Medical Case Study: Evaluating Respiratory & Metabolic Acidosis
VerifiedAdded on 2023/06/14
|5
|1452
|118
Case Study
AI Summary
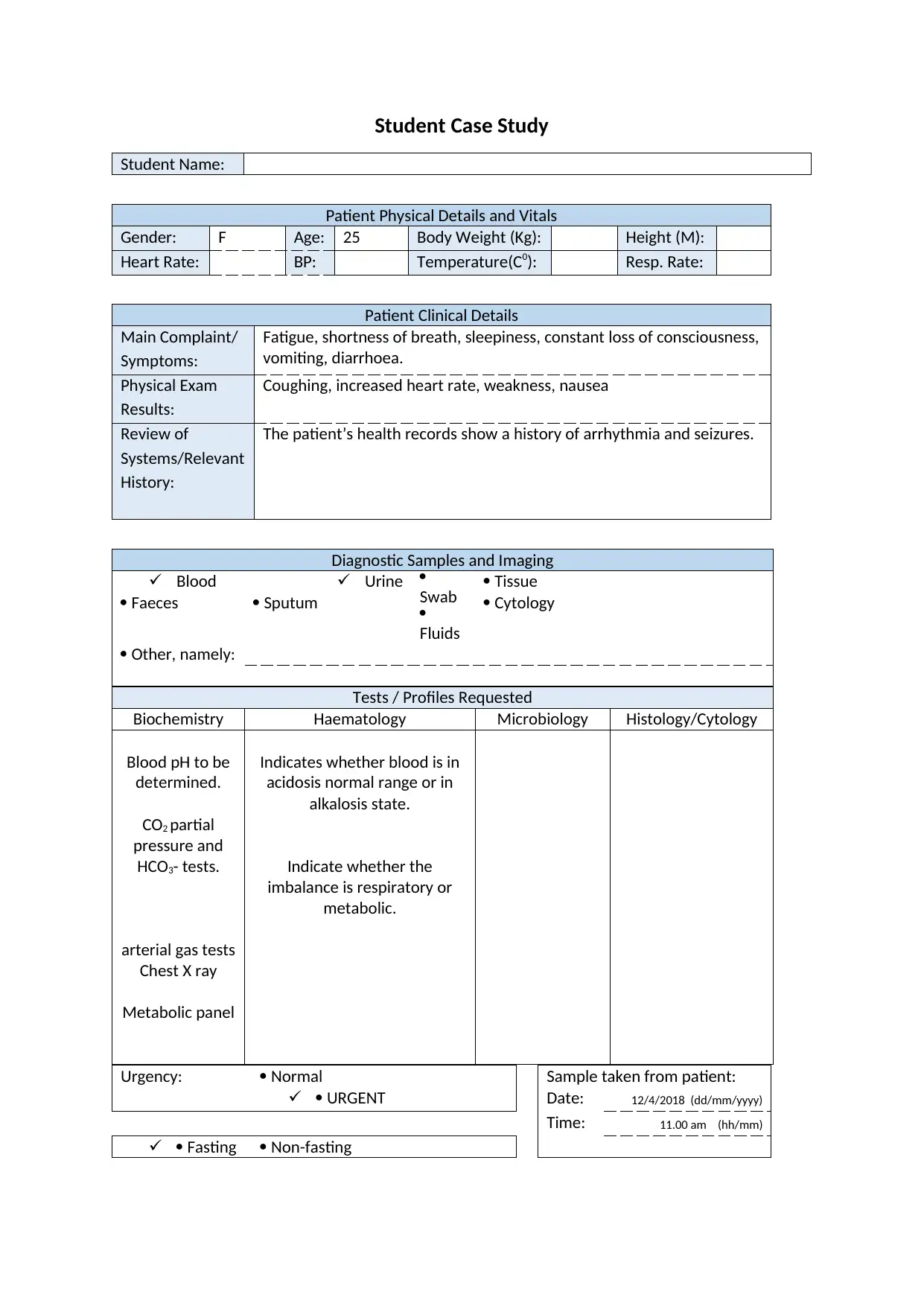
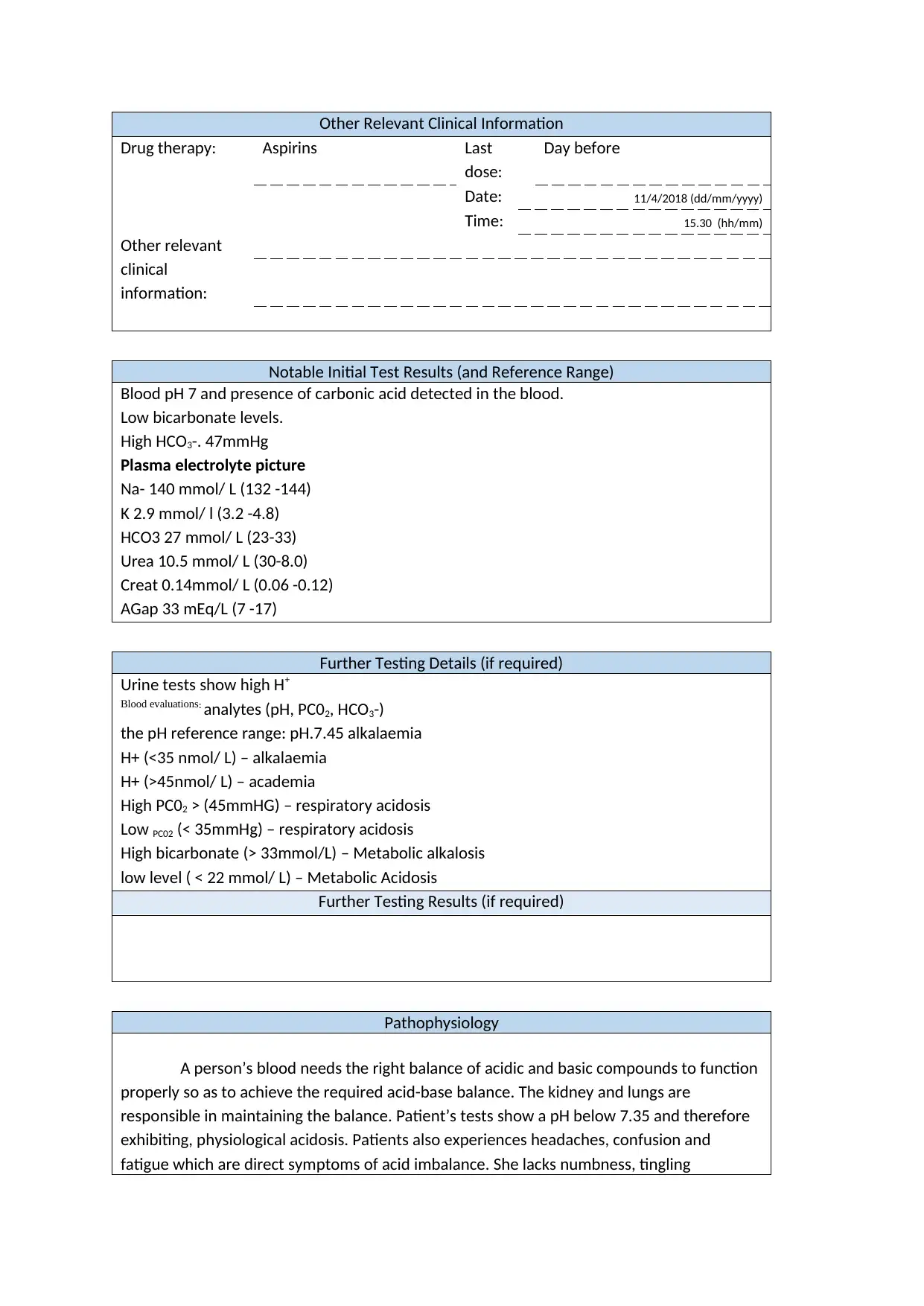
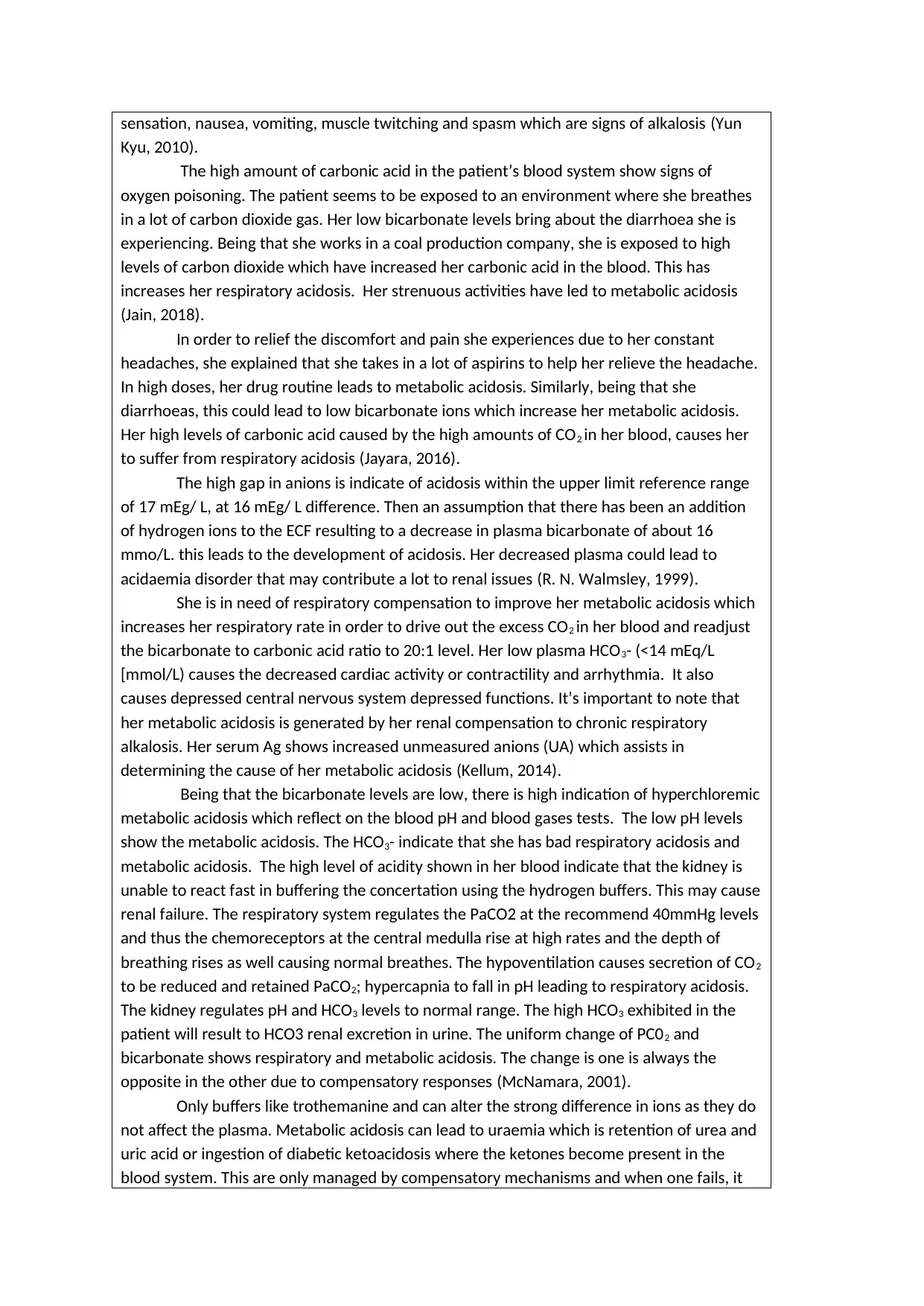
This case study presents a 25-year-old female patient experiencing fatigue, shortness of breath, and loss of consciousness, revealing a history of arrhythmia and seizures. Diagnostic tests indicate a blood pH of 7, high carbonic acid levels, low bicarbonate, and elevated anion gap, pointing towards physiological acidosis. The patient's symptoms and lab results suggest both respiratory and metabolic acidosis, potentially linked to her occupation in coal production, aspirin use, and diarrhea. The analysis explores the pathophysiology of acid-base imbalances, the compensatory mechanisms of the kidneys and lungs, and the potential for renal failure if the condition worsens. High levels of hydrogen ion was also found in urine samples due to retention of bicarbonate ions by the kidney. The study references various articles related to the diagnosis and treatment of acid-base disorders. Desklib provides access to similar case studies and solved assignments for students.

1 out of 5
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.