Alternatives to Home Care: Legislative Framework and Team Competencies
VerifiedAdded on 2023/06/15
|9
|2722
|418
Report
AI Summary
This report provides an in-depth analysis of alternative care services for individuals with intellectual disabilities in Ireland, emphasizing the shift towards community-based care and the evolving role of public care services. It highlights the demographic need for structured support, referencing statistics on the population requiring intellectual disability support and relevant government policies like 'Towards 2016' and the National Disability Strategy. The report examines the mix of public and private care structures, the reliance on unpaid care, and the preference for home-based support among the elderly. It also addresses the limitations of community-based services and the legislative framework supporting disability care, including the Disability Act 2005 and the National Housing Strategy. Furthermore, the report includes a reflection on teamwork competencies using the UNSTAR model, discussing communication, problem-solving, and the challenges faced in healthcare teams.

Running head: ALTERNATIVE TO HOME CARE
Alternative to home care
Name of the student
University name
Authors’ note
Alternative to home care
Name of the student
University name
Authors’ note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
ALTERNATIVE TO HOME CARE
Table of Contents
Discussion of current home care provision................................................................................2
Legislative framework and policy provision..............................................................................3
Reflection on team work competencies (UNSTAR model).......................................................4
References..................................................................................................................................7
ALTERNATIVE TO HOME CARE
Table of Contents
Discussion of current home care provision................................................................................2
Legislative framework and policy provision..............................................................................3
Reflection on team work competencies (UNSTAR model).......................................................4
References..................................................................................................................................7
2
ALTERNATIVE TO HOME CARE
Discussion of current home care provision
The current study discusses the aspect of care services for the ones with intellectual
disabilities in Ireland. It is believed that family based or community based care is the best
suited approach for care in Ireland (Murphy et al. 2015). Therefore, public care services are
only thought to be convenient options in case the community based care services are not
available. Additionally, for longer periods of time the responsibility of care for the
intellectually challenged or less able was shifted on the shoulders of the women in the family
who continued to do it for free (Taggart et al. 2012). However, amidst the changing
circumstances the government has made major changes within some of the healthcare
policies in order to accommodate advanced care for the ones with cognitive impairment.
The need for a more structured public care services could be explained with the help
of few of important figures and statistics. As per the estimates from the year 2006, there were
113,000 people aged between 12-55 years who were possessing some kind of intellectual
disabilities and needed support (Colomer and de Vries 2016). In order to support the mentally
less able the government formulated a number of effective policies and programs. This could
further help in restoring the autonomy they could have in making choices regarding the kind
of support services they would want to receive. The intellectual disabilities could be
attributed to the presence of a number of conditions such developmental delay, fragile X
syndrome and Down’s syndrome (Millar et al. 2015).
The Irish support care consists of a mixture of public and private care structures. A
large portion of supportive care is provided by private market based services. The Irish
healthcare relies heavily on women and most of it is unpaid care (Simplican et al. 2015).
Majority of the care services are attended by general medical practitioners within their homes
rather than specialised care services at hospitals. As commented by McMahon et al. (2017),
extended form of care is provided by some of the healthcare organizations such as providing
‘meal on wheels’ for the ones with limited capacitates. Reports and figures have also
suggested that two-thirds within the elderly population of Ireland had functional disability
and would prefer to receive support care within the comfort of their homes (Chadwick et al.
2013). However, most of the times the ones with cognitive disabilities are left alone at home
by their respective family members who often need to travel out of the country due to work
purpose. Additionally, the community based voluntary care services are not comprehensive in
ALTERNATIVE TO HOME CARE
Discussion of current home care provision
The current study discusses the aspect of care services for the ones with intellectual
disabilities in Ireland. It is believed that family based or community based care is the best
suited approach for care in Ireland (Murphy et al. 2015). Therefore, public care services are
only thought to be convenient options in case the community based care services are not
available. Additionally, for longer periods of time the responsibility of care for the
intellectually challenged or less able was shifted on the shoulders of the women in the family
who continued to do it for free (Taggart et al. 2012). However, amidst the changing
circumstances the government has made major changes within some of the healthcare
policies in order to accommodate advanced care for the ones with cognitive impairment.
The need for a more structured public care services could be explained with the help
of few of important figures and statistics. As per the estimates from the year 2006, there were
113,000 people aged between 12-55 years who were possessing some kind of intellectual
disabilities and needed support (Colomer and de Vries 2016). In order to support the mentally
less able the government formulated a number of effective policies and programs. This could
further help in restoring the autonomy they could have in making choices regarding the kind
of support services they would want to receive. The intellectual disabilities could be
attributed to the presence of a number of conditions such developmental delay, fragile X
syndrome and Down’s syndrome (Millar et al. 2015).
The Irish support care consists of a mixture of public and private care structures. A
large portion of supportive care is provided by private market based services. The Irish
healthcare relies heavily on women and most of it is unpaid care (Simplican et al. 2015).
Majority of the care services are attended by general medical practitioners within their homes
rather than specialised care services at hospitals. As commented by McMahon et al. (2017),
extended form of care is provided by some of the healthcare organizations such as providing
‘meal on wheels’ for the ones with limited capacitates. Reports and figures have also
suggested that two-thirds within the elderly population of Ireland had functional disability
and would prefer to receive support care within the comfort of their homes (Chadwick et al.
2013). However, most of the times the ones with cognitive disabilities are left alone at home
by their respective family members who often need to travel out of the country due to work
purpose. Additionally, the community based voluntary care services are not comprehensive in
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
ALTERNATIVE TO HOME CARE
its approach and design and therefore lack the basic skills for the delivery of specialised
health support services (Doody 2012). As per the breakdown of residential accommodation,
in 61% of the cases the family members of the ones with intellectual disabilities would prefer
privatized care services over public support services. As mentioned by Murphy et al. (2015),
lack of sufficient infrastructure and less availability of finances deteriorated the quality of
mental health care services offered by the Ireland based public health care organizations.
Legislative framework and policy provision
There are a number of policies and legal framework underlining the care of the disabled
population in Ireland. One such framework which could be discussed over here is ‘Towards
2016; Ten -Year Framework Social Partnership Agreement 2006-2015’. Some of the
objectives outlined in the Towards 2016 framework are to provide the individuals with
intellectual disability the chance to live an independent and autonomous life (Ali et al. 2012).
This was to ensure that they are able to make their decisions without depending on others
from support. Additionally, the National Disability Strategy (NDS), 2004, was introduced
with the aim of improving the participation of people with disabilities within the society. The
main legislative structure supporting the policy is the Disability Act, 2005, which focuses
upon making such disability services as a part of the mainstream (McCarron et al. 2013).
Under this act the people with disabilities were entitled to a number of services such as:
Having their health needs accessed
Accessing of individual complaints and appeals
The department of justice and equality has been working together for the integration of
the National Disability Strategy and the UN convention on the Rights of People with
disabilities (inclusionireland.ie 2018). Additionally, the Equal Status Act 2000 and 2004
promote equality and prohibit discrimination against people with discrimination. One of the
most important legislation which was drawn in this favour was the National Housing Strategy
for people with a disability, 2011-2016. Most people in Ireland with intellectual disabilities
have their services delivered by one organization only (Ryan et al. 2014). These include
accommodation needs, medical and social services. The service providers receive funding
from the HSE to look after the various needs of a disabled person (Coppus 2013). In this
respect, a person is assigned a particular service provider from the very beginning leaving
them with very few options for change. As argued by McGlinchey et al. (2013), this
ALTERNATIVE TO HOME CARE
its approach and design and therefore lack the basic skills for the delivery of specialised
health support services (Doody 2012). As per the breakdown of residential accommodation,
in 61% of the cases the family members of the ones with intellectual disabilities would prefer
privatized care services over public support services. As mentioned by Murphy et al. (2015),
lack of sufficient infrastructure and less availability of finances deteriorated the quality of
mental health care services offered by the Ireland based public health care organizations.
Legislative framework and policy provision
There are a number of policies and legal framework underlining the care of the disabled
population in Ireland. One such framework which could be discussed over here is ‘Towards
2016; Ten -Year Framework Social Partnership Agreement 2006-2015’. Some of the
objectives outlined in the Towards 2016 framework are to provide the individuals with
intellectual disability the chance to live an independent and autonomous life (Ali et al. 2012).
This was to ensure that they are able to make their decisions without depending on others
from support. Additionally, the National Disability Strategy (NDS), 2004, was introduced
with the aim of improving the participation of people with disabilities within the society. The
main legislative structure supporting the policy is the Disability Act, 2005, which focuses
upon making such disability services as a part of the mainstream (McCarron et al. 2013).
Under this act the people with disabilities were entitled to a number of services such as:
Having their health needs accessed
Accessing of individual complaints and appeals
The department of justice and equality has been working together for the integration of
the National Disability Strategy and the UN convention on the Rights of People with
disabilities (inclusionireland.ie 2018). Additionally, the Equal Status Act 2000 and 2004
promote equality and prohibit discrimination against people with discrimination. One of the
most important legislation which was drawn in this favour was the National Housing Strategy
for people with a disability, 2011-2016. Most people in Ireland with intellectual disabilities
have their services delivered by one organization only (Ryan et al. 2014). These include
accommodation needs, medical and social services. The service providers receive funding
from the HSE to look after the various needs of a disabled person (Coppus 2013). In this
respect, a person is assigned a particular service provider from the very beginning leaving
them with very few options for change. As argued by McGlinchey et al. (2013), this
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
ALTERNATIVE TO HOME CARE
provides the disabled population with intellectual disabilities little or no option to excise their
personal choice in the selection of care provider. As per new regulation, people with
disability regardless of their housing situation were to be considered for allotment of new
housing options under the residential care scheme (Iacono et al. 2013).
Reflection on team work competencies (UNSTAR model)
Team work is one of the most important attributes of health care and support. A well
coordinated team ensures that effective flow of services is maintained for the maximum
welfare of the patient and their respective families. Therefore, undertaking group project and
presentation can help me develop teamwork skills and competencies. Working as a part of
team and taking part in combined projects requires a number of key skills and competencies.
Some of these are communication skills, problem solving skills, listening and feedback skills.
The amalgamation and optimization of such skills can make a team strong. However, as
supported by García Iriarte et al. (2014), individual contribution is necessary for the success
of the entire or the whole team in a care setup. Therefore, working as a part of a team in an
aged care set up helped me in developing my communication as well as problem solving
skills. It was required that I communicate actively across the team in order to understand the
different requirements of the care process delivery. One of the manner in which the team
communication aspect could be supported is by active note taking. Note taking and roster
formation are some of the habits which can help me prevent the occurrence of an untoward
incident within a care set up. Additionally, participating in group presentations has helped
me develop my analytical skills further. The sharing of feedback during preparation of group
presentation helped me develop my creative thinking skills.
Additionally, practising of active listening approaches can help me relate better with
the grievances faced by the patients as well as understand my tasks well during the team
briefing sessions. In addition, dealing with patients with intellectual disabilities often results
in situations where the patient may be showing challenging behaviour. As commented by
Amado et al. (2013), practising therapeutic communication approaches with patients with
cognitive disabilities can help me in understanding the issues faced by them. However, I
have also faced a number of challenges working as part of a team. Some of these were
regarding communication issues faced due to language mismatch. In this respect, some of my
co-workers within the healthcare team were from different nationalities, which resulted in a
communication gap. I often felt that lack of support from a supervisor also result in service
ALTERNATIVE TO HOME CARE
provides the disabled population with intellectual disabilities little or no option to excise their
personal choice in the selection of care provider. As per new regulation, people with
disability regardless of their housing situation were to be considered for allotment of new
housing options under the residential care scheme (Iacono et al. 2013).
Reflection on team work competencies (UNSTAR model)
Team work is one of the most important attributes of health care and support. A well
coordinated team ensures that effective flow of services is maintained for the maximum
welfare of the patient and their respective families. Therefore, undertaking group project and
presentation can help me develop teamwork skills and competencies. Working as a part of
team and taking part in combined projects requires a number of key skills and competencies.
Some of these are communication skills, problem solving skills, listening and feedback skills.
The amalgamation and optimization of such skills can make a team strong. However, as
supported by García Iriarte et al. (2014), individual contribution is necessary for the success
of the entire or the whole team in a care setup. Therefore, working as a part of a team in an
aged care set up helped me in developing my communication as well as problem solving
skills. It was required that I communicate actively across the team in order to understand the
different requirements of the care process delivery. One of the manner in which the team
communication aspect could be supported is by active note taking. Note taking and roster
formation are some of the habits which can help me prevent the occurrence of an untoward
incident within a care set up. Additionally, participating in group presentations has helped
me develop my analytical skills further. The sharing of feedback during preparation of group
presentation helped me develop my creative thinking skills.
Additionally, practising of active listening approaches can help me relate better with
the grievances faced by the patients as well as understand my tasks well during the team
briefing sessions. In addition, dealing with patients with intellectual disabilities often results
in situations where the patient may be showing challenging behaviour. As commented by
Amado et al. (2013), practising therapeutic communication approaches with patients with
cognitive disabilities can help me in understanding the issues faced by them. However, I
have also faced a number of challenges working as part of a team. Some of these were
regarding communication issues faced due to language mismatch. In this respect, some of my
co-workers within the healthcare team were from different nationalities, which resulted in a
communication gap. I often felt that lack of support from a supervisor also result in service
5
ALTERNATIVE TO HOME CARE
gaps. As commented by Iacono et al. (2014), a number of ethical barriers are faced when
dealing with old age group patients with intellectual disabilities admitted in hospitals.
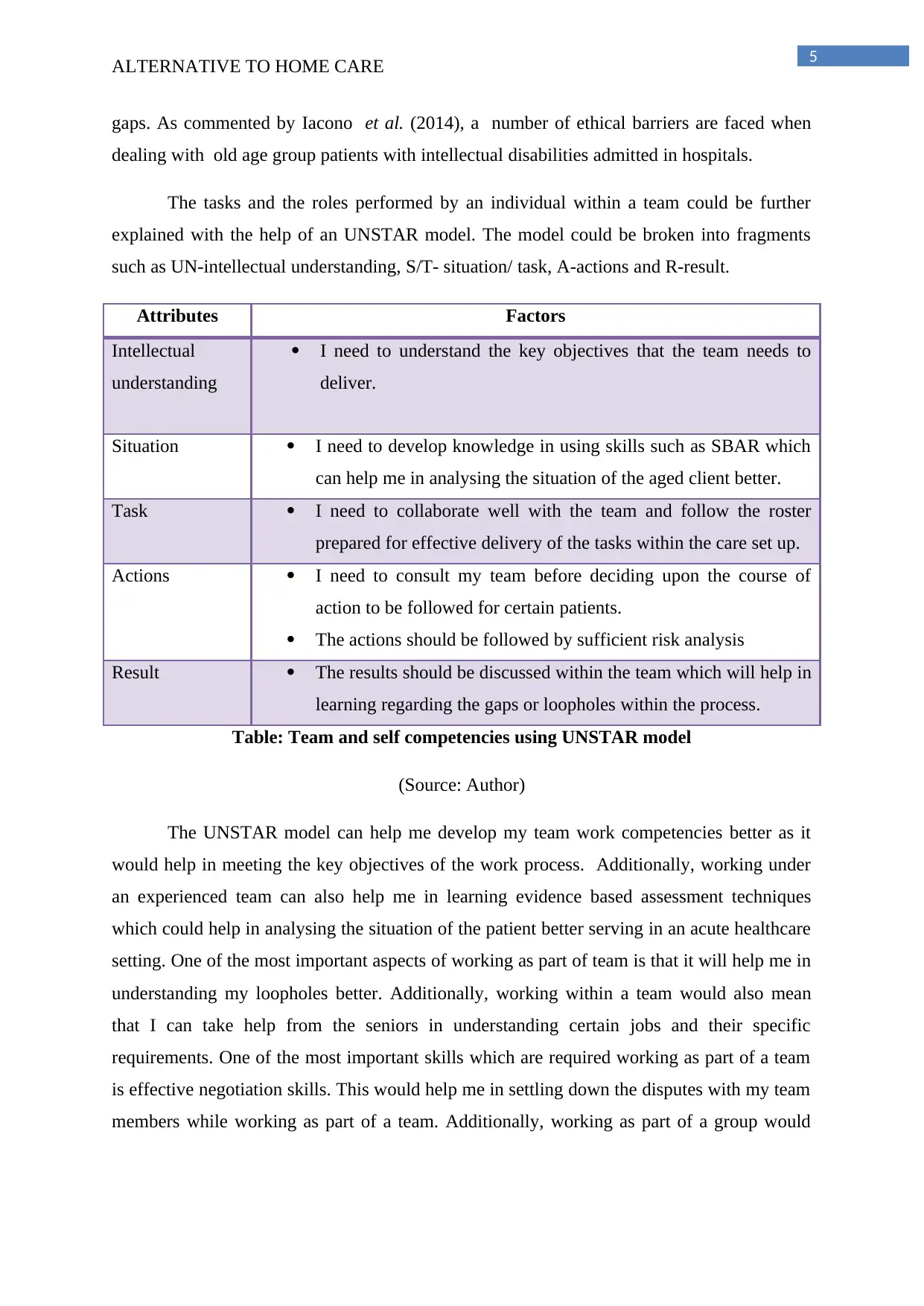
The tasks and the roles performed by an individual within a team could be further
explained with the help of an UNSTAR model. The model could be broken into fragments
such as UN-intellectual understanding, S/T- situation/ task, A-actions and R-result.
Attributes Factors
Intellectual
understanding
I need to understand the key objectives that the team needs to
deliver.
Situation I need to develop knowledge in using skills such as SBAR which
can help me in analysing the situation of the aged client better.
Task I need to collaborate well with the team and follow the roster
prepared for effective delivery of the tasks within the care set up.
Actions I need to consult my team before deciding upon the course of
action to be followed for certain patients.
The actions should be followed by sufficient risk analysis
Result The results should be discussed within the team which will help in
learning regarding the gaps or loopholes within the process.
Table: Team and self competencies using UNSTAR model
(Source: Author)
The UNSTAR model can help me develop my team work competencies better as it
would help in meeting the key objectives of the work process. Additionally, working under
an experienced team can also help me in learning evidence based assessment techniques
which could help in analysing the situation of the patient better serving in an acute healthcare
setting. One of the most important aspects of working as part of team is that it will help me in
understanding my loopholes better. Additionally, working within a team would also mean
that I can take help from the seniors in understanding certain jobs and their specific
requirements. One of the most important skills which are required working as part of a team
is effective negotiation skills. This would help me in settling down the disputes with my team
members while working as part of a team. Additionally, working as part of a group would
ALTERNATIVE TO HOME CARE
gaps. As commented by Iacono et al. (2014), a number of ethical barriers are faced when
dealing with old age group patients with intellectual disabilities admitted in hospitals.
The tasks and the roles performed by an individual within a team could be further
explained with the help of an UNSTAR model. The model could be broken into fragments
such as UN-intellectual understanding, S/T- situation/ task, A-actions and R-result.
Attributes Factors
Intellectual
understanding
I need to understand the key objectives that the team needs to
deliver.
Situation I need to develop knowledge in using skills such as SBAR which
can help me in analysing the situation of the aged client better.
Task I need to collaborate well with the team and follow the roster
prepared for effective delivery of the tasks within the care set up.
Actions I need to consult my team before deciding upon the course of
action to be followed for certain patients.
The actions should be followed by sufficient risk analysis
Result The results should be discussed within the team which will help in
learning regarding the gaps or loopholes within the process.
Table: Team and self competencies using UNSTAR model
(Source: Author)
The UNSTAR model can help me develop my team work competencies better as it
would help in meeting the key objectives of the work process. Additionally, working under
an experienced team can also help me in learning evidence based assessment techniques
which could help in analysing the situation of the patient better serving in an acute healthcare
setting. One of the most important aspects of working as part of team is that it will help me in
understanding my loopholes better. Additionally, working within a team would also mean
that I can take help from the seniors in understanding certain jobs and their specific
requirements. One of the most important skills which are required working as part of a team
is effective negotiation skills. This would help me in settling down the disputes with my team
members while working as part of a team. Additionally, working as part of a group would
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

6
ALTERNATIVE TO HOME CARE
also help me develop better problem solving approach which will help me deal with future
challenges affectively.
ALTERNATIVE TO HOME CARE
also help me develop better problem solving approach which will help me deal with future
challenges affectively.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
ALTERNATIVE TO HOME CARE
References
Ali, A., Hassiotis, A., Strydom, A. and King, M., 2012. Self stigma in people with intellectual
disabilities and courtesy stigma in family carers: A systematic review. Research in
developmental disabilities, 33(6), pp.2122-2140.
Amado, A.N., Stancliffe, R.J., McCarron, M. and McCallion, P., 2013. Social inclusion and
community participation of individuals with intellectual/developmental
disabilities. Intellectual and developmental disabilities, 51(5), pp.360-375.
Chadwick, D.D., Mannan, H., Garcia Iriarte, E., McConkey, R., O'brien, P., Finlay, F.,
Lawlor, A. and Harrington, G., 2013. Family voices: life for family carers of people with
intellectual disabilities in Ireland. Journal of Applied Research in Intellectual
Disabilities, 26(2), pp.119-132.
Colomer, J. and de Vries, J., 2016. Person-centred dementia care: a reality check in two
nursing homes in Ireland. Dementia, 15(5), pp.1158-1170.
Coppus, A.M.W., 2013. People with intellectual disability: What do we know about
adulthood and life expectancy?. Developmental disabilities research reviews, 18(1), pp.6-16.
Doody, O., 2012. Families’ views on their relatives with intellectual disability moving from a
long‐stay psychiatric institution to a community‐based intellectual disability service: an Irish
context. British Journal of Learning Disabilities, 40(1), pp.46-54.
García Iriarte, E., O'brien, P., McConkey, R., Wolfe, M. and O'doherty, S., 2014. Identifying
the key concerns of Irish persons with intellectual disability. Journal of Applied Research in
Intellectual Disabilities, 27(6), pp.564-575.
Iacono, T., Bigby, C., Unsworth, C., Douglas, J. and Fitzpatrick, P., 2014. A systematic
review of hospital experiences of people with intellectual disability. BMC health services
research, 14(1), p.505.
inclusionireland.ie (2018), inclusionireland.ie , Available at :
https://www.inclusionireland.ie/sites/default/files/documents/position_paper_on_implementin
g_the_nds_ [Accessed on 25 Feb. 2018]
ALTERNATIVE TO HOME CARE
References
Ali, A., Hassiotis, A., Strydom, A. and King, M., 2012. Self stigma in people with intellectual
disabilities and courtesy stigma in family carers: A systematic review. Research in
developmental disabilities, 33(6), pp.2122-2140.
Amado, A.N., Stancliffe, R.J., McCarron, M. and McCallion, P., 2013. Social inclusion and
community participation of individuals with intellectual/developmental
disabilities. Intellectual and developmental disabilities, 51(5), pp.360-375.
Chadwick, D.D., Mannan, H., Garcia Iriarte, E., McConkey, R., O'brien, P., Finlay, F.,
Lawlor, A. and Harrington, G., 2013. Family voices: life for family carers of people with
intellectual disabilities in Ireland. Journal of Applied Research in Intellectual
Disabilities, 26(2), pp.119-132.
Colomer, J. and de Vries, J., 2016. Person-centred dementia care: a reality check in two
nursing homes in Ireland. Dementia, 15(5), pp.1158-1170.
Coppus, A.M.W., 2013. People with intellectual disability: What do we know about
adulthood and life expectancy?. Developmental disabilities research reviews, 18(1), pp.6-16.
Doody, O., 2012. Families’ views on their relatives with intellectual disability moving from a
long‐stay psychiatric institution to a community‐based intellectual disability service: an Irish
context. British Journal of Learning Disabilities, 40(1), pp.46-54.
García Iriarte, E., O'brien, P., McConkey, R., Wolfe, M. and O'doherty, S., 2014. Identifying
the key concerns of Irish persons with intellectual disability. Journal of Applied Research in
Intellectual Disabilities, 27(6), pp.564-575.
Iacono, T., Bigby, C., Unsworth, C., Douglas, J. and Fitzpatrick, P., 2014. A systematic
review of hospital experiences of people with intellectual disability. BMC health services
research, 14(1), p.505.
inclusionireland.ie (2018), inclusionireland.ie , Available at :
https://www.inclusionireland.ie/sites/default/files/documents/position_paper_on_implementin
g_the_nds_ [Accessed on 25 Feb. 2018]
8
ALTERNATIVE TO HOME CARE
McCarron, M., Swinburne, J., Burke, E., McGlinchey, E., Carroll, R. and McCallion, P.,
2013. Patterns of multimorbidity in an older population of persons with an intellectual
disability: results from the intellectual disability supplement to the Irish longitudinal study on
aging (IDS-TILDA). Research in developmental disabilities, 34(1), pp.521-527.
McGlinchey, E., McCallion, P., Burke, E., Carroll, R. and McCarron, M., 2013. Exploring
the issue of employment for adults with an intellectual disability in Ireland. Journal of
Applied Research in Intellectual Disabilities, 26(4), pp.335-343.
McMahon, D.L., Twomey, M., O’Reilly, M. and Devins, M., 2017. Referrals to a perinatal
specialist palliative care consult service in Ireland, 2012–2015. Archives of Disease in
Childhood-Fetal and Neonatal Edition, pp.17.
Millar, A.N., Hughes, C.M. and Ryan, C., 2015. “It’s very complicated”: a qualitative study
of medicines management in intermediate care facilities in Northern Ireland. BMC health
services research, 15(1), p.216.
Murphy, C.M., Whelan, B.J. and Normand, C., 2015. Formal home‐care utilisation by older
adults in Ireland: evidence from the Irish Longitudinal Study on Ageing (TILDA). Health &
social care in the community, 23(4), pp.408-418.
Ryan, A., Taggart, L., Truesdale‐Kennedy, M. and Slevin, E., 2014. Issues in caregiving for
older people with intellectual disabilities and their ageing family carers: a review and
commentary. International journal of older people nursing, 9(3), pp.217-226.
Simplican, S.C., Leader, G., Kosciulek, J. and Leahy, M., 2015. Defining social inclusion of
people with intellectual and developmental disabilities: An ecological model of social
networks and community participation. Research in developmental disabilities, 38, pp.18-29.
Taggart, L., Truesdale-Kennedy, M., Ryan, A. and McConkey, R., 2012. Examining the
support needs of ageing family carers in developing future plans for a relative with an
intellectual disability. Journal of Intellectual Disabilities, 16(3), pp.217-234.
ALTERNATIVE TO HOME CARE
McCarron, M., Swinburne, J., Burke, E., McGlinchey, E., Carroll, R. and McCallion, P.,
2013. Patterns of multimorbidity in an older population of persons with an intellectual
disability: results from the intellectual disability supplement to the Irish longitudinal study on
aging (IDS-TILDA). Research in developmental disabilities, 34(1), pp.521-527.
McGlinchey, E., McCallion, P., Burke, E., Carroll, R. and McCarron, M., 2013. Exploring
the issue of employment for adults with an intellectual disability in Ireland. Journal of
Applied Research in Intellectual Disabilities, 26(4), pp.335-343.
McMahon, D.L., Twomey, M., O’Reilly, M. and Devins, M., 2017. Referrals to a perinatal
specialist palliative care consult service in Ireland, 2012–2015. Archives of Disease in
Childhood-Fetal and Neonatal Edition, pp.17.
Millar, A.N., Hughes, C.M. and Ryan, C., 2015. “It’s very complicated”: a qualitative study
of medicines management in intermediate care facilities in Northern Ireland. BMC health
services research, 15(1), p.216.
Murphy, C.M., Whelan, B.J. and Normand, C., 2015. Formal home‐care utilisation by older
adults in Ireland: evidence from the Irish Longitudinal Study on Ageing (TILDA). Health &
social care in the community, 23(4), pp.408-418.
Ryan, A., Taggart, L., Truesdale‐Kennedy, M. and Slevin, E., 2014. Issues in caregiving for
older people with intellectual disabilities and their ageing family carers: a review and
commentary. International journal of older people nursing, 9(3), pp.217-226.
Simplican, S.C., Leader, G., Kosciulek, J. and Leahy, M., 2015. Defining social inclusion of
people with intellectual and developmental disabilities: An ecological model of social
networks and community participation. Research in developmental disabilities, 38, pp.18-29.
Taggart, L., Truesdale-Kennedy, M., Ryan, A. and McConkey, R., 2012. Examining the
support needs of ageing family carers in developing future plans for a relative with an
intellectual disability. Journal of Intellectual Disabilities, 16(3), pp.217-234.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.