Wound Management Case Study
VerifiedAdded on 2023/01/18
|9
|2236
|51
AI Summary
This article provides a holistic wound management plan for Mr Will Jackson and Mrs Miriam Gold, including evaluation, expected healing process, and wound management plan for each type of wound.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: WOUND MANAGEMENT
Wound Management Case Study
Name of the Student
Name of the University
Author’s Note:
Wound Management Case Study
Name of the Student
Name of the University
Author’s Note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1WOUND MANAGEMENT
Healing process of open is a dynamic and complex process and it is varies according to the
patients’ medical condition, health status and wound environment. The principles of wound
management depended on the principles of physiology (Flanagan, 2013). Generally, it is
follows the phases of haemostasis, inflammation, granulation and maturation. Wounds which
does not heal as normally and expected should be approached with holistic, patient- centred,
collaborative, and inter professional approach. The best practice principles of wound
management are provided below:
Identification of best available treatment.
Evaluation of risk factors related to patients
Recognition of limitations (Dimauro et al., 2014)
Therefore, the purpose of this article is to provide a holistic wound management plan for the
Mr Will Jackson and Mrs Miriam Gold.
Case study of Mr Will Jackson:
Medical History: Mr Will Jackson is 77 years old man who was admitted to the hospital for
the pain from his diabetic foot ulcer and arterial ulcer. The patient has another pressure ulcer
on his sacrum bone which was discovered after his admission to the hospital. In addition to
this, patient also had a burn injury in his left hand which has happened due to the spilled
coffee. Diabetic ulcer generally caused around 15 per cent of diabetic patient under the foot
while arterial ulcer occurs due to poor perfusion and is generally occurs in the lower
extremities of the body. In accordance to the previous statement, Mr Jackson diabetic ulcer is
situated under his left toe and his arterial ulcer is in his right lower leg. In addition, he also
has bedsores which commonly occur due constant pressure in his skin. Mr Jackson’s arterial
ulcer is infected and it should investigated for the type of infection and which bacteria are
responsible for the infection.
Healing process of open is a dynamic and complex process and it is varies according to the
patients’ medical condition, health status and wound environment. The principles of wound
management depended on the principles of physiology (Flanagan, 2013). Generally, it is
follows the phases of haemostasis, inflammation, granulation and maturation. Wounds which
does not heal as normally and expected should be approached with holistic, patient- centred,
collaborative, and inter professional approach. The best practice principles of wound
management are provided below:
Identification of best available treatment.
Evaluation of risk factors related to patients
Recognition of limitations (Dimauro et al., 2014)
Therefore, the purpose of this article is to provide a holistic wound management plan for the
Mr Will Jackson and Mrs Miriam Gold.
Case study of Mr Will Jackson:
Medical History: Mr Will Jackson is 77 years old man who was admitted to the hospital for
the pain from his diabetic foot ulcer and arterial ulcer. The patient has another pressure ulcer
on his sacrum bone which was discovered after his admission to the hospital. In addition to
this, patient also had a burn injury in his left hand which has happened due to the spilled
coffee. Diabetic ulcer generally caused around 15 per cent of diabetic patient under the foot
while arterial ulcer occurs due to poor perfusion and is generally occurs in the lower
extremities of the body. In accordance to the previous statement, Mr Jackson diabetic ulcer is
situated under his left toe and his arterial ulcer is in his right lower leg. In addition, he also
has bedsores which commonly occur due constant pressure in his skin. Mr Jackson’s arterial
ulcer is infected and it should investigated for the type of infection and which bacteria are
responsible for the infection.
2WOUND MANAGEMENT
Mr Jackson’s each type of wound’s evaluation, expected healing process, wound
management plan is presented in the following table.
Type of
wound
Evaluation Expected healing
process
Wound management
plan
Diabetic foot
ulcer
This wound is around 3
cm in diameter and it is
around 2 cm deep. The
wound bed is pinkish
in colour which might
indicate the presence
of pus. There is slight
wound exudate in the
wound bed. Skin
around the wound is
breaking down
slightly. This wound
should be checked for
infection (Moura et al.,
2013).
Expected healing
process is complete
epithelialization of the
wound and no exudate
will be present.
Expected healing time
is around 1 month.
Wound management
plan for this type of
wound is:
Infection
prevention
Taking off
pressure form
the wound
Managing
blood glucose
level
The wound
need to be
bandaged and
clean
Daily cleaning
of the wound
(Moura et al.,
2013)
Infected
Arterial
Ulcer
The wound is around 2
– 3 cm in diameter.
The wound bed and the
surrounding skin is
pink coloured. The
skin around the wound
is intact. There is a
presence of slight
exudate (clear fluid) is
noticeable in the
wound. This wound is
infected and as the
patient is staying in
hospital, MRSA
infection in the wound
should be checked.
This type of ulcer
wounds are very hard
to heal and proper
treatment is require for
healing process.
Expected healing time
for this type of wound
is 1 – 2 month with
proper care.
Wound management
plan for this type of
wound is:
Increment of
peripheral
blood flow
Managing
blood glucose
level
Elevated
sleeping
position at the
head end
Avoidance of
vasoconstrictive
drug (Powers et
al., 2016)
Wound should
be dressed with
Mr Jackson’s each type of wound’s evaluation, expected healing process, wound
management plan is presented in the following table.
Type of
wound
Evaluation Expected healing
process
Wound management
plan
Diabetic foot
ulcer
This wound is around 3
cm in diameter and it is
around 2 cm deep. The
wound bed is pinkish
in colour which might
indicate the presence
of pus. There is slight
wound exudate in the
wound bed. Skin
around the wound is
breaking down
slightly. This wound
should be checked for
infection (Moura et al.,
2013).
Expected healing
process is complete
epithelialization of the
wound and no exudate
will be present.
Expected healing time
is around 1 month.
Wound management
plan for this type of
wound is:
Infection
prevention
Taking off
pressure form
the wound
Managing
blood glucose
level
The wound
need to be
bandaged and
clean
Daily cleaning
of the wound
(Moura et al.,
2013)
Infected
Arterial
Ulcer
The wound is around 2
– 3 cm in diameter.
The wound bed and the
surrounding skin is
pink coloured. The
skin around the wound
is intact. There is a
presence of slight
exudate (clear fluid) is
noticeable in the
wound. This wound is
infected and as the
patient is staying in
hospital, MRSA
infection in the wound
should be checked.
This type of ulcer
wounds are very hard
to heal and proper
treatment is require for
healing process.
Expected healing time
for this type of wound
is 1 – 2 month with
proper care.
Wound management
plan for this type of
wound is:
Increment of
peripheral
blood flow
Managing
blood glucose
level
Elevated
sleeping
position at the
head end
Avoidance of
vasoconstrictive
drug (Powers et
al., 2016)
Wound should
be dressed with
3WOUND MANAGEMENT
Type of
wound
Evaluation Expected healing
process
Wound management
plan
bandage daily
Pressure
Ulcer
This an open and deep
wound. The wound is
clean and there is no
presence of exudate.
The wound bed is
moist and deep red in
colour. The skin
around the wound is
intact. This is a stage II
pressure ulcer.
Pressure ulcer requires
time to heal and this
wound might take 6 –
8 week time to heal
whereas if left
untreated it may take
up to one year.
Wound management
plan for this type of
wound is:
The wound
should be
cleaned daily
and normal
saline solution
can be used
Changing of
dressing daily
Prevention of
infection in the
wound.
Management of
blood glucose
level
Adequate
hydration and
nutrition
(Moore, &
Cowman, 2013)
Burn injury This not an open
wound. Blisters have
generated due to burn
injury. The skin is
intact and no opening
is noticed. Skin tissue
and around the area is
red.
This type of wound is
expected to heal within
1 week, however skin
might be discoloured
after healing.
Wound management
plan for this type of
wound is:
The wound
should not be
bandaged. The
wound should
be allowed to
breathe.
Blisters should
not break.
Lotion can be
applied to the
blisters.
Health education: Health care professionals should provide the information about the self-
management of ulcer to the patient. The patient should also be advise about the nutritional
Type of
wound
Evaluation Expected healing
process
Wound management
plan
bandage daily
Pressure
Ulcer
This an open and deep
wound. The wound is
clean and there is no
presence of exudate.
The wound bed is
moist and deep red in
colour. The skin
around the wound is
intact. This is a stage II
pressure ulcer.
Pressure ulcer requires
time to heal and this
wound might take 6 –
8 week time to heal
whereas if left
untreated it may take
up to one year.
Wound management
plan for this type of
wound is:
The wound
should be
cleaned daily
and normal
saline solution
can be used
Changing of
dressing daily
Prevention of
infection in the
wound.
Management of
blood glucose
level
Adequate
hydration and
nutrition
(Moore, &
Cowman, 2013)
Burn injury This not an open
wound. Blisters have
generated due to burn
injury. The skin is
intact and no opening
is noticed. Skin tissue
and around the area is
red.
This type of wound is
expected to heal within
1 week, however skin
might be discoloured
after healing.
Wound management
plan for this type of
wound is:
The wound
should not be
bandaged. The
wound should
be allowed to
breathe.
Blisters should
not break.
Lotion can be
applied to the
blisters.
Health education: Health care professionals should provide the information about the self-
management of ulcer to the patient. The patient should also be advise about the nutritional
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4WOUND MANAGEMENT
intake and the patient should avoid sugary and carbohydrate rich food. The patient should
also be adequately hydrated. The patient will also be advised about the harmful and
hazardous progression of ulcers if not proper care had been taken. All of the patient wound
was exacerbated due to high blood glucose level and patient should monitor his blood glucose
level.
Pain management: Mr Jackson is suffering from three types of ulcer and one minor burn
blisters. The ulcers can be pretty painful and the patient might medicine to relieve his pain.
The patient can be prescribed to take fentanyl (Derry et al., 2016). It is a synthetic opioid for
pain reliever and the 25 – 50 mg does can be administered to the patient daily.
Case study of Mrs Miriam Gold:
Medical History: Mrs Miriam Gold is an 85 years old woman who admitted to ward due to
extreme pain and she was admitted for palliative care. At the time of the admittance, the
patient was drowsy and has very vague cognitive feelings. She was admitted with a malignant
wound with extreme pain and she needed immediate pain reliever before any dressing change
can be done to her wound. Malignant wound is a type of wound which generally occurs due
to cancerous cells which invades the blood vessels and lymph of the skin. It is an open
malignant lesion on the skin and tissues die in this type of wound. The wound was filled with
oozing pus and the wound has developed sinus with a very strong odour. The patient wound
area and peri- anal area is burning red from the bowel incontinence and discharge. This is the
result of her cervical cancer. Furthermore, the patient has also developed a recto- vaginal
fistula due progression of cervical cancer and side effects of radiation. In addition to this, Mrs
Gold also had a venous ulcer which is not healing. Venous ulcer is a type of ulcer which
occurs due to improper functioning of the venous valves and it is generally occurs in the
lower extremities of the body.
intake and the patient should avoid sugary and carbohydrate rich food. The patient should
also be adequately hydrated. The patient will also be advised about the harmful and
hazardous progression of ulcers if not proper care had been taken. All of the patient wound
was exacerbated due to high blood glucose level and patient should monitor his blood glucose
level.
Pain management: Mr Jackson is suffering from three types of ulcer and one minor burn
blisters. The ulcers can be pretty painful and the patient might medicine to relieve his pain.
The patient can be prescribed to take fentanyl (Derry et al., 2016). It is a synthetic opioid for
pain reliever and the 25 – 50 mg does can be administered to the patient daily.
Case study of Mrs Miriam Gold:
Medical History: Mrs Miriam Gold is an 85 years old woman who admitted to ward due to
extreme pain and she was admitted for palliative care. At the time of the admittance, the
patient was drowsy and has very vague cognitive feelings. She was admitted with a malignant
wound with extreme pain and she needed immediate pain reliever before any dressing change
can be done to her wound. Malignant wound is a type of wound which generally occurs due
to cancerous cells which invades the blood vessels and lymph of the skin. It is an open
malignant lesion on the skin and tissues die in this type of wound. The wound was filled with
oozing pus and the wound has developed sinus with a very strong odour. The patient wound
area and peri- anal area is burning red from the bowel incontinence and discharge. This is the
result of her cervical cancer. Furthermore, the patient has also developed a recto- vaginal
fistula due progression of cervical cancer and side effects of radiation. In addition to this, Mrs
Gold also had a venous ulcer which is not healing. Venous ulcer is a type of ulcer which
occurs due to improper functioning of the venous valves and it is generally occurs in the
lower extremities of the body.
5WOUND MANAGEMENT
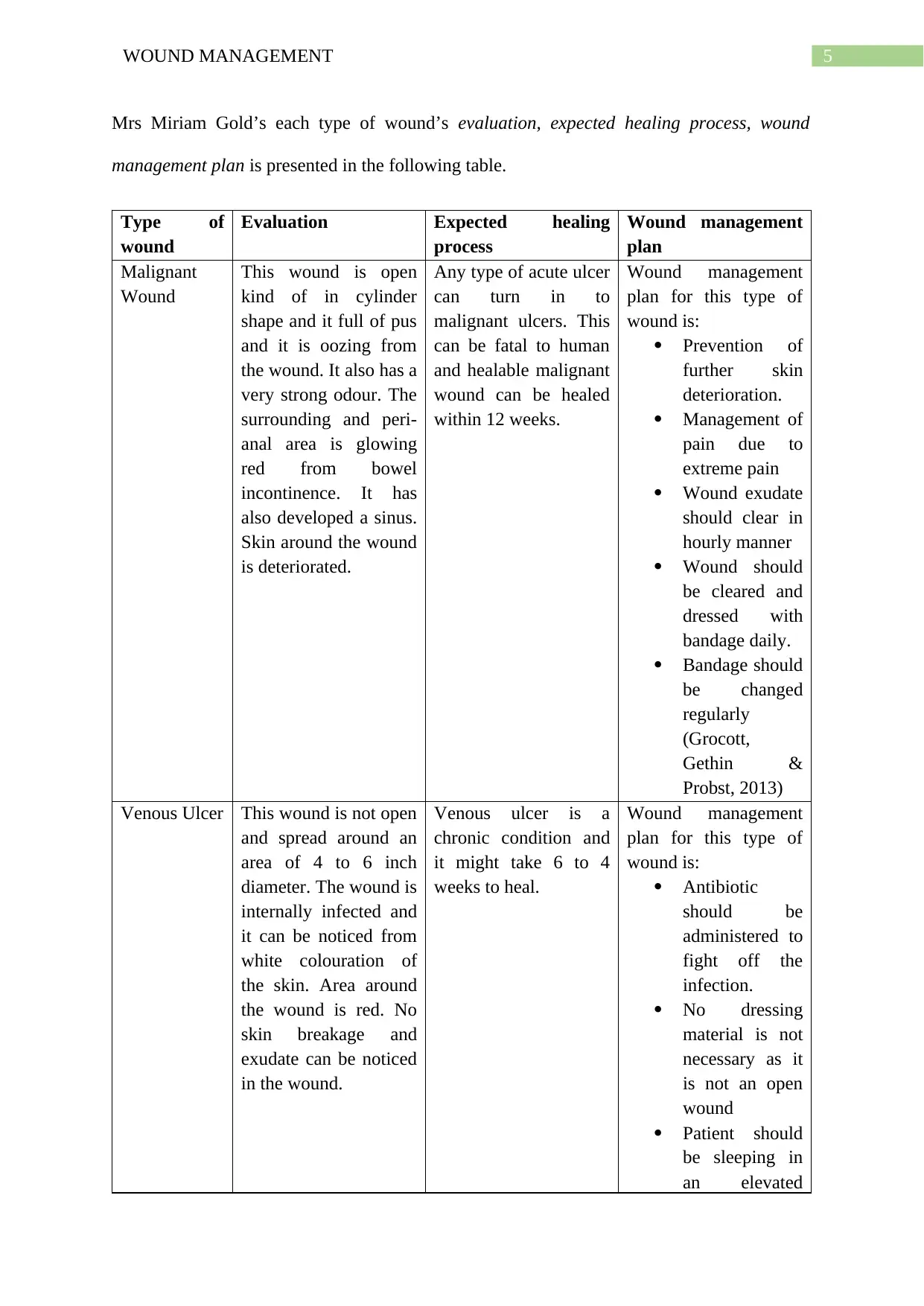
Mrs Miriam Gold’s each type of wound’s evaluation, expected healing process, wound
management plan is presented in the following table.
Type of
wound
Evaluation Expected healing
process
Wound management
plan
Malignant
Wound
This wound is open
kind of in cylinder
shape and it full of pus
and it is oozing from
the wound. It also has a
very strong odour. The
surrounding and peri-
anal area is glowing
red from bowel
incontinence. It has
also developed a sinus.
Skin around the wound
is deteriorated.
Any type of acute ulcer
can turn in to
malignant ulcers. This
can be fatal to human
and healable malignant
wound can be healed
within 12 weeks.
Wound management
plan for this type of
wound is:
Prevention of
further skin
deterioration.
Management of
pain due to
extreme pain
Wound exudate
should clear in
hourly manner
Wound should
be cleared and
dressed with
bandage daily.
Bandage should
be changed
regularly
(Grocott,
Gethin &
Probst, 2013)
Venous Ulcer This wound is not open
and spread around an
area of 4 to 6 inch
diameter. The wound is
internally infected and
it can be noticed from
white colouration of
the skin. Area around
the wound is red. No
skin breakage and
exudate can be noticed
in the wound.
Venous ulcer is a
chronic condition and
it might take 6 to 4
weeks to heal.
Wound management
plan for this type of
wound is:
Antibiotic
should be
administered to
fight off the
infection.
No dressing
material is not
necessary as it
is not an open
wound
Patient should
be sleeping in
an elevated
Mrs Miriam Gold’s each type of wound’s evaluation, expected healing process, wound
management plan is presented in the following table.
Type of
wound
Evaluation Expected healing
process
Wound management
plan
Malignant
Wound
This wound is open
kind of in cylinder
shape and it full of pus
and it is oozing from
the wound. It also has a
very strong odour. The
surrounding and peri-
anal area is glowing
red from bowel
incontinence. It has
also developed a sinus.
Skin around the wound
is deteriorated.
Any type of acute ulcer
can turn in to
malignant ulcers. This
can be fatal to human
and healable malignant
wound can be healed
within 12 weeks.
Wound management
plan for this type of
wound is:
Prevention of
further skin
deterioration.
Management of
pain due to
extreme pain
Wound exudate
should clear in
hourly manner
Wound should
be cleared and
dressed with
bandage daily.
Bandage should
be changed
regularly
(Grocott,
Gethin &
Probst, 2013)
Venous Ulcer This wound is not open
and spread around an
area of 4 to 6 inch
diameter. The wound is
internally infected and
it can be noticed from
white colouration of
the skin. Area around
the wound is red. No
skin breakage and
exudate can be noticed
in the wound.
Venous ulcer is a
chronic condition and
it might take 6 to 4
weeks to heal.
Wound management
plan for this type of
wound is:
Antibiotic
should be
administered to
fight off the
infection.
No dressing
material is not
necessary as it
is not an open
wound
Patient should
be sleeping in
an elevated
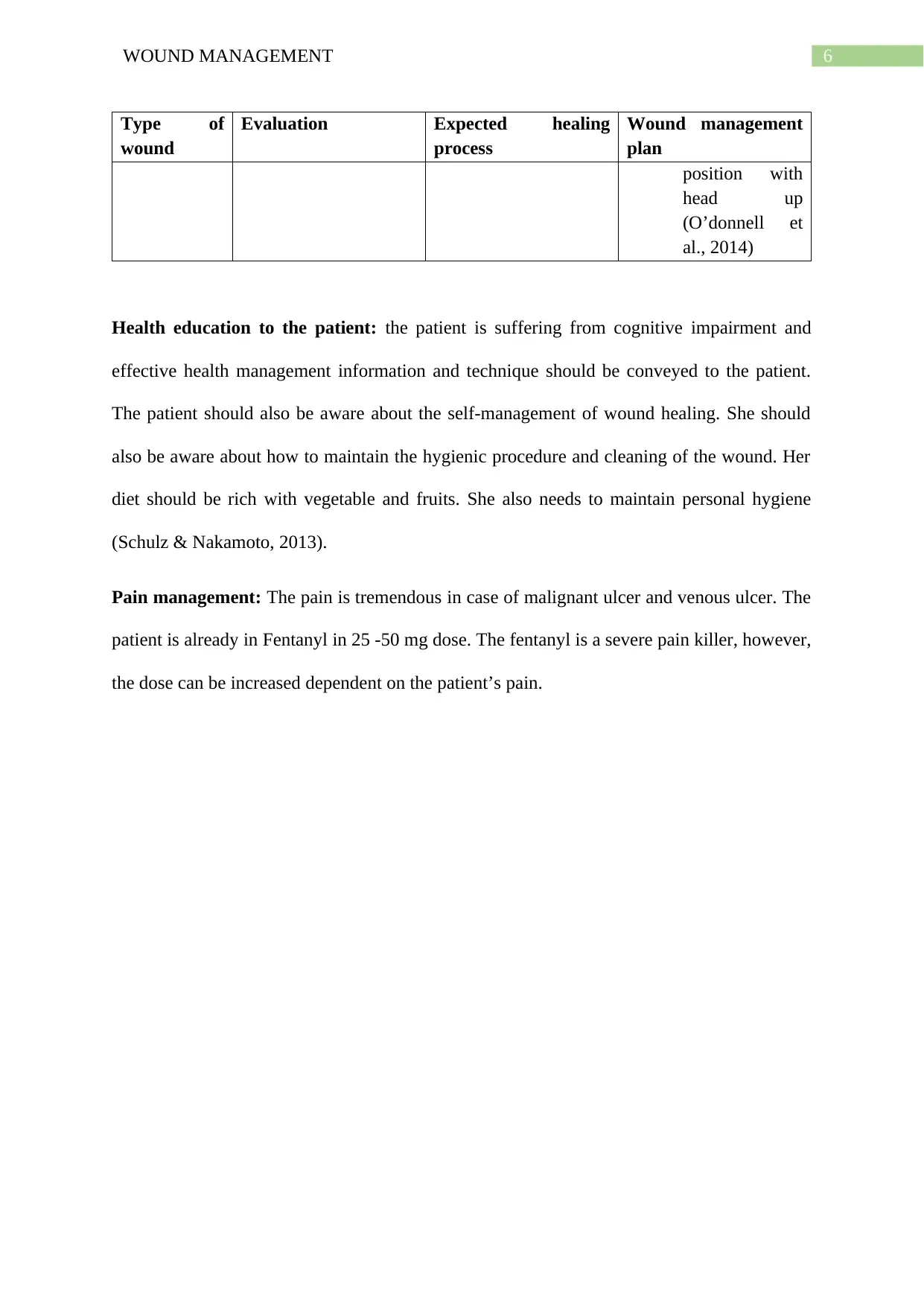
6WOUND MANAGEMENT
Type of
wound
Evaluation Expected healing
process
Wound management
plan
position with
head up
(O’donnell et
al., 2014)
Health education to the patient: the patient is suffering from cognitive impairment and
effective health management information and technique should be conveyed to the patient.
The patient should also be aware about the self-management of wound healing. She should
also be aware about how to maintain the hygienic procedure and cleaning of the wound. Her
diet should be rich with vegetable and fruits. She also needs to maintain personal hygiene
(Schulz & Nakamoto, 2013).
Pain management: The pain is tremendous in case of malignant ulcer and venous ulcer. The
patient is already in Fentanyl in 25 -50 mg dose. The fentanyl is a severe pain killer, however,
the dose can be increased dependent on the patient’s pain.
Type of
wound
Evaluation Expected healing
process
Wound management
plan
position with
head up
(O’donnell et
al., 2014)
Health education to the patient: the patient is suffering from cognitive impairment and
effective health management information and technique should be conveyed to the patient.
The patient should also be aware about the self-management of wound healing. She should
also be aware about how to maintain the hygienic procedure and cleaning of the wound. Her
diet should be rich with vegetable and fruits. She also needs to maintain personal hygiene
(Schulz & Nakamoto, 2013).
Pain management: The pain is tremendous in case of malignant ulcer and venous ulcer. The
patient is already in Fentanyl in 25 -50 mg dose. The fentanyl is a severe pain killer, however,
the dose can be increased dependent on the patient’s pain.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7WOUND MANAGEMENT
References:
Derry, S., Stannard, C., Cole, P., Wiffen, P. J., Knaggs, R., Aldington, D., & Moore, R. A.
(2016). Fentanyl for neuropathic pain in adults. Cochrane Database of Systematic
Reviews, (10).
Dimauro, I., Grasso, L., Fittipaldi, S., Fantini, C., Mercatelli, N., Racca, S., ... & Borrione, P.
(2014). Platelet-rich plasma and skeletal muscle healing: a molecular analysis of the
early phases of the regeneration process in an experimental animal model. PloS
one, 9(7), e102993.
Flanagan, M. (2013). Wound healing and skin integrity: principles and practice. John Wiley
& Sons.
Grocott, P., Gethin, G., & Probst, S. (2013). Malignant wound management in advanced
illness: new insights. Current opinion in supportive and palliative care, 7(1), 101-
105.
Moore, Z. E., & Cowman, S. (2013). Wound cleansing for pressure ulcers. Cochrane
Database of Systematic Reviews, (3).
Moura, L. I., Dias, A. M., Carvalho, E., & de Sousa, H. C. (2013). Recent advances on the
development of wound dressings for diabetic foot ulcer treatment—a review. Acta
biomaterialia, 9(7), 7093-7114.
O’donnell, T. F., Passman, M. A., Marston, W. A., Ennis, W. J., Dalsing, M., Kistner, R.
L., ... & Stoughton, J. (2014). Management of venous leg ulcers: Clinical practice
guidelines of the Society for Vascular Surgery® and the American Venous
Forum. Journal of vascular surgery, 60(2), 3S-59S.
References:
Derry, S., Stannard, C., Cole, P., Wiffen, P. J., Knaggs, R., Aldington, D., & Moore, R. A.
(2016). Fentanyl for neuropathic pain in adults. Cochrane Database of Systematic
Reviews, (10).
Dimauro, I., Grasso, L., Fittipaldi, S., Fantini, C., Mercatelli, N., Racca, S., ... & Borrione, P.
(2014). Platelet-rich plasma and skeletal muscle healing: a molecular analysis of the
early phases of the regeneration process in an experimental animal model. PloS
one, 9(7), e102993.
Flanagan, M. (2013). Wound healing and skin integrity: principles and practice. John Wiley
& Sons.
Grocott, P., Gethin, G., & Probst, S. (2013). Malignant wound management in advanced
illness: new insights. Current opinion in supportive and palliative care, 7(1), 101-
105.
Moore, Z. E., & Cowman, S. (2013). Wound cleansing for pressure ulcers. Cochrane
Database of Systematic Reviews, (3).
Moura, L. I., Dias, A. M., Carvalho, E., & de Sousa, H. C. (2013). Recent advances on the
development of wound dressings for diabetic foot ulcer treatment—a review. Acta
biomaterialia, 9(7), 7093-7114.
O’donnell, T. F., Passman, M. A., Marston, W. A., Ennis, W. J., Dalsing, M., Kistner, R.
L., ... & Stoughton, J. (2014). Management of venous leg ulcers: Clinical practice
guidelines of the Society for Vascular Surgery® and the American Venous
Forum. Journal of vascular surgery, 60(2), 3S-59S.
8WOUND MANAGEMENT
Powers, J. G., Higham, C., Broussard, K., & Phillips, T. J. (2016). Wound healing and
treating wounds: Chronic wound care and management. Journal of the American
Academy of Dermatology, 74(4), 607-625.
Schulz, P. J., & Nakamoto, K. (2013). Health literacy and patient empowerment in health
communication: the importance of separating conjoined twins. Patient education and
counseling, 90(1), 4-11.
Powers, J. G., Higham, C., Broussard, K., & Phillips, T. J. (2016). Wound healing and
treating wounds: Chronic wound care and management. Journal of the American
Academy of Dermatology, 74(4), 607-625.
Schulz, P. J., & Nakamoto, K. (2013). Health literacy and patient empowerment in health
communication: the importance of separating conjoined twins. Patient education and
counseling, 90(1), 4-11.
1 out of 9
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.