Alzheimer's Disease: A Comprehensive Report on Causes and Treatment
VerifiedAdded on 2021/05/31
|1
|808
|327
Report
AI Summary
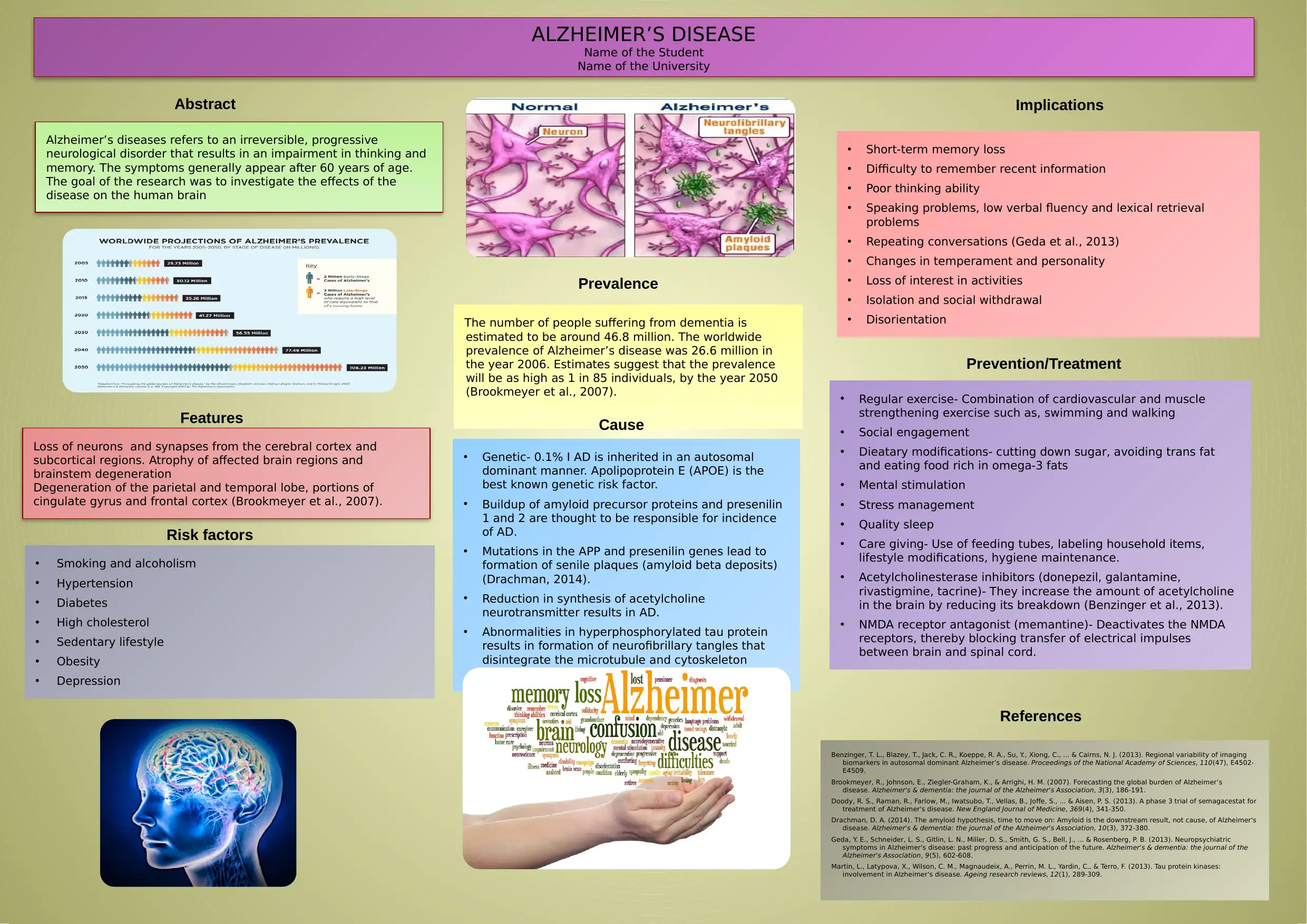
This report provides a comprehensive overview of Alzheimer's disease, an irreversible neurological disorder characterized by progressive impairment of thinking and memory, typically appearing after age 60. It delves into the disease's features, including short-term memory loss, poor thinking ability, and changes in temperament. The report explores the causes, such as genetic factors (APOE gene, mutations in APP and presenilin genes), neurotransmitter deficiencies (acetylcholine), and the formation of neurofibrillary tangles. It also discusses risk factors like smoking, alcoholism, hypertension, and lifestyle choices. Furthermore, the report highlights potential treatments and preventative measures, including acetylcholinesterase inhibitors, NMDA receptor antagonists, regular exercise, dietary modifications, mental stimulation, and caregiving strategies. The report also provides prevalence estimates and implications of the disease.
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.