Critical Analysis: Fourth National Mental Health Plan (2009-2014)
VerifiedAdded on 2023/06/15
|20
|5388
|486
Report
AI Summary
This report provides a detailed analysis of the Fourth National Mental Health Plan in Australia, utilizing the World Health Organization's Health Service Planning and Policy Toolkit. It examines the policy's objectives, including social inclusion, prevention, service access, quality improvement, and accountability, within the context of Australia's mental health landscape. The analysis covers the policy's background, significance, and the influences that shaped its objectives, highlighting the collaborative approach taken by the Australian government. The report further assesses the policy's strengths and areas for improvement, focusing on its impact on indigenous populations and the broader mental health service delivery across the country. Desklib is a platform where students can find a wide array of solved assignments and study resources.
Introduction
In Australia, mental illness is widespread and has significant impact on the social,
personal and economic levels. However, the rate of prevalence varies across the life-span
(Sunderland, Newby & Andrews, 2013). The National Mental Health Strategy has guided the
reforms in mental health in Australia since 1992. The First National Mental Health Plan
represented co-ordinated mental health reform(Commonwealth of Australia(CoA), 2009),
while the second and the third National Mental Health Plansidentified the importance of
cross-sectoral partnership between mental health and well-being while responding to the
complication of mental illness via an integrated service system (CoA, 2009). According to
National Mental Health Plan, mental illness of regarded as the most common and impactful
complication in the areas like oncology, strokes and myocardial infraction. The mental illness
associated with this complex disease affects the quality of life. The comprehensive
implementation of the objectives drafted by the first, second and third National Mental Health
Plan led to a significant change in the mental health condition in Australia (CoA, 2009). This
led to the growth in the state-territory of mental health workforce along with increase in the
quality of the community based service. The Fourth National Mental Health Plan
acknowledges that there is still much to be done in the mental health sector in Australia.
According to the National Survey of Mental Health and Wellbeing (2007), conducted by the
Australian Bureau of Statistics (ABS), there is a major disparity in the mental health
condition and available treatment amongst the states and the territories. Only one-third of the
population sufferingfrom mental illness avail mental health services each year. The main
victims of mental illness are early adult population and common mental illnesses are anxiety
and mood disorders. There is also a high demand formental health care in acute and
In Australia, mental illness is widespread and has significant impact on the social,
personal and economic levels. However, the rate of prevalence varies across the life-span
(Sunderland, Newby & Andrews, 2013). The National Mental Health Strategy has guided the
reforms in mental health in Australia since 1992. The First National Mental Health Plan
represented co-ordinated mental health reform(Commonwealth of Australia(CoA), 2009),
while the second and the third National Mental Health Plansidentified the importance of
cross-sectoral partnership between mental health and well-being while responding to the
complication of mental illness via an integrated service system (CoA, 2009). According to
National Mental Health Plan, mental illness of regarded as the most common and impactful
complication in the areas like oncology, strokes and myocardial infraction. The mental illness
associated with this complex disease affects the quality of life. The comprehensive
implementation of the objectives drafted by the first, second and third National Mental Health
Plan led to a significant change in the mental health condition in Australia (CoA, 2009). This
led to the growth in the state-territory of mental health workforce along with increase in the
quality of the community based service. The Fourth National Mental Health Plan
acknowledges that there is still much to be done in the mental health sector in Australia.
According to the National Survey of Mental Health and Wellbeing (2007), conducted by the
Australian Bureau of Statistics (ABS), there is a major disparity in the mental health
condition and available treatment amongst the states and the territories. Only one-third of the
population sufferingfrom mental illness avail mental health services each year. The main
victims of mental illness are early adult population and common mental illnesses are anxiety
and mood disorders. There is also a high demand formental health care in acute and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
emergency units. Challenges exist in relationto recruiting and retaining the mental health
workforce. Moreover, mental health consumers still report that they face problems in
accessing comprehensive mental health care. Thus the Fourth National Mental Health Plan
aims to improve these gaps in the mental health procurement in Australia via collaborative
approach that will help in fostering complementary programs that will deliver responsive
services(CoA, 2009). Such a wide mental health improvement perspective as taken by the
Fourth Plan is of interest as it is the first ever plan to highlighta collaborative approach in
mental health(CoA, 2009). Collaborative approach is an important domain of mental health
as it helps in the participation or formation of an inter-disciplinary team and this will in-turn
help the patient of avail an informed yet quality care (Dogra,FrakeWarner-Gale &, Parkin,
2017).
The following report aims to analyse the Fourth National Mental Health Plan based
on the framework of Health Service Planning and Policy Toolkit by World Health
Organisation (2005).
Policy analysis
Understanding on policy
The Fourth National Mental Health Policy came into action when there is a major
focus on the responsibilities and roles of government inside the mental health framework.
The idea of the plan is to guide reform and identify the principal actions that can lead towards
a meaningful progress towards accomplishment of the vision of the second and the third
National Mental Health Policy. The plan was framed to assist the reforms in mental health.
The main priority area of the plan is to promote mental health and wellbeing among the
population of Australia via reducing the impact of mental illness. The reduction in the
chronicity of mental illness will be promoted via addressing the gaps identified within the
1
workforce. Moreover, mental health consumers still report that they face problems in
accessing comprehensive mental health care. Thus the Fourth National Mental Health Plan
aims to improve these gaps in the mental health procurement in Australia via collaborative
approach that will help in fostering complementary programs that will deliver responsive
services(CoA, 2009). Such a wide mental health improvement perspective as taken by the
Fourth Plan is of interest as it is the first ever plan to highlighta collaborative approach in
mental health(CoA, 2009). Collaborative approach is an important domain of mental health
as it helps in the participation or formation of an inter-disciplinary team and this will in-turn
help the patient of avail an informed yet quality care (Dogra,FrakeWarner-Gale &, Parkin,
2017).
The following report aims to analyse the Fourth National Mental Health Plan based
on the framework of Health Service Planning and Policy Toolkit by World Health
Organisation (2005).
Policy analysis
Understanding on policy
The Fourth National Mental Health Policy came into action when there is a major
focus on the responsibilities and roles of government inside the mental health framework.
The idea of the plan is to guide reform and identify the principal actions that can lead towards
a meaningful progress towards accomplishment of the vision of the second and the third
National Mental Health Policy. The plan was framed to assist the reforms in mental health.
The main priority area of the plan is to promote mental health and wellbeing among the
population of Australia via reducing the impact of mental illness. The reduction in the
chronicity of mental illness will be promoted via addressing the gaps identified within the
1
mental healthcare system. The Fourth Plan also recognises the mental health care needs of the
indigenous population in Australia while delivering comprehensive mental health care(CoA,
2009). Thus this plan was different from other plan in the aspect that it adopts a population
based mental health framework. This framework recognises the determinants of mental health
while acknowledging the importance of mental health across the lifespan.
Critical analysisof the policy
Health service planning and policy toolkit by WHO (2005)
Policy selected for Critique
Mental Health Policy by the Department of Health Government of Australia
Policy title
Fourth national mental health plan: an agenda for collaborative government action
in mental health 2009-2014
Reason for selection of policy
Mental illness is widespread in Australia, according to the National Survey of Mental
Health and Wellbeing Australia (2017), one out of the 5 people aged between 16 to 85 years
of age suffers from mental illnesses like anxiety, mood disorders. This cast a substantial
impact on the social, personal and socio-economic domains of life(CoA, 2009). The Fourth
Plan emphasises the manner in which the reforms in the mental health domain can co-relate
with the policy direction of other associated government portfolios with an aim towards
ensuring that people with mental health problems can take advantage from them in the
highest possible manner (CoA, 2009)
.
2
indigenous population in Australia while delivering comprehensive mental health care(CoA,
2009). Thus this plan was different from other plan in the aspect that it adopts a population
based mental health framework. This framework recognises the determinants of mental health
while acknowledging the importance of mental health across the lifespan.
Critical analysisof the policy
Health service planning and policy toolkit by WHO (2005)
Policy selected for Critique
Mental Health Policy by the Department of Health Government of Australia
Policy title
Fourth national mental health plan: an agenda for collaborative government action
in mental health 2009-2014
Reason for selection of policy
Mental illness is widespread in Australia, according to the National Survey of Mental
Health and Wellbeing Australia (2017), one out of the 5 people aged between 16 to 85 years
of age suffers from mental illnesses like anxiety, mood disorders. This cast a substantial
impact on the social, personal and socio-economic domains of life(CoA, 2009). The Fourth
Plan emphasises the manner in which the reforms in the mental health domain can co-relate
with the policy direction of other associated government portfolios with an aim towards
ensuring that people with mental health problems can take advantage from them in the
highest possible manner (CoA, 2009)
.
2
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Significance of policy for the health of the population
The significance of the policy liesin the fact that it prioritisesthe rights of the consumers,
carers and the families and gives importance to informed decision-making regarding the
process of service options, selection of benefits and anticipated risks (CoA, 2009). The policy
also addresses social exclusion, differential care plan for different age groups along with
service equity. Thus the policy casts an over-arching vision for a stable mental health system
that assists recovery while preventing early mental illness and comprehensive treatment for
all the Australians (CoA, 2009). Fourth National Mental Health Plan shares relationships with
each and every aspect of the National Mental Health Strategy and thereby making it more
significant (details given in appendix). It also gives the mental health plan a whole
government approach thus linking every aspect of mental health with the government
framework (CoA, 2009).
Professional or personal interest
Interest in this policy is derived from the fact that the policy targets a proportion of the
population who are suffering from mental illness. The plan also covers interest of the carers
or the family members of the persons who are suffering from mental illness. According to the
reports published by the Government of Australia, Department of Health, mental illness
impacts on a person’s life at different levels of severity and increases the risk of those
affected, experiencing a range of adverse health, economic and social outcomes. Another aim
of the fourth policy plan is to address the system weakness through consultation and process
and this has generated personal interest in me for selecting this policy as it assures a complete
revamp of the existing mental health policy (CoA, 2009).
How, when and why policy came into existence
The Fourth National Mental Health Plan came into existence in December 2008. The
policy was designed to provide an overarching vision and intent for a comprehensive mental
3
The significance of the policy liesin the fact that it prioritisesthe rights of the consumers,
carers and the families and gives importance to informed decision-making regarding the
process of service options, selection of benefits and anticipated risks (CoA, 2009). The policy
also addresses social exclusion, differential care plan for different age groups along with
service equity. Thus the policy casts an over-arching vision for a stable mental health system
that assists recovery while preventing early mental illness and comprehensive treatment for
all the Australians (CoA, 2009). Fourth National Mental Health Plan shares relationships with
each and every aspect of the National Mental Health Strategy and thereby making it more
significant (details given in appendix). It also gives the mental health plan a whole
government approach thus linking every aspect of mental health with the government
framework (CoA, 2009).
Professional or personal interest
Interest in this policy is derived from the fact that the policy targets a proportion of the
population who are suffering from mental illness. The plan also covers interest of the carers
or the family members of the persons who are suffering from mental illness. According to the
reports published by the Government of Australia, Department of Health, mental illness
impacts on a person’s life at different levels of severity and increases the risk of those
affected, experiencing a range of adverse health, economic and social outcomes. Another aim
of the fourth policy plan is to address the system weakness through consultation and process
and this has generated personal interest in me for selecting this policy as it assures a complete
revamp of the existing mental health policy (CoA, 2009).
How, when and why policy came into existence
The Fourth National Mental Health Plan came into existence in December 2008. The
policy was designed to provide an overarching vision and intent for a comprehensive mental
3
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
health framework in Australia. The policy was endorsed by the health ministers to guide
reforms while identifying principal actions that can effect significant progress towards
accomplishing the aim of the policy (CoA, 2009). The main conceptualize the mental health
under the framework of the population health thus providing a comprehensive approach
towards health care. In this comprehensive population based mental health approach, the
fourth national mental health plan emphasise the framing of the mental health policy based on
the pre-designed government mental health portfolio. This population health framework and
whole government approach are the two most prominent components that make this fourth
national mental health plan an important mental health aspect for Australia (CoA, 2009).
What influenced policy makers to adopt this policy (policy objectives)
The five objectives of the Fourth National Mental Health Plan are: social inclusion and
recovery via improving the service and community understanding and attitudes towards
sustained national stigma reduction strategy; prevention and early intervention via working
with in collaboration with schools and workplaces and delivering programs to improve the
mental health literacy which enhancing resilience; prioritisation of service access along with
proper co-ordination and continuity of care via developing framework of national service
planning that helps in the establishment of targets for the mental health services which are
backed by innovative funding models; quality improvement along with innovation via
critically reviewing the Mental Health Statement of Rights and Responsibilities;
accountability via reporting progress through national mental health data (CoA, 2009).
The framing of the policies are mainly based on few principles of ideal procurement of
the mental health in Australia. The major influence of the Fourth National Mental Health
Plan include respect and right of the comprehensive mental health for the consumers and their
family members, committed service delivery approach, eradication of the social exclusion
4
reforms while identifying principal actions that can effect significant progress towards
accomplishing the aim of the policy (CoA, 2009). The main conceptualize the mental health
under the framework of the population health thus providing a comprehensive approach
towards health care. In this comprehensive population based mental health approach, the
fourth national mental health plan emphasise the framing of the mental health policy based on
the pre-designed government mental health portfolio. This population health framework and
whole government approach are the two most prominent components that make this fourth
national mental health plan an important mental health aspect for Australia (CoA, 2009).
What influenced policy makers to adopt this policy (policy objectives)
The five objectives of the Fourth National Mental Health Plan are: social inclusion and
recovery via improving the service and community understanding and attitudes towards
sustained national stigma reduction strategy; prevention and early intervention via working
with in collaboration with schools and workplaces and delivering programs to improve the
mental health literacy which enhancing resilience; prioritisation of service access along with
proper co-ordination and continuity of care via developing framework of national service
planning that helps in the establishment of targets for the mental health services which are
backed by innovative funding models; quality improvement along with innovation via
critically reviewing the Mental Health Statement of Rights and Responsibilities;
accountability via reporting progress through national mental health data (CoA, 2009).
The framing of the policies are mainly based on few principles of ideal procurement of
the mental health in Australia. The major influence of the Fourth National Mental Health
Plan include respect and right of the comprehensive mental health for the consumers and their
family members, committed service delivery approach, eradication of the social exclusion
4
and providing mental health service based on the cultural diversity across the communities
and throughout the lifespan (CoA, 2009).
Who are the policy makers?
Ministerial Advisory Council is the main contributor towards the Fourth National Mental
Health Plan(CoA, 2009).
Interest group they represent
The Fourth Plan targets a population residing (this is the wrong word here. What do you
mean?...is it “living”? with mental health complications and mental illness. Since the entire
Australian population is targeted, this Mental Health plan constitutes the whole of the
Australian government approach to mental health reform. This approach of government
encompasses a national effort that includes Commonwealth, state and territory level (CoA,
2009).
Stages of policy making process
The first stage of policy making includes collaborative national efforts coming from all
stages of government. This helped in underlying the loopholes of existing mental health
polices and thereby redesigning the new aims of the policy based on the identified loopholes
(Commonwealth of Australia, 2009).
Is the process orderly or chaotic?
The process thus undertaken is ordered and less chaotic.
5
and throughout the lifespan (CoA, 2009).
Who are the policy makers?
Ministerial Advisory Council is the main contributor towards the Fourth National Mental
Health Plan(CoA, 2009).
Interest group they represent
The Fourth Plan targets a population residing (this is the wrong word here. What do you
mean?...is it “living”? with mental health complications and mental illness. Since the entire
Australian population is targeted, this Mental Health plan constitutes the whole of the
Australian government approach to mental health reform. This approach of government
encompasses a national effort that includes Commonwealth, state and territory level (CoA,
2009).
Stages of policy making process
The first stage of policy making includes collaborative national efforts coming from all
stages of government. This helped in underlying the loopholes of existing mental health
polices and thereby redesigning the new aims of the policy based on the identified loopholes
(Commonwealth of Australia, 2009).
Is the process orderly or chaotic?
The process thus undertaken is ordered and less chaotic.
5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
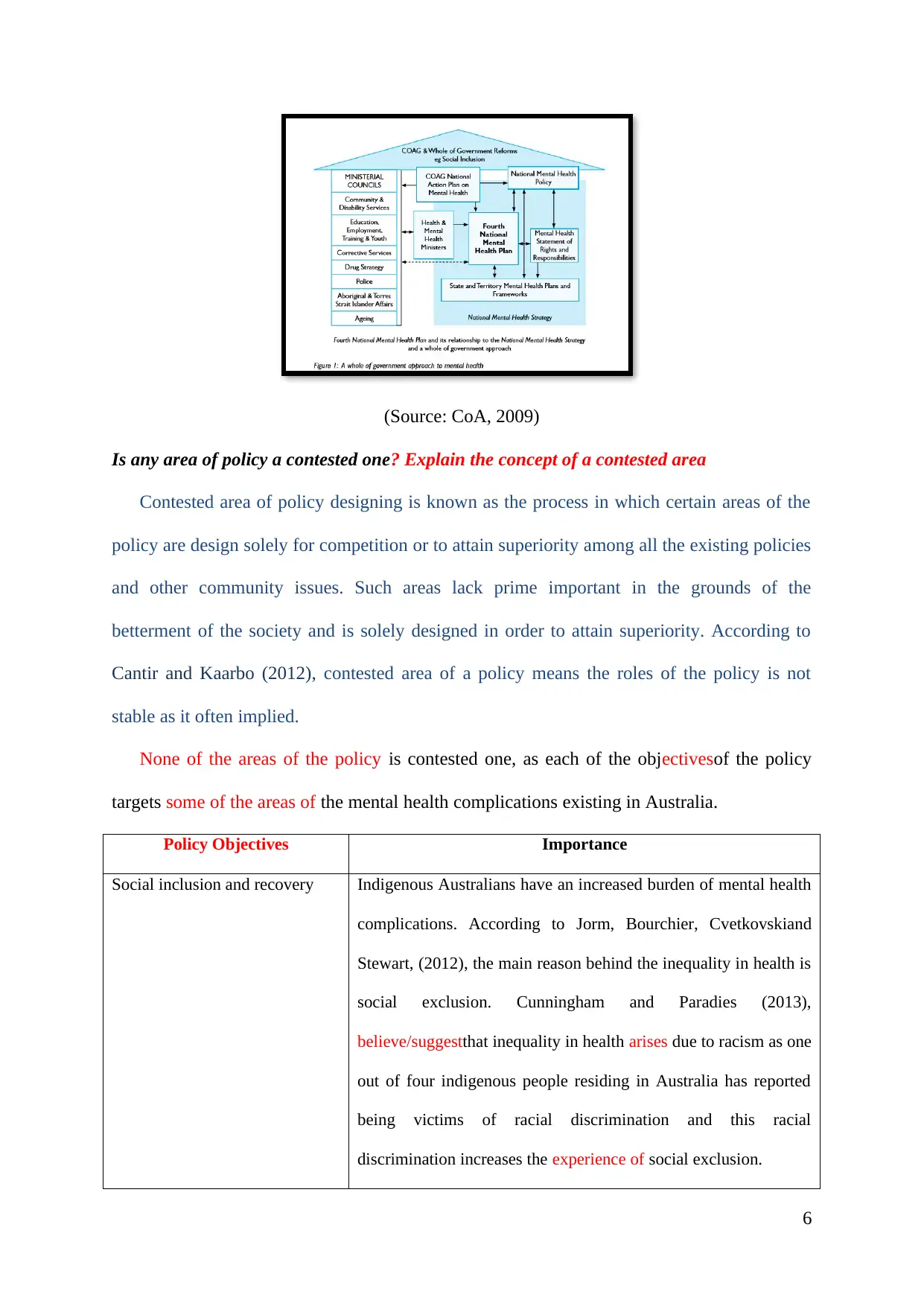
(Source: CoA, 2009)
Is any area of policy a contested one? Explain the concept of a contested area
Contested area of policy designing is known as the process in which certain areas of the
policy are design solely for competition or to attain superiority among all the existing policies
and other community issues. Such areas lack prime important in the grounds of the
betterment of the society and is solely designed in order to attain superiority. According to
Cantir and Kaarbo (2012), contested area of a policy means the roles of the policy is not
stable as it often implied.
None of the areas of the policy is contested one, as each of the objectivesof the policy
targets some of the areas of the mental health complications existing in Australia.
Policy Objectives Importance
Social inclusion and recovery Indigenous Australians have an increased burden of mental health
complications. According to Jorm, Bourchier, Cvetkovskiand
Stewart, (2012), the main reason behind the inequality in health is
social exclusion. Cunningham and Paradies (2013),
believe/suggestthat inequality in health arises due to racism as one
out of four indigenous people residing in Australia has reported
being victims of racial discrimination and this racial
discrimination increases the experience of social exclusion.
6
Is any area of policy a contested one? Explain the concept of a contested area
Contested area of policy designing is known as the process in which certain areas of the
policy are design solely for competition or to attain superiority among all the existing policies
and other community issues. Such areas lack prime important in the grounds of the
betterment of the society and is solely designed in order to attain superiority. According to
Cantir and Kaarbo (2012), contested area of a policy means the roles of the policy is not
stable as it often implied.
None of the areas of the policy is contested one, as each of the objectivesof the policy
targets some of the areas of the mental health complications existing in Australia.
Policy Objectives Importance
Social inclusion and recovery Indigenous Australians have an increased burden of mental health
complications. According to Jorm, Bourchier, Cvetkovskiand
Stewart, (2012), the main reason behind the inequality in health is
social exclusion. Cunningham and Paradies (2013),
believe/suggestthat inequality in health arises due to racism as one
out of four indigenous people residing in Australia has reported
being victims of racial discrimination and this racial
discrimination increases the experience of social exclusion.
6
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
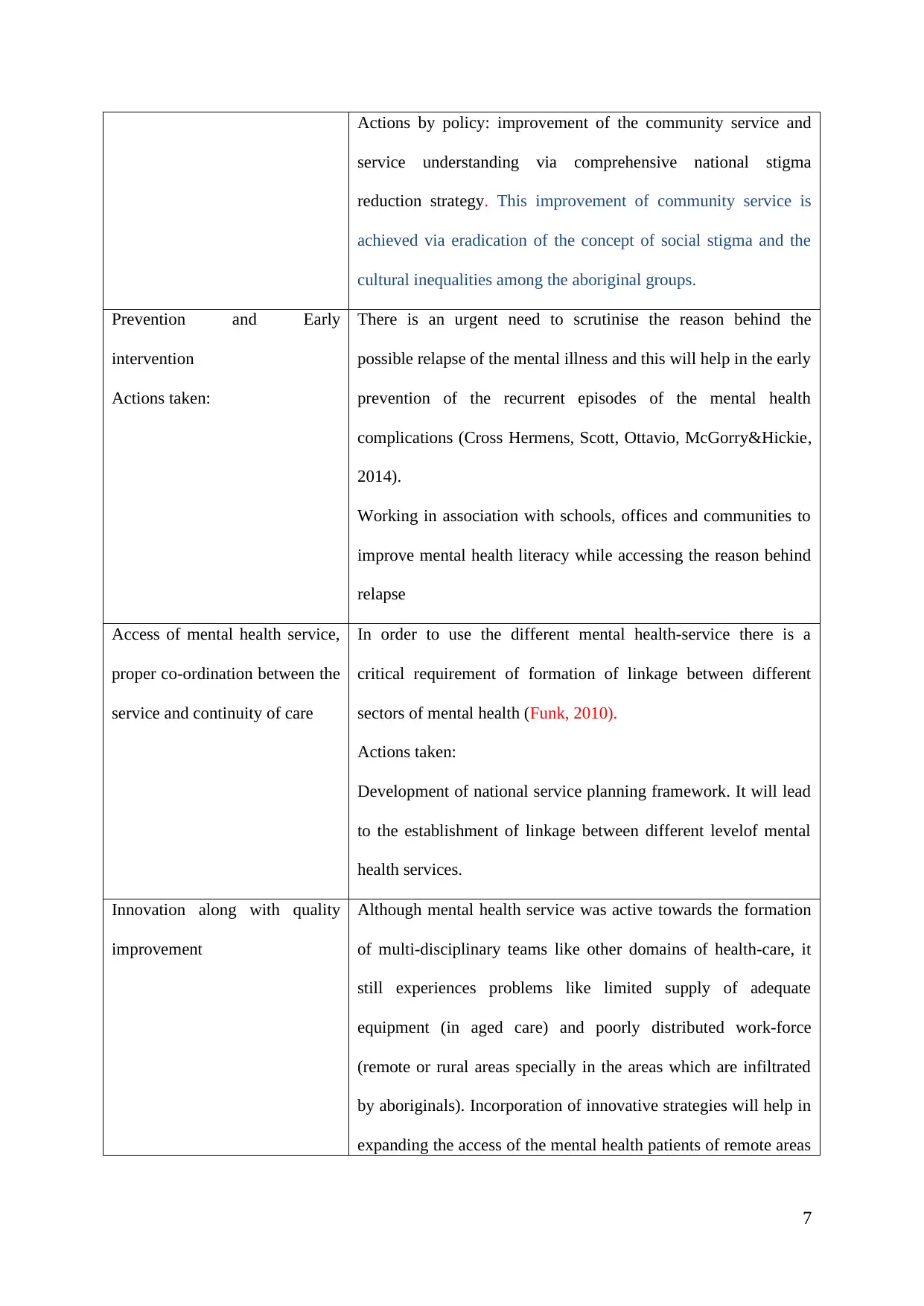
Actions by policy: improvement of the community service and
service understanding via comprehensive national stigma
reduction strategy. This improvement of community service is
achieved via eradication of the concept of social stigma and the
cultural inequalities among the aboriginal groups.
Prevention and Early
intervention
Actions taken:
There is an urgent need to scrutinise the reason behind the
possible relapse of the mental illness and this will help in the early
prevention of the recurrent episodes of the mental health
complications (Cross Hermens, Scott, Ottavio, McGorry&Hickie,
2014).
Working in association with schools, offices and communities to
improve mental health literacy while accessing the reason behind
relapse
Access of mental health service,
proper co-ordination between the
service and continuity of care
In order to use the different mental health-service there is a
critical requirement of formation of linkage between different
sectors of mental health (Funk, 2010).
Actions taken:
Development of national service planning framework. It will lead
to the establishment of linkage between different levelof mental
health services.
Innovation along with quality
improvement
Although mental health service was active towards the formation
of multi-disciplinary teams like other domains of health-care, it
still experiences problems like limited supply of adequate
equipment (in aged care) and poorly distributed work-force
(remote or rural areas specially in the areas which are infiltrated
by aboriginals). Incorporation of innovative strategies will help in
expanding the access of the mental health patients of remote areas
7
service understanding via comprehensive national stigma
reduction strategy. This improvement of community service is
achieved via eradication of the concept of social stigma and the
cultural inequalities among the aboriginal groups.
Prevention and Early
intervention
Actions taken:
There is an urgent need to scrutinise the reason behind the
possible relapse of the mental illness and this will help in the early
prevention of the recurrent episodes of the mental health
complications (Cross Hermens, Scott, Ottavio, McGorry&Hickie,
2014).
Working in association with schools, offices and communities to
improve mental health literacy while accessing the reason behind
relapse
Access of mental health service,
proper co-ordination between the
service and continuity of care
In order to use the different mental health-service there is a
critical requirement of formation of linkage between different
sectors of mental health (Funk, 2010).
Actions taken:
Development of national service planning framework. It will lead
to the establishment of linkage between different levelof mental
health services.
Innovation along with quality
improvement
Although mental health service was active towards the formation
of multi-disciplinary teams like other domains of health-care, it
still experiences problems like limited supply of adequate
equipment (in aged care) and poorly distributed work-force
(remote or rural areas specially in the areas which are infiltrated
by aboriginals). Incorporation of innovative strategies will help in
expanding the access of the mental health patients of remote areas
7
(King, Wei & Howe, 2013).
Innovative strategy includes increase in the consumer and carer
employment in community and clinical settings of mental health.
Measuring and reporting the
overall progress
Generating an accountable and transparent mental health system
is one of the most important steps towards the establishment of
public confidence. Earlier, the patients and their carer’s are unable
to make informed judgements in mental health care (Hansson,
Jormfeldt, Svedberg &Svensson, 2013). At policy level, public
confidence in the mental health reforms drafted by government is
important. At service delivery level mental health consumers need
to be confident about the available mental health services. Both
aspects of confidence are the central to the actions taken under the
Fourth Plan (Bao, Casalino&Pincus, 2013). The gain in
confidence will be achievedvia enabling consumers and their
carers to access information about the nature of services that is
responsible for the care across the range of health quality
domains.
Was there a consultation process in place?
The consultation process was in place because each aim has its detailed objectives along
with the action plan and expected outcome. The Fourth Plan emphasizes the manner in which
reforms in mental health can inter-relate with the direction of the policy directions
inaccordance with the other portfolios of government. Overall it aims towards ensuring that
the group of population with mental health complications can gain highest possible
benefit(CoA, 2009).
8
Innovative strategy includes increase in the consumer and carer
employment in community and clinical settings of mental health.
Measuring and reporting the
overall progress
Generating an accountable and transparent mental health system
is one of the most important steps towards the establishment of
public confidence. Earlier, the patients and their carer’s are unable
to make informed judgements in mental health care (Hansson,
Jormfeldt, Svedberg &Svensson, 2013). At policy level, public
confidence in the mental health reforms drafted by government is
important. At service delivery level mental health consumers need
to be confident about the available mental health services. Both
aspects of confidence are the central to the actions taken under the
Fourth Plan (Bao, Casalino&Pincus, 2013). The gain in
confidence will be achievedvia enabling consumers and their
carers to access information about the nature of services that is
responsible for the care across the range of health quality
domains.
Was there a consultation process in place?
The consultation process was in place because each aim has its detailed objectives along
with the action plan and expected outcome. The Fourth Plan emphasizes the manner in which
reforms in mental health can inter-relate with the direction of the policy directions
inaccordance with the other portfolios of government. Overall it aims towards ensuring that
the group of population with mental health complications can gain highest possible
benefit(CoA, 2009).
8
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
What interested groups, if any, have beenconsulted and what sources and kinds of advice
havebeenobtained
Ministerial Advisory Councils beyond the health care domain are included in the process
of development of Fourth Plan. This helped in articulation of present responsibilities and
roles of other portfolios as they coincide in the path of improving the outcome of mental
health services. The advice obtained from inclusion of interested groups (who and why ids
this important in any policy development and analysis?)from different sectors of healthcare is
apart from the health care professionals consumers and their carers should also be actively
engaged in the service and policy development in health care. While the mental health service
provides should work as a team within the designed framework to procure comprehensive
care to the mental health consumers. Now such advice goes in sync with reports published by
Brett, Staniszewska, Mockford, Herron‐Marx, Hughes, Tysall and Suleman (2014), which
also emphasises on patient and public involvement in all principal stages of research process.
Did the consultation process and its outcomes have an impact on what was included
in the policy?
The consultation through First and Second Mental Health Plans revealed several
aspects of mental health requirements in Australia and this includes respect of rights of
mental health consumers and their carers, requirement for culturally diverse mental
health care plan which prevents social exclusion, different mental health plan for the
people of different age group along with service equity. All these highlighted areas of
concern are stringently incorporated in the policy planning. For example, the Fourth
National Mental Health Plan aims towards developing an integrated program to
support mental health services via providing tailored assistance to people with mental
illness living in the community (CoA, 2009). Moreover, these highlighted areas like
community diverse mental health plans, culturally diverse mental health plans are in
9
havebeenobtained
Ministerial Advisory Councils beyond the health care domain are included in the process
of development of Fourth Plan. This helped in articulation of present responsibilities and
roles of other portfolios as they coincide in the path of improving the outcome of mental
health services. The advice obtained from inclusion of interested groups (who and why ids
this important in any policy development and analysis?)from different sectors of healthcare is
apart from the health care professionals consumers and their carers should also be actively
engaged in the service and policy development in health care. While the mental health service
provides should work as a team within the designed framework to procure comprehensive
care to the mental health consumers. Now such advice goes in sync with reports published by
Brett, Staniszewska, Mockford, Herron‐Marx, Hughes, Tysall and Suleman (2014), which
also emphasises on patient and public involvement in all principal stages of research process.
Did the consultation process and its outcomes have an impact on what was included
in the policy?
The consultation through First and Second Mental Health Plans revealed several
aspects of mental health requirements in Australia and this includes respect of rights of
mental health consumers and their carers, requirement for culturally diverse mental
health care plan which prevents social exclusion, different mental health plan for the
people of different age group along with service equity. All these highlighted areas of
concern are stringently incorporated in the policy planning. For example, the Fourth
National Mental Health Plan aims towards developing an integrated program to
support mental health services via providing tailored assistance to people with mental
illness living in the community (CoA, 2009). Moreover, these highlighted areas like
community diverse mental health plans, culturally diverse mental health plans are in
9
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
accordance with the reports published by Patel and Saxena (2014). Every identified
gap (reference and what were the identified gaps and how were they identified?)is
covered in objectives of the policy planning along with projected plan of outcomes and
desired outcomes.
Is there a process in place for ongoing consultation and review?
In order to review the ongoing consultation, the fourth plan aims to establish a
comprehensive national reporting process that will track the progress of the mental health
reforms. Such security will also access the needs of the stakeholders. The review of the
ongoing consultation satisfies the requirement stated in the published works of Patel and
Saxena (2014). According to Patel and Saxena (2014), the implementation of the mental
health services should be based on the current gaps in mental health that has been prioritised
by the policy makers and stakeholders.
Is the adopted process of policy-making the best that could be hoped for? If not how might
it beimproved
The adopted process of policy is best that could be hoped for as it encompasses nearly
(what is missing??) all the sectors of the mental health complications prevalent in Australia
(CoA, 2009). Moreover, the policy also aims to increase the employment of the carers and
consumers under community and clinical settings. This incorporation of the caregivers or the
family members under process of policy planning is the principal feature, making this mental
health policy a success (Tambuyzer, Pieters& Van Audenhove, 2014). This will help in the
improvement of the quality of the mental health service while increasing the accountability.
Was the policy development process a good process? Is the policy a good policy? How do
you know?
10
gap (reference and what were the identified gaps and how were they identified?)is
covered in objectives of the policy planning along with projected plan of outcomes and
desired outcomes.
Is there a process in place for ongoing consultation and review?
In order to review the ongoing consultation, the fourth plan aims to establish a
comprehensive national reporting process that will track the progress of the mental health
reforms. Such security will also access the needs of the stakeholders. The review of the
ongoing consultation satisfies the requirement stated in the published works of Patel and
Saxena (2014). According to Patel and Saxena (2014), the implementation of the mental
health services should be based on the current gaps in mental health that has been prioritised
by the policy makers and stakeholders.
Is the adopted process of policy-making the best that could be hoped for? If not how might
it beimproved
The adopted process of policy is best that could be hoped for as it encompasses nearly
(what is missing??) all the sectors of the mental health complications prevalent in Australia
(CoA, 2009). Moreover, the policy also aims to increase the employment of the carers and
consumers under community and clinical settings. This incorporation of the caregivers or the
family members under process of policy planning is the principal feature, making this mental
health policy a success (Tambuyzer, Pieters& Van Audenhove, 2014). This will help in the
improvement of the quality of the mental health service while increasing the accountability.
Was the policy development process a good process? Is the policy a good policy? How do
you know?
10
The policy is a standard health care policy in the mental health sector because it
adopts the population health framework which emphasizes the need of developing an
effective preventive approach towards common mental illness like anxiety and depression.
According to Jacka, Mykletun and Berk (2012), sustainable, effective population-level
initiatives for prevention of mental illness will help to develop approaches addressing to non-
communicable somatic disease. The sustainable and population level approaches will help in
the generation of awareness among the community level and thereby helping to combat the
non-communicable disease in an informed manner (Jacka, Mykletun & Berk, 2012)
Has the policy achieved required outcomes?
The main aimof the policy is to provide mental health services in a co-ordinated manner.
In 2007, Australian National Mental Health Survey data revealed that Australian youth have
the highest prevalence of mental illness and the worst service accessthan any group in the
population ???. Only 21.8% of Australian youth (16 to 24 years), who are diagnosed with
mental disorders have access to professional help. However, the implementation of Fourth
Policy has improved the youth mental health outcome. At present nearly 50 000 Australian
youths receive mental health services through the 30 centres round the country (McGorry,
Bates & Birchwood, 2013).This needs a comparison between now and before the fourth
mental health plan…is there acknowledged improvement and what part of the plan achieved
this?
Would a different policy be likely to yield better results?
This policy is a comprehensive policy for mental health sector in Australia. However,
it has certain limitation. The policy fails to highlight the increasing rate of depression and
dementia among aged population of Australia and the steps that should be taken in order
to overcome such problems (CoA, 2009). Moreover, the policy does not provide a
detailed insight about the person centred care in mental health (CoA, 2009). According to
11
adopts the population health framework which emphasizes the need of developing an
effective preventive approach towards common mental illness like anxiety and depression.
According to Jacka, Mykletun and Berk (2012), sustainable, effective population-level
initiatives for prevention of mental illness will help to develop approaches addressing to non-
communicable somatic disease. The sustainable and population level approaches will help in
the generation of awareness among the community level and thereby helping to combat the
non-communicable disease in an informed manner (Jacka, Mykletun & Berk, 2012)
Has the policy achieved required outcomes?
The main aimof the policy is to provide mental health services in a co-ordinated manner.
In 2007, Australian National Mental Health Survey data revealed that Australian youth have
the highest prevalence of mental illness and the worst service accessthan any group in the
population ???. Only 21.8% of Australian youth (16 to 24 years), who are diagnosed with
mental disorders have access to professional help. However, the implementation of Fourth
Policy has improved the youth mental health outcome. At present nearly 50 000 Australian
youths receive mental health services through the 30 centres round the country (McGorry,
Bates & Birchwood, 2013).This needs a comparison between now and before the fourth
mental health plan…is there acknowledged improvement and what part of the plan achieved
this?
Would a different policy be likely to yield better results?
This policy is a comprehensive policy for mental health sector in Australia. However,
it has certain limitation. The policy fails to highlight the increasing rate of depression and
dementia among aged population of Australia and the steps that should be taken in order
to overcome such problems (CoA, 2009). Moreover, the policy does not provide a
detailed insight about the person centred care in mental health (CoA, 2009). According to
11
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 20
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.