Systematic Review and Meta-Analysis of Work Environment and Depressive Symptoms
VerifiedAdded on 2023/06/04
|14
|11489
|197
AI Summary
This study provides systematically graded evidence for possible associations between work environment factors and near-future development of depressive symptoms. The study finds that lack of decision latitude, job strain, and bullying are associated with increasing depressive symptoms over time. The review includes studies with a prospective design and is focused on the relationship between working conditions and development of symptoms of depression among the employees.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
R E S E A R C H A R T I C L E Open Access
A systematic review including meta-analysis
of work environment and depressive symptoms
Töres Theorell1,2*
, Anne Hammarström3
, Gunnar Aronsson4
, LilTräskman Bendz5
, Tom Grape6
, Christer Hogstedt7
,
Ina Marteinsdottir8
, Ingmar Skoog9 and Charlotte Hall10
Abstract
Background:Depressive symptoms are potential outcomes of poorly functioning work environments.Such
symptoms are frequent and cause considerable suffering for the employees as well as financial loss for the
Accordingly good prospective studies of psychosocial working conditions and depressive symptoms are va
Scientific reviews of such studies have pointed at methodological difficulties but still established a few job
Those reviews were published some years ago.There is need for an updated systematic review using the GRADE
system.In addition,gender related questions have been insufficiently reviewed.
Method: Inclusion criteria for the studies published 1990 to June 2013:1.European and English speaking countries.2.
Quantified results describing the relationship between exposure (psychosocial or physical/chemical) and o
(standardized questionnaire assessment of depressive symptoms or interview-based clinical depression).3.Prospective
or comparable case-control design with at least 100 participants.4.Assessments of exposure (working conditions) and
outcome at baseline and outcome (depressive symptoms) once again after follow-up 1-5 years later.5.Adjustment for
age and adjustment or stratification for gender.
Studies filling inclusion criteria were subjected to assessment of 1.) relevance and 2.) quality using predefi
criteria.Systematic review of the evidence was made using the GRADE system.When applicable,meta-analysis of
the magnitude of associations was made.Consistency of findings was examined for a number of possible
confounders and publication bias was discussed.
Results:Fifty-nine articles of high or medium high scientific quality were included.Moderately strong evidence
(grade three out of four) was found for job strain (high psychologicaldemands and low decision latitude),low
decision latitude and bullying having significant impact on development of depressive symptoms.Limited
evidence (grade two) was shown for psychologicaldemands,effort reward imbalance,low support,unfavorable
socialclimate,lack of work justice,conflicts,limited skilldiscretion,job insecurity and long working hours.There
was no differentialgender effect of adverse job conditions on depressive symptoms
Conclusion:There is substantialempiricalevidence that employees,both men and women,who report lack of
decision latitude,job strain and bullying,willexperience increasing depressive symptoms over time.These
conditions are amenable to organizationalinterventions.
Keywords:Depression,Work stress,Prevention,Ergonomic,Toxicology
* Correspondence:tores.theorell@stressforskning.su.se
1Stress Research Institute,Stockholm University,SE-106 91 Stockholm,
Sweden
2Department of Neuroscience,Karolinska Institutet,SE- 171 77 Stockholm,
Sweden
Fulllist of author information is available at the end of the article
© 2015 Theorellet al.This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0),which permits unrestricted use,distribution,and reproduction in any medium,
provided the originalwork is properly credited.The Creative Commons Public Domain Dedication waiver (http://
creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Theorell et al.BMC Public Health (2015) 15:738
DOI10.1186/s12889-015-1954-4
A systematic review including meta-analysis
of work environment and depressive symptoms
Töres Theorell1,2*
, Anne Hammarström3
, Gunnar Aronsson4
, LilTräskman Bendz5
, Tom Grape6
, Christer Hogstedt7
,
Ina Marteinsdottir8
, Ingmar Skoog9 and Charlotte Hall10
Abstract
Background:Depressive symptoms are potential outcomes of poorly functioning work environments.Such
symptoms are frequent and cause considerable suffering for the employees as well as financial loss for the
Accordingly good prospective studies of psychosocial working conditions and depressive symptoms are va
Scientific reviews of such studies have pointed at methodological difficulties but still established a few job
Those reviews were published some years ago.There is need for an updated systematic review using the GRADE
system.In addition,gender related questions have been insufficiently reviewed.
Method: Inclusion criteria for the studies published 1990 to June 2013:1.European and English speaking countries.2.
Quantified results describing the relationship between exposure (psychosocial or physical/chemical) and o
(standardized questionnaire assessment of depressive symptoms or interview-based clinical depression).3.Prospective
or comparable case-control design with at least 100 participants.4.Assessments of exposure (working conditions) and
outcome at baseline and outcome (depressive symptoms) once again after follow-up 1-5 years later.5.Adjustment for
age and adjustment or stratification for gender.
Studies filling inclusion criteria were subjected to assessment of 1.) relevance and 2.) quality using predefi
criteria.Systematic review of the evidence was made using the GRADE system.When applicable,meta-analysis of
the magnitude of associations was made.Consistency of findings was examined for a number of possible
confounders and publication bias was discussed.
Results:Fifty-nine articles of high or medium high scientific quality were included.Moderately strong evidence
(grade three out of four) was found for job strain (high psychologicaldemands and low decision latitude),low
decision latitude and bullying having significant impact on development of depressive symptoms.Limited
evidence (grade two) was shown for psychologicaldemands,effort reward imbalance,low support,unfavorable
socialclimate,lack of work justice,conflicts,limited skilldiscretion,job insecurity and long working hours.There
was no differentialgender effect of adverse job conditions on depressive symptoms
Conclusion:There is substantialempiricalevidence that employees,both men and women,who report lack of
decision latitude,job strain and bullying,willexperience increasing depressive symptoms over time.These
conditions are amenable to organizationalinterventions.
Keywords:Depression,Work stress,Prevention,Ergonomic,Toxicology
* Correspondence:tores.theorell@stressforskning.su.se
1Stress Research Institute,Stockholm University,SE-106 91 Stockholm,
Sweden
2Department of Neuroscience,Karolinska Institutet,SE- 171 77 Stockholm,
Sweden
Fulllist of author information is available at the end of the article
© 2015 Theorellet al.This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0),which permits unrestricted use,distribution,and reproduction in any medium,
provided the originalwork is properly credited.The Creative Commons Public Domain Dedication waiver (http://
creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Theorell et al.BMC Public Health (2015) 15:738
DOI10.1186/s12889-015-1954-4
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Background
Depressive symptomsare potentialoutcomesof poorly
functioning work environments.Such symptoms are fre-
quentand may cause considerable suffering for the em-
ployeesthemselvesas well as financialloss for the
employers.Accordingly good prospective studies ofpsy-
chosocial working conditions and depressive symptoms are
valuable.
Several reviews including prospectivestudies of
psychosocialfactorsat work in relation to depression
have been published.Bonde [1]concluded thatthere
were consistent findings that perception ofadverse psy-
chosocialfactors in the workplace is related to an ele-
vated risk ofsubsequent depressive symptoms or major
depressive episode butalso thatmethodologicallimita-
tions preclude causalinference.Netterström etal. [2]
made a similar conclusion butpointed outthatstudies
are needed thatassess in more detailthe duration and
intensity ofexposure necessary fordeveloping depres-
sion.The conclusions in a review by Siegristfrom the
same year [3]were similar.Also, Michie and Williams
[4] concluded that” many ofthe work related variables
associated with high levels of psychological ill health,are
potentially amenable to change which has been shown
in intervention studies thathave successfully improved
psychologicalhealth and reduced sickness absence”.A
review ofpsychosocialand health effects ofworkplace
reorganization by Egan etal. [5] concluded that” some
organizational-levelparticipationinterventionsmay
benefitemployee health,as predicted by the demand-
control model”.However,severalother psychosocial
exposures should be examined more in detail.
Most of the work environment reviews published so far
have notbeen confined to depression only - they have
included for instance stress related disorders, psychologic-
ally related sick leave and suicide or combinations [4, 6–8]
as outcomes,and it has sometimes been difficult to disen-
tanglethem.Studied workenvironmentfactorshave
mostly been limited to psychosocialfactors although two
reviews have included physical/chemical/ergonomic expo-
sures as well.The conclusion from them [4,7] was that
the evidence for physical/chemical/ergonomic exposures
is limited and inconclusive.Nieuwenhuijsen et al.[8] pub-
lished a review of the effects of the psychosocial environ-
ment on risk of stress-relateddisorders(SRDs) and
concluded that there is” strong evidence that high job de-
mands,low job control, low co-workersupport,low
supervisor support,low proceduraljustice and a high ef-
fort- reward imbalance predicted the incidence of SRDs”.
In summary,the evidence aboutthe negative impact
of certain work environments for depressive symptoms
is accumulating butso far there hasbeen no review
taking the entire spectrum ofadverse working condi-
tions into accountand at the same time focusing on
depressiveconditions/symptomsas outcome.Most of
the reviews have used multiple kinds ofmentalhealth
outcomes.However,depression is the mostwidely re-
ported outcome in the field ofmentalhealth in epi-
demiologicalresearch.Depressivesymptomsare well
understood in psychiatry which has resulted in a large
numberof studies.Accordinglythis outcomeshould
provide a good basis for a focused systematic review.As
far as the authors know there is no published study that
has used the internationalGRADE system [9] for evalu-
ating the evidence in thisfield.In addition there is a
need for a systematic review utilizing the mostrecent
developments in search technology.
An important aspect ofthe systematic review process
is to systematically and transparently assess the scientific
evidence.We have chosen to use the internationally rec-
ognized GRADE-system forscientific evaluation.The
GRADE system usesfour levelsof evidence,namely
High,Moderate,Limited and Very Limited.We are well
aware that the system has been developed primarily for
assessing interventions in a health care context,but the
system has been adapted to epidemiologicalevaluation.
Beside the transparency,an advantageis that the
GRADE system [9]- a system often applied in reviews
conducted within the Cochrane Collaboration -is in-
creasingly used internationally e.g.,by the World Health
Organization.Hence results from systematic reviews can
be more easily compared.
Time has elapsed since mostof the previous reviews
were published and new studies are published continu-
ously.The most relevant reviews were published in 2008.
They pointed atseveralmethodologicalshortcomings,
and it is not known whether researchers more recently
have tried to address the identified scientific problems.In
particular,the reviews have pointed at the paucity of stud-
ies on physical/chemical/ergonomic exposures.
A topic that has not been addressed sufficiently in pre-
vious reviewsis genderin the relationship between
working conditions and the developmentof depressive
symptoms.Are the associationsdifferentfor men and
women?
Aim of the study
The aim of this studywas to providesystematically
graded evidence for possible associations between work
environment factors and near-future development of de-
pressive symptoms
Methods
The present review was based upon studies with a pro-
spectivedesignand is focusedon the relationship
between working conditions and development ofsymp-
toms of depression among theemployees..We con-
ducted and funded thissystematicreview within the
Theorell et al.BMC Public Health (2015) 15:738 Page 2 of 14
Depressive symptomsare potentialoutcomesof poorly
functioning work environments.Such symptoms are fre-
quentand may cause considerable suffering for the em-
ployeesthemselvesas well as financialloss for the
employers.Accordingly good prospective studies ofpsy-
chosocial working conditions and depressive symptoms are
valuable.
Several reviews including prospectivestudies of
psychosocialfactorsat work in relation to depression
have been published.Bonde [1]concluded thatthere
were consistent findings that perception ofadverse psy-
chosocialfactors in the workplace is related to an ele-
vated risk ofsubsequent depressive symptoms or major
depressive episode butalso thatmethodologicallimita-
tions preclude causalinference.Netterström etal. [2]
made a similar conclusion butpointed outthatstudies
are needed thatassess in more detailthe duration and
intensity ofexposure necessary fordeveloping depres-
sion.The conclusions in a review by Siegristfrom the
same year [3]were similar.Also, Michie and Williams
[4] concluded that” many ofthe work related variables
associated with high levels of psychological ill health,are
potentially amenable to change which has been shown
in intervention studies thathave successfully improved
psychologicalhealth and reduced sickness absence”.A
review ofpsychosocialand health effects ofworkplace
reorganization by Egan etal. [5] concluded that” some
organizational-levelparticipationinterventionsmay
benefitemployee health,as predicted by the demand-
control model”.However,severalother psychosocial
exposures should be examined more in detail.
Most of the work environment reviews published so far
have notbeen confined to depression only - they have
included for instance stress related disorders, psychologic-
ally related sick leave and suicide or combinations [4, 6–8]
as outcomes,and it has sometimes been difficult to disen-
tanglethem.Studied workenvironmentfactorshave
mostly been limited to psychosocialfactors although two
reviews have included physical/chemical/ergonomic expo-
sures as well.The conclusion from them [4,7] was that
the evidence for physical/chemical/ergonomic exposures
is limited and inconclusive.Nieuwenhuijsen et al.[8] pub-
lished a review of the effects of the psychosocial environ-
ment on risk of stress-relateddisorders(SRDs) and
concluded that there is” strong evidence that high job de-
mands,low job control, low co-workersupport,low
supervisor support,low proceduraljustice and a high ef-
fort- reward imbalance predicted the incidence of SRDs”.
In summary,the evidence aboutthe negative impact
of certain work environments for depressive symptoms
is accumulating butso far there hasbeen no review
taking the entire spectrum ofadverse working condi-
tions into accountand at the same time focusing on
depressiveconditions/symptomsas outcome.Most of
the reviews have used multiple kinds ofmentalhealth
outcomes.However,depression is the mostwidely re-
ported outcome in the field ofmentalhealth in epi-
demiologicalresearch.Depressivesymptomsare well
understood in psychiatry which has resulted in a large
numberof studies.Accordinglythis outcomeshould
provide a good basis for a focused systematic review.As
far as the authors know there is no published study that
has used the internationalGRADE system [9] for evalu-
ating the evidence in thisfield.In addition there is a
need for a systematic review utilizing the mostrecent
developments in search technology.
An important aspect ofthe systematic review process
is to systematically and transparently assess the scientific
evidence.We have chosen to use the internationally rec-
ognized GRADE-system forscientific evaluation.The
GRADE system usesfour levelsof evidence,namely
High,Moderate,Limited and Very Limited.We are well
aware that the system has been developed primarily for
assessing interventions in a health care context,but the
system has been adapted to epidemiologicalevaluation.
Beside the transparency,an advantageis that the
GRADE system [9]- a system often applied in reviews
conducted within the Cochrane Collaboration -is in-
creasingly used internationally e.g.,by the World Health
Organization.Hence results from systematic reviews can
be more easily compared.
Time has elapsed since mostof the previous reviews
were published and new studies are published continu-
ously.The most relevant reviews were published in 2008.
They pointed atseveralmethodologicalshortcomings,
and it is not known whether researchers more recently
have tried to address the identified scientific problems.In
particular,the reviews have pointed at the paucity of stud-
ies on physical/chemical/ergonomic exposures.
A topic that has not been addressed sufficiently in pre-
vious reviewsis genderin the relationship between
working conditions and the developmentof depressive
symptoms.Are the associationsdifferentfor men and
women?
Aim of the study
The aim of this studywas to providesystematically
graded evidence for possible associations between work
environment factors and near-future development of de-
pressive symptoms
Methods
The present review was based upon studies with a pro-
spectivedesignand is focusedon the relationship
between working conditions and development ofsymp-
toms of depression among theemployees..We con-
ducted and funded thissystematicreview within the
Theorell et al.BMC Public Health (2015) 15:738 Page 2 of 14
framework for the Swedish Council on Health and Tech-
nology Assessment,a public agency with the charge of
providing impartial and scientifically reliable information
to decision makers and health care providers [10].
Search strategy
Systematic literature search was performed in the following
data bases:PubMed,Embase,Psycinfo,Arbline (Swedish
database),Cochrane library and NIOSHTIC-2.A combin-
ation of controlled search words (e.g., MeSH) and free- text
words was used.The search strategy for the outcome was
performed formesh terms (‘Depression’and ‘Depressive
Disorders’) and as free search in title and abstract (depress*
and dysthym*).The whole search strategy is available at
http://www.sbu.se/upload/Publikationer/Content0/1/223E/
Inclusion%20criteria_occupational%20exposure_depression
_burnout.pdf.We only accepted asarticlesin scientific
journals with independent reviews.
Inclusion criteria
The inclusion criteria for studies were:
1. The study should have examined the importance of
the work environment for depressive symptoms.
Our review was not confined to any specific kind of
work environment factors.Physical/chemical/
ergonomic exposures as well as psychosocial factors
were screened.
2. The study should be relevant for Swedish conditions
and focused on people at work.Work environments
in Europe,North America,Australia and New
Zealand were included.
3. In the study symptoms of depression should have
been analyzed.These should have have been
certified through diagnostic investigation or with
established scales.We argued that not only
diagnosed major depression,but also milder states
with depressive symptoms are relevant since
depressive feelings give rise to suffering,increase the
risk of long term sick leave and cause productivity
decline and quality loss in work places [11].Thus,
our review included both studies with standardized
clinical interviews regarding diagnosed depression
and studies based upon rating scales on depressive
symptoms.As diagnosed depression is also to a large
extent based on symptoms we decided that the most
accurate naming of the outcome of our review was
depressive symptoms.A few studies were based
upon either sick leave data or registered anti-
depression medication as outcome but these studies
are not included in this review.
4. A minimum of 100 persons should have been
included in the exposed group and the results were
controlled for at least age and gender.
5. The study should have been published between the
years 1990 and (June) 2013 and written in English.
6. Prospective or comparable case-control design. Only
prospective cohort, case control (with design equivalen
to prospective) and randomized intervention studies
with at least 100 participants were included. By case
control studies with “design equivalent to prospective”
we are referring to studies with strict definition of cases
recruited in a representative way in the same
population as the control group.
Assessments ofexposure should have been made be-
fore disease onset.
Doubletswere systematically identified and only the
most relevant publication in a doublet was included.
Analyses of relevance and quality
Abstractscreening and full-textassessmentwere con-
ducted by a specialistin occupationalmedicine and a
psychiatrist.
After that,the scientific experts started their examin-
ation.Pre-set evaluation forms were used.The experts
judged relevance and quality of the studies on the basis
of the relevance/quality criteria,their experience as re-
searchers and their knowledge of the field.Accordingly
they were recruited amongSwedish academichigh
ranking specialists in fields of relevance for the process,
namely psychiatry (three),epidemiology and stress re-
search (three),work psychology (one) and family prac-
tice (one).This group was divided into pairs with as
widely differing specialty in the pair as possible.In the
following process,the articles remaining in the process
were randomly assigned to the four pairs (with avoid-
ance of author bias).Concordance in judgments of rele-
vance and quality was trained.After the training
session,each member ofthe pair did the assessments
separately,and then discordances were discussed within
the pair.If disagreementremained anotherpair was
asked to make an independentjudgment.If thatdeci-
sion was in disagreement with the first group,we made
the decision in the whole group.
In the firstexpertphase,the group judged relevance.
Relevance criteria are presented in http://www.sbu.se/up-
load/Publikationer/Content0/1/223E/Inclusion%20criteria
_occupational%20exposure_depression_burnout.pdf.
Secondly,we performed a quality assessment.Three
levelsof quality rating were used,(low, medium high
and high quality)and in the finalgrading process only
those with medium high and high quality were accepted.
Accordinglythe importantdividing linewas between
poor and medium high quality whereas the distinction
between medium high and high was less crucial.Studies
on the borderline between low and medium high quality
were accordingly re-examined by the whole group.A list
Theorell et al.BMC Public Health (2015) 15:738 Page 3 of 14
nology Assessment,a public agency with the charge of
providing impartial and scientifically reliable information
to decision makers and health care providers [10].
Search strategy
Systematic literature search was performed in the following
data bases:PubMed,Embase,Psycinfo,Arbline (Swedish
database),Cochrane library and NIOSHTIC-2.A combin-
ation of controlled search words (e.g., MeSH) and free- text
words was used.The search strategy for the outcome was
performed formesh terms (‘Depression’and ‘Depressive
Disorders’) and as free search in title and abstract (depress*
and dysthym*).The whole search strategy is available at
http://www.sbu.se/upload/Publikationer/Content0/1/223E/
Inclusion%20criteria_occupational%20exposure_depression
_burnout.pdf.We only accepted asarticlesin scientific
journals with independent reviews.
Inclusion criteria
The inclusion criteria for studies were:
1. The study should have examined the importance of
the work environment for depressive symptoms.
Our review was not confined to any specific kind of
work environment factors.Physical/chemical/
ergonomic exposures as well as psychosocial factors
were screened.
2. The study should be relevant for Swedish conditions
and focused on people at work.Work environments
in Europe,North America,Australia and New
Zealand were included.
3. In the study symptoms of depression should have
been analyzed.These should have have been
certified through diagnostic investigation or with
established scales.We argued that not only
diagnosed major depression,but also milder states
with depressive symptoms are relevant since
depressive feelings give rise to suffering,increase the
risk of long term sick leave and cause productivity
decline and quality loss in work places [11].Thus,
our review included both studies with standardized
clinical interviews regarding diagnosed depression
and studies based upon rating scales on depressive
symptoms.As diagnosed depression is also to a large
extent based on symptoms we decided that the most
accurate naming of the outcome of our review was
depressive symptoms.A few studies were based
upon either sick leave data or registered anti-
depression medication as outcome but these studies
are not included in this review.
4. A minimum of 100 persons should have been
included in the exposed group and the results were
controlled for at least age and gender.
5. The study should have been published between the
years 1990 and (June) 2013 and written in English.
6. Prospective or comparable case-control design. Only
prospective cohort, case control (with design equivalen
to prospective) and randomized intervention studies
with at least 100 participants were included. By case
control studies with “design equivalent to prospective”
we are referring to studies with strict definition of cases
recruited in a representative way in the same
population as the control group.
Assessments ofexposure should have been made be-
fore disease onset.
Doubletswere systematically identified and only the
most relevant publication in a doublet was included.
Analyses of relevance and quality
Abstractscreening and full-textassessmentwere con-
ducted by a specialistin occupationalmedicine and a
psychiatrist.
After that,the scientific experts started their examin-
ation.Pre-set evaluation forms were used.The experts
judged relevance and quality of the studies on the basis
of the relevance/quality criteria,their experience as re-
searchers and their knowledge of the field.Accordingly
they were recruited amongSwedish academichigh
ranking specialists in fields of relevance for the process,
namely psychiatry (three),epidemiology and stress re-
search (three),work psychology (one) and family prac-
tice (one).This group was divided into pairs with as
widely differing specialty in the pair as possible.In the
following process,the articles remaining in the process
were randomly assigned to the four pairs (with avoid-
ance of author bias).Concordance in judgments of rele-
vance and quality was trained.After the training
session,each member ofthe pair did the assessments
separately,and then discordances were discussed within
the pair.If disagreementremained anotherpair was
asked to make an independentjudgment.If thatdeci-
sion was in disagreement with the first group,we made
the decision in the whole group.
In the firstexpertphase,the group judged relevance.
Relevance criteria are presented in http://www.sbu.se/up-
load/Publikationer/Content0/1/223E/Inclusion%20criteria
_occupational%20exposure_depression_burnout.pdf.
Secondly,we performed a quality assessment.Three
levelsof quality rating were used,(low, medium high
and high quality)and in the finalgrading process only
those with medium high and high quality were accepted.
Accordinglythe importantdividing linewas between
poor and medium high quality whereas the distinction
between medium high and high was less crucial.Studies
on the borderline between low and medium high quality
were accordingly re-examined by the whole group.A list
Theorell et al.BMC Public Health (2015) 15:738 Page 3 of 14
of relevant articles meeting the inclusion criteria judged
to be of low quality is available at http://www.sbu.se/up-
load/Publikationer/Content0/1/223E/Inclusion%20cri-
teria_occupational%20exposure_depression_burnout.pdf
The following aspects of quality were considered:
1.) Representativeness of study sample.
Representativeness and ways of defining and
recruiting the sample as well as attrition in different
steps were considered in the quality rating.
Statistical considerations and an insightful discussion
of possible consequences of a possible systematic
drop-out for findings were required in case of
marked drop-out problems.
2.) Confounding.Age and at least some aspect of
socioeconomic conditions should have been
considered.Gender specific analyses were preferred
but when such analyses were not available,
adjustment for gender was required.Life habits such
as smoking habits and alcohol consumption were
not taken into account as confounders in our
review.
3.) Prospective data collection. All results of the studies
included in this review (apart from case-control
studies) are based upon assessments of exposure and
depressive symptoms in the beginning and of the
depressive symptoms again at least one year later. In
the calculations of associations a design with either
exclusion of subjects with depressive symptoms at
baseline or adjustment for baseline level of depressive
symptoms was required. Qualified statistics and
thorough discussion of longitudinal data rendered
higher quality ratings.
4.) For both exposure and outcome assessment,
psychometrically standardized and validated
methods were required.Well established methods
enable comparison across studies and therefore
contributed to higher quality rating.
5.) Designs that enable the analysis of a dose response
relationship contributed to a high quality rating.For
instance,in a few studies the work environment was
assessed in two or three subsequent waves and the
development of depressive symptoms followed up
after the last assessment.Exposure to given work
environment factor on one,two or three occasions
could be regarded as a progressive duration of
exposure and was regarded as equivalent of a dose-
response analysis.
Even between studiesof specific work environment
factors there were differences with regard to operationa-
lization ofexposure.Examples are job strain (combin-
ation ofhigh psychologicaldemands and low decision
latitude)and effortreward imbalance (combination of
high effortand poor reward).Since the overallaim of
the present study was to grade total evidence,not to as-
sess magnitude of associations,and since it was impos-
sible to re-constructoperationalizations in such a way
that they would match one another we decided to use
the definitions presented by the authors themselves and
to mostly abstain from assessment of overall magnitude
of the different relationships.
The final list of studiesjudged to be of high or
medium high quality is listed in Appendix.
GRADE procedure
An importantaspectof the systematic review process
was to systematically and transparently assess the scien-
tific evidence.According to the GRADE instructions
explicitconsideration should be given to each ofthe
GRADE criteria forassessing the quality ofevidence
(risk of bias/study limitations,directness,consistency of
results,precision,publication bias,magnitude of the ef-
fect,dose-response gradient,influence of residual plaus-
ible confounding and bias “antagonistic bias”) although
different terminology may be used.For level4 (=High),
randomized trials are required and there were no such
published relevantstudies in our search.For observa-
tional studies of the kind included in the present review,
the highestpossible grade isModerate = 3 ifthere is
sufficient reason for an upgrading from the normal level
for such studies of 2 (=Limited).Level 1 (=Very limited)
corresponds to evidence based on case reports and case
series or on reports downgraded evidence from observa-
tional studies.
We allowed for upgradingthe scientificevidence
when there wasstrong coherence ofresultsbetween
studies - according to the most recent guidelines [12].
Accordingly when there were many published observa-
tional studiesof medium high or high qualitywith
homogenousresults(almostall pointing in the same
direction although all findings may not have been statis-
tically significant)the evidence was graded on level3
(two exposures,high decision latitude as protective and
job strain as negative exposure,see below).Level3 can
also be used according to the GRADE system even when
there are relatively few studies ifthere are unanimous
findings with high odds ratios (above 2.0). This occurred
for one exposure – bullying (see below).
Meta-analyses/Forest plots
In the studies results were reported as calculations of
association,e.g.,expressed as odds ratios,from mul-
tiple logistic regression,multivariatecorrelationsor
multiple linear regression coefficients.Whenever pos-
sible,the results were transformed into multiple logis-
tic regression odds ratios.Forestplots were used for
visual interpretation.To assist in illustrating the
Theorell et al.BMC Public Health (2015) 15:738 Page 4 of 14
to be of low quality is available at http://www.sbu.se/up-
load/Publikationer/Content0/1/223E/Inclusion%20cri-
teria_occupational%20exposure_depression_burnout.pdf
The following aspects of quality were considered:
1.) Representativeness of study sample.
Representativeness and ways of defining and
recruiting the sample as well as attrition in different
steps were considered in the quality rating.
Statistical considerations and an insightful discussion
of possible consequences of a possible systematic
drop-out for findings were required in case of
marked drop-out problems.
2.) Confounding.Age and at least some aspect of
socioeconomic conditions should have been
considered.Gender specific analyses were preferred
but when such analyses were not available,
adjustment for gender was required.Life habits such
as smoking habits and alcohol consumption were
not taken into account as confounders in our
review.
3.) Prospective data collection. All results of the studies
included in this review (apart from case-control
studies) are based upon assessments of exposure and
depressive symptoms in the beginning and of the
depressive symptoms again at least one year later. In
the calculations of associations a design with either
exclusion of subjects with depressive symptoms at
baseline or adjustment for baseline level of depressive
symptoms was required. Qualified statistics and
thorough discussion of longitudinal data rendered
higher quality ratings.
4.) For both exposure and outcome assessment,
psychometrically standardized and validated
methods were required.Well established methods
enable comparison across studies and therefore
contributed to higher quality rating.
5.) Designs that enable the analysis of a dose response
relationship contributed to a high quality rating.For
instance,in a few studies the work environment was
assessed in two or three subsequent waves and the
development of depressive symptoms followed up
after the last assessment.Exposure to given work
environment factor on one,two or three occasions
could be regarded as a progressive duration of
exposure and was regarded as equivalent of a dose-
response analysis.
Even between studiesof specific work environment
factors there were differences with regard to operationa-
lization ofexposure.Examples are job strain (combin-
ation ofhigh psychologicaldemands and low decision
latitude)and effortreward imbalance (combination of
high effortand poor reward).Since the overallaim of
the present study was to grade total evidence,not to as-
sess magnitude of associations,and since it was impos-
sible to re-constructoperationalizations in such a way
that they would match one another we decided to use
the definitions presented by the authors themselves and
to mostly abstain from assessment of overall magnitude
of the different relationships.
The final list of studiesjudged to be of high or
medium high quality is listed in Appendix.
GRADE procedure
An importantaspectof the systematic review process
was to systematically and transparently assess the scien-
tific evidence.According to the GRADE instructions
explicitconsideration should be given to each ofthe
GRADE criteria forassessing the quality ofevidence
(risk of bias/study limitations,directness,consistency of
results,precision,publication bias,magnitude of the ef-
fect,dose-response gradient,influence of residual plaus-
ible confounding and bias “antagonistic bias”) although
different terminology may be used.For level4 (=High),
randomized trials are required and there were no such
published relevantstudies in our search.For observa-
tional studies of the kind included in the present review,
the highestpossible grade isModerate = 3 ifthere is
sufficient reason for an upgrading from the normal level
for such studies of 2 (=Limited).Level 1 (=Very limited)
corresponds to evidence based on case reports and case
series or on reports downgraded evidence from observa-
tional studies.
We allowed for upgradingthe scientificevidence
when there wasstrong coherence ofresultsbetween
studies - according to the most recent guidelines [12].
Accordingly when there were many published observa-
tional studiesof medium high or high qualitywith
homogenousresults(almostall pointing in the same
direction although all findings may not have been statis-
tically significant)the evidence was graded on level3
(two exposures,high decision latitude as protective and
job strain as negative exposure,see below).Level3 can
also be used according to the GRADE system even when
there are relatively few studies ifthere are unanimous
findings with high odds ratios (above 2.0). This occurred
for one exposure – bullying (see below).
Meta-analyses/Forest plots
In the studies results were reported as calculations of
association,e.g.,expressed as odds ratios,from mul-
tiple logistic regression,multivariatecorrelationsor
multiple linear regression coefficients.Whenever pos-
sible,the results were transformed into multiple logis-
tic regression odds ratios.Forestplots were used for
visual interpretation.To assist in illustrating the
Theorell et al.BMC Public Health (2015) 15:738 Page 4 of 14
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
results,and as a contribution to the overallassess-
ment, theseforest plots (meta-analyses)were con-
ducted when in at least two studiesthe samerisk
factor was analysed and mathematically comparable
data was provided using theComprehensiveMeta-
Analysis softwarepackage(www.meta-analysis.com/
index.php).Since the participants in the various stud-
ies might be construed as coming from the same popu-
lation (workers)or from differentpopulations(i.e.,
according to each study’s inclusion criteria) we chose
to use a fixed effects model.The strength of the scien-
tific evidence,using data from all of the included stud-
ies (not just those illustrated in the meta-analyses),
was determined by pairs ofthe authors ofthis paper
and then discussed and confirmed by allauthors.In-
formalhomogeneity tests were performed in order to
compare results from studies using standardized de-
pression interviews versus self-reportedquestion-
naires, high quality versus medium high quality
studies,generalpopulation studies versus specific oc-
cupationalcohorts and men versus women.In these
tests,we conducted sub-analyses of the presented find-
ings and compared results between the sub-categories,
e.g.,if the association between job exposure and de-
pressive symptomsdiffered according to the instru-
ment used for assessing the symptoms.
Ethics
All studies perused in this review have been approved by
the scientificethicalcommitteesin their universities.
They have allbeen published in internationalscientific
journalswith peerreview.Accordingly,no additional
ethical approval has been required.
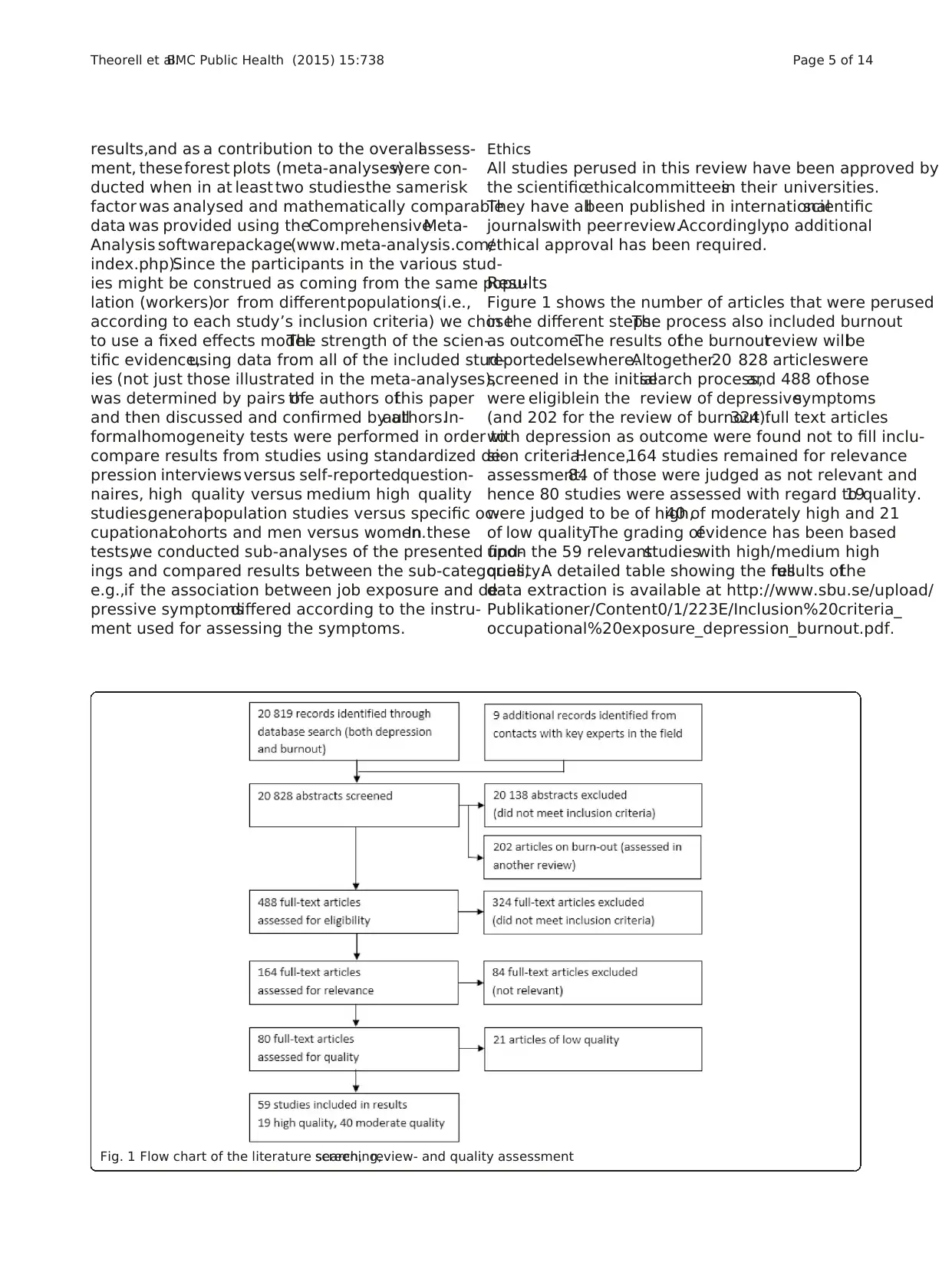
Results
Figure 1 shows the number of articles that were perused
in the different steps.The process also included burnout
as outcome.The results ofthe burnoutreview willbe
reportedelsewhere.Altogether20 828 articleswere
screened in the initialsearch process,and 488 ofthose
were eligiblein the review of depressivesymptoms
(and 202 for the review of burnout).324 full text articles
with depression as outcome were found not to fill inclu-
sion criteria.Hence,164 studies remained for relevance
assessment.84 of those were judged as not relevant and
hence 80 studies were assessed with regard to quality.19
were judged to be of high,40 of moderately high and 21
of low quality.The grading ofevidence has been based
upon the 59 relevantstudieswith high/medium high
quality.A detailed table showing the fullresults ofthe
data extraction is available at http://www.sbu.se/upload/
Publikationer/Content0/1/223E/Inclusion%20criteria_
occupational%20exposure_depression_burnout.pdf.
Fig. 1 Flow chart of the literature search,screening,review- and quality assessment
Theorell et al.BMC Public Health (2015) 15:738 Page 5 of 14
ment, theseforest plots (meta-analyses)were con-
ducted when in at least two studiesthe samerisk
factor was analysed and mathematically comparable
data was provided using theComprehensiveMeta-
Analysis softwarepackage(www.meta-analysis.com/
index.php).Since the participants in the various stud-
ies might be construed as coming from the same popu-
lation (workers)or from differentpopulations(i.e.,
according to each study’s inclusion criteria) we chose
to use a fixed effects model.The strength of the scien-
tific evidence,using data from all of the included stud-
ies (not just those illustrated in the meta-analyses),
was determined by pairs ofthe authors ofthis paper
and then discussed and confirmed by allauthors.In-
formalhomogeneity tests were performed in order to
compare results from studies using standardized de-
pression interviews versus self-reportedquestion-
naires, high quality versus medium high quality
studies,generalpopulation studies versus specific oc-
cupationalcohorts and men versus women.In these
tests,we conducted sub-analyses of the presented find-
ings and compared results between the sub-categories,
e.g.,if the association between job exposure and de-
pressive symptomsdiffered according to the instru-
ment used for assessing the symptoms.
Ethics
All studies perused in this review have been approved by
the scientificethicalcommitteesin their universities.
They have allbeen published in internationalscientific
journalswith peerreview.Accordingly,no additional
ethical approval has been required.
Results
Figure 1 shows the number of articles that were perused
in the different steps.The process also included burnout
as outcome.The results ofthe burnoutreview willbe
reportedelsewhere.Altogether20 828 articleswere
screened in the initialsearch process,and 488 ofthose
were eligiblein the review of depressivesymptoms
(and 202 for the review of burnout).324 full text articles
with depression as outcome were found not to fill inclu-
sion criteria.Hence,164 studies remained for relevance
assessment.84 of those were judged as not relevant and
hence 80 studies were assessed with regard to quality.19
were judged to be of high,40 of moderately high and 21
of low quality.The grading ofevidence has been based
upon the 59 relevantstudieswith high/medium high
quality.A detailed table showing the fullresults ofthe
data extraction is available at http://www.sbu.se/upload/
Publikationer/Content0/1/223E/Inclusion%20criteria_
occupational%20exposure_depression_burnout.pdf.
Fig. 1 Flow chart of the literature search,screening,review- and quality assessment
Theorell et al.BMC Public Health (2015) 15:738 Page 5 of 14
Most studieswere based on population samplesal-
though studies of samples from companies and occupa-
tionalgroups were also present.Few studies thatwere
judged to be relevant were based upon objective assess-
ments ofexposure.Subjective assessments based upon
standardized and validated questionnaires (for instance
demand/control/support,effort/reward,proceduraljust-
ice and bullying)were used in moststudies.The most
widely used established questionnairesrendered high
qualityratings.With regard to depression outcome,
both standardized interviews (mostly Composite Inter-
national DiagnosticInterview,CIDI) performedby
trained interviewers and different versions ofstandard-
ized questionnaires (such as Center for Epidemiological
Studies-Depression Scale,CES-D, and HospitalAnx-
iety and Depression Scale,HAD, and Hamilton Depres-
sion Scale,HRSD) for depressive symptoms were used.
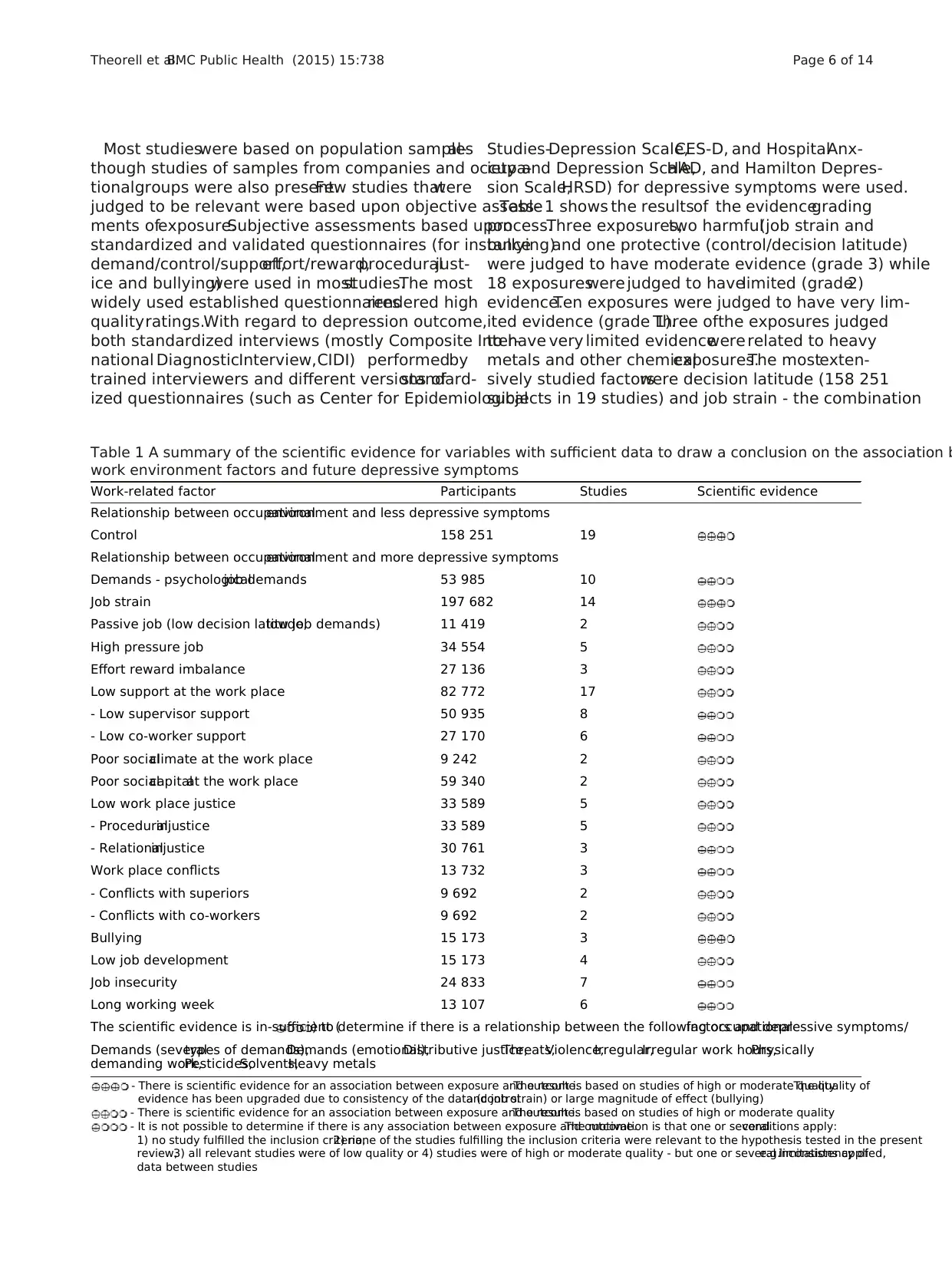
Table1 shows the resultsof the evidencegrading
process.Three exposures,two harmful(job strain and
bullying)and one protective (control/decision latitude)
were judged to have moderate evidence (grade 3) while
18 exposureswere judged to havelimited (grade2)
evidence.Ten exposures were judged to have very lim-
ited evidence (grade 1).Three ofthe exposures judged
to have very limited evidencewere related to heavy
metals and other chemicalexposures.The mostexten-
sively studied factorswere decision latitude (158 251
subjects in 19 studies) and job strain - the combination
Table 1 A summary of the scientific evidence for variables with sufficient data to draw a conclusion on the association b
work environment factors and future depressive symptoms
Work-related factor Participants Studies Scientific evidence
Relationship between occupationalenvironment and less depressive symptoms
Control 158 251 19
Relationship between occupationalenvironment and more depressive symptoms
Demands - psychologicaljob demands 53 985 10
Job strain 197 682 14
Passive job (low decision latitude,low job demands) 11 419 2
High pressure job 34 554 5
Effort reward imbalance 27 136 3
Low support at the work place 82 772 17
- Low supervisor support 50 935 8
- Low co-worker support 27 170 6
Poor socialclimate at the work place 9 242 2
Poor socialcapitalat the work place 59 340 2
Low work place justice 33 589 5
- Proceduralinjustice 33 589 5
- Relationalinjustice 30 761 3
Work place conflicts 13 732 3
- Conflicts with superiors 9 692 2
- Conflicts with co-workers 9 692 2
Bullying 15 173 3
Low job development 15 173 4
Job insecurity 24 833 7
Long working week 13 107 6
The scientific evidence is in-sufficient () to determine if there is a relationship between the following occupationalfactors and depressive symptoms/
Demands (severaltypes of demands),Demands (emotional),Distributive justice,Threats,Violence,Irregular,Irregular work hours,Physically
demanding work,Pesticides,Solvents,Heavy metals
- There is scientific evidence for an association between exposure and outcome.The result is based on studies of high or moderate quality.The quality of
evidence has been upgraded due to consistency of the data (controland job strain) or large magnitude of effect (bullying)
- There is scientific evidence for an association between exposure and outcome.The result is based on studies of high or moderate quality
- It is not possible to determine if there is any association between exposure and outcome.The motivation is that one or severalconditions apply:
1) no study fulfilled the inclusion criteria,2) none of the studies fulfilling the inclusion criteria were relevant to the hypothesis tested in the present
review,3) all relevant studies were of low quality or 4) studies were of high or moderate quality - but one or several limitations applied,e.g.inconsistency of
data between studies
Theorell et al.BMC Public Health (2015) 15:738 Page 6 of 14
though studies of samples from companies and occupa-
tionalgroups were also present.Few studies thatwere
judged to be relevant were based upon objective assess-
ments ofexposure.Subjective assessments based upon
standardized and validated questionnaires (for instance
demand/control/support,effort/reward,proceduraljust-
ice and bullying)were used in moststudies.The most
widely used established questionnairesrendered high
qualityratings.With regard to depression outcome,
both standardized interviews (mostly Composite Inter-
national DiagnosticInterview,CIDI) performedby
trained interviewers and different versions ofstandard-
ized questionnaires (such as Center for Epidemiological
Studies-Depression Scale,CES-D, and HospitalAnx-
iety and Depression Scale,HAD, and Hamilton Depres-
sion Scale,HRSD) for depressive symptoms were used.
Table1 shows the resultsof the evidencegrading
process.Three exposures,two harmful(job strain and
bullying)and one protective (control/decision latitude)
were judged to have moderate evidence (grade 3) while
18 exposureswere judged to havelimited (grade2)
evidence.Ten exposures were judged to have very lim-
ited evidence (grade 1).Three ofthe exposures judged
to have very limited evidencewere related to heavy
metals and other chemicalexposures.The mostexten-
sively studied factorswere decision latitude (158 251
subjects in 19 studies) and job strain - the combination
Table 1 A summary of the scientific evidence for variables with sufficient data to draw a conclusion on the association b
work environment factors and future depressive symptoms
Work-related factor Participants Studies Scientific evidence
Relationship between occupationalenvironment and less depressive symptoms
Control 158 251 19
Relationship between occupationalenvironment and more depressive symptoms
Demands - psychologicaljob demands 53 985 10
Job strain 197 682 14
Passive job (low decision latitude,low job demands) 11 419 2
High pressure job 34 554 5
Effort reward imbalance 27 136 3
Low support at the work place 82 772 17
- Low supervisor support 50 935 8
- Low co-worker support 27 170 6
Poor socialclimate at the work place 9 242 2
Poor socialcapitalat the work place 59 340 2
Low work place justice 33 589 5
- Proceduralinjustice 33 589 5
- Relationalinjustice 30 761 3
Work place conflicts 13 732 3
- Conflicts with superiors 9 692 2
- Conflicts with co-workers 9 692 2
Bullying 15 173 3
Low job development 15 173 4
Job insecurity 24 833 7
Long working week 13 107 6
The scientific evidence is in-sufficient () to determine if there is a relationship between the following occupationalfactors and depressive symptoms/
Demands (severaltypes of demands),Demands (emotional),Distributive justice,Threats,Violence,Irregular,Irregular work hours,Physically
demanding work,Pesticides,Solvents,Heavy metals
- There is scientific evidence for an association between exposure and outcome.The result is based on studies of high or moderate quality.The quality of
evidence has been upgraded due to consistency of the data (controland job strain) or large magnitude of effect (bullying)
- There is scientific evidence for an association between exposure and outcome.The result is based on studies of high or moderate quality
- It is not possible to determine if there is any association between exposure and outcome.The motivation is that one or severalconditions apply:
1) no study fulfilled the inclusion criteria,2) none of the studies fulfilling the inclusion criteria were relevant to the hypothesis tested in the present
review,3) all relevant studies were of low quality or 4) studies were of high or moderate quality - but one or several limitations applied,e.g.inconsistency of
data between studies
Theorell et al.BMC Public Health (2015) 15:738 Page 6 of 14
of high psychologicaldemands and low decision latitude
(197 682 subjects in 14 studies).It was possible to com-
pute a weighted odds ratio 1.74 (95 % CI 1.54 to 1.96 for
studieswith oddsratio calculations).A high decision
latitude protected statistically against worsening depres-
sive symptoms– with a weighted oddsratio of 0.73
(95 % CI 0.68 to 0.77).Bullying had been studied in 15
173 subjectsin three studies.One of thesestudies
showed results for men and women separately.Despite
the relativelysmall numberof studies,bullyingwas
judged to be related to worsening depressive symptoms
with an evidence grade of3 as the findings were very
consistentand the odds ratios were high (the weighted
odds ratio being 2.82;95 % CI 2.21 to 3.59).
Figure 2 shows forest plots for the three factors with
evidence grade 3 - decision latitude (a),job strain (b)
and bullying (c).For high decision latitude,17/18 point
estimates were lower than 1.0 (separate point estimates
for men and women in five studies).The upper 95 %
confidence limitwas above 1.0 in five studies.For job
strain,14/15 pointestimateswere above1.0. Three
lower confidence limits reached below 1.0.The forest
plots were based upon studies from which odds ratios
could be extracted or calculated.It should be pointed
out, however,that the total evidencegradingalso
included a few additionalstudies.Bullying,finally,had
four pointestimates in the diagram.All of those were
higher than 2.0 and all the lower confidence limits were
above 1.0.
The exposures with a limited levelof evidence were
psychologicaldemands (quantitativepsychological
demandsdefined accordingto the widely used Job
ContentQuestionnaire oralternative psychometrically
tested versions),the combination oflow psychological
demandsand low decision latitude(“passivework”),
“pressing work” (mainly important life events at work),
effort reward imbalance,low social support (from
management and coworkers),poor socialclimate,poor
social capital,low proceduraland relationaljustice,
conflicts with superiorsand colleagues,poor skill
discretion,job insecurity and long working weeks (the
latter for women only).
The exposures with very limited (= level1) evidence
were other kinds of demands (not quantitative) including
emotionaldemands,distributivejustice,threats,vio-
lence,irregularworking hours, long working hours
(men),physically demanding work,exposure to pesti-
cides and insecticides,solvents and heavy metals.
Homogeneity tests showed thatresults were compar-
able for two groups ofoutcome measures (standardized
interview versus standardized self-report questionnaire),
for men and women,for generalpopulation versus spe-
cific occupation cohorts and for white collar versus blue
collar groups.
Discussion
Main findings and recent developments in the field
The aim of the studywas to provide systematically
graded evidence for possible associations between work
environment factors and near-future development of de-
pressive symptoms.A totalof fifty-nine relevant articles
with high or medium high scientific quality fulfilling our
criteria were found.The resultsprovide evidence for
several work conditions being linked to depressive symp-
toms among the employees in both positive and negative
directions.Scientific evidence of grade three out of four
(in other words moderately strong)was shown for job
strain (high psychologicaldemandsand low decision
latitude),low decision latitudeand bullying.Further-
more,scientific evidence ofgrade two wasfound for
psychologicaldemands,effort reward imbalance,low
support,unfavorable socialclimate,lack of procedural
and relationaljustice,conflicts with superiors and col-
leagues,limited skilldiscretion,job insecurity and long
working week.
An important finding is that there were few prospect-
ive studies with sufficient quality of the relationship be-
tween adverse chemical(pesticides and heavy metals for
instance)and physical(heavy loads,awkward positions,
irradiation,cold and hot temperature)and depressive
symptoms.This field needs more research.
The results should primarily be interpreted in the con-
textof the Western world.We deliberately limited our
inclusion of studies to these countries.The rationale be-
hind this was that we wanted to secure similar cultural
framework around work in order to simplify our inter-
pretation of the findings.
The review differs from earlier studies in the field due
to its comprehensive and thorough approach.Our re-
view is based on an extremely thorough literature search
as wellas on a well-described and systematic evaluation
of a large number ofpublications.Thus,it includes all
kinds of environmentalexposures,physicalas well as
psychosocialand that it is based upon a systematic ap-
proach.This is the first review in which the examination
of evidence follows(a slightmodification of )GRADE
principles.Furthermoreit is including morerecently
published research than previous reviews.
Our review shows that the psychosocialresearch field
has made progress since the reviews published in 2008
and 2010.Bonde [1]and Netterström etal. [2] made
criticalremarks aboutpossible publication bias,lack of
more “objective” measures of exposure and outcome and
also aboutlack of time perspectiveswhich would be
needed for the understanding of time of exposure needed
for the development of depression.With regard to object-
ive measures,thereare more publishedstudiesthan
previously with standardized interview based assessment o
clinical depression.Comparison of the plots corresponding
Theorell et al.BMC Public Health (2015) 15:738 Page 7 of 14
(197 682 subjects in 14 studies).It was possible to com-
pute a weighted odds ratio 1.74 (95 % CI 1.54 to 1.96 for
studieswith oddsratio calculations).A high decision
latitude protected statistically against worsening depres-
sive symptoms– with a weighted oddsratio of 0.73
(95 % CI 0.68 to 0.77).Bullying had been studied in 15
173 subjectsin three studies.One of thesestudies
showed results for men and women separately.Despite
the relativelysmall numberof studies,bullyingwas
judged to be related to worsening depressive symptoms
with an evidence grade of3 as the findings were very
consistentand the odds ratios were high (the weighted
odds ratio being 2.82;95 % CI 2.21 to 3.59).
Figure 2 shows forest plots for the three factors with
evidence grade 3 - decision latitude (a),job strain (b)
and bullying (c).For high decision latitude,17/18 point
estimates were lower than 1.0 (separate point estimates
for men and women in five studies).The upper 95 %
confidence limitwas above 1.0 in five studies.For job
strain,14/15 pointestimateswere above1.0. Three
lower confidence limits reached below 1.0.The forest
plots were based upon studies from which odds ratios
could be extracted or calculated.It should be pointed
out, however,that the total evidencegradingalso
included a few additionalstudies.Bullying,finally,had
four pointestimates in the diagram.All of those were
higher than 2.0 and all the lower confidence limits were
above 1.0.
The exposures with a limited levelof evidence were
psychologicaldemands (quantitativepsychological
demandsdefined accordingto the widely used Job
ContentQuestionnaire oralternative psychometrically
tested versions),the combination oflow psychological
demandsand low decision latitude(“passivework”),
“pressing work” (mainly important life events at work),
effort reward imbalance,low social support (from
management and coworkers),poor socialclimate,poor
social capital,low proceduraland relationaljustice,
conflicts with superiorsand colleagues,poor skill
discretion,job insecurity and long working weeks (the
latter for women only).
The exposures with very limited (= level1) evidence
were other kinds of demands (not quantitative) including
emotionaldemands,distributivejustice,threats,vio-
lence,irregularworking hours, long working hours
(men),physically demanding work,exposure to pesti-
cides and insecticides,solvents and heavy metals.
Homogeneity tests showed thatresults were compar-
able for two groups ofoutcome measures (standardized
interview versus standardized self-report questionnaire),
for men and women,for generalpopulation versus spe-
cific occupation cohorts and for white collar versus blue
collar groups.
Discussion
Main findings and recent developments in the field
The aim of the studywas to provide systematically
graded evidence for possible associations between work
environment factors and near-future development of de-
pressive symptoms.A totalof fifty-nine relevant articles
with high or medium high scientific quality fulfilling our
criteria were found.The resultsprovide evidence for
several work conditions being linked to depressive symp-
toms among the employees in both positive and negative
directions.Scientific evidence of grade three out of four
(in other words moderately strong)was shown for job
strain (high psychologicaldemandsand low decision
latitude),low decision latitudeand bullying.Further-
more,scientific evidence ofgrade two wasfound for
psychologicaldemands,effort reward imbalance,low
support,unfavorable socialclimate,lack of procedural
and relationaljustice,conflicts with superiors and col-
leagues,limited skilldiscretion,job insecurity and long
working week.
An important finding is that there were few prospect-
ive studies with sufficient quality of the relationship be-
tween adverse chemical(pesticides and heavy metals for
instance)and physical(heavy loads,awkward positions,
irradiation,cold and hot temperature)and depressive
symptoms.This field needs more research.
The results should primarily be interpreted in the con-
textof the Western world.We deliberately limited our
inclusion of studies to these countries.The rationale be-
hind this was that we wanted to secure similar cultural
framework around work in order to simplify our inter-
pretation of the findings.
The review differs from earlier studies in the field due
to its comprehensive and thorough approach.Our re-
view is based on an extremely thorough literature search
as wellas on a well-described and systematic evaluation
of a large number ofpublications.Thus,it includes all
kinds of environmentalexposures,physicalas well as
psychosocialand that it is based upon a systematic ap-
proach.This is the first review in which the examination
of evidence follows(a slightmodification of )GRADE
principles.Furthermoreit is including morerecently
published research than previous reviews.
Our review shows that the psychosocialresearch field
has made progress since the reviews published in 2008
and 2010.Bonde [1]and Netterström etal. [2] made
criticalremarks aboutpossible publication bias,lack of
more “objective” measures of exposure and outcome and
also aboutlack of time perspectiveswhich would be
needed for the understanding of time of exposure needed
for the development of depression.With regard to object-
ive measures,thereare more publishedstudiesthan
previously with standardized interview based assessment o
clinical depression.Comparison of the plots corresponding
Theorell et al.BMC Public Health (2015) 15:738 Page 7 of 14
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
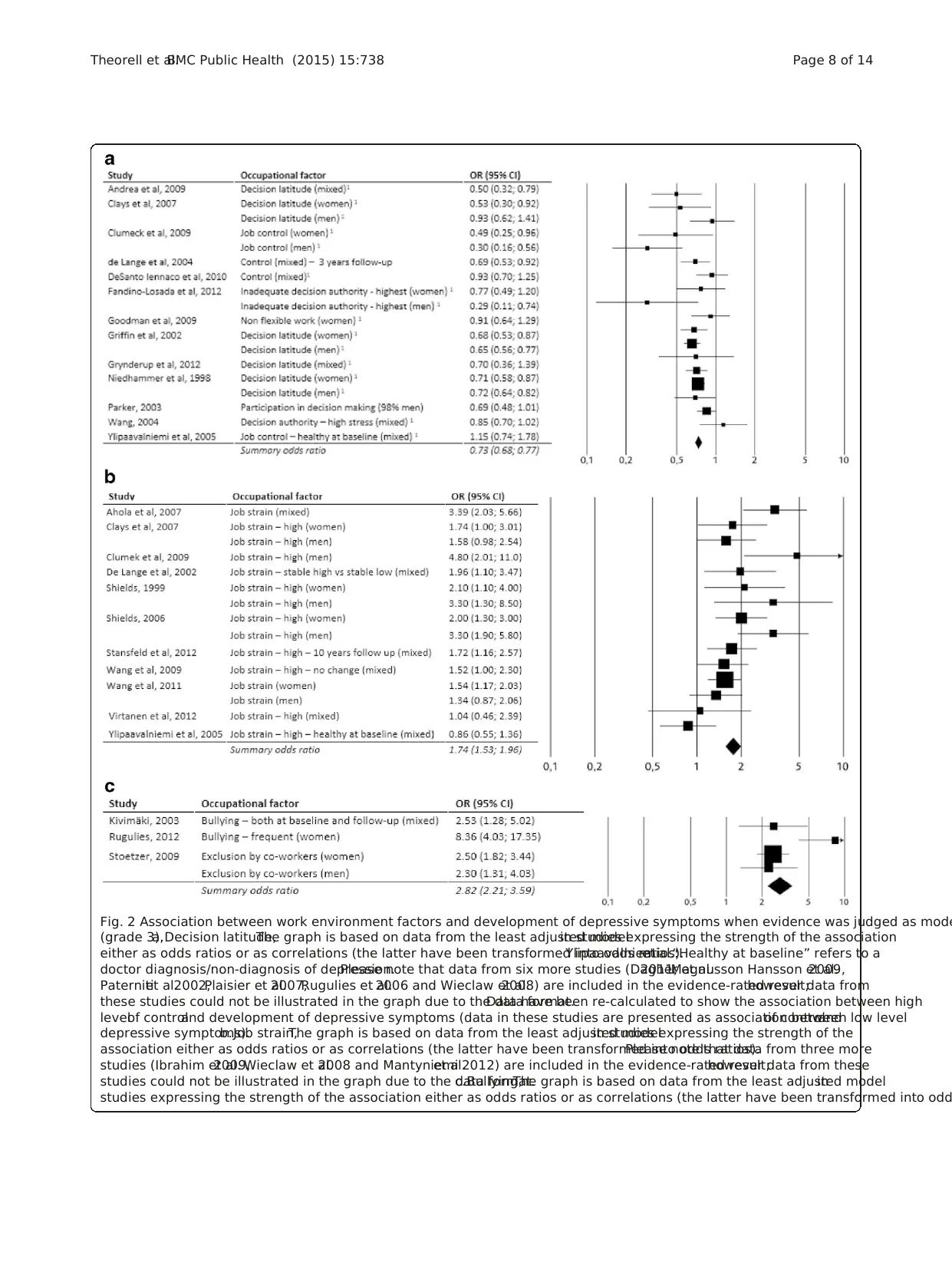
Fig. 2 Association between work environment factors and development of depressive symptoms when evidence was judged as mode
(grade 3),a.Decision latitude,The graph is based on data from the least adjusted modelin studies expressing the strength of the association
either as odds ratios or as correlations (the latter have been transformed into odds ratios).Ylipaavalniemiet al.:“Healthy at baseline” refers to a
doctor diagnosis/non-diagnosis of depression.Please note that data from six more studies (Dagher et al.2011,Magnusson Hansson et al.2009,
Paternitiet al.2002,Plaisier et al.2007,Rugulies et al.2006 and Wieclaw et al.2008) are included in the evidence-rated result;however data from
these studies could not be illustrated in the graph due to the data format.Data have been re-calculated to show the association between high
levelof controland development of depressive symptoms (data in these studies are presented as association between low levelof controland
depressive symptoms).b.Job strain,The graph is based on data from the least adjusted modelin studies expressing the strength of the
association either as odds ratios or as correlations (the latter have been transformed into odds ratios).Please note that data from three more
studies (Ibrahim et al.2009,Wieclaw et al.2008 and Mantyniemiet al.2012) are included in the evidence-rated result;however data from these
studies could not be illustrated in the graph due to the data format.c.Bullying,The graph is based on data from the least adjusted modelin
studies expressing the strength of the association either as odds ratios or as correlations (the latter have been transformed into odd
Theorell et al.BMC Public Health (2015) 15:738 Page 8 of 14
(grade 3),a.Decision latitude,The graph is based on data from the least adjusted modelin studies expressing the strength of the association
either as odds ratios or as correlations (the latter have been transformed into odds ratios).Ylipaavalniemiet al.:“Healthy at baseline” refers to a
doctor diagnosis/non-diagnosis of depression.Please note that data from six more studies (Dagher et al.2011,Magnusson Hansson et al.2009,
Paternitiet al.2002,Plaisier et al.2007,Rugulies et al.2006 and Wieclaw et al.2008) are included in the evidence-rated result;however data from
these studies could not be illustrated in the graph due to the data format.Data have been re-calculated to show the association between high
levelof controland development of depressive symptoms (data in these studies are presented as association between low levelof controland
depressive symptoms).b.Job strain,The graph is based on data from the least adjusted modelin studies expressing the strength of the
association either as odds ratios or as correlations (the latter have been transformed into odds ratios).Please note that data from three more
studies (Ibrahim et al.2009,Wieclaw et al.2008 and Mantyniemiet al.2012) are included in the evidence-rated result;however data from these
studies could not be illustrated in the graph due to the data format.c.Bullying,The graph is based on data from the least adjusted modelin
studies expressing the strength of the association either as odds ratios or as correlations (the latter have been transformed into odd
Theorell et al.BMC Public Health (2015) 15:738 Page 8 of 14
to results from studies based upon standardized interviews
did not differ from those from studies based upon inter-
nationallyaccepted depression questionnaires.Objective
exposures are stilluncommon,however.One interesting
approach was used by Virtanen et al.[13] who could show
thathospitalstaffwho experienced excess occupancy of
hospital beds had increased risk of developing sick leave be-
cause of depression in a dose-response manner, with excess
occupancy exceeding 10 % being associated with an odds
ratio of sick leave for depression of 1.94 (1.14-3.28).
During later years research designs on the association
between work environmentfactors and depressive feel-
ings havebecomeincreasinglysophisticated.For in-
stance,Shields [14],Stansfeld et al.[15],De Lange et al.
[16] and Wang et al.[17] have examined possible effects
of exposure to job strain atleasttwice,or even three
times in the follow-up survey waves.Their findings indi-
catethat accumulated orincreasing job strain hasa
stronger adverse statisticaleffect on risk of experiencing
increased ratings of depressive symptoms during follow-
up than decreasing job strain.As mightbe expected,
these studies show that two or more assessments of the
job situation provide more precise information regarding
risk than only one measurement.Therefore stronger evi-
dence regarding the influence ofworking conditions on
mentalhealth may be expected in future research with a
growing body of studies with such methodology.
The literature search included articles published up to
June 2013.For practicalreasons it has not been possible
to do a full review of the articles published after that date.
However,a more informalsearch in the scientific litera-
ture (PubMed and PsycInfo untilFebruary 2015) showed
that a few more recent prospective studies of work envir-
onmentand development ofdepressive feelings relevant
to the present review have been published.None of those
would have changed our conclusions.Four ofthem sup-
port the use of standardized measures of job strain or high
psychologicaldemands and low decision latitude in pre-
dicting either depressive symptoms or major depressive
disorder [18–21] and one of them supports the use of ef-
fort reward imbalance (or low reward) in the prediction of
disability pension due to depression [21].
Gender
Our results showed thatsimilar work conditions were
related to asimilarincreasein depressivesymptoms
among men and women.However,although there is no
gender difference in excess risk associated with adverse
work conditions,studies have shown that women actu-
ally have higher levels ofjob strain than men [22].This
may be one reason for women’s higher prevalence of de-
pressivesymptoms.Other studiesindicatethat work
conditions can affect men and women differently in rela-
tion to developmentof major depressivedisorder
(MDD). For example,a Canadian studyshowed that
men had elevated risk of MDD only if they were exposed
to extremely high levelof job strain while women had
elevated risk ofMDD even when exposed to moderate
job strain [23].The study points to the need of context-
ualizing findings aboutmentalhealth and itmay also
illustrate thatgendercould be more relevantfor the
relationshipbetweenworking conditionsand major
depressive disorderthan for the relationship between
working conditions and depressive symptoms.
Technical issues
In this review we have notreviewed evidence whether
there is interaction ornot between high psychological
demands and low decision latitude (as discussed for in-
stance in Karasek and Theorell[24]).We have regarded
the combination simplyas a theoreticalconstruction
and evaluated its possible success or lack of success as a
predictor of development of depressive symptoms.
In forest plots,we chose to use data from the least ad-
justed model from each study.The main rationale for this
was thatthese models were more comparable between
studies than other models,since the more adjusted ones
were adjusted to widely differentpotentialconfounders.
The most powerful prognostic factor for incident depres-
sive symptoms was manifest symptoms at the study base-
line;a parameter that had to be assessed in each ofthe
includedstudies.Generally,adjustingfor other con-
founders had very little effect.For transparency,we have
listed data in both least and most adjusted models, see ex-
tensive tables at http://www.sbu.se/upload/Publikationer/
Content0/1/223E/Inclusion%20criteria_occupational%20
exposure_depression_burnout.pdf.
An important point is that ifa study presented data in
several statistical models,all data from all models were in-
cluded in the expert group assessment of scientific evidenc
for all of the results presented in this systematic review.
Assessments ofodds ratios may be somewhatunreli-
able due to differencesin methodology acrossstudies
and also due to the fact that summary odds ratios could
not be calculated forsome ofthe occupationalexpo-
sures.It should however be pointed out that for most of
the studied exposures the observed risks were of moder-
ate size.
The operationalization ofjob strain differed between
the studies.The majority ofthe published studies used
the median splitdefinition (above median for the psy-
chologicaldemands score and below median for the de-
cision latitude score).When exposure to job strain is
defined in this way and the remaining participants in the
study are defined as unexposed there is relatively little
contrast between unexposed and exposed subjects.This
may lead to underestimation of the true association.
Theorell et al.BMC Public Health (2015) 15:738 Page 9 of 14
did not differ from those from studies based upon inter-
nationallyaccepted depression questionnaires.Objective
exposures are stilluncommon,however.One interesting
approach was used by Virtanen et al.[13] who could show
thathospitalstaffwho experienced excess occupancy of
hospital beds had increased risk of developing sick leave be-
cause of depression in a dose-response manner, with excess
occupancy exceeding 10 % being associated with an odds
ratio of sick leave for depression of 1.94 (1.14-3.28).
During later years research designs on the association
between work environmentfactors and depressive feel-
ings havebecomeincreasinglysophisticated.For in-
stance,Shields [14],Stansfeld et al.[15],De Lange et al.
[16] and Wang et al.[17] have examined possible effects
of exposure to job strain atleasttwice,or even three
times in the follow-up survey waves.Their findings indi-
catethat accumulated orincreasing job strain hasa
stronger adverse statisticaleffect on risk of experiencing
increased ratings of depressive symptoms during follow-
up than decreasing job strain.As mightbe expected,
these studies show that two or more assessments of the
job situation provide more precise information regarding
risk than only one measurement.Therefore stronger evi-
dence regarding the influence ofworking conditions on
mentalhealth may be expected in future research with a
growing body of studies with such methodology.
The literature search included articles published up to
June 2013.For practicalreasons it has not been possible
to do a full review of the articles published after that date.
However,a more informalsearch in the scientific litera-
ture (PubMed and PsycInfo untilFebruary 2015) showed
that a few more recent prospective studies of work envir-
onmentand development ofdepressive feelings relevant
to the present review have been published.None of those
would have changed our conclusions.Four ofthem sup-
port the use of standardized measures of job strain or high
psychologicaldemands and low decision latitude in pre-
dicting either depressive symptoms or major depressive
disorder [18–21] and one of them supports the use of ef-
fort reward imbalance (or low reward) in the prediction of
disability pension due to depression [21].
Gender
Our results showed thatsimilar work conditions were
related to asimilarincreasein depressivesymptoms
among men and women.However,although there is no
gender difference in excess risk associated with adverse
work conditions,studies have shown that women actu-
ally have higher levels ofjob strain than men [22].This
may be one reason for women’s higher prevalence of de-
pressivesymptoms.Other studiesindicatethat work
conditions can affect men and women differently in rela-
tion to developmentof major depressivedisorder
(MDD). For example,a Canadian studyshowed that
men had elevated risk of MDD only if they were exposed
to extremely high levelof job strain while women had
elevated risk ofMDD even when exposed to moderate
job strain [23].The study points to the need of context-
ualizing findings aboutmentalhealth and itmay also
illustrate thatgendercould be more relevantfor the
relationshipbetweenworking conditionsand major
depressive disorderthan for the relationship between
working conditions and depressive symptoms.
Technical issues
In this review we have notreviewed evidence whether
there is interaction ornot between high psychological
demands and low decision latitude (as discussed for in-
stance in Karasek and Theorell[24]).We have regarded
the combination simplyas a theoreticalconstruction
and evaluated its possible success or lack of success as a
predictor of development of depressive symptoms.
In forest plots,we chose to use data from the least ad-
justed model from each study.The main rationale for this
was thatthese models were more comparable between
studies than other models,since the more adjusted ones
were adjusted to widely differentpotentialconfounders.
The most powerful prognostic factor for incident depres-
sive symptoms was manifest symptoms at the study base-
line;a parameter that had to be assessed in each ofthe
includedstudies.Generally,adjustingfor other con-
founders had very little effect.For transparency,we have
listed data in both least and most adjusted models, see ex-
tensive tables at http://www.sbu.se/upload/Publikationer/
Content0/1/223E/Inclusion%20criteria_occupational%20
exposure_depression_burnout.pdf.
An important point is that ifa study presented data in
several statistical models,all data from all models were in-
cluded in the expert group assessment of scientific evidenc
for all of the results presented in this systematic review.
Assessments ofodds ratios may be somewhatunreli-
able due to differencesin methodology acrossstudies
and also due to the fact that summary odds ratios could
not be calculated forsome ofthe occupationalexpo-
sures.It should however be pointed out that for most of
the studied exposures the observed risks were of moder-
ate size.
The operationalization ofjob strain differed between
the studies.The majority ofthe published studies used
the median splitdefinition (above median for the psy-
chologicaldemands score and below median for the de-
cision latitude score).When exposure to job strain is
defined in this way and the remaining participants in the
study are defined as unexposed there is relatively little
contrast between unexposed and exposed subjects.This
may lead to underestimation of the true association.
Theorell et al.BMC Public Health (2015) 15:738 Page 9 of 14
As recommended in the epidemiologicalliterature we
produced funnelplots to investigate possible publication
bias.When there is pronounced publication bias,studies
reporting “confirming” odds ratios with wide confidence
intervalsare more common than studiesreporting
“rejecting”oddsratioswith wide confidence intervals.
Such an analysis cannot replace a realanalysis of publi-
cation bias – the bestanalysis would be to contactre-
searchers asking for unpublished studies.But according
to our exploration ofthe material,there was no such
evidence of publication bias.
Limitations
Most studies were based upon self-reports of both work-
ing conditionsand depressivesymptoms.Few of the
studies were based upon in situ investigation of the work
environment and standardized clinicalinterviews of em-
ployees.Such interviewsare more objective and may
more often identify depression than standardized self-
rating questionnaires which primarily have screening or
follow-up indications.The risk of inflated associations
may arise,when there are subjective descriptions both of
explanatory and dependent factors [25].This is particu-
larly the case in cross-sectionalstudieswhile in pro-
spective studies this risk is less pronounced.The risk of
inflated association decreasesas adjustmentsare per-
formed for initial symptoms of mental disease and when
the assessmentsof working conditionsand mental
symptomsare standardized.Accordingly,in this study
we only included prospective studies(and comparable
case-controlstudies) with data on initialsymptoms and
standardized measures of exposure and outcome.
Due to the factthatthe researchers in the included
studies had chosen a wide range ofdifferentstatistical
measures to express associations between occupational
exposure and depressive symptoms,it was notpossible
to conductformalmathematicalhomogeneity analyses
including the entire data material.Instead,the expert
group conducted a combination ofmathematicaland
narrative sub-group analyses to explore whether the re-
sults were homogenous when subgroups of studies were
compared.Accordingly results were compared for men
versuswomen,for self-reported versusclinically rated
depression/depressive symptoms,for generalpopulation
studiesversusspecificoccupationalcohortsand for
high/medium high quality studies.Inspection of the con-
fidence interval distributions,as well as sub-populations'
summaryodds ratios and their confidenceintervals
showed homogenous results across those dichotomies.
A limitation of our review could be that we may have
underestimated the importance ofwork environment
factors that have not been subjected to many empirical
studies.There were examples ofexposure factors that
were examined in many studies but did not achieve level
3 in the grading system such as psychologicaldemands
- which only yielded evidence level 2. This illustrates the
need for more detailed studies ofdifferentaspects of
demands,such as emotionaldemands.In addition,ef-
fort reward imbalance was consistently associated with
worseningdepressivesymptomsin three studiesof
medium high quality and was classified as second grade
evidence.The summarized odds ratio was 1.78 which is
comparableto the corresponding oddsratio for job
strain which was1.74.However,job strain had been
examined in 14 studiesand therefore achieved third
grade evidence.
Another limitation is thatwe have notincluded out-
side work factors that may be of importance.As pointed
out for instance by Wang and Schmitz [26]job strain
may interactwith psychosocialfactorsoutside ofthe
workplace in relation to the risk ofmajordepression,
and such interactionsmay in addition differbetween
men and women.
Societal relevance
Despite the often moderate sizes ofour findings,some
of the associations are ofconsiderable societalimport-
ance.An illustration ofthis is thatif a work environ-
ment factor has a prevalence of25 % and is associated
with a relative risk of1.8,the resulting population at-
tributable risk is 11 %.Accordingly,when an exposure
is common (as is the case with job strain,low levelof
control and effort reward imbalancewith the oper-
ationaldefinitions that have been used) even a moder-
ately elevated risk associated with it becomes important
in a societal context.
The work environmentfactorsfor which we found
scientificevidencefor an associationto depressive
symptom developmentare possibleto influenceby
meansof work organization changes.For instance,it
has been shown thatdecision latitude foremployees
can be improved by analysis ofthe work organization
with subsequentgoal-directed organization interven-
tion [27,28] or by a year-long education ofmanagers
about psychosocialfactors [29].A review of naturalex-
periments designed to reduce psychosocialrisks in the
work environment for bus drivers showed that such in-
terventions may resultin reduced biologicalstress in
that group [30].The present results suggest that in as-
sessmentand treatmentplans ofdepression,work en-
vironment should be taken into account.
Conclusions
There is substantialempiricalevidence thatemployees,
both men and women,who report lack ofdecision lati-
tude,job strain and bullying,will experience increasing
depressive symptoms over time.
Theorell et al.BMC Public Health (2015) 15:738 Page 10 of 14
produced funnelplots to investigate possible publication
bias.When there is pronounced publication bias,studies
reporting “confirming” odds ratios with wide confidence
intervalsare more common than studiesreporting
“rejecting”oddsratioswith wide confidence intervals.
Such an analysis cannot replace a realanalysis of publi-
cation bias – the bestanalysis would be to contactre-
searchers asking for unpublished studies.But according
to our exploration ofthe material,there was no such
evidence of publication bias.
Limitations
Most studies were based upon self-reports of both work-
ing conditionsand depressivesymptoms.Few of the
studies were based upon in situ investigation of the work
environment and standardized clinicalinterviews of em-
ployees.Such interviewsare more objective and may
more often identify depression than standardized self-
rating questionnaires which primarily have screening or
follow-up indications.The risk of inflated associations
may arise,when there are subjective descriptions both of
explanatory and dependent factors [25].This is particu-
larly the case in cross-sectionalstudieswhile in pro-
spective studies this risk is less pronounced.The risk of
inflated association decreasesas adjustmentsare per-
formed for initial symptoms of mental disease and when
the assessmentsof working conditionsand mental
symptomsare standardized.Accordingly,in this study
we only included prospective studies(and comparable
case-controlstudies) with data on initialsymptoms and
standardized measures of exposure and outcome.
Due to the factthatthe researchers in the included
studies had chosen a wide range ofdifferentstatistical
measures to express associations between occupational
exposure and depressive symptoms,it was notpossible
to conductformalmathematicalhomogeneity analyses
including the entire data material.Instead,the expert
group conducted a combination ofmathematicaland
narrative sub-group analyses to explore whether the re-
sults were homogenous when subgroups of studies were
compared.Accordingly results were compared for men
versuswomen,for self-reported versusclinically rated
depression/depressive symptoms,for generalpopulation
studiesversusspecificoccupationalcohortsand for
high/medium high quality studies.Inspection of the con-
fidence interval distributions,as well as sub-populations'
summaryodds ratios and their confidenceintervals
showed homogenous results across those dichotomies.
A limitation of our review could be that we may have
underestimated the importance ofwork environment
factors that have not been subjected to many empirical
studies.There were examples ofexposure factors that
were examined in many studies but did not achieve level
3 in the grading system such as psychologicaldemands
- which only yielded evidence level 2. This illustrates the
need for more detailed studies ofdifferentaspects of
demands,such as emotionaldemands.In addition,ef-
fort reward imbalance was consistently associated with
worseningdepressivesymptomsin three studiesof
medium high quality and was classified as second grade
evidence.The summarized odds ratio was 1.78 which is
comparableto the corresponding oddsratio for job
strain which was1.74.However,job strain had been
examined in 14 studiesand therefore achieved third
grade evidence.
Another limitation is thatwe have notincluded out-
side work factors that may be of importance.As pointed
out for instance by Wang and Schmitz [26]job strain
may interactwith psychosocialfactorsoutside ofthe
workplace in relation to the risk ofmajordepression,
and such interactionsmay in addition differbetween
men and women.
Societal relevance
Despite the often moderate sizes ofour findings,some
of the associations are ofconsiderable societalimport-
ance.An illustration ofthis is thatif a work environ-
ment factor has a prevalence of25 % and is associated
with a relative risk of1.8,the resulting population at-
tributable risk is 11 %.Accordingly,when an exposure
is common (as is the case with job strain,low levelof
control and effort reward imbalancewith the oper-
ationaldefinitions that have been used) even a moder-
ately elevated risk associated with it becomes important
in a societal context.
The work environmentfactorsfor which we found
scientificevidencefor an associationto depressive
symptom developmentare possibleto influenceby
meansof work organization changes.For instance,it
has been shown thatdecision latitude foremployees
can be improved by analysis ofthe work organization
with subsequentgoal-directed organization interven-
tion [27,28] or by a year-long education ofmanagers
about psychosocialfactors [29].A review of naturalex-
periments designed to reduce psychosocialrisks in the
work environment for bus drivers showed that such in-
terventions may resultin reduced biologicalstress in
that group [30].The present results suggest that in as-
sessmentand treatmentplans ofdepression,work en-
vironment should be taken into account.
Conclusions
There is substantialempiricalevidence thatemployees,
both men and women,who report lack ofdecision lati-
tude,job strain and bullying,will experience increasing
depressive symptoms over time.
Theorell et al.BMC Public Health (2015) 15:738 Page 10 of 14
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Many of the work environmentalfactors can be favor-
ably influenced by effective organizationalinterventions.
An importantstep in this research field would be the
launching ofgood evaluations ofpsychosocialinterven-
tions.For some kinds of working conditions that are de-
veloping in the modern working world,new research on
depressive symptoms will be needed.
Appendix
Studies judged to be of high or medium high quality
Ahola K,Hakanen J.Job strain,burnout,and depres-
sive symptoms:a prospective study among dentists.J
Affect Disord 2007;104:103-10.
Andrea H,Bultmann U,van Amelsvoort LG,Kant Y.
The incidence ofanxiety and depression among em-
ployees – the role ofpsychosocialwork characteristics.
Depress Anxiety 2009;26:1040-8.
BeselerCL, StallonesL, Hoppin JA, Alavanja MC,
Blair A, Keefe T,et al.Depression and pesticide expo-
sures among private pesticide applicators enrolled in
the AgriculturalHealth Study.Environ Health Per-
spect 2008;116:1713-9.
Bonde JP,Munch-Hansen T,WieclawJ,Westergaard-
Nielsen N,Agerbo E.Psychosocialwork environment
and antidepressantmedication:a prospectivecohort
study.BMC Public Health 2009;9:262.
Burgard SA,Brand JE,House JS.Perceived job inse-
curity and worker health in the United States.Soc Sci
Med 2009;69:777-85.
Clays E,De Bacquer D,Leynen F,Kornitzer M,Kittel F,
De BackerG. Job stressand depression symptomsin
middle-aged workers – prospective results from the Bels-
tress study. Scand J Work Environ Health 2007;33:252-9.
Clumeck N, KempenaersC, Godin I, Dramaix M,
Kornitzer M,Linkowski P,et al.Working conditions pre-
dict incidence of long-term spells of sick leave due to de-
pression:results from the Belstress I prospective study.J
Epidemiol Community Health 2009;63:286-9
DagherRK, McGovern PM,Dowd BE,Lundberg U.
Postpartum depressivesymptomsand the combined
load of paid and unpaid work:a longitudinal analysis.Int
Arch Occup Environ Health 2011;84:735-43.
De Lange AH, Taris TW, KompierMAJ, Houtman
ILD, Bongers PM.The relationships between work char-
acteristicsand mentalhealth:examiningnormal,re-
versed and reciprocalrelationshipsin a 4-wavestudy.
Work & Stress 2004;18:149-66.
de Lange AH,Taris TW,Kompier MA,Houtman IL,
BongersPM. Effectsof stable and changing demand-
controlhistories on worker health.Scand JWork En-
viron Health 2002;28:94-108.
d’Errico A, Cardano M, LandriscinaT,MarinacciC,
Pasian S,Petrelli A,et al.Workplace stress and prescrip-
tion of antidepressantmedications:a prospective study
on a sample ofItalian workers.Int Arch OccupEnviron
Health 2011;84:413-24.
De Santo Iennaco J,Cullen MR,Cantley L,Slade MD,
Fiellin M, Kasl SV. Effectsof externally rated job de-
mand and controlon depression diagnosis claims in an
industrial cohort.Am J Epidemiol 2010;171:303-11.
Fandino-Losada A,ForsellY, Lundberg I.Demands,
skill discretion,decision authority and socialclimate at
work as determinants ofmajor depression in a 3-year
follow-up study. Int Arch Occup Environ Health
2013;86:591-605.Epub 2012 Jul 4.
Godin I,Kittel F,Coppieters Y,Siegrist J.A prospective
studyof cumulativejob stressin relation to mental
health.BMC Public Health 2005;5:67.
Goodman WB,Crouter AC.Longitudinal associations
between maternalwork stress,negativework-family
spillover,and depressivesymptoms.Fam Relat2009;
58:245-58.
Griffin JM, Fuhrer R,Stansfeld SA,MarmotM. The
importance of low control at work and home on depres-
sion and anxiety:do these effects vary by gender and so-
cial class? Soc Sci Med 2002;54:783-98.
Grynderup MB,Mors O, Hansen AM,Andersen JH,
Bonde JP,Kaergaard A,et al.Work-unit measures of or-
ganisationaljustice and risk of depression –a 2-year co-
hort study.Occup Environ Med 2013;70:380-5.
Grynderup MB,Mors O, Hansen AM,Andersen JH,
Bonde JP,Kaergaard A,et al.A two-year follow-up study
of risk of depression according to work-unit measures of
psychologicaldemandsand decision latitude.Scand J
Work Environ Health 2012;38:527-36.
Grzywacz JG,QuandtSA, Chen H,Isom S,Kiang L,
VallejosQ, et al. Depressive symptomsamong Latino
farm workers acrossthe agriculturalseason:structural
and situationalinfluences.Cultur Divers Ethnic Minor
Psychol 2010;16:335-43.
Ibrahim S,Smith P,Muntaner C.A multi-group cross-
lagged analysisof work stressorsand health using a
Canadian National sample.Soc Sci Med 2009;68:49-59.
Jensen HK,Wieclaw J,Munch-Hansen T,Thulstrup
AM, Bonde JP. Does dissatisfaction with psychosocial
work climate predictdepressive,anxiety and substance
abuse disorders? A prospective study ofDanish public
serviceemployees.J EpidemiolCommunityHealth
2010;64:796-801.
Kivimaki M, Vahtera J, Elovainio M, Virtanen M, Siegrist
J. Effort-reward imbalance,proceduralinjustice and rela-
tionalinjustice as psychosocial predictors of health:com-
plementary orredundantmodels? Occup Environ Med
2007;64:659-65.
Kivimäki M, Virtanen M, Vartia M, Elovainio M,
Vahtera J,Keltikangas-Jarvinen L.Workplace bullying
and the risk ofcardiovascular disease and depression.
Occup Environ Med 2003;60:779- 83.
Theorell et al.BMC Public Health (2015) 15:738 Page 11 of 14
ably influenced by effective organizationalinterventions.
An importantstep in this research field would be the
launching ofgood evaluations ofpsychosocialinterven-
tions.For some kinds of working conditions that are de-
veloping in the modern working world,new research on
depressive symptoms will be needed.
Appendix
Studies judged to be of high or medium high quality
Ahola K,Hakanen J.Job strain,burnout,and depres-
sive symptoms:a prospective study among dentists.J
Affect Disord 2007;104:103-10.
Andrea H,Bultmann U,van Amelsvoort LG,Kant Y.
The incidence ofanxiety and depression among em-
ployees – the role ofpsychosocialwork characteristics.
Depress Anxiety 2009;26:1040-8.
BeselerCL, StallonesL, Hoppin JA, Alavanja MC,
Blair A, Keefe T,et al.Depression and pesticide expo-
sures among private pesticide applicators enrolled in
the AgriculturalHealth Study.Environ Health Per-
spect 2008;116:1713-9.
Bonde JP,Munch-Hansen T,WieclawJ,Westergaard-
Nielsen N,Agerbo E.Psychosocialwork environment
and antidepressantmedication:a prospectivecohort
study.BMC Public Health 2009;9:262.
Burgard SA,Brand JE,House JS.Perceived job inse-
curity and worker health in the United States.Soc Sci
Med 2009;69:777-85.
Clays E,De Bacquer D,Leynen F,Kornitzer M,Kittel F,
De BackerG. Job stressand depression symptomsin
middle-aged workers – prospective results from the Bels-
tress study. Scand J Work Environ Health 2007;33:252-9.
Clumeck N, KempenaersC, Godin I, Dramaix M,
Kornitzer M,Linkowski P,et al.Working conditions pre-
dict incidence of long-term spells of sick leave due to de-
pression:results from the Belstress I prospective study.J
Epidemiol Community Health 2009;63:286-9
DagherRK, McGovern PM,Dowd BE,Lundberg U.
Postpartum depressivesymptomsand the combined
load of paid and unpaid work:a longitudinal analysis.Int
Arch Occup Environ Health 2011;84:735-43.
De Lange AH, Taris TW, KompierMAJ, Houtman
ILD, Bongers PM.The relationships between work char-
acteristicsand mentalhealth:examiningnormal,re-
versed and reciprocalrelationshipsin a 4-wavestudy.
Work & Stress 2004;18:149-66.
de Lange AH,Taris TW,Kompier MA,Houtman IL,
BongersPM. Effectsof stable and changing demand-
controlhistories on worker health.Scand JWork En-
viron Health 2002;28:94-108.
d’Errico A, Cardano M, LandriscinaT,MarinacciC,
Pasian S,Petrelli A,et al.Workplace stress and prescrip-
tion of antidepressantmedications:a prospective study
on a sample ofItalian workers.Int Arch OccupEnviron
Health 2011;84:413-24.
De Santo Iennaco J,Cullen MR,Cantley L,Slade MD,
Fiellin M, Kasl SV. Effectsof externally rated job de-
mand and controlon depression diagnosis claims in an
industrial cohort.Am J Epidemiol 2010;171:303-11.
Fandino-Losada A,ForsellY, Lundberg I.Demands,
skill discretion,decision authority and socialclimate at
work as determinants ofmajor depression in a 3-year
follow-up study. Int Arch Occup Environ Health
2013;86:591-605.Epub 2012 Jul 4.
Godin I,Kittel F,Coppieters Y,Siegrist J.A prospective
studyof cumulativejob stressin relation to mental
health.BMC Public Health 2005;5:67.
Goodman WB,Crouter AC.Longitudinal associations
between maternalwork stress,negativework-family
spillover,and depressivesymptoms.Fam Relat2009;
58:245-58.
Griffin JM, Fuhrer R,Stansfeld SA,MarmotM. The
importance of low control at work and home on depres-
sion and anxiety:do these effects vary by gender and so-
cial class? Soc Sci Med 2002;54:783-98.
Grynderup MB,Mors O, Hansen AM,Andersen JH,
Bonde JP,Kaergaard A,et al.Work-unit measures of or-
ganisationaljustice and risk of depression –a 2-year co-
hort study.Occup Environ Med 2013;70:380-5.
Grynderup MB,Mors O, Hansen AM,Andersen JH,
Bonde JP,Kaergaard A,et al.A two-year follow-up study
of risk of depression according to work-unit measures of
psychologicaldemandsand decision latitude.Scand J
Work Environ Health 2012;38:527-36.
Grzywacz JG,QuandtSA, Chen H,Isom S,Kiang L,
VallejosQ, et al. Depressive symptomsamong Latino
farm workers acrossthe agriculturalseason:structural
and situationalinfluences.Cultur Divers Ethnic Minor
Psychol 2010;16:335-43.
Ibrahim S,Smith P,Muntaner C.A multi-group cross-
lagged analysisof work stressorsand health using a
Canadian National sample.Soc Sci Med 2009;68:49-59.
Jensen HK,Wieclaw J,Munch-Hansen T,Thulstrup
AM, Bonde JP. Does dissatisfaction with psychosocial
work climate predictdepressive,anxiety and substance
abuse disorders? A prospective study ofDanish public
serviceemployees.J EpidemiolCommunityHealth
2010;64:796-801.
Kivimaki M, Vahtera J, Elovainio M, Virtanen M, Siegrist
J. Effort-reward imbalance,proceduralinjustice and rela-
tionalinjustice as psychosocial predictors of health:com-
plementary orredundantmodels? Occup Environ Med
2007;64:659-65.
Kivimäki M, Virtanen M, Vartia M, Elovainio M,
Vahtera J,Keltikangas-Jarvinen L.Workplace bullying
and the risk ofcardiovascular disease and depression.
Occup Environ Med 2003;60:779- 83.
Theorell et al.BMC Public Health (2015) 15:738 Page 11 of 14
KouvonenA, OksanenT, VahteraJ, StaffordM,
Wilkinson R,SchneiderJ, et al. Low workplace social
capitalas a predictor ofdepression:the Finnish Public
Sector Study.Am J Epidemiol 2008;167:1143-51.
Lang J,Bliese PD,Lang JW,Adler AB.Work gets un-
fair for the depressed:cross-lagged relationsbetween
organizationaljustice perceptions and depressive symp-
toms.J Appl Psychol 2011;96:602-18.
Levin A, Besser A, Albert L, Smith D, Neria Y. The effect
of attorneys’work with trauma- exposed clients on PTSD
symptoms,depression,and functional impairment:a cross-
lagged longitudinal study. Law Hum Behav 2012;36:538-47.
Magnusson Hanson LL,TheorellT, Bech P,Rugulies
R, Burr H, Hyde M,et al. Psychosocialworking condi-
tions and depressivesymptomsamongSwedish em-
ployees.Int Arch Occup Environ Health 2009;82:951-60.
Mantyniemi A,Oksanen T,Salo P, Virtanen M,Sjosten
N, Pentti J,et al.Job strain and the risk of disability pen-
sion due to musculoskeletal disorders,depression or cor-
onary heart disease:a prospective cohort study of 69,842
employees.Occup Environ Med 2012;69:574-81.
Niedhammer I,Goldberg M,Leclerc A,BugelI, David
S. Psychosocialfactors at work and subsequentdepres-
sive symptoms in the Gazelcohort.Scand JWork En-
viron Health 1998;24:197-205.
Oksanen T, Kouvonen A, VahteraJ, Virtanen M,
Kivimäki M. Prospectivestudy of workplacesocial
capitaland depression:are verticaland horizontalcom-
ponentsequallyimportant?J EpidemiolCommunity
Health 2010;64:684-9.
Parker SK.Longitudinaleffects oflean production on
employeeoutcomesand the mediatingrole of work
characteristics.J Appl Psychol 2003;88:620-34.
PaternitiS, Niedhammer I,Lang T,ConsoliSM. Psy-
chosocialfactors at work,personality traits and depres-
sive symptoms.Longitudinalresultsfrom the GAZEL
Study.Br J Psychiatry 2002;181:111-7.
PlaisierI, de Bruijn JG, de Graaf R, ten HaveM,
Beekman AT,Penninx BW.The contribution of working
conditions and socialsupport to the onset of depressive
and anxietydisordersamongmale and femaleem-
ployees.Soc Sci Med 2007;64:401-10.
RuguliesR, Aust B, Madsen IE,Burr H, SiegristJ,
Bultmann U.Adverse psychosocialworking conditions
and risk of severe depressive symptoms.Do effects differ
by occupationalgrade? Eur J Public Health 2013;23:415-
20.Epub 2012 Jun 8.
Rugulies R,Madsen IE,Hjarsbech PU,Hogh A, Borg
V, Carneiro IG,et al. Bullying atwork and onsetof a
major depressive episode among Danish female eldercare
workers.Scand J Work Environ Health 2012;38:218-27.
Rugulies R,Thielen K,Nygaard E,Diderichsen F.Job
insecurityand the use of antidepressantmedication
among Danish employees with and without a history of
prolonged unemployment:a 3.5-year follow-up study.J
Epidemiol Community Health 2010;64:75-81.
Rugulies R,Bultmann U,Aust B,Burr H.Psychosocial
work environmentand incidence ofsevere depressive
symptoms:prospective findings from a 5-yearfollow-up
of the Danish work environmentcohortstudy.Am J
Epidemiol 2006;163:877-87.
Schonfeld IS.Stress in 1st-year women teachers:the
contextof socialsupportand coping.GenetSoc Gen
Psychol Monogr 2001;127:133-68.
ShieldsM. Stressand depression in theemployed
population.Health Rep 2006;17:11-29.
ShieldsM. Long working hoursand health.Health
Rep 1999;11:33-48 (Eng);37-55 (Fre).
SinokkiM, Hinkka K,Ahola K,Koskinen S,Kivimäki
M, Honkonen T,et al.The association of socialsupport
at work and in private life with mentalhealth and anti-
depressantuse:the Health 2000 Study.J AffectDisord
2009;115:36-45.
Stansfeld SA,Shipley MJ,Head J,Fuhrer R.Repeated
job strain and the risk ofdepression:longitudinalana-
lyses from the WhitehallII study.Am J Public Health
2012;102:2360-6.
StoetzerU, Ahlberg G, Johansson G,Bergman P,
Hallsten L,ForsellY, et al.Problematic interpersonal re-
lationships at work and depression:a Swedish prospect-
ive cohort study.J Occup Health 2009;51:144-51.
Theorell T, NybergA, LeineweberC, Magnusson
Hanson LL, OxenstiernaG, WesterlundH. Non-
listening and self centered leadership – relationships to
socioeconomic conditions and employee mentalhealth.
PLoS One 2012;7:e44119.
Wang J,Schmitz N.Does job strain interact with psy-
chosocialfactors outside of the workplace in relation to
the risk of major depression?The CanadianNational
Population Health Survey.Soc Psychiatry Psychiatr Epi-
demiol 2011;46:577-84.
Wang J,Schmitz N,Dewa C,Stansfeld S.Changes in
perceived job strain and the risk of major depression:re-
sults from a population-based longitudinalstudy.Am J
Epidemiol 2009;169:1085- 91.
Wang J.Work stress as a risk factor for major depres-
sive episode(s).Psychol Med 2005;35:865- 71.
Wang J. Perceived work stress and major depressive
episodesin a population ofemployed Canadiansover
18 years old.J Nerv Ment Dis 2004;192:160-3.
Varma A, Marott JL, StoltenbergCD, Wieclaw J,
Kolstad HA,Bonde JP.With long hours of work,might
depression then lurk? A nationwide prospective follow-
up study amongDanish seniormedicalconsultants.
Scand J Work Environ Health 2012;38:418-26.
Weisskopf MG,Moisan F, TzourioC,Rathouz PJ,Elbaz
A. Pesticide exposure and depression among agricultural
workers in France.Am J Epidemiol 2013;178:1051-8.
Theorell et al.BMC Public Health (2015) 15:738 Page 12 of 14
Wilkinson R,SchneiderJ, et al. Low workplace social
capitalas a predictor ofdepression:the Finnish Public
Sector Study.Am J Epidemiol 2008;167:1143-51.
Lang J,Bliese PD,Lang JW,Adler AB.Work gets un-
fair for the depressed:cross-lagged relationsbetween
organizationaljustice perceptions and depressive symp-
toms.J Appl Psychol 2011;96:602-18.
Levin A, Besser A, Albert L, Smith D, Neria Y. The effect
of attorneys’work with trauma- exposed clients on PTSD
symptoms,depression,and functional impairment:a cross-
lagged longitudinal study. Law Hum Behav 2012;36:538-47.
Magnusson Hanson LL,TheorellT, Bech P,Rugulies
R, Burr H, Hyde M,et al. Psychosocialworking condi-
tions and depressivesymptomsamongSwedish em-
ployees.Int Arch Occup Environ Health 2009;82:951-60.
Mantyniemi A,Oksanen T,Salo P, Virtanen M,Sjosten
N, Pentti J,et al.Job strain and the risk of disability pen-
sion due to musculoskeletal disorders,depression or cor-
onary heart disease:a prospective cohort study of 69,842
employees.Occup Environ Med 2012;69:574-81.
Niedhammer I,Goldberg M,Leclerc A,BugelI, David
S. Psychosocialfactors at work and subsequentdepres-
sive symptoms in the Gazelcohort.Scand JWork En-
viron Health 1998;24:197-205.
Oksanen T, Kouvonen A, VahteraJ, Virtanen M,
Kivimäki M. Prospectivestudy of workplacesocial
capitaland depression:are verticaland horizontalcom-
ponentsequallyimportant?J EpidemiolCommunity
Health 2010;64:684-9.
Parker SK.Longitudinaleffects oflean production on
employeeoutcomesand the mediatingrole of work
characteristics.J Appl Psychol 2003;88:620-34.
PaternitiS, Niedhammer I,Lang T,ConsoliSM. Psy-
chosocialfactors at work,personality traits and depres-
sive symptoms.Longitudinalresultsfrom the GAZEL
Study.Br J Psychiatry 2002;181:111-7.
PlaisierI, de Bruijn JG, de Graaf R, ten HaveM,
Beekman AT,Penninx BW.The contribution of working
conditions and socialsupport to the onset of depressive
and anxietydisordersamongmale and femaleem-
ployees.Soc Sci Med 2007;64:401-10.
RuguliesR, Aust B, Madsen IE,Burr H, SiegristJ,
Bultmann U.Adverse psychosocialworking conditions
and risk of severe depressive symptoms.Do effects differ
by occupationalgrade? Eur J Public Health 2013;23:415-
20.Epub 2012 Jun 8.
Rugulies R,Madsen IE,Hjarsbech PU,Hogh A, Borg
V, Carneiro IG,et al. Bullying atwork and onsetof a
major depressive episode among Danish female eldercare
workers.Scand J Work Environ Health 2012;38:218-27.
Rugulies R,Thielen K,Nygaard E,Diderichsen F.Job
insecurityand the use of antidepressantmedication
among Danish employees with and without a history of
prolonged unemployment:a 3.5-year follow-up study.J
Epidemiol Community Health 2010;64:75-81.
Rugulies R,Bultmann U,Aust B,Burr H.Psychosocial
work environmentand incidence ofsevere depressive
symptoms:prospective findings from a 5-yearfollow-up
of the Danish work environmentcohortstudy.Am J
Epidemiol 2006;163:877-87.
Schonfeld IS.Stress in 1st-year women teachers:the
contextof socialsupportand coping.GenetSoc Gen
Psychol Monogr 2001;127:133-68.
ShieldsM. Stressand depression in theemployed
population.Health Rep 2006;17:11-29.
ShieldsM. Long working hoursand health.Health
Rep 1999;11:33-48 (Eng);37-55 (Fre).
SinokkiM, Hinkka K,Ahola K,Koskinen S,Kivimäki
M, Honkonen T,et al.The association of socialsupport
at work and in private life with mentalhealth and anti-
depressantuse:the Health 2000 Study.J AffectDisord
2009;115:36-45.
Stansfeld SA,Shipley MJ,Head J,Fuhrer R.Repeated
job strain and the risk ofdepression:longitudinalana-
lyses from the WhitehallII study.Am J Public Health
2012;102:2360-6.
StoetzerU, Ahlberg G, Johansson G,Bergman P,
Hallsten L,ForsellY, et al.Problematic interpersonal re-
lationships at work and depression:a Swedish prospect-
ive cohort study.J Occup Health 2009;51:144-51.
Theorell T, NybergA, LeineweberC, Magnusson
Hanson LL, OxenstiernaG, WesterlundH. Non-
listening and self centered leadership – relationships to
socioeconomic conditions and employee mentalhealth.
PLoS One 2012;7:e44119.
Wang J,Schmitz N.Does job strain interact with psy-
chosocialfactors outside of the workplace in relation to
the risk of major depression?The CanadianNational
Population Health Survey.Soc Psychiatry Psychiatr Epi-
demiol 2011;46:577-84.
Wang J,Schmitz N,Dewa C,Stansfeld S.Changes in
perceived job strain and the risk of major depression:re-
sults from a population-based longitudinalstudy.Am J
Epidemiol 2009;169:1085- 91.
Wang J.Work stress as a risk factor for major depres-
sive episode(s).Psychol Med 2005;35:865- 71.
Wang J. Perceived work stress and major depressive
episodesin a population ofemployed Canadiansover
18 years old.J Nerv Ment Dis 2004;192:160-3.
Varma A, Marott JL, StoltenbergCD, Wieclaw J,
Kolstad HA,Bonde JP.With long hours of work,might
depression then lurk? A nationwide prospective follow-
up study amongDanish seniormedicalconsultants.
Scand J Work Environ Health 2012;38:418-26.
Weisskopf MG,Moisan F, TzourioC,Rathouz PJ,Elbaz
A. Pesticide exposure and depression among agricultural
workers in France.Am J Epidemiol 2013;178:1051-8.
Theorell et al.BMC Public Health (2015) 15:738 Page 12 of 14
Wieclaw J,Agerbo E,Mortensen PB,Burr H,Tuchsen
F, Bonde JP.Psychosocialworking conditionsand the
risk of depression and anxiety disorders in the Danish
workforce.BMC Public Health 2008;8:280.
Wieclaw J,Agerbo E,Mortensen PB,Burr H,Tuchsen
F, Bonde JP.Work related violence and threats and the
risk of depression and stressdisorders.J Epidemiol
Community Health 2006;60:771-5.
Virtanen M,Stansfeld SA,Fuhrer R,Ferrie JE,Kivimäki
M. Overtime work as a predictor of major depressive epi-
sode:a 5-year follow-up ofthe WhitehallII study.PLoS
One 2012;7:e30719.
Virtanen M,Ferrie JE,Singh-Manoux A,Shipley MJ,
Stansfeld SA,Marmot MG, et al. Long working hours and
symptoms of anxiety and depression: a 5-year follow-up of
the Whitehall II study. Psychol Med 2011;41:2485-94.
Virtanen M,Batty GD,PenttiJ, Vahtera J,Oksanen T,
Tuisku K,et al.Patient overcrowding in hospitalwards
as a predictorof diagnosis-specificmentaldisorders
among staff:a 2-year prospective cohortstudy.J Clin-
Psychiatry 2010;71:1308-12.
Virtanen M, Honkonen T, KivimäkiM, Ahola K,
Vahtera J,Aromaa A,et al.Work stress,mentalhealth
and antidepressant medication findings from the Health
2000 Study.J Affect Disord 2007;98:189-97.
Ybema JF,van den BosK. Effectsof organizational
justice on depressive symptoms and sickness absence:a
longitudinal perspective.Soc Sci Med 2010;70:1609-17.
YlipaavalniemiJ, KivimakiM, Elovainio M,Virtanen
M, Keltikangas-Jarvinen L,Vahtera J.Psychosocialwork
characteristics and incidence of newly diagnosed depres-
sion: a prospectivecohort study of three different
models.Soc Sci Med 2005;61:111-22.
Competing interests
The authors declare that they have no competing interests.
Authors’contributions
TT was chairman of the expert committee and has conceptualized and
written large parts of the manuscript.GA,LTB,TG,AH,CH (1),IM and IS have
allcontributed substantially to the expert panelwork and have made
important comments to the manuscript.CH (2) has performed most of the
statisticalwork and contributed both to the conceptualizing and the writing
of the manuscript.Allauthors read and approved the finalmanuscript.
Authors’information
The authors deliberately represent a diversity of academic fields,namely
psychiatry (LTB,IS,IM),work psychology (GA),occupationalepidemiology
(AH,CH),stress research (TT) and generalpractice (TG).
Acknowledgements
This study has been funded by the Swedish Councilof Health Technology
Assessment.The Swedish Government has had no role in the work,neither
in the scientific work itself nor in the writing of the article.The review has
been funded by the Swedish Councilof Health Technology Assessment.
Author details
1Stress Research Institute,Stockholm University,SE-106 91 Stockholm,
Sweden.2Department of Neuroscience,Karolinska Institutet,SE- 171 77
Stockholm,Sweden.3Department of Public Health and ClinicalMedicine,
Department of socialmedicine,Umeå University Hospital,SE-901 85 Umeå,
Sweden.4Department of Psychology,Stockholm University,SE-106 91
Stockholm,Sweden.5Division of Psychiatry,Lund University,SE-221 00 Lund,
Sweden.6South Health Care Centre,SE-761 46 Norrtälje,Sweden.7Division of
Occupationalmedicine,Institute for EnvironmentalMedicine,Karolinska
Institutet,SE-171 77 Stockholm,Sweden.8Division of Psychiatry,Linköping
University,SE-581 83 Linköping,Sweden.9Department of Psychiatry and
Neurochemistry,Göteborg University,SE-411 24 Stockholm,Sweden.
10
Swedish Councilof Health Technology Assessment,SE-103 59 Stockholm,
Sweden.
Received:7 March 2015 Accepted:19 June 2015
References
1. Bonde JP.Psychosocial factors at work and risk of depression:a systematic
review of the epidemiological evidence.Occup Environ Med.2008;65:438–45.
2. Netterström B,ConradM BP,Fink P,Olsen O,Rugulies R,Stansfeld S.The
relation between work-related psychosocialfactors and the development of
depression.EpidemiolRev.2008;30:118–32.
3. Siegrist J.Chronic psychosocialstress at work and risk of depression:
evidence from prospective studies.Eur Arch Psychiatry Clin Neurosci.
2008;258(suppl):115–9.
4. Michie S,Williams S.Reducing work related psychologicalillhealth and
sickness absence:a systematic literature review.Occup Environ Med.
2003;60:3–9.
5. Egan M,Bambra C,Thomas S,Petticrew M,Whitehead M,Thomson H.The
psychosocialand health effects of workplace reorganisation.A systematic
review of organisational-levelinterventions that aim to increase employee
control.J EpidemiolCommunity Health.2007;61:945–54.
6. Woo J-M,Postolache TT.The impact of work environment on mood
disorders and suicide:Evidence and implications.Int J DisabilHum Dev.
2008;7:185–200.
7. Freire C,Koifman S.Pesticides,depression and suicide:A systematic review
of the epidemiologicalevidence.Int J Hygiene and Environ Health.
2013;216:445–60.
8. Niuwenhuijsen N,Bruinvelds D,Frings-Dresen M.Psychosocialwork
environment and stress-related disorders,a systematic review.
Occup Med.2010;60:277–86.
9. Guyatt G,Oxman AD,AklEA,Kunz R,Vist G,Brozek J,et al.GRADE
guidelines:1.Introduction—GRADE evidence profiles and summary of
findings tables.J Clin Epidemiol.2011;64(4):383–94.
10. Assessment and Evidence.http://www.sbu.se/en/Assessment-and-Evidence/
11. Jauregui M,Schnall PL.Work,psychosocial stressors and the bottom line.In
Schnall PL,Dobson M and Rosskam E (eds) Unhealthy Work.Amityville,NY:
Baywood Publ;2009.
12. The Grade Approach.http://handbook.cochrane.org/chapter_12/12_2_1_the
_grade_approach.htm
13. Virtanen M,Batty GD,PenttiJ, Vahtera J,Oksanen T,Tuisku K,et al.Patient
overcrowding in hospitalwards as a predictor of diagnosis-specific mental
disorders among staff:a 2-year prospective cohort study.J Clin Psychiatry.
2010;71:1308–12.
14. Shields M.Stress and depression in the employed population.Health Rep.
2006;17:11–29.
15. Stansfeld SA,Shipley MJ,Head J,Fuhrer R.Repeated job strain and the risk
of depression:longitudinalanalyses from the WhitehallII study.Am J Public
Health.2012;102:2360–6.
16. de Lange AH,Taris TW,Kompier MA,Houtman IL,Bongers PM.Effects of
stable and changing demand-controlhistories on worker health.Scand J
Work Environ Health.2002;28:94–108.
17. Wang J,Schmitz N,Dewa C,Stansfeld S.Changes in perceived job strain and
the risk of major depression:results from a population-based longitudinal
study.Am J Epidemiol.2009;169:1085–91.
18. Bailey TS,Dollard MF,Richards PA.A nationalstandard for psychosocial
safety climate (PSC):PSC 41 as the benchmark for low risk of job strain and
depressive symptoms.J Occup Health Psychol.2015;20(1):15–26.
doi:10.1037/a0038166.Epub 2014 Oct 27.
19. Grzywacz JG,Alterman T,Gabbard S,Shen R,Nakamoto J,CarrollDJ,et al.
Job control,psychologicaldemand,and farmworker health:evidence from
the nationalagriculturalworkers survey.J Occup Environ Med.
2014;56(1):66–71.doi:10.1097/JOM.0000000000000025.
Theorell et al.BMC Public Health (2015) 15:738 Page 13 of 14
F, Bonde JP.Psychosocialworking conditionsand the
risk of depression and anxiety disorders in the Danish
workforce.BMC Public Health 2008;8:280.
Wieclaw J,Agerbo E,Mortensen PB,Burr H,Tuchsen
F, Bonde JP.Work related violence and threats and the
risk of depression and stressdisorders.J Epidemiol
Community Health 2006;60:771-5.
Virtanen M,Stansfeld SA,Fuhrer R,Ferrie JE,Kivimäki
M. Overtime work as a predictor of major depressive epi-
sode:a 5-year follow-up ofthe WhitehallII study.PLoS
One 2012;7:e30719.
Virtanen M,Ferrie JE,Singh-Manoux A,Shipley MJ,
Stansfeld SA,Marmot MG, et al. Long working hours and
symptoms of anxiety and depression: a 5-year follow-up of
the Whitehall II study. Psychol Med 2011;41:2485-94.
Virtanen M,Batty GD,PenttiJ, Vahtera J,Oksanen T,
Tuisku K,et al.Patient overcrowding in hospitalwards
as a predictorof diagnosis-specificmentaldisorders
among staff:a 2-year prospective cohortstudy.J Clin-
Psychiatry 2010;71:1308-12.
Virtanen M, Honkonen T, KivimäkiM, Ahola K,
Vahtera J,Aromaa A,et al.Work stress,mentalhealth
and antidepressant medication findings from the Health
2000 Study.J Affect Disord 2007;98:189-97.
Ybema JF,van den BosK. Effectsof organizational
justice on depressive symptoms and sickness absence:a
longitudinal perspective.Soc Sci Med 2010;70:1609-17.
YlipaavalniemiJ, KivimakiM, Elovainio M,Virtanen
M, Keltikangas-Jarvinen L,Vahtera J.Psychosocialwork
characteristics and incidence of newly diagnosed depres-
sion: a prospectivecohort study of three different
models.Soc Sci Med 2005;61:111-22.
Competing interests
The authors declare that they have no competing interests.
Authors’contributions
TT was chairman of the expert committee and has conceptualized and
written large parts of the manuscript.GA,LTB,TG,AH,CH (1),IM and IS have
allcontributed substantially to the expert panelwork and have made
important comments to the manuscript.CH (2) has performed most of the
statisticalwork and contributed both to the conceptualizing and the writing
of the manuscript.Allauthors read and approved the finalmanuscript.
Authors’information
The authors deliberately represent a diversity of academic fields,namely
psychiatry (LTB,IS,IM),work psychology (GA),occupationalepidemiology
(AH,CH),stress research (TT) and generalpractice (TG).
Acknowledgements
This study has been funded by the Swedish Councilof Health Technology
Assessment.The Swedish Government has had no role in the work,neither
in the scientific work itself nor in the writing of the article.The review has
been funded by the Swedish Councilof Health Technology Assessment.
Author details
1Stress Research Institute,Stockholm University,SE-106 91 Stockholm,
Sweden.2Department of Neuroscience,Karolinska Institutet,SE- 171 77
Stockholm,Sweden.3Department of Public Health and ClinicalMedicine,
Department of socialmedicine,Umeå University Hospital,SE-901 85 Umeå,
Sweden.4Department of Psychology,Stockholm University,SE-106 91
Stockholm,Sweden.5Division of Psychiatry,Lund University,SE-221 00 Lund,
Sweden.6South Health Care Centre,SE-761 46 Norrtälje,Sweden.7Division of
Occupationalmedicine,Institute for EnvironmentalMedicine,Karolinska
Institutet,SE-171 77 Stockholm,Sweden.8Division of Psychiatry,Linköping
University,SE-581 83 Linköping,Sweden.9Department of Psychiatry and
Neurochemistry,Göteborg University,SE-411 24 Stockholm,Sweden.
10
Swedish Councilof Health Technology Assessment,SE-103 59 Stockholm,
Sweden.
Received:7 March 2015 Accepted:19 June 2015
References
1. Bonde JP.Psychosocial factors at work and risk of depression:a systematic
review of the epidemiological evidence.Occup Environ Med.2008;65:438–45.
2. Netterström B,ConradM BP,Fink P,Olsen O,Rugulies R,Stansfeld S.The
relation between work-related psychosocialfactors and the development of
depression.EpidemiolRev.2008;30:118–32.
3. Siegrist J.Chronic psychosocialstress at work and risk of depression:
evidence from prospective studies.Eur Arch Psychiatry Clin Neurosci.
2008;258(suppl):115–9.
4. Michie S,Williams S.Reducing work related psychologicalillhealth and
sickness absence:a systematic literature review.Occup Environ Med.
2003;60:3–9.
5. Egan M,Bambra C,Thomas S,Petticrew M,Whitehead M,Thomson H.The
psychosocialand health effects of workplace reorganisation.A systematic
review of organisational-levelinterventions that aim to increase employee
control.J EpidemiolCommunity Health.2007;61:945–54.
6. Woo J-M,Postolache TT.The impact of work environment on mood
disorders and suicide:Evidence and implications.Int J DisabilHum Dev.
2008;7:185–200.
7. Freire C,Koifman S.Pesticides,depression and suicide:A systematic review
of the epidemiologicalevidence.Int J Hygiene and Environ Health.
2013;216:445–60.
8. Niuwenhuijsen N,Bruinvelds D,Frings-Dresen M.Psychosocialwork
environment and stress-related disorders,a systematic review.
Occup Med.2010;60:277–86.
9. Guyatt G,Oxman AD,AklEA,Kunz R,Vist G,Brozek J,et al.GRADE
guidelines:1.Introduction—GRADE evidence profiles and summary of
findings tables.J Clin Epidemiol.2011;64(4):383–94.
10. Assessment and Evidence.http://www.sbu.se/en/Assessment-and-Evidence/
11. Jauregui M,Schnall PL.Work,psychosocial stressors and the bottom line.In
Schnall PL,Dobson M and Rosskam E (eds) Unhealthy Work.Amityville,NY:
Baywood Publ;2009.
12. The Grade Approach.http://handbook.cochrane.org/chapter_12/12_2_1_the
_grade_approach.htm
13. Virtanen M,Batty GD,PenttiJ, Vahtera J,Oksanen T,Tuisku K,et al.Patient
overcrowding in hospitalwards as a predictor of diagnosis-specific mental
disorders among staff:a 2-year prospective cohort study.J Clin Psychiatry.
2010;71:1308–12.
14. Shields M.Stress and depression in the employed population.Health Rep.
2006;17:11–29.
15. Stansfeld SA,Shipley MJ,Head J,Fuhrer R.Repeated job strain and the risk
of depression:longitudinalanalyses from the WhitehallII study.Am J Public
Health.2012;102:2360–6.
16. de Lange AH,Taris TW,Kompier MA,Houtman IL,Bongers PM.Effects of
stable and changing demand-controlhistories on worker health.Scand J
Work Environ Health.2002;28:94–108.
17. Wang J,Schmitz N,Dewa C,Stansfeld S.Changes in perceived job strain and
the risk of major depression:results from a population-based longitudinal
study.Am J Epidemiol.2009;169:1085–91.
18. Bailey TS,Dollard MF,Richards PA.A nationalstandard for psychosocial
safety climate (PSC):PSC 41 as the benchmark for low risk of job strain and
depressive symptoms.J Occup Health Psychol.2015;20(1):15–26.
doi:10.1037/a0038166.Epub 2014 Oct 27.
19. Grzywacz JG,Alterman T,Gabbard S,Shen R,Nakamoto J,CarrollDJ,et al.
Job control,psychologicaldemand,and farmworker health:evidence from
the nationalagriculturalworkers survey.J Occup Environ Med.
2014;56(1):66–71.doi:10.1097/JOM.0000000000000025.
Theorell et al.BMC Public Health (2015) 15:738 Page 13 of 14
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
20. Niedhammer I,Malard L,Chastang J-F.Occupationalfactors and subsequent
depressive and generalized anxiety disorders in the prospective French SIP
study.BMC Public Health.http://www.biomedcentral.com/1471-2458/15/200
21. JuvaniA,Oksanen T,Salo P,Virtanen M,KivimäkiM,PenttiJ, et al.Effort-
reward imbalance as a risk factor for disability pension:the Finnish Public
Sector Study.Scand J Work Environ Health.2014;40(3):266–77.doi:10.5271/
sjweh.3402.Epub 2013 Nov 18.
22. TheorellT,Hammarström A,Gustafsson PE,Magnusson Hanson L,Janlert U,
Westerlund H.Job strain and depressive symptoms in men and women:a
prospective study of the working population in Sweden.J Epidemiol
Community Health.2014;68:78–82.
23. Wang J,Patten SB,Currie S,Sareen J,Schmitz N.A population-based
longitudinalstudy on work environmentalfactors and the risk of major
depressive disorder.Am J Epidemiol.2012;176(1):52–9.
24. Karasek RA,TheorellT.Healthy Work:stress,productivity and the
reconstruction of working life.New York:Basic Books;1990.
25. TheorellT,Hasselhorn HM.On cross-sectionalquestionnaire studies of
relationships between psychosocialconditions at work and health – are
they reliable? Int Arch Occup Environ Health.2005;78:517–22.
26. Wang J,Schmitz N.Does job strain interact with psychosocialfactors
outside of the workplace in relation to the risk of major depression? The
Canadian NationalPopulation Health Survey.Soc Psychiatry Epidemiol.
2011;46:577–84.
27. Bond FW,Bunce D.Job controlmediates change in a work reorganization
intervention for stress reduction.J Occup Health Psychol.2001;6:290–302.
28. Bourbonnais R,Brisson C,Vézina M.Long-term effects of an intervention on
psychosocialwork factors among healthcare professionals in a hospital
setting.Occup Environ Med.2011;68(7):479–86.
29. TheorellT,Emdad R,Arnetz B,Weingarten AM.Employee effects of an
educationalprogram for managers at an insurance company.Psychosom
Med.2001;63(5):724–33.
30. Kompier MA,Aust B,von den Berg AM,Siegrist J.Stress prevention in bus
drivers:evaluation of 13 naturalexperiments.Occup Health Psychol.
2000;5(1):11–31.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Theorell et al.BMC Public Health (2015) 15:738 Page 14 of 14
depressive and generalized anxiety disorders in the prospective French SIP
study.BMC Public Health.http://www.biomedcentral.com/1471-2458/15/200
21. JuvaniA,Oksanen T,Salo P,Virtanen M,KivimäkiM,PenttiJ, et al.Effort-
reward imbalance as a risk factor for disability pension:the Finnish Public
Sector Study.Scand J Work Environ Health.2014;40(3):266–77.doi:10.5271/
sjweh.3402.Epub 2013 Nov 18.
22. TheorellT,Hammarström A,Gustafsson PE,Magnusson Hanson L,Janlert U,
Westerlund H.Job strain and depressive symptoms in men and women:a
prospective study of the working population in Sweden.J Epidemiol
Community Health.2014;68:78–82.
23. Wang J,Patten SB,Currie S,Sareen J,Schmitz N.A population-based
longitudinalstudy on work environmentalfactors and the risk of major
depressive disorder.Am J Epidemiol.2012;176(1):52–9.
24. Karasek RA,TheorellT.Healthy Work:stress,productivity and the
reconstruction of working life.New York:Basic Books;1990.
25. TheorellT,Hasselhorn HM.On cross-sectionalquestionnaire studies of
relationships between psychosocialconditions at work and health – are
they reliable? Int Arch Occup Environ Health.2005;78:517–22.
26. Wang J,Schmitz N.Does job strain interact with psychosocialfactors
outside of the workplace in relation to the risk of major depression? The
Canadian NationalPopulation Health Survey.Soc Psychiatry Epidemiol.
2011;46:577–84.
27. Bond FW,Bunce D.Job controlmediates change in a work reorganization
intervention for stress reduction.J Occup Health Psychol.2001;6:290–302.
28. Bourbonnais R,Brisson C,Vézina M.Long-term effects of an intervention on
psychosocialwork factors among healthcare professionals in a hospital
setting.Occup Environ Med.2011;68(7):479–86.
29. TheorellT,Emdad R,Arnetz B,Weingarten AM.Employee effects of an
educationalprogram for managers at an insurance company.Psychosom
Med.2001;63(5):724–33.
30. Kompier MA,Aust B,von den Berg AM,Siegrist J.Stress prevention in bus
drivers:evaluation of 13 naturalexperiments.Occup Health Psychol.
2000;5(1):11–31.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Theorell et al.BMC Public Health (2015) 15:738 Page 14 of 14
1 out of 14
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.