Investigating Anxiety's Impact on Cognitive Abilities in Older Adults
VerifiedAdded on 2020/07/22
|32
|9062
|81
Report
AI Summary
This report investigates the impact of anxiety on cognitive functions, specifically focusing on information processing speed, memory, and attention in older adults. The study employs a comparative analysis between younger and older adult groups using various assessment tools, including anxiety inventories, cognitive function tests, and visual search tasks. The findings reveal detrimental effects of anxiety, particularly in older males, with higher depression scores correlating to longer visual search times. The research aligns with prior studies suggesting anxiety's influence on response times and highlights the importance of considering subjective cognitive function and intra-individual variability. The report also examines the potential influence of sex and educational level on information processing speed and discusses the implications of these findings for understanding cognitive decline in ageing and age-related diseases. The study emphasizes the need for further research to explore the complex interplay between anxiety and cognitive performance in the context of ageing.
1
Does Anxiety influence Information Processing Speed and variability, Memory and attention in
ageing?
Does Anxiety influence Information Processing Speed and variability, Memory and attention in
ageing?
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
ABSTRACT
INTRODUCTION: The main objective behind carry out study is to analyze the extent to
which anxiety level has high level of impact on information processing speed, memory and
attention in older adulthood.
METHODS: Tests of anxiety, including beck anxiety inventory, state and trait anxiety,
sleep quality, depression and subjective and objective cognitive functioning and visual search
task were administered to two groups of adults, one younger (n= 52; 18-25 years) and one older
(n= 52; 50-80 years).
RESULTS: From assessment, it has identified that detrimental effects of anxiety are not
limited to the clinical disorders. Hence, higher depression scores resulted in longer Visual
Search Effect times. All these were statistically significant, and occurred only in older males.
Prior studies have indicated that anxiety lengthens response times, and the Visual Search task
displayed impacts of anxiety levels.
DISCUSSION: From assessment, it has identified that results were consistent with prior
studies pertaining to anxiety lengthens response times. Along with this, it has found from visual
search task results that anxiety level has influence on response times.
Keywords: Anxiety, Attention, Information processing speed, Subjective memory
function, Objective cognitive function, Ageing.
ABSTRACT
INTRODUCTION: The main objective behind carry out study is to analyze the extent to
which anxiety level has high level of impact on information processing speed, memory and
attention in older adulthood.
METHODS: Tests of anxiety, including beck anxiety inventory, state and trait anxiety,
sleep quality, depression and subjective and objective cognitive functioning and visual search
task were administered to two groups of adults, one younger (n= 52; 18-25 years) and one older
(n= 52; 50-80 years).
RESULTS: From assessment, it has identified that detrimental effects of anxiety are not
limited to the clinical disorders. Hence, higher depression scores resulted in longer Visual
Search Effect times. All these were statistically significant, and occurred only in older males.
Prior studies have indicated that anxiety lengthens response times, and the Visual Search task
displayed impacts of anxiety levels.
DISCUSSION: From assessment, it has identified that results were consistent with prior
studies pertaining to anxiety lengthens response times. Along with this, it has found from visual
search task results that anxiety level has influence on response times.
Keywords: Anxiety, Attention, Information processing speed, Subjective memory
function, Objective cognitive function, Ageing.
3
Introduction
Mild cognitive impairment implies for the situation of abnormality that is higher as
compared to expected aspects pertaining to age and education. From assessment, it has found
that situation of self-perceived cognitive decline pertaining to memory aspect usually occurred
among older adults having both MCI and dementia at early stage. Along with this, it has found
that memory function closely influences daily life and mental health of individual. In both
cognitively healthy ageing and ageing–related diseases states such as Alzheimer’s disease, a
large body of evidence supports an association between information processing speed and the
functional integrity of both cognitive and of neuroanatomical aspects of the mind. These impacts
include changes to the brain’s white matter, and alterations to components of information
processing system (Anstey et al., 2007; Haynes et al., 2017; Kennedy et al., 2013; Lövdén, Shing
& Lindberger, 2007; Voelker et al., 2017). Neuroanatomical studies have identified age-related
differences in the interhemispheric data transfer rates and activation as well as differences in
white matter integrity, with older adults demonstrating greater transfer rates than younger ones,
possibly as a compensatory strategy to overcome ageing-related cognitive declines (Anstey et al.,
2007; Haynes et al., 2017). These differences are identifiable using reaction time tasks as
fundamental measures of both interhemispheric transfer and cognitive changes due to ageing
(Antsey et al., 2007).
As defined in the American Psychiatric Association’s (APA’s) Diagnostic and Statistical
Manual of Mental Disorders (DSM-5) mild cognitive impairment (MCI) occurs when an
individual experiences memory and other core brain functions problems that do not interfere
with independent living and which are not due to delirium or another mental disorder (APA,
Introduction
Mild cognitive impairment implies for the situation of abnormality that is higher as
compared to expected aspects pertaining to age and education. From assessment, it has found
that situation of self-perceived cognitive decline pertaining to memory aspect usually occurred
among older adults having both MCI and dementia at early stage. Along with this, it has found
that memory function closely influences daily life and mental health of individual. In both
cognitively healthy ageing and ageing–related diseases states such as Alzheimer’s disease, a
large body of evidence supports an association between information processing speed and the
functional integrity of both cognitive and of neuroanatomical aspects of the mind. These impacts
include changes to the brain’s white matter, and alterations to components of information
processing system (Anstey et al., 2007; Haynes et al., 2017; Kennedy et al., 2013; Lövdén, Shing
& Lindberger, 2007; Voelker et al., 2017). Neuroanatomical studies have identified age-related
differences in the interhemispheric data transfer rates and activation as well as differences in
white matter integrity, with older adults demonstrating greater transfer rates than younger ones,
possibly as a compensatory strategy to overcome ageing-related cognitive declines (Anstey et al.,
2007; Haynes et al., 2017). These differences are identifiable using reaction time tasks as
fundamental measures of both interhemispheric transfer and cognitive changes due to ageing
(Antsey et al., 2007).
As defined in the American Psychiatric Association’s (APA’s) Diagnostic and Statistical
Manual of Mental Disorders (DSM-5) mild cognitive impairment (MCI) occurs when an
individual experiences memory and other core brain functions problems that do not interfere
with independent living and which are not due to delirium or another mental disorder (APA,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

4
2013). Brain studies of individuals with MCI demonstrate that as many as 10 to 15 percent of
those with MCI develop full dementia within a year (Fauzan & Amran, 2015).
Information processing speed is commonly measured as part of the diagnosis of dementia
and cognitive impairment. In normal aging, the brain functions slow while intelligence measures
stabilise, and recall ability decreases significantly. Research evidence indicates that information
processing speed can vary significantly with respect to methodological factors such as the task
used and thus areas of the brain recruited for performance and response demands (Rodrigues &
Pandeirada, 2014; Valeriani et al., 2003) and person-related factors such as sex (Commmodari &
Guanera, 2013), education (Tales & Basoudan, 2016), and possibly genetic factors (Luo et al.,
2017). Interactions between these factors can result in significantly different impacts on
processing speeds depending on specific brain areas required for performance of tasks (Tales et
al., 2010; Tales & Basoudan, 2016). Hence, older individuals often experience greater difficulty
remembering the name of people, places and other aspects. Mild cognitive impairment (MCI)
occurs when the individual experiences measureable problems in relation to memory and another
core brain functions. MCI is also associated with increased risk of developing Alzheimer’s
disease in the short term.
RT variability is impacted by a combination of three physiological effects: hemispheric
specialization, individual neuroanatomy, and transient functional fluctuations between trials
(Antonova et al., 2016), Thus, RT measures need to consider many aspects of typical behavior
and environmental interaction (Rodrigues & Pandeirada, 2014, Tales & Basoudan, 2016).
Results of information processing speed tests in clinical populations may need to be interpreted
with respect to such caveats, making it difficult to relate clinical to research findings. It is
included in DSM-5 for measurement specifically with respect to attention-related processing
2013). Brain studies of individuals with MCI demonstrate that as many as 10 to 15 percent of
those with MCI develop full dementia within a year (Fauzan & Amran, 2015).
Information processing speed is commonly measured as part of the diagnosis of dementia
and cognitive impairment. In normal aging, the brain functions slow while intelligence measures
stabilise, and recall ability decreases significantly. Research evidence indicates that information
processing speed can vary significantly with respect to methodological factors such as the task
used and thus areas of the brain recruited for performance and response demands (Rodrigues &
Pandeirada, 2014; Valeriani et al., 2003) and person-related factors such as sex (Commmodari &
Guanera, 2013), education (Tales & Basoudan, 2016), and possibly genetic factors (Luo et al.,
2017). Interactions between these factors can result in significantly different impacts on
processing speeds depending on specific brain areas required for performance of tasks (Tales et
al., 2010; Tales & Basoudan, 2016). Hence, older individuals often experience greater difficulty
remembering the name of people, places and other aspects. Mild cognitive impairment (MCI)
occurs when the individual experiences measureable problems in relation to memory and another
core brain functions. MCI is also associated with increased risk of developing Alzheimer’s
disease in the short term.
RT variability is impacted by a combination of three physiological effects: hemispheric
specialization, individual neuroanatomy, and transient functional fluctuations between trials
(Antonova et al., 2016), Thus, RT measures need to consider many aspects of typical behavior
and environmental interaction (Rodrigues & Pandeirada, 2014, Tales & Basoudan, 2016).
Results of information processing speed tests in clinical populations may need to be interpreted
with respect to such caveats, making it difficult to relate clinical to research findings. It is
included in DSM-5 for measurement specifically with respect to attention-related processing
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
(Naveteur et.al., 2005). Research indicates that information processing speed can vary
significantly with respect to methodological factors such as the task used and thus areas of the
brain recruited for performance and response demands and person-related factors such as sex and
educational level (Tales, Bayer, Haworth & Snowden, 2010). Such research evidence indicates
that the results of information processing speed tests in clinical populations may need to be
interpreted with respect to such caveats, especially as there is a high degree in variability in the
tasks used to measure information processing speeds in clinical populations, making the
comparison of results within the clinical arena problematic and also making it difficult to relate
clinical to research findings.
It is important to measure information processing speed because slowing of information
processing can have a negative influence upon many aspects of real life [Increased RT in older
adults has been shown to be associated to increased antagonist muscle co-activation. In older
subjects, the RTs for both measures were significantly longer than for younger adults (Arnold et
al., 2015). From assessment, it has identified that three physiological effects namely hemispheric
specialization, individual neuroanatomy and transient functional fluctuations between trials has
an impact on RT variability (Antonova et al., 2016). Thus, RT measures need to be assessed
appropriately and in relation to many aspects of typical behaviour and environmental interaction
(Rodrigues & Pandeirada, 2014).
By doing research, it has identified that risk of dementia can be reduced significantly
through the means of resourcefulness training. From evaluation, it has asserted that RT training
provides high level of assistance in reducing the level of caregiver stress. It is possible that other
factors that are rarely researched and rarely tested in clinical conditions, may also affect
information processing speed. One such factor is anxiety. Salthouse (2011) highlighted the
(Naveteur et.al., 2005). Research indicates that information processing speed can vary
significantly with respect to methodological factors such as the task used and thus areas of the
brain recruited for performance and response demands and person-related factors such as sex and
educational level (Tales, Bayer, Haworth & Snowden, 2010). Such research evidence indicates
that the results of information processing speed tests in clinical populations may need to be
interpreted with respect to such caveats, especially as there is a high degree in variability in the
tasks used to measure information processing speeds in clinical populations, making the
comparison of results within the clinical arena problematic and also making it difficult to relate
clinical to research findings.
It is important to measure information processing speed because slowing of information
processing can have a negative influence upon many aspects of real life [Increased RT in older
adults has been shown to be associated to increased antagonist muscle co-activation. In older
subjects, the RTs for both measures were significantly longer than for younger adults (Arnold et
al., 2015). From assessment, it has identified that three physiological effects namely hemispheric
specialization, individual neuroanatomy and transient functional fluctuations between trials has
an impact on RT variability (Antonova et al., 2016). Thus, RT measures need to be assessed
appropriately and in relation to many aspects of typical behaviour and environmental interaction
(Rodrigues & Pandeirada, 2014).
By doing research, it has identified that risk of dementia can be reduced significantly
through the means of resourcefulness training. From evaluation, it has asserted that RT training
provides high level of assistance in reducing the level of caregiver stress. It is possible that other
factors that are rarely researched and rarely tested in clinical conditions, may also affect
information processing speed. One such factor is anxiety. Salthouse (2011) highlighted the
6
possibility that anxiety may affect RT performance and that although high levels of clinical
anxiety may be acknowledged to affect information processing speeds, lower levels of anxiety
are generally not considered to have any effect. In contrast, however, Tales and Basoudan (2016)
noted that anxiety has a high prevalence in older adults and that even non-clinical anxiety may
impact cognitive performance. One aim of this research is to determine the potential for anxiety
to affect the outcome of information processing speed in older adults.
Subjective Cognitive Function
Another factor that has rarely been considered in the investigation of information
processing speed in ageing and ageing-related disease is subjective cognitive function. Although
most studies examining information processing speed in ageing measure and factor in the
potential influence of objectively measured status of cognitive function it is rare for research
results to consider how subjective feelings or assessment of cognitive function may influence
information processing speed. Objective measures of poor general cognition are often found to
be related to slower information processing speeds compared to intact cognition in older adults
(Tales & Basoudan, 2016). It is possible that subjectively poor cognition may also affect
information processing speed (either via similar or different mechanisms as yet to be fully
identified).
If this is the case then both clinical and research findings would need to be interpreted
with respect to this caveat also. A further aim of this study is also to determine whether in older
adults either objectively measured or subjectively experienced cognitive function influences
information processing speed. Finally, the potential influence of sex (male/female) and
educational level upon information processing speed will also be investigated.
possibility that anxiety may affect RT performance and that although high levels of clinical
anxiety may be acknowledged to affect information processing speeds, lower levels of anxiety
are generally not considered to have any effect. In contrast, however, Tales and Basoudan (2016)
noted that anxiety has a high prevalence in older adults and that even non-clinical anxiety may
impact cognitive performance. One aim of this research is to determine the potential for anxiety
to affect the outcome of information processing speed in older adults.
Subjective Cognitive Function
Another factor that has rarely been considered in the investigation of information
processing speed in ageing and ageing-related disease is subjective cognitive function. Although
most studies examining information processing speed in ageing measure and factor in the
potential influence of objectively measured status of cognitive function it is rare for research
results to consider how subjective feelings or assessment of cognitive function may influence
information processing speed. Objective measures of poor general cognition are often found to
be related to slower information processing speeds compared to intact cognition in older adults
(Tales & Basoudan, 2016). It is possible that subjectively poor cognition may also affect
information processing speed (either via similar or different mechanisms as yet to be fully
identified).
If this is the case then both clinical and research findings would need to be interpreted
with respect to this caveat also. A further aim of this study is also to determine whether in older
adults either objectively measured or subjectively experienced cognitive function influences
information processing speed. Finally, the potential influence of sex (male/female) and
educational level upon information processing speed will also be investigated.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
Intra-Individual Variability
In the research arena in addition to measuring information processing speed it has been
common to measure also its intra-individual variability (IIVRT). IIVRT like information processing
speed is also related to cognitive and neuroanatomical factors, with increased variability
commonly but not always, related to disease related ageing such as Alzheimer’s disease, and in
some cases, has been found to be more sensitive to ageing and or disease than mean information
processing speed per se (Luo et al., 2017; Tales & Basoudan, 2016). Although previous research
has examined IIVRT with respect to objectively measured cognitive function very little research
has examined the influence of subjective cognitive function and anxiety. This measure will thus
also be investigated in the present also be investigated in the present study considering gender
and level of education.
Attention
Attention is one of the cognitive functions most affected by ageing. The loss of function
in attention can impact a wide variety of cognitive activities and daily living functions (Akimoto
et al., 2014). Valeriani, Ranghi and Giaquinto (2003) identified differences in somatosensory
evoked potentials (SEPs) to median nerve stimulation between tasks requiring neutral
stimulation conditions and selective attention conditions for both older (mean age 71.7) and
younger (mean age 26.9) adults and abnormal attention function found in MCI and various
aetiologies of dementia (Tales, Bayer, Haworth & Snowden, 2010). Of particular context for the
current study is the demand by DSM-5 that information processing speed should be measured
with respect to attentional function. In this study, therefore, these questions are investigated
Intra-Individual Variability
In the research arena in addition to measuring information processing speed it has been
common to measure also its intra-individual variability (IIVRT). IIVRT like information processing
speed is also related to cognitive and neuroanatomical factors, with increased variability
commonly but not always, related to disease related ageing such as Alzheimer’s disease, and in
some cases, has been found to be more sensitive to ageing and or disease than mean information
processing speed per se (Luo et al., 2017; Tales & Basoudan, 2016). Although previous research
has examined IIVRT with respect to objectively measured cognitive function very little research
has examined the influence of subjective cognitive function and anxiety. This measure will thus
also be investigated in the present also be investigated in the present study considering gender
and level of education.
Attention
Attention is one of the cognitive functions most affected by ageing. The loss of function
in attention can impact a wide variety of cognitive activities and daily living functions (Akimoto
et al., 2014). Valeriani, Ranghi and Giaquinto (2003) identified differences in somatosensory
evoked potentials (SEPs) to median nerve stimulation between tasks requiring neutral
stimulation conditions and selective attention conditions for both older (mean age 71.7) and
younger (mean age 26.9) adults and abnormal attention function found in MCI and various
aetiologies of dementia (Tales, Bayer, Haworth & Snowden, 2010). Of particular context for the
current study is the demand by DSM-5 that information processing speed should be measured
with respect to attentional function. In this study, therefore, these questions are investigated
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
using a computer-based visual search task which allows measurement of attention-related choice
reaction time and attentional function (Therrien & Hunsley, 2011).
Anxiety
Anxiety prevalence and levels vary with respect to age and age-related conditions such as
subjective and objective cognitive impairment, and Alzheimer’s disease (AD). Estimates vary
from 1 to 28% depending on whether clinical or community-dwelling populations are used
(Bryant et al., 2008; Therrien & Hunsley, 2011; Wolitzky-Taylor, et al., 2010). Anxiety also
impact visuals search tasks, with generalized anxiety disorder patients showing slower RTs, but
not enhanced detection of threats (Rinck et al., 2003). There exists, however, a paucity of
evidence regarding the potential influence anxiety, especially non-clinical anxiety, may have
upon research outcome and therefore potentially clinical results and interpretation. Evidence
exists that associates anxiety with the ventral prefrontal cortex and the amygdala. These two
areas of the brain have greater activation in anxious situations as they are the main activation
sector to responses accorded by the brain (Guyer et al, 2008). Anxiety brings about an increase in
stimulus-driven processes that negatively impact efficient top-down control and consequently
have a detrimental effect on the ability to regulate emotional inhibitions (Ansari & Derakshan,
2011).
Anxiety also impact visuals search tasks, with generalized anxiety disorder patients
showing slower RTs, but not demonstrating enhanced detection of threats (Rinck et al., 2003).
Dennis, Scialfa and Ho (2004) found that older adults were no more reliant on bottom-up vs. top-
down learning in visual search tasks compared to younger adults, and were no more susceptible
to distractions.
using a computer-based visual search task which allows measurement of attention-related choice
reaction time and attentional function (Therrien & Hunsley, 2011).
Anxiety
Anxiety prevalence and levels vary with respect to age and age-related conditions such as
subjective and objective cognitive impairment, and Alzheimer’s disease (AD). Estimates vary
from 1 to 28% depending on whether clinical or community-dwelling populations are used
(Bryant et al., 2008; Therrien & Hunsley, 2011; Wolitzky-Taylor, et al., 2010). Anxiety also
impact visuals search tasks, with generalized anxiety disorder patients showing slower RTs, but
not enhanced detection of threats (Rinck et al., 2003). There exists, however, a paucity of
evidence regarding the potential influence anxiety, especially non-clinical anxiety, may have
upon research outcome and therefore potentially clinical results and interpretation. Evidence
exists that associates anxiety with the ventral prefrontal cortex and the amygdala. These two
areas of the brain have greater activation in anxious situations as they are the main activation
sector to responses accorded by the brain (Guyer et al, 2008). Anxiety brings about an increase in
stimulus-driven processes that negatively impact efficient top-down control and consequently
have a detrimental effect on the ability to regulate emotional inhibitions (Ansari & Derakshan,
2011).
Anxiety also impact visuals search tasks, with generalized anxiety disorder patients
showing slower RTs, but not demonstrating enhanced detection of threats (Rinck et al., 2003).
Dennis, Scialfa and Ho (2004) found that older adults were no more reliant on bottom-up vs. top-
down learning in visual search tasks compared to younger adults, and were no more susceptible
to distractions.
9
Subjective feelings of cognitive impairment
Subjective cognitive impairment (SCI), while not recognized as a mental disorder in the
DSM-V, may presage future decline in cognitive abilities. Symptoms of SCI reports are similar
to those for MCI: increasing level of forgetfulness, depression, overwhelmed feelings, etc.
(Stewart, 2012). SCI is considered subjective in nature because patients with SCI do not fail
objective tests of cognitive functioning, though they report cognitive lapses performing daily
cognitive tasks. Stewart (2012) noted that SCI is associated with some brain abnormalities
similar to those associated with dementia. Some underlying brain changes may be amenable to
interventions that slow or even stop further. An emerging area of research in ageing and
dementia is the characterization of subjective feelings of cognitive impairment and the
development of dementia and effects upon behaviour, daily living and social interaction
irrespective of aetiology (Torrens-Burton et al., 2017).
Methods
Participants
Participants included a group of younger (n =52) undergraduates chosen from the
psychology department at the University, with 31 females and 21 males (mean 19.9; s.d. 1.6;
range 18 to 25 years) and older adults (n =52) recruited from the general public, 32 females and
20 males (mean 66.5; s.d. 4.5; range 50 to 80 years). Exclusion criteria included severe
depression, poor self-reported general health; history of head injury or neurological, medical, or
psychological problems; medically diagnosed subjective cognitive impairment and self-reported
medications that impact cognitive functioning. All had normal or corrected to normal vision and
hearing.
Subjective feelings of cognitive impairment
Subjective cognitive impairment (SCI), while not recognized as a mental disorder in the
DSM-V, may presage future decline in cognitive abilities. Symptoms of SCI reports are similar
to those for MCI: increasing level of forgetfulness, depression, overwhelmed feelings, etc.
(Stewart, 2012). SCI is considered subjective in nature because patients with SCI do not fail
objective tests of cognitive functioning, though they report cognitive lapses performing daily
cognitive tasks. Stewart (2012) noted that SCI is associated with some brain abnormalities
similar to those associated with dementia. Some underlying brain changes may be amenable to
interventions that slow or even stop further. An emerging area of research in ageing and
dementia is the characterization of subjective feelings of cognitive impairment and the
development of dementia and effects upon behaviour, daily living and social interaction
irrespective of aetiology (Torrens-Burton et al., 2017).
Methods
Participants
Participants included a group of younger (n =52) undergraduates chosen from the
psychology department at the University, with 31 females and 21 males (mean 19.9; s.d. 1.6;
range 18 to 25 years) and older adults (n =52) recruited from the general public, 32 females and
20 males (mean 66.5; s.d. 4.5; range 50 to 80 years). Exclusion criteria included severe
depression, poor self-reported general health; history of head injury or neurological, medical, or
psychological problems; medically diagnosed subjective cognitive impairment and self-reported
medications that impact cognitive functioning. All had normal or corrected to normal vision and
hearing.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
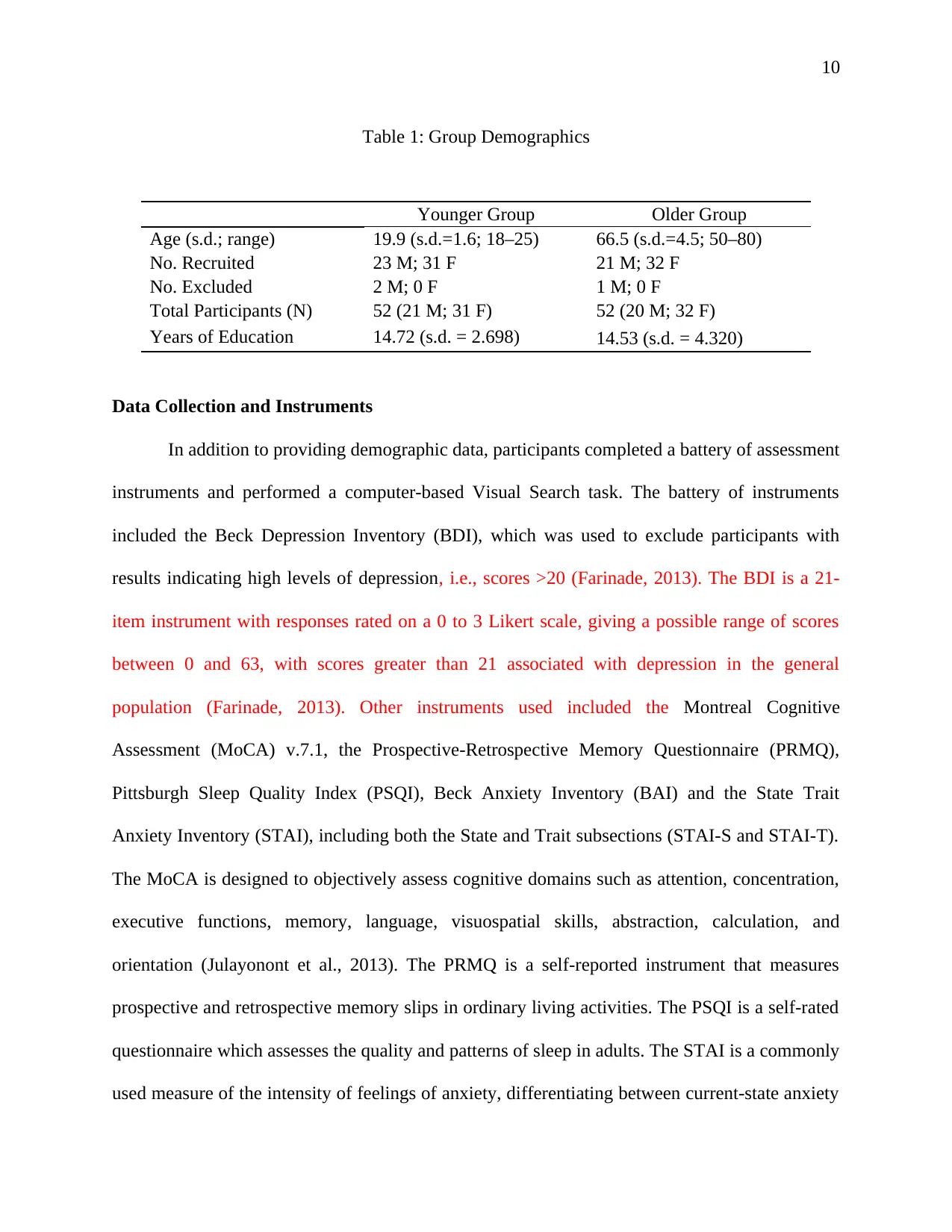
Table 1: Group Demographics
Younger Group Older Group
Age (s.d.; range) 19.9 (s.d.=1.6; 18–25) 66.5 (s.d.=4.5; 50–80)
No. Recruited 23 M; 31 F 21 M; 32 F
No. Excluded 2 M; 0 F 1 M; 0 F
Total Participants (N) 52 (21 M; 31 F) 52 (20 M; 32 F)
Years of Education 14.72 (s.d. = 2.698) 14.53 (s.d. = 4.320)
Data Collection and Instruments
In addition to providing demographic data, participants completed a battery of assessment
instruments and performed a computer-based Visual Search task. The battery of instruments
included the Beck Depression Inventory (BDI), which was used to exclude participants with
results indicating high levels of depression, i.e., scores >20 (Farinade, 2013). The BDI is a 21-
item instrument with responses rated on a 0 to 3 Likert scale, giving a possible range of scores
between 0 and 63, with scores greater than 21 associated with depression in the general
population (Farinade, 2013). Other instruments used included the Montreal Cognitive
Assessment (MoCA) v.7.1, the Prospective-Retrospective Memory Questionnaire (PRMQ),
Pittsburgh Sleep Quality Index (PSQI), Beck Anxiety Inventory (BAI) and the State Trait
Anxiety Inventory (STAI), including both the State and Trait subsections (STAI-S and STAI-T).
The MoCA is designed to objectively assess cognitive domains such as attention, concentration,
executive functions, memory, language, visuospatial skills, abstraction, calculation, and
orientation (Julayonont et al., 2013). The PRMQ is a self-reported instrument that measures
prospective and retrospective memory slips in ordinary living activities. The PSQI is a self-rated
questionnaire which assesses the quality and patterns of sleep in adults. The STAI is a commonly
used measure of the intensity of feelings of anxiety, differentiating between current-state anxiety
Table 1: Group Demographics
Younger Group Older Group
Age (s.d.; range) 19.9 (s.d.=1.6; 18–25) 66.5 (s.d.=4.5; 50–80)
No. Recruited 23 M; 31 F 21 M; 32 F
No. Excluded 2 M; 0 F 1 M; 0 F
Total Participants (N) 52 (21 M; 31 F) 52 (20 M; 32 F)
Years of Education 14.72 (s.d. = 2.698) 14.53 (s.d. = 4.320)
Data Collection and Instruments
In addition to providing demographic data, participants completed a battery of assessment
instruments and performed a computer-based Visual Search task. The battery of instruments
included the Beck Depression Inventory (BDI), which was used to exclude participants with
results indicating high levels of depression, i.e., scores >20 (Farinade, 2013). The BDI is a 21-
item instrument with responses rated on a 0 to 3 Likert scale, giving a possible range of scores
between 0 and 63, with scores greater than 21 associated with depression in the general
population (Farinade, 2013). Other instruments used included the Montreal Cognitive
Assessment (MoCA) v.7.1, the Prospective-Retrospective Memory Questionnaire (PRMQ),
Pittsburgh Sleep Quality Index (PSQI), Beck Anxiety Inventory (BAI) and the State Trait
Anxiety Inventory (STAI), including both the State and Trait subsections (STAI-S and STAI-T).
The MoCA is designed to objectively assess cognitive domains such as attention, concentration,
executive functions, memory, language, visuospatial skills, abstraction, calculation, and
orientation (Julayonont et al., 2013). The PRMQ is a self-reported instrument that measures
prospective and retrospective memory slips in ordinary living activities. The PSQI is a self-rated
questionnaire which assesses the quality and patterns of sleep in adults. The STAI is a commonly
used measure of the intensity of feelings of anxiety, differentiating between current-state anxiety
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
in the present moment and trait anxiety that is a general tendency to perceive situations as
threatening or anxiety-producing (McDowell, 2006). The full STAI has two scales, the STAI-S
Anxiety scale evaluates current state of anxiety, and the STAI-T Anxiety scale evaluates general,
long-lasting feelings of anxiety. The STAI is highly reliable in both scales, and across a variety
of samples, including older adults, working adults, general population, students, and others
(McDowell, 2006). The BAI measure is designed to distinguish between anxiety and depression
using a 21-item instrument with a 4-point Likert scale range, between 0 to 3. Total scores range
between 0 and 63, with scores between 0–9 indicating normal or no anxiety, 10–18 indicating
mild anxiety levels, 19–29 indicating moderate to severe anxiety, and 30 or greater indicating
severe anxiety (Julian, 2011).
Visual Search Task
For the purpose of computer-based visual search task, time which is taken to respond the
target in the context of isolation and irrelevant as well as distracting stimuli was determined. All
such investigation was conducted on a Dell Precision PC running Windows XP X86 CPU,
viewed at a distance of 57 cm. In order to meet the goals and objectives all trials were made
including black target. In this task, participants were shown a specific figure, either a left-
pointing or a right-pointing arrow. They were asked to determine whether the arrow pointed left
or right. The target appeared alone 8 times at each of the locations around the circle and 8 times
when it was surrounded by 7 distracting figures as shown in Figure 1. For recording time that is
taken for position the target when it is appeared alone and with 7 distracters clock face
configuration was used. In this, total number of 64 trials were made in which target is appearing
8 times at every clock face locations. Under half of the trials, distracters were presented, whereas
in the present moment and trait anxiety that is a general tendency to perceive situations as
threatening or anxiety-producing (McDowell, 2006). The full STAI has two scales, the STAI-S
Anxiety scale evaluates current state of anxiety, and the STAI-T Anxiety scale evaluates general,
long-lasting feelings of anxiety. The STAI is highly reliable in both scales, and across a variety
of samples, including older adults, working adults, general population, students, and others
(McDowell, 2006). The BAI measure is designed to distinguish between anxiety and depression
using a 21-item instrument with a 4-point Likert scale range, between 0 to 3. Total scores range
between 0 and 63, with scores between 0–9 indicating normal or no anxiety, 10–18 indicating
mild anxiety levels, 19–29 indicating moderate to severe anxiety, and 30 or greater indicating
severe anxiety (Julian, 2011).
Visual Search Task
For the purpose of computer-based visual search task, time which is taken to respond the
target in the context of isolation and irrelevant as well as distracting stimuli was determined. All
such investigation was conducted on a Dell Precision PC running Windows XP X86 CPU,
viewed at a distance of 57 cm. In order to meet the goals and objectives all trials were made
including black target. In this task, participants were shown a specific figure, either a left-
pointing or a right-pointing arrow. They were asked to determine whether the arrow pointed left
or right. The target appeared alone 8 times at each of the locations around the circle and 8 times
when it was surrounded by 7 distracting figures as shown in Figure 1. For recording time that is
taken for position the target when it is appeared alone and with 7 distracters clock face
configuration was used. In this, total number of 64 trials were made in which target is appearing
8 times at every clock face locations. Under half of the trials, distracters were presented, whereas
12
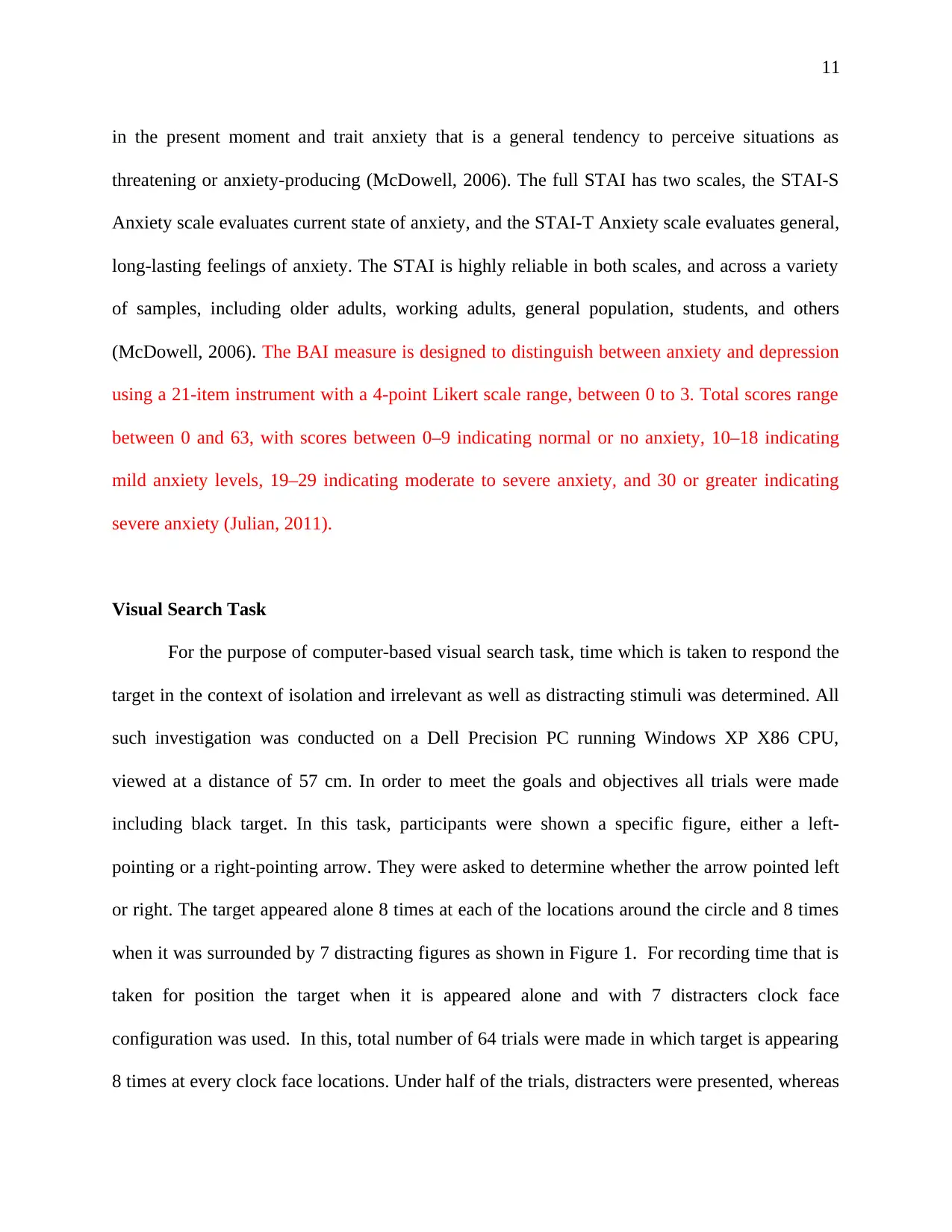
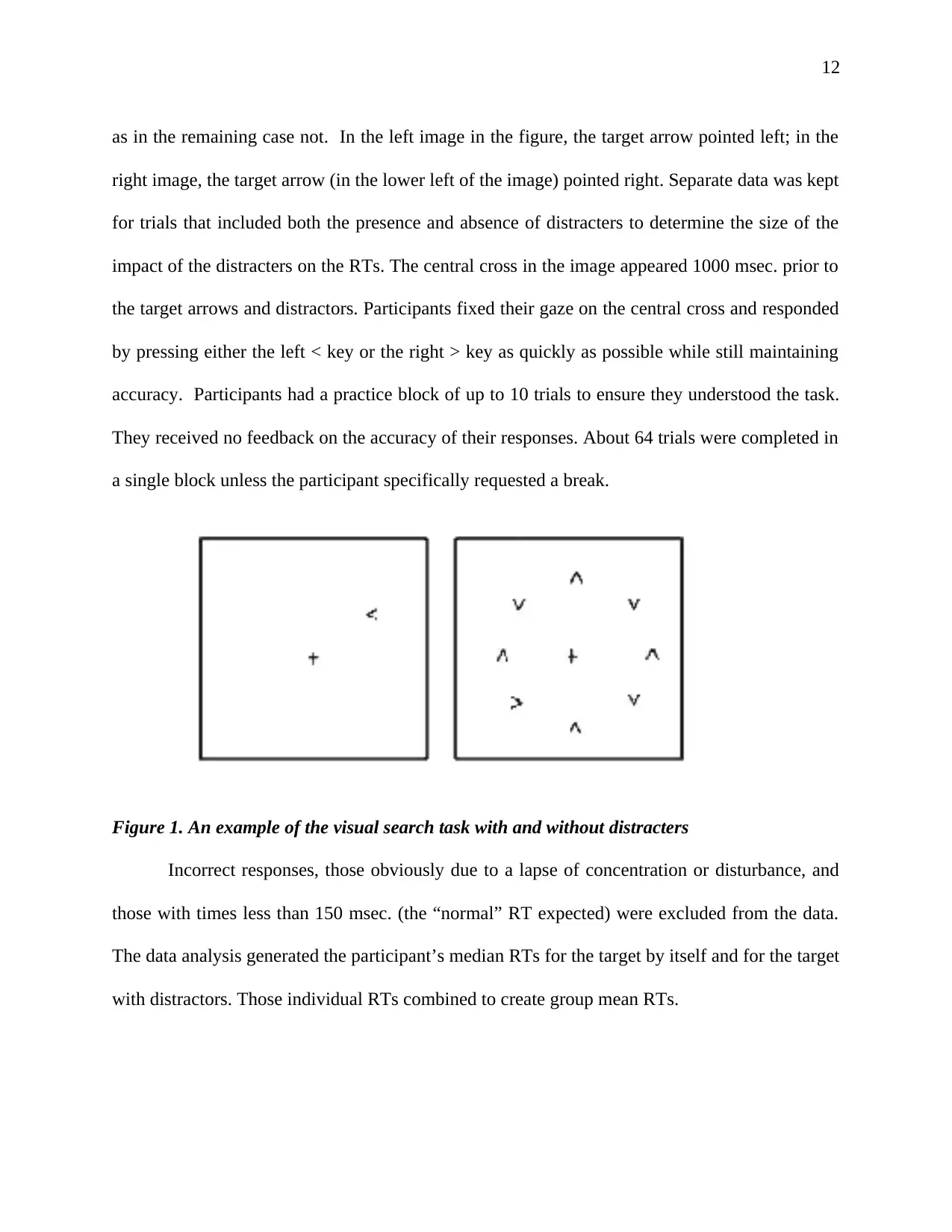
as in the remaining case not. In the left image in the figure, the target arrow pointed left; in the
right image, the target arrow (in the lower left of the image) pointed right. Separate data was kept
for trials that included both the presence and absence of distracters to determine the size of the
impact of the distracters on the RTs. The central cross in the image appeared 1000 msec. prior to
the target arrows and distractors. Participants fixed their gaze on the central cross and responded
by pressing either the left < key or the right > key as quickly as possible while still maintaining
accuracy. Participants had a practice block of up to 10 trials to ensure they understood the task.
They received no feedback on the accuracy of their responses. About 64 trials were completed in
a single block unless the participant specifically requested a break.
Figure 1. An example of the visual search task with and without distracters
Incorrect responses, those obviously due to a lapse of concentration or disturbance, and
those with times less than 150 msec. (the “normal” RT expected) were excluded from the data.
The data analysis generated the participant’s median RTs for the target by itself and for the target
with distractors. Those individual RTs combined to create group mean RTs.
as in the remaining case not. In the left image in the figure, the target arrow pointed left; in the
right image, the target arrow (in the lower left of the image) pointed right. Separate data was kept
for trials that included both the presence and absence of distracters to determine the size of the
impact of the distracters on the RTs. The central cross in the image appeared 1000 msec. prior to
the target arrows and distractors. Participants fixed their gaze on the central cross and responded
by pressing either the left < key or the right > key as quickly as possible while still maintaining
accuracy. Participants had a practice block of up to 10 trials to ensure they understood the task.
They received no feedback on the accuracy of their responses. About 64 trials were completed in
a single block unless the participant specifically requested a break.
Figure 1. An example of the visual search task with and without distracters
Incorrect responses, those obviously due to a lapse of concentration or disturbance, and
those with times less than 150 msec. (the “normal” RT expected) were excluded from the data.
The data analysis generated the participant’s median RTs for the target by itself and for the target
with distractors. Those individual RTs combined to create group mean RTs.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 32
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.