Case Study Analysis: Annette's Mental Health and Eating Habits
VerifiedAdded on 2022/09/14
|16
|4008
|9
Case Study
AI Summary
This case study analyzes Annette's mental health challenges, focusing on cognitive and behavioral approaches. It examines how Annette's maladaptive thought processes, stemming from her perceptions of herself, her body, and eating, contribute to her difficulties. The analysis references Beck's cognitive model and other relevant research to explain the development of Annette's negative self-image and eating habits. The study then compares and contrasts cognitive and behavioral approaches, highlighting how they explain Annette's mental health problems. Furthermore, it proposes treatment guidelines, including Cognitive Behavioral Therapy (CBT) and family-based therapy, outlining specific phases and techniques to address Annette's issues, including the use of self-monitoring, goal setting, and family involvement to promote positive changes in her behavior and mental well-being.

Running Head: CASE STUDY
Case study
Name of the student
Name of the University
Author’s note
Case study
Name of the student
Name of the University
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CASE STUDY
Design/Concept of Annette’s complications built on cognitive and behaviour
approach
Annette’s cognitive viewpoint might have not adjusting to the assumed procedures about
herself, her physique, and an adverse approach in the direction of eating (Ratcliffe & Ellison,
2015). Annette, though, has gradually declined her diet program and replicated detoxification
habits, and it is unclear if she has negative attitudes toward herself. According to Beck’s
cognitive model (1974), Poor and inaccurate perceptions can be the basis of Annette's
undesirable perception of the physique and appearance. Beck assumes that Annette's essential
views about this woman, society, and the environment are developed initial in life and
unintentionally impact her opinion of this girl; this impacts her unhealthy perceptions about her
body, impacting her weight management habits to fit in. According to Saito and Annette’s
cognitive viewpoint might have not adjusting to the assumed procedures about herself, her
physique, and an adverse approach towards food consumption (Ratcliffe & Ellison, 2015).
Annette, though, has gradually cut her diet program and replicated detoxification habits, and it is
unclear if she has negative attitudes toward herself. According to Beck’s cognitive model (1974),
Poor and inaccurate perceptions can be the basis of Annette's undesirable perception of the
physique and appearance. Beck assumes that Annette's essential beliefs about oneself, society,
and the environment are developed initial in life and unintentionally impact her view of herself;
this impacts her unhealthy perceptions about her body, impacting her weight management habits
to fit in. According to Saito and Izumi-Barton (2018)
the presumption that unhealthy weight perceptions projected nutritional regulation, contributed
to reduced conscience esteem and enhanced thin idealization, this is also related to misdirection,
that further fosters skinny perceptions and weight losses.
Design/Concept of Annette’s complications built on cognitive and behaviour
approach
Annette’s cognitive viewpoint might have not adjusting to the assumed procedures about
herself, her physique, and an adverse approach in the direction of eating (Ratcliffe & Ellison,
2015). Annette, though, has gradually declined her diet program and replicated detoxification
habits, and it is unclear if she has negative attitudes toward herself. According to Beck’s
cognitive model (1974), Poor and inaccurate perceptions can be the basis of Annette's
undesirable perception of the physique and appearance. Beck assumes that Annette's essential
views about this woman, society, and the environment are developed initial in life and
unintentionally impact her opinion of this girl; this impacts her unhealthy perceptions about her
body, impacting her weight management habits to fit in. According to Saito and Annette’s
cognitive viewpoint might have not adjusting to the assumed procedures about herself, her
physique, and an adverse approach towards food consumption (Ratcliffe & Ellison, 2015).
Annette, though, has gradually cut her diet program and replicated detoxification habits, and it is
unclear if she has negative attitudes toward herself. According to Beck’s cognitive model (1974),
Poor and inaccurate perceptions can be the basis of Annette's undesirable perception of the
physique and appearance. Beck assumes that Annette's essential beliefs about oneself, society,
and the environment are developed initial in life and unintentionally impact her view of herself;
this impacts her unhealthy perceptions about her body, impacting her weight management habits
to fit in. According to Saito and Izumi-Barton (2018)
the presumption that unhealthy weight perceptions projected nutritional regulation, contributed
to reduced conscience esteem and enhanced thin idealization, this is also related to misdirection,
that further fosters skinny perceptions and weight losses.
2CASE STUDY
Signs of an unhealthy lifestyle are propagated by a distinctive spectrum of overvalued thought re
garding personal body weight implications. The behaviour of Annette may be extracted from the
connection between healthy personality traits and female socio-cultural views (Saunders &
Frazier, 2017), which led to low esteem in Annette. The poor self-esteem of Annette can stem
from poor confidence, which is a driving force in eating disorders as well as high levels of
frustration she is unable to express properly. Anger is considered to be dangerous, and this could
be Annette's reason to deprive herself from the self against the body (Fox &Power, 2009), this
will also act as motivation for Annette to be malnourished herself. According to Schmidt and
Treasure (2006), Physiological preferences and behavioural traits that can be called dispositional
and close and characteristic. According to them, cognitive style and personality factors will lead
to disposition and trait. One may, for example, find Annette having traits of personality, for
instance conscientiousness, and poor self-confidence. Conscientiousness the unrealistic
aspirations individually assigned or socially influenced, which creates and generates excessively
high self-expectancy (Hurst & Zimmer-Gembeck, 2015). This may be confirmed by Butler and
Montgomery (2005) discovering that fifty percent of adolescents with consumption disorder
exhibited conscientiousness.
Through a humanistic view point, action is deliberate, taught by the way people view and
experience experiences and, if the result is good, will affect those behaviours. Annette mixes
thinness with success and thus duplicates the actions of famous girls to attract attention. Allyon,
Haughton, and Osmond (1964) note that interest is developed by the refusal of nourishment that
is being used as a means of obtaining the interest of her mother, the common teen-agers, and
youngsters. Nutrition is more gratifying until concentration and energy are obtained and thus
leads to self-actualization (Wadden et al, 1991). Self-actualization is obtained only by optimistic
Signs of an unhealthy lifestyle are propagated by a distinctive spectrum of overvalued thought re
garding personal body weight implications. The behaviour of Annette may be extracted from the
connection between healthy personality traits and female socio-cultural views (Saunders &
Frazier, 2017), which led to low esteem in Annette. The poor self-esteem of Annette can stem
from poor confidence, which is a driving force in eating disorders as well as high levels of
frustration she is unable to express properly. Anger is considered to be dangerous, and this could
be Annette's reason to deprive herself from the self against the body (Fox &Power, 2009), this
will also act as motivation for Annette to be malnourished herself. According to Schmidt and
Treasure (2006), Physiological preferences and behavioural traits that can be called dispositional
and close and characteristic. According to them, cognitive style and personality factors will lead
to disposition and trait. One may, for example, find Annette having traits of personality, for
instance conscientiousness, and poor self-confidence. Conscientiousness the unrealistic
aspirations individually assigned or socially influenced, which creates and generates excessively
high self-expectancy (Hurst & Zimmer-Gembeck, 2015). This may be confirmed by Butler and
Montgomery (2005) discovering that fifty percent of adolescents with consumption disorder
exhibited conscientiousness.
Through a humanistic view point, action is deliberate, taught by the way people view and
experience experiences and, if the result is good, will affect those behaviours. Annette mixes
thinness with success and thus duplicates the actions of famous girls to attract attention. Allyon,
Haughton, and Osmond (1964) note that interest is developed by the refusal of nourishment that
is being used as a means of obtaining the interest of her mother, the common teen-agers, and
youngsters. Nutrition is more gratifying until concentration and energy are obtained and thus
leads to self-actualization (Wadden et al, 1991). Self-actualization is obtained only by optimistic
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CASE STUDY
self-consciousness, which can only be done by constructive understanding by others; this can be
accomplished through others 'interest. Annette's eating habits are also motivated by weight loss,
as she assumes that replicating common girls 'activities will attract attention. Annette to face
competition to adapt to being famous, which she correlates with becoming slim, equivalent to the
common girls; this has caused her to measure her own success by watching peer conduct. She
also desire to be a part of the dance group. Therefore, she restricted her eating habit. Because of
her mother’s growing weight, she developed fear of becoming fat. At the same time, she wanted
to improve her relationship wuth her mother by spending more time with her (Rabinor, 2002).
Compare and contrast the ways in which cognitive and behavioral approache
s explain the mental health problems and challenges Annette faces
Humanistic psychology originated from the unhappiness with how cognitive science
described the actions of the person. Although the logical approach would claim that the eating
behaviour of Annette is the product of knowledge through studying the actions of the famous
people, the humanistic approach will claim that Annette does not attain self-realization. For
instance, Thogersen-Ntoumani, Ntourmanis and Nikitaras (2009) observed that promoting parent
flexibility and proactive goals in life influence the risk of woman teenagers participating in
inappropriate weight management measures to meet physiological need. The way we view our
perceptions, from a logical perspective, defines the way we act and respond. Nevertheless, the
humanistic philosophy claims that the brain creates and forms individual perceptions, and thus
Annette's own behaviour about its weight.
Also logical and humanistic, emphasis on the subconscious mind's influence. Many
believe that their eating disorder is not the product of their previous encounters, so they believe
self-consciousness, which can only be done by constructive understanding by others; this can be
accomplished through others 'interest. Annette's eating habits are also motivated by weight loss,
as she assumes that replicating common girls 'activities will attract attention. Annette to face
competition to adapt to being famous, which she correlates with becoming slim, equivalent to the
common girls; this has caused her to measure her own success by watching peer conduct. She
also desire to be a part of the dance group. Therefore, she restricted her eating habit. Because of
her mother’s growing weight, she developed fear of becoming fat. At the same time, she wanted
to improve her relationship wuth her mother by spending more time with her (Rabinor, 2002).
Compare and contrast the ways in which cognitive and behavioral approache
s explain the mental health problems and challenges Annette faces
Humanistic psychology originated from the unhappiness with how cognitive science
described the actions of the person. Although the logical approach would claim that the eating
behaviour of Annette is the product of knowledge through studying the actions of the famous
people, the humanistic approach will claim that Annette does not attain self-realization. For
instance, Thogersen-Ntoumani, Ntourmanis and Nikitaras (2009) observed that promoting parent
flexibility and proactive goals in life influence the risk of woman teenagers participating in
inappropriate weight management measures to meet physiological need. The way we view our
perceptions, from a logical perspective, defines the way we act and respond. Nevertheless, the
humanistic philosophy claims that the brain creates and forms individual perceptions, and thus
Annette's own behaviour about its weight.
Also logical and humanistic, emphasis on the subconscious mind's influence. Many
believe that their eating disorder is not the product of their previous encounters, so they believe
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CASE STUDY
that it is flexible, and they can decide their own destiny. According to Vitousek and Orimoto
(1993), Persons with eating disorder struggle from a skewed view of their bodies and constantly
feel that they should shed obesity in order to gain regulator over their weightiness; this is denoted
to in cognitive terms as ‘weight-related self-schemata’. Both techniques are directed towards
reducing the eating condition of Annette, either by conscience-actualization or by slowly
changing her maladaptive patterns. All strategies include cognitive behavioural theory (CBT), in
which key principles of sympathy are introduced, genuine constructive thinking is simplified and
relationship building is promoted.
Provide treatment and/or medication guidelines that reflect the social and
Behavioral approach
Cognitive behavioural therapy (CBT) helps participants to realize how their negative self-
image moral views affect their vulnerability to anorexia (Grohol, 2006). Cognitive behavioural
therapy is a psycho-social involvement which aims at improving the mental health. This therapy
helps in the improving emotional intelligence, helps in the development of personality, in coping
the current personality disorders. CBT allows people, such as Annette, to decrease lengthy-
standing poor self-assessment of body shape; that's because body fat is something which can be
monitored and eating habits and loss of weight are something that is socially enhanced
(Hepworth, 1999). Though, Improved Cognitive Behavioural Therapy (CBT-E) was reviewed as
a cure for eating disorders and was shown to be more effective in directly treating anorexia
patients (Dalle Grave, 2013).
that it is flexible, and they can decide their own destiny. According to Vitousek and Orimoto
(1993), Persons with eating disorder struggle from a skewed view of their bodies and constantly
feel that they should shed obesity in order to gain regulator over their weightiness; this is denoted
to in cognitive terms as ‘weight-related self-schemata’. Both techniques are directed towards
reducing the eating condition of Annette, either by conscience-actualization or by slowly
changing her maladaptive patterns. All strategies include cognitive behavioural theory (CBT), in
which key principles of sympathy are introduced, genuine constructive thinking is simplified and
relationship building is promoted.
Provide treatment and/or medication guidelines that reflect the social and
Behavioral approach
Cognitive behavioural therapy (CBT) helps participants to realize how their negative self-
image moral views affect their vulnerability to anorexia (Grohol, 2006). Cognitive behavioural
therapy is a psycho-social involvement which aims at improving the mental health. This therapy
helps in the improving emotional intelligence, helps in the development of personality, in coping
the current personality disorders. CBT allows people, such as Annette, to decrease lengthy-
standing poor self-assessment of body shape; that's because body fat is something which can be
monitored and eating habits and loss of weight are something that is socially enhanced
(Hepworth, 1999). Though, Improved Cognitive Behavioural Therapy (CBT-E) was reviewed as
a cure for eating disorders and was shown to be more effective in directly treating anorexia
patients (Dalle Grave, 2013).
5CASE STUDY
PHASE 1
Therapist and
Annette work to
identify eating
disorder and establish
PHASE 2
Plans are designed to help
Annette understand and
improve food patterns, and to
help her cope with poor self-
assessment
PHASE 3
Normal eating habits
established with self-
monitoring timetable to reduce
nutritional control
PHASE 3
Discussing poor self-esteem
by reconfirming values
PHASE 3
Emphasis on actions, mood and
self-evaluation
PHASE 3
Developing future goals
PHASE 4
Considering opportunities to
overcome challenges and
keeping a good outlook
PHASE 1
Therapist and
Annette work to
identify eating
disorder and establish
PHASE 2
Plans are designed to help
Annette understand and
improve food patterns, and to
help her cope with poor self-
assessment
PHASE 3
Normal eating habits
established with self-
monitoring timetable to reduce
nutritional control
PHASE 3
Discussing poor self-esteem
by reconfirming values
PHASE 3
Emphasis on actions, mood and
self-evaluation
PHASE 3
Developing future goals
PHASE 4
Considering opportunities to
overcome challenges and
keeping a good outlook
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CASE STUDY
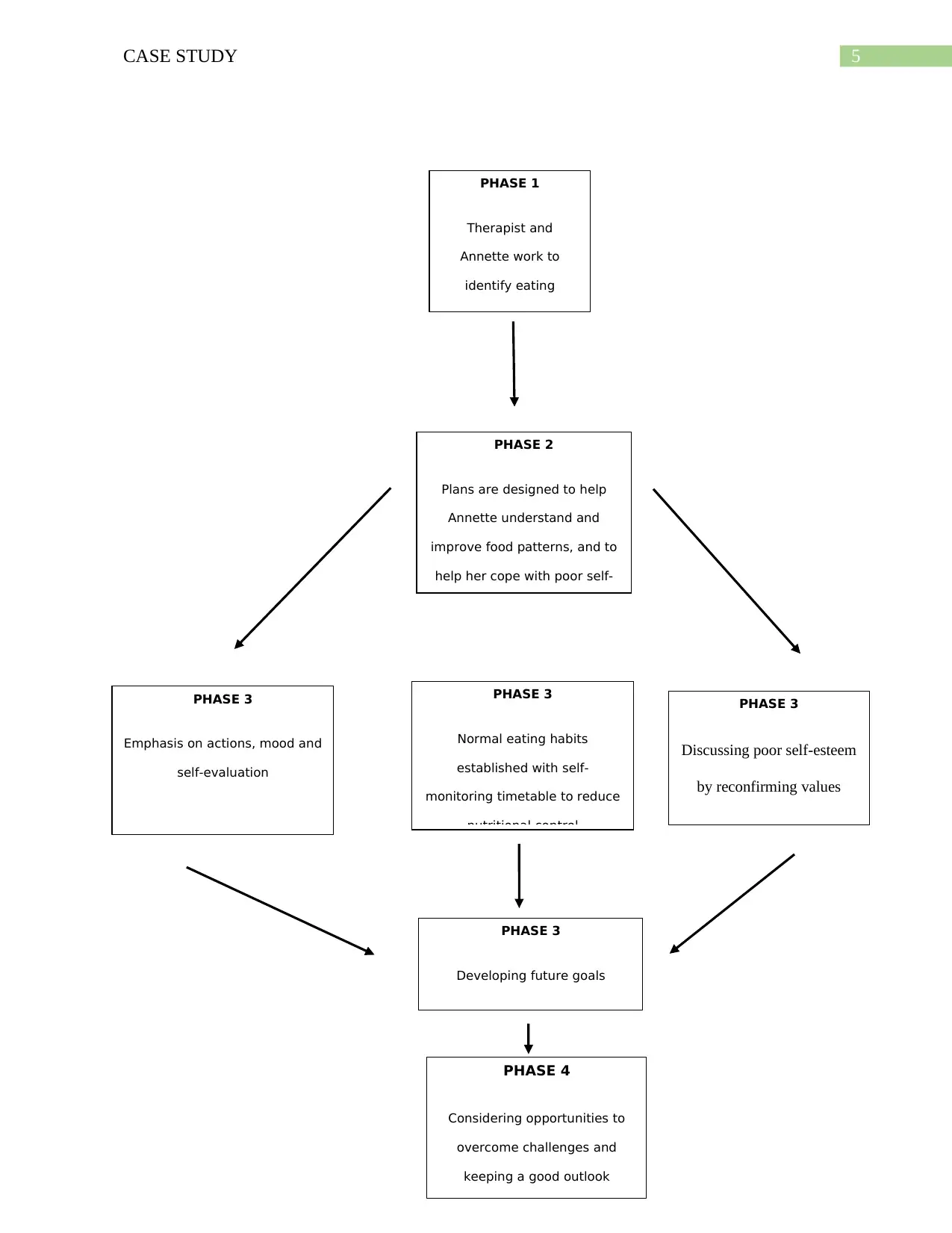
Phase one includes having a shared awareness of Annette's anorexia (Wright, 2010), and
then mutually developing a plan that demonstrates her eating problems are understood and open
to improvement. Those preliminary sessions will consist of two weekly meetings.
The second phase implies a thorough review of the changes gained by Annette, so that
preparations can be achieved for the next care process. The exercises include finding ways to
improve and manage their dietary habits by customized physically and mentally dimensions
therapy (Cooper & Fairburn, 2010). Then raise weight issues, and educate her on the negative
consequences of continually reassessing self-image (Geller & Srikameswaran, 2001). An effort
should be initiated to provide assistance to Annette for coping with the contradictions she is
facing inside herself (Serpell et al, 1999); this includes the usage of personal observing so that
she can grasp what is going on at the moment.
The third phase contains therapy sessions focused on discussing topics about shape and
weight; that the willingness of Annette to deal with day-to-day emotions and activities that can
influence her attitudes toward herself. Trainings would then try to overcome her severe dietary
limitation (Waller et al, 2007). Session will try to persuade Annette to consider the inflexibility
of her actualization-evaluation and promote reassertion of certain facets of her life by altering
dualistic thought (Shafran, Cooper, & Fairburn, 2002). Poor self-esteem can be overcome by
taking into account the good aspects and overgeneralizing potential shortcomings, reaffirming
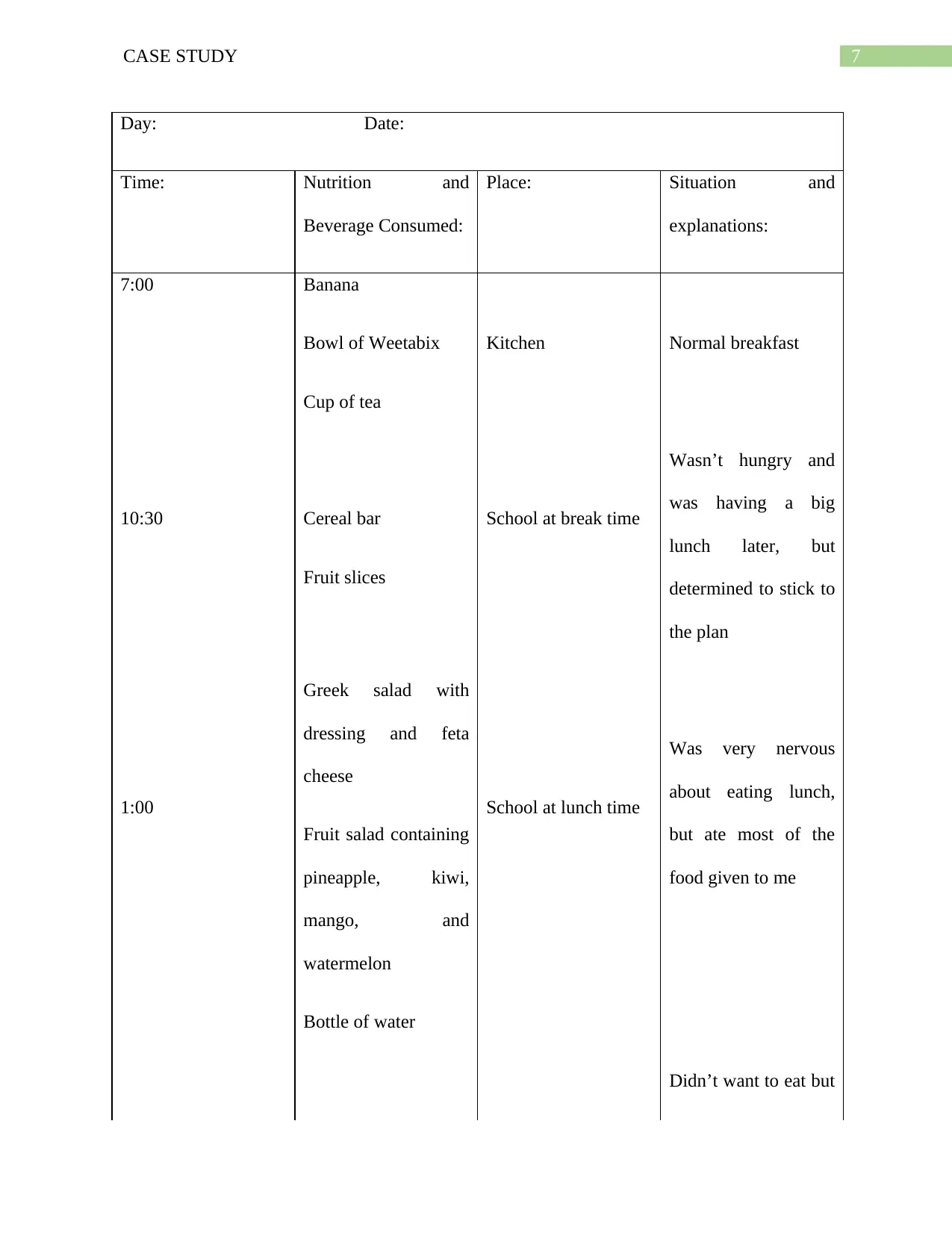
previous perceptions of the self. A daily eating schedule should then be established and
promoted, under the provision that no diarrhea is to be accompanied by feeding; this is
accomplished by keeping an auto-monitoring notebook (Fairburn et al., 2008).
Phase one includes having a shared awareness of Annette's anorexia (Wright, 2010), and
then mutually developing a plan that demonstrates her eating problems are understood and open
to improvement. Those preliminary sessions will consist of two weekly meetings.
The second phase implies a thorough review of the changes gained by Annette, so that
preparations can be achieved for the next care process. The exercises include finding ways to
improve and manage their dietary habits by customized physically and mentally dimensions
therapy (Cooper & Fairburn, 2010). Then raise weight issues, and educate her on the negative
consequences of continually reassessing self-image (Geller & Srikameswaran, 2001). An effort
should be initiated to provide assistance to Annette for coping with the contradictions she is
facing inside herself (Serpell et al, 1999); this includes the usage of personal observing so that
she can grasp what is going on at the moment.
The third phase contains therapy sessions focused on discussing topics about shape and
weight; that the willingness of Annette to deal with day-to-day emotions and activities that can
influence her attitudes toward herself. Trainings would then try to overcome her severe dietary
limitation (Waller et al, 2007). Session will try to persuade Annette to consider the inflexibility
of her actualization-evaluation and promote reassertion of certain facets of her life by altering
dualistic thought (Shafran, Cooper, & Fairburn, 2002). Poor self-esteem can be overcome by
taking into account the good aspects and overgeneralizing potential shortcomings, reaffirming
previous perceptions of the self. A daily eating schedule should then be established and
promoted, under the provision that no diarrhea is to be accompanied by feeding; this is
accomplished by keeping an auto-monitoring notebook (Fairburn et al., 2008).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CASE STUDY
Day: Date:
Time: Nutrition and
Beverage Consumed:
Place: Situation and
explanations:
7:00 Banana
Bowl of Weetabix
Cup of tea
Kitchen Normal breakfast
10:30 Cereal bar
Fruit slices
School at break time
Wasn’t hungry and
was having a big
lunch later, but
determined to stick to
the plan
1:00
Greek salad with
dressing and feta
cheese
Fruit salad containing
pineapple, kiwi,
mango, and
watermelon
Bottle of water
School at lunch time
Was very nervous
about eating lunch,
but ate most of the
food given to me
Didn’t want to eat but
Day: Date:
Time: Nutrition and
Beverage Consumed:
Place: Situation and
explanations:
7:00 Banana
Bowl of Weetabix
Cup of tea
Kitchen Normal breakfast
10:30 Cereal bar
Fruit slices
School at break time
Wasn’t hungry and
was having a big
lunch later, but
determined to stick to
the plan
1:00
Greek salad with
dressing and feta
cheese
Fruit salad containing
pineapple, kiwi,
mango, and
watermelon
Bottle of water
School at lunch time
Was very nervous
about eating lunch,
but ate most of the
food given to me
Didn’t want to eat but
8CASE STUDY
3:45 Yogurt Kitchen
also didn’t want to
leave a big gap
6:30
Salmon
Rice
Spinach
Kitchen Feeling ok as it
wasn’t too much food
8:00 Ice cream with
chocolate toppings
Ice cream parlour
with friends
Really enjoyed
getting ice cream
with friends, and even
finished the ice cream
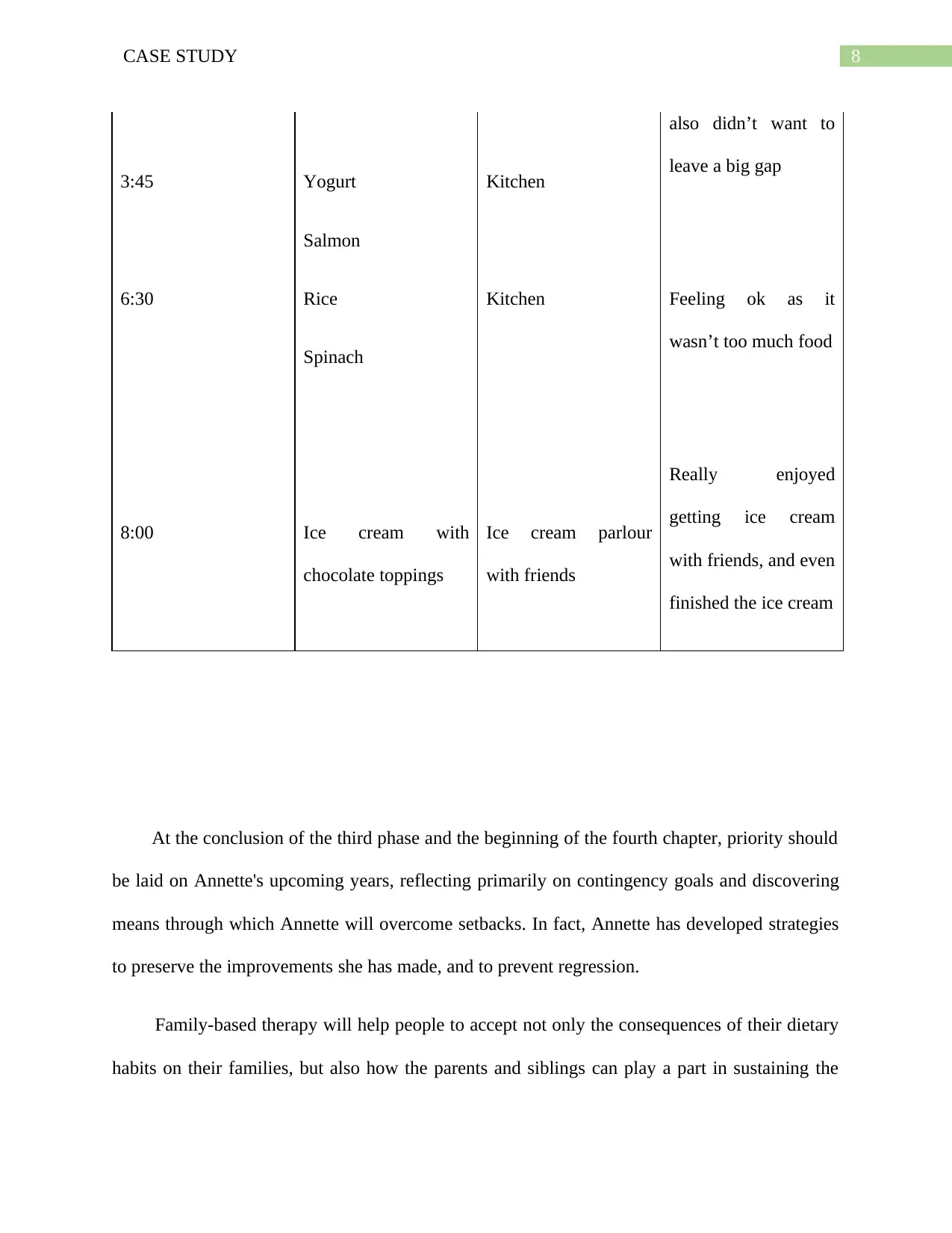
At the conclusion of the third phase and the beginning of the fourth chapter, priority should
be laid on Annette's upcoming years, reflecting primarily on contingency goals and discovering
means through which Annette will overcome setbacks. In fact, Annette has developed strategies
to preserve the improvements she has made, and to prevent regression.
Family-based therapy will help people to accept not only the consequences of their dietary
habits on their families, but also how the parents and siblings can play a part in sustaining the
3:45 Yogurt Kitchen
also didn’t want to
leave a big gap
6:30
Salmon
Rice
Spinach
Kitchen Feeling ok as it
wasn’t too much food
8:00 Ice cream with
chocolate toppings
Ice cream parlour
with friends
Really enjoyed
getting ice cream
with friends, and even
finished the ice cream
At the conclusion of the third phase and the beginning of the fourth chapter, priority should
be laid on Annette's upcoming years, reflecting primarily on contingency goals and discovering
means through which Annette will overcome setbacks. In fact, Annette has developed strategies
to preserve the improvements she has made, and to prevent regression.
Family-based therapy will help people to accept not only the consequences of their dietary
habits on their families, but also how the parents and siblings can play a part in sustaining the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CASE STUDY
addiction to food (Grohol, 2006). The Maudsley model is the most frequently used family
therapy approach; this includes gaining care of Annette's diet and gradually slowly reducing her
social influence as Annette continues to behave as per her authority (Wilson et al, 2007). This
form of therapy tends to interact effectively within the family, which tells Annette's mother that
she can encourage enablement in reducing the effects of eating disorder in Annette (Schmidt et
al, 2007). Use three stages, the Maudsley method is usually performed within 15 to 20 courses.
The first stage comprises constructing a structure combining the disease-related views of
both Annette and her mother (NICE, 2017). Annette's mother is advised to support her by being
compassionate to her body appearance challenges; this will allow Annette to be more aware of
her mother's support (Frank et al, 2012). Training is provided on dietary habits and the hazards
of malnutrition. An approach is initiated called the 'mini food' where Annette is patiently and
firmly motivated to consume a limited quantity of food, with encouragement being offered. A
family food to improve the Annette's relationship with her mother (Assis de Silva, 2013) is
added.
The second step of therapy includes urging Annette's mother to help Annette develop
better control over her diet, and to make her sleep better regularly. White et al (2017) noticed
parental incitement to consume more. Annette and her mother are encouraged to continue eating
together so that after she has consumed, her mother will monitor. Conversations on other issues
will be kept, draw attention from anorexia, and Annette becomes mindful of the love and
participation of her mother in her life (Smith, 2004). Parental support of consumption of food is
something that needs to be examined closely, so that Annette understands that it is a sign of
genuine treatment, not efforts by Annette's mother to retake charge over her; this relates to poor
tolerance to confusion, typical among those that experience anorexia (Frank et al, 2012).
addiction to food (Grohol, 2006). The Maudsley model is the most frequently used family
therapy approach; this includes gaining care of Annette's diet and gradually slowly reducing her
social influence as Annette continues to behave as per her authority (Wilson et al, 2007). This
form of therapy tends to interact effectively within the family, which tells Annette's mother that
she can encourage enablement in reducing the effects of eating disorder in Annette (Schmidt et
al, 2007). Use three stages, the Maudsley method is usually performed within 15 to 20 courses.
The first stage comprises constructing a structure combining the disease-related views of
both Annette and her mother (NICE, 2017). Annette's mother is advised to support her by being
compassionate to her body appearance challenges; this will allow Annette to be more aware of
her mother's support (Frank et al, 2012). Training is provided on dietary habits and the hazards
of malnutrition. An approach is initiated called the 'mini food' where Annette is patiently and
firmly motivated to consume a limited quantity of food, with encouragement being offered. A
family food to improve the Annette's relationship with her mother (Assis de Silva, 2013) is
added.
The second step of therapy includes urging Annette's mother to help Annette develop
better control over her diet, and to make her sleep better regularly. White et al (2017) noticed
parental incitement to consume more. Annette and her mother are encouraged to continue eating
together so that after she has consumed, her mother will monitor. Conversations on other issues
will be kept, draw attention from anorexia, and Annette becomes mindful of the love and
participation of her mother in her life (Smith, 2004). Parental support of consumption of food is
something that needs to be examined closely, so that Annette understands that it is a sign of
genuine treatment, not efforts by Annette's mother to retake charge over her; this relates to poor
tolerance to confusion, typical among those that experience anorexia (Frank et al, 2012).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10CASE STUDY
The third and final process ends with Annette being able to maintain her weight at a
healthier weight by using inappropriate weight management methods; that is because Annette is
gradually granted responsibility over food. The final step emphasizes on the psychological
impact of the unhealthy lifestyle on the individual and how it has contributed to a healthier
identity being established; this is accomplished by relying on both Annette and her mother's
abilities, thereby reducing potential eating disorder influence.
Offer a short summary of the scientific findings justifying the use of CBT and
Family Therapy
Cognitive behavioural therapy (CBT) is frequently used as recovery approaches, but
strengthened Cognitive Behavioural Therapy (CBT-E) has been proved to be extra successful
because it is additional customized to fit the anorexia diagnosis of the patient, including eating
habits adjustment, weight management activity, and food, weight, and appearance issues
(Fairburn, 2008). CBT-E evaluations have shown positive prolonged-term recovery following
treatment with eating disorders (Signorini, Sheffield, Rhodes, Fleming, & Ward, 2018); this
could be due to the fact that the meetings are twice as long as the standard CBT (Fairburn et al,
2015). The period of diagnosis, however, is questioned for being very resource consuming
(Layard & Clark, 2014). Study by Byrne, Fusland, Allen and Watson (2011) used CBT-E in
people with eating disorders, particularly those with a body mass index (BMI) of above fourteen.
Researchers discovered that the patients 'dietary habits and overall sociopath changed
dramatically. Turner et al (2015) has observed that the severity of patient eating disorder, their
depression and anxiety, as well as general increase in their daily mental health, was substantially
decreased. Family-based treatment is recognized one of the most successful treatments for
people with an eating disorder, especially teenagers (Lock & Le Grange, 2015). Moreover,
The third and final process ends with Annette being able to maintain her weight at a
healthier weight by using inappropriate weight management methods; that is because Annette is
gradually granted responsibility over food. The final step emphasizes on the psychological
impact of the unhealthy lifestyle on the individual and how it has contributed to a healthier
identity being established; this is accomplished by relying on both Annette and her mother's
abilities, thereby reducing potential eating disorder influence.
Offer a short summary of the scientific findings justifying the use of CBT and
Family Therapy
Cognitive behavioural therapy (CBT) is frequently used as recovery approaches, but
strengthened Cognitive Behavioural Therapy (CBT-E) has been proved to be extra successful
because it is additional customized to fit the anorexia diagnosis of the patient, including eating
habits adjustment, weight management activity, and food, weight, and appearance issues
(Fairburn, 2008). CBT-E evaluations have shown positive prolonged-term recovery following
treatment with eating disorders (Signorini, Sheffield, Rhodes, Fleming, & Ward, 2018); this
could be due to the fact that the meetings are twice as long as the standard CBT (Fairburn et al,
2015). The period of diagnosis, however, is questioned for being very resource consuming
(Layard & Clark, 2014). Study by Byrne, Fusland, Allen and Watson (2011) used CBT-E in
people with eating disorders, particularly those with a body mass index (BMI) of above fourteen.
Researchers discovered that the patients 'dietary habits and overall sociopath changed
dramatically. Turner et al (2015) has observed that the severity of patient eating disorder, their
depression and anxiety, as well as general increase in their daily mental health, was substantially
decreased. Family-based treatment is recognized one of the most successful treatments for
people with an eating disorder, especially teenagers (Lock & Le Grange, 2015). Moreover,
11CASE STUDY
DerMarderosian et al (2018) notes that family-based therapy is by far the most effective
therapeutic tool, since it facilitates long-term recovery for eating disordered juveniles. Grange et
al (2007) study showed a significant decrease in effects of the anorexia after family-based
therapy. Couturier, Kimber, and Szatmari (2013) note that family-based counselling has been
successful due to follow-ups after diagnosis of eating disorders in youths. Robinson et al (2013)
reported that in family, a boost in personality-efficacy in the family-based family as well as a
decline in symptoms of anorexia. White et al (2015) observed during the use of family meal
approach, used during family-based treatment, was beneficial in improving eating through the
use of parental incentives; this is further endorsed by Sadeh-Sharvit et al (2018), who suggested
that parents 'awareness of eating disorders and knowledge the need to modify social roles and
laws tended to lead to early weight. Lock et al (2016) reported family-based counseling to
minimize hospitalization rates for teenagers with disordered eating. Evidence from a study
directed by Halvorsen et al (2017) described that family-based intervention resulted in weight
loss and decreased eating disorder patterns.
Elaborate how your own personal views and capabilities have formed your
selections and reactions in developing this coursework
While I never encountered an eating disorder myself, I have friends who've already
experienced from eating disorders recently, and so I am aware of their thoughts and ideas about
themselves and the medications they have undergone. I had long discussions on how they think
for themselves and asked them how you see yourself in the mirror. I think they all had a blurred
image of themselves, because they saw themselves as bloated in the mirror. Most of them
criticized media depictions that provide perceptions and guidelines about how they should look
DerMarderosian et al (2018) notes that family-based therapy is by far the most effective
therapeutic tool, since it facilitates long-term recovery for eating disordered juveniles. Grange et
al (2007) study showed a significant decrease in effects of the anorexia after family-based
therapy. Couturier, Kimber, and Szatmari (2013) note that family-based counselling has been
successful due to follow-ups after diagnosis of eating disorders in youths. Robinson et al (2013)
reported that in family, a boost in personality-efficacy in the family-based family as well as a
decline in symptoms of anorexia. White et al (2015) observed during the use of family meal
approach, used during family-based treatment, was beneficial in improving eating through the
use of parental incentives; this is further endorsed by Sadeh-Sharvit et al (2018), who suggested
that parents 'awareness of eating disorders and knowledge the need to modify social roles and
laws tended to lead to early weight. Lock et al (2016) reported family-based counseling to
minimize hospitalization rates for teenagers with disordered eating. Evidence from a study
directed by Halvorsen et al (2017) described that family-based intervention resulted in weight
loss and decreased eating disorder patterns.
Elaborate how your own personal views and capabilities have formed your
selections and reactions in developing this coursework
While I never encountered an eating disorder myself, I have friends who've already
experienced from eating disorders recently, and so I am aware of their thoughts and ideas about
themselves and the medications they have undergone. I had long discussions on how they think
for themselves and asked them how you see yourself in the mirror. I think they all had a blurred
image of themselves, because they saw themselves as bloated in the mirror. Most of them
criticized media depictions that provide perceptions and guidelines about how they should look
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.