Esophageal Cancer Epidemiology and Risk Factors
VerifiedAdded on 2020/05/04
|10
|3279
|124
AI Summary
This assignment delves into the epidemiology of esophageal cancer, examining global trends, differences in incidence between Asian and Western populations, and the influence of various risk factors. It analyzes the role of tobacco, alcohol, obesity, dietary habits (particularly consumption of vegetables, fruits, and reflux-inducing foods), and genetic predispositions in esophageal cancer development. The assignment also touches upon the impact of Barrett's esophagus on the progression to adenocarcinoma.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: CRITICAL ANALYSIS
Critical Analysis
Name of the Student
Name of the University
Author note
Critical Analysis
Name of the Student
Name of the University
Author note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
2
CRITICAL ANALYSIS
Paper Selected: Reflux-Inducing Dietary Factors and Risk of Adenocarcinoma of the
Esophagus and Gastric Cardia
Overview of the Paper
Issues addressed in the paper
Over the last decades, the reported cases of adenocarcinoma of the esophagus
amounts to about less than 10% of all the esophageal cancers in the Western population
(Zhang, Jin, &Shen,2012). Reflux is the common risk factor associated with the esophageal
adenocarcinoma and gastric cardia cancer (Pohl et al., 2013). Moreover, the long term
sufferers with severe reflux symptoms, the risk of developing esophageal cancer increases
40-fold (Zhang, Jin, &Shen, 2012; Pohl et al., 2013). The reflux disease common among the
Western populations is chronic gastroesophageal reflux (GER) (Zhang, Jin, &Shen, 2012).
Western suffers from reflux at least once per week. In Sweden, there is an annual increase of
1.5% of the reflux disease over the tenure of 24 years (Stefanidis et al., 2010). Therefore,
identification of the factors responsible for the development of the reflux disease is important
for the individuals who are suffering from the discomfort of reflux like heartburn (Kahrilas et
al., 2012). Moreover, identification of the disease causing factors will also help towards the
development towards esophageal cancer prevention steps. There are multiple foods, which
are known to relax the lower esophageal sphincter (LES) and thus promoting reflux. These
reflux promoting food includes dietary fat, mints, chocolate, coffee, citrus food, tomato and
onions (Gonsalves et al., 2012). Not only this, dietary fat consumed in diet retards the process
of gastric emptying (Gonsalves et al., 2012) and this further increases the possibility of GER.
The principle aim of the study, conducted by Paul Terry et al.,2000, is to explore the
unaddressed parts in the esophageal carcinoma that is the effect of diet in development of
disease susceptibility. Their research question was whether observation of specific reflux-
provoking diet imparts any amount of risk towards the development of susceptibility of
adenocarcinoma of the esophagus and gastric cardia. The study also tries to elucidate the
effect of meal size and time of meal consumption (that is bedtime) on esophageal
adenocarcinoma.
Outcome of the research
There lays a strong association between the severity and frequency of reflux and risk
factor for developing esophageal and gastric cardia adeno carcinomas. The findings suggest
CRITICAL ANALYSIS
Paper Selected: Reflux-Inducing Dietary Factors and Risk of Adenocarcinoma of the
Esophagus and Gastric Cardia
Overview of the Paper
Issues addressed in the paper
Over the last decades, the reported cases of adenocarcinoma of the esophagus
amounts to about less than 10% of all the esophageal cancers in the Western population
(Zhang, Jin, &Shen,2012). Reflux is the common risk factor associated with the esophageal
adenocarcinoma and gastric cardia cancer (Pohl et al., 2013). Moreover, the long term
sufferers with severe reflux symptoms, the risk of developing esophageal cancer increases
40-fold (Zhang, Jin, &Shen, 2012; Pohl et al., 2013). The reflux disease common among the
Western populations is chronic gastroesophageal reflux (GER) (Zhang, Jin, &Shen, 2012).
Western suffers from reflux at least once per week. In Sweden, there is an annual increase of
1.5% of the reflux disease over the tenure of 24 years (Stefanidis et al., 2010). Therefore,
identification of the factors responsible for the development of the reflux disease is important
for the individuals who are suffering from the discomfort of reflux like heartburn (Kahrilas et
al., 2012). Moreover, identification of the disease causing factors will also help towards the
development towards esophageal cancer prevention steps. There are multiple foods, which
are known to relax the lower esophageal sphincter (LES) and thus promoting reflux. These
reflux promoting food includes dietary fat, mints, chocolate, coffee, citrus food, tomato and
onions (Gonsalves et al., 2012). Not only this, dietary fat consumed in diet retards the process
of gastric emptying (Gonsalves et al., 2012) and this further increases the possibility of GER.
The principle aim of the study, conducted by Paul Terry et al.,2000, is to explore the
unaddressed parts in the esophageal carcinoma that is the effect of diet in development of
disease susceptibility. Their research question was whether observation of specific reflux-
provoking diet imparts any amount of risk towards the development of susceptibility of
adenocarcinoma of the esophagus and gastric cardia. The study also tries to elucidate the
effect of meal size and time of meal consumption (that is bedtime) on esophageal
adenocarcinoma.
Outcome of the research
There lays a strong association between the severity and frequency of reflux and risk
factor for developing esophageal and gastric cardia adeno carcinomas. The findings suggest
3
CRITICAL ANALYSIS
that consumption of reflux promoting food is not a concern of public health for the general
population as dietary factors are not related with the threats of developing adenocarcinoma of
the esophagus or gastric cardia.
No significant trends were observed towards the development of the esophageal
adeno carcinoma upon consumption of the reflux promoting food. Moreover there was a
presence of non-significant, decreased risk of the disease development with the greater
consumption of leeks, onions and garlic. Not only this, there was no relation between the
development of squamous cell carcinoma and consumption of reflux causing food (however,
data was not shown in this case). The size and the time of the meal also turned out to be non-
significant in relation to the risk of the disease development, as elucidated via statistical
analysis. The additional adjustments like the presence or severity of the reflux symptoms
showed no significant alteration in the findings.
Study Design
The study was done via analyzing the affect of intake of LES-relaxing foods in a
nationwide population based case control study, which was done in Sweden. The study also
tried to elucidate dietary habits of these people and the subsequent affect on the
predisposition of esophagealadenocarcinoma. The study on done based on two core pillars of
biology, histology and anatomy. The histological slides were analysed by the pathologist.
Based on the histological and anatomical classification, the patients of cardia cancer and
adenocarcinoma were separated. Cardia cancer was isolated based as adenocarcinoma when
the centre was with the 2 cm proximal end and 3 cm from the distal end in comparison to the
gastroesophageal junction (Yan, Wistuba, Emmert-Buck & Erickson, 2011). If there was
visible appearance of Barrett's metaplasia, it was classified as esophageal, even if the
presence is within the cardia (Zhang, 2013).
All the subjects of the focus group gave a face-to-face interview, which was
conducted by a group of professional interviewers from Statistics Sweden and the entire
process of interview was computer oriented. A structured food frequency questionnaire
containing 63 different items of food and beverage was utilised to evaluate the dietary habits
of from the date of interview to 2 decades back. The questions mostly encompasses the rate
of consumption of food, the number of servings (per day, month or annually), the time of
dinner, average size of the meals and it was assessed by photographs of 4 different proportion
of 7 common Swedish dishes. The reflux symptoms are classified on the basis of presence or
CRITICAL ANALYSIS
that consumption of reflux promoting food is not a concern of public health for the general
population as dietary factors are not related with the threats of developing adenocarcinoma of
the esophagus or gastric cardia.
No significant trends were observed towards the development of the esophageal
adeno carcinoma upon consumption of the reflux promoting food. Moreover there was a
presence of non-significant, decreased risk of the disease development with the greater
consumption of leeks, onions and garlic. Not only this, there was no relation between the
development of squamous cell carcinoma and consumption of reflux causing food (however,
data was not shown in this case). The size and the time of the meal also turned out to be non-
significant in relation to the risk of the disease development, as elucidated via statistical
analysis. The additional adjustments like the presence or severity of the reflux symptoms
showed no significant alteration in the findings.
Study Design
The study was done via analyzing the affect of intake of LES-relaxing foods in a
nationwide population based case control study, which was done in Sweden. The study also
tried to elucidate dietary habits of these people and the subsequent affect on the
predisposition of esophagealadenocarcinoma. The study on done based on two core pillars of
biology, histology and anatomy. The histological slides were analysed by the pathologist.
Based on the histological and anatomical classification, the patients of cardia cancer and
adenocarcinoma were separated. Cardia cancer was isolated based as adenocarcinoma when
the centre was with the 2 cm proximal end and 3 cm from the distal end in comparison to the
gastroesophageal junction (Yan, Wistuba, Emmert-Buck & Erickson, 2011). If there was
visible appearance of Barrett's metaplasia, it was classified as esophageal, even if the
presence is within the cardia (Zhang, 2013).
All the subjects of the focus group gave a face-to-face interview, which was
conducted by a group of professional interviewers from Statistics Sweden and the entire
process of interview was computer oriented. A structured food frequency questionnaire
containing 63 different items of food and beverage was utilised to evaluate the dietary habits
of from the date of interview to 2 decades back. The questions mostly encompasses the rate
of consumption of food, the number of servings (per day, month or annually), the time of
dinner, average size of the meals and it was assessed by photographs of 4 different proportion
of 7 common Swedish dishes. The reflux symptoms are classified on the basis of presence or
4
CRITICAL ANALYSIS
absence of heart burn, its duration, frequency and severity. A severity index of the heart burn
was also created based on the nature and frequency of reflux.
The analysis of the data was done via statistical analysis via using Spearman
correlation co-efficient. Unconditional logistic regression was used based on multivariable
model. This multi-variable model include gender, BMI, total intake of energy, energy
adjusted intake of alcohol, intake of total fruits and vegetables and degree of cigarette
smoking.
Study population
The study was designed on the native population of Sweden and included people who
were less than 80 years old as on 1st December 1994 to 31st December 1997. All the people
who were recently diagnosed with esophageal adenocarcinoma (n = 216) and gastric cardia (n
= 313) were considered suitable for this study. The patients, who were suffering from the
squamous cell carcinoma of the esophagus and were under 80 years of age, were excluded
from the study. This is due to the fact squamous cell carcinoma and
esophagaladenocarcinoma has different disease mechanism all together (Agrawal et al.,
2012). Moreover, the risk of the squamous cell carcinoma is unrelated with GER.
The exclusion criteria or the non-participation among the esophagealadeno carcinoma
was 21.5 % (n = 27) and the cardia cancer patients was 16.3% (n = 51). So the total number
of the non-participations amounted to 84.6% (n=66). This non-participation is based on the
poor clinical condition of the patients or death, immediately after the diagnosis. Moreover
non-participation among the control group (n=308 or 27%) was attributed due to
unwillingness to participate. 7 subjects were excluded from the analysis due to their poor
total energy intake, indicating erroneous dietary questions responses. 3 subjects were
excluded because of the lack of information of the Body Mass Index (BMI). The other 2
subjects were excluded from the study due to poor response of the dietary questions. After
implementing all the exclusion criteria there were 185 participants under
esophagealadenocarcinoma, 258 participants of cardiaadenocarcinoma and 815 participants
were used a placebo group or control.
Main findings
The food, which have shown positive effects in the development of temporary GER or
relaxed LER in previous laboratory experiments, may not taken in significant quantity.
CRITICAL ANALYSIS
absence of heart burn, its duration, frequency and severity. A severity index of the heart burn
was also created based on the nature and frequency of reflux.
The analysis of the data was done via statistical analysis via using Spearman
correlation co-efficient. Unconditional logistic regression was used based on multivariable
model. This multi-variable model include gender, BMI, total intake of energy, energy
adjusted intake of alcohol, intake of total fruits and vegetables and degree of cigarette
smoking.
Study population
The study was designed on the native population of Sweden and included people who
were less than 80 years old as on 1st December 1994 to 31st December 1997. All the people
who were recently diagnosed with esophageal adenocarcinoma (n = 216) and gastric cardia (n
= 313) were considered suitable for this study. The patients, who were suffering from the
squamous cell carcinoma of the esophagus and were under 80 years of age, were excluded
from the study. This is due to the fact squamous cell carcinoma and
esophagaladenocarcinoma has different disease mechanism all together (Agrawal et al.,
2012). Moreover, the risk of the squamous cell carcinoma is unrelated with GER.
The exclusion criteria or the non-participation among the esophagealadeno carcinoma
was 21.5 % (n = 27) and the cardia cancer patients was 16.3% (n = 51). So the total number
of the non-participations amounted to 84.6% (n=66). This non-participation is based on the
poor clinical condition of the patients or death, immediately after the diagnosis. Moreover
non-participation among the control group (n=308 or 27%) was attributed due to
unwillingness to participate. 7 subjects were excluded from the analysis due to their poor
total energy intake, indicating erroneous dietary questions responses. 3 subjects were
excluded because of the lack of information of the Body Mass Index (BMI). The other 2
subjects were excluded from the study due to poor response of the dietary questions. After
implementing all the exclusion criteria there were 185 participants under
esophagealadenocarcinoma, 258 participants of cardiaadenocarcinoma and 815 participants
were used a placebo group or control.
Main findings
The food, which have shown positive effects in the development of temporary GER or
relaxed LER in previous laboratory experiments, may not taken in significant quantity.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
5
CRITICAL ANALYSIS
Moreover, the development of the temporary reflux caused by the exposure of food as
elucidated in previous laboratory study might be qualitatively different. As proposed by this
study, such disease may be different from inflammation-causing reflux characteristic of GER.
Another possible explanation given by the researchers of this study behind the non-
dependence of the food habit on the development of the GERD and subsequent
esophagealadeno carcinoma is people who suffers from GERD feels fuller due to lack of
appetite and hence consume small servings of food(Bohdjalian et al., 2010). Moreover, the
reflux promoting foods like tomato, citrus food, onions and garlic are rich on anti-
carcinogenic content and hence can be claimed to be related with the development of GERD
linked esophagealadeno carcinoma (Steevens, Schouten, Goldbohm& van den Brandt, 2011).
Future research scope
The findings to this study are completely different from the other previous findings.
Previous findings showed that the consumption of the reflux initiating food is associated with
the development of GERD, promoting the increase in the susceptibility of esophagusadeno
carcinoma. However, the research carried out by Terry et al., showed no significant
association with the dietary habits with the disease development. Future research scope will
be thus directed towards the further refinement of the research in order to strengthen of the
findings. This refinement of the research must be done via choosing a different population
group in the western population apart from the Swedish population. The refinement of the
results obtained can also be done via testing the validity of the research on potent reflux
generating food which scores zero in the amount of anti-carcinogenic content like the
carbonated beverages.
Internal Validity
Confounding
The results are likely to be affected by the biases including cofounding. The
cofounding will arise as a result of the baseline characteristic of the study subjects. The
median age of the controls (68 years) and the target group (67 years) was not kept same; there
exist a one year difference between the two. Apart from these minor biases, there also exists
some significant bias factor in this study done by Terry et al., (2000). The target Swedish
population, which was selected for the study lacks equality in gender. Here the men
comprised of 86% of the cases with 83% attributing for the control group. Moreover, the
CRITICAL ANALYSIS
Moreover, the development of the temporary reflux caused by the exposure of food as
elucidated in previous laboratory study might be qualitatively different. As proposed by this
study, such disease may be different from inflammation-causing reflux characteristic of GER.
Another possible explanation given by the researchers of this study behind the non-
dependence of the food habit on the development of the GERD and subsequent
esophagealadeno carcinoma is people who suffers from GERD feels fuller due to lack of
appetite and hence consume small servings of food(Bohdjalian et al., 2010). Moreover, the
reflux promoting foods like tomato, citrus food, onions and garlic are rich on anti-
carcinogenic content and hence can be claimed to be related with the development of GERD
linked esophagealadeno carcinoma (Steevens, Schouten, Goldbohm& van den Brandt, 2011).
Future research scope
The findings to this study are completely different from the other previous findings.
Previous findings showed that the consumption of the reflux initiating food is associated with
the development of GERD, promoting the increase in the susceptibility of esophagusadeno
carcinoma. However, the research carried out by Terry et al., showed no significant
association with the dietary habits with the disease development. Future research scope will
be thus directed towards the further refinement of the research in order to strengthen of the
findings. This refinement of the research must be done via choosing a different population
group in the western population apart from the Swedish population. The refinement of the
results obtained can also be done via testing the validity of the research on potent reflux
generating food which scores zero in the amount of anti-carcinogenic content like the
carbonated beverages.
Internal Validity
Confounding
The results are likely to be affected by the biases including cofounding. The
cofounding will arise as a result of the baseline characteristic of the study subjects. The
median age of the controls (68 years) and the target group (67 years) was not kept same; there
exist a one year difference between the two. Apart from these minor biases, there also exists
some significant bias factor in this study done by Terry et al., (2000). The target Swedish
population, which was selected for the study lacks equality in gender. Here the men
comprised of 86% of the cases with 83% attributing for the control group. Moreover, the
6
CRITICAL ANALYSIS
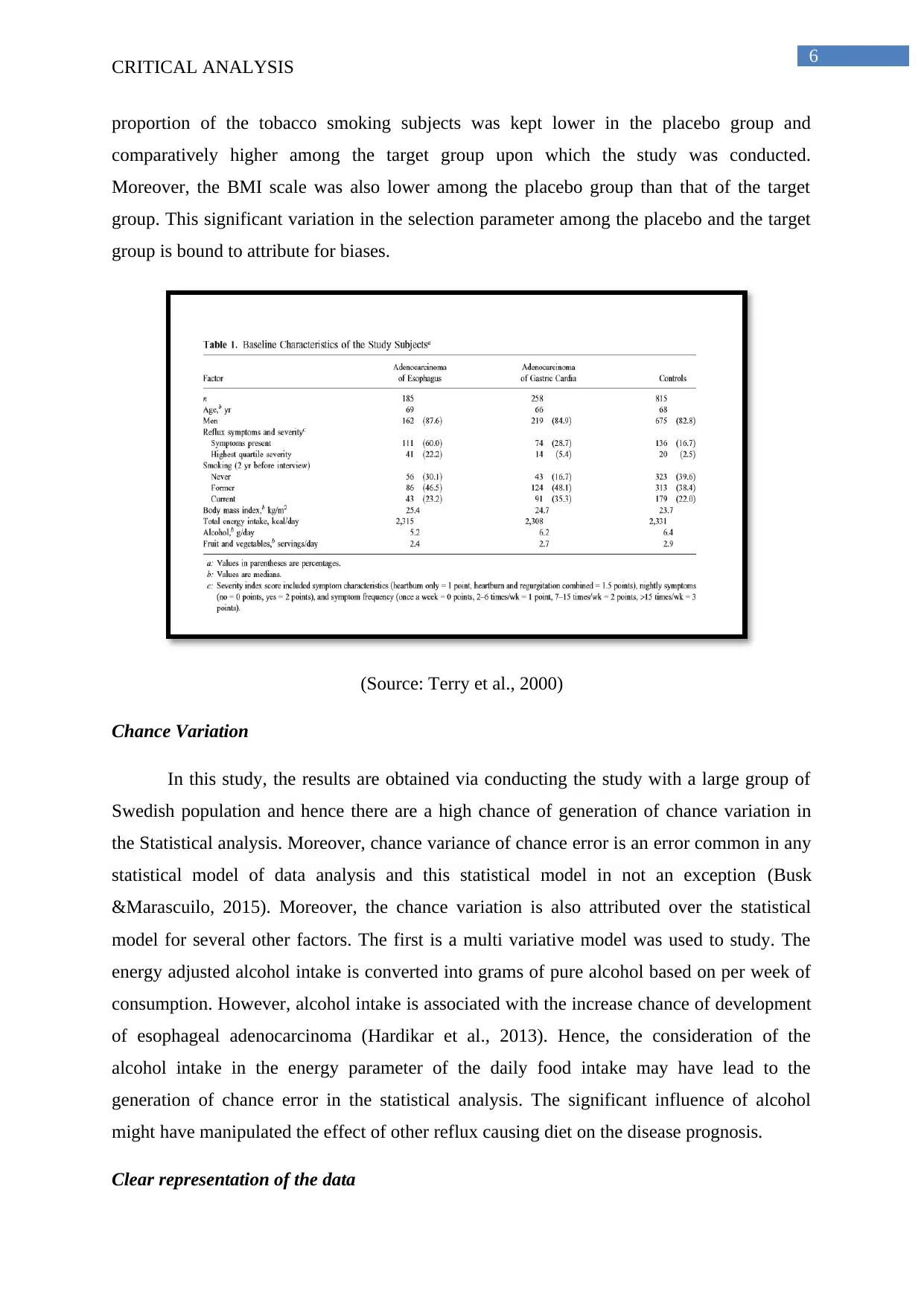
proportion of the tobacco smoking subjects was kept lower in the placebo group and
comparatively higher among the target group upon which the study was conducted.
Moreover, the BMI scale was also lower among the placebo group than that of the target
group. This significant variation in the selection parameter among the placebo and the target
group is bound to attribute for biases.
(Source: Terry et al., 2000)
Chance Variation
In this study, the results are obtained via conducting the study with a large group of
Swedish population and hence there are a high chance of generation of chance variation in
the Statistical analysis. Moreover, chance variance of chance error is an error common in any
statistical model of data analysis and this statistical model in not an exception (Busk
&Marascuilo, 2015). Moreover, the chance variation is also attributed over the statistical
model for several other factors. The first is a multi variative model was used to study. The
energy adjusted alcohol intake is converted into grams of pure alcohol based on per week of
consumption. However, alcohol intake is associated with the increase chance of development
of esophageal adenocarcinoma (Hardikar et al., 2013). Hence, the consideration of the
alcohol intake in the energy parameter of the daily food intake may have lead to the
generation of chance error in the statistical analysis. The significant influence of alcohol
might have manipulated the effect of other reflux causing diet on the disease prognosis.
Clear representation of the data
CRITICAL ANALYSIS
proportion of the tobacco smoking subjects was kept lower in the placebo group and
comparatively higher among the target group upon which the study was conducted.
Moreover, the BMI scale was also lower among the placebo group than that of the target
group. This significant variation in the selection parameter among the placebo and the target
group is bound to attribute for biases.
(Source: Terry et al., 2000)
Chance Variation
In this study, the results are obtained via conducting the study with a large group of
Swedish population and hence there are a high chance of generation of chance variation in
the Statistical analysis. Moreover, chance variance of chance error is an error common in any
statistical model of data analysis and this statistical model in not an exception (Busk
&Marascuilo, 2015). Moreover, the chance variation is also attributed over the statistical
model for several other factors. The first is a multi variative model was used to study. The
energy adjusted alcohol intake is converted into grams of pure alcohol based on per week of
consumption. However, alcohol intake is associated with the increase chance of development
of esophageal adenocarcinoma (Hardikar et al., 2013). Hence, the consideration of the
alcohol intake in the energy parameter of the daily food intake may have lead to the
generation of chance error in the statistical analysis. The significant influence of alcohol
might have manipulated the effect of other reflux causing diet on the disease prognosis.
Clear representation of the data
7
CRITICAL ANALYSIS
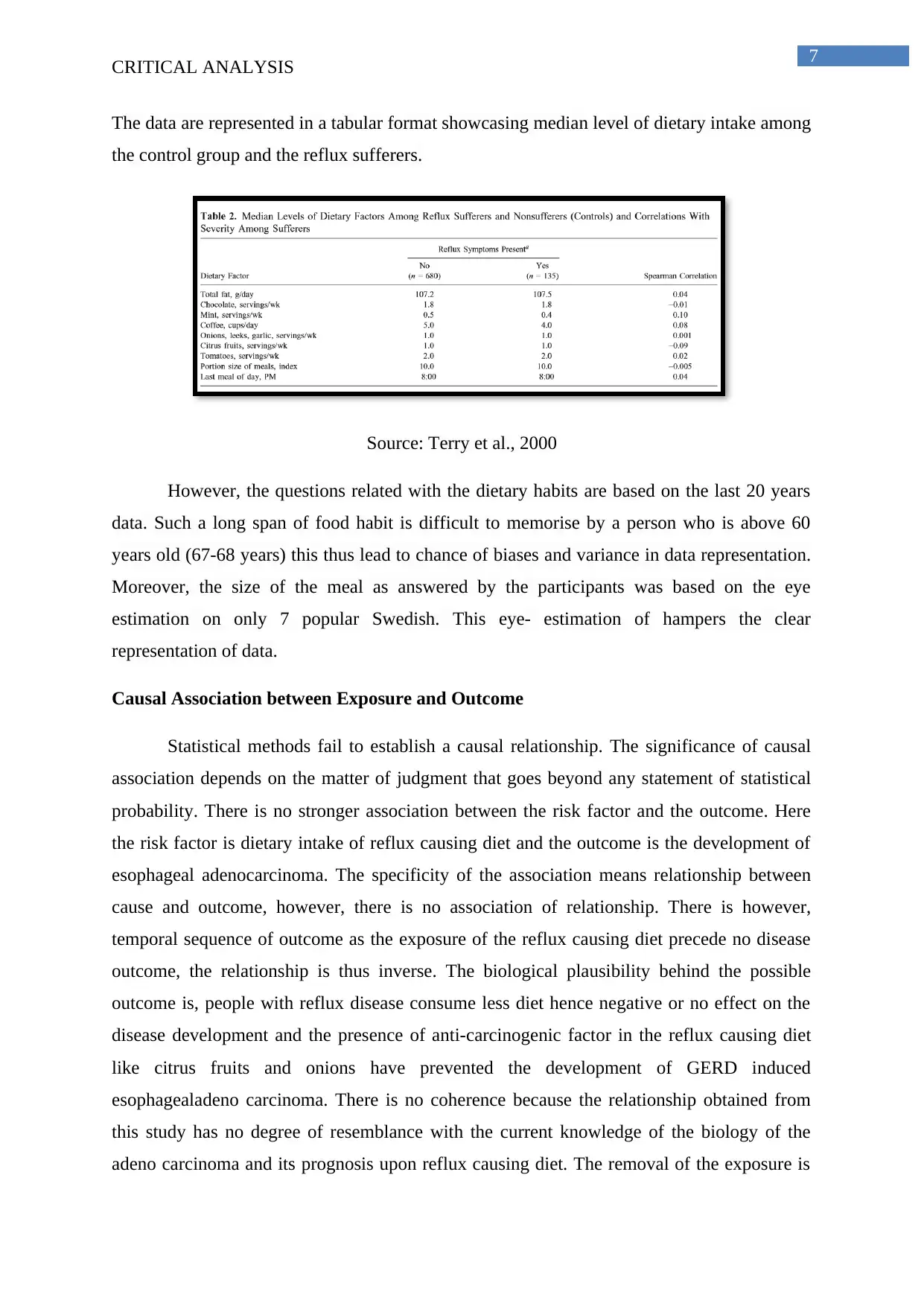
The data are represented in a tabular format showcasing median level of dietary intake among
the control group and the reflux sufferers.
Source: Terry et al., 2000
However, the questions related with the dietary habits are based on the last 20 years
data. Such a long span of food habit is difficult to memorise by a person who is above 60
years old (67-68 years) this thus lead to chance of biases and variance in data representation.
Moreover, the size of the meal as answered by the participants was based on the eye
estimation on only 7 popular Swedish. This eye- estimation of hampers the clear
representation of data.
Causal Association between Exposure and Outcome
Statistical methods fail to establish a causal relationship. The significance of causal
association depends on the matter of judgment that goes beyond any statement of statistical
probability. There is no stronger association between the risk factor and the outcome. Here
the risk factor is dietary intake of reflux causing diet and the outcome is the development of
esophageal adenocarcinoma. The specificity of the association means relationship between
cause and outcome, however, there is no association of relationship. There is however,
temporal sequence of outcome as the exposure of the reflux causing diet precede no disease
outcome, the relationship is thus inverse. The biological plausibility behind the possible
outcome is, people with reflux disease consume less diet hence negative or no effect on the
disease development and the presence of anti-carcinogenic factor in the reflux causing diet
like citrus fruits and onions have prevented the development of GERD induced
esophagealadeno carcinoma. There is no coherence because the relationship obtained from
this study has no degree of resemblance with the current knowledge of the biology of the
adeno carcinoma and its prognosis upon reflux causing diet. The removal of the exposure is
CRITICAL ANALYSIS
The data are represented in a tabular format showcasing median level of dietary intake among
the control group and the reflux sufferers.
Source: Terry et al., 2000
However, the questions related with the dietary habits are based on the last 20 years
data. Such a long span of food habit is difficult to memorise by a person who is above 60
years old (67-68 years) this thus lead to chance of biases and variance in data representation.
Moreover, the size of the meal as answered by the participants was based on the eye
estimation on only 7 popular Swedish. This eye- estimation of hampers the clear
representation of data.
Causal Association between Exposure and Outcome
Statistical methods fail to establish a causal relationship. The significance of causal
association depends on the matter of judgment that goes beyond any statement of statistical
probability. There is no stronger association between the risk factor and the outcome. Here
the risk factor is dietary intake of reflux causing diet and the outcome is the development of
esophageal adenocarcinoma. The specificity of the association means relationship between
cause and outcome, however, there is no association of relationship. There is however,
temporal sequence of outcome as the exposure of the reflux causing diet precede no disease
outcome, the relationship is thus inverse. The biological plausibility behind the possible
outcome is, people with reflux disease consume less diet hence negative or no effect on the
disease development and the presence of anti-carcinogenic factor in the reflux causing diet
like citrus fruits and onions have prevented the development of GERD induced
esophagealadeno carcinoma. There is no coherence because the relationship obtained from
this study has no degree of resemblance with the current knowledge of the biology of the
adeno carcinoma and its prognosis upon reflux causing diet. The removal of the exposure is
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
CRITICAL ANALYSIS
expected to alter the frequency of the outcomes as shown by the placebo group. Thus overall,
there is a lack of causal relationship.
External Validity
Application to source population
Here the source population is the Swedish population. But the majority of the
epidemiological analysis was done over males who were 67-68 years old. Thus the final
results though significant with this specific population group, may extract different results
altogether when applied over females who are suppose 50 to 55 years (or more than that).
Here the population taken for the study smokes tobacco and consumes alcohol and hence the
results may be different when applied to a Swedish population of same age group and gender
but are non-smokers.
Application to relevant population
The external validity of the study is determined by the fact that how it can be
successfully implemented over other relevant population. The present research uses
population based case-control study, Swedish population. The external validity will be
established when other western populations, apart from Sweden, produce same results on the
disease pre-disposition and effects of dietary intake. However, the criteria, which have been
undertaken for sampling and for separating the placebo group from the target group must also
be maintain or applied to other population. The criteria taken for sampling is not generalised
and hence the relevancy of external validity is questionable.
CRITICAL ANALYSIS
expected to alter the frequency of the outcomes as shown by the placebo group. Thus overall,
there is a lack of causal relationship.
External Validity
Application to source population
Here the source population is the Swedish population. But the majority of the
epidemiological analysis was done over males who were 67-68 years old. Thus the final
results though significant with this specific population group, may extract different results
altogether when applied over females who are suppose 50 to 55 years (or more than that).
Here the population taken for the study smokes tobacco and consumes alcohol and hence the
results may be different when applied to a Swedish population of same age group and gender
but are non-smokers.
Application to relevant population
The external validity of the study is determined by the fact that how it can be
successfully implemented over other relevant population. The present research uses
population based case-control study, Swedish population. The external validity will be
established when other western populations, apart from Sweden, produce same results on the
disease pre-disposition and effects of dietary intake. However, the criteria, which have been
undertaken for sampling and for separating the placebo group from the target group must also
be maintain or applied to other population. The criteria taken for sampling is not generalised
and hence the relevancy of external validity is questionable.
9
CRITICAL ANALYSIS
References
Agrawal, N., Jiao, Y., Bettegowda, C., Hutfless, S. M., Wang, Y., David, S., ...& Wang, L. D.
(2012). Comparative genomic analysis of esophageal adenocarcinoma and squamous
cell carcinoma. Cancer discovery, 2(10), 899-905.
Bohdjalian, A., Langer, F. B., Shakeri-Leidenmühler, S., Gfrerer, L., Ludvik, B., Zacherl, J.,
&Prager, G. (2010). Sleeve gastrectomy as sole and definitive bariatric procedure: 5-
year results for weight loss and ghrelin. Obesity surgery, 20(5), 535-540.
Busk, P. L., &Marascuilo, L. A. (2015). Statistical Analysis in Single-Case Research. Single-
Case Research Design and Analysis (Psychology Revivals): New Directions for
Psychology and Education, 159.
Gonsalves, N., Yang, G. Y., Doerfler, B., Ritz, S., Ditto, A. M., & Hirano, I. (2012).
Elimination diet effectively treats eosinophilic esophagitis in adults; food
reintroduction identifies causative factors. Gastroenterology, 142(7), 1451-1459.
Hardikar, S., Onstad, L., Blount, P. L., Odze, R. D., Reid, B. J., & Vaughan, T. L. (2013).
The role of tobacco, alcohol, and obesity in neoplastic progression to esophageal
adenocarcinoma: a prospective study of Barrett's esophagus. PloS one, 8(1), e52192.
Kahrilas, P. J., Jonsson, A., Denison, H., Wernersson, B., Hughes, N., &Howden, C. W.
(2012). Regurgitation is less responsive to acid suppression than heartburn in patients
with gastroesophageal reflux disease. Clinical Gastroenterology and
Hepatology, 10(6), 612-619.
Pohl, H., Wrobel, K., Bojarski, C., Voderholzer, W., Sonnenberg, A., Rösch, T., &Baumgart,
D. C. (2013).Risk factors in the development of esophageal adenocarcinoma. The
American journal of gastroenterology, 108(2), 200-207.
Steevens, J., Schouten, L. J., Goldbohm, R. A., & van den Brandt, P. A. (2011).Vegetables
and fruits consumption and risk of esophageal and gastric cancer subtypes in the
Netherlands Cohort Study. International journal of cancer, 129(11), 2681-2693.
Stefanidis, D., Hope, W. W., Kohn, G. P., Reardon, P. R., Richardson, W. S., Fanelli, R. D.,
& SAGES Guidelines Committee. (2010). Guidelines for surgical treatment of
gastroesophageal reflux disease. Surgical endoscopy, 24(11), 2647-2669.
CRITICAL ANALYSIS
References
Agrawal, N., Jiao, Y., Bettegowda, C., Hutfless, S. M., Wang, Y., David, S., ...& Wang, L. D.
(2012). Comparative genomic analysis of esophageal adenocarcinoma and squamous
cell carcinoma. Cancer discovery, 2(10), 899-905.
Bohdjalian, A., Langer, F. B., Shakeri-Leidenmühler, S., Gfrerer, L., Ludvik, B., Zacherl, J.,
&Prager, G. (2010). Sleeve gastrectomy as sole and definitive bariatric procedure: 5-
year results for weight loss and ghrelin. Obesity surgery, 20(5), 535-540.
Busk, P. L., &Marascuilo, L. A. (2015). Statistical Analysis in Single-Case Research. Single-
Case Research Design and Analysis (Psychology Revivals): New Directions for
Psychology and Education, 159.
Gonsalves, N., Yang, G. Y., Doerfler, B., Ritz, S., Ditto, A. M., & Hirano, I. (2012).
Elimination diet effectively treats eosinophilic esophagitis in adults; food
reintroduction identifies causative factors. Gastroenterology, 142(7), 1451-1459.
Hardikar, S., Onstad, L., Blount, P. L., Odze, R. D., Reid, B. J., & Vaughan, T. L. (2013).
The role of tobacco, alcohol, and obesity in neoplastic progression to esophageal
adenocarcinoma: a prospective study of Barrett's esophagus. PloS one, 8(1), e52192.
Kahrilas, P. J., Jonsson, A., Denison, H., Wernersson, B., Hughes, N., &Howden, C. W.
(2012). Regurgitation is less responsive to acid suppression than heartburn in patients
with gastroesophageal reflux disease. Clinical Gastroenterology and
Hepatology, 10(6), 612-619.
Pohl, H., Wrobel, K., Bojarski, C., Voderholzer, W., Sonnenberg, A., Rösch, T., &Baumgart,
D. C. (2013).Risk factors in the development of esophageal adenocarcinoma. The
American journal of gastroenterology, 108(2), 200-207.
Steevens, J., Schouten, L. J., Goldbohm, R. A., & van den Brandt, P. A. (2011).Vegetables
and fruits consumption and risk of esophageal and gastric cancer subtypes in the
Netherlands Cohort Study. International journal of cancer, 129(11), 2681-2693.
Stefanidis, D., Hope, W. W., Kohn, G. P., Reardon, P. R., Richardson, W. S., Fanelli, R. D.,
& SAGES Guidelines Committee. (2010). Guidelines for surgical treatment of
gastroesophageal reflux disease. Surgical endoscopy, 24(11), 2647-2669.
10
CRITICAL ANALYSIS
Terry, P., Lagergren, J., Wolk, A., &Nyrén, O. (2000).Reflux-Inducing Dietary Factors and
Risk ofAdenocarcinoma of the Esophagus and Gastric Cardia. Nutrition and
cancer, 38(2), 186-191.
Yan, W., Wistuba, I. I., Emmert-Buck, M. R., & Erickson, H. S. (2011).Squamous cell
carcinoma–similarities and differences among anatomical sites. American journal of
cancer research, 1(3), 275.
Zhang, H. Z., Jin, G. F., &Shen, H. B. (2012).Epidemiologic differences in esophageal cancer
between Asian and Western populations. Chinese journal of cancer, 31(6), 281.
Zhang, Y. (2013). Epidemiology of esophageal cancer. World journal of gastroenterology:
WJG, 19(34), 5598.
CRITICAL ANALYSIS
Terry, P., Lagergren, J., Wolk, A., &Nyrén, O. (2000).Reflux-Inducing Dietary Factors and
Risk ofAdenocarcinoma of the Esophagus and Gastric Cardia. Nutrition and
cancer, 38(2), 186-191.
Yan, W., Wistuba, I. I., Emmert-Buck, M. R., & Erickson, H. S. (2011).Squamous cell
carcinoma–similarities and differences among anatomical sites. American journal of
cancer research, 1(3), 275.
Zhang, H. Z., Jin, G. F., &Shen, H. B. (2012).Epidemiologic differences in esophageal cancer
between Asian and Western populations. Chinese journal of cancer, 31(6), 281.
Zhang, Y. (2013). Epidemiology of esophageal cancer. World journal of gastroenterology:
WJG, 19(34), 5598.
1 out of 10


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.