UNRS 212 Acute Pancreatitis: A Comprehensive Case Study Analysis
VerifiedAdded on 2023/04/21
|15
|3411
|53
Case Study
AI Summary
This case study presents a 52-year-old male admitted to the emergency department with acute pancreatitis. The patient's history includes hypertension, hyperlipidemia, peptic ulcer, appendectomy, and cholecystectomy. The case details the patient's chief complaints of abdominal pain, physical assessment findings, and relevant past medical history. Diagnostic workup included blood tests, EKG, and a CT scan, which revealed elevated white blood cell count, total bilirubin, and lipase enzyme levels. The pathophysiology of acute pancreatitis, focusing on gallstones and alcohol use, is discussed, along with the patient's medication management, treatment strategies including potential surgical interventions, and considerations for psychosocial and spiritual well-being, particularly adherence to Jewish dietary laws. The study also includes a nursing care plan addressing ineffective breathing patterns related to severe abdominal pain, with specific goals, interventions, and rationales.

Running header: ACUTE PANCREATITIS 1
Acute pancreatitis
Student name
Student ID
Specialty area
Date
Acute pancreatitis
Student name
Student ID
Specialty area
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Acute pancreatitis case study
Introduction
Pancreatitis refers to the inflammation of the pancreas. The pancreas is a long, leaf-like organ
about 13 cm long located in the upper abdomen. The pancreas has three functions of great
importance. It produces a digestive enzyme into the duodenum, it secretes insulin and glucagon
which help control the blood glucose level and lastly secretion of sodium bicarbonate which
neutralizes the acid originating from the stomach (Balthazar, Ranson, & Megibow).
Pancreatitis can be caused by gallstones, viral infections, various drugs, and last but not least
alcohol. Pancreatic inflammation can occur as acute pancreatitis meaning it develops suddenly
and lasts for days. In some cases, however, the inflammation may last for a long time and slowly
damage the pancreatic function (Balthazar, 2012). This is called chronic pancreatitis. The
objectives of this paper include pathogenesis of acute pancreatitis and management of a client
suffering from the condition.
Identifying data
Name: Mr. X
Sex: Male
Age: 52 years
Source of information: client
Chief complaints
“Abdominal pain, it feels like last time when I had surgery”
Acute pancreatitis case study
Introduction
Pancreatitis refers to the inflammation of the pancreas. The pancreas is a long, leaf-like organ
about 13 cm long located in the upper abdomen. The pancreas has three functions of great
importance. It produces a digestive enzyme into the duodenum, it secretes insulin and glucagon
which help control the blood glucose level and lastly secretion of sodium bicarbonate which
neutralizes the acid originating from the stomach (Balthazar, Ranson, & Megibow).
Pancreatitis can be caused by gallstones, viral infections, various drugs, and last but not least
alcohol. Pancreatic inflammation can occur as acute pancreatitis meaning it develops suddenly
and lasts for days. In some cases, however, the inflammation may last for a long time and slowly
damage the pancreatic function (Balthazar, 2012). This is called chronic pancreatitis. The
objectives of this paper include pathogenesis of acute pancreatitis and management of a client
suffering from the condition.
Identifying data
Name: Mr. X
Sex: Male
Age: 52 years
Source of information: client
Chief complaints
“Abdominal pain, it feels like last time when I had surgery”
3
History of presenting illness
Mr. X was admitted to the emergency department presenting with abdominal pain. The pain
gradually began at 8 pm last night. The client complained of a sharp stabbing epigastric pain
occurring mostly on the right upper and lower quadrant. Associated manifestation includes
nausea without vomiting. The client reports negative on back pains, fever, urinary infection, and
recent travel and lastly is not on any antibiotic medication.
Past medical history
i. Adult illnesses
The client has had hypertension, hyperlipidemia, and peptic ulcer
ii. Operations
The client has had multiple abdominal surgeries, appendectomy, and lastly cholecystectomy.
Medical diagnosis
The client was diagnosed with acute pancreatitis which presented with upper abdominal pain.
On palpation the abdomen was tender and the abdominal muscles rigid. Pain caused by
gallstones starts immediately and reaches its peak over minutes. If the pancreatitis is caused by
alcohol develops over a few days. The diagnostic done included blood tests and imaging tests.
Home medications
The client denies any prescribed home medication.
Physical assessment
History of presenting illness
Mr. X was admitted to the emergency department presenting with abdominal pain. The pain
gradually began at 8 pm last night. The client complained of a sharp stabbing epigastric pain
occurring mostly on the right upper and lower quadrant. Associated manifestation includes
nausea without vomiting. The client reports negative on back pains, fever, urinary infection, and
recent travel and lastly is not on any antibiotic medication.
Past medical history
i. Adult illnesses
The client has had hypertension, hyperlipidemia, and peptic ulcer
ii. Operations
The client has had multiple abdominal surgeries, appendectomy, and lastly cholecystectomy.
Medical diagnosis
The client was diagnosed with acute pancreatitis which presented with upper abdominal pain.
On palpation the abdomen was tender and the abdominal muscles rigid. Pain caused by
gallstones starts immediately and reaches its peak over minutes. If the pancreatitis is caused by
alcohol develops over a few days. The diagnostic done included blood tests and imaging tests.
Home medications
The client denies any prescribed home medication.
Physical assessment
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
I. General survey
The client had a blood pressure of 159/99mm/Hg, the pulse of 66 beats/minute,
temperature was 36.4 degree Celsius, respiration of 20 and peripheral capillary oxygen
saturation of 97%. His height was 1.676m, weight of 100.8kg and lastly a BMI of
35.87kg/m2.
II. General appearance and mental status
No signs of distress observed in facial expression and posture. The client’s weight, height
is proportionate to his age. He is clean and neat nobody or breath odor. The quantity and
quality of speech is moderate pace and clear tone. The client is in a good frame of mind, he
shows cooperation and adheres to instruction. His thoughts are well organized, logic and
have a sense of reality.
III. Integumentary
The skin color under natural light varies from light to deep brown, the skin is generally
uniform the palms, nail bed and lips are lighter in pigmentation. There are no signs of edema or
skin lesions. The skin folds and axillae are well moisturized, the surface temperatures are
uniform and within the normal range in all areas of the body. The client has a normal skin turgor
when pinched the skin goes back to its original state quickly. The hair is evenly distributed, there
is no sign of infection or infestation behind the ears or the hairline at the neck. The nails are
smooth in texture, the nail plate has a convex curvature of about 1600. The toenail and the
fingernail are highly vascular, pink in color and have a good capillary refill.
iii. Head
I. General survey
The client had a blood pressure of 159/99mm/Hg, the pulse of 66 beats/minute,
temperature was 36.4 degree Celsius, respiration of 20 and peripheral capillary oxygen
saturation of 97%. His height was 1.676m, weight of 100.8kg and lastly a BMI of
35.87kg/m2.
II. General appearance and mental status
No signs of distress observed in facial expression and posture. The client’s weight, height
is proportionate to his age. He is clean and neat nobody or breath odor. The quantity and
quality of speech is moderate pace and clear tone. The client is in a good frame of mind, he
shows cooperation and adheres to instruction. His thoughts are well organized, logic and
have a sense of reality.
III. Integumentary
The skin color under natural light varies from light to deep brown, the skin is generally
uniform the palms, nail bed and lips are lighter in pigmentation. There are no signs of edema or
skin lesions. The skin folds and axillae are well moisturized, the surface temperatures are
uniform and within the normal range in all areas of the body. The client has a normal skin turgor
when pinched the skin goes back to its original state quickly. The hair is evenly distributed, there
is no sign of infection or infestation behind the ears or the hairline at the neck. The nails are
smooth in texture, the nail plate has a convex curvature of about 1600. The toenail and the
fingernail are highly vascular, pink in color and have a good capillary refill.
iii. Head
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
The skull is rounded and symmetric with occipital, frontal and parietal prominence. The client
has a symmetric facial expression with no sign of edema around the face. The eyebrow is evenly
distributed with the symmetrically aligned. The bulbar conjunctiva is transparent and the sclera
appears white in color. The cornea is transparent and smooth in texture, the pupils are brown in
color with a size of 7mm in diameter. The illuminated and non-illuminated pupils constrict. The
auricles are symmetrical and of the same color as the facial skin. The tympanic membrane is
gray in color and semitransparent. The sound is heard in both ears. Distal third of the ear canal
contains hair follicle and dry cerumen. The lips are pink, moist and smooth in texture. The
tongue is pink and moves freely no signs of tenderness. The tonsils are pink and smooth, of
normal size and no discharge present.
iv. Thorax and lungs
The spinal column is uniform in alignment, the right, and left shoulders are of the same size.
No sign of tenderness or masses on the chest wall. Thorax expansion is equal in size. There are
normal percussion sounds on the posterior thorax. The anterior thorax expansion is equal in size
during inspiration and expiration. Vesicular and bronchial vesicular sounds are heard during
inspiration and expiration. Bronchial and vesicular sounds are clearly heard when auscultated
along the trachea. The lung tissue shows no presence of liquid or solid material after percussion.
The client demonstrates normal breathing patterns and sounds.
v. Cardiovascular and peripheral vascular system
On auscultation S1 sound is heard at all sites and heard best at the apical area. The S2
sound is heard louder at the base of the heart. No sound is heard on auscultation of the
carotid artery. The jugular veins are not distended indicating that the heart is functioning
The skull is rounded and symmetric with occipital, frontal and parietal prominence. The client
has a symmetric facial expression with no sign of edema around the face. The eyebrow is evenly
distributed with the symmetrically aligned. The bulbar conjunctiva is transparent and the sclera
appears white in color. The cornea is transparent and smooth in texture, the pupils are brown in
color with a size of 7mm in diameter. The illuminated and non-illuminated pupils constrict. The
auricles are symmetrical and of the same color as the facial skin. The tympanic membrane is
gray in color and semitransparent. The sound is heard in both ears. Distal third of the ear canal
contains hair follicle and dry cerumen. The lips are pink, moist and smooth in texture. The
tongue is pink and moves freely no signs of tenderness. The tonsils are pink and smooth, of
normal size and no discharge present.
iv. Thorax and lungs
The spinal column is uniform in alignment, the right, and left shoulders are of the same size.
No sign of tenderness or masses on the chest wall. Thorax expansion is equal in size. There are
normal percussion sounds on the posterior thorax. The anterior thorax expansion is equal in size
during inspiration and expiration. Vesicular and bronchial vesicular sounds are heard during
inspiration and expiration. Bronchial and vesicular sounds are clearly heard when auscultated
along the trachea. The lung tissue shows no presence of liquid or solid material after percussion.
The client demonstrates normal breathing patterns and sounds.
v. Cardiovascular and peripheral vascular system
On auscultation S1 sound is heard at all sites and heard best at the apical area. The S2
sound is heard louder at the base of the heart. No sound is heard on auscultation of the
carotid artery. The jugular veins are not distended indicating that the heart is functioning
6
normally. Peripheral pulse is symmetrical in both sides of the arm. Peripheral perfusion is
normal, the skin temperature is not too much warm or cold. On auscultation, the point of
maximum impulse is located on the fifth intercostal space.
Abdomen
There is no evidence of an enlarged liver or spleen. On auscultation bowel, sounds are
heard audibly. The intestinal sounds are heard best on the diaphragm. Arterial bruits are
absent on auscultation of the aorta and femoral arteries. Peritoneal friction rubs are absent.
There is tenderness on palpation of the abdomen. On percussion of the abdomen, there is
dullness, especially over the liver and spleen.
Musculoskeletal
There are no deformities in the musculoskeletal structure. There is no swelling,
tenderness, nodules on the joints. The muscles are equal in size on both sides of the body.
There is no evidence of tremor in the muscles.
Neurologic system
The client quickly touches each finger to thumb with each hand and shows equal
coordination when asked to place the heel of one foot below the opposite knee. His
sensitivity light-touch is unremarkable, the client is sensitive to light touch and sensation.
The client can readily discriminate between sharp or dull sensations.
Pathophysiology
Gall stones are the major cause of acute pancreatitis. Gallstones are aggregated solid material
in the gallbladder. Autodigestion of the pancreas by its own activated enzyme primary trypsin is
normally. Peripheral pulse is symmetrical in both sides of the arm. Peripheral perfusion is
normal, the skin temperature is not too much warm or cold. On auscultation, the point of
maximum impulse is located on the fifth intercostal space.
Abdomen
There is no evidence of an enlarged liver or spleen. On auscultation bowel, sounds are
heard audibly. The intestinal sounds are heard best on the diaphragm. Arterial bruits are
absent on auscultation of the aorta and femoral arteries. Peritoneal friction rubs are absent.
There is tenderness on palpation of the abdomen. On percussion of the abdomen, there is
dullness, especially over the liver and spleen.
Musculoskeletal
There are no deformities in the musculoskeletal structure. There is no swelling,
tenderness, nodules on the joints. The muscles are equal in size on both sides of the body.
There is no evidence of tremor in the muscles.
Neurologic system
The client quickly touches each finger to thumb with each hand and shows equal
coordination when asked to place the heel of one foot below the opposite knee. His
sensitivity light-touch is unremarkable, the client is sensitive to light touch and sensation.
The client can readily discriminate between sharp or dull sensations.
Pathophysiology
Gall stones are the major cause of acute pancreatitis. Gallstones are aggregated solid material
in the gallbladder. Autodigestion of the pancreas by its own activated enzyme primary trypsin is
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
the major cause of acute pancreatitis (Lerch, Runzi, & Saluja, 2014). On certain occasions, this
stones pass into and block the bile duct. Under normal conditions, the bile duct produces
pancreatic fluid through the pancreatic duct into the duodenum. The major function of this
pancreatic fluid is to help digest food. If a gallstone blocks the sphincter of Oddi, a hole in which
the pancreatic duct opens into the duodenum, the pancreatic juice comes into a halt. The
blockage causes the accumulation of pancreatic juice and begins digesting the cells of the
pancreas leading to severe inflammation (Acosta & Ledesma, 2013). Prolonged use of alcohol is
also linked to acute pancreatitis. Alcohol is broken down to toxic chemicals that cause damage to
pancreatic cells. Other less common causes include viral infection, spasms of the ampulla of
Vater, hyperlipidemia, use of corticosteroids, and last but not least hypercalcemia (Lormbadi,
Estes, & Longnecker, 2015).
Diagnostic work up
Diagnostic test and procedure
100 milliliters of contrast called omnipaques was given intravenously and a CT scan was
conducted. The following findings were noted.
a. Abdomen
The lung bases, liver, and adrenal glands were unremarkable. The client is status post
cholecystectomy. The spleen shows to be normal in size. There is the presence of mild fat around
the head of the pancreas. There is no evidence of abscess, pseudocyst or acute necrosis. The
kidneys appear to be normal in size, there is no presence of renal mass, calculi, and
hydronephrosis. The client presents with mild atherosclerosis without an aneurysm. There is no
evidence of ascites, fluid collection, pneumoperitoneum, and abdominal adenopathy. There is
the major cause of acute pancreatitis (Lerch, Runzi, & Saluja, 2014). On certain occasions, this
stones pass into and block the bile duct. Under normal conditions, the bile duct produces
pancreatic fluid through the pancreatic duct into the duodenum. The major function of this
pancreatic fluid is to help digest food. If a gallstone blocks the sphincter of Oddi, a hole in which
the pancreatic duct opens into the duodenum, the pancreatic juice comes into a halt. The
blockage causes the accumulation of pancreatic juice and begins digesting the cells of the
pancreas leading to severe inflammation (Acosta & Ledesma, 2013). Prolonged use of alcohol is
also linked to acute pancreatitis. Alcohol is broken down to toxic chemicals that cause damage to
pancreatic cells. Other less common causes include viral infection, spasms of the ampulla of
Vater, hyperlipidemia, use of corticosteroids, and last but not least hypercalcemia (Lormbadi,
Estes, & Longnecker, 2015).
Diagnostic work up
Diagnostic test and procedure
100 milliliters of contrast called omnipaques was given intravenously and a CT scan was
conducted. The following findings were noted.
a. Abdomen
The lung bases, liver, and adrenal glands were unremarkable. The client is status post
cholecystectomy. The spleen shows to be normal in size. There is the presence of mild fat around
the head of the pancreas. There is no evidence of abscess, pseudocyst or acute necrosis. The
kidneys appear to be normal in size, there is no presence of renal mass, calculi, and
hydronephrosis. The client presents with mild atherosclerosis without an aneurysm. There is no
evidence of ascites, fluid collection, pneumoperitoneum, and abdominal adenopathy. There is
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
evidence bowel surgery on the right. The client has no bowel obstruction and lastly, there is no
identification of the appendix.
b. Pelvis
The urinary bladder is unremarkable, the presence of metal clips in the inguinal canal and
lastly no presence of adenopathy.
Lab findings
Upon admission, an EKG, liver function test, complete blood count, troponin level test and
electrolyte test was conducted and the following findings were noted. The white blood cell
count is higher than the normal range indicating a sign of infection (Moon & Cho, 2012). The
EKG shows that the client has sinus bradycardia of 55 beats per minute. Acute pancreatitis
normally associated with arrhythmias and repolarization. Bradycardia is experienced is due
to the damage of the parasympathetic nerve located in the pancreas. Total bilirubin is
elevated, it’s caused by gallstones obstructing the flow of bile in the bile duct (Smotkin &
Tenner, 2012). Lipase enzyme is also elevated. Lipase is an enzyme produced by the
pancreas and helps digest fat in the bodies. High levels of lipase mostly signify that there is
an inflammation of the pancreas.
Medication
Management of clients with acute pancreatitis is aimed at relieving symptoms and prevent
any complication from happening. All oral medication are prohibited so as to prevent
pancreas from secreting a pancreatic enzyme (Roston & Jacobson, 2013). Clients with high
evidence bowel surgery on the right. The client has no bowel obstruction and lastly, there is no
identification of the appendix.
b. Pelvis
The urinary bladder is unremarkable, the presence of metal clips in the inguinal canal and
lastly no presence of adenopathy.
Lab findings
Upon admission, an EKG, liver function test, complete blood count, troponin level test and
electrolyte test was conducted and the following findings were noted. The white blood cell
count is higher than the normal range indicating a sign of infection (Moon & Cho, 2012). The
EKG shows that the client has sinus bradycardia of 55 beats per minute. Acute pancreatitis
normally associated with arrhythmias and repolarization. Bradycardia is experienced is due
to the damage of the parasympathetic nerve located in the pancreas. Total bilirubin is
elevated, it’s caused by gallstones obstructing the flow of bile in the bile duct (Smotkin &
Tenner, 2012). Lipase enzyme is also elevated. Lipase is an enzyme produced by the
pancreas and helps digest fat in the bodies. High levels of lipase mostly signify that there is
an inflammation of the pancreas.
Medication
Management of clients with acute pancreatitis is aimed at relieving symptoms and prevent
any complication from happening. All oral medication are prohibited so as to prevent
pancreas from secreting a pancreatic enzyme (Roston & Jacobson, 2013). Clients with high
9
metabolic stress are given parenteral nutrition. Nasogastric sanction is used to prevent nausea
and vomiting, remove excess hydrochloric acid to prevent it from entering the duodenum,
and reduce paralytic ileus and painful abdominal distension. Ranitidine and cimetidine are
prescribed to reduce hydrochloric acid secretion. Morphine and its derivatives are mostly
avoided in pain management since they are known to cause spasm of the sphincter of Oddi.
Antiemetic’s drugs are also administered to prevent vomiting. Antibiotics agents are given to
reduce the infection (Cohen, Slezac, & Wells, 2012).
Treatment
Surgical intervention includes positioning of biliary drains in the pancreatic duct through
the process called endoscopy. This is done to reduce pain and increase weight gain.
Diagnostic laparotomy is done to check pancreatic drainage and to remove the necrotized
pancreas. Follow-up care includes CT scans and X-rays (Johnson & Levy, 2012).
Psychosocial subsystem
Psychosocial covers
Psychosocial covers social, emotional and spiritual health. The best approach of
improving the psychosocial wellbeing is to learn on the management of conflict with others.
Mr. X is a good listener and respects an individual’s viewpoint, he is cautious on the tone
when speaking and lastly he accepts unfair judgment from other people, admits feelings and
focuses on current issues.
Spiritual subsystem
metabolic stress are given parenteral nutrition. Nasogastric sanction is used to prevent nausea
and vomiting, remove excess hydrochloric acid to prevent it from entering the duodenum,
and reduce paralytic ileus and painful abdominal distension. Ranitidine and cimetidine are
prescribed to reduce hydrochloric acid secretion. Morphine and its derivatives are mostly
avoided in pain management since they are known to cause spasm of the sphincter of Oddi.
Antiemetic’s drugs are also administered to prevent vomiting. Antibiotics agents are given to
reduce the infection (Cohen, Slezac, & Wells, 2012).
Treatment
Surgical intervention includes positioning of biliary drains in the pancreatic duct through
the process called endoscopy. This is done to reduce pain and increase weight gain.
Diagnostic laparotomy is done to check pancreatic drainage and to remove the necrotized
pancreas. Follow-up care includes CT scans and X-rays (Johnson & Levy, 2012).
Psychosocial subsystem
Psychosocial covers
Psychosocial covers social, emotional and spiritual health. The best approach of
improving the psychosocial wellbeing is to learn on the management of conflict with others.
Mr. X is a good listener and respects an individual’s viewpoint, he is cautious on the tone
when speaking and lastly he accepts unfair judgment from other people, admits feelings and
focuses on current issues.
Spiritual subsystem
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
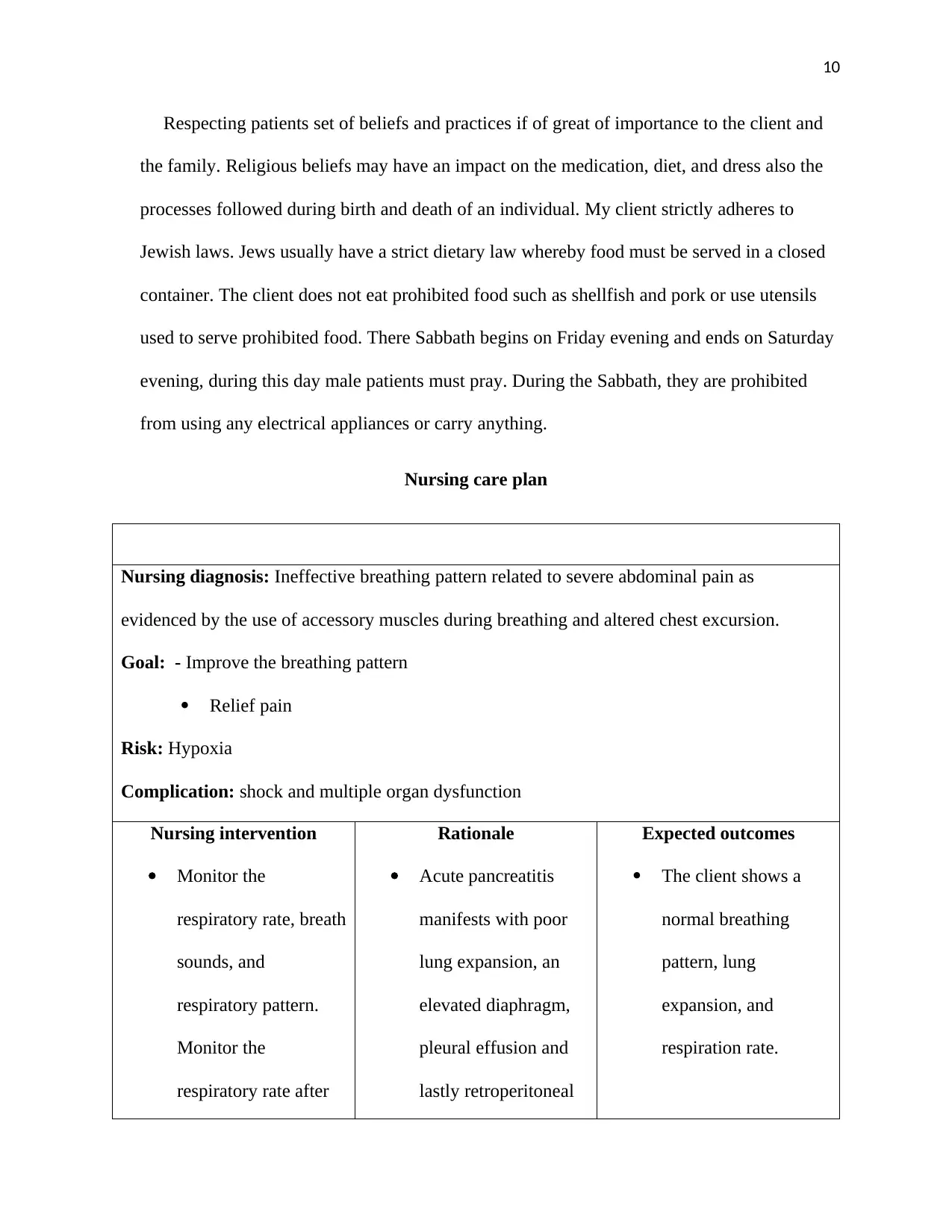
Respecting patients set of beliefs and practices if of great of importance to the client and
the family. Religious beliefs may have an impact on the medication, diet, and dress also the
processes followed during birth and death of an individual. My client strictly adheres to
Jewish laws. Jews usually have a strict dietary law whereby food must be served in a closed
container. The client does not eat prohibited food such as shellfish and pork or use utensils
used to serve prohibited food. There Sabbath begins on Friday evening and ends on Saturday
evening, during this day male patients must pray. During the Sabbath, they are prohibited
from using any electrical appliances or carry anything.
Nursing care plan
Nursing diagnosis: Ineffective breathing pattern related to severe abdominal pain as
evidenced by the use of accessory muscles during breathing and altered chest excursion.
Goal: - Improve the breathing pattern
Relief pain
Risk: Hypoxia
Complication: shock and multiple organ dysfunction
Nursing intervention
Monitor the
respiratory rate, breath
sounds, and
respiratory pattern.
Monitor the
respiratory rate after
Rationale
Acute pancreatitis
manifests with poor
lung expansion, an
elevated diaphragm,
pleural effusion and
lastly retroperitoneal
Expected outcomes
The client shows a
normal breathing
pattern, lung
expansion, and
respiration rate.
Respecting patients set of beliefs and practices if of great of importance to the client and
the family. Religious beliefs may have an impact on the medication, diet, and dress also the
processes followed during birth and death of an individual. My client strictly adheres to
Jewish laws. Jews usually have a strict dietary law whereby food must be served in a closed
container. The client does not eat prohibited food such as shellfish and pork or use utensils
used to serve prohibited food. There Sabbath begins on Friday evening and ends on Saturday
evening, during this day male patients must pray. During the Sabbath, they are prohibited
from using any electrical appliances or carry anything.
Nursing care plan
Nursing diagnosis: Ineffective breathing pattern related to severe abdominal pain as
evidenced by the use of accessory muscles during breathing and altered chest excursion.
Goal: - Improve the breathing pattern
Relief pain
Risk: Hypoxia
Complication: shock and multiple organ dysfunction
Nursing intervention
Monitor the
respiratory rate, breath
sounds, and
respiratory pattern.
Monitor the
respiratory rate after
Rationale
Acute pancreatitis
manifests with poor
lung expansion, an
elevated diaphragm,
pleural effusion and
lastly retroperitoneal
Expected outcomes
The client shows a
normal breathing
pattern, lung
expansion, and
respiration rate.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
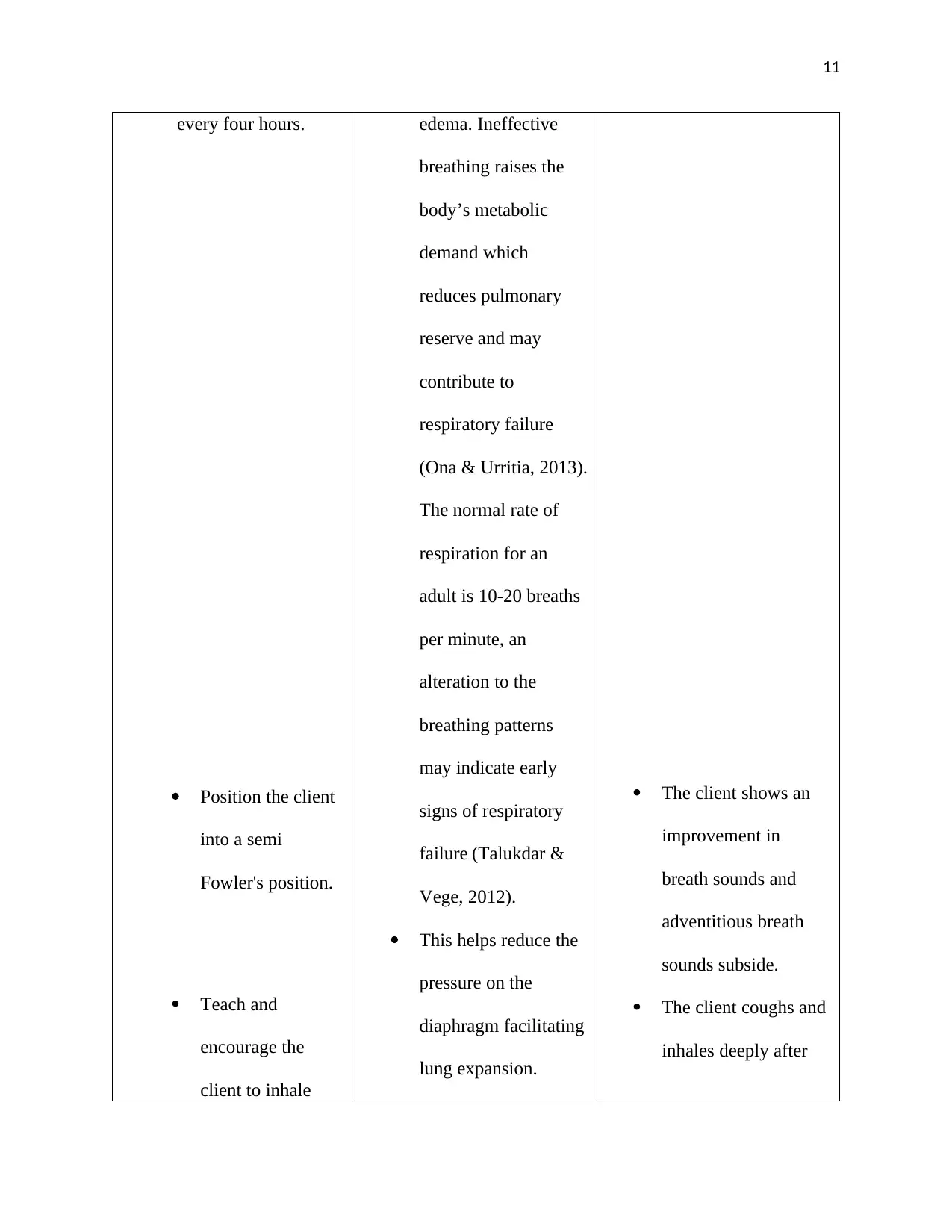
every four hours.
Position the client
into a semi
Fowler's position.
Teach and
encourage the
client to inhale
edema. Ineffective
breathing raises the
body’s metabolic
demand which
reduces pulmonary
reserve and may
contribute to
respiratory failure
(Ona & Urritia, 2013).
The normal rate of
respiration for an
adult is 10-20 breaths
per minute, an
alteration to the
breathing patterns
may indicate early
signs of respiratory
failure (Talukdar &
Vege, 2012).
This helps reduce the
pressure on the
diaphragm facilitating
lung expansion.
The client shows an
improvement in
breath sounds and
adventitious breath
sounds subside.
The client coughs and
inhales deeply after
every four hours.
Position the client
into a semi
Fowler's position.
Teach and
encourage the
client to inhale
edema. Ineffective
breathing raises the
body’s metabolic
demand which
reduces pulmonary
reserve and may
contribute to
respiratory failure
(Ona & Urritia, 2013).
The normal rate of
respiration for an
adult is 10-20 breaths
per minute, an
alteration to the
breathing patterns
may indicate early
signs of respiratory
failure (Talukdar &
Vege, 2012).
This helps reduce the
pressure on the
diaphragm facilitating
lung expansion.
The client shows an
improvement in
breath sounds and
adventitious breath
sounds subside.
The client coughs and
inhales deeply after
12
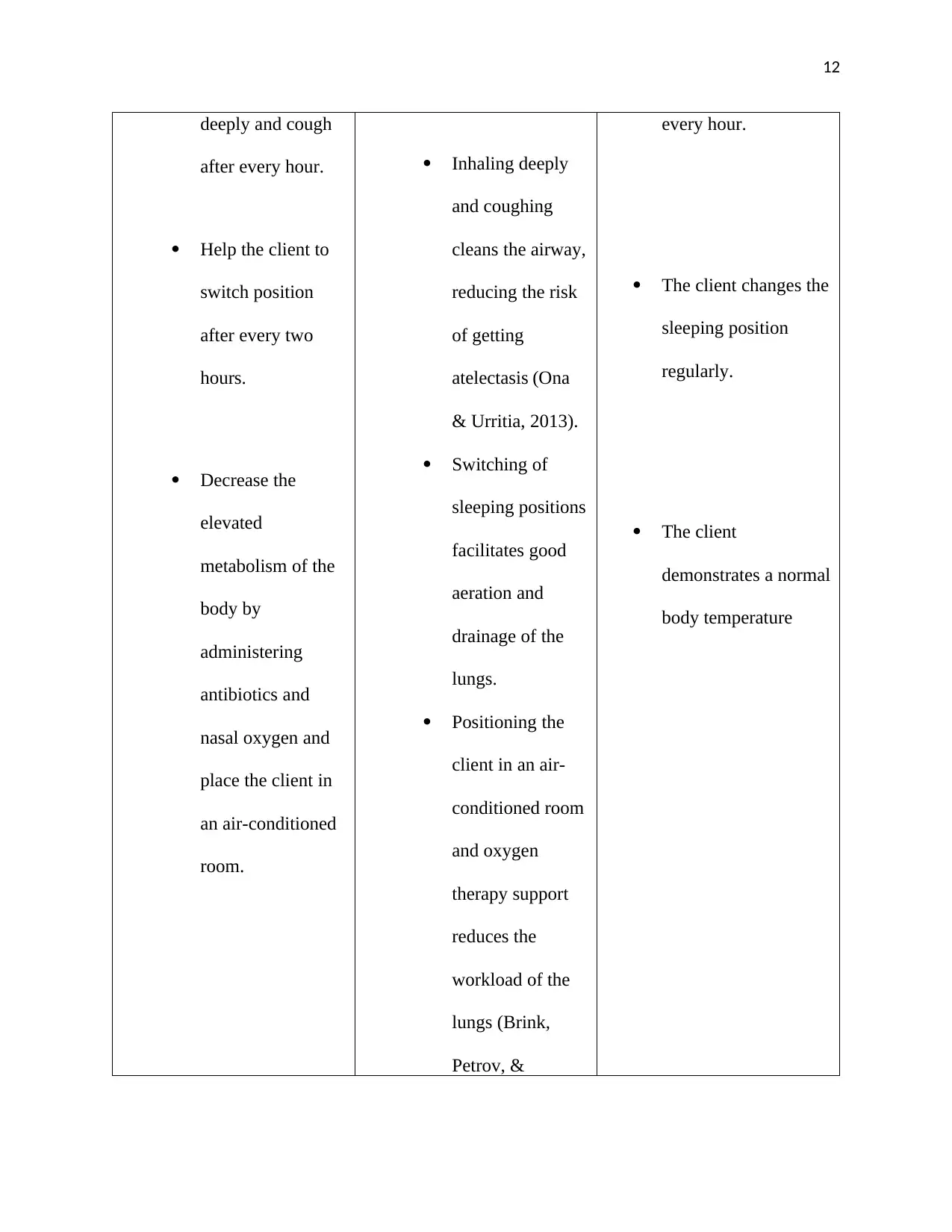
deeply and cough
after every hour.
Help the client to
switch position
after every two
hours.
Decrease the
elevated
metabolism of the
body by
administering
antibiotics and
nasal oxygen and
place the client in
an air-conditioned
room.
Inhaling deeply
and coughing
cleans the airway,
reducing the risk
of getting
atelectasis (Ona
& Urritia, 2013).
Switching of
sleeping positions
facilitates good
aeration and
drainage of the
lungs.
Positioning the
client in an air-
conditioned room
and oxygen
therapy support
reduces the
workload of the
lungs (Brink,
Petrov, &
every hour.
The client changes the
sleeping position
regularly.
The client
demonstrates a normal
body temperature
deeply and cough
after every hour.
Help the client to
switch position
after every two
hours.
Decrease the
elevated
metabolism of the
body by
administering
antibiotics and
nasal oxygen and
place the client in
an air-conditioned
room.
Inhaling deeply
and coughing
cleans the airway,
reducing the risk
of getting
atelectasis (Ona
& Urritia, 2013).
Switching of
sleeping positions
facilitates good
aeration and
drainage of the
lungs.
Positioning the
client in an air-
conditioned room
and oxygen
therapy support
reduces the
workload of the
lungs (Brink,
Petrov, &
every hour.
The client changes the
sleeping position
regularly.
The client
demonstrates a normal
body temperature
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.