Western Sydney University: Health Variations 3 - Mrs. Brown Case Study
VerifiedAdded on 2022/10/14
|8
|1871
|10
Report
AI Summary
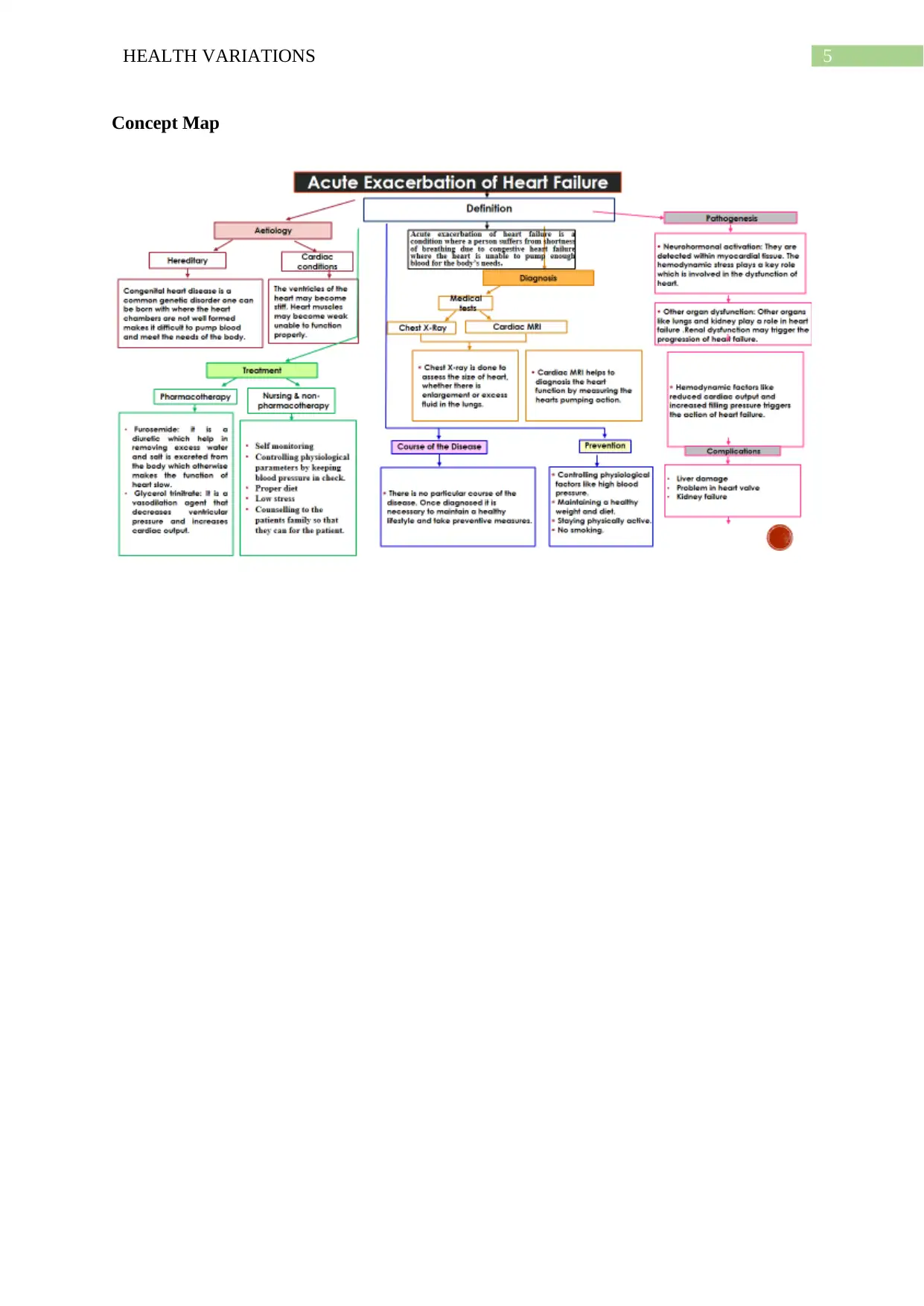
This report presents a comprehensive analysis of Mrs. Brown's case, who is suffering from acute shortness of breath and chronic respiratory disease, with a focus on the pathogenesis of her clinical manifestations. The report details her symptoms, including severe dyspnea and the presence of bilateral basal cracks, linking these to potential causes such as heart failure and atrial fibrillation. It explores the role of aging and other organ system diseases in her condition. Nursing interventions, including oxygen therapy, breathing exercises, patient counseling, and medication management (Furosemide and sublingual glycerol trinitrate), are discussed to manage her condition. The report also explains the mechanism of action of Furosemide and glycerol trinitrate, highlighting their roles in managing fluid balance and cardiovascular function. The importance of nursing assessment, care, and rehabilitation is emphasized, along with the need for health education and self-monitoring. The report concludes with a concept map and references, providing a structured overview of Mrs. Brown's health variations and the strategies for her care.

1 out of 8
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.