Exploring Pathophysiology and Nursing Care for Acute Severe Asthma
VerifiedAdded on 2023/06/04
|9
|2116
|88
Case Study
AI Summary
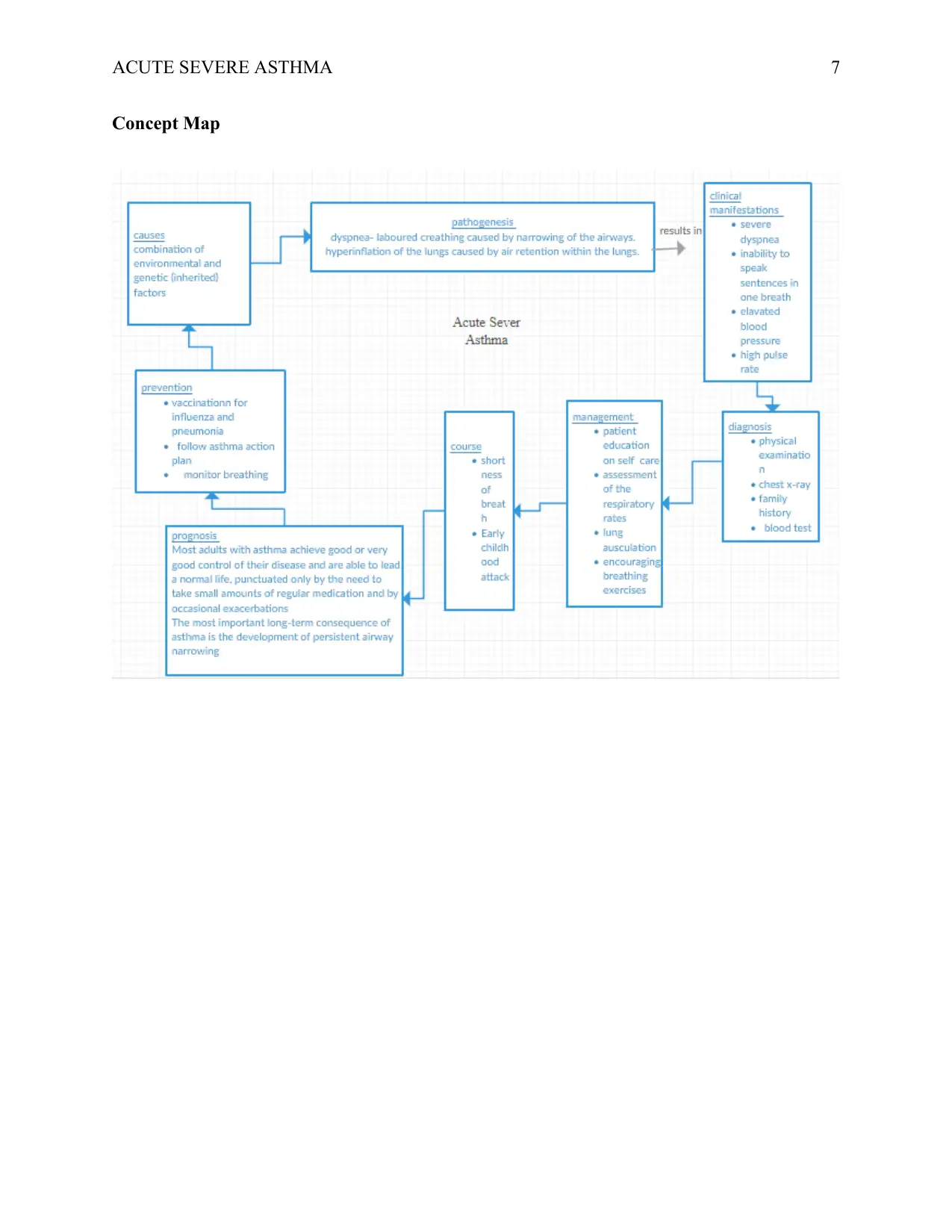
This case study provides a comprehensive analysis of acute severe asthma, focusing on its pathogenesis, clinical manifestations, and nursing management. It begins by explaining the underlying causes and mechanisms of asthma, particularly in the context of Jackson Smith's case, highlighting factors like early onset, environmental triggers, and physiological responses such as airway narrowing, mucus production, and reduced oxygen saturation. The study then delves into specific clinical observations, including dyspnea, increased respiratory rate, elevated blood pressure, tachycardia, and abnormal blood gas values, linking these to the pathophysiology of the condition. Furthermore, the case study outlines key nursing strategies, such as addressing ineffective airway clearance and promoting health-seeking behaviors related to asthma prevention, detailing specific interventions and their rationales. Finally, it discusses the mechanism of action and nursing implications of commonly used drugs like nebulized salbutamol, ipratropium bromide, and IV hydrocortisone, emphasizing the importance of patient education and monitoring for adverse effects. The case study concludes with a concept map visually summarizing the key aspects of acute severe asthma.

1 out of 9
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.