Report on Work Placement
VerifiedAdded on 2023/01/13
|25
|5964
|1
AI Summary
This report provides an in-depth analysis of work placement, focusing on primary care reform in Ontario, the number of PC groups operating, the description of PC groups and their mode of operations, interview sessions, and other underway PC reforms. It also includes an interview with an African origin person and a comparison of the healthcare system in Canada and Africa. The report concludes with recommendations for change and personal opinions.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running Head: WORK PLACEMENT
Topic- Report on work placement
Student name
University name
Author notes
Topic- Report on work placement
Student name
University name
Author notes
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

WORK PLACEMENT
TABLE OF CONTENTS
Answer to question 1.......................................................................................................................3
Research of Primary Care (PC) reform in Ontario province.......................................................3
Number of PC groups operating..................................................................................................4
Description of the setting up of PC groups and their mode of operations...................................4
Interview session and other underway PC reforms......................................................................7
Answer to question 2.......................................................................................................................8
Interview with a different cultural people....................................................................................8
Comparison of healthcare system in Canada and Africa.............................................................8
Identification and resolution of problems....................................................................................9
Recommendations for change and personal opinions................................................................10
Answer to question 3.....................................................................................................................11
Layout of office and reception areas..........................................................................................11
Change required in the layout....................................................................................................12
Designing an ideal health office layout......................................................................................12
References......................................................................................................................................17
Appendices....................................................................................................................................19
A sample interview form of clients/ patients.............................................................................19
Thank you letter to interviewees................................................................................................20
Confidentiality statement...........................................................................................................21
Agreement and personal information.........................................................................................22
Interview session with an African origin people.......................................................................23
2
TABLE OF CONTENTS
Answer to question 1.......................................................................................................................3
Research of Primary Care (PC) reform in Ontario province.......................................................3
Number of PC groups operating..................................................................................................4
Description of the setting up of PC groups and their mode of operations...................................4
Interview session and other underway PC reforms......................................................................7
Answer to question 2.......................................................................................................................8
Interview with a different cultural people....................................................................................8
Comparison of healthcare system in Canada and Africa.............................................................8
Identification and resolution of problems....................................................................................9
Recommendations for change and personal opinions................................................................10
Answer to question 3.....................................................................................................................11
Layout of office and reception areas..........................................................................................11
Change required in the layout....................................................................................................12
Designing an ideal health office layout......................................................................................12
References......................................................................................................................................17
Appendices....................................................................................................................................19
A sample interview form of clients/ patients.............................................................................19
Thank you letter to interviewees................................................................................................20
Confidentiality statement...........................................................................................................21
Agreement and personal information.........................................................................................22
Interview session with an African origin people.......................................................................23
2
WORK PLACEMENT
PROJECT A
Answer to question 1
Research of Primary Care (PC) reform in Ontario province
Ontario is one of the most innovative provinces in pursuing primary care reform in
Canada. A number of primary care reform models are introduced to improve overall primacy
care support in Ontario. The multi-dimensional and complex structures created inconveniences
in many areas (Chatwood, 2018). The PC framework is based on three governing bodies namely
Primary Health Care, professional autonomy and neo-institutionalism. The PCR models fail to
balance structural and institutional relationships simultaneously. As a result, there is difficulty in
control areas of political, economic and clinical care aspects (Freund et al., 2015). Thus, greatest
amount of reform is required in altering the structural relationship between the medical
associations and the state. Power balance need to be emphasized more in reform areas. The
Ontario government has already invested in huge amount in regard to PC in the province but
deteriorating fiscal position has increased conflicts in regard to organized medicine and
physician budgets and a radical restructuring of the PC was hindered greatly (Hutchison &
Glazier, 2013). But Ontario still stands out among other Canadian provinces and the single-
minded focus of the government on PC is worth praising. The flexibility of the Universal
Medical Care coverage and Saskatoon Agreement has been increased by the PC reform in
Ontario (Jeffords & Jones, 2019). The PC in areas of care transition funding, home care and
coverage of catastrophic drugs has also been reformed greatly. To support reforms in PC changes
in physician remuneration was focused along with additional provinces of bonuses and other
performance-based incentives providence (Marchildon, 2013). This change has direct positive
impact on the number of graduates entering into Primary Care and there is a sharp increase in
3
PROJECT A
Answer to question 1
Research of Primary Care (PC) reform in Ontario province
Ontario is one of the most innovative provinces in pursuing primary care reform in
Canada. A number of primary care reform models are introduced to improve overall primacy
care support in Ontario. The multi-dimensional and complex structures created inconveniences
in many areas (Chatwood, 2018). The PC framework is based on three governing bodies namely
Primary Health Care, professional autonomy and neo-institutionalism. The PCR models fail to
balance structural and institutional relationships simultaneously. As a result, there is difficulty in
control areas of political, economic and clinical care aspects (Freund et al., 2015). Thus, greatest
amount of reform is required in altering the structural relationship between the medical
associations and the state. Power balance need to be emphasized more in reform areas. The
Ontario government has already invested in huge amount in regard to PC in the province but
deteriorating fiscal position has increased conflicts in regard to organized medicine and
physician budgets and a radical restructuring of the PC was hindered greatly (Hutchison &
Glazier, 2013). But Ontario still stands out among other Canadian provinces and the single-
minded focus of the government on PC is worth praising. The flexibility of the Universal
Medical Care coverage and Saskatoon Agreement has been increased by the PC reform in
Ontario (Jeffords & Jones, 2019). The PC in areas of care transition funding, home care and
coverage of catastrophic drugs has also been reformed greatly. To support reforms in PC changes
in physician remuneration was focused along with additional provinces of bonuses and other
performance-based incentives providence (Marchildon, 2013). This change has direct positive
impact on the number of graduates entering into Primary Care and there is a sharp increase in
3
WORK PLACEMENT
their numbers in recent times. Though the reform is still in work-in-process stage in regard to
quality of care providence.
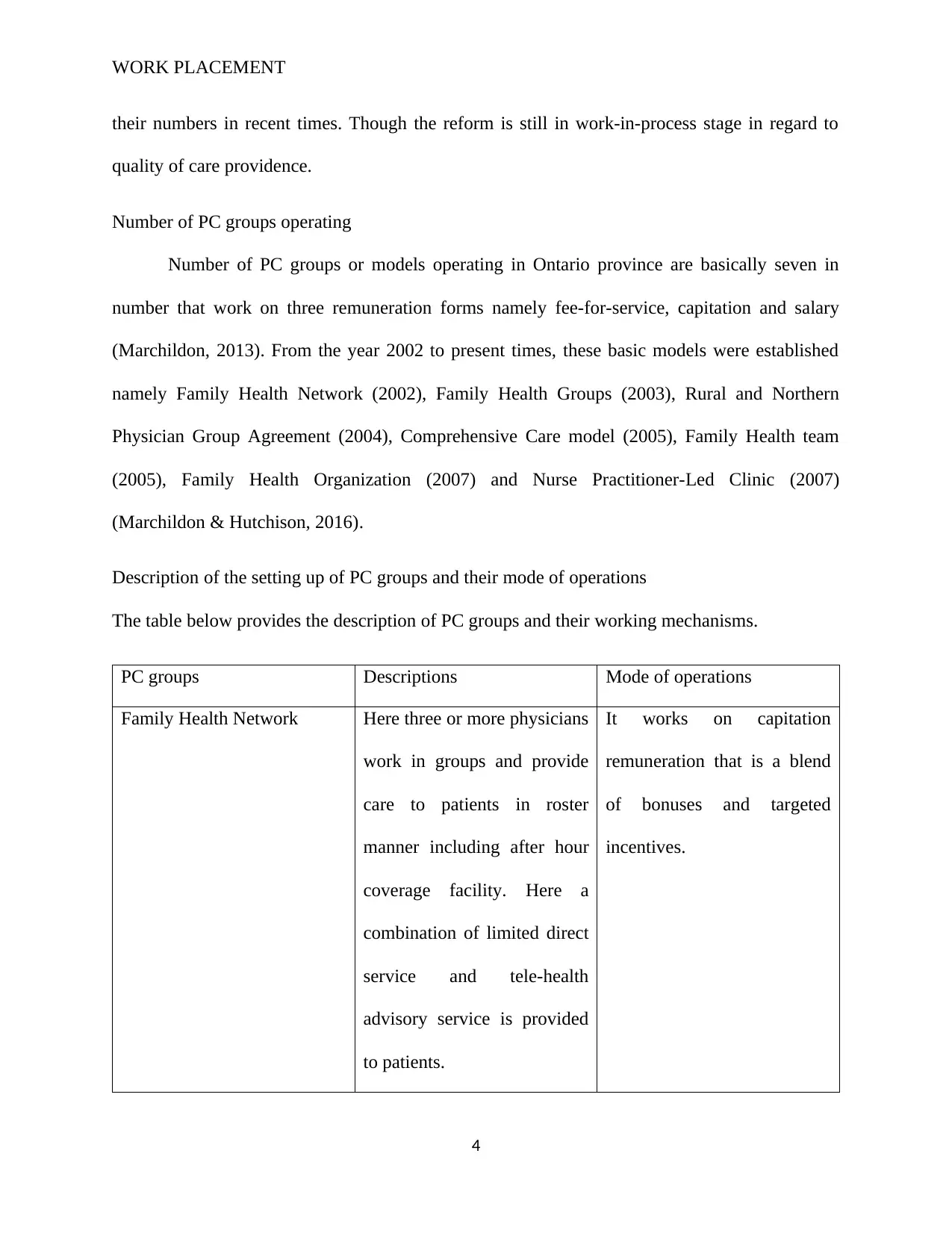
Number of PC groups operating
Number of PC groups or models operating in Ontario province are basically seven in
number that work on three remuneration forms namely fee-for-service, capitation and salary
(Marchildon, 2013). From the year 2002 to present times, these basic models were established
namely Family Health Network (2002), Family Health Groups (2003), Rural and Northern
Physician Group Agreement (2004), Comprehensive Care model (2005), Family Health team
(2005), Family Health Organization (2007) and Nurse Practitioner-Led Clinic (2007)
(Marchildon & Hutchison, 2016).
Description of the setting up of PC groups and their mode of operations
The table below provides the description of PC groups and their working mechanisms.
PC groups Descriptions Mode of operations
Family Health Network Here three or more physicians
work in groups and provide
care to patients in roster
manner including after hour
coverage facility. Here a
combination of limited direct
service and tele-health
advisory service is provided
to patients.
It works on capitation
remuneration that is a blend
of bonuses and targeted
incentives.
4
their numbers in recent times. Though the reform is still in work-in-process stage in regard to
quality of care providence.
Number of PC groups operating
Number of PC groups or models operating in Ontario province are basically seven in
number that work on three remuneration forms namely fee-for-service, capitation and salary
(Marchildon, 2013). From the year 2002 to present times, these basic models were established
namely Family Health Network (2002), Family Health Groups (2003), Rural and Northern
Physician Group Agreement (2004), Comprehensive Care model (2005), Family Health team
(2005), Family Health Organization (2007) and Nurse Practitioner-Led Clinic (2007)
(Marchildon & Hutchison, 2016).
Description of the setting up of PC groups and their mode of operations
The table below provides the description of PC groups and their working mechanisms.
PC groups Descriptions Mode of operations
Family Health Network Here three or more physicians
work in groups and provide
care to patients in roster
manner including after hour
coverage facility. Here a
combination of limited direct
service and tele-health
advisory service is provided
to patients.
It works on capitation
remuneration that is a blend
of bonuses and targeted
incentives.
4
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
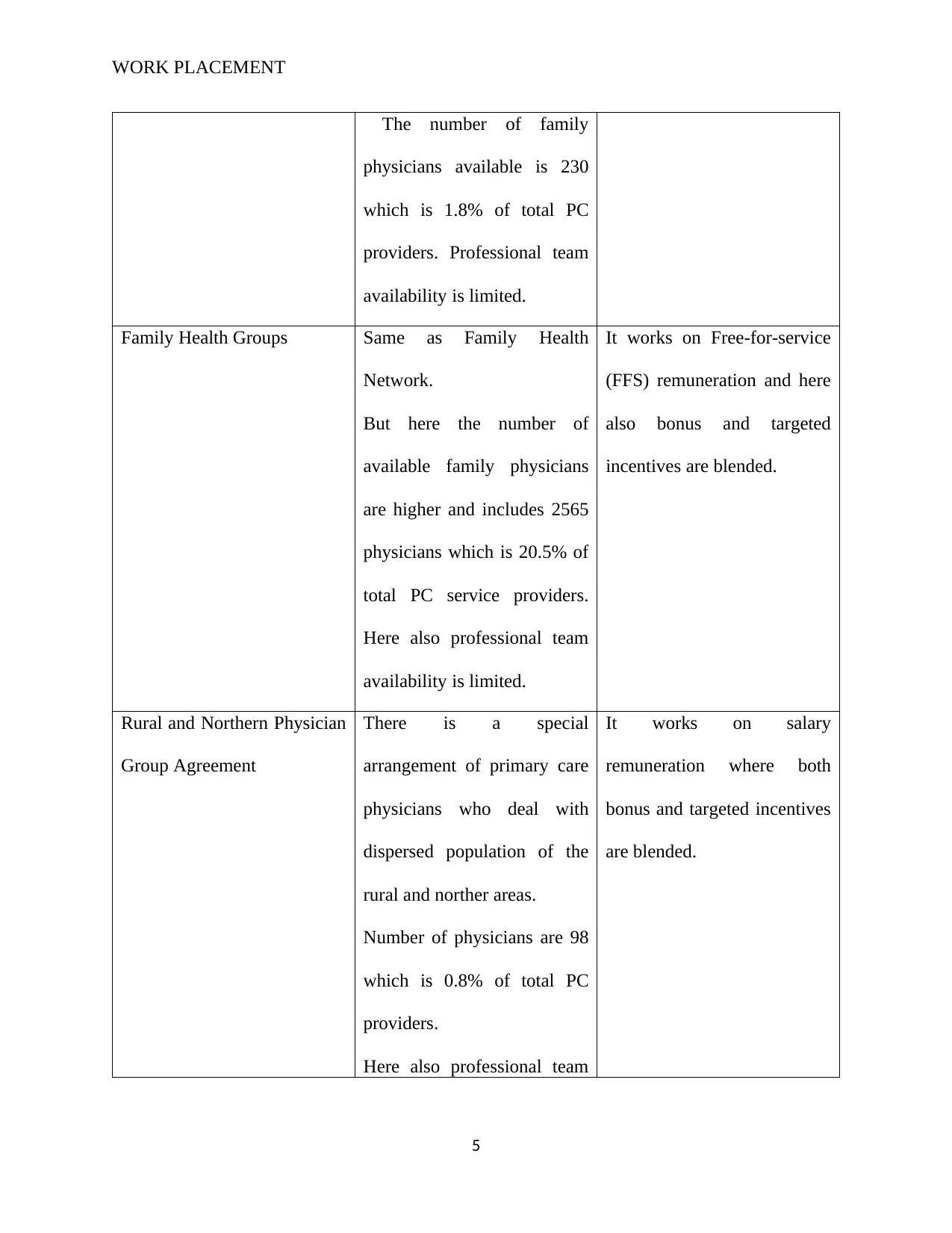
WORK PLACEMENT
The number of family
physicians available is 230
which is 1.8% of total PC
providers. Professional team
availability is limited.
Family Health Groups Same as Family Health
Network.
But here the number of
available family physicians
are higher and includes 2565
physicians which is 20.5% of
total PC service providers.
Here also professional team
availability is limited.
It works on Free-for-service
(FFS) remuneration and here
also bonus and targeted
incentives are blended.
Rural and Northern Physician
Group Agreement
There is a special
arrangement of primary care
physicians who deal with
dispersed population of the
rural and norther areas.
Number of physicians are 98
which is 0.8% of total PC
providers.
Here also professional team
It works on salary
remuneration where both
bonus and targeted incentives
are blended.
5
The number of family
physicians available is 230
which is 1.8% of total PC
providers. Professional team
availability is limited.
Family Health Groups Same as Family Health
Network.
But here the number of
available family physicians
are higher and includes 2565
physicians which is 20.5% of
total PC service providers.
Here also professional team
availability is limited.
It works on Free-for-service
(FFS) remuneration and here
also bonus and targeted
incentives are blended.
Rural and Northern Physician
Group Agreement
There is a special
arrangement of primary care
physicians who deal with
dispersed population of the
rural and norther areas.
Number of physicians are 98
which is 0.8% of total PC
providers.
Here also professional team
It works on salary
remuneration where both
bonus and targeted incentives
are blended.
5
WORK PLACEMENT
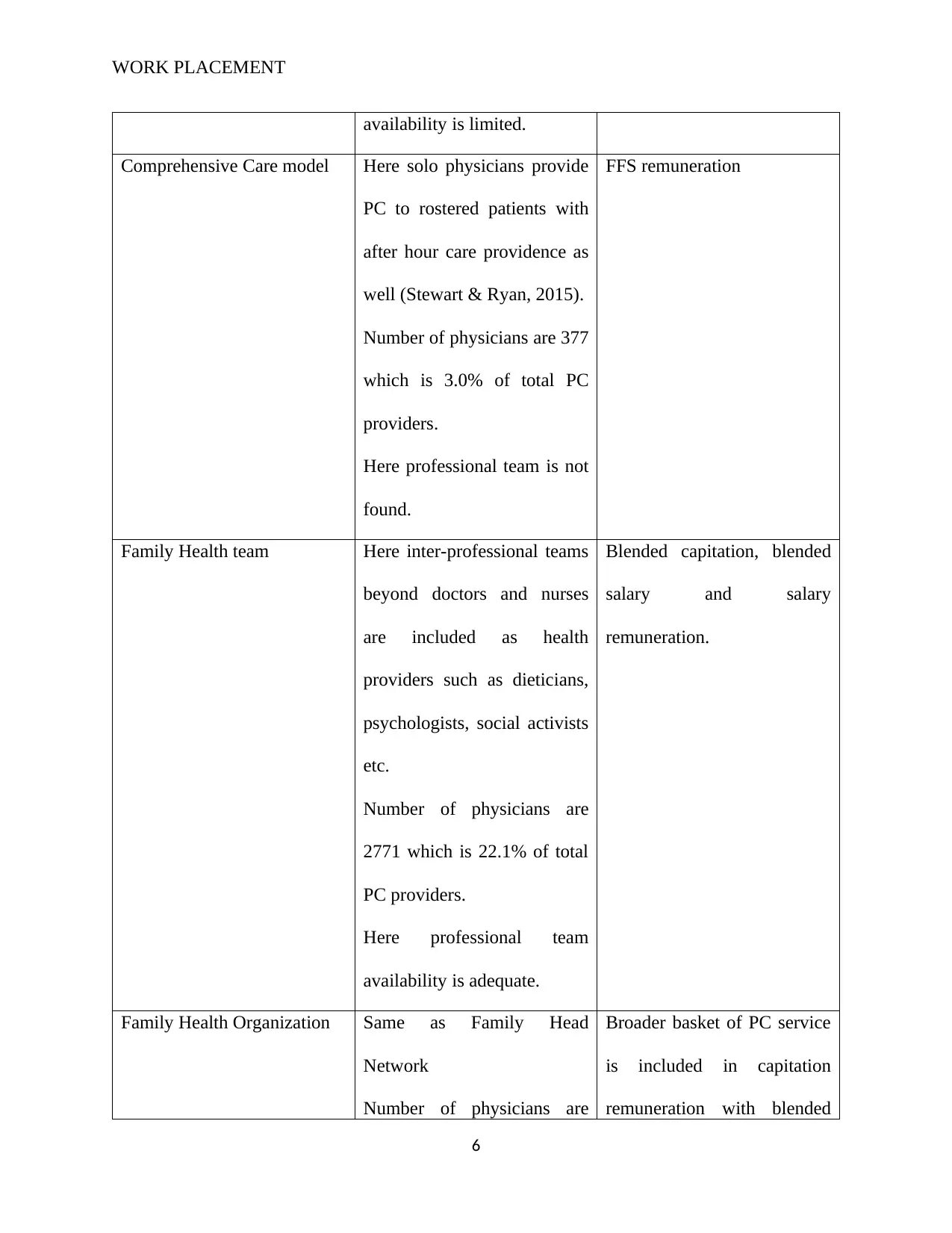
availability is limited.
Comprehensive Care model Here solo physicians provide
PC to rostered patients with
after hour care providence as
well (Stewart & Ryan, 2015).
Number of physicians are 377
which is 3.0% of total PC
providers.
Here professional team is not
found.
FFS remuneration
Family Health team Here inter-professional teams
beyond doctors and nurses
are included as health
providers such as dieticians,
psychologists, social activists
etc.
Number of physicians are
2771 which is 22.1% of total
PC providers.
Here professional team
availability is adequate.
Blended capitation, blended
salary and salary
remuneration.
Family Health Organization Same as Family Head
Network
Number of physicians are
Broader basket of PC service
is included in capitation
remuneration with blended
6
availability is limited.
Comprehensive Care model Here solo physicians provide
PC to rostered patients with
after hour care providence as
well (Stewart & Ryan, 2015).
Number of physicians are 377
which is 3.0% of total PC
providers.
Here professional team is not
found.
FFS remuneration
Family Health team Here inter-professional teams
beyond doctors and nurses
are included as health
providers such as dieticians,
psychologists, social activists
etc.
Number of physicians are
2771 which is 22.1% of total
PC providers.
Here professional team
availability is adequate.
Blended capitation, blended
salary and salary
remuneration.
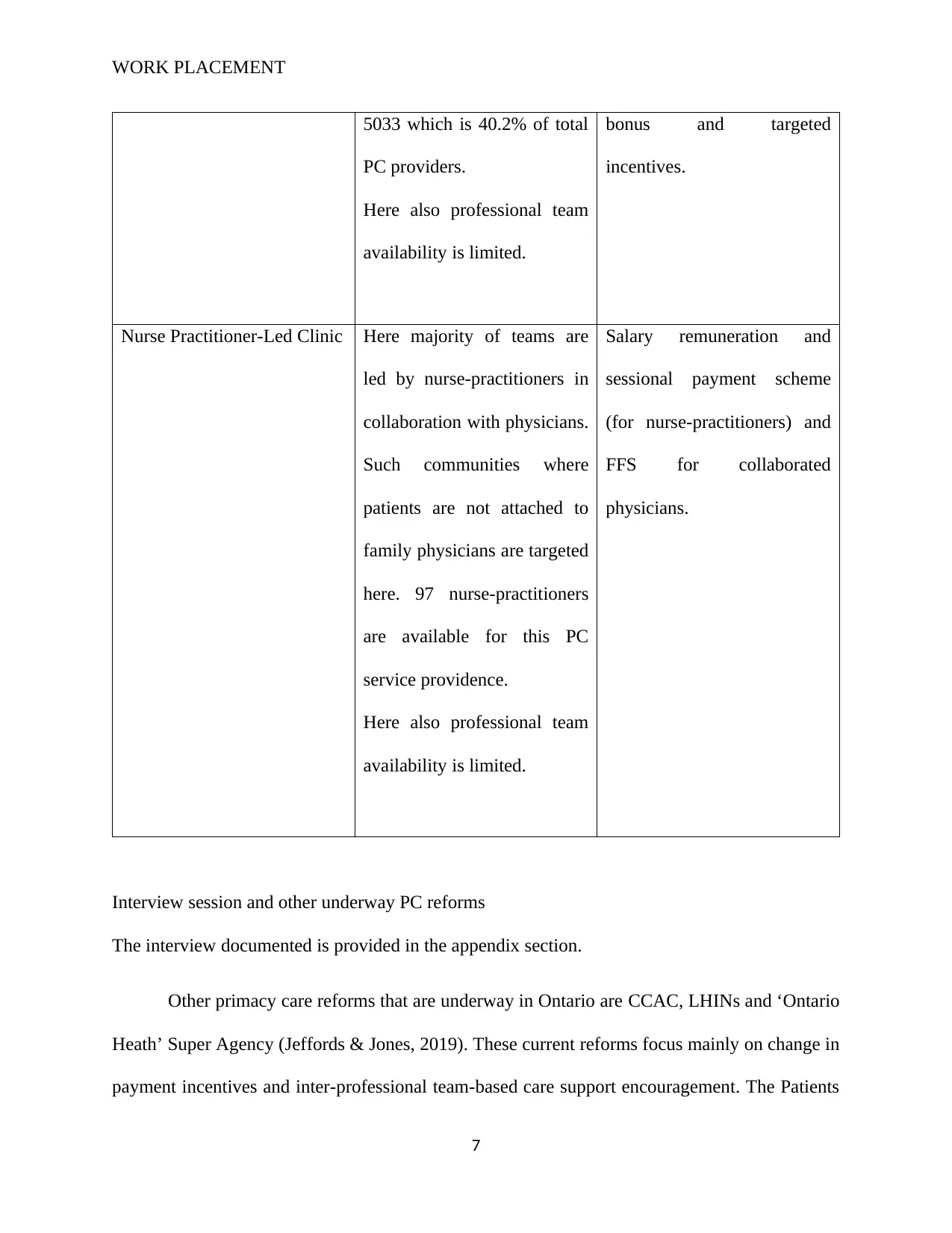
Family Health Organization Same as Family Head
Network
Number of physicians are
Broader basket of PC service
is included in capitation
remuneration with blended
6
WORK PLACEMENT
5033 which is 40.2% of total
PC providers.
Here also professional team
availability is limited.
bonus and targeted
incentives.
Nurse Practitioner-Led Clinic Here majority of teams are
led by nurse-practitioners in
collaboration with physicians.
Such communities where
patients are not attached to
family physicians are targeted
here. 97 nurse-practitioners
are available for this PC
service providence.
Here also professional team
availability is limited.
Salary remuneration and
sessional payment scheme
(for nurse-practitioners) and
FFS for collaborated
physicians.
Interview session and other underway PC reforms
The interview documented is provided in the appendix section.
Other primacy care reforms that are underway in Ontario are CCAC, LHINs and ‘Ontario
Heath’ Super Agency (Jeffords & Jones, 2019). These current reforms focus mainly on change in
payment incentives and inter-professional team-based care support encouragement. The Patients
7
5033 which is 40.2% of total
PC providers.
Here also professional team
availability is limited.
bonus and targeted
incentives.
Nurse Practitioner-Led Clinic Here majority of teams are
led by nurse-practitioners in
collaboration with physicians.
Such communities where
patients are not attached to
family physicians are targeted
here. 97 nurse-practitioners
are available for this PC
service providence.
Here also professional team
availability is limited.
Salary remuneration and
sessional payment scheme
(for nurse-practitioners) and
FFS for collaborated
physicians.
Interview session and other underway PC reforms
The interview documented is provided in the appendix section.
Other primacy care reforms that are underway in Ontario are CCAC, LHINs and ‘Ontario
Heath’ Super Agency (Jeffords & Jones, 2019). These current reforms focus mainly on change in
payment incentives and inter-professional team-based care support encouragement. The Patients
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

WORK PLACEMENT
first Act has also been recently implemented which widened the role of the Local Health
Integration Networks (LHINs) (Young et al., 2016).
Answer to question 2
Interview with a different cultural people
Details of interview session is provided in appendix. Here an African original, inhabitant
of Angola is interviewed for having knowledge on the African Healthcare system.
Comparison of healthcare system in Canada and Africa
Angola has a relatively higher population than Canada although the healthcare system is
not fully resilient to support the diverse needs of patients. While Canada is ranked 115th global
population wise, Angola enjoys a 55th global population ranking. It is important to note that the
Canadian healthcare system has tight guidelines. For instance, healthcare is not interested in
fraud but spending. The Canada Health Transfer is a fund set aside to finance citizens' medical
and healthcare needs – and it is distributed to municipal hospitals and local clinics. However, the
Angola government has a selected set of government hospitals that they fund. As a result, a key
discrepancy is that while the Canadian healthcare system is fully government sponsored, the
African healthcare system tends to receive funding from private players, foreign aid, and internal
funding.
Canada is a developed economy and as a result, most people enjoy relatively stable
healthcare. Over 75% of the population has access to quality healthcare, and an additional 15%
have private health insurance. The Canadian healthcare system further shows that all citizens
may access publicly available healthcare services in diverse settings; clinics, dispensaries, public
care facilities, and medical centers (Samuels, 2013). Angola, on the other hand, does not have a
8
first Act has also been recently implemented which widened the role of the Local Health
Integration Networks (LHINs) (Young et al., 2016).
Answer to question 2
Interview with a different cultural people
Details of interview session is provided in appendix. Here an African original, inhabitant
of Angola is interviewed for having knowledge on the African Healthcare system.
Comparison of healthcare system in Canada and Africa
Angola has a relatively higher population than Canada although the healthcare system is
not fully resilient to support the diverse needs of patients. While Canada is ranked 115th global
population wise, Angola enjoys a 55th global population ranking. It is important to note that the
Canadian healthcare system has tight guidelines. For instance, healthcare is not interested in
fraud but spending. The Canada Health Transfer is a fund set aside to finance citizens' medical
and healthcare needs – and it is distributed to municipal hospitals and local clinics. However, the
Angola government has a selected set of government hospitals that they fund. As a result, a key
discrepancy is that while the Canadian healthcare system is fully government sponsored, the
African healthcare system tends to receive funding from private players, foreign aid, and internal
funding.
Canada is a developed economy and as a result, most people enjoy relatively stable
healthcare. Over 75% of the population has access to quality healthcare, and an additional 15%
have private health insurance. The Canadian healthcare system further shows that all citizens
may access publicly available healthcare services in diverse settings; clinics, dispensaries, public
care facilities, and medical centers (Samuels, 2013). Angola, on the other hand, does not have a
8
WORK PLACEMENT
stable healthcare environment and only 40% of the population is covered by available insurance
plans. Lack of an integrated state system to secure user information, identify healthcare needs,
source, and deliver funding and financing makes it challenging for Angola and Africa in general
to have equitable access to healthcare services to the citizens. As a result, this analysis
establishes that a fully secure insurance plan will expand access to insurance services, and in the
process enable Angola and African, in general, realize better healthcare standards.
The problems experienced by the Canadian healthcare system are similarly reflected in
Angola. For instance, inadequate staff and lack of well-trained practitioners ails many clinics,
hospitals, and care centers. Similarly, poorly developed infrastructure and lack of adequate
clinical resources and equipment inhibits the quality of care and impedes the delivery of clinical
care. Angola and Africa suffer from similar problems although little has been invested to remedy
the situation. This analysis observes that in the comparison of the healthcare system of the two
nations, there are common problems that need re-evaluation.
Identification and resolution of problems
Well, the African healthcare system ails from the lack of a strong support structure. Poor
government funding leads to inadequate staffing suppressing the level of care. This problem can
be solved by strengthening the education system, provision of government sponsorships for
medical courses, and investment into healthcare research and vocational training.
A stark shortage of medical facilities ails most healthcare institutions. In Angola,
machines and equipment to diagnose and treat chronic illnesses are noticeably lacking, and in the
process undermining the quality and speed of clinical delivery. An important solution is to adopt
better management principles, to change the governance of public hospitals, and conduct
accountability as part of assessing and quantifying the utilizing of public healthcare resources.
9
stable healthcare environment and only 40% of the population is covered by available insurance
plans. Lack of an integrated state system to secure user information, identify healthcare needs,
source, and deliver funding and financing makes it challenging for Angola and Africa in general
to have equitable access to healthcare services to the citizens. As a result, this analysis
establishes that a fully secure insurance plan will expand access to insurance services, and in the
process enable Angola and African, in general, realize better healthcare standards.
The problems experienced by the Canadian healthcare system are similarly reflected in
Angola. For instance, inadequate staff and lack of well-trained practitioners ails many clinics,
hospitals, and care centers. Similarly, poorly developed infrastructure and lack of adequate
clinical resources and equipment inhibits the quality of care and impedes the delivery of clinical
care. Angola and Africa suffer from similar problems although little has been invested to remedy
the situation. This analysis observes that in the comparison of the healthcare system of the two
nations, there are common problems that need re-evaluation.
Identification and resolution of problems
Well, the African healthcare system ails from the lack of a strong support structure. Poor
government funding leads to inadequate staffing suppressing the level of care. This problem can
be solved by strengthening the education system, provision of government sponsorships for
medical courses, and investment into healthcare research and vocational training.
A stark shortage of medical facilities ails most healthcare institutions. In Angola,
machines and equipment to diagnose and treat chronic illnesses are noticeably lacking, and in the
process undermining the quality and speed of clinical delivery. An important solution is to adopt
better management principles, to change the governance of public hospitals, and conduct
accountability as part of assessing and quantifying the utilizing of public healthcare resources.
9
WORK PLACEMENT
The emergence of chronic conditions and new epidemiological patterns continues to put
healthcare systems in shambles. In Africa for example, chronic conditions are accountable for
80% healthcare expenditure. This means that the government spends significantly to deal with
specific illnesses and ailments. In this realization, there is a need to conduct market targeting to
determine ways to fight a certain group of ailments.
For instance, HIV/AIDS, Cancer, and diabetes cost 65% of the population and
approximated 47% of their income expenditure (Thompson, 2015). This means that individuals
suffering from such ailments are likely to spend a significant sum for diagnosis, treatment, and
self-management. This means that specific targeting of epidemiological conditions will help to
identify lasting solutions.
Finally, a major problem is that hospitals are yet to adopt new technologies to streamline
processes and enhance the quality of care. Nowadays, technologies provide a viable model to
secure patient data, integrate systems and networks, and streamline clinical care processes (Tony,
Brace, & Lois, 2018). This means that a major solution is to support a national-wide campaign to
build transparency on the potential and impact of new e-health technologies. Such resources will
help improve the speed and quality of care in local, national, and international jurisdictions.
Recommendations for change and personal opinions
Personally, I agree that low funding from the government affects most healthcare systems
in the developing world. Lack of transparency and accountability has led to misallocation and
misappropriate of public health funding, and in the process undermined the quality and the speed
of care. I also agree with the fact that most hospitals are yet to adopt e-health resources as
substitutes for quality care. This means that African cap taps into the emerging technologies to
boost their level and scale of service delivery. This recommendation adds insight into the fact
10
The emergence of chronic conditions and new epidemiological patterns continues to put
healthcare systems in shambles. In Africa for example, chronic conditions are accountable for
80% healthcare expenditure. This means that the government spends significantly to deal with
specific illnesses and ailments. In this realization, there is a need to conduct market targeting to
determine ways to fight a certain group of ailments.
For instance, HIV/AIDS, Cancer, and diabetes cost 65% of the population and
approximated 47% of their income expenditure (Thompson, 2015). This means that individuals
suffering from such ailments are likely to spend a significant sum for diagnosis, treatment, and
self-management. This means that specific targeting of epidemiological conditions will help to
identify lasting solutions.
Finally, a major problem is that hospitals are yet to adopt new technologies to streamline
processes and enhance the quality of care. Nowadays, technologies provide a viable model to
secure patient data, integrate systems and networks, and streamline clinical care processes (Tony,
Brace, & Lois, 2018). This means that a major solution is to support a national-wide campaign to
build transparency on the potential and impact of new e-health technologies. Such resources will
help improve the speed and quality of care in local, national, and international jurisdictions.
Recommendations for change and personal opinions
Personally, I agree that low funding from the government affects most healthcare systems
in the developing world. Lack of transparency and accountability has led to misallocation and
misappropriate of public health funding, and in the process undermined the quality and the speed
of care. I also agree with the fact that most hospitals are yet to adopt e-health resources as
substitutes for quality care. This means that African cap taps into the emerging technologies to
boost their level and scale of service delivery. This recommendation adds insight into the fact
10
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
WORK PLACEMENT
that governments and states must invest exhaustively in financing public and private health
facilities.
Such efforts will go a long way to ensure that citizens have equitable access to quality
and affordable healthcare. However, I disagree with the fact that targeting of epidemiological
conditions will help alleviate the prevalence of most diseases and illnesses. What should be
adopted is a complete change in lifestyle, including nutritional and dietary habits. Governments
must establish cross-tier partnerships with hospitals to fund community educational campaigns
that act as agents for positive lifestyle changes. This initiative will go a long way to ensure that
populations lead healthier lives and are immune to lifestyle chronic conditions such as cancer,
diabetes, obesity, heart disease, and cardiopulmonary diseases.
Answer to question 3
Layout of office and reception areas
The setting of health care offices may not be stunning examples of architectural designs
but are designed in a convenient manner so that patients can be put at ease and their healing
process can be accelerated (Yu, 2014). A number of health care offices are been reviewed and a
general discussion of their office and reception center layout is provided here. Most offices are
designed based on a single direction traffic flow. Total space availability is less important in
regard to layout design where in most cases the reception counter is located just after the main
entrance gate. This facilitates patients to clarify their queries in regard to various health issues. A
standardized layout map is also provided in the reception counter wall to guide patient parties to
the exact place they need to go. Traffic in most offices flows in a loop where both starting point
and ending point is same, that is the reception area (Gunn et al., 2015). Directional flow placards
are provided in intervals to guide patients conveniently. Various doctor consultancy rooms, lab
11
that governments and states must invest exhaustively in financing public and private health
facilities.
Such efforts will go a long way to ensure that citizens have equitable access to quality
and affordable healthcare. However, I disagree with the fact that targeting of epidemiological
conditions will help alleviate the prevalence of most diseases and illnesses. What should be
adopted is a complete change in lifestyle, including nutritional and dietary habits. Governments
must establish cross-tier partnerships with hospitals to fund community educational campaigns
that act as agents for positive lifestyle changes. This initiative will go a long way to ensure that
populations lead healthier lives and are immune to lifestyle chronic conditions such as cancer,
diabetes, obesity, heart disease, and cardiopulmonary diseases.
Answer to question 3
Layout of office and reception areas
The setting of health care offices may not be stunning examples of architectural designs
but are designed in a convenient manner so that patients can be put at ease and their healing
process can be accelerated (Yu, 2014). A number of health care offices are been reviewed and a
general discussion of their office and reception center layout is provided here. Most offices are
designed based on a single direction traffic flow. Total space availability is less important in
regard to layout design where in most cases the reception counter is located just after the main
entrance gate. This facilitates patients to clarify their queries in regard to various health issues. A
standardized layout map is also provided in the reception counter wall to guide patient parties to
the exact place they need to go. Traffic in most offices flows in a loop where both starting point
and ending point is same, that is the reception area (Gunn et al., 2015). Directional flow placards
are provided in intervals to guide patients conveniently. Various doctor consultancy rooms, lab
11
WORK PLACEMENT
testing rooms and other specialized treatment providence rooms are generally located in the
perimeter of the layout and open work stations are in the central location. The pod design system
of patient flow management use round robin pattern in many cases (Yu, 2014). Color also plays
crucial role in designing of the reception halls and other areas. Use of bright color is avoided and
eye-soothing colors like green, light blue etc. is used in most cases. The reception area is open
with an arch shaped desk in most cases where one or two receptionists are available 24 hours.
The emergency casualty and pharmacy departments are also present near to the reception.
Change required in the layout
The change layout is quite functional and the interviewees agree to the fact. Sitting
arrangement facility in the reception is fine but in many cases patients’ condition are more
serious and for that separate waiting room with bed-facility is highly recommended on their
behalf. Also, personal space of keeping belongings should be improved. Rest things are fine with
them.
Designing an ideal health office layout
An ideal health office should be designed in a manner so that quality care providence is
maximized. The design should be done keeping these major aspects in consideration namely
safety, employee comfort and patient flow (Gunn et al., 2015). Safety can be in terms of injury
safety, fire safety and safety from various stress related injuries. Furnitures in relation to a health
care office may include chairs, tables, desks, benches, single beds, stretchers, wardrobes and
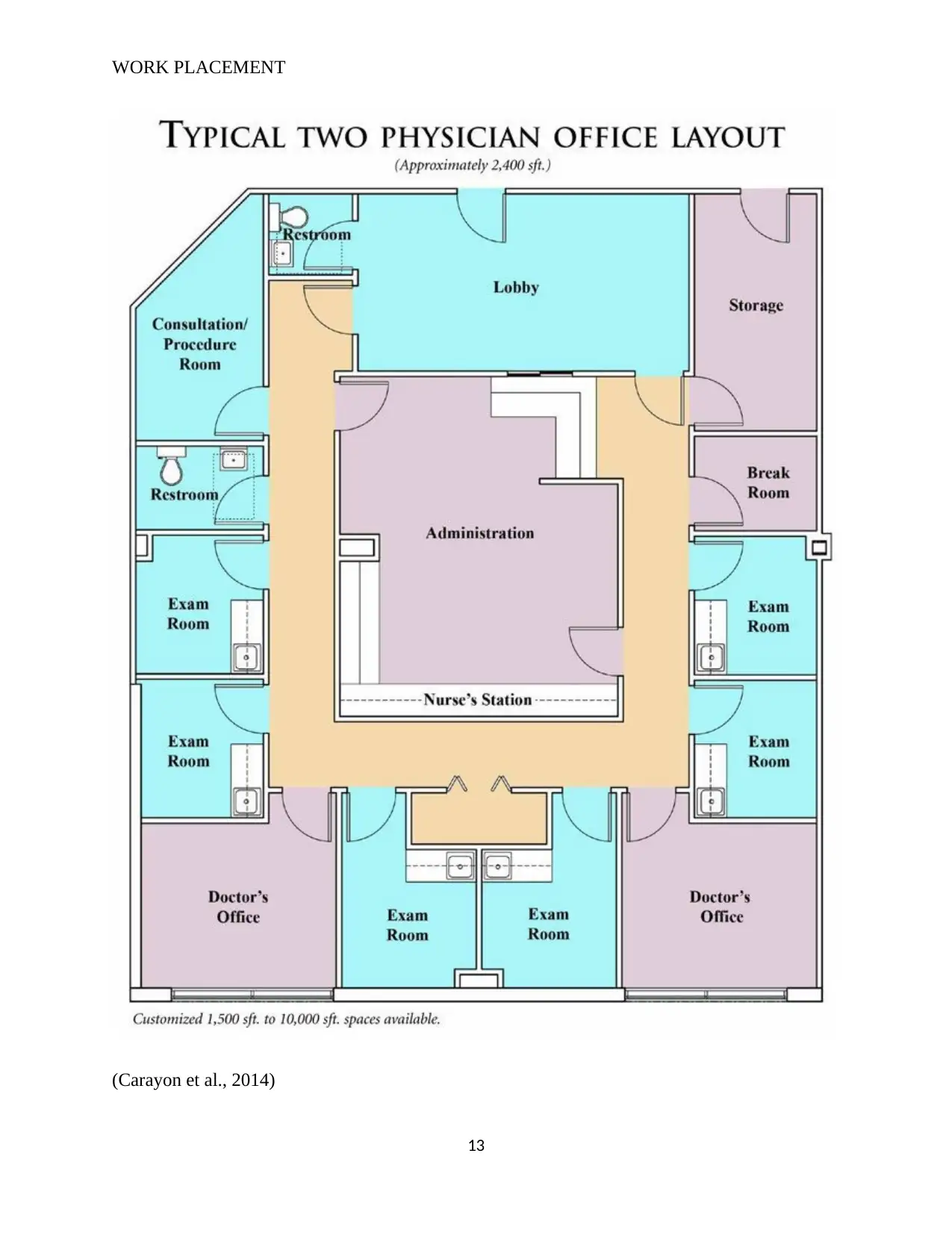
wheelchairs for physically challenged patients (Carayon et al., 2014). The diagrammatic
representation of an ideal office layout is provided below. Here physician availability is limited
to two but it can be more than that where the same floor planning may be applicable.
12
testing rooms and other specialized treatment providence rooms are generally located in the
perimeter of the layout and open work stations are in the central location. The pod design system
of patient flow management use round robin pattern in many cases (Yu, 2014). Color also plays
crucial role in designing of the reception halls and other areas. Use of bright color is avoided and
eye-soothing colors like green, light blue etc. is used in most cases. The reception area is open
with an arch shaped desk in most cases where one or two receptionists are available 24 hours.
The emergency casualty and pharmacy departments are also present near to the reception.
Change required in the layout
The change layout is quite functional and the interviewees agree to the fact. Sitting
arrangement facility in the reception is fine but in many cases patients’ condition are more
serious and for that separate waiting room with bed-facility is highly recommended on their
behalf. Also, personal space of keeping belongings should be improved. Rest things are fine with
them.
Designing an ideal health office layout
An ideal health office should be designed in a manner so that quality care providence is
maximized. The design should be done keeping these major aspects in consideration namely
safety, employee comfort and patient flow (Gunn et al., 2015). Safety can be in terms of injury
safety, fire safety and safety from various stress related injuries. Furnitures in relation to a health
care office may include chairs, tables, desks, benches, single beds, stretchers, wardrobes and
wheelchairs for physically challenged patients (Carayon et al., 2014). The diagrammatic
representation of an ideal office layout is provided below. Here physician availability is limited
to two but it can be more than that where the same floor planning may be applicable.
12
WORK PLACEMENT
(Carayon et al., 2014)
13
(Carayon et al., 2014)
13
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
WORK PLACEMENT
Each point of consideration is discussed below.
Safety is the most vital thing that is considered while planning a health care office layout
in Ergonomics. Both employees and patients’ safety are focused upon. To avoid injury and
accidents, the space available should be optimized and a proper systematic way of keeping
furniture and fixtures need to be designed (Carayon et al., 2014). For a single way traffic flow
generally, a common corridor is provided for patient movement and flow is generally
unidirectional. The floor is regularly washed and any kind of waterlogging or unhygienic
conditions are to be mitigated to the earliest by the housekeeping staffs. For fire safety purposes
a common fluorescent strip movement way is provided in the floor and in case of casualties’
patients and employees need to follow the direction provided and move outwards (Gunn et al.,
2015). Generally, for multi-sorted buildings, it is recommended to use staircases during fire
evacuation and avoid escalators and lifts. Also, in the layout map fire safety guide is to be
provided. Fire extinguishers are also to be kept in certain intervals to handle any kind of fire
injuries to the earliest. To avoid stress related injuries the color and space should be optimized
(Carayon et al., 2014). Eye-soothing color for the walls is recommended with soothing
wallpapers as well. For example, for maternity health care offices, a large wallpaper of a mother
and her child in her arms can be apt. For pediatric units, various cartoons wallpapers can be
recommended. Air and light also play immense role in reducing stress and fatigue. The layout
should be such that natural light comes in greater proportion (Carayon et al., 2014). In other
cases, not-so intense lightings will do. Labs and test centers may be facilitated with intense
lighting facilities. A centralized air conditioning system should be developed to support
optimized air flow.
14
Each point of consideration is discussed below.
Safety is the most vital thing that is considered while planning a health care office layout
in Ergonomics. Both employees and patients’ safety are focused upon. To avoid injury and
accidents, the space available should be optimized and a proper systematic way of keeping
furniture and fixtures need to be designed (Carayon et al., 2014). For a single way traffic flow
generally, a common corridor is provided for patient movement and flow is generally
unidirectional. The floor is regularly washed and any kind of waterlogging or unhygienic
conditions are to be mitigated to the earliest by the housekeeping staffs. For fire safety purposes
a common fluorescent strip movement way is provided in the floor and in case of casualties’
patients and employees need to follow the direction provided and move outwards (Gunn et al.,
2015). Generally, for multi-sorted buildings, it is recommended to use staircases during fire
evacuation and avoid escalators and lifts. Also, in the layout map fire safety guide is to be
provided. Fire extinguishers are also to be kept in certain intervals to handle any kind of fire
injuries to the earliest. To avoid stress related injuries the color and space should be optimized
(Carayon et al., 2014). Eye-soothing color for the walls is recommended with soothing
wallpapers as well. For example, for maternity health care offices, a large wallpaper of a mother
and her child in her arms can be apt. For pediatric units, various cartoons wallpapers can be
recommended. Air and light also play immense role in reducing stress and fatigue. The layout
should be such that natural light comes in greater proportion (Carayon et al., 2014). In other
cases, not-so intense lightings will do. Labs and test centers may be facilitated with intense
lighting facilities. A centralized air conditioning system should be developed to support
optimized air flow.
14
WORK PLACEMENT
To support employee comfort there should be adequate rest rooms, changing rooms,
washrooms, canteen facilities and communication facilities. Facilities for male and female
employees should be segregated (Gunn et al., 2015). Intercom connectivity should be well
developed with advanced IT support.
For optimizing patient traffic and patient flow the layout should be focused on single and
unidirectional traffic flow system which is generally a U-shaped layout where initial and end
points are same and is the reception or lobby area (Gunn et al., 2015). Separate washrooms,
customer service desks, rest rooms, waiting halls etc. should be emphasized in the floor planning
to increase convenience for the patients.
The furniture should be non-porous, smooth, and can be easily cleaned. Chair seat height
should be standard and should have arm rests. Reclining facilities if provided will add to patient
comfort. Chairs need to be stable and sturdy (Carayon et al., 2014). Rolling furniture like
stretchers wheel chairs should also be available. There should not be any sharp and hard edges in
chairs. Patient beds should be hygienic and comfortable.
15
To support employee comfort there should be adequate rest rooms, changing rooms,
washrooms, canteen facilities and communication facilities. Facilities for male and female
employees should be segregated (Gunn et al., 2015). Intercom connectivity should be well
developed with advanced IT support.
For optimizing patient traffic and patient flow the layout should be focused on single and
unidirectional traffic flow system which is generally a U-shaped layout where initial and end
points are same and is the reception or lobby area (Gunn et al., 2015). Separate washrooms,
customer service desks, rest rooms, waiting halls etc. should be emphasized in the floor planning
to increase convenience for the patients.
The furniture should be non-porous, smooth, and can be easily cleaned. Chair seat height
should be standard and should have arm rests. Reclining facilities if provided will add to patient
comfort. Chairs need to be stable and sturdy (Carayon et al., 2014). Rolling furniture like
stretchers wheel chairs should also be available. There should not be any sharp and hard edges in
chairs. Patient beds should be hygienic and comfortable.
15
WORK PLACEMENT
References
Carayon, P., Wetterneck, T. B., Rivera-Rodriguez, A. J., Hundt, A. S., Hoonakker, P., Holden,
R., & Gurses, A. P. (2014). Human factors systems approach to healthcare quality and
patient safety. Applied ergonomics, 45(1), 14-25.
Chatwood, S. (2018). Building on Primary Care Reforms and Indigenous Self-Determination in
the Northwest Territories: Physician Accountability and Performance in
Context. Healthcarepapers, 17(4), 70-76. doi: 10.12927/hcpap.2018.25573
Fierlbeck, K. (2011). Health care in Canada: A citizen's guide to policy and politics. Toronto:
University of Toronto Press.
Freund, T., Everett, C., Griffiths, P., Hudon, C., Naccarella, L., & Laurant, M. (2015). Skill mix,
roles and remuneration in the primary care workforce: who are the healthcare
professionals in the primary care teams across the world?. International Journal of
Nursing Studies, 52(3), 727-743.
Gunn, R., Davis, M. M., Hall, J., Heintzman, J., Muench, J., Smeds, B., ... & Brown, J. (2015).
Designing clinical space for the delivery of integrated behavioral health and primary
care. J Am Board Fam Med, 28(Supplement 1), S52-S62.
Hutchison, B., & Glazier, R. (2013). Ontario’s primary care reforms have transformed the local
care landscape, but a plan is needed for ongoing improvement. Health affairs, 32(4), 695-
703.
Jeffords, S., & Jones, A. (2019). Ontario Health super agency to co-ordinate provincial health-
care system. Retrieved from https://globalnews.ca/news/4999295/ontario-health-care-
system-overhaul/
16
References
Carayon, P., Wetterneck, T. B., Rivera-Rodriguez, A. J., Hundt, A. S., Hoonakker, P., Holden,
R., & Gurses, A. P. (2014). Human factors systems approach to healthcare quality and
patient safety. Applied ergonomics, 45(1), 14-25.
Chatwood, S. (2018). Building on Primary Care Reforms and Indigenous Self-Determination in
the Northwest Territories: Physician Accountability and Performance in
Context. Healthcarepapers, 17(4), 70-76. doi: 10.12927/hcpap.2018.25573
Fierlbeck, K. (2011). Health care in Canada: A citizen's guide to policy and politics. Toronto:
University of Toronto Press.
Freund, T., Everett, C., Griffiths, P., Hudon, C., Naccarella, L., & Laurant, M. (2015). Skill mix,
roles and remuneration in the primary care workforce: who are the healthcare
professionals in the primary care teams across the world?. International Journal of
Nursing Studies, 52(3), 727-743.
Gunn, R., Davis, M. M., Hall, J., Heintzman, J., Muench, J., Smeds, B., ... & Brown, J. (2015).
Designing clinical space for the delivery of integrated behavioral health and primary
care. J Am Board Fam Med, 28(Supplement 1), S52-S62.
Hutchison, B., & Glazier, R. (2013). Ontario’s primary care reforms have transformed the local
care landscape, but a plan is needed for ongoing improvement. Health affairs, 32(4), 695-
703.
Jeffords, S., & Jones, A. (2019). Ontario Health super agency to co-ordinate provincial health-
care system. Retrieved from https://globalnews.ca/news/4999295/ontario-health-care-
system-overhaul/
16
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
WORK PLACEMENT
Marchildon, G. (2013). Canada: health system review. Health systems in transition, 15(1), 1-179.
Marchildon, G. P. (2013). Health systems in transition: Canada(No. 1). University of Toronto
Press.
Marchildon, G. P., & Hutchison, B. (2016). Primary care in Ontario, Canada: New proposals
after 15 years of reform. Health Policy, 120(7), 732-738.
Samuels, R. (2013). Constitutionalizing universal public healthcare in Canada: Integrating
quality-of-life considerations with the Canadian Charter of Rights and Freedoms.
Ottawa: Agora Cosmopolitan.
Stewart, M., & Ryan, B. (2015). Ecology of health care in Canada. Canadian Family
Physician, 61(5), 449-453.
Thompson, V. D. (2015). Health and health care delivery in Canada. Vancouver, B.C: Langara
College.
Tony, D., Brace, C., & Lois, G. M. (2018). Health and Canadian society: Sociological
Perspectives. Toronto: University of Toronto Press.
Young, T. K., Chatwood, S., Ford, J., Healey, G., Jong, M., Lavoie, J., & White, M. (2016,
August). Transforming health care in remote communities: report on an international
conference. In BMC proceedings (Vol. 10, No. 6, p. 6). BioMed Central.
Yu, A. (2014). How a Well-Designed Doctor's Office Could Help Patients. Retrieved
from https://www.wnpr.org/post/how-well-designed-doctors-office-could-help-patients
17
Marchildon, G. (2013). Canada: health system review. Health systems in transition, 15(1), 1-179.
Marchildon, G. P. (2013). Health systems in transition: Canada(No. 1). University of Toronto
Press.
Marchildon, G. P., & Hutchison, B. (2016). Primary care in Ontario, Canada: New proposals
after 15 years of reform. Health Policy, 120(7), 732-738.
Samuels, R. (2013). Constitutionalizing universal public healthcare in Canada: Integrating
quality-of-life considerations with the Canadian Charter of Rights and Freedoms.
Ottawa: Agora Cosmopolitan.
Stewart, M., & Ryan, B. (2015). Ecology of health care in Canada. Canadian Family
Physician, 61(5), 449-453.
Thompson, V. D. (2015). Health and health care delivery in Canada. Vancouver, B.C: Langara
College.
Tony, D., Brace, C., & Lois, G. M. (2018). Health and Canadian society: Sociological
Perspectives. Toronto: University of Toronto Press.
Young, T. K., Chatwood, S., Ford, J., Healey, G., Jong, M., Lavoie, J., & White, M. (2016,
August). Transforming health care in remote communities: report on an international
conference. In BMC proceedings (Vol. 10, No. 6, p. 6). BioMed Central.
Yu, A. (2014). How a Well-Designed Doctor's Office Could Help Patients. Retrieved
from https://www.wnpr.org/post/how-well-designed-doctors-office-could-help-patients
17
WORK PLACEMENT
Appendices
A sample interview form of clients/ patients.
A middle-aged male patient is interviewed in this context who has come for first time check up
in a health care office.
1. Which Primary Care service you prefer, the present one or the fee-for service care?
Interviewee: I personally support the Canadian Health Service based on family physician
concept.
2. What are the differences and how do you prove your point?
Interviewee: family physician concept is more convenient to me because it is on time. The
waiting time for fee-for service care of specialized doctors is much higher and also having
prior appointment is very difficult. Moreover, the system of family physician provides quality
care and are really good towards patient service providence.
3. Which model is more convenient and is there any similarity between the two?
Interviewee: the family physician model is more convenient to me, specially the solo concept.
The physicians also work in groups and their income is derived from fee-for-service payments.
So, one way of the other the physician’s caliber is same. The family physician model has
reduced waiting time and is free from appointment hurdles. Though in both cases medical
charges are to be paid.
4. Are there any changes you would propose to the present PC model?
Interviewee: I would suggest work on the part of the medical insurance aspects. In spite of
Mediclaim we have to pay for health check ups and services which should be synchronized to
the insurance system.
18
Appendices
A sample interview form of clients/ patients.
A middle-aged male patient is interviewed in this context who has come for first time check up
in a health care office.
1. Which Primary Care service you prefer, the present one or the fee-for service care?
Interviewee: I personally support the Canadian Health Service based on family physician
concept.
2. What are the differences and how do you prove your point?
Interviewee: family physician concept is more convenient to me because it is on time. The
waiting time for fee-for service care of specialized doctors is much higher and also having
prior appointment is very difficult. Moreover, the system of family physician provides quality
care and are really good towards patient service providence.
3. Which model is more convenient and is there any similarity between the two?
Interviewee: the family physician model is more convenient to me, specially the solo concept.
The physicians also work in groups and their income is derived from fee-for-service payments.
So, one way of the other the physician’s caliber is same. The family physician model has
reduced waiting time and is free from appointment hurdles. Though in both cases medical
charges are to be paid.
4. Are there any changes you would propose to the present PC model?
Interviewee: I would suggest work on the part of the medical insurance aspects. In spite of
Mediclaim we have to pay for health check ups and services which should be synchronized to
the insurance system.
18
WORK PLACEMENT
5. Please provide some recommendations for the fee-for service care model on areas of
patient outcomes and quality care providence.
Interviewee: Quality of care providence is definitely reduced when any emergency patient
needs to wait for such a long time to have specialized treatment and patients naturally become
irritated. We are paying for the service, but still we have to suffer before reducing the actual
suffering.
Thank you letter to interviewees
Dear…….
Thank you very much for taking the time to interview with us and helping us in completing our
work placement project as a part of graduation from the Office Administration- Health Services
program by sharing your ideas, experience, opinion and knowledge. Your feedback really
mattered in our project evaluation in finding the gaps and we highly appreciate your
contribution.
Thank you
Regards
Name…………
Date ………….
19
5. Please provide some recommendations for the fee-for service care model on areas of
patient outcomes and quality care providence.
Interviewee: Quality of care providence is definitely reduced when any emergency patient
needs to wait for such a long time to have specialized treatment and patients naturally become
irritated. We are paying for the service, but still we have to suffer before reducing the actual
suffering.
Thank you letter to interviewees
Dear…….
Thank you very much for taking the time to interview with us and helping us in completing our
work placement project as a part of graduation from the Office Administration- Health Services
program by sharing your ideas, experience, opinion and knowledge. Your feedback really
mattered in our project evaluation in finding the gaps and we highly appreciate your
contribution.
Thank you
Regards
Name…………
Date ………….
19
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
WORK PLACEMENT
Confidentiality statement
The statement holds equal for every people. The principle of upholding the protection of patient
and practitioner information is recognized and collective feedback is exclusively sued for the
research purposes. As a result, in consideration to the mentioned terms and conditions and
related laws and policies on privacy and confidentiality of patient information, this
confidentiality statement outlines some major clauses, policies and actions that will be followed
throughout the interview process.
I. This research aims at collecting information from respondents purely for research
purposes and no other personal intention is there. It identifies that primary research from
patients and practitioners is of utmost importance in the realization of advanced patient
outcomes and high-quality care providence.
II. The research will holistically protect the information of respondents. Information to be
protected includes; names, addresses, email addresses, phone contacts, physical
addresses, and other personal identification information.
III. Respondents purely hold their ultimate will and decision about their participation in the
interview. Due consent will be sought beforehand and respondents are free to withdraw
themselves from this interview session either in writing or through any other formal
methods.
IV. The information collected from the interview will be used within the limitations and
boundaries of the research. The responses will not be used outside the area of this
research – and if there are any intentions of doing so, the respondents will be informed
prior to.
20
Confidentiality statement
The statement holds equal for every people. The principle of upholding the protection of patient
and practitioner information is recognized and collective feedback is exclusively sued for the
research purposes. As a result, in consideration to the mentioned terms and conditions and
related laws and policies on privacy and confidentiality of patient information, this
confidentiality statement outlines some major clauses, policies and actions that will be followed
throughout the interview process.
I. This research aims at collecting information from respondents purely for research
purposes and no other personal intention is there. It identifies that primary research from
patients and practitioners is of utmost importance in the realization of advanced patient
outcomes and high-quality care providence.
II. The research will holistically protect the information of respondents. Information to be
protected includes; names, addresses, email addresses, phone contacts, physical
addresses, and other personal identification information.
III. Respondents purely hold their ultimate will and decision about their participation in the
interview. Due consent will be sought beforehand and respondents are free to withdraw
themselves from this interview session either in writing or through any other formal
methods.
IV. The information collected from the interview will be used within the limitations and
boundaries of the research. The responses will not be used outside the area of this
research – and if there are any intentions of doing so, the respondents will be informed
prior to.
20
WORK PLACEMENT
V. Respondents are free to participate in the research and to ask any relevant questions in
relation to their information privacy, confidentiality and other related issues of privacy.
Agreement and personal information
The agreement
I………………………Name…………. Agree to participate in this research in the realization
of positive patient outcomes and better-quality care. By participating in this research, I
acknowledge that the information presented herein is truthful as per my knowledge and I will
provide clear and transparent information (Samuels, 2013). I also confirm that the
organization/personnel responsible for the interview process shall protect the personally
identifying information and prevent the loss of data to third parties.
Personal Contact Information
Name…………………………………………………………………….
Phone…………………………………………………………………….
Email………………………………………………………………………
Signature……………………………………………………………….
Date……………………………………………………………………….
21
V. Respondents are free to participate in the research and to ask any relevant questions in
relation to their information privacy, confidentiality and other related issues of privacy.
Agreement and personal information
The agreement
I………………………Name…………. Agree to participate in this research in the realization
of positive patient outcomes and better-quality care. By participating in this research, I
acknowledge that the information presented herein is truthful as per my knowledge and I will
provide clear and transparent information (Samuels, 2013). I also confirm that the
organization/personnel responsible for the interview process shall protect the personally
identifying information and prevent the loss of data to third parties.
Personal Contact Information
Name…………………………………………………………………….
Phone…………………………………………………………………….
Email………………………………………………………………………
Signature……………………………………………………………….
Date……………………………………………………………………….
21
WORK PLACEMENT
Interview session with an African origin people
Interview to an African origin about the Canadian Healthcare System
A. What is your country of origin and kindly describe the main facilities for healthcare
provision?
Answer: My country of origin is Angola. We usually have municipal county hospitals
divided into different levels including level four and level five depending on the quality of
healthcare delivery. However, there are emerging private healthcare systems that are
supported by private stakeholders and they include; dispensaries, clinics, hospitals, and
medical facilities.
B. How can you describe the quality of healthcare services between Africa and Canada?
Are there any discrepancies in quality and effectiveness?
Answer: Well, Angola has relatively lower quality healthcare as opposed to Canada. This
is particularly due to inadequate clinical staff, poor healthcare systems, and lack of
adequate funding and financing. As a result, the level of healthcare delivery tends to be
significantly lower than in developed economies such as Canada.
C. What additions do you think should be included in the Canada healthcare system to
improve the quality of service delivery?
Answer: I believe that patient confidentiality and privacy should be key concerns in the
continuum of care. Other than supporting effective system implementation, it helps to
improve the quality of service delivery. Most importantly is the adoption of enabling
technologies to optimize service delivery and improve client retention.
D. How can you describe your experience with the Canadian healthcare system and what
22
Interview session with an African origin people
Interview to an African origin about the Canadian Healthcare System
A. What is your country of origin and kindly describe the main facilities for healthcare
provision?
Answer: My country of origin is Angola. We usually have municipal county hospitals
divided into different levels including level four and level five depending on the quality of
healthcare delivery. However, there are emerging private healthcare systems that are
supported by private stakeholders and they include; dispensaries, clinics, hospitals, and
medical facilities.
B. How can you describe the quality of healthcare services between Africa and Canada?
Are there any discrepancies in quality and effectiveness?
Answer: Well, Angola has relatively lower quality healthcare as opposed to Canada. This
is particularly due to inadequate clinical staff, poor healthcare systems, and lack of
adequate funding and financing. As a result, the level of healthcare delivery tends to be
significantly lower than in developed economies such as Canada.
C. What additions do you think should be included in the Canada healthcare system to
improve the quality of service delivery?
Answer: I believe that patient confidentiality and privacy should be key concerns in the
continuum of care. Other than supporting effective system implementation, it helps to
improve the quality of service delivery. Most importantly is the adoption of enabling
technologies to optimize service delivery and improve client retention.
D. How can you describe your experience with the Canadian healthcare system and what
22
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
WORK PLACEMENT
are the major strengths and limitations?
Answer: I personally think that the Canadian healthcare system is well secured as it
requires that patients have insurance coverage and it provides quality care for low-
income families.
E. How can you compare the Canadian healthcare system with those of the world?
It is important to note that although both Canada and Africa have effective and
functional healthcare systems, the two faces similar challenges. For instance, there is a
stark shortage of pediatrician staff and resources in both nations. As a result, the
healthcare systems of both nations are strengthening nursing and practitioner training
programs to equip practitioners with advanced skills, enhance their knowledge, and
boost the quality of service delivery.
This means that presently the nation has a stark shortage of staff and this means that
patient workload may overgrow the available capacity and competency. While the
Canadian government has deployed resources to ensure there are adequate practitioners
to offer adequate services in fulfilling different healthcare needs, there are still gaps to
be bridged. First, it is crucial that hospitals, healthcare institutions, and clinics manage
the available workforce and optimize labor through the use of digitization.
Additionally, both the Canadian and African healthcare insurance plans cover a narrow
scope of health services. Some services such as dental care, physiotherapy, and out-of-
hospital pharmaceuticals are not covered in the insurance plans. As such, patients have
to seek these services from private insurance providers or reach deep into their pockets
to get these services.
There is a great deal of government involvement in the healthcare system of both
23
are the major strengths and limitations?
Answer: I personally think that the Canadian healthcare system is well secured as it
requires that patients have insurance coverage and it provides quality care for low-
income families.
E. How can you compare the Canadian healthcare system with those of the world?
It is important to note that although both Canada and Africa have effective and
functional healthcare systems, the two faces similar challenges. For instance, there is a
stark shortage of pediatrician staff and resources in both nations. As a result, the
healthcare systems of both nations are strengthening nursing and practitioner training
programs to equip practitioners with advanced skills, enhance their knowledge, and
boost the quality of service delivery.
This means that presently the nation has a stark shortage of staff and this means that
patient workload may overgrow the available capacity and competency. While the
Canadian government has deployed resources to ensure there are adequate practitioners
to offer adequate services in fulfilling different healthcare needs, there are still gaps to
be bridged. First, it is crucial that hospitals, healthcare institutions, and clinics manage
the available workforce and optimize labor through the use of digitization.
Additionally, both the Canadian and African healthcare insurance plans cover a narrow
scope of health services. Some services such as dental care, physiotherapy, and out-of-
hospital pharmaceuticals are not covered in the insurance plans. As such, patients have
to seek these services from private insurance providers or reach deep into their pockets
to get these services.
There is a great deal of government involvement in the healthcare system of both
23
WORK PLACEMENT
Canada and the United States. The Canadian federal government provides the provincial
governments with healthcare funding and support. Similarly, the US government
provides healthcare funding through Medicare, Medicaid, and the Veterans
Administration.
F. What are the major challenges and solutions to both Angola and the Canadian
healthcare system? Also, kindly elaborate on what is pediatric care in both nations, what
is involved, and how the healthcare system of both nations can be improved.
Pediatric care is concerned with the dispensation of care to children. Usually, pediatric
care is well-aligned with the healthcare needs of children and in the process, it must
afford solutions that are sustainable to the health of children. As a result, this analysis
notes that constant research and development is required to understand and know how
effective, high-quality care can be delivered even during high-pressure times.
As noted, both Angola and Canada suffer from a similar healthcare challenge which in
this case is the provision of quality care from a small workforce or pool of employees. It
is further established to note that a limited set of advanced, high-tech resources inhibit
the dispensation of care, and in the process presents a significant challenge to the
government and healthcare stakeholders at large. This analysis notes that while the
Canada and Angola feature a large population, the dispensation of care may present
fundamental challenges and problems. As a result, it is important to encourage higher
admissions in medical schools, provide professional development opportunities,
training, and conduct advanced research and studies.
Both Canada and Angola face the challenge of access to healthcare services. According
to statistics, more than 40% of Canadians and 70% of people from Angola do not have
24
Canada and the United States. The Canadian federal government provides the provincial
governments with healthcare funding and support. Similarly, the US government
provides healthcare funding through Medicare, Medicaid, and the Veterans
Administration.
F. What are the major challenges and solutions to both Angola and the Canadian
healthcare system? Also, kindly elaborate on what is pediatric care in both nations, what
is involved, and how the healthcare system of both nations can be improved.
Pediatric care is concerned with the dispensation of care to children. Usually, pediatric
care is well-aligned with the healthcare needs of children and in the process, it must
afford solutions that are sustainable to the health of children. As a result, this analysis
notes that constant research and development is required to understand and know how
effective, high-quality care can be delivered even during high-pressure times.
As noted, both Angola and Canada suffer from a similar healthcare challenge which in
this case is the provision of quality care from a small workforce or pool of employees. It
is further established to note that a limited set of advanced, high-tech resources inhibit
the dispensation of care, and in the process presents a significant challenge to the
government and healthcare stakeholders at large. This analysis notes that while the
Canada and Angola feature a large population, the dispensation of care may present
fundamental challenges and problems. As a result, it is important to encourage higher
admissions in medical schools, provide professional development opportunities,
training, and conduct advanced research and studies.
Both Canada and Angola face the challenge of access to healthcare services. According
to statistics, more than 40% of Canadians and 70% of people from Angola do not have
24
WORK PLACEMENT
access to health insurance. Further, some of the people with medical insurance in
Canada and Angola have a skeletal insurance cover that barely meets their medical
needs. As such, they cannot access various health care services when the need arises. To
solve this problem, both countries need to increase access to healthcare services by
providing affordable health insurance.
Further, Canada and Angola face the challenge of long wait times. For emergency
issues such as heart attack, patients have timely access to health care. However, the wait
is long for patients who need care for less urgent problems like cataract surgery or knee
replacement. Patients can wait for as long as 6 months or a year. As a solution, both
countries need to ensure that they have enough medical practitioners to ensure that the
ratio of patients to doctors is as the expected and appropriate level.
G. Is there any healthcare reform or legislation changes in your area?
The government introduced free maternal healthcare for pregnant women to curb the rising
number of infant deaths. This reform will ensure that significant public healthcare
expenditure is channeled to finance maternal health programs.
25
access to health insurance. Further, some of the people with medical insurance in
Canada and Angola have a skeletal insurance cover that barely meets their medical
needs. As such, they cannot access various health care services when the need arises. To
solve this problem, both countries need to increase access to healthcare services by
providing affordable health insurance.
Further, Canada and Angola face the challenge of long wait times. For emergency
issues such as heart attack, patients have timely access to health care. However, the wait
is long for patients who need care for less urgent problems like cataract surgery or knee
replacement. Patients can wait for as long as 6 months or a year. As a solution, both
countries need to ensure that they have enough medical practitioners to ensure that the
ratio of patients to doctors is as the expected and appropriate level.
G. Is there any healthcare reform or legislation changes in your area?
The government introduced free maternal healthcare for pregnant women to curb the rising
number of infant deaths. This reform will ensure that significant public healthcare
expenditure is channeled to finance maternal health programs.
25
1 out of 25
Related Documents

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.