Y-BOCS Symptom Checklist for OCD: Symptoms, Examples, and Types
VerifiedAdded on 2023/06/15
|21
|6501
|485
AI Summary
The Y-BOCS Symptom Checklist is a comprehensive checklist for OCD symptoms, including aggressive obsessions, contamination obsessions, sexual obsessions, hoarding/saving obsessions, religious obsessions, somatic obsessions, cleaning/washing compulsions, checking compulsions, repeating compulsions, ordering/arranging compulsions, hoarding/collecting compulsions, and miscellaneous compulsions. The checklist includes current and past symptoms, examples, and types of each obsession and compulsion.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
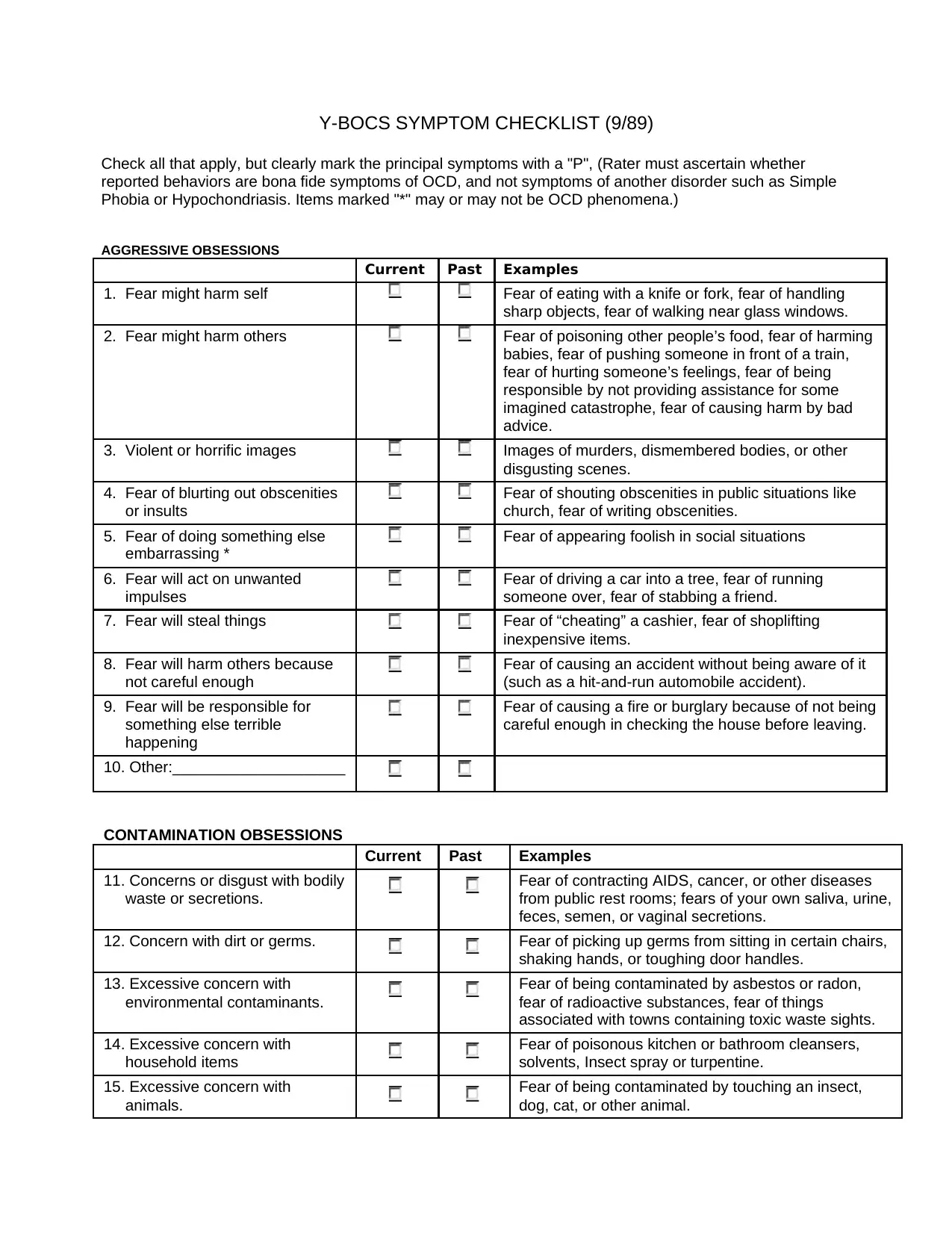
Y-BOCS SYMPTOM CHECKLIST (9/89)
Check all that apply, but clearly mark the principal symptoms with a "P", (Rater must ascertain whether
reported behaviors are bona fide symptoms of OCD, and not symptoms of another disorder such as Simple
Phobia or Hypochondriasis. Items marked "*" may or may not be OCD phenomena.)
AGGRESSIVE OBSESSIONS
Current Past Examples
1. Fear might harm self Fear of eating with a knife or fork, fear of handling
sharp objects, fear of walking near glass windows.
2. Fear might harm others Fear of poisoning other people’s food, fear of harming
babies, fear of pushing someone in front of a train,
fear of hurting someone’s feelings, fear of being
responsible by not providing assistance for some
imagined catastrophe, fear of causing harm by bad
advice.
3. Violent or horrific images Images of murders, dismembered bodies, or other
disgusting scenes.
4. Fear of blurting out obscenities Fear of shouting obscenities in public situations like
or insults church, fear of writing obscenities.
5. Fear of doing something else Fear of appearing foolish in social situations
embarrassing *
6. Fear will act on unwanted Fear of driving a car into a tree, fear of running
impulses someone over, fear of stabbing a friend.
7. Fear will steal things Fear of “cheating” a cashier, fear of shoplifting
inexpensive items.
8. Fear will harm others because Fear of causing an accident without being aware of it
not careful enough (such as a hit-and-run automobile accident).
9. Fear will be responsible for Fear of causing a fire or burglary because of not being
something else terrible careful enough in checking the house before leaving.
happening
10. Other:____________________
CONTAMINATION OBSESSIONS
Current Past Examples
11. Concerns or disgust with bodily Fear of contracting AIDS, cancer, or other diseases
waste or secretions. from public rest rooms; fears of your own saliva, urine,
feces, semen, or vaginal secretions.
12. Concern with dirt or germs. Fear of picking up germs from sitting in certain chairs,
shaking hands, or toughing door handles.
13. Excessive concern with Fear of being contaminated by asbestos or radon,
environmental contaminants. fear of radioactive substances, fear of things
associated with towns containing toxic waste sights.
14. Excessive concern with Fear of poisonous kitchen or bathroom cleansers,
household items solvents, Insect spray or turpentine.
15. Excessive concern with Fear of being contaminated by touching an insect,
animals. dog, cat, or other animal.
Check all that apply, but clearly mark the principal symptoms with a "P", (Rater must ascertain whether
reported behaviors are bona fide symptoms of OCD, and not symptoms of another disorder such as Simple
Phobia or Hypochondriasis. Items marked "*" may or may not be OCD phenomena.)
AGGRESSIVE OBSESSIONS
Current Past Examples
1. Fear might harm self Fear of eating with a knife or fork, fear of handling
sharp objects, fear of walking near glass windows.
2. Fear might harm others Fear of poisoning other people’s food, fear of harming
babies, fear of pushing someone in front of a train,
fear of hurting someone’s feelings, fear of being
responsible by not providing assistance for some
imagined catastrophe, fear of causing harm by bad
advice.
3. Violent or horrific images Images of murders, dismembered bodies, or other
disgusting scenes.
4. Fear of blurting out obscenities Fear of shouting obscenities in public situations like
or insults church, fear of writing obscenities.
5. Fear of doing something else Fear of appearing foolish in social situations
embarrassing *
6. Fear will act on unwanted Fear of driving a car into a tree, fear of running
impulses someone over, fear of stabbing a friend.
7. Fear will steal things Fear of “cheating” a cashier, fear of shoplifting
inexpensive items.
8. Fear will harm others because Fear of causing an accident without being aware of it
not careful enough (such as a hit-and-run automobile accident).
9. Fear will be responsible for Fear of causing a fire or burglary because of not being
something else terrible careful enough in checking the house before leaving.
happening
10. Other:____________________
CONTAMINATION OBSESSIONS
Current Past Examples
11. Concerns or disgust with bodily Fear of contracting AIDS, cancer, or other diseases
waste or secretions. from public rest rooms; fears of your own saliva, urine,
feces, semen, or vaginal secretions.
12. Concern with dirt or germs. Fear of picking up germs from sitting in certain chairs,
shaking hands, or toughing door handles.
13. Excessive concern with Fear of being contaminated by asbestos or radon,
environmental contaminants. fear of radioactive substances, fear of things
associated with towns containing toxic waste sights.
14. Excessive concern with Fear of poisonous kitchen or bathroom cleansers,
household items solvents, Insect spray or turpentine.
15. Excessive concern with Fear of being contaminated by touching an insect,
animals. dog, cat, or other animal.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
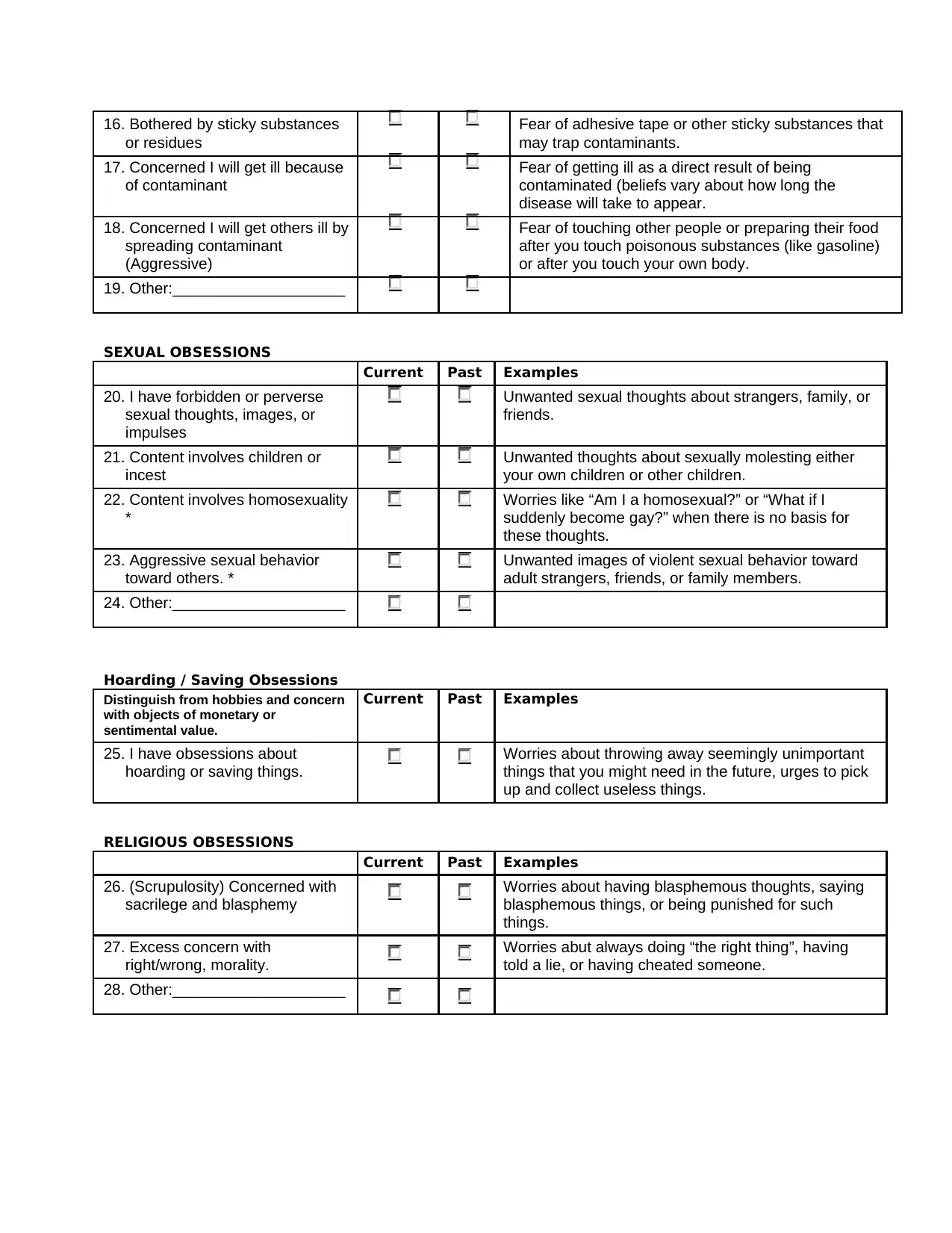
16. Bothered by sticky substances Fear of adhesive tape or other sticky substances that
or residues may trap contaminants.
17. Concerned I will get ill because Fear of getting ill as a direct result of being
of contaminant contaminated (beliefs vary about how long the
disease will take to appear.
18. Concerned I will get others ill by Fear of touching other people or preparing their food
spreading contaminant after you touch poisonous substances (like gasoline)
(Aggressive) or after you touch your own body.
19. Other:____________________
SEXUAL OBSESSIONS
Current Past Examples
20. I have forbidden or perverse Unwanted sexual thoughts about strangers, family, or
sexual thoughts, images, or friends.
impulses
21. Content involves children or Unwanted thoughts about sexually molesting either
incest your own children or other children.
22. Content involves homosexuality Worries like “Am I a homosexual?” or “What if I
* suddenly become gay?” when there is no basis for
these thoughts.
23. Aggressive sexual behavior Unwanted images of violent sexual behavior toward
toward others. * adult strangers, friends, or family members.
24. Other:____________________
Hoarding / Saving Obsessions
Distinguish from hobbies and concern Current Past Examples
with objects of monetary or
sentimental value.
25. I have obsessions about Worries about throwing away seemingly unimportant
hoarding or saving things. things that you might need in the future, urges to pick
up and collect useless things.
RELIGIOUS OBSESSIONS
Current Past Examples
26. (Scrupulosity) Concerned with Worries about having blasphemous thoughts, saying
sacrilege and blasphemy blasphemous things, or being punished for such
things.
27. Excess concern with Worries abut always doing “the right thing”, having
right/wrong, morality. told a lie, or having cheated someone.
28. Other:____________________
or residues may trap contaminants.
17. Concerned I will get ill because Fear of getting ill as a direct result of being
of contaminant contaminated (beliefs vary about how long the
disease will take to appear.
18. Concerned I will get others ill by Fear of touching other people or preparing their food
spreading contaminant after you touch poisonous substances (like gasoline)
(Aggressive) or after you touch your own body.
19. Other:____________________
SEXUAL OBSESSIONS
Current Past Examples
20. I have forbidden or perverse Unwanted sexual thoughts about strangers, family, or
sexual thoughts, images, or friends.
impulses
21. Content involves children or Unwanted thoughts about sexually molesting either
incest your own children or other children.
22. Content involves homosexuality Worries like “Am I a homosexual?” or “What if I
* suddenly become gay?” when there is no basis for
these thoughts.
23. Aggressive sexual behavior Unwanted images of violent sexual behavior toward
toward others. * adult strangers, friends, or family members.
24. Other:____________________
Hoarding / Saving Obsessions
Distinguish from hobbies and concern Current Past Examples
with objects of monetary or
sentimental value.
25. I have obsessions about Worries about throwing away seemingly unimportant
hoarding or saving things. things that you might need in the future, urges to pick
up and collect useless things.
RELIGIOUS OBSESSIONS
Current Past Examples
26. (Scrupulosity) Concerned with Worries about having blasphemous thoughts, saying
sacrilege and blasphemy blasphemous things, or being punished for such
things.
27. Excess concern with Worries abut always doing “the right thing”, having
right/wrong, morality. told a lie, or having cheated someone.
28. Other:____________________
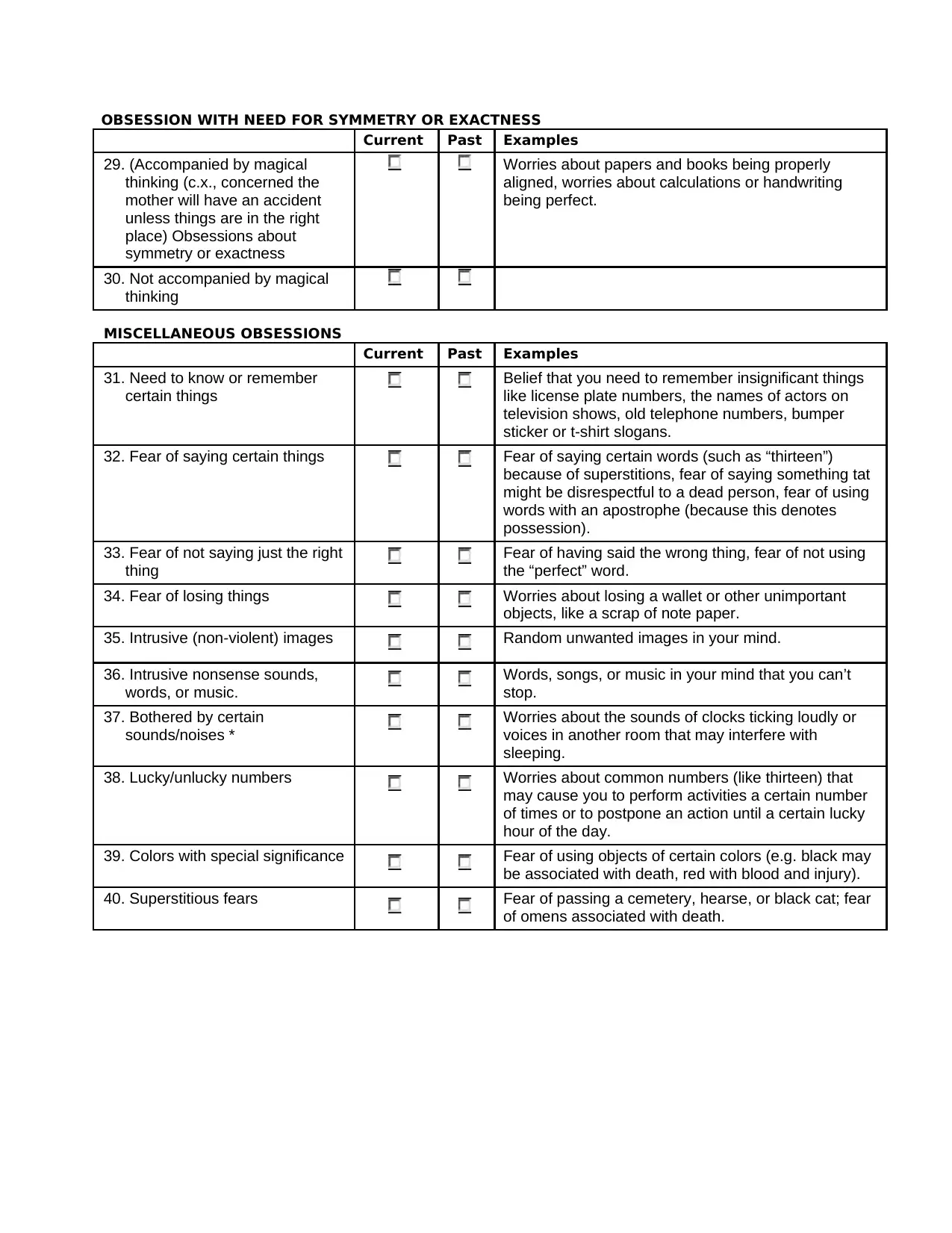
OBSESSION WITH NEED FOR SYMMETRY OR EXACTNESS
Current Past Examples
29. (Accompanied by magical Worries about papers and books being properly
thinking (c.x., concerned the aligned, worries about calculations or handwriting
mother will have an accident being perfect.
unless things are in the right
place) Obsessions about
symmetry or exactness
30. Not accompanied by magical
thinking
MISCELLANEOUS OBSESSIONS
Current Past Examples
31. Need to know or remember Belief that you need to remember insignificant things
certain things like license plate numbers, the names of actors on
television shows, old telephone numbers, bumper
sticker or t-shirt slogans.
32. Fear of saying certain things Fear of saying certain words (such as “thirteen”)
because of superstitions, fear of saying something tat
might be disrespectful to a dead person, fear of using
words with an apostrophe (because this denotes
possession).
33. Fear of not saying just the right Fear of having said the wrong thing, fear of not using
thing the “perfect” word.
34. Fear of losing things Worries about losing a wallet or other unimportant
objects, like a scrap of note paper.
35. Intrusive (non-violent) images Random unwanted images in your mind.
36. Intrusive nonsense sounds, Words, songs, or music in your mind that you can’t
words, or music. stop.
37. Bothered by certain Worries about the sounds of clocks ticking loudly or
sounds/noises * voices in another room that may interfere with
sleeping.
38. Lucky/unlucky numbers Worries about common numbers (like thirteen) that
may cause you to perform activities a certain number
of times or to postpone an action until a certain lucky
hour of the day.
39. Colors with special significance Fear of using objects of certain colors (e.g. black may
be associated with death, red with blood and injury).
40. Superstitious fears Fear of passing a cemetery, hearse, or black cat; fear
of omens associated with death.
Current Past Examples
29. (Accompanied by magical Worries about papers and books being properly
thinking (c.x., concerned the aligned, worries about calculations or handwriting
mother will have an accident being perfect.
unless things are in the right
place) Obsessions about
symmetry or exactness
30. Not accompanied by magical
thinking
MISCELLANEOUS OBSESSIONS
Current Past Examples
31. Need to know or remember Belief that you need to remember insignificant things
certain things like license plate numbers, the names of actors on
television shows, old telephone numbers, bumper
sticker or t-shirt slogans.
32. Fear of saying certain things Fear of saying certain words (such as “thirteen”)
because of superstitions, fear of saying something tat
might be disrespectful to a dead person, fear of using
words with an apostrophe (because this denotes
possession).
33. Fear of not saying just the right Fear of having said the wrong thing, fear of not using
thing the “perfect” word.
34. Fear of losing things Worries about losing a wallet or other unimportant
objects, like a scrap of note paper.
35. Intrusive (non-violent) images Random unwanted images in your mind.
36. Intrusive nonsense sounds, Words, songs, or music in your mind that you can’t
words, or music. stop.
37. Bothered by certain Worries about the sounds of clocks ticking loudly or
sounds/noises * voices in another room that may interfere with
sleeping.
38. Lucky/unlucky numbers Worries about common numbers (like thirteen) that
may cause you to perform activities a certain number
of times or to postpone an action until a certain lucky
hour of the day.
39. Colors with special significance Fear of using objects of certain colors (e.g. black may
be associated with death, red with blood and injury).
40. Superstitious fears Fear of passing a cemetery, hearse, or black cat; fear
of omens associated with death.
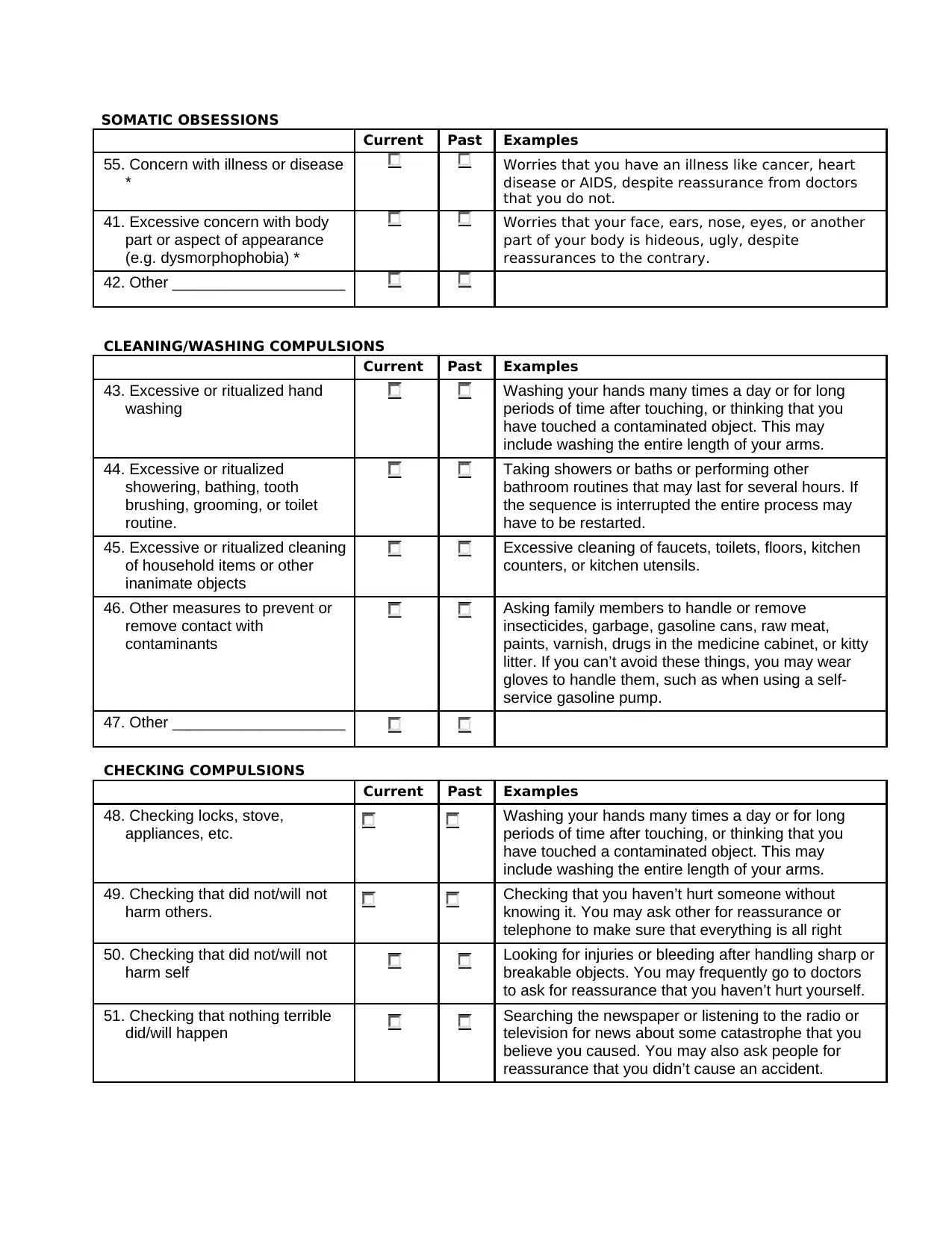
SOMATIC OBSESSIONS
Current Past Examples
55. Concern with illness or disease Worries that you have an illness like cancer, heart
* disease or AIDS, despite reassurance from doctors
that you do not.
41. Excessive concern with body Worries that your face, ears, nose, eyes, or another
part or aspect of appearance part of your body is hideous, ugly, despite
(e.g. dysmorphophobia) * reassurances to the contrary.
42. Other ____________________
CLEANING/WASHING COMPULSIONS
Current Past Examples
43. Excessive or ritualized hand Washing your hands many times a day or for long
washing periods of time after touching, or thinking that you
have touched a contaminated object. This may
include washing the entire length of your arms.
44. Excessive or ritualized Taking showers or baths or performing other
showering, bathing, tooth bathroom routines that may last for several hours. If
brushing, grooming, or toilet the sequence is interrupted the entire process may
routine. have to be restarted.
45. Excessive or ritualized cleaning Excessive cleaning of faucets, toilets, floors, kitchen
of household items or other counters, or kitchen utensils.
inanimate objects
46. Other measures to prevent or Asking family members to handle or remove
remove contact with insecticides, garbage, gasoline cans, raw meat,
contaminants paints, varnish, drugs in the medicine cabinet, or kitty
litter. If you can’t avoid these things, you may wear
gloves to handle them, such as when using a self-
service gasoline pump.
47. Other ____________________
CHECKING COMPULSIONS
Current Past Examples
48. Checking locks, stove, Washing your hands many times a day or for long
appliances, etc. periods of time after touching, or thinking that you
have touched a contaminated object. This may
include washing the entire length of your arms.
49. Checking that did not/will not Checking that you haven’t hurt someone without
harm others. knowing it. You may ask other for reassurance or
telephone to make sure that everything is all right
50. Checking that did not/will not Looking for injuries or bleeding after handling sharp or
harm self breakable objects. You may frequently go to doctors
to ask for reassurance that you haven’t hurt yourself.
51. Checking that nothing terrible Searching the newspaper or listening to the radio or
did/will happen television for news about some catastrophe that you
believe you caused. You may also ask people for
reassurance that you didn’t cause an accident.
Current Past Examples
55. Concern with illness or disease Worries that you have an illness like cancer, heart
* disease or AIDS, despite reassurance from doctors
that you do not.
41. Excessive concern with body Worries that your face, ears, nose, eyes, or another
part or aspect of appearance part of your body is hideous, ugly, despite
(e.g. dysmorphophobia) * reassurances to the contrary.
42. Other ____________________
CLEANING/WASHING COMPULSIONS
Current Past Examples
43. Excessive or ritualized hand Washing your hands many times a day or for long
washing periods of time after touching, or thinking that you
have touched a contaminated object. This may
include washing the entire length of your arms.
44. Excessive or ritualized Taking showers or baths or performing other
showering, bathing, tooth bathroom routines that may last for several hours. If
brushing, grooming, or toilet the sequence is interrupted the entire process may
routine. have to be restarted.
45. Excessive or ritualized cleaning Excessive cleaning of faucets, toilets, floors, kitchen
of household items or other counters, or kitchen utensils.
inanimate objects
46. Other measures to prevent or Asking family members to handle or remove
remove contact with insecticides, garbage, gasoline cans, raw meat,
contaminants paints, varnish, drugs in the medicine cabinet, or kitty
litter. If you can’t avoid these things, you may wear
gloves to handle them, such as when using a self-
service gasoline pump.
47. Other ____________________
CHECKING COMPULSIONS
Current Past Examples
48. Checking locks, stove, Washing your hands many times a day or for long
appliances, etc. periods of time after touching, or thinking that you
have touched a contaminated object. This may
include washing the entire length of your arms.
49. Checking that did not/will not Checking that you haven’t hurt someone without
harm others. knowing it. You may ask other for reassurance or
telephone to make sure that everything is all right
50. Checking that did not/will not Looking for injuries or bleeding after handling sharp or
harm self breakable objects. You may frequently go to doctors
to ask for reassurance that you haven’t hurt yourself.
51. Checking that nothing terrible Searching the newspaper or listening to the radio or
did/will happen television for news about some catastrophe that you
believe you caused. You may also ask people for
reassurance that you didn’t cause an accident.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
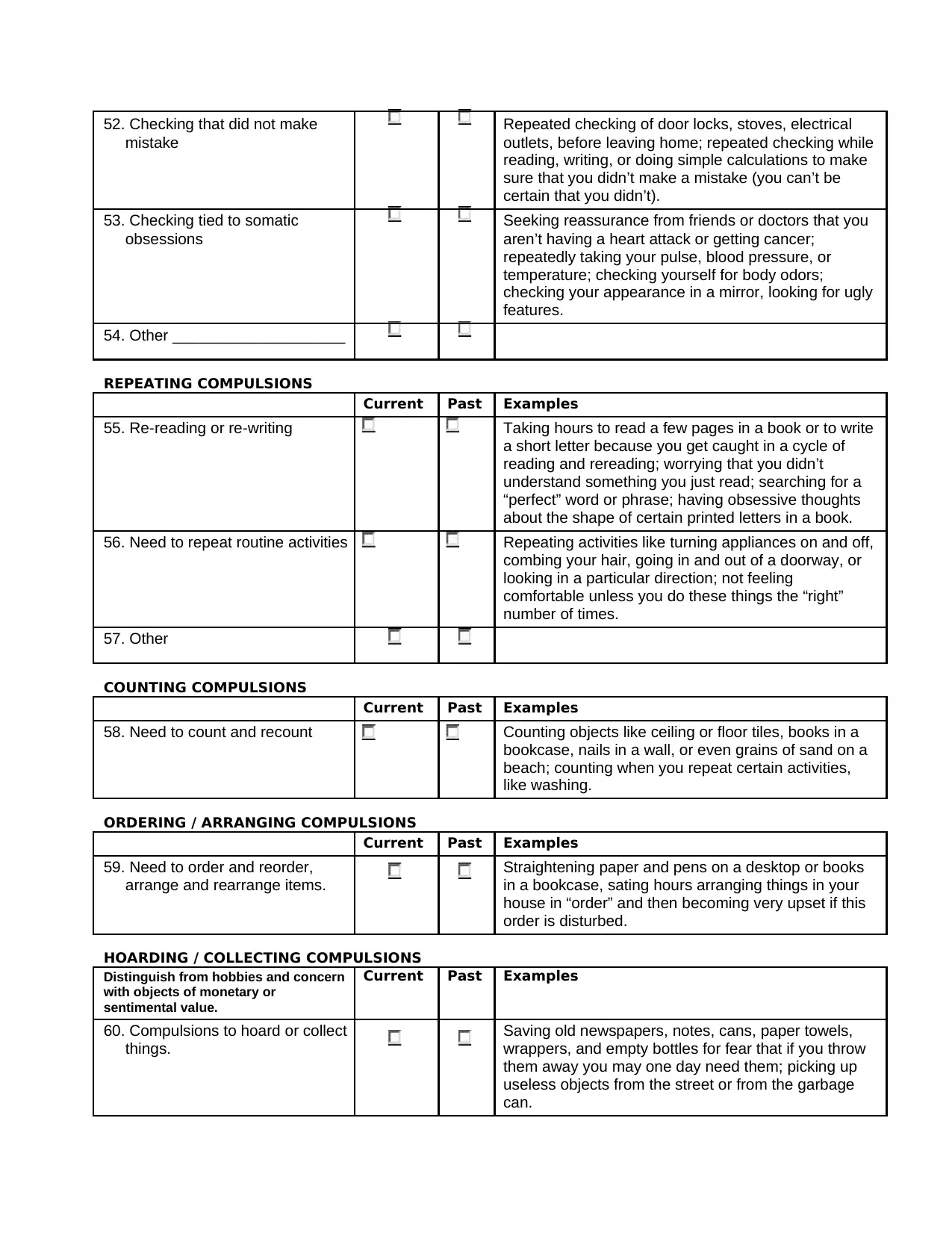
52. Checking that did not make Repeated checking of door locks, stoves, electrical
mistake outlets, before leaving home; repeated checking while
reading, writing, or doing simple calculations to make
sure that you didn’t make a mistake (you can’t be
certain that you didn’t).
53. Checking tied to somatic Seeking reassurance from friends or doctors that you
obsessions aren’t having a heart attack or getting cancer;
repeatedly taking your pulse, blood pressure, or
temperature; checking yourself for body odors;
checking your appearance in a mirror, looking for ugly
features.
54. Other ____________________
REPEATING COMPULSIONS
Current Past Examples
55. Re-reading or re-writing Taking hours to read a few pages in a book or to write
a short letter because you get caught in a cycle of
reading and rereading; worrying that you didn’t
understand something you just read; searching for a
“perfect” word or phrase; having obsessive thoughts
about the shape of certain printed letters in a book.
56. Need to repeat routine activities Repeating activities like turning appliances on and off,
combing your hair, going in and out of a doorway, or
looking in a particular direction; not feeling
comfortable unless you do these things the “right”
number of times.
57. Other
COUNTING COMPULSIONS
Current Past Examples
58. Need to count and recount Counting objects like ceiling or floor tiles, books in a
bookcase, nails in a wall, or even grains of sand on a
beach; counting when you repeat certain activities,
like washing.
ORDERING / ARRANGING COMPULSIONS
Current Past Examples
59. Need to order and reorder, Straightening paper and pens on a desktop or books
arrange and rearrange items. in a bookcase, sating hours arranging things in your
house in “order” and then becoming very upset if this
order is disturbed.
HOARDING / COLLECTING COMPULSIONS
Distinguish from hobbies and concern Current Past Examples
with objects of monetary or
sentimental value.
60. Compulsions to hoard or collect Saving old newspapers, notes, cans, paper towels,
things. wrappers, and empty bottles for fear that if you throw
them away you may one day need them; picking up
useless objects from the street or from the garbage
can.
mistake outlets, before leaving home; repeated checking while
reading, writing, or doing simple calculations to make
sure that you didn’t make a mistake (you can’t be
certain that you didn’t).
53. Checking tied to somatic Seeking reassurance from friends or doctors that you
obsessions aren’t having a heart attack or getting cancer;
repeatedly taking your pulse, blood pressure, or
temperature; checking yourself for body odors;
checking your appearance in a mirror, looking for ugly
features.
54. Other ____________________
REPEATING COMPULSIONS
Current Past Examples
55. Re-reading or re-writing Taking hours to read a few pages in a book or to write
a short letter because you get caught in a cycle of
reading and rereading; worrying that you didn’t
understand something you just read; searching for a
“perfect” word or phrase; having obsessive thoughts
about the shape of certain printed letters in a book.
56. Need to repeat routine activities Repeating activities like turning appliances on and off,
combing your hair, going in and out of a doorway, or
looking in a particular direction; not feeling
comfortable unless you do these things the “right”
number of times.
57. Other
COUNTING COMPULSIONS
Current Past Examples
58. Need to count and recount Counting objects like ceiling or floor tiles, books in a
bookcase, nails in a wall, or even grains of sand on a
beach; counting when you repeat certain activities,
like washing.
ORDERING / ARRANGING COMPULSIONS
Current Past Examples
59. Need to order and reorder, Straightening paper and pens on a desktop or books
arrange and rearrange items. in a bookcase, sating hours arranging things in your
house in “order” and then becoming very upset if this
order is disturbed.
HOARDING / COLLECTING COMPULSIONS
Distinguish from hobbies and concern Current Past Examples
with objects of monetary or
sentimental value.
60. Compulsions to hoard or collect Saving old newspapers, notes, cans, paper towels,
things. wrappers, and empty bottles for fear that if you throw
them away you may one day need them; picking up
useless objects from the street or from the garbage
can.
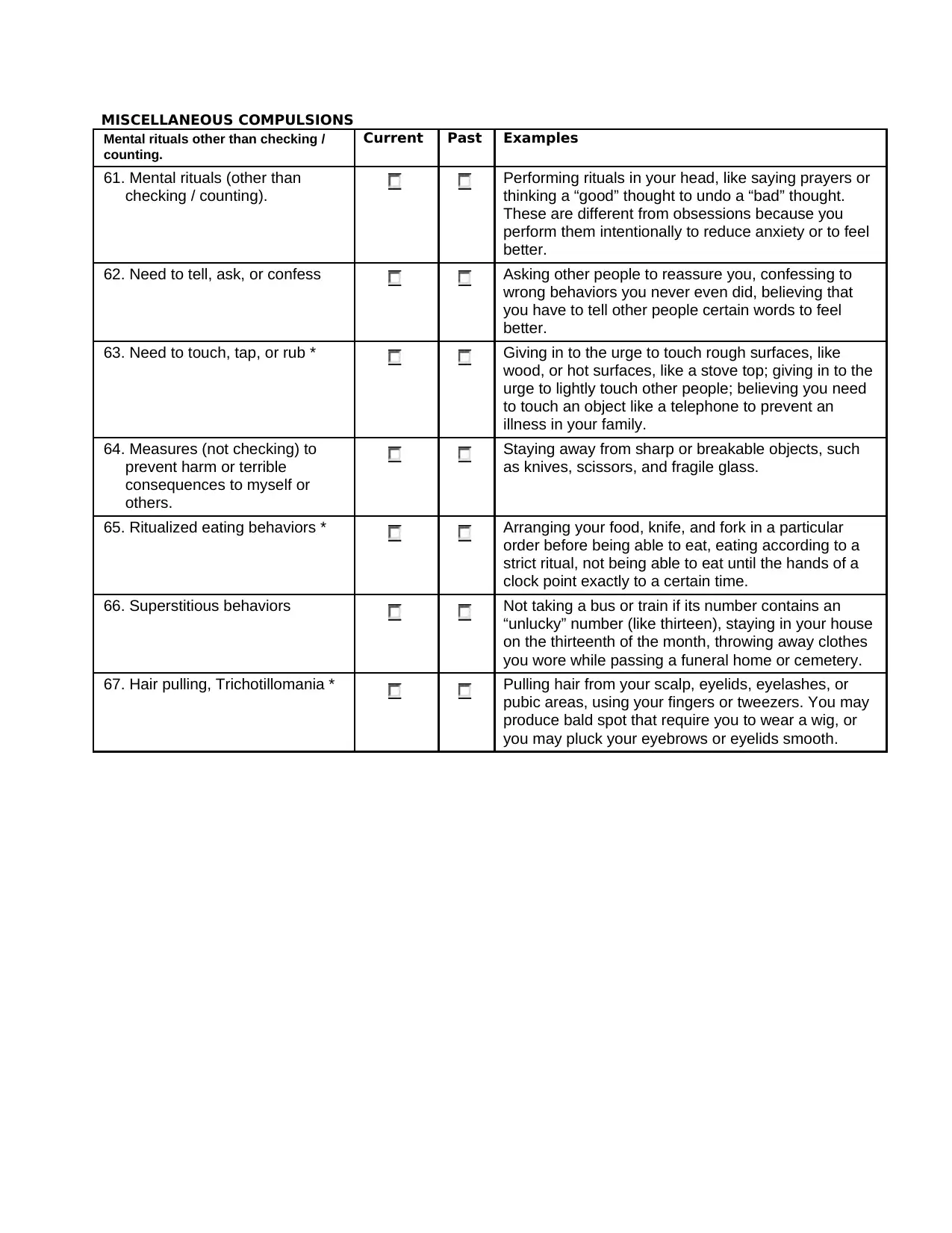
MISCELLANEOUS COMPULSIONS
Mental rituals other than checking / Current Past Examples
counting.
61. Mental rituals (other than Performing rituals in your head, like saying prayers or
checking / counting). thinking a “good” thought to undo a “bad” thought.
These are different from obsessions because you
perform them intentionally to reduce anxiety or to feel
better.
62. Need to tell, ask, or confess Asking other people to reassure you, confessing to
wrong behaviors you never even did, believing that
you have to tell other people certain words to feel
better.
63. Need to touch, tap, or rub * Giving in to the urge to touch rough surfaces, like
wood, or hot surfaces, like a stove top; giving in to the
urge to lightly touch other people; believing you need
to touch an object like a telephone to prevent an
illness in your family.
64. Measures (not checking) to Staying away from sharp or breakable objects, such
prevent harm or terrible as knives, scissors, and fragile glass.
consequences to myself or
others.
65. Ritualized eating behaviors * Arranging your food, knife, and fork in a particular
order before being able to eat, eating according to a
strict ritual, not being able to eat until the hands of a
clock point exactly to a certain time.
66. Superstitious behaviors Not taking a bus or train if its number contains an
“unlucky” number (like thirteen), staying in your house
on the thirteenth of the month, throwing away clothes
you wore while passing a funeral home or cemetery.
67. Hair pulling, Trichotillomania * Pulling hair from your scalp, eyelids, eyelashes, or
pubic areas, using your fingers or tweezers. You may
produce bald spot that require you to wear a wig, or
you may pluck your eyebrows or eyelids smooth.
Mental rituals other than checking / Current Past Examples
counting.
61. Mental rituals (other than Performing rituals in your head, like saying prayers or
checking / counting). thinking a “good” thought to undo a “bad” thought.
These are different from obsessions because you
perform them intentionally to reduce anxiety or to feel
better.
62. Need to tell, ask, or confess Asking other people to reassure you, confessing to
wrong behaviors you never even did, believing that
you have to tell other people certain words to feel
better.
63. Need to touch, tap, or rub * Giving in to the urge to touch rough surfaces, like
wood, or hot surfaces, like a stove top; giving in to the
urge to lightly touch other people; believing you need
to touch an object like a telephone to prevent an
illness in your family.
64. Measures (not checking) to Staying away from sharp or breakable objects, such
prevent harm or terrible as knives, scissors, and fragile glass.
consequences to myself or
others.
65. Ritualized eating behaviors * Arranging your food, knife, and fork in a particular
order before being able to eat, eating according to a
strict ritual, not being able to eat until the hands of a
clock point exactly to a certain time.
66. Superstitious behaviors Not taking a bus or train if its number contains an
“unlucky” number (like thirteen), staying in your house
on the thirteenth of the month, throwing away clothes
you wore while passing a funeral home or cemetery.
67. Hair pulling, Trichotillomania * Pulling hair from your scalp, eyelids, eyelashes, or
pubic areas, using your fingers or tweezers. You may
produce bald spot that require you to wear a wig, or
you may pluck your eyebrows or eyelids smooth.
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
TARGET SYMPTOM LIST
Obsessions:
1.
2.
3.
COMPULSIONS:
1.
2.
3.
AVOIDANCE:
1.
2.
3.
WWW.CNSFORUM.COM 10
TARGET SYMPTOM LIST
Obsessions:
1.
2.
3.
COMPULSIONS:
1.
2.
3.
AVOIDANCE:
1.
2.
3.
WWW.CNSFORUM.COM 10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
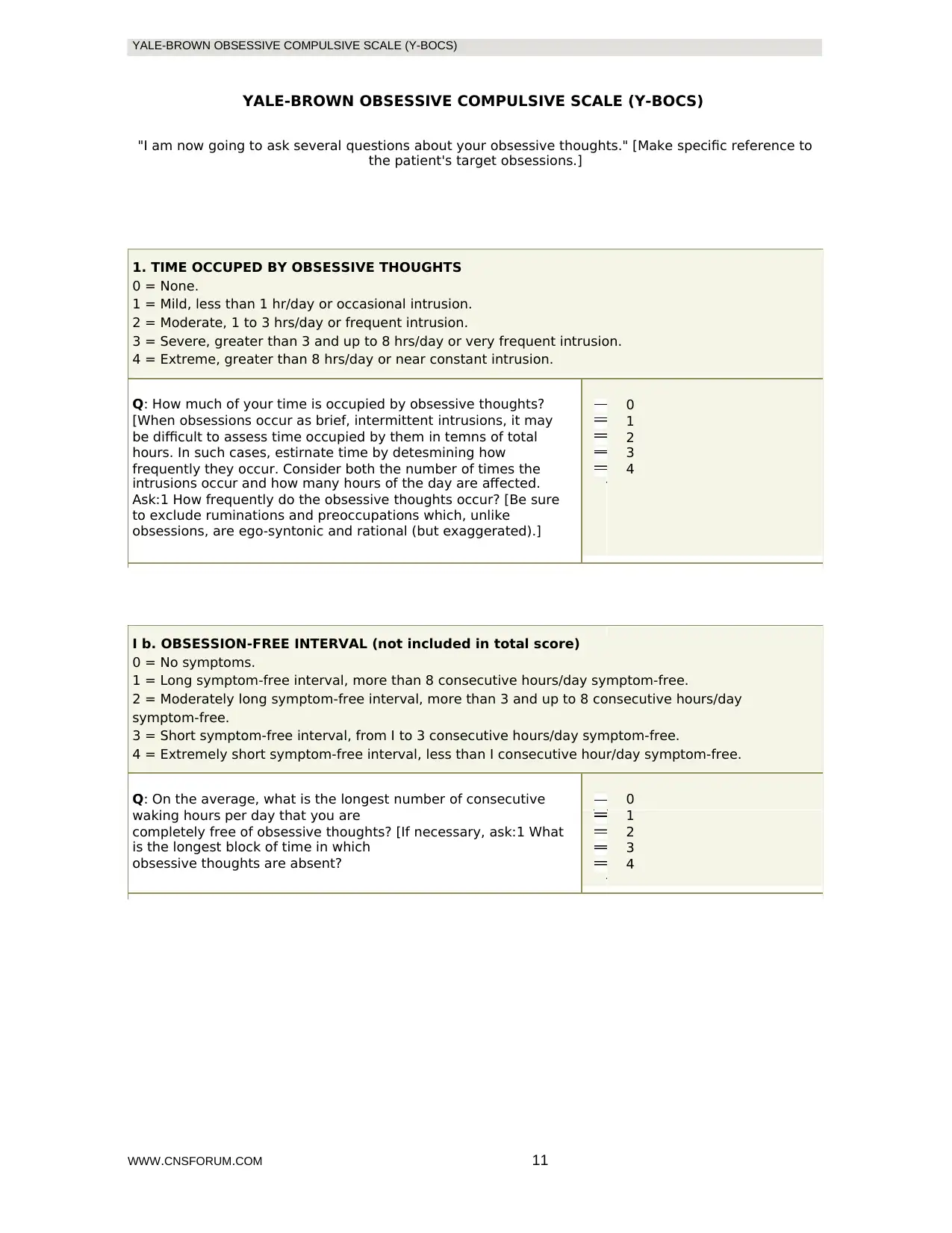
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
"I am now going to ask several questions about your obsessive thoughts." [Make specific reference to
the patient's target obsessions.]
1. TIME OCCUPED BY OBSESSIVE THOUGHTS
0 = None.
1 = Mild, less than 1 hr/day or occasional intrusion.
2 = Moderate, 1 to 3 hrs/day or frequent intrusion.
3 = Severe, greater than 3 and up to 8 hrs/day or very frequent intrusion.
4 = Extreme, greater than 8 hrs/day or near constant intrusion.
Q: How much of your time is occupied by obsessive thoughts? 0
[When obsessions occur as brief, intermittent intrusions, it may 1
be difficult to assess time occupied by them in temns of total 2
hours. In such cases, estirnate time by detesmining how 3
frequently they occur. Consider both the number of times the 4
intrusions occur and how many hours of the day are affected.
Ask:1 How frequently do the obsessive thoughts occur? [Be sure
to exclude ruminations and preoccupations which, unlike
obsessions, are ego-syntonic and rational (but exaggerated).]
I b. OBSESSION-FREE INTERVAL (not included in total score)
0 = No symptoms.
1 = Long symptom-free interval, more than 8 consecutive hours/day symptom-free.
2 = Moderately long symptom-free interval, more than 3 and up to 8 consecutive hours/day
symptom-free.
3 = Short symptom-free interval, from I to 3 consecutive hours/day symptom-free.
4 = Extremely short symptom-free interval, less than I consecutive hour/day symptom-free.
Q: On the average, what is the longest number of consecutive 0
waking hours per day that you are 1
completely free of obsessive thoughts? [If necessary, ask:1 What 2
is the longest block of time in which 3
obsessive thoughts are absent? 4
WWW.CNSFORUM.COM 11
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
"I am now going to ask several questions about your obsessive thoughts." [Make specific reference to
the patient's target obsessions.]
1. TIME OCCUPED BY OBSESSIVE THOUGHTS
0 = None.
1 = Mild, less than 1 hr/day or occasional intrusion.
2 = Moderate, 1 to 3 hrs/day or frequent intrusion.
3 = Severe, greater than 3 and up to 8 hrs/day or very frequent intrusion.
4 = Extreme, greater than 8 hrs/day or near constant intrusion.
Q: How much of your time is occupied by obsessive thoughts? 0
[When obsessions occur as brief, intermittent intrusions, it may 1
be difficult to assess time occupied by them in temns of total 2
hours. In such cases, estirnate time by detesmining how 3
frequently they occur. Consider both the number of times the 4
intrusions occur and how many hours of the day are affected.
Ask:1 How frequently do the obsessive thoughts occur? [Be sure
to exclude ruminations and preoccupations which, unlike
obsessions, are ego-syntonic and rational (but exaggerated).]
I b. OBSESSION-FREE INTERVAL (not included in total score)
0 = No symptoms.
1 = Long symptom-free interval, more than 8 consecutive hours/day symptom-free.
2 = Moderately long symptom-free interval, more than 3 and up to 8 consecutive hours/day
symptom-free.
3 = Short symptom-free interval, from I to 3 consecutive hours/day symptom-free.
4 = Extremely short symptom-free interval, less than I consecutive hour/day symptom-free.
Q: On the average, what is the longest number of consecutive 0
waking hours per day that you are 1
completely free of obsessive thoughts? [If necessary, ask:1 What 2
is the longest block of time in which 3
obsessive thoughts are absent? 4
WWW.CNSFORUM.COM 11
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
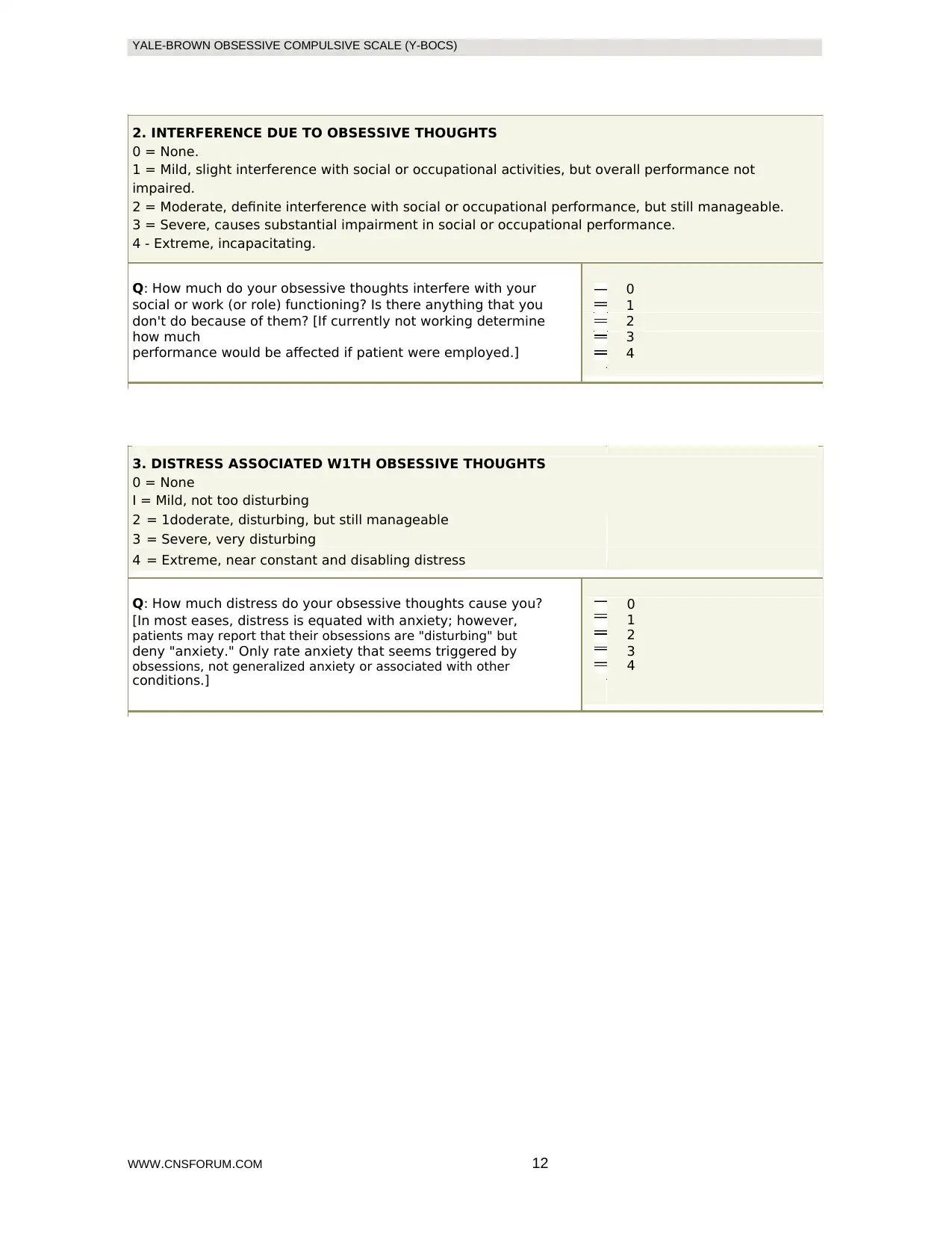
2. INTERFERENCE DUE TO OBSESSIVE THOUGHTS
0 = None.
1 = Mild, slight interference with social or occupational activities, but overall performance not
impaired.
2 = Moderate, definite interference with social or occupational performance, but still manageable.
3 = Severe, causes substantial impairment in social or occupational performance.
4 - Extreme, incapacitating.
Q: How much do your obsessive thoughts interfere with your 0
social or work (or role) functioning? Is there anything that you 1
don't do because of them? [If currently not working determine 2
how much 3
performance would be affected if patient were employed.] 4
3. DISTRESS ASSOCIATED W1TH OBSESSIVE THOUGHTS
0 = None
I = Mild, not too disturbing
2 = 1doderate, disturbing, but still manageable
3 = Severe, very disturbing
4 = Extreme, near constant and disabling distress
Q: How much distress do your obsessive thoughts cause you? 0
[In most eases, distress is equated with anxiety; however, 1
patients may report that their obsessions are "disturbing" but 2
deny "anxiety." Only rate anxiety that seems triggered by 3
obsessions, not generalized anxiety or associated with other 4
conditions.]
WWW.CNSFORUM.COM 12
2. INTERFERENCE DUE TO OBSESSIVE THOUGHTS
0 = None.
1 = Mild, slight interference with social or occupational activities, but overall performance not
impaired.
2 = Moderate, definite interference with social or occupational performance, but still manageable.
3 = Severe, causes substantial impairment in social or occupational performance.
4 - Extreme, incapacitating.
Q: How much do your obsessive thoughts interfere with your 0
social or work (or role) functioning? Is there anything that you 1
don't do because of them? [If currently not working determine 2
how much 3
performance would be affected if patient were employed.] 4
3. DISTRESS ASSOCIATED W1TH OBSESSIVE THOUGHTS
0 = None
I = Mild, not too disturbing
2 = 1doderate, disturbing, but still manageable
3 = Severe, very disturbing
4 = Extreme, near constant and disabling distress
Q: How much distress do your obsessive thoughts cause you? 0
[In most eases, distress is equated with anxiety; however, 1
patients may report that their obsessions are "disturbing" but 2
deny "anxiety." Only rate anxiety that seems triggered by 3
obsessions, not generalized anxiety or associated with other 4
conditions.]
WWW.CNSFORUM.COM 12
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
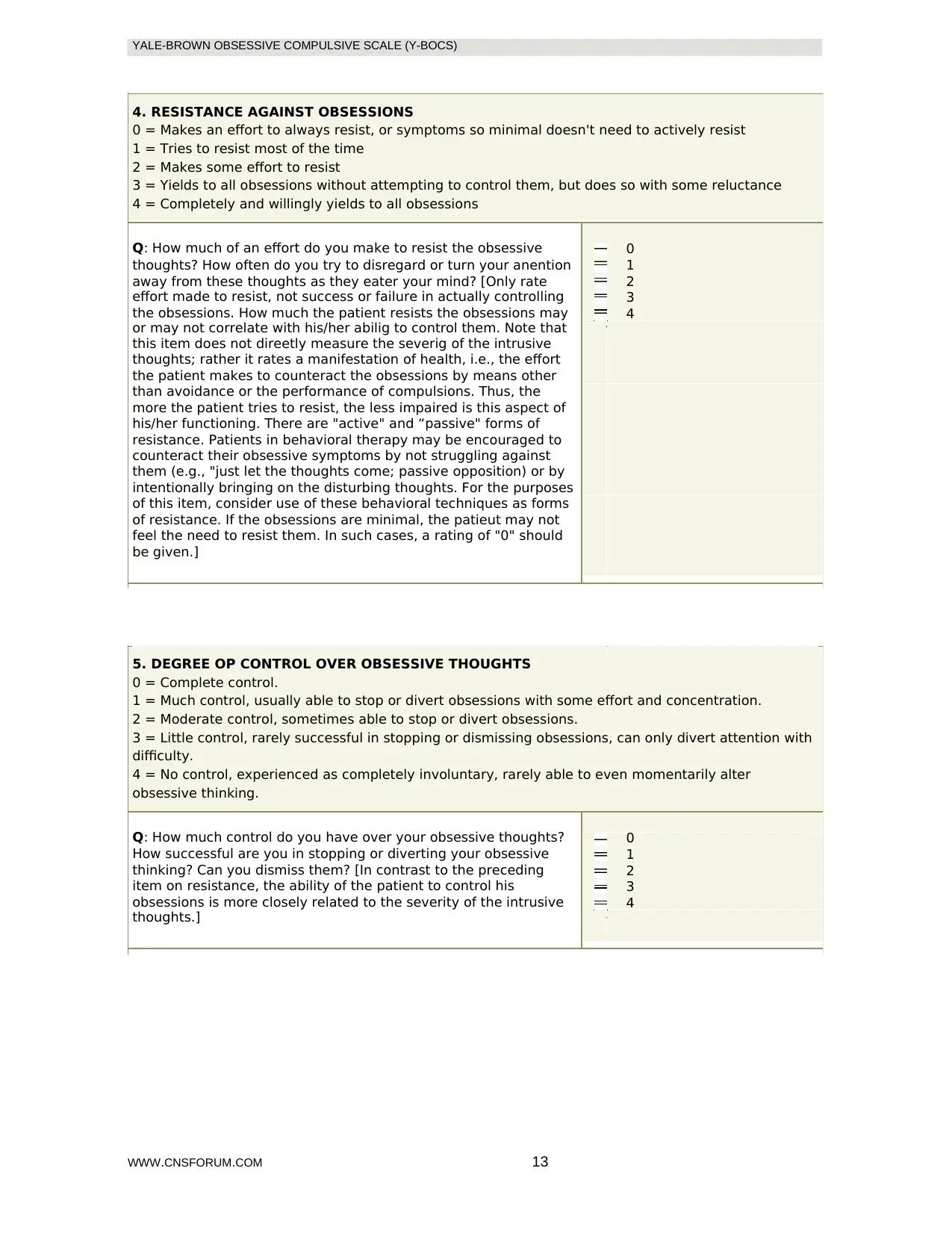
4. RESISTANCE AGAINST OBSESSIONS
0 = Makes an effort to always resist, or symptoms so minimal doesn't need to actively resist
1 = Tries to resist most of the time
2 = Makes some effort to resist
3 = Yields to all obsessions without attempting to control them, but does so with some reluctance
4 = Completely and willingly yields to all obsessions
Q: How much of an effort do you make to resist the obsessive 0
thoughts? How often do you try to disregard or turn your anention 1
away from these thoughts as they eater your mind? [Only rate 2
effort made to resist, not success or failure in actually controlling 3
the obsessions. How much the patient resists the obsessions may 4
or may not correlate with his/her abilig to control them. Note that
this item does not direetly measure the severig of the intrusive
thoughts; rather it rates a manifestation of health, i.e., the effort
the patient makes to counteract the obsessions by means other
than avoidance or the performance of compulsions. Thus, the
more the patient tries to resist, the less impaired is this aspect of
his/her functioning. There are "active" and “passive" forms of
resistance. Patients in behavioral therapy may be encouraged to
counteract their obsessive symptoms by not struggling against
them (e.g., "just let the thoughts come; passive opposition) or by
intentionally bringing on the disturbing thoughts. For the purposes
of this item, consider use of these behavioral techniques as forms
of resistance. If the obsessions are minimal, the patieut may not
feel the need to resist them. In such cases, a rating of "0" should
be given.]
5. DEGREE OP CONTROL OVER OBSESSIVE THOUGHTS
0 = Complete control.
1 = Much control, usually able to stop or divert obsessions with some effort and concentration.
2 = Moderate control, sometimes able to stop or divert obsessions.
3 = Little control, rarely successful in stopping or dismissing obsessions, can only divert attention with
difficulty.
4 = No control, experienced as completely involuntary, rarely able to even momentarily alter
obsessive thinking.
Q: How much control do you have over your obsessive thoughts? 0
How successful are you in stopping or diverting your obsessive 1
thinking? Can you dismiss them? [In contrast to the preceding 2
item on resistance, the ability of the patient to control his 3
obsessions is more closely related to the severity of the intrusive 4
thoughts.]
WWW.CNSFORUM.COM 13
4. RESISTANCE AGAINST OBSESSIONS
0 = Makes an effort to always resist, or symptoms so minimal doesn't need to actively resist
1 = Tries to resist most of the time
2 = Makes some effort to resist
3 = Yields to all obsessions without attempting to control them, but does so with some reluctance
4 = Completely and willingly yields to all obsessions
Q: How much of an effort do you make to resist the obsessive 0
thoughts? How often do you try to disregard or turn your anention 1
away from these thoughts as they eater your mind? [Only rate 2
effort made to resist, not success or failure in actually controlling 3
the obsessions. How much the patient resists the obsessions may 4
or may not correlate with his/her abilig to control them. Note that
this item does not direetly measure the severig of the intrusive
thoughts; rather it rates a manifestation of health, i.e., the effort
the patient makes to counteract the obsessions by means other
than avoidance or the performance of compulsions. Thus, the
more the patient tries to resist, the less impaired is this aspect of
his/her functioning. There are "active" and “passive" forms of
resistance. Patients in behavioral therapy may be encouraged to
counteract their obsessive symptoms by not struggling against
them (e.g., "just let the thoughts come; passive opposition) or by
intentionally bringing on the disturbing thoughts. For the purposes
of this item, consider use of these behavioral techniques as forms
of resistance. If the obsessions are minimal, the patieut may not
feel the need to resist them. In such cases, a rating of "0" should
be given.]
5. DEGREE OP CONTROL OVER OBSESSIVE THOUGHTS
0 = Complete control.
1 = Much control, usually able to stop or divert obsessions with some effort and concentration.
2 = Moderate control, sometimes able to stop or divert obsessions.
3 = Little control, rarely successful in stopping or dismissing obsessions, can only divert attention with
difficulty.
4 = No control, experienced as completely involuntary, rarely able to even momentarily alter
obsessive thinking.
Q: How much control do you have over your obsessive thoughts? 0
How successful are you in stopping or diverting your obsessive 1
thinking? Can you dismiss them? [In contrast to the preceding 2
item on resistance, the ability of the patient to control his 3
obsessions is more closely related to the severity of the intrusive 4
thoughts.]
WWW.CNSFORUM.COM 13
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
"The next several questions are about your compulsive behaviors." [Make
specific reference to the patient's target compulsions.]
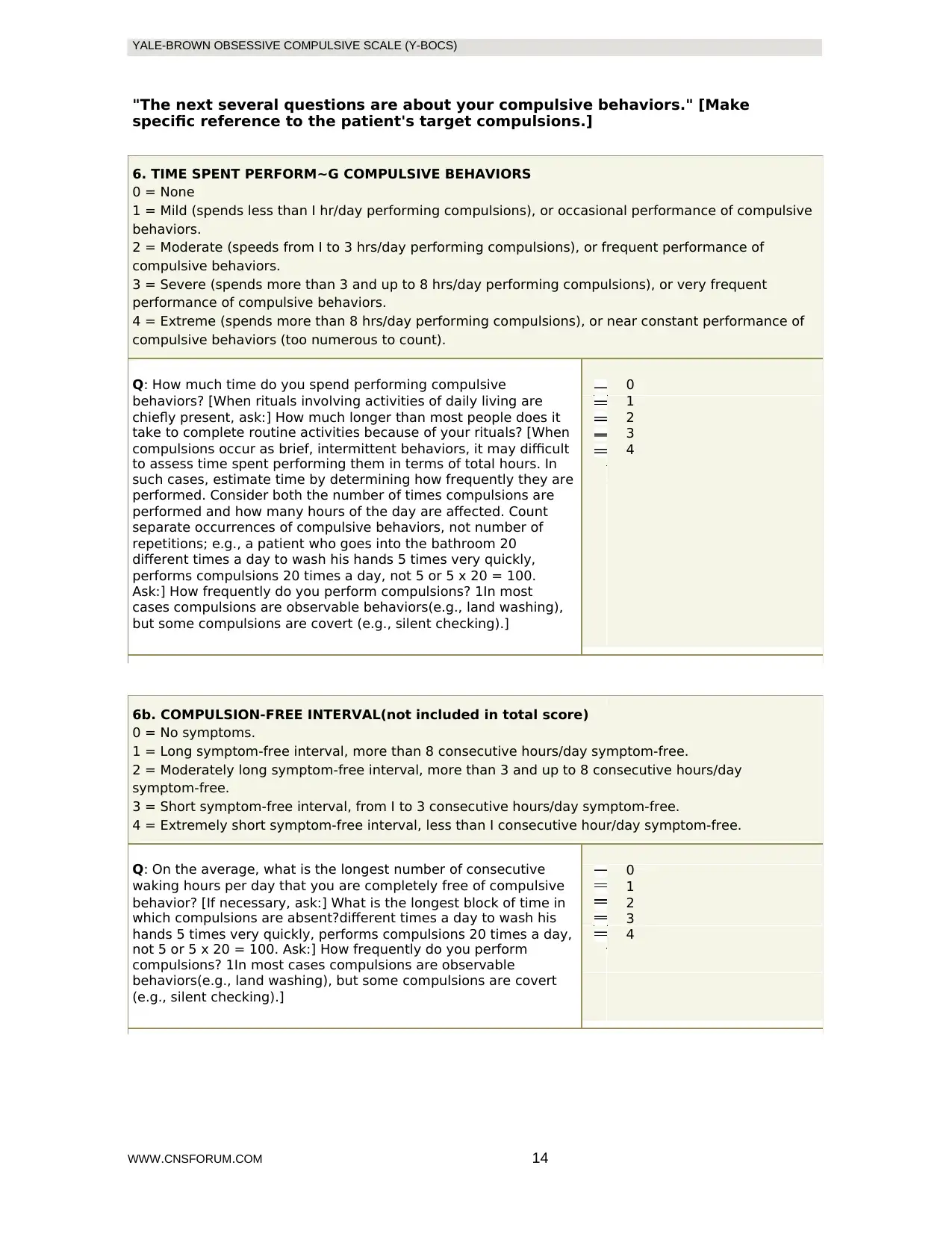
6. TIME SPENT PERFORM~G COMPULSIVE BEHAVIORS
0 = None
1 = Mild (spends less than I hr/day performing compulsions), or occasional performance of compulsive
behaviors.
2 = Moderate (speeds from I to 3 hrs/day performing compulsions), or frequent performance of
compulsive behaviors.
3 = Severe (spends more than 3 and up to 8 hrs/day performing compulsions), or very frequent
performance of compulsive behaviors.
4 = Extreme (spends more than 8 hrs/day performing compulsions), or near constant performance of
compulsive behaviors (too numerous to count).
Q: How much time do you spend performing compulsive 0
behaviors? [When rituals involving activities of daily living are 1
chiefly present, ask:] How much longer than most people does it 2
take to complete routine activities because of your rituals? [When 3
compulsions occur as brief, intermittent behaviors, it may difficult 4
to assess time spent performing them in terms of total hours. In
such cases, estimate time by determining how frequently they are
performed. Consider both the number of times compulsions are
performed and how many hours of the day are affected. Count
separate occurrences of compulsive behaviors, not number of
repetitions; e.g., a patient who goes into the bathroom 20
different times a day to wash his hands 5 times very quickly,
performs compulsions 20 times a day, not 5 or 5 x 20 = 100.
Ask:] How frequently do you perform compulsions? 1In most
cases compulsions are observable behaviors(e.g., land washing),
but some compulsions are covert (e.g., silent checking).]
6b. COMPULSION-FREE INTERVAL(not included in total score)
0 = No symptoms.
1 = Long symptom-free interval, more than 8 consecutive hours/day symptom-free.
2 = Moderately long symptom-free interval, more than 3 and up to 8 consecutive hours/day
symptom-free.
3 = Short symptom-free interval, from I to 3 consecutive hours/day symptom-free.
4 = Extremely short symptom-free interval, less than I consecutive hour/day symptom-free.
Q: On the average, what is the longest number of consecutive 0
waking hours per day that you are completely free of compulsive 1
behavior? [If necessary, ask:] What is the longest block of time in 2
which compulsions are absent?different times a day to wash his 3
hands 5 times very quickly, performs compulsions 20 times a day, 4
not 5 or 5 x 20 = 100. Ask:] How frequently do you perform
compulsions? 1In most cases compulsions are observable
behaviors(e.g., land washing), but some compulsions are covert
(e.g., silent checking).]
WWW.CNSFORUM.COM 14
"The next several questions are about your compulsive behaviors." [Make
specific reference to the patient's target compulsions.]
6. TIME SPENT PERFORM~G COMPULSIVE BEHAVIORS
0 = None
1 = Mild (spends less than I hr/day performing compulsions), or occasional performance of compulsive
behaviors.
2 = Moderate (speeds from I to 3 hrs/day performing compulsions), or frequent performance of
compulsive behaviors.
3 = Severe (spends more than 3 and up to 8 hrs/day performing compulsions), or very frequent
performance of compulsive behaviors.
4 = Extreme (spends more than 8 hrs/day performing compulsions), or near constant performance of
compulsive behaviors (too numerous to count).
Q: How much time do you spend performing compulsive 0
behaviors? [When rituals involving activities of daily living are 1
chiefly present, ask:] How much longer than most people does it 2
take to complete routine activities because of your rituals? [When 3
compulsions occur as brief, intermittent behaviors, it may difficult 4
to assess time spent performing them in terms of total hours. In
such cases, estimate time by determining how frequently they are
performed. Consider both the number of times compulsions are
performed and how many hours of the day are affected. Count
separate occurrences of compulsive behaviors, not number of
repetitions; e.g., a patient who goes into the bathroom 20
different times a day to wash his hands 5 times very quickly,
performs compulsions 20 times a day, not 5 or 5 x 20 = 100.
Ask:] How frequently do you perform compulsions? 1In most
cases compulsions are observable behaviors(e.g., land washing),
but some compulsions are covert (e.g., silent checking).]
6b. COMPULSION-FREE INTERVAL(not included in total score)
0 = No symptoms.
1 = Long symptom-free interval, more than 8 consecutive hours/day symptom-free.
2 = Moderately long symptom-free interval, more than 3 and up to 8 consecutive hours/day
symptom-free.
3 = Short symptom-free interval, from I to 3 consecutive hours/day symptom-free.
4 = Extremely short symptom-free interval, less than I consecutive hour/day symptom-free.
Q: On the average, what is the longest number of consecutive 0
waking hours per day that you are completely free of compulsive 1
behavior? [If necessary, ask:] What is the longest block of time in 2
which compulsions are absent?different times a day to wash his 3
hands 5 times very quickly, performs compulsions 20 times a day, 4
not 5 or 5 x 20 = 100. Ask:] How frequently do you perform
compulsions? 1In most cases compulsions are observable
behaviors(e.g., land washing), but some compulsions are covert
(e.g., silent checking).]
WWW.CNSFORUM.COM 14
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
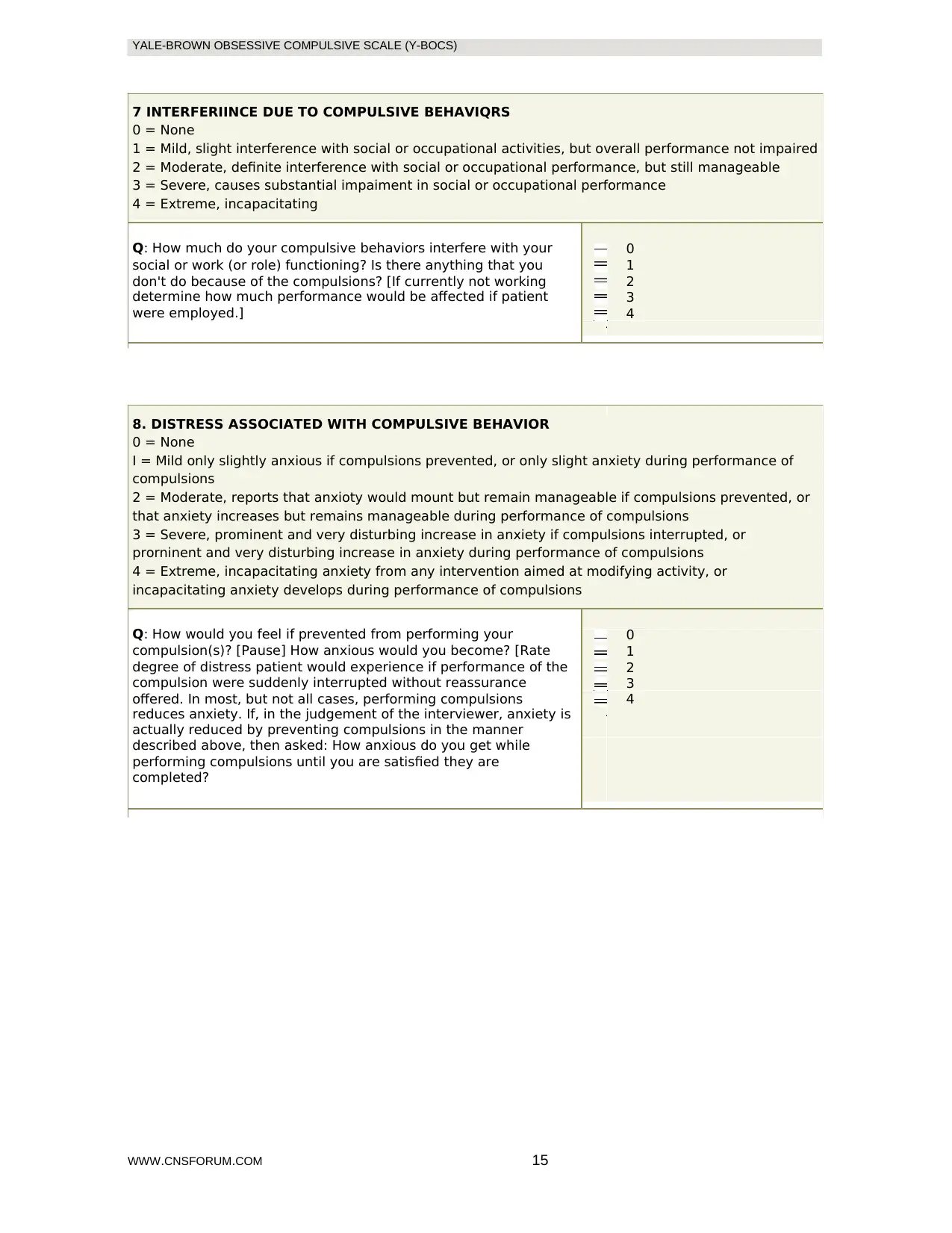
7 INTERFERIINCE DUE TO COMPULSIVE BEHAVIQRS
0 = None
1 = Mild, slight interference with social or occupational activities, but overall performance not impaired
2 = Moderate, definite interference with social or occupational performance, but still manageable
3 = Severe, causes substantial impaiment in social or occupational performance
4 = Extreme, incapacitating
Q: How much do your compulsive behaviors interfere with your 0
social or work (or role) functioning? Is there anything that you 1
don't do because of the compulsions? [If currently not working 2
determine how much performance would be affected if patient 3
were employed.] 4
8. DISTRESS ASSOCIATED WITH COMPULSIVE BEHAVIOR
0 = None
I = Mild only slightly anxious if compulsions prevented, or only slight anxiety during performance of
compulsions
2 = Moderate, reports that anxioty would mount but remain manageable if compulsions prevented, or
that anxiety increases but remains manageable during performance of compulsions
3 = Severe, prominent and very disturbing increase in anxiety if compulsions interrupted, or
prorninent and very disturbing increase in anxiety during performance of compulsions
4 = Extreme, incapacitating anxiety from any intervention aimed at modifying activity, or
incapacitating anxiety develops during performance of compulsions
Q: How would you feel if prevented from performing your 0
compulsion(s)? [Pause] How anxious would you become? [Rate 1
degree of distress patient would experience if performance of the 2
compulsion were suddenly interrupted without reassurance 3
offered. In most, but not all cases, performing compulsions 4
reduces anxiety. If, in the judgement of the interviewer, anxiety is
actually reduced by preventing compulsions in the manner
described above, then asked: How anxious do you get while
performing compulsions until you are satisfied they are
completed?
WWW.CNSFORUM.COM 15
7 INTERFERIINCE DUE TO COMPULSIVE BEHAVIQRS
0 = None
1 = Mild, slight interference with social or occupational activities, but overall performance not impaired
2 = Moderate, definite interference with social or occupational performance, but still manageable
3 = Severe, causes substantial impaiment in social or occupational performance
4 = Extreme, incapacitating
Q: How much do your compulsive behaviors interfere with your 0
social or work (or role) functioning? Is there anything that you 1
don't do because of the compulsions? [If currently not working 2
determine how much performance would be affected if patient 3
were employed.] 4
8. DISTRESS ASSOCIATED WITH COMPULSIVE BEHAVIOR
0 = None
I = Mild only slightly anxious if compulsions prevented, or only slight anxiety during performance of
compulsions
2 = Moderate, reports that anxioty would mount but remain manageable if compulsions prevented, or
that anxiety increases but remains manageable during performance of compulsions
3 = Severe, prominent and very disturbing increase in anxiety if compulsions interrupted, or
prorninent and very disturbing increase in anxiety during performance of compulsions
4 = Extreme, incapacitating anxiety from any intervention aimed at modifying activity, or
incapacitating anxiety develops during performance of compulsions
Q: How would you feel if prevented from performing your 0
compulsion(s)? [Pause] How anxious would you become? [Rate 1
degree of distress patient would experience if performance of the 2
compulsion were suddenly interrupted without reassurance 3
offered. In most, but not all cases, performing compulsions 4
reduces anxiety. If, in the judgement of the interviewer, anxiety is
actually reduced by preventing compulsions in the manner
described above, then asked: How anxious do you get while
performing compulsions until you are satisfied they are
completed?
WWW.CNSFORUM.COM 15
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
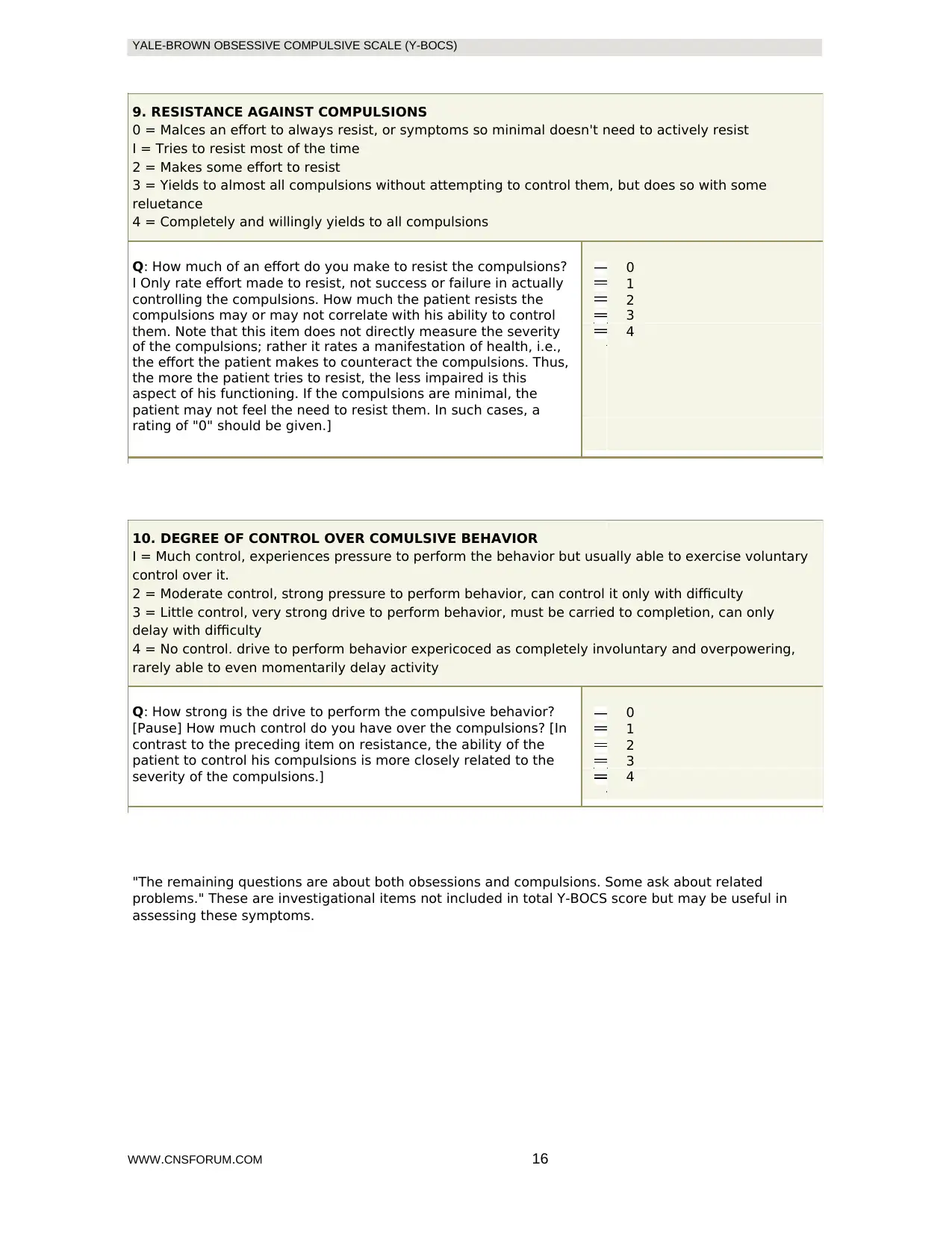
9. RESISTANCE AGAINST COMPULSIONS
0 = Malces an effort to always resist, or symptoms so minimal doesn't need to actively resist
I = Tries to resist most of the time
2 = Makes some effort to resist
3 = Yields to almost all compulsions without attempting to control them, but does so with some
reluetance
4 = Completely and willingly yields to all compulsions
Q: How much of an effort do you make to resist the compulsions? 0
I Only rate effort made to resist, not success or failure in actually 1
controlling the compulsions. How much the patient resists the 2
compulsions may or may not correlate with his ability to control 3
them. Note that this item does not directly measure the severity 4
of the compulsions; rather it rates a manifestation of health, i.e.,
the effort the patient makes to counteract the compulsions. Thus,
the more the patient tries to resist, the less impaired is this
aspect of his functioning. If the compulsions are minimal, the
patient may not feel the need to resist them. In such cases, a
rating of "0" should be given.]
10. DEGREE OF CONTROL OVER COMULSIVE BEHAVIOR
I = Much control, experiences pressure to perform the behavior but usually able to exercise voluntary
control over it.
2 = Moderate control, strong pressure to perform behavior, can control it only with difficulty
3 = Little control, very strong drive to perform behavior, must be carried to completion, can only
delay with difficulty
4 = No control. drive to perform behavior expericoced as completely involuntary and overpowering,
rarely able to even momentarily delay activity
Q: How strong is the drive to perform the compulsive behavior? 0
[Pause] How much control do you have over the compulsions? [In 1
contrast to the preceding item on resistance, the ability of the 2
patient to control his compulsions is more closely related to the 3
severity of the compulsions.] 4
"The remaining questions are about both obsessions and compulsions. Some ask about related
problems." These are investigational items not included in total Y-BOCS score but may be useful in
assessing these symptoms.
WWW.CNSFORUM.COM 16
9. RESISTANCE AGAINST COMPULSIONS
0 = Malces an effort to always resist, or symptoms so minimal doesn't need to actively resist
I = Tries to resist most of the time
2 = Makes some effort to resist
3 = Yields to almost all compulsions without attempting to control them, but does so with some
reluetance
4 = Completely and willingly yields to all compulsions
Q: How much of an effort do you make to resist the compulsions? 0
I Only rate effort made to resist, not success or failure in actually 1
controlling the compulsions. How much the patient resists the 2
compulsions may or may not correlate with his ability to control 3
them. Note that this item does not directly measure the severity 4
of the compulsions; rather it rates a manifestation of health, i.e.,
the effort the patient makes to counteract the compulsions. Thus,
the more the patient tries to resist, the less impaired is this
aspect of his functioning. If the compulsions are minimal, the
patient may not feel the need to resist them. In such cases, a
rating of "0" should be given.]
10. DEGREE OF CONTROL OVER COMULSIVE BEHAVIOR
I = Much control, experiences pressure to perform the behavior but usually able to exercise voluntary
control over it.
2 = Moderate control, strong pressure to perform behavior, can control it only with difficulty
3 = Little control, very strong drive to perform behavior, must be carried to completion, can only
delay with difficulty
4 = No control. drive to perform behavior expericoced as completely involuntary and overpowering,
rarely able to even momentarily delay activity
Q: How strong is the drive to perform the compulsive behavior? 0
[Pause] How much control do you have over the compulsions? [In 1
contrast to the preceding item on resistance, the ability of the 2
patient to control his compulsions is more closely related to the 3
severity of the compulsions.] 4
"The remaining questions are about both obsessions and compulsions. Some ask about related
problems." These are investigational items not included in total Y-BOCS score but may be useful in
assessing these symptoms.
WWW.CNSFORUM.COM 16
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
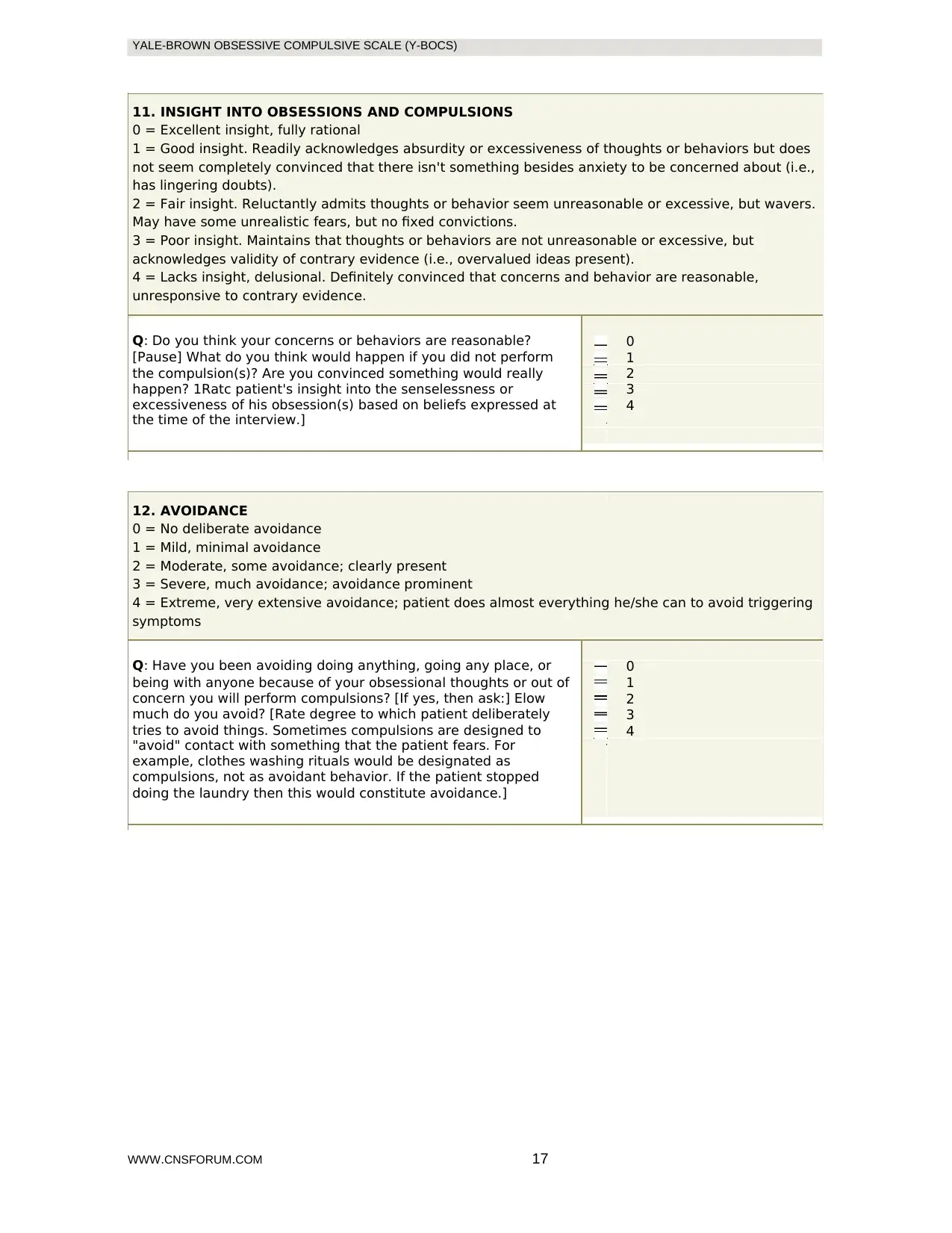
11. INSIGHT INTO OBSESSIONS AND COMPULSIONS
0 = Excellent insight, fully rational
1 = Good insight. Readily acknowledges absurdity or excessiveness of thoughts or behaviors but does
not seem completely convinced that there isn't something besides anxiety to be concerned about (i.e.,
has lingering doubts).
2 = Fair insight. Reluctantly admits thoughts or behavior seem unreasonable or excessive, but wavers.
May have some unrealistic fears, but no fixed convictions.
3 = Poor insight. Maintains that thoughts or behaviors are not unreasonable or excessive, but
acknowledges validity of contrary evidence (i.e., overvalued ideas present).
4 = Lacks insight, delusional. Definitely convinced that concerns and behavior are reasonable,
unresponsive to contrary evidence.
Q: Do you think your concerns or behaviors are reasonable? 0
[Pause] What do you think would happen if you did not perform 1
the compulsion(s)? Are you convinced something would really 2
happen? 1Ratc patient's insight into the senselessness or 3
excessiveness of his obsession(s) based on beliefs expressed at 4
the time of the interview.]
12. AVOIDANCE
0 = No deliberate avoidance
1 = Mild, minimal avoidance
2 = Moderate, some avoidance; clearly present
3 = Severe, much avoidance; avoidance prominent
4 = Extreme, very extensive avoidance; patient does almost everything he/she can to avoid triggering
symptoms
Q: Have you been avoiding doing anything, going any place, or 0
being with anyone because of your obsessional thoughts or out of 1
concern you will perform compulsions? [If yes, then ask:] Elow 2
much do you avoid? [Rate degree to which patient deliberately 3
tries to avoid things. Sometimes compulsions are designed to 4
"avoid" contact with something that the patient fears. For
example, clothes washing rituals would be designated as
compulsions, not as avoidant behavior. If the patient stopped
doing the laundry then this would constitute avoidance.]
WWW.CNSFORUM.COM 17
11. INSIGHT INTO OBSESSIONS AND COMPULSIONS
0 = Excellent insight, fully rational
1 = Good insight. Readily acknowledges absurdity or excessiveness of thoughts or behaviors but does
not seem completely convinced that there isn't something besides anxiety to be concerned about (i.e.,
has lingering doubts).
2 = Fair insight. Reluctantly admits thoughts or behavior seem unreasonable or excessive, but wavers.
May have some unrealistic fears, but no fixed convictions.
3 = Poor insight. Maintains that thoughts or behaviors are not unreasonable or excessive, but
acknowledges validity of contrary evidence (i.e., overvalued ideas present).
4 = Lacks insight, delusional. Definitely convinced that concerns and behavior are reasonable,
unresponsive to contrary evidence.
Q: Do you think your concerns or behaviors are reasonable? 0
[Pause] What do you think would happen if you did not perform 1
the compulsion(s)? Are you convinced something would really 2
happen? 1Ratc patient's insight into the senselessness or 3
excessiveness of his obsession(s) based on beliefs expressed at 4
the time of the interview.]
12. AVOIDANCE
0 = No deliberate avoidance
1 = Mild, minimal avoidance
2 = Moderate, some avoidance; clearly present
3 = Severe, much avoidance; avoidance prominent
4 = Extreme, very extensive avoidance; patient does almost everything he/she can to avoid triggering
symptoms
Q: Have you been avoiding doing anything, going any place, or 0
being with anyone because of your obsessional thoughts or out of 1
concern you will perform compulsions? [If yes, then ask:] Elow 2
much do you avoid? [Rate degree to which patient deliberately 3
tries to avoid things. Sometimes compulsions are designed to 4
"avoid" contact with something that the patient fears. For
example, clothes washing rituals would be designated as
compulsions, not as avoidant behavior. If the patient stopped
doing the laundry then this would constitute avoidance.]
WWW.CNSFORUM.COM 17
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
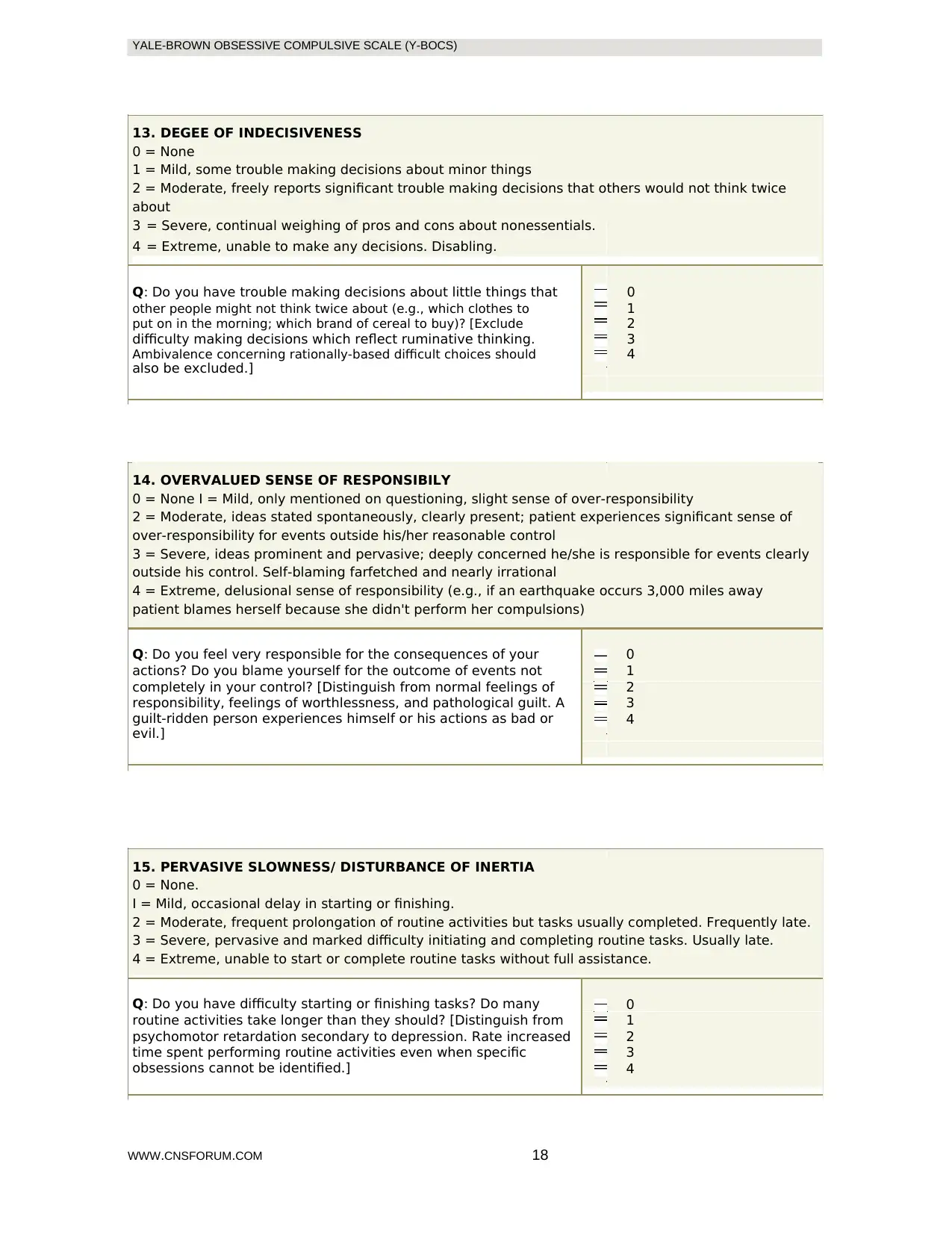
13. DEGEE OF INDECISIVENESS
0 = None
1 = Mild, some trouble making decisions about minor things
2 = Moderate, freely reports significant trouble making decisions that others would not think twice
about
3 = Severe, continual weighing of pros and cons about nonessentials.
4 = Extreme, unable to make any decisions. Disabling.
Q: Do you have trouble making decisions about little things that 0
other people might not think twice about (e.g., which clothes to 1
put on in the morning; which brand of cereal to buy)? [Exclude 2
difficulty making decisions which reflect ruminative thinking. 3
Ambivalence concerning rationally-based difficult choices should 4
also be excluded.]
14. OVERVALUED SENSE OF RESPONSIBILY
0 = None I = Mild, only mentioned on questioning, slight sense of over-responsibility
2 = Moderate, ideas stated spontaneously, clearly present; patient experiences significant sense of
over-responsibility for events outside his/her reasonable control
3 = Severe, ideas prominent and pervasive; deeply concerned he/she is responsible for events clearly
outside his control. Self-blaming farfetched and nearly irrational
4 = Extreme, delusional sense of responsibility (e.g., if an earthquake occurs 3,000 miles away
patient blames herself because she didn't perform her compulsions)
Q: Do you feel very responsible for the consequences of your 0
actions? Do you blame yourself for the outcome of events not 1
completely in your control? [Distinguish from normal feelings of 2
responsibility, feelings of worthlessness, and pathological guilt. A 3
guilt-ridden person experiences himself or his actions as bad or 4
evil.]
15. PERVASIVE SLOWNESS/ DISTURBANCE OF INERTIA
0 = None.
I = Mild, occasional delay in starting or finishing.
2 = Moderate, frequent prolongation of routine activities but tasks usually completed. Frequently late.
3 = Severe, pervasive and marked difficulty initiating and completing routine tasks. Usually late.
4 = Extreme, unable to start or complete routine tasks without full assistance.
Q: Do you have difficulty starting or finishing tasks? Do many 0
routine activities take longer than they should? [Distinguish from 1
psychomotor retardation secondary to depression. Rate increased 2
time spent performing routine activities even when specific 3
obsessions cannot be identified.] 4
WWW.CNSFORUM.COM 18
13. DEGEE OF INDECISIVENESS
0 = None
1 = Mild, some trouble making decisions about minor things
2 = Moderate, freely reports significant trouble making decisions that others would not think twice
about
3 = Severe, continual weighing of pros and cons about nonessentials.
4 = Extreme, unable to make any decisions. Disabling.
Q: Do you have trouble making decisions about little things that 0
other people might not think twice about (e.g., which clothes to 1
put on in the morning; which brand of cereal to buy)? [Exclude 2
difficulty making decisions which reflect ruminative thinking. 3
Ambivalence concerning rationally-based difficult choices should 4
also be excluded.]
14. OVERVALUED SENSE OF RESPONSIBILY
0 = None I = Mild, only mentioned on questioning, slight sense of over-responsibility
2 = Moderate, ideas stated spontaneously, clearly present; patient experiences significant sense of
over-responsibility for events outside his/her reasonable control
3 = Severe, ideas prominent and pervasive; deeply concerned he/she is responsible for events clearly
outside his control. Self-blaming farfetched and nearly irrational
4 = Extreme, delusional sense of responsibility (e.g., if an earthquake occurs 3,000 miles away
patient blames herself because she didn't perform her compulsions)
Q: Do you feel very responsible for the consequences of your 0
actions? Do you blame yourself for the outcome of events not 1
completely in your control? [Distinguish from normal feelings of 2
responsibility, feelings of worthlessness, and pathological guilt. A 3
guilt-ridden person experiences himself or his actions as bad or 4
evil.]
15. PERVASIVE SLOWNESS/ DISTURBANCE OF INERTIA
0 = None.
I = Mild, occasional delay in starting or finishing.
2 = Moderate, frequent prolongation of routine activities but tasks usually completed. Frequently late.
3 = Severe, pervasive and marked difficulty initiating and completing routine tasks. Usually late.
4 = Extreme, unable to start or complete routine tasks without full assistance.
Q: Do you have difficulty starting or finishing tasks? Do many 0
routine activities take longer than they should? [Distinguish from 1
psychomotor retardation secondary to depression. Rate increased 2
time spent performing routine activities even when specific 3
obsessions cannot be identified.] 4
WWW.CNSFORUM.COM 18
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
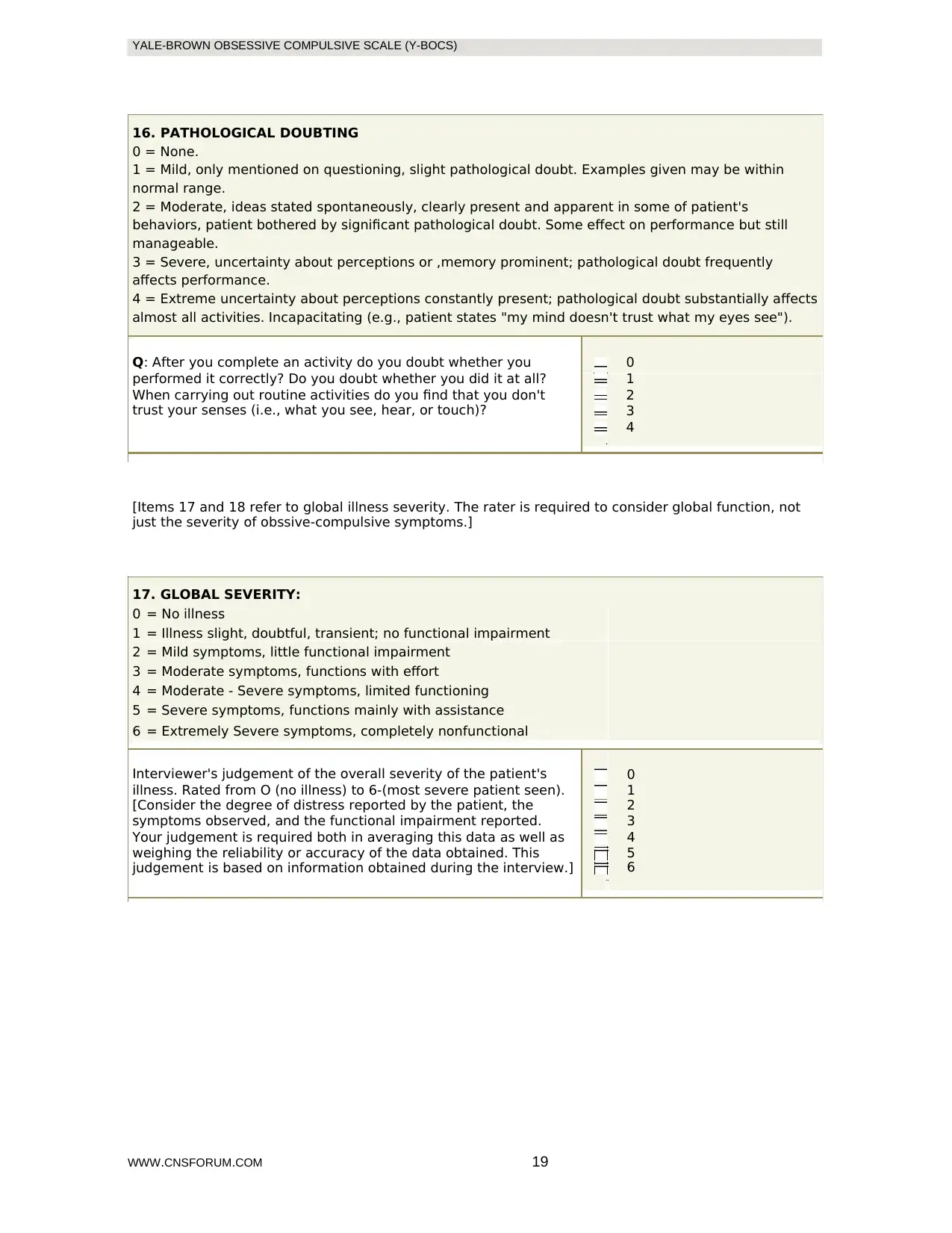
16. PATHOLOGICAL DOUBTING
0 = None.
1 = Mild, only mentioned on questioning, slight pathological doubt. Examples given may be within
normal range.
2 = Moderate, ideas stated spontaneously, clearly present and apparent in some of patient's
behaviors, patient bothered by significant pathological doubt. Some effect on performance but still
manageable.
3 = Severe, uncertainty about perceptions or ,memory prominent; pathological doubt frequently
affects performance.
4 = Extreme uncertainty about perceptions constantly present; pathological doubt substantially affects
almost all activities. Incapacitating (e.g., patient states "my mind doesn't trust what my eyes see").
Q: After you complete an activity do you doubt whether you 0
performed it correctly? Do you doubt whether you did it at all? 1
When carrying out routine activities do you find that you don't 2
trust your senses (i.e., what you see, hear, or touch)? 3
4
[Items 17 and 18 refer to global illness severity. The rater is required to consider global function, not
just the severity of obssive-compulsive symptoms.]
17. GLOBAL SEVERITY:
0 = No illness
1 = Illness slight, doubtful, transient; no functional impairment
2 = Mild symptoms, little functional impairment
3 = Moderate symptoms, functions with effort
4 = Moderate - Severe symptoms, limited functioning
5 = Severe symptoms, functions mainly with assistance
6 = Extremely Severe symptoms, completely nonfunctional
Interviewer's judgement of the overall severity of the patient's 0
illness. Rated from O (no illness) to 6-(most severe patient seen). 1
[Consider the degree of distress reported by the patient, the 2
symptoms observed, and the functional impairment reported. 3
Your judgement is required both in averaging this data as well as 4
weighing the reliability or accuracy of the data obtained. This 5
judgement is based on information obtained during the interview.] 6
WWW.CNSFORUM.COM 19
16. PATHOLOGICAL DOUBTING
0 = None.
1 = Mild, only mentioned on questioning, slight pathological doubt. Examples given may be within
normal range.
2 = Moderate, ideas stated spontaneously, clearly present and apparent in some of patient's
behaviors, patient bothered by significant pathological doubt. Some effect on performance but still
manageable.
3 = Severe, uncertainty about perceptions or ,memory prominent; pathological doubt frequently
affects performance.
4 = Extreme uncertainty about perceptions constantly present; pathological doubt substantially affects
almost all activities. Incapacitating (e.g., patient states "my mind doesn't trust what my eyes see").
Q: After you complete an activity do you doubt whether you 0
performed it correctly? Do you doubt whether you did it at all? 1
When carrying out routine activities do you find that you don't 2
trust your senses (i.e., what you see, hear, or touch)? 3
4
[Items 17 and 18 refer to global illness severity. The rater is required to consider global function, not
just the severity of obssive-compulsive symptoms.]
17. GLOBAL SEVERITY:
0 = No illness
1 = Illness slight, doubtful, transient; no functional impairment
2 = Mild symptoms, little functional impairment
3 = Moderate symptoms, functions with effort
4 = Moderate - Severe symptoms, limited functioning
5 = Severe symptoms, functions mainly with assistance
6 = Extremely Severe symptoms, completely nonfunctional
Interviewer's judgement of the overall severity of the patient's 0
illness. Rated from O (no illness) to 6-(most severe patient seen). 1
[Consider the degree of distress reported by the patient, the 2
symptoms observed, and the functional impairment reported. 3
Your judgement is required both in averaging this data as well as 4
weighing the reliability or accuracy of the data obtained. This 5
judgement is based on information obtained during the interview.] 6
WWW.CNSFORUM.COM 19
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
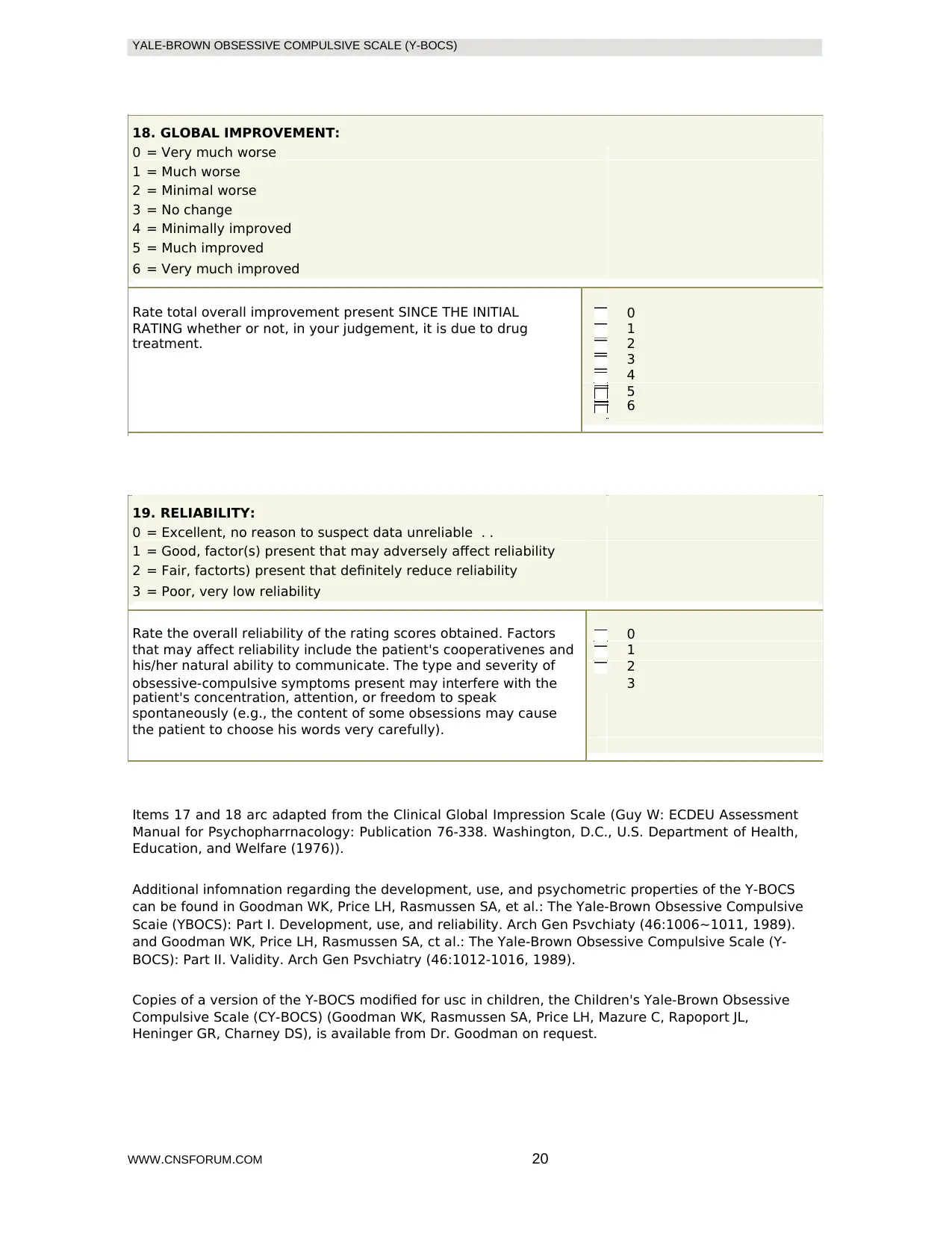
18. GLOBAL IMPROVEMENT:
0 = Very much worse
1 = Much worse
2 = Minimal worse
3 = No change
4 = Minimally improved
5 = Much improved
6 = Very much improved
Rate total overall improvement present SINCE THE INITIAL 0
RATING whether or not, in your judgement, it is due to drug 1
treatment. 2
3
4
5
6
19. RELIABILITY:
0 = Excellent, no reason to suspect data unreliable . .
1 = Good, factor(s) present that may adversely affect reliability
2 = Fair, factorts) present that definitely reduce reliability
3 = Poor, very low reliability
Rate the overall reliability of the rating scores obtained. Factors 0
that may affect reliability include the patient's cooperativenes and 1
his/her natural ability to communicate. The type and severity of 2
obsessive-compulsive symptoms present may interfere with the 3
patient's concentration, attention, or freedom to speak
spontaneously (e.g., the content of some obsessions may cause
the patient to choose his words very carefully).
Items 17 and 18 arc adapted from the Clinical Global Impression Scale (Guy W: ECDEU Assessment
Manual for Psychopharrnacology: Publication 76-338. Washington, D.C., U.S. Department of Health,
Education, and Welfare (1976)).
Additional infomnation regarding the development, use, and psychometric properties of the Y-BOCS
can be found in Goodman WK, Price LH, Rasmussen SA, et al.: The Yale-Brown Obsessive Compulsive
Scaie (YBOCS): Part I. Development, use, and reliability. Arch Gen Psvchiaty (46:1006~1011, 1989).
and Goodman WK, Price LH, Rasmussen SA, ct al.: The Yale-Brown Obsessive Compulsive Scale (Y-
BOCS): Part II. Validity. Arch Gen Psvchiatry (46:1012-1016, 1989).
Copies of a version of the Y-BOCS modified for usc in children, the Children's Yale-Brown Obsessive
Compulsive Scale (CY-BOCS) (Goodman WK, Rasmussen SA, Price LH, Mazure C, Rapoport JL,
Heninger GR, Charney DS), is available from Dr. Goodman on request.
WWW.CNSFORUM.COM 20
18. GLOBAL IMPROVEMENT:
0 = Very much worse
1 = Much worse
2 = Minimal worse
3 = No change
4 = Minimally improved
5 = Much improved
6 = Very much improved
Rate total overall improvement present SINCE THE INITIAL 0
RATING whether or not, in your judgement, it is due to drug 1
treatment. 2
3
4
5
6
19. RELIABILITY:
0 = Excellent, no reason to suspect data unreliable . .
1 = Good, factor(s) present that may adversely affect reliability
2 = Fair, factorts) present that definitely reduce reliability
3 = Poor, very low reliability
Rate the overall reliability of the rating scores obtained. Factors 0
that may affect reliability include the patient's cooperativenes and 1
his/her natural ability to communicate. The type and severity of 2
obsessive-compulsive symptoms present may interfere with the 3
patient's concentration, attention, or freedom to speak
spontaneously (e.g., the content of some obsessions may cause
the patient to choose his words very carefully).
Items 17 and 18 arc adapted from the Clinical Global Impression Scale (Guy W: ECDEU Assessment
Manual for Psychopharrnacology: Publication 76-338. Washington, D.C., U.S. Department of Health,
Education, and Welfare (1976)).
Additional infomnation regarding the development, use, and psychometric properties of the Y-BOCS
can be found in Goodman WK, Price LH, Rasmussen SA, et al.: The Yale-Brown Obsessive Compulsive
Scaie (YBOCS): Part I. Development, use, and reliability. Arch Gen Psvchiaty (46:1006~1011, 1989).
and Goodman WK, Price LH, Rasmussen SA, ct al.: The Yale-Brown Obsessive Compulsive Scale (Y-
BOCS): Part II. Validity. Arch Gen Psvchiatry (46:1012-1016, 1989).
Copies of a version of the Y-BOCS modified for usc in children, the Children's Yale-Brown Obsessive
Compulsive Scale (CY-BOCS) (Goodman WK, Rasmussen SA, Price LH, Mazure C, Rapoport JL,
Heninger GR, Charney DS), is available from Dr. Goodman on request.
WWW.CNSFORUM.COM 20
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
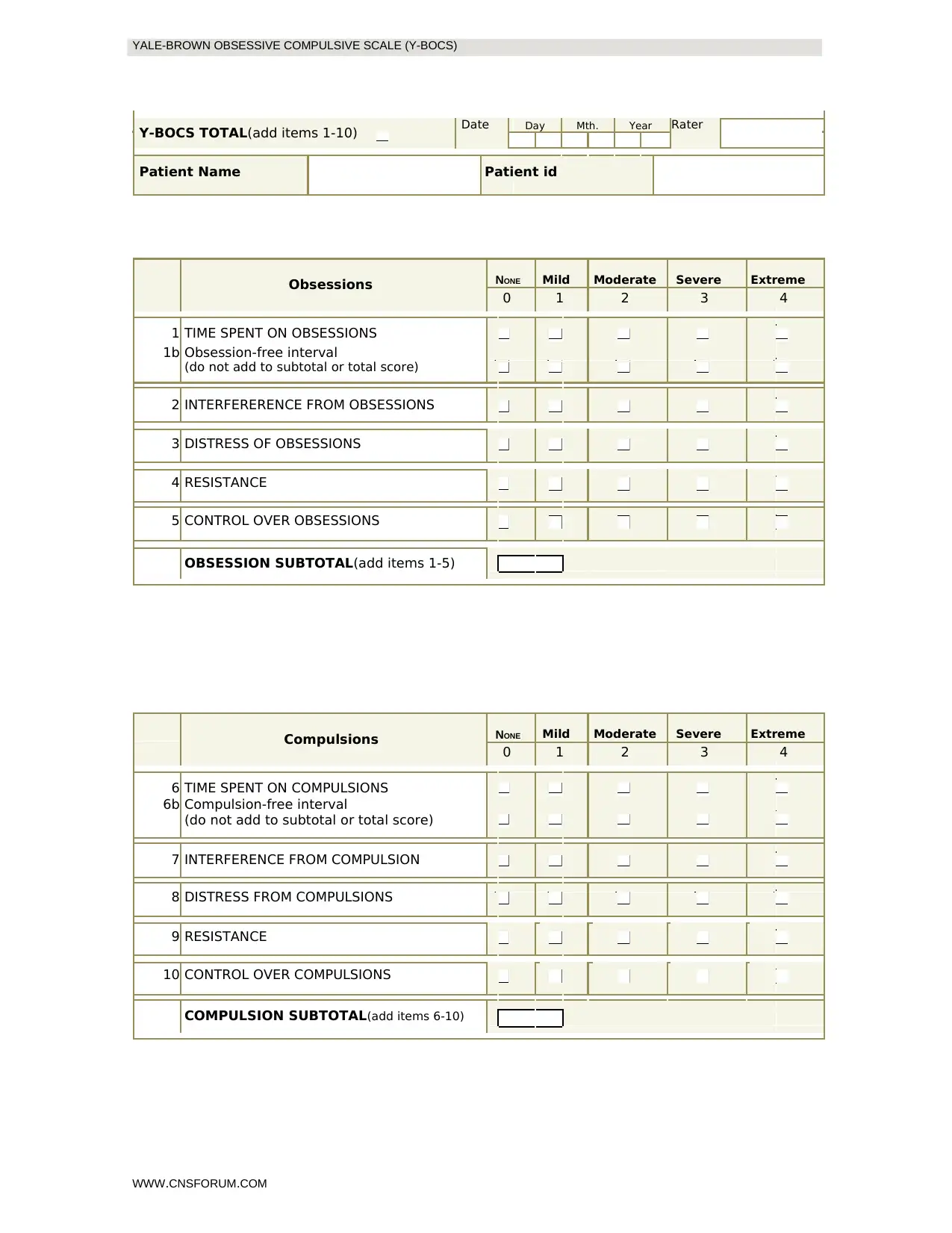
Y-BOCS TOTAL(add items 1-10) Date Day Mth. Year Rater
Patient Name Patient id
Obsessions NONE Mild Moderate Severe Extreme
0 1 2 3 4
1 TIME SPENT ON OBSESSIONS
1b Obsession-free interval
(do not add to subtotal or total score)
2 INTERFERERENCE FROM OBSESSIONS
3 DISTRESS OF OBSESSIONS
4 RESISTANCE
5 CONTROL OVER OBSESSIONS
OBSESSION SUBTOTAL(add items 1-5)
Compulsions NONE Mild Moderate Severe Extreme
0 1 2 3 4
6 TIME SPENT ON COMPULSIONS
6b Compulsion-free interval
(do not add to subtotal or total score)
7 INTERFERENCE FROM COMPULSION
8 DISTRESS FROM COMPULSIONS
9 RESISTANCE
10 CONTROL OVER COMPULSIONS
COMPULSION SUBTOTAL(add items 6-10)
WWW.CNSFORUM.COM
Y-BOCS TOTAL(add items 1-10) Date Day Mth. Year Rater
Patient Name Patient id
Obsessions NONE Mild Moderate Severe Extreme
0 1 2 3 4
1 TIME SPENT ON OBSESSIONS
1b Obsession-free interval
(do not add to subtotal or total score)
2 INTERFERERENCE FROM OBSESSIONS
3 DISTRESS OF OBSESSIONS
4 RESISTANCE
5 CONTROL OVER OBSESSIONS
OBSESSION SUBTOTAL(add items 1-5)
Compulsions NONE Mild Moderate Severe Extreme
0 1 2 3 4
6 TIME SPENT ON COMPULSIONS
6b Compulsion-free interval
(do not add to subtotal or total score)
7 INTERFERENCE FROM COMPULSION
8 DISTRESS FROM COMPULSIONS
9 RESISTANCE
10 CONTROL OVER COMPULSIONS
COMPULSION SUBTOTAL(add items 6-10)
WWW.CNSFORUM.COM

21
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
YALE-BROWN OBSESSIVE COMPULSIVE SCALE (Y-BOCS)
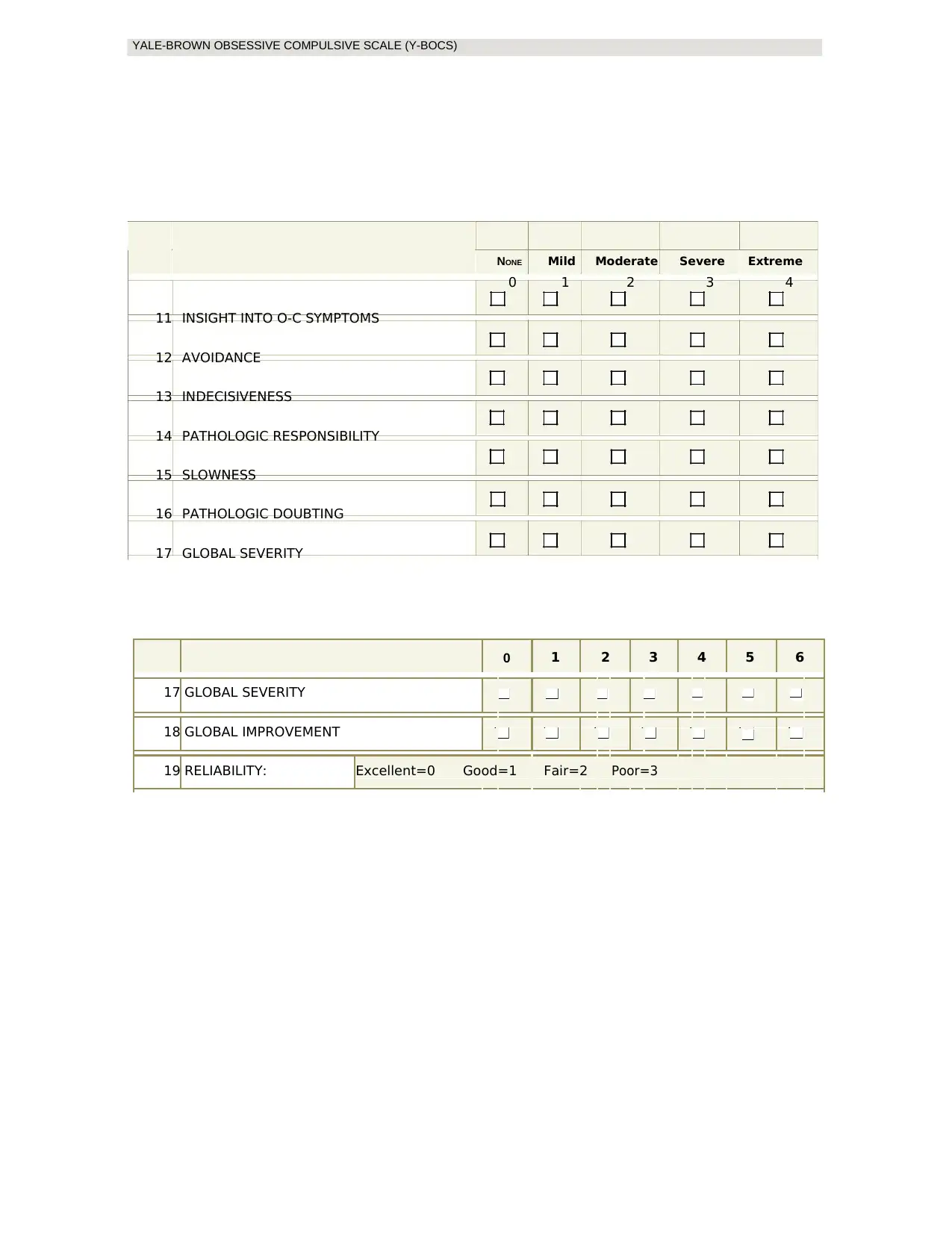
NONE Mild Moderate Severe Extreme
0 1 2 3 4
11 INSIGHT INTO O-C SYMPTOMS
12 AVOIDANCE
13 INDECISIVENESS
14 PATHOLOGIC RESPONSIBILITY
15 SLOWNESS
16 PATHOLOGIC DOUBTING
17 GLOBAL SEVERITY
0 1 2 3 4 5 6
17 GLOBAL SEVERITY
18 GLOBAL IMPROVEMENT
19 RELIABILITY: Excellent=0 Good=1 Fair=2 Poor=3
NONE Mild Moderate Severe Extreme
0 1 2 3 4
11 INSIGHT INTO O-C SYMPTOMS
12 AVOIDANCE
13 INDECISIVENESS
14 PATHOLOGIC RESPONSIBILITY
15 SLOWNESS
16 PATHOLOGIC DOUBTING
17 GLOBAL SEVERITY
0 1 2 3 4 5 6
17 GLOBAL SEVERITY
18 GLOBAL IMPROVEMENT
19 RELIABILITY: Excellent=0 Good=1 Fair=2 Poor=3
WWW.CNSFORUM.COM
22
22
1 out of 21
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.