NUR4111: iSAP Framework Application: Annie's Safe Community Transition
VerifiedAdded on 2022/09/18
|8
|1904
|17
Homework Assignment
AI Summary
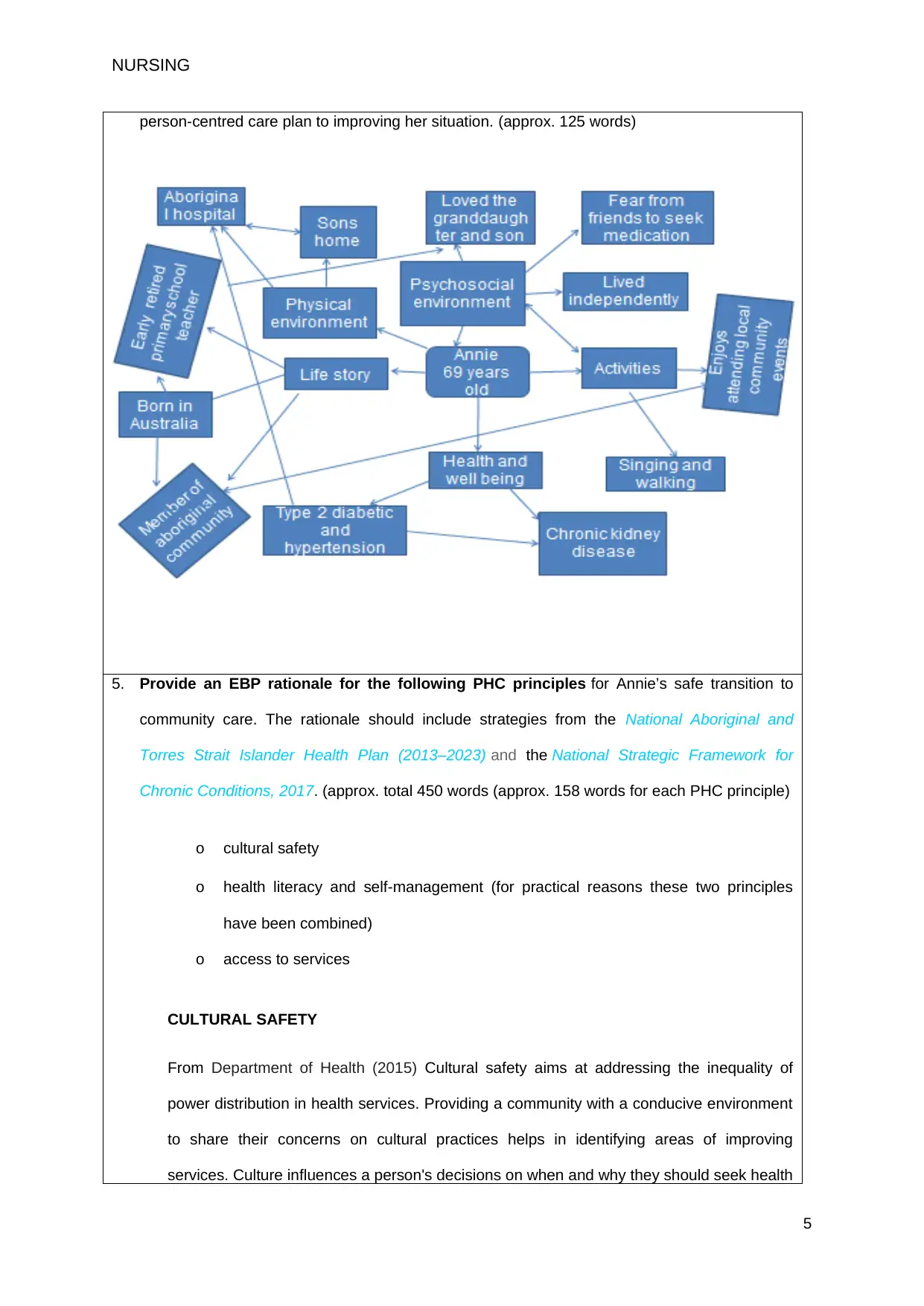
This assignment delves into a case study of Annie, a 69-year-old Indigenous woman with diabetes, hypertension, and chronic kidney problems, who requires a safe transition from acute care to the community. The assignment begins by defining discharge planning and discussing its importance in Annie's context, emphasizing its role in reducing hospital readmissions and ensuring medication adherence. It then identifies and discusses four key barriers to effective discharge planning, including communication gaps, lack of role clarity, resource limitations, and ineffective planning. The assignment outlines the key steps for planning and implementing safe transfer of care, emphasizing early risk assessment, individualized care plans, and the importance of communication with patients and their families. A concept map is constructed to illustrate a strengths-based, person-centered care plan. Finally, the assignment provides an evidence-based practice (EBP) rationale for the principles of cultural safety, health literacy, self-management, and access to services, drawing on the National Aboriginal and Torres Strait Islander Health Plan (2013–2023) and the National Strategic Framework for Chronic Conditions (2017) to support Annie's safe transition to community care.


1 out of 8
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.