
The defendant has been imprisoned since (24.01.2020) and is probably not
ready for how a lot of the outside world has changed within that time period.
Mr Brown doesn't have a GED, he has restricted employment abilities, and he
has no social support as it is constrained (Persson et al., 2017). After his
release from his sentence, he should continue his duty regarding keeping a
living arrangement, cooking, cleaning, and so on. In conclusion, Mr Brown's
release plan as of now gives off an impression of being deficient. He knows,
in any case, that he should finish his release arrangement classes and
realizes which staff individuals he needs to work with to build up a superior
release plan. In spite of the fact that he is now truly stable on psychiatric
medication, his understanding into his requirement for progressing need for
psychological wellness treatment stays uncertain, and he will be presented to
huge burdens and stresses when he will be released to the community. To the
degree that such concerns could be approached, the defendant's risk for
future issues could be decreased. Considering the HCR-20, and the particular
risk and defensive factors that were considered, it was inferred that the
defendant was recognized to be at low-moderate risk to participate in future
violence if he was to return to the community (Persson et al., 2017).
8. RISK MANAGEMENT RECOMMENDATIONS
It should be noticed that the foresight of dangerousness is of constrained
certainty at the point of risk formulation, and the precision of an expectation
lessens after some time. The Risk Assessment report created a view on
whether Mr Brown is experiencing a psychological illness or deformity as the
consequence of which his release would make a generous risk of real injury to
someone else or substantial damage to the property of another. Variables not
identified with psychological instability may add to the person's being a more
substantial risk for violence, criminal, or inconvenience behaviour. The current
evaluation distinguished a few historical variables that may put the prisoner in
risk, and those elements were discussed earlier. As per the law, moreover,
Peter Brown DOB: 07/07/1993
Page 12 of 28
coping in the context of stressors (Persson et al., 2017).
The defendant has been imprisoned since (24.01.2020) and is probably not
ready for how a lot of the outside world has changed within that time period.
Mr Brown doesn't have a GED, he has restricted employment abilities, and he
has no social support as it is constrained (Persson et al., 2017). After his
release from his sentence, he should continue his duty regarding keeping a
living arrangement, cooking, cleaning, and so on. In conclusion, Mr Brown's
release plan as of now gives off an impression of being deficient. He knows,
in any case, that he should finish his release arrangement classes and
realizes which staff individuals he needs to work with to build up a superior
release plan. In spite of the fact that he is now truly stable on psychiatric
medication, his understanding into his requirement for progressing need for
psychological wellness treatment stays uncertain, and he will be presented to
huge burdens and stresses when he will be released to the community. To the
degree that such concerns could be approached, the defendant's risk for
future issues could be decreased. Considering the HCR-20, and the particular
risk and defensive factors that were considered, it was inferred that the
defendant was recognized to be at low-moderate risk to participate in future
violence if he was to return to the community (Persson et al., 2017).
8. RISK MANAGEMENT RECOMMENDATIONS
It should be noticed that the foresight of dangerousness is of constrained
certainty at the point of risk formulation, and the precision of an expectation
lessens after some time. The Risk Assessment report created a view on
whether Mr Brown is experiencing a psychological illness or deformity as the
consequence of which his release would make a generous risk of real injury to
someone else or substantial damage to the property of another. Variables not
identified with psychological instability may add to the person's being a more
substantial risk for violence, criminal, or inconvenience behaviour. The current
evaluation distinguished a few historical variables that may put the prisoner in
risk, and those elements were discussed earlier. As per the law, moreover,
Peter Brown DOB: 07/07/1993
Page 12 of 28
the prediction especially concerns the risk of violence risk that occurs from a
psychological disorder. He shows psychotic side effects, including
hallucinations, delusions, as well as disorganized behaviour (Picchioni &
Dickens, 2014). Accordingly, he seems to meet the initial criteria, in that he
has a psychological disorder. However, the question with respect to whether
he is dangerous in view of the mental disorder still remains (Picchioni &
Dickens, 2014).
Mr Brown has had broad contact with mental health services in Queensland
through his occasional imprisonments. He detailed that he got a scope of
mental drugs (antidepressants and antipsychotics) however couldn't provide
an unmistakable diagnosis. Case notes of 24 March 2020 relating to the
diagnosis gave to help his exchange to the HHSIS. He was seen on various
events by the Healthy Correctional Center Visiting Medical Officer (WMO)
through his last imprisonment and was treated with a state of mind stabilizer
and benzodiazepines because of concerns raised by the nursing and
custodial staff about an increased degree of complication and unsettling, and
worries for his wellbeing following a suicide effort (01.11.2019). He was then
referred to the Healthy Prison Mental Health Service (HPMHS) on two events
all through that period yet was considered to have no mental illness and was
not opened to the services around then. Mr Brown is right now carrying out a
punishment of 4 years and a half year. Mr Brown tried to end it all by cutting
his throat with razors taken from a security razor. It was noticed that the one
count of Common Assault and 2 counts of Wilful Damage happened while in
guardianship. Mr Brown went to the health centre on 13 November 2019 and
when he discovered it was to see the counselling therapist he got agitated
and forceful and attempted to leave the health centre without authorization
from the custodial official answerable for detainee developments. This
occurrence brought about Mr Brown being indicted for a count of common
assault and 2 counts of wilful damage. Mr Brown was not affected by
substances at the hour of this occurrence. Based on his psychopathology and
the obstacles of the accommodation area, Mr Brown was referred for inpatient
appraisal in the Healthy High-Security Inpatient Service (HHSIS) (Piel, 2015).
Mr Brown is eager to participate in an intervention to address his mental
Peter Brown DOB: 07/07/1993
Page 13 of 28
psychological disorder. He shows psychotic side effects, including
hallucinations, delusions, as well as disorganized behaviour (Picchioni &
Dickens, 2014). Accordingly, he seems to meet the initial criteria, in that he
has a psychological disorder. However, the question with respect to whether
he is dangerous in view of the mental disorder still remains (Picchioni &
Dickens, 2014).
Mr Brown has had broad contact with mental health services in Queensland
through his occasional imprisonments. He detailed that he got a scope of
mental drugs (antidepressants and antipsychotics) however couldn't provide
an unmistakable diagnosis. Case notes of 24 March 2020 relating to the
diagnosis gave to help his exchange to the HHSIS. He was seen on various
events by the Healthy Correctional Center Visiting Medical Officer (WMO)
through his last imprisonment and was treated with a state of mind stabilizer
and benzodiazepines because of concerns raised by the nursing and
custodial staff about an increased degree of complication and unsettling, and
worries for his wellbeing following a suicide effort (01.11.2019). He was then
referred to the Healthy Prison Mental Health Service (HPMHS) on two events
all through that period yet was considered to have no mental illness and was
not opened to the services around then. Mr Brown is right now carrying out a
punishment of 4 years and a half year. Mr Brown tried to end it all by cutting
his throat with razors taken from a security razor. It was noticed that the one
count of Common Assault and 2 counts of Wilful Damage happened while in
guardianship. Mr Brown went to the health centre on 13 November 2019 and
when he discovered it was to see the counselling therapist he got agitated
and forceful and attempted to leave the health centre without authorization
from the custodial official answerable for detainee developments. This
occurrence brought about Mr Brown being indicted for a count of common
assault and 2 counts of wilful damage. Mr Brown was not affected by
substances at the hour of this occurrence. Based on his psychopathology and
the obstacles of the accommodation area, Mr Brown was referred for inpatient
appraisal in the Healthy High-Security Inpatient Service (HHSIS) (Piel, 2015).
Mr Brown is eager to participate in an intervention to address his mental
Peter Brown DOB: 07/07/1993
Page 13 of 28
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
health issues however not the risk of violence or substance misuse (Ramesh
et al., 2018).
The defendant depicts a pattern of getting irritable, forceful, and hostile when
he is not taking a psychiatric drug. Mr Brown would take part in several
troublesome and risky practices while he was not on drugs, including assault
with inpatient staff, spitting at staff, and making unjustifiable dangers.
Interestingly, Mr Brown presents as friendly as well as helpful when he is
taking mental medicine and has gotten hardly any incident reports while he
has been effectively occupied with treatment (Roychowdhury & Adshead,
2014). This proposes the defendant's psychological instability makes it
progressively hard to manage his feelings, use great reality testing, and
control his behaviour. Considering that, he is bound to consider others to be
dangers and act violently when he is effectively psychotic. In view of these
perceptions, the defendant's dysfunctional behaviour seems to put him at an
enhanced risk of acting dangerously. Right now, in any case, Mr Brown is not
under medication as recommended yet he has been working admirably on an
open unit for a while. Given the defendant's reaction to treatment, almost
certainly, his dysfunctional behaviour can be successfully overseen in the
community as long as he stays consistent with medicine and psychological
wellness aftercare (Harris et al., 2019).
In shaping their last opinion, the assessment panel acknowledged a few
factors that may affect Mr Brown's capacity to control a restrictive release.
Explicit variables that were investigated incorporated his diagnosis, history of
violence, his present compliance with a mental prescription, his institutional
change, his polysubstance abuse history, and his arrangements for coming
back to the community. The board likewise noted Mr Brown's risk and
defensive components recognized by the HCR-20 (Fazel et al., 2016). It was
noticed that Mr Brown is now working at a significant level inside the
institution and noticed his initial approval for managed release. After Mr Brown
was interviewed, the defendant and the factors considered, the evaluation of
the Risk Assessment report was that Mr Brown presently experiences
psychological disorder that places him in the risk of hurting others, or the
property of others, in the event that he is untreated when released. They
explained, however, that they accepted that he is right now working at a
Peter Brown DOB: 07/07/1993
Page 14 of 28
et al., 2018).
The defendant depicts a pattern of getting irritable, forceful, and hostile when
he is not taking a psychiatric drug. Mr Brown would take part in several
troublesome and risky practices while he was not on drugs, including assault
with inpatient staff, spitting at staff, and making unjustifiable dangers.
Interestingly, Mr Brown presents as friendly as well as helpful when he is
taking mental medicine and has gotten hardly any incident reports while he
has been effectively occupied with treatment (Roychowdhury & Adshead,
2014). This proposes the defendant's psychological instability makes it
progressively hard to manage his feelings, use great reality testing, and
control his behaviour. Considering that, he is bound to consider others to be
dangers and act violently when he is effectively psychotic. In view of these
perceptions, the defendant's dysfunctional behaviour seems to put him at an
enhanced risk of acting dangerously. Right now, in any case, Mr Brown is not
under medication as recommended yet he has been working admirably on an
open unit for a while. Given the defendant's reaction to treatment, almost
certainly, his dysfunctional behaviour can be successfully overseen in the
community as long as he stays consistent with medicine and psychological
wellness aftercare (Harris et al., 2019).
In shaping their last opinion, the assessment panel acknowledged a few
factors that may affect Mr Brown's capacity to control a restrictive release.
Explicit variables that were investigated incorporated his diagnosis, history of
violence, his present compliance with a mental prescription, his institutional
change, his polysubstance abuse history, and his arrangements for coming
back to the community. The board likewise noted Mr Brown's risk and
defensive components recognized by the HCR-20 (Fazel et al., 2016). It was
noticed that Mr Brown is now working at a significant level inside the
institution and noticed his initial approval for managed release. After Mr Brown
was interviewed, the defendant and the factors considered, the evaluation of
the Risk Assessment report was that Mr Brown presently experiences
psychological disorder that places him in the risk of hurting others, or the
property of others, in the event that he is untreated when released. They
explained, however, that they accepted that he is right now working at a
Peter Brown DOB: 07/07/1993
Page 14 of 28
sufficiently high level that the risk can be supervised in a community setting
provided Mr Brown gets noteworthy supervision and aftercare treatment. The
board proposed that the defendant may improve in a setting where his
medication compliance can be firmly checked (Fazel et al., 2016). They
additionally prescribed that the defendant may profit by different sorts of
programming including GED classes, work training, and polysubstance abuse
treatment. It was communicated that the defendant is prepared for restrictive
release to a community setting under proper supervision (Anderson & Jenson,
2019).
Regarding his communication with the stakeholders, Mr Brown, until his
temporary move to the Healthy High Secure Inpatient Service (HHSIS) was
accommodated in the Healthy Correctional Centre (HCC). The Offender
Health service has an in-reach Prison Mental Health Service (PMHS) which is
responsible for the mental health of prisoners. Through the Offender Health
service, PMHS prisoners such as Mr Brown refers to consulting psychiatrists
and visiting medical officers (doctors) who work for the Health department but
come into the prison to treat prisoners. Mr Brown was referred to the HCC or
prison’s own psychological and counselling services which make referrals to
Offender Health services and PMHS (Fazel et al., 2016).
[Insert your name]
Healthy Rehabilitation Forensic Service
Date: 20 April 2020
Peter Brown DOB: 07/07/1993
Page 15 of 28
provided Mr Brown gets noteworthy supervision and aftercare treatment. The
board proposed that the defendant may improve in a setting where his
medication compliance can be firmly checked (Fazel et al., 2016). They
additionally prescribed that the defendant may profit by different sorts of
programming including GED classes, work training, and polysubstance abuse
treatment. It was communicated that the defendant is prepared for restrictive
release to a community setting under proper supervision (Anderson & Jenson,
2019).
Regarding his communication with the stakeholders, Mr Brown, until his
temporary move to the Healthy High Secure Inpatient Service (HHSIS) was
accommodated in the Healthy Correctional Centre (HCC). The Offender
Health service has an in-reach Prison Mental Health Service (PMHS) which is
responsible for the mental health of prisoners. Through the Offender Health
service, PMHS prisoners such as Mr Brown refers to consulting psychiatrists
and visiting medical officers (doctors) who work for the Health department but
come into the prison to treat prisoners. Mr Brown was referred to the HCC or
prison’s own psychological and counselling services which make referrals to
Offender Health services and PMHS (Fazel et al., 2016).
[Insert your name]
Healthy Rehabilitation Forensic Service
Date: 20 April 2020
Peter Brown DOB: 07/07/1993
Page 15 of 28
References
Anderson, K., & Jenson, C. (2019). Violence risk–assessment screening tools
for acute care mental health settings: Literature review. Archives Of
Psychiatric Nursing, 33(1), 112-119.
https://doi.org/10.1016/j.apnu.2018.08.012
Dickens, G., & O’Shea, L. (2017). Use of the HCR-20 for violence risk
assessment: views of clinicians working in a secure inpatient mental health
setting. The Journal Of Forensic Practice, 19(2), 130-138.
https://doi.org/10.1108/jfp-08-2016-0039
Douglas, K. (2014). Version 3 of the Historical-Clinical-Risk Management-20
(HCR-20V3): Relevance to Violence Risk Assessment and Management in
Forensic Conditional Release Contexts. Behavioral Sciences & The Law,
32(5), 557-576. https://doi.org/10.1002/bsl.2134
Fazel, S., Fimińska, Z., Cocks, C., & Coid, J. (2016). Patient outcomes following
discharge from secure psychiatric hospitals: Systematic review and meta-
analysis. British Journal Of Psychiatry, 208(1), 17-25.
https://doi.org/10.1192/bjp.bp.114.149997
Peter Brown DOB: 07/07/1993
Page 16 of 28
Anderson, K., & Jenson, C. (2019). Violence risk–assessment screening tools
for acute care mental health settings: Literature review. Archives Of
Psychiatric Nursing, 33(1), 112-119.
https://doi.org/10.1016/j.apnu.2018.08.012
Dickens, G., & O’Shea, L. (2017). Use of the HCR-20 for violence risk
assessment: views of clinicians working in a secure inpatient mental health
setting. The Journal Of Forensic Practice, 19(2), 130-138.
https://doi.org/10.1108/jfp-08-2016-0039
Douglas, K. (2014). Version 3 of the Historical-Clinical-Risk Management-20
(HCR-20V3): Relevance to Violence Risk Assessment and Management in
Forensic Conditional Release Contexts. Behavioral Sciences & The Law,
32(5), 557-576. https://doi.org/10.1002/bsl.2134
Fazel, S., Fimińska, Z., Cocks, C., & Coid, J. (2016). Patient outcomes following
discharge from secure psychiatric hospitals: Systematic review and meta-
analysis. British Journal Of Psychiatry, 208(1), 17-25.
https://doi.org/10.1192/bjp.bp.114.149997
Peter Brown DOB: 07/07/1993
Page 16 of 28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Harris, I., Beese, S., & Moore, D. (2019). Predicting repeated self-harm or
suicide in adolescents and young adults using risk assessment scales/tools:
a systematic review protocol. Systematic Reviews, 8(1).
https://doi.org/10.1186/s13643-019-1007-7
Iozzino, L., Ferrari, C., Large, M., Nielssen, O., & de Girolamo, G. (2015).
Prevalence and Risk Factors of Violence by Psychiatric Acute Inpatients: A
Systematic Review and Meta-Analysis. PLOS ONE, 10(6), e0128536.
https://doi.org/10.1371/journal.pone.0128536
Neil, C., O’Rourke, S., Ferreira, N., & Flynn, L. (2019). Protective Factors in
Violence Risk Assessment: Predictive Validity of the SAPROF and HCR-
20V3. International Journal Of Forensic Mental Health, 19(1), 84-102.
https://doi.org/10.1080/14999013.2019.1643811
Persson, M., Belfrage, H., Fredriksson, B., & Kristiansson, M. (2017). Violence
During Imprisonment, Forensic Psychiatric Care, and Probation:
Correlations and Predictive Validity of the Risk Assessment Instruments
COVR, LSI-R, HCR-20V3, and SAPROF. International Journal Of Forensic
Mental Health, 16(2), 117-129.
https://doi.org/10.1080/14999013.2016.1266420
Picchioni, M., & Dickens, G. (2014). EPA-0469 – Translating hcr-20 risk
assessment into evidence based risk management. European Psychiatry,
29, 1. https://doi.org/10.1016/s0924-9338(14)77880-0
Piel, J. (2015). Hospital-based Clinical Forensic Program in Violence Risk
Assessment: Utilization and Management Considerations. European
Psychiatry, 30, 755. https://doi.org/10.1016/s0924-9338(15)30597-6
Ramesh, T., Igoumenou, A., Vazquez Montes, M., & Fazel, S. (2018). Use of
risk assessment instruments to predict violence in forensic psychiatric
hospitals: a systematic review and meta-analysis. European Psychiatry, 52,
47-53. https://doi.org/10.1016/j.eurpsy.2018.02.007
Roychowdhury, A., & Adshead, G. (2014). Violence risk assessment as a
medical intervention: ethical tensions. The Psychiatric Bulletin, 38(2), 75-82.
https://doi.org/10.1192/pb.bp.113.043315
Peter Brown DOB: 07/07/1993
Page 17 of 28
suicide in adolescents and young adults using risk assessment scales/tools:
a systematic review protocol. Systematic Reviews, 8(1).
https://doi.org/10.1186/s13643-019-1007-7
Iozzino, L., Ferrari, C., Large, M., Nielssen, O., & de Girolamo, G. (2015).
Prevalence and Risk Factors of Violence by Psychiatric Acute Inpatients: A
Systematic Review and Meta-Analysis. PLOS ONE, 10(6), e0128536.
https://doi.org/10.1371/journal.pone.0128536
Neil, C., O’Rourke, S., Ferreira, N., & Flynn, L. (2019). Protective Factors in
Violence Risk Assessment: Predictive Validity of the SAPROF and HCR-
20V3. International Journal Of Forensic Mental Health, 19(1), 84-102.
https://doi.org/10.1080/14999013.2019.1643811
Persson, M., Belfrage, H., Fredriksson, B., & Kristiansson, M. (2017). Violence
During Imprisonment, Forensic Psychiatric Care, and Probation:
Correlations and Predictive Validity of the Risk Assessment Instruments
COVR, LSI-R, HCR-20V3, and SAPROF. International Journal Of Forensic
Mental Health, 16(2), 117-129.
https://doi.org/10.1080/14999013.2016.1266420
Picchioni, M., & Dickens, G. (2014). EPA-0469 – Translating hcr-20 risk
assessment into evidence based risk management. European Psychiatry,
29, 1. https://doi.org/10.1016/s0924-9338(14)77880-0
Piel, J. (2015). Hospital-based Clinical Forensic Program in Violence Risk
Assessment: Utilization and Management Considerations. European
Psychiatry, 30, 755. https://doi.org/10.1016/s0924-9338(15)30597-6
Ramesh, T., Igoumenou, A., Vazquez Montes, M., & Fazel, S. (2018). Use of
risk assessment instruments to predict violence in forensic psychiatric
hospitals: a systematic review and meta-analysis. European Psychiatry, 52,
47-53. https://doi.org/10.1016/j.eurpsy.2018.02.007
Roychowdhury, A., & Adshead, G. (2014). Violence risk assessment as a
medical intervention: ethical tensions. The Psychiatric Bulletin, 38(2), 75-82.
https://doi.org/10.1192/pb.bp.113.043315
Peter Brown DOB: 07/07/1993
Page 17 of 28

Peter Brown DOB: 07/07/1993
Page 18 of 28
Page 18 of 28
Appendix A
(Begin completing as part of Assessment – insert description of HCR-20v3)
H1: Presence=Yes, Relevance=High
Mr. Brown first expressed violence at the age of 12. Mr Brown's conviction for
deprivation of liberty meets criteria for definition of violence according to the HCR-
20v3.
H2: Presence=Yes, Relevance=High
As a young child, having no history of antisocial behaviour and there is no file
information or collateral to contradict this in antisocial behaviours that affected both
his education and his home life, before the age of 12 years he was often out to all
hours. Antisocial behaviours occur if the prosocial skills are not met and those who
suffer with childhood antisocial behaviour are more likely as an adult to offend.
H3: Presence=Yes, Relevance=High
Although intimate relationships were casual, Mr. Brown had a difficult relationship
with his second partner. His maltreatment is associated with antisocial personality
disorder and such individuals are more at risk of violent offending.
H4: Presence=Yes, Relevance=Moderate
In terms of his employment, Mr Brown lost an apprenticeship opportunity when he
was 16 and before his sentence he was unable to hold down a job.
H5: Presence=Yes, Relevance=High
Mr Brown suffered from polysubstance abuse problems, mainly amphetamines and
alcohol. Those who experienced trauma are more likely to use substances which are
linked to the levels of violence used.
H6: Presence=Yes, Relevance=High
Peter Brown DOB: 07/07/1993
Page 19 of 28
(Begin completing as part of Assessment – insert description of HCR-20v3)
H1: Presence=Yes, Relevance=High
Mr. Brown first expressed violence at the age of 12. Mr Brown's conviction for
deprivation of liberty meets criteria for definition of violence according to the HCR-
20v3.
H2: Presence=Yes, Relevance=High
As a young child, having no history of antisocial behaviour and there is no file
information or collateral to contradict this in antisocial behaviours that affected both
his education and his home life, before the age of 12 years he was often out to all
hours. Antisocial behaviours occur if the prosocial skills are not met and those who
suffer with childhood antisocial behaviour are more likely as an adult to offend.
H3: Presence=Yes, Relevance=High
Although intimate relationships were casual, Mr. Brown had a difficult relationship
with his second partner. His maltreatment is associated with antisocial personality
disorder and such individuals are more at risk of violent offending.
H4: Presence=Yes, Relevance=Moderate
In terms of his employment, Mr Brown lost an apprenticeship opportunity when he
was 16 and before his sentence he was unable to hold down a job.
H5: Presence=Yes, Relevance=High
Mr Brown suffered from polysubstance abuse problems, mainly amphetamines and
alcohol. Those who experienced trauma are more likely to use substances which are
linked to the levels of violence used.
H6: Presence=Yes, Relevance=High
Peter Brown DOB: 07/07/1993
Page 19 of 28
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
There is a possibility that Mr Brown suffers from a mood disorder due to his sudden
outbursts and change in mood, he explained how he could feel happy one minute
and angry the next.
H7: Presence-Possibility, Relevance=Moderate
In regards to personality disorder Mr Brown is being referred for an assessment for
anti-social personality disorder. Mr Jones experienced severe impulsivity in terms of
his emotions which lead to anger which is mainly associated with personality
disorders.
H8: Presence=Nil, Relevance=Low
Mr Brown denies any history of victimisation or trauma.
H9: Presence=Yes, Relevance=High
Mr Brown’ attitude towards his own personal violence does not leave much to be
desired. He constantly blames others for his own violent outbursts and when he
acknowledges these he condones his behaviour with some form of rationale.
H10: Presence=Yes, Relevance=High
He was exposed to substance misuse as his brothers were involved with the
substance abuse groups but unfortunately still felt he would continue using drugs
and held this negative attitude throughout the session.
Clinical Scale: Presence=Yes, Relevance=High
His education could play a role in his offending and anti-socialness as he never
succeeded academically. The negative experience at school could lead to violent
behaviours.
C1: Presence=Possible, Relevance=Moderate
Mr Brown’ insight is poor regarding his offence, drug abuse as well as the possibility
of having a mental illness. Regarding the assessment of mental illness Mr Brown
voices his opinion relating to the matter. He believes that he does not suffer from a
Peter Brown DOB: 07/07/1993
Page 20 of 28
outbursts and change in mood, he explained how he could feel happy one minute
and angry the next.
H7: Presence-Possibility, Relevance=Moderate
In regards to personality disorder Mr Brown is being referred for an assessment for
anti-social personality disorder. Mr Jones experienced severe impulsivity in terms of
his emotions which lead to anger which is mainly associated with personality
disorders.
H8: Presence=Nil, Relevance=Low
Mr Brown denies any history of victimisation or trauma.
H9: Presence=Yes, Relevance=High
Mr Brown’ attitude towards his own personal violence does not leave much to be
desired. He constantly blames others for his own violent outbursts and when he
acknowledges these he condones his behaviour with some form of rationale.
H10: Presence=Yes, Relevance=High
He was exposed to substance misuse as his brothers were involved with the
substance abuse groups but unfortunately still felt he would continue using drugs
and held this negative attitude throughout the session.
Clinical Scale: Presence=Yes, Relevance=High
His education could play a role in his offending and anti-socialness as he never
succeeded academically. The negative experience at school could lead to violent
behaviours.
C1: Presence=Possible, Relevance=Moderate
Mr Brown’ insight is poor regarding his offence, drug abuse as well as the possibility
of having a mental illness. Regarding the assessment of mental illness Mr Brown
voices his opinion relating to the matter. He believes that he does not suffer from a
Peter Brown DOB: 07/07/1993
Page 20 of 28
mental condition. Evidence regarding his behaviour states otherwise as for those
who use substances and have a mental illness, and violence is more common.
C2: Presence=Yes, Relevance=High
The cause of his violent outbursts is due to the anger he feels, he has mentioned he
often feels angry, leading to violence.
C3: Presence=Yes, Relevance=High
Based on what he has described regarding his feelings and emotions there is a
potentiality for a mood disorder of some form. An assessment on mood disorder is
required with regards to both major mental and psychotic disorders. Anger links with
unipolar depression and is mostly associated with major depressive episodes.
C4: Presence=Yes, Relevance=High
Both mood and behaviour are an issue for Mr Brown and his mood fluctuates from
day to day. Struggles with emotions and anger is associated with offending.
R1: Presence=Yes, Relevance=High
Regarding alcohol and drug focus groups Mr Brown has no problem with attending
these but he does not find them useful, he still has the same belief. Regarding the
offence neither of these substances are related.
R2: Presence=Yes Relevance=High
Based on his intimate relationships, Mr Brown has no real community support.
R3: Presence=Yes, Relevance=High
His family relationships, friendships and intimate relationships all appear to be
unstable. He is not having any contact with his family hence, affecting his mental
health and anger.
R4: Presence=Yes, Relevance=High
Mr Brown will experience problems with receiving help in the future as he has a risk
of non-compliance with medication.
Peter Brown DOB: 07/07/1993
Page 21 of 28
who use substances and have a mental illness, and violence is more common.
C2: Presence=Yes, Relevance=High
The cause of his violent outbursts is due to the anger he feels, he has mentioned he
often feels angry, leading to violence.
C3: Presence=Yes, Relevance=High
Based on what he has described regarding his feelings and emotions there is a
potentiality for a mood disorder of some form. An assessment on mood disorder is
required with regards to both major mental and psychotic disorders. Anger links with
unipolar depression and is mostly associated with major depressive episodes.
C4: Presence=Yes, Relevance=High
Both mood and behaviour are an issue for Mr Brown and his mood fluctuates from
day to day. Struggles with emotions and anger is associated with offending.
R1: Presence=Yes, Relevance=High
Regarding alcohol and drug focus groups Mr Brown has no problem with attending
these but he does not find them useful, he still has the same belief. Regarding the
offence neither of these substances are related.
R2: Presence=Yes Relevance=High
Based on his intimate relationships, Mr Brown has no real community support.
R3: Presence=Yes, Relevance=High
His family relationships, friendships and intimate relationships all appear to be
unstable. He is not having any contact with his family hence, affecting his mental
health and anger.
R4: Presence=Yes, Relevance=High
Mr Brown will experience problems with receiving help in the future as he has a risk
of non-compliance with medication.
Peter Brown DOB: 07/07/1993
Page 21 of 28
R5: Presence=Yes, Relevance=High
It’s established that Mr Brown certainly struggles with coping more so than stress in
the inpatient setting. His coping strategy is his anger and he uses this to deal with an
event.
Peter Brown DOB: 07/07/1993
Page 22 of 28
It’s established that Mr Brown certainly struggles with coping more so than stress in
the inpatient setting. His coping strategy is his anger and he uses this to deal with an
event.
Peter Brown DOB: 07/07/1993
Page 22 of 28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
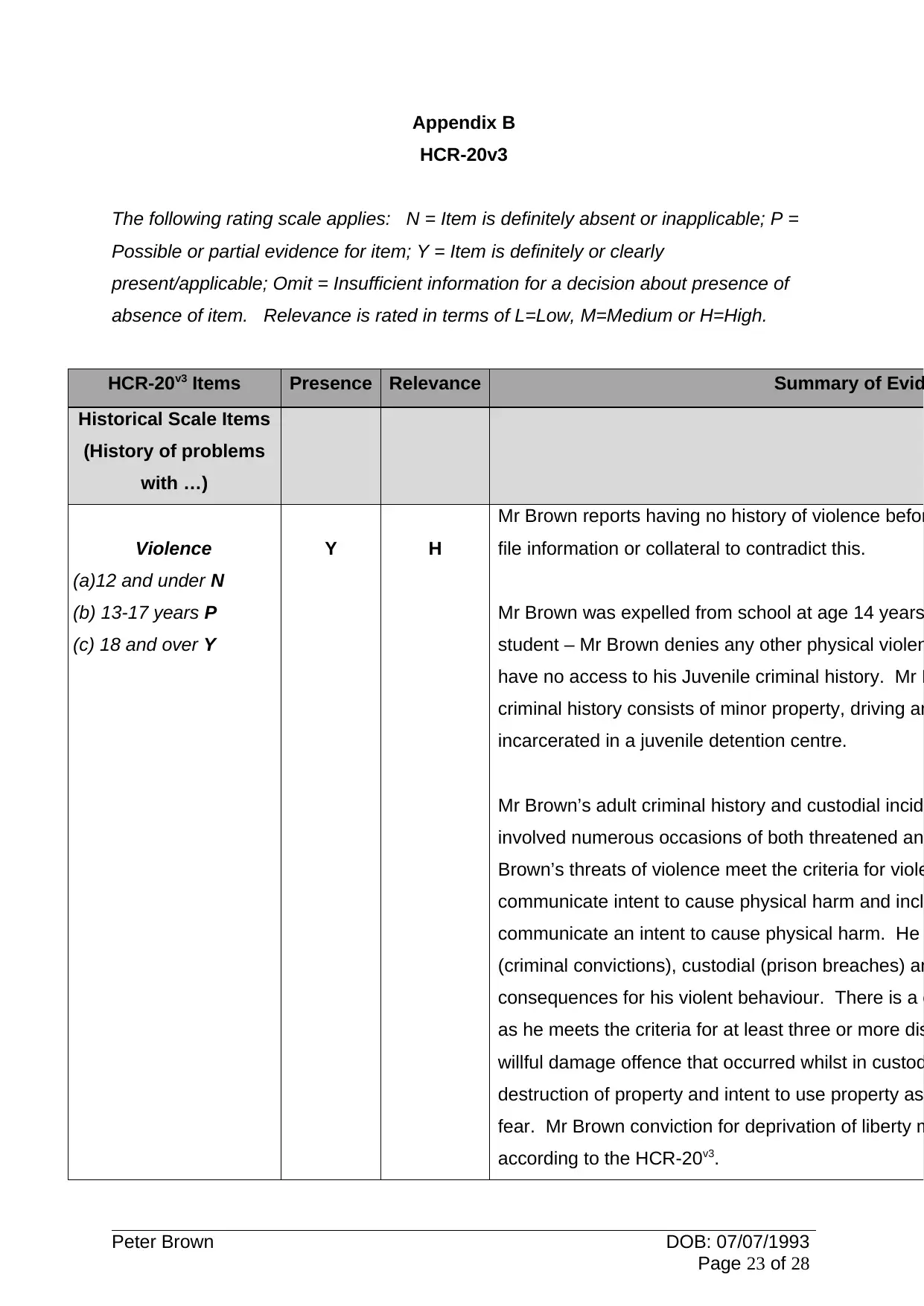
Appendix B
HCR-20v3
The following rating scale applies: N = Item is definitely absent or inapplicable; P =
Possible or partial evidence for item; Y = Item is definitely or clearly
present/applicable; Omit = Insufficient information for a decision about presence of
absence of item. Relevance is rated in terms of L=Low, M=Medium or H=High.
HCR-20v3 Items Presence Relevance Summary of Evid
Historical Scale Items
(History of problems
with …)
Violence
(a)12 and under N
(b) 13-17 years P
(c) 18 and over Y
Y H
Mr Brown reports having no history of violence befor
file information or collateral to contradict this.
Mr Brown was expelled from school at age 14 years
student – Mr Brown denies any other physical violen
have no access to his Juvenile criminal history. Mr B
criminal history consists of minor property, driving an
incarcerated in a juvenile detention centre.
Mr Brown’s adult criminal history and custodial incid
involved numerous occasions of both threatened an
Brown’s threats of violence meet the criteria for viole
communicate intent to cause physical harm and incl
communicate an intent to cause physical harm. He
(criminal convictions), custodial (prison breaches) an
consequences for his violent behaviour. There is a c
as he meets the criteria for at least three or more dis
willful damage offence that occurred whilst in custod
destruction of property and intent to use property as
fear. Mr Brown conviction for deprivation of liberty m
according to the HCR-20v3.
Peter Brown DOB: 07/07/1993
Page 23 of 28
HCR-20v3
The following rating scale applies: N = Item is definitely absent or inapplicable; P =
Possible or partial evidence for item; Y = Item is definitely or clearly
present/applicable; Omit = Insufficient information for a decision about presence of
absence of item. Relevance is rated in terms of L=Low, M=Medium or H=High.
HCR-20v3 Items Presence Relevance Summary of Evid
Historical Scale Items
(History of problems
with …)
Violence
(a)12 and under N
(b) 13-17 years P
(c) 18 and over Y
Y H
Mr Brown reports having no history of violence befor
file information or collateral to contradict this.
Mr Brown was expelled from school at age 14 years
student – Mr Brown denies any other physical violen
have no access to his Juvenile criminal history. Mr B
criminal history consists of minor property, driving an
incarcerated in a juvenile detention centre.
Mr Brown’s adult criminal history and custodial incid
involved numerous occasions of both threatened an
Brown’s threats of violence meet the criteria for viole
communicate intent to cause physical harm and incl
communicate an intent to cause physical harm. He
(criminal convictions), custodial (prison breaches) an
consequences for his violent behaviour. There is a c
as he meets the criteria for at least three or more dis
willful damage offence that occurred whilst in custod
destruction of property and intent to use property as
fear. Mr Brown conviction for deprivation of liberty m
according to the HCR-20v3.
Peter Brown DOB: 07/07/1993
Page 23 of 28
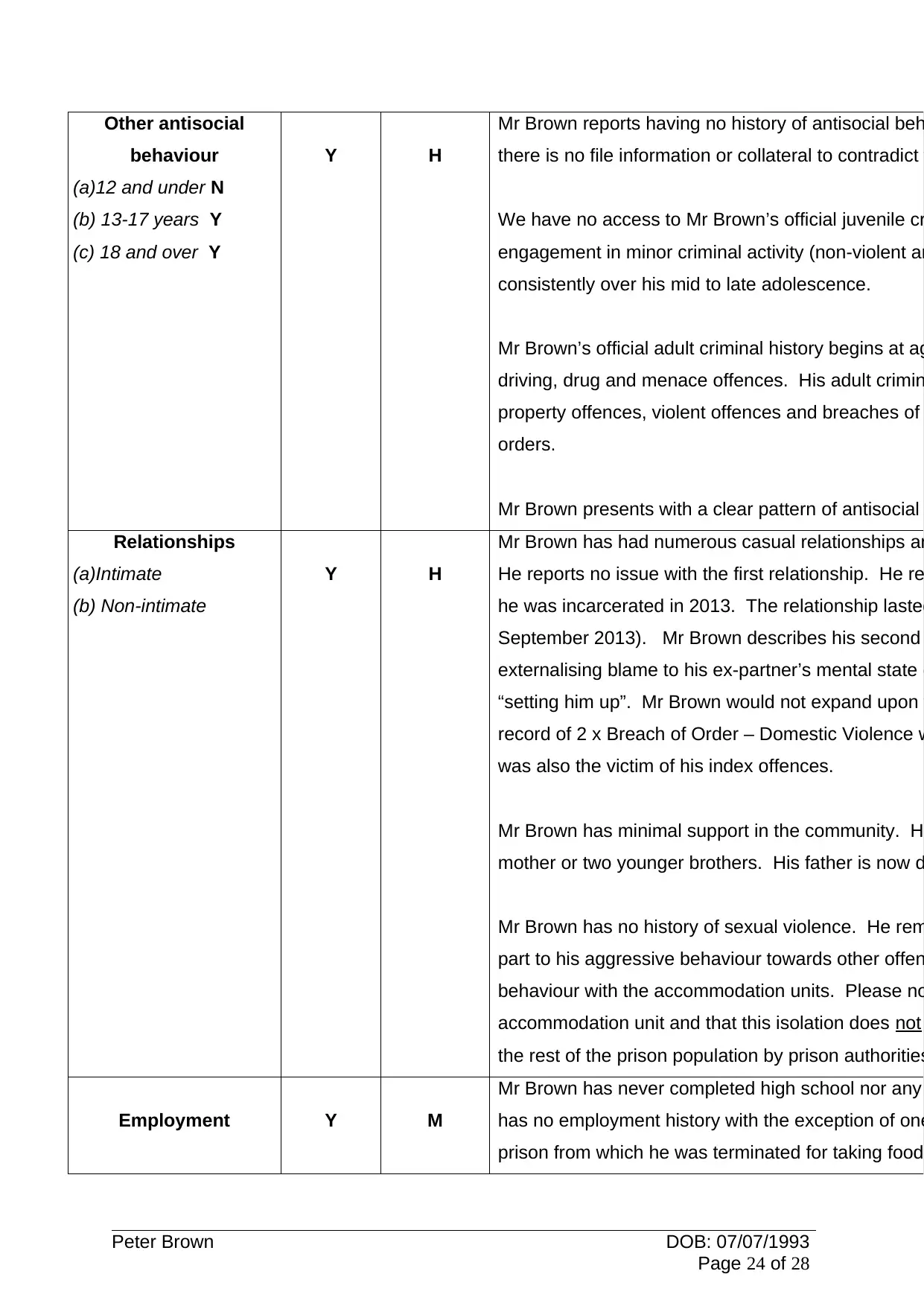
Other antisocial
behaviour
(a)12 and under N
(b) 13-17 years Y
(c) 18 and over Y
Y H
Mr Brown reports having no history of antisocial beh
there is no file information or collateral to contradict
We have no access to Mr Brown’s official juvenile cr
engagement in minor criminal activity (non-violent an
consistently over his mid to late adolescence.
Mr Brown’s official adult criminal history begins at ag
driving, drug and menace offences. His adult crimin
property offences, violent offences and breaches of
orders.
Mr Brown presents with a clear pattern of antisocial
Relationships
(a)Intimate
(b) Non-intimate
Y H
Mr Brown has had numerous casual relationships an
He reports no issue with the first relationship. He re
he was incarcerated in 2013. The relationship lasted
September 2013). Mr Brown describes his second
externalising blame to his ex-partner’s mental state (
“setting him up”. Mr Brown would not expand upon
record of 2 x Breach of Order – Domestic Violence w
was also the victim of his index offences.
Mr Brown has minimal support in the community. H
mother or two younger brothers. His father is now d
Mr Brown has no history of sexual violence. He rem
part to his aggressive behaviour towards other offen
behaviour with the accommodation units. Please no
accommodation unit and that this isolation does not
the rest of the prison population by prison authorities
Employment Y M
Mr Brown has never completed high school nor any
has no employment history with the exception of one
prison from which he was terminated for taking food
Peter Brown DOB: 07/07/1993
Page 24 of 28
behaviour
(a)12 and under N
(b) 13-17 years Y
(c) 18 and over Y
Y H
Mr Brown reports having no history of antisocial beh
there is no file information or collateral to contradict
We have no access to Mr Brown’s official juvenile cr
engagement in minor criminal activity (non-violent an
consistently over his mid to late adolescence.
Mr Brown’s official adult criminal history begins at ag
driving, drug and menace offences. His adult crimin
property offences, violent offences and breaches of
orders.
Mr Brown presents with a clear pattern of antisocial
Relationships
(a)Intimate
(b) Non-intimate
Y H
Mr Brown has had numerous casual relationships an
He reports no issue with the first relationship. He re
he was incarcerated in 2013. The relationship lasted
September 2013). Mr Brown describes his second
externalising blame to his ex-partner’s mental state (
“setting him up”. Mr Brown would not expand upon
record of 2 x Breach of Order – Domestic Violence w
was also the victim of his index offences.
Mr Brown has minimal support in the community. H
mother or two younger brothers. His father is now d
Mr Brown has no history of sexual violence. He rem
part to his aggressive behaviour towards other offen
behaviour with the accommodation units. Please no
accommodation unit and that this isolation does not
the rest of the prison population by prison authorities
Employment Y M
Mr Brown has never completed high school nor any
has no employment history with the exception of one
prison from which he was terminated for taking food
Peter Brown DOB: 07/07/1993
Page 24 of 28
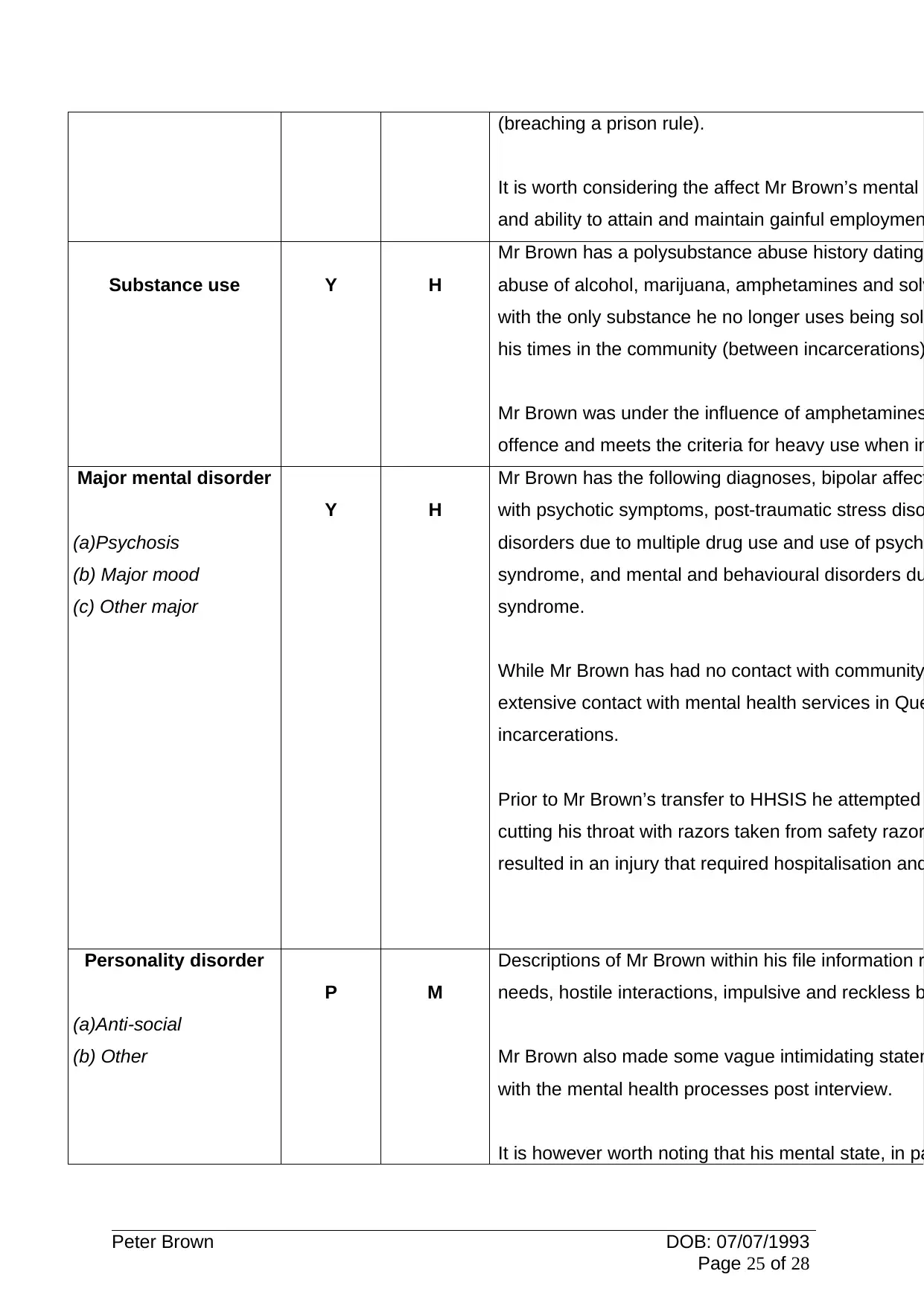
(breaching a prison rule).
It is worth considering the affect Mr Brown’s mental
and ability to attain and maintain gainful employmen
Substance use Y H
Mr Brown has a polysubstance abuse history dating
abuse of alcohol, marijuana, amphetamines and solv
with the only substance he no longer uses being sol
his times in the community (between incarcerations)
Mr Brown was under the influence of amphetamines
offence and meets the criteria for heavy use when in
Major mental disorder
(a)Psychosis
(b) Major mood
(c) Other major
Y H
Mr Brown has the following diagnoses, bipolar affect
with psychotic symptoms, post-traumatic stress diso
disorders due to multiple drug use and use of psych
syndrome, and mental and behavioural disorders du
syndrome.
While Mr Brown has had no contact with community
extensive contact with mental health services in Que
incarcerations.
Prior to Mr Brown’s transfer to HHSIS he attempted
cutting his throat with razors taken from safety razor
resulted in an injury that required hospitalisation and
Personality disorder
(a)Anti-social
(b) Other
P M
Descriptions of Mr Brown within his file information r
needs, hostile interactions, impulsive and reckless b
Mr Brown also made some vague intimidating statem
with the mental health processes post interview.
It is however worth noting that his mental state, in pa
Peter Brown DOB: 07/07/1993
Page 25 of 28
It is worth considering the affect Mr Brown’s mental
and ability to attain and maintain gainful employmen
Substance use Y H
Mr Brown has a polysubstance abuse history dating
abuse of alcohol, marijuana, amphetamines and solv
with the only substance he no longer uses being sol
his times in the community (between incarcerations)
Mr Brown was under the influence of amphetamines
offence and meets the criteria for heavy use when in
Major mental disorder
(a)Psychosis
(b) Major mood
(c) Other major
Y H
Mr Brown has the following diagnoses, bipolar affect
with psychotic symptoms, post-traumatic stress diso
disorders due to multiple drug use and use of psych
syndrome, and mental and behavioural disorders du
syndrome.
While Mr Brown has had no contact with community
extensive contact with mental health services in Que
incarcerations.
Prior to Mr Brown’s transfer to HHSIS he attempted
cutting his throat with razors taken from safety razor
resulted in an injury that required hospitalisation and
Personality disorder
(a)Anti-social
(b) Other
P M
Descriptions of Mr Brown within his file information r
needs, hostile interactions, impulsive and reckless b
Mr Brown also made some vague intimidating statem
with the mental health processes post interview.
It is however worth noting that his mental state, in pa
Peter Brown DOB: 07/07/1993
Page 25 of 28
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
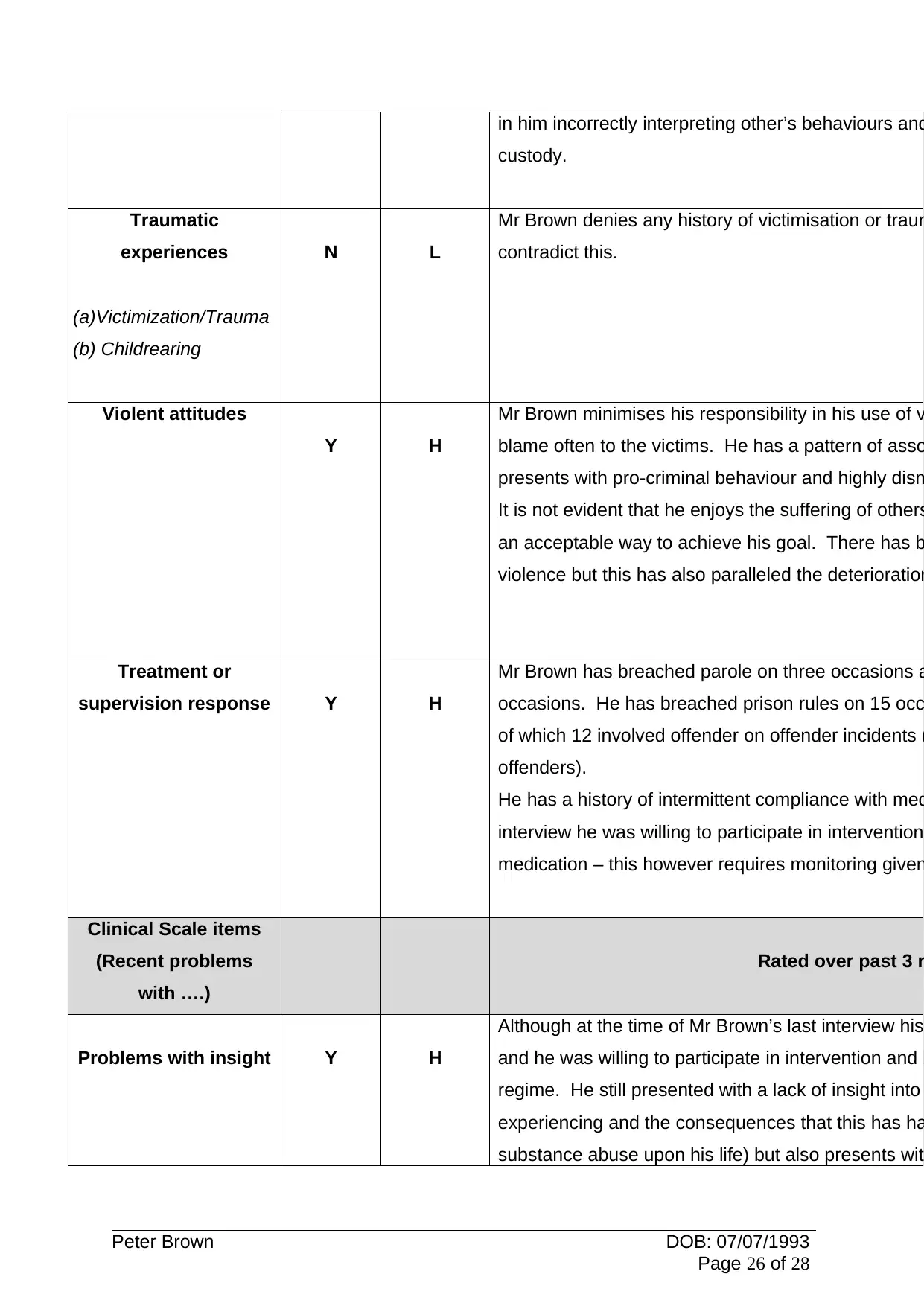
in him incorrectly interpreting other’s behaviours and
custody.
Traumatic
experiences
(a)Victimization/Trauma
(b) Childrearing
N L
Mr Brown denies any history of victimisation or traum
contradict this.
Violent attitudes
Y H
Mr Brown minimises his responsibility in his use of v
blame often to the victims. He has a pattern of asso
presents with pro-criminal behaviour and highly dism
It is not evident that he enjoys the suffering of others
an acceptable way to achieve his goal. There has b
violence but this has also paralleled the deterioration
Treatment or
supervision response Y H
Mr Brown has breached parole on three occasions a
occasions. He has breached prison rules on 15 occ
of which 12 involved offender on offender incidents (
offenders).
He has a history of intermittent compliance with med
interview he was willing to participate in intervention
medication – this however requires monitoring given
Clinical Scale items
(Recent problems
with ….)
Rated over past 3 m
Problems with insight Y H
Although at the time of Mr Brown’s last interview his
and he was willing to participate in intervention and b
regime. He still presented with a lack of insight into
experiencing and the consequences that this has ha
substance abuse upon his life) but also presents wit
Peter Brown DOB: 07/07/1993
Page 26 of 28
custody.
Traumatic
experiences
(a)Victimization/Trauma
(b) Childrearing
N L
Mr Brown denies any history of victimisation or traum
contradict this.
Violent attitudes
Y H
Mr Brown minimises his responsibility in his use of v
blame often to the victims. He has a pattern of asso
presents with pro-criminal behaviour and highly dism
It is not evident that he enjoys the suffering of others
an acceptable way to achieve his goal. There has b
violence but this has also paralleled the deterioration
Treatment or
supervision response Y H
Mr Brown has breached parole on three occasions a
occasions. He has breached prison rules on 15 occ
of which 12 involved offender on offender incidents (
offenders).
He has a history of intermittent compliance with med
interview he was willing to participate in intervention
medication – this however requires monitoring given
Clinical Scale items
(Recent problems
with ….)
Rated over past 3 m
Problems with insight Y H
Although at the time of Mr Brown’s last interview his
and he was willing to participate in intervention and b
regime. He still presented with a lack of insight into
experiencing and the consequences that this has ha
substance abuse upon his life) but also presents wit
Peter Brown DOB: 07/07/1993
Page 26 of 28
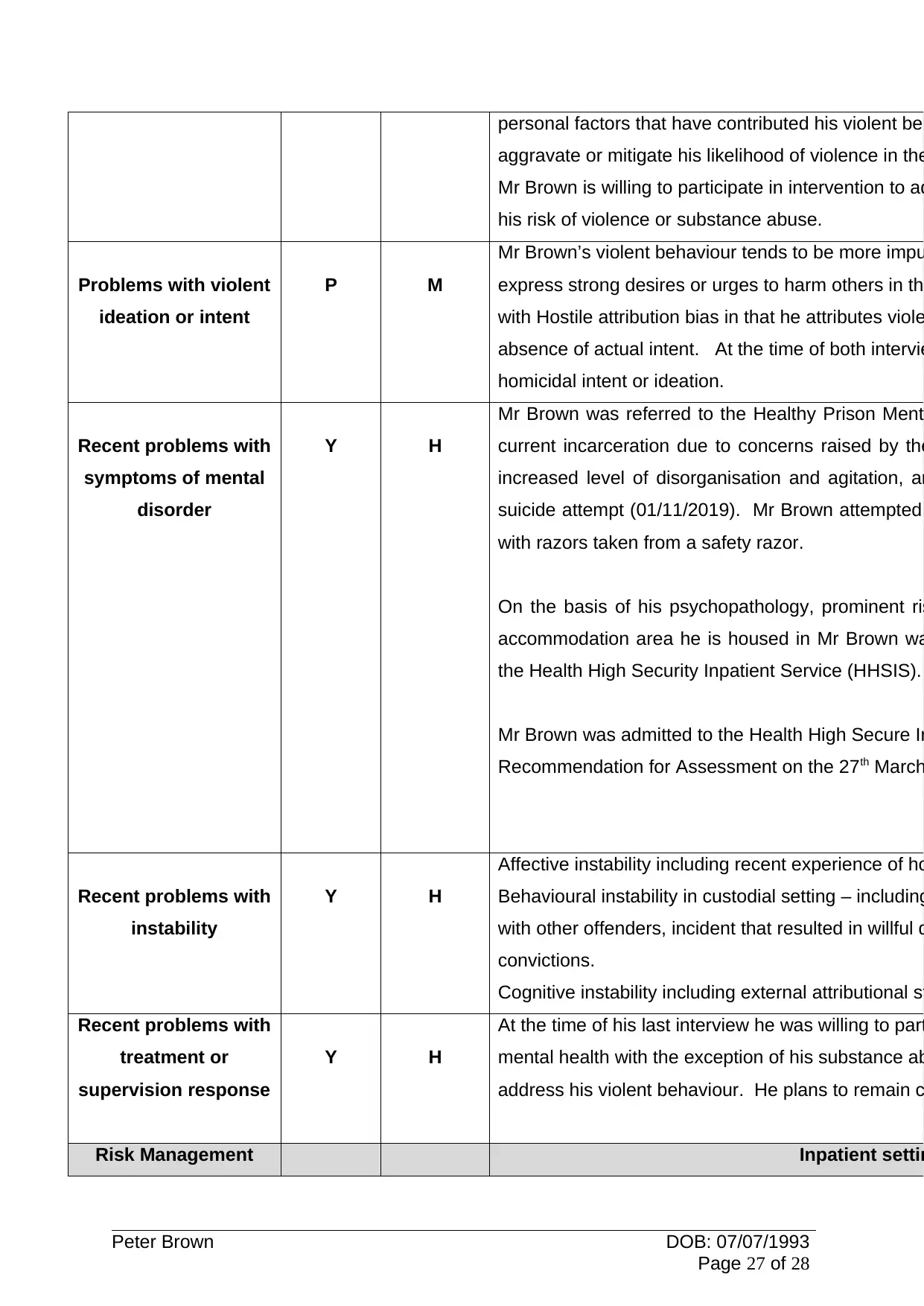
personal factors that have contributed his violent beh
aggravate or mitigate his likelihood of violence in the
Mr Brown is willing to participate in intervention to ad
his risk of violence or substance abuse.
Problems with violent
ideation or intent
P M
Mr Brown’s violent behaviour tends to be more impu
express strong desires or urges to harm others in th
with Hostile attribution bias in that he attributes viole
absence of actual intent. At the time of both intervie
homicidal intent or ideation.
Recent problems with
symptoms of mental
disorder
Y H
Mr Brown was referred to the Healthy Prison Ment
current incarceration due to concerns raised by the
increased level of disorganisation and agitation, an
suicide attempt (01/11/2019). Mr Brown attempted
with razors taken from a safety razor.
On the basis of his psychopathology, prominent ris
accommodation area he is housed in Mr Brown wa
the Health High Security Inpatient Service (HHSIS).
Mr Brown was admitted to the Health High Secure In
Recommendation for Assessment on the 27th March
Recent problems with
instability
Y H
Affective instability including recent experience of ho
Behavioural instability in custodial setting – including
with other offenders, incident that resulted in willful d
convictions.
Cognitive instability including external attributional st
Recent problems with
treatment or
supervision response
Y H
At the time of his last interview he was willing to part
mental health with the exception of his substance ab
address his violent behaviour. He plans to remain c
Risk Management Inpatient settin
Peter Brown DOB: 07/07/1993
Page 27 of 28
aggravate or mitigate his likelihood of violence in the
Mr Brown is willing to participate in intervention to ad
his risk of violence or substance abuse.
Problems with violent
ideation or intent
P M
Mr Brown’s violent behaviour tends to be more impu
express strong desires or urges to harm others in th
with Hostile attribution bias in that he attributes viole
absence of actual intent. At the time of both intervie
homicidal intent or ideation.
Recent problems with
symptoms of mental
disorder
Y H
Mr Brown was referred to the Healthy Prison Ment
current incarceration due to concerns raised by the
increased level of disorganisation and agitation, an
suicide attempt (01/11/2019). Mr Brown attempted
with razors taken from a safety razor.
On the basis of his psychopathology, prominent ris
accommodation area he is housed in Mr Brown wa
the Health High Security Inpatient Service (HHSIS).
Mr Brown was admitted to the Health High Secure In
Recommendation for Assessment on the 27th March
Recent problems with
instability
Y H
Affective instability including recent experience of ho
Behavioural instability in custodial setting – including
with other offenders, incident that resulted in willful d
convictions.
Cognitive instability including external attributional st
Recent problems with
treatment or
supervision response
Y H
At the time of his last interview he was willing to part
mental health with the exception of his substance ab
address his violent behaviour. He plans to remain c
Risk Management Inpatient settin
Peter Brown DOB: 07/07/1993
Page 27 of 28
1 out of 27
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.