Acute Life Threatening Conditions Analysis: Nursing Assignment 401211
VerifiedAdded on 2022/12/23
|7
|1658
|81
Homework Assignment
AI Summary
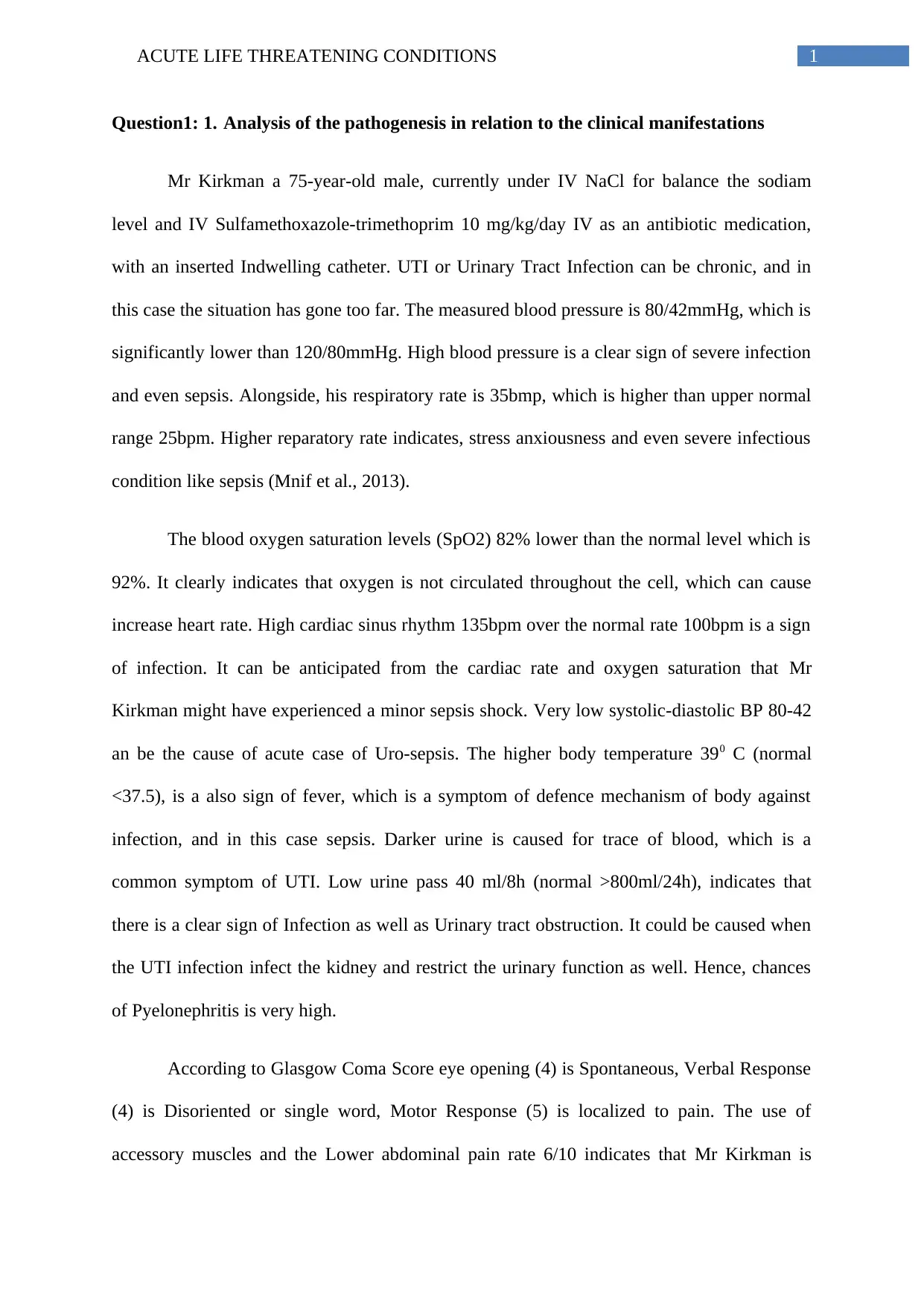
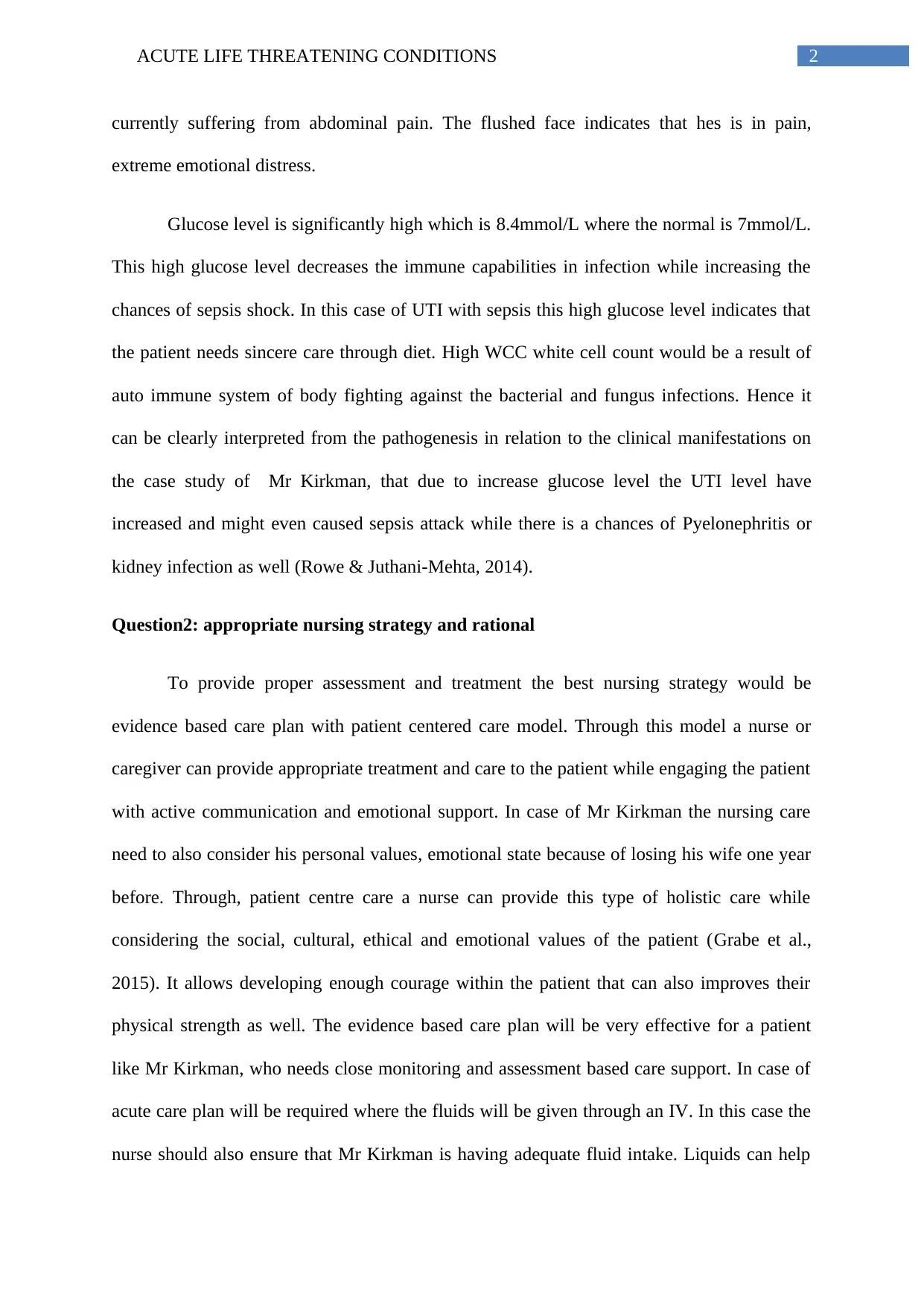
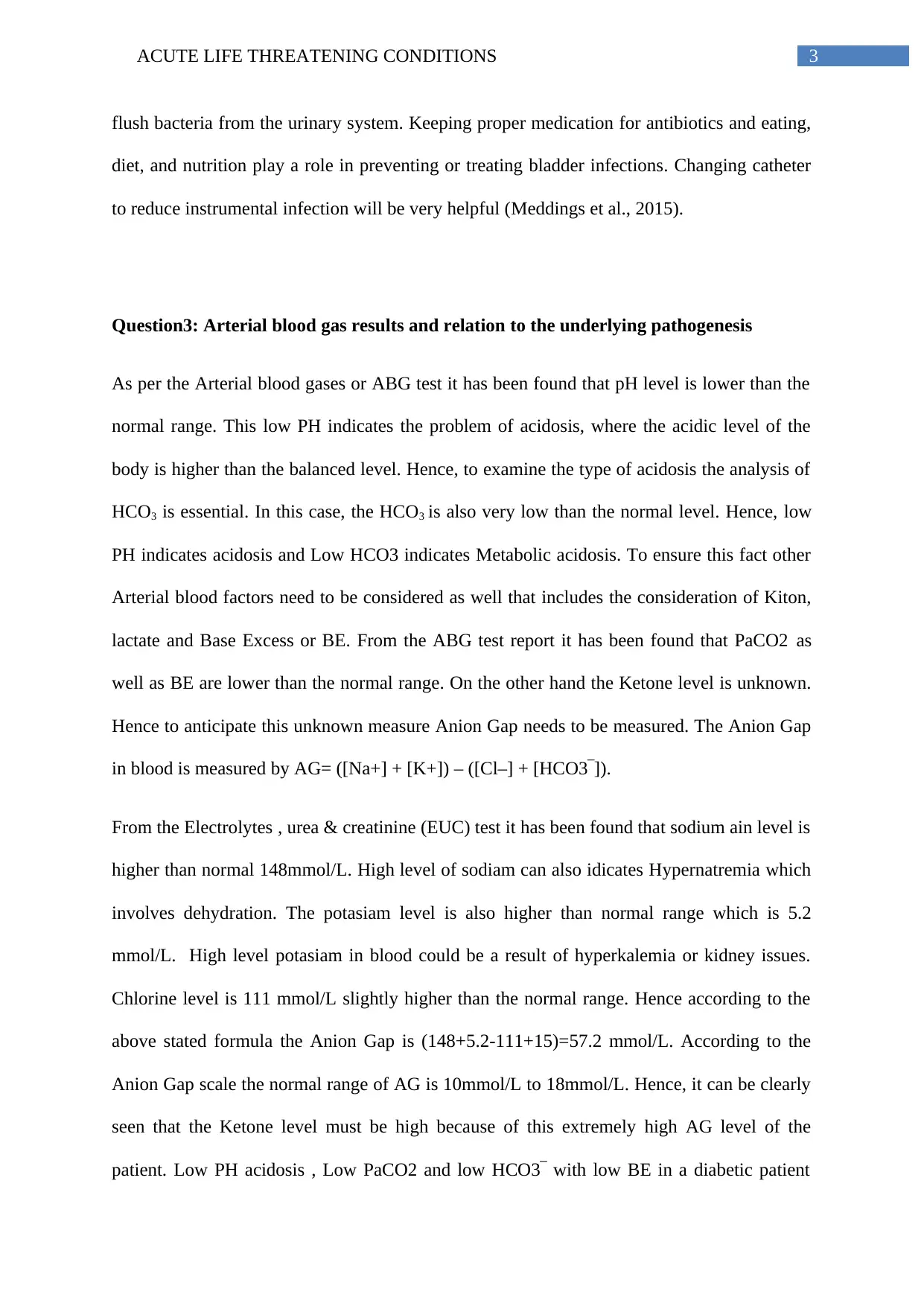
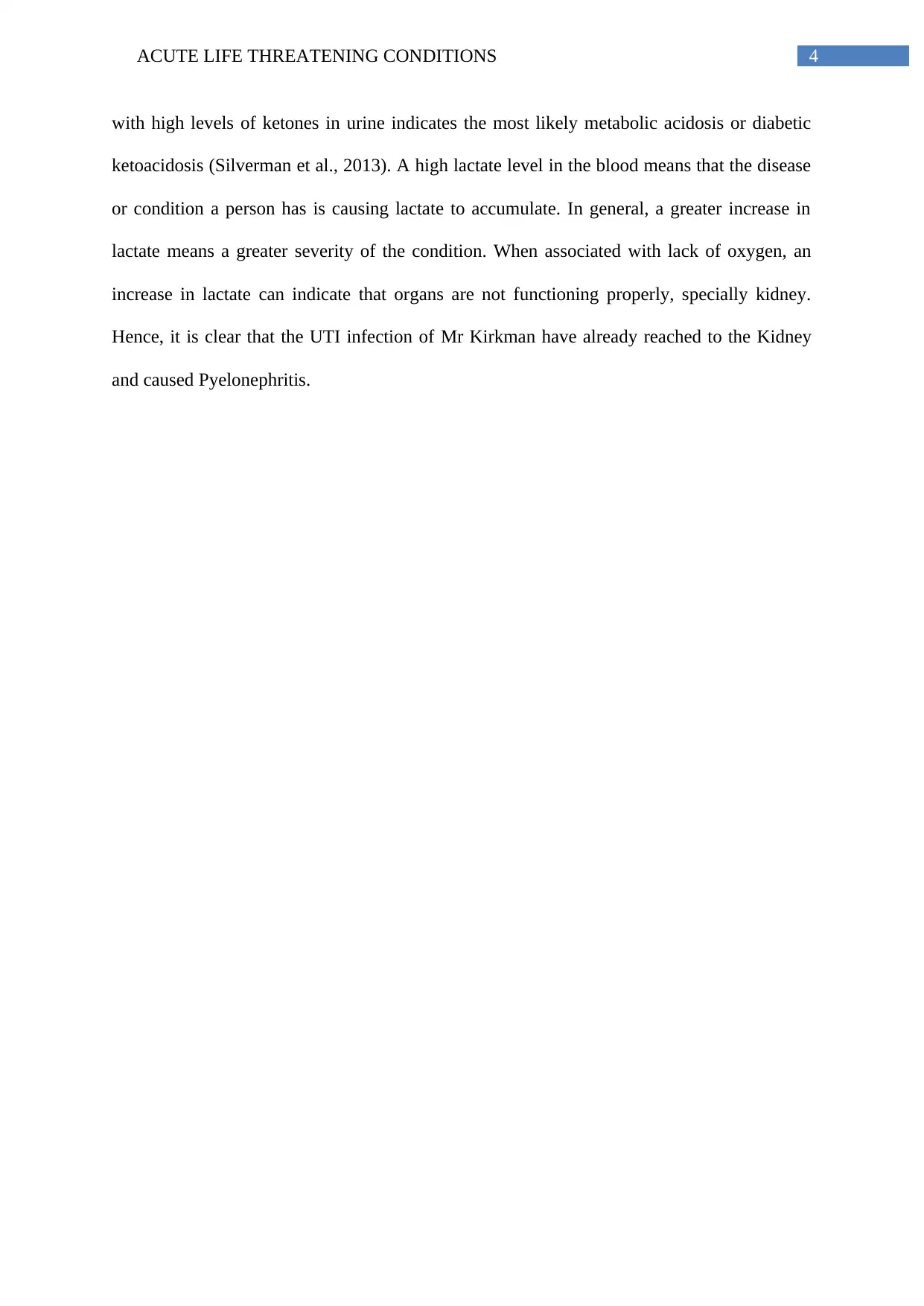
This assignment analyzes a case study of a 75-year-old male, Mr. Kirkman, presenting with acute life-threatening conditions. The analysis begins with an examination of the pathogenesis of Mr. Kirkman's symptoms, including low blood pressure, elevated respiratory and heart rates, low oxygen saturation, fever, and abnormal urine characteristics, all indicative of a severe urinary tract infection (UTI) potentially progressing to sepsis and pyelonephritis. The assignment then proposes an evidence-based nursing strategy, emphasizing patient-centered care and fluid management to flush out bacteria and prevent further infection. Lastly, the assignment critically analyzes arterial blood gas (ABG) results, revealing metabolic acidosis, and relates these findings to the underlying pathogenesis, including high sodium, potassium and chlorine levels. The analysis concludes that the patient is suffering from diabetic ketoacidosis or metabolic acidosis and the UTI infection has already reached the kidney and caused Pyelonephritis.


1 out of 7
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.