Comparative Study of Anxiety Levels in Young and Older Adults
VerifiedAdded on 2021/06/17
|34
|9370
|58
Report
AI Summary
This report investigates the disparities in non-clinical anxiety levels between young and older adults, examining their relationship with depression, cognitive functions, and demographic parameters. The study employed various assessment tools, including the Progressive Retrogressive Memory Questionnaire (PRMQ), Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), State and Trait Anxiety Inventory (STAI), Trait and Anxiety Inventory (TAI), and Montreal Cognitive Assessment (MoCA). The findings reveal that older adults exhibit lower susceptibility to subclinical anxiety and demonstrate better inhibitory cognitive control compared to younger adults. Demographic factors were found to have a minimal impact on non-clinical anxiety levels. The research highlights the significance of understanding these differences for developing effective interventions to mitigate the negative effects of anxiety and depression on cognitive performance across different age groups. The report also discusses the methodologies used, including participant selection, ethical considerations, and the instruments employed for data collection, providing a comprehensive overview of the research process and its outcomes.
CHAPTER TWO 1
Difference in Non-Clinical Anxiety Levels between Young and Older Adults and in
Respect to Depression, Cognitive Functions and Demographic Parameters
ABSTRACT
INTRODUCTION:
METHODS:
RESULTS:
CONCLUSION:
Keywords: Non-Clinical Anxiety, Depression, Subjective memory function, and Objective
Cognitive Function, Demographic Parameters, Younger adults, Older adults.
Difference in Non-Clinical Anxiety Levels between Young and Older Adults and in
Respect to Depression, Cognitive Functions and Demographic Parameters
ABSTRACT
INTRODUCTION:
METHODS:
RESULTS:
CONCLUSION:
Keywords: Non-Clinical Anxiety, Depression, Subjective memory function, and Objective
Cognitive Function, Demographic Parameters, Younger adults, Older adults.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 2
ABSTRACT
Relationship between anxiety levels and speed of information processing in young and older
adults has hardly been researched on, in relation to the plethora of brain functions that
encompass attention and other cognitive functions. This research taps into this gap,
evaluating the relationship between subclinical anxiety, cognitive functions and demographic
factors.
Methods used in data collection include Progressive Retrogressive Memory Questionnaire
(PRMQ), Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), State and Trait
Anxiety Inventory (STAI), Trait and Anxiety Inventory (TAI) and Montreal Cognitive
Assessment (MoCA). The results obtained from these methods were closely related,
confirming their reliability.
Older group was found to be less susceptible to different subclinical anxiety levels and its
effects than the younger group; inhibitory cognitive control is better managed by the older
group than the younger group. Demographic factors do not cause much non-clinical anxiety
as is seen in the results section.
ABSTRACT
Relationship between anxiety levels and speed of information processing in young and older
adults has hardly been researched on, in relation to the plethora of brain functions that
encompass attention and other cognitive functions. This research taps into this gap,
evaluating the relationship between subclinical anxiety, cognitive functions and demographic
factors.
Methods used in data collection include Progressive Retrogressive Memory Questionnaire
(PRMQ), Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), State and Trait
Anxiety Inventory (STAI), Trait and Anxiety Inventory (TAI) and Montreal Cognitive
Assessment (MoCA). The results obtained from these methods were closely related,
confirming their reliability.
Older group was found to be less susceptible to different subclinical anxiety levels and its
effects than the younger group; inhibitory cognitive control is better managed by the older
group than the younger group. Demographic factors do not cause much non-clinical anxiety
as is seen in the results section.
CHAPTER TWO 3
INTRODUCTION
This study aims at examining the difference in subclinical anxiety levels between young and
older adults in relation to depression, subjective memory function, objective cognitive
function and demographic factors, that isare, age, gender, years of education, handedness,
eyesight which are not extensively iterated in previous studies is also examined. . etc. we
also need to say, why it is important to look at all those terms and see the correlation between
them, before start looking at attention and information processing speed deeply. Does that
provide you a sign or and evidence re. non-clinical anxiety influences or something?The
primary objective of this research is to evaluate the existing association between the speed of
information processing and non-clinical anxiety levels, among older and younger adults, in
relation to plethora of brain functions that encompass attention. These functions are generally
related to visual attention, selective attention, inhibitory cognitive control, reaction time (RT)
and intra-individual reactive time (IIRT).
The research also aims to determine the relationship between the aforementioned non-clinical
anxiety levels and cognitive function, both subjective and objective, quality of sleep and
demographics such as age, gender, handedness, education levels or attainment and vision of
the participants.
Depression and anxiety disorders are linked with abnormal cognitive control in the form of an
attentional bias towards negative information and reduced inhibitory control (Cisler &
Koster, 2010). Even though there is a high rate for comorbidity of the anxiety disorders and
depression, above 75%, they have various underlying neural correlates. The high comorbidity
implies commonality in etiology (Peckham, McHugh & Otto, 2010). The dorsal anterior
cingulate cortex is involved in inhibitory cognitive control. It detects conflict between
INTRODUCTION
This study aims at examining the difference in subclinical anxiety levels between young and
older adults in relation to depression, subjective memory function, objective cognitive
function and demographic factors, that isare, age, gender, years of education, handedness,
eyesight which are not extensively iterated in previous studies is also examined. . etc. we
also need to say, why it is important to look at all those terms and see the correlation between
them, before start looking at attention and information processing speed deeply. Does that
provide you a sign or and evidence re. non-clinical anxiety influences or something?The
primary objective of this research is to evaluate the existing association between the speed of
information processing and non-clinical anxiety levels, among older and younger adults, in
relation to plethora of brain functions that encompass attention. These functions are generally
related to visual attention, selective attention, inhibitory cognitive control, reaction time (RT)
and intra-individual reactive time (IIRT).
The research also aims to determine the relationship between the aforementioned non-clinical
anxiety levels and cognitive function, both subjective and objective, quality of sleep and
demographics such as age, gender, handedness, education levels or attainment and vision of
the participants.
Depression and anxiety disorders are linked with abnormal cognitive control in the form of an
attentional bias towards negative information and reduced inhibitory control (Cisler &
Koster, 2010). Even though there is a high rate for comorbidity of the anxiety disorders and
depression, above 75%, they have various underlying neural correlates. The high comorbidity
implies commonality in etiology (Peckham, McHugh & Otto, 2010). The dorsal anterior
cingulate cortex is involved in inhibitory cognitive control. It detects conflict between
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CHAPTER TWO 4
competing neural representations in the perceptuo-motor system and gives a signal to the
dorso-lateral prefrontal cortex to help in adjusting the system to a regulated level.
Depression and clinical anxiety disorders are severe diseases that affect lives of people, both
mentally and physically (Association, 1998). Some symptoms appear in milder forms even
among individuals considered as psychologically healthy (Park et al., 2010). At the clinical
levels, anxiety and depression severely affect the inhibitory cognitive control (Eysneck &
Derakshan, 2007). The clinical symptoms show existence of some relationship withThere is
considerable decrease in activity within anterior cortical control structures which is
responsible for most cognitive functions including attention allocation, decision making,
impulse control etc. . For example, levels of clinical anxiety happen to inversely correlate to
dorsolateral prefrontal cortex (DIPFC) activity in a conflict task (Roma A., 2013). There
exists evidence of an inverse relationship between depression and resting-state activity
of the anterior cingulate cortex (ACC) (Robinson M. D., 2007). A highly depressed
individual has a hyperactive performance in the ACC, and at certain levels of anxiety and
depression, it goes into a resting state, bringing a halt to important cognitive functions like
attention allocation (Aaron T beck, Norman Epstein, & Robert a Steer, 1988). Moreover, as it
is evidenced that
Jjust like in clinical anxiety and depression, increased levels of subclinical anxiety and
depression symptoms occur together pointing to the likelihood of the same cause
(Pizzagalli et al., 2006). Taking this approach ends up in major theoretical challenges.
This is why most researchers treat the two as one, since they both point to the same
etiologies. in the interpretation of the finding that if anxiety and depression are related though
separate dysfunctions, then it means that their frequent co-occurrence results in considerable
muddle. Studies done by various authors (Sadock, 2009) and Anxiety And Depression
Association Of America (ADAA) show that anxiety and depression could have the same
competing neural representations in the perceptuo-motor system and gives a signal to the
dorso-lateral prefrontal cortex to help in adjusting the system to a regulated level.
Depression and clinical anxiety disorders are severe diseases that affect lives of people, both
mentally and physically (Association, 1998). Some symptoms appear in milder forms even
among individuals considered as psychologically healthy (Park et al., 2010). At the clinical
levels, anxiety and depression severely affect the inhibitory cognitive control (Eysneck &
Derakshan, 2007). The clinical symptoms show existence of some relationship withThere is
considerable decrease in activity within anterior cortical control structures which is
responsible for most cognitive functions including attention allocation, decision making,
impulse control etc. . For example, levels of clinical anxiety happen to inversely correlate to
dorsolateral prefrontal cortex (DIPFC) activity in a conflict task (Roma A., 2013). There
exists evidence of an inverse relationship between depression and resting-state activity
of the anterior cingulate cortex (ACC) (Robinson M. D., 2007). A highly depressed
individual has a hyperactive performance in the ACC, and at certain levels of anxiety and
depression, it goes into a resting state, bringing a halt to important cognitive functions like
attention allocation (Aaron T beck, Norman Epstein, & Robert a Steer, 1988). Moreover, as it
is evidenced that
Jjust like in clinical anxiety and depression, increased levels of subclinical anxiety and
depression symptoms occur together pointing to the likelihood of the same cause
(Pizzagalli et al., 2006). Taking this approach ends up in major theoretical challenges.
This is why most researchers treat the two as one, since they both point to the same
etiologies. in the interpretation of the finding that if anxiety and depression are related though
separate dysfunctions, then it means that their frequent co-occurrence results in considerable
muddle. Studies done by various authors (Sadock, 2009) and Anxiety And Depression
Association Of America (ADAA) show that anxiety and depression could have the same
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 5
or different causes or etiologies (Association, 1998), thus, it is acceptable to test the two
separately and compare results thereafter. Nonetheless, very few studies have focused
on determining the difference in anxiety level especially subclinical levels between young
and older adults. Coming up with a more conclusive distinction could help in developing
proper interventions aimed at minimizing the negative affective states of anxiety and
depression.We need to understand the difference between anxiety and depression terms, and
see how the levels of anxiety could lead to depression. We also need to clarify the big overlap
that exists between depression and anxiety as most studies normally treat them as one
disorder and a whole clinical illness. Coming up with a more conclusive distinction could
help in developing proper interventions aimed at minimizing the negative affective states of
anxiety and depression.
Anxiety and depression levels have been known to lower the cognitive performance of
people across all the age groups (Endler, Johnson, & Flett, 2001). These two emotions
have complex pathophysiology with many stimuli. Anatomically, emotions are
integrated by the limbic system. Well demonstrated by papiz circuit, cognition is a
higher function performed by the prefrontal cortex and involves formation of new
neurons and connections. Emotions and cognition share pathways depending on stimuli.
Anxiety and depression load the brain and cognition requires brain alertness. When the
two are active simultaneously, they interfere with C1 neurons and divert attention
making the brain less receptive and less effective in information integration (Shah A,
Jhawar, & Goel A, 2011). There is evidence of significant decline in cognitive abilities
among older adults considered to have anxiety disorders which result in cognitive
impairment (Price and Mohlman,2007). Apart from clinical experiments (Williams
JMG & MacLeod, 1998), subclinical anxiety levels have not been seriously researched
or different causes or etiologies (Association, 1998), thus, it is acceptable to test the two
separately and compare results thereafter. Nonetheless, very few studies have focused
on determining the difference in anxiety level especially subclinical levels between young
and older adults. Coming up with a more conclusive distinction could help in developing
proper interventions aimed at minimizing the negative affective states of anxiety and
depression.We need to understand the difference between anxiety and depression terms, and
see how the levels of anxiety could lead to depression. We also need to clarify the big overlap
that exists between depression and anxiety as most studies normally treat them as one
disorder and a whole clinical illness. Coming up with a more conclusive distinction could
help in developing proper interventions aimed at minimizing the negative affective states of
anxiety and depression.
Anxiety and depression levels have been known to lower the cognitive performance of
people across all the age groups (Endler, Johnson, & Flett, 2001). These two emotions
have complex pathophysiology with many stimuli. Anatomically, emotions are
integrated by the limbic system. Well demonstrated by papiz circuit, cognition is a
higher function performed by the prefrontal cortex and involves formation of new
neurons and connections. Emotions and cognition share pathways depending on stimuli.
Anxiety and depression load the brain and cognition requires brain alertness. When the
two are active simultaneously, they interfere with C1 neurons and divert attention
making the brain less receptive and less effective in information integration (Shah A,
Jhawar, & Goel A, 2011). There is evidence of significant decline in cognitive abilities
among older adults considered to have anxiety disorders which result in cognitive
impairment (Price and Mohlman,2007). Apart from clinical experiments (Williams
JMG & MacLeod, 1998), subclinical anxiety levels have not been seriously researched
CHAPTER TWO 6
on in relation to depression and cognitive impairment in a population-based sample
across all age groups. Non-clinical anxiety affects both subjective and objective
cognitive and memory processing ability of any individual, though no extensive research
has been done on effects of anxiety on attention and information processing speed.
Goldberg et al., (2003) compared the effect of anxiety and depression on cognitive
function of older and younger people and found that the cognitive ability of the
youngerolder group is lowered in relation to thought process, perception and general
problem solving, more than that of the olderyounger group. However, Unterrainer et al.,
(2018) differ with this observation based on the evidence from their study, that
subclinical low anxiety levels and cognitive function of people are not related regardless
of age. The associations they observed in clinical groups differed with ones in
population-based samples. Higher ratings of anxiety were associated with lower
planning performance independent of age. When they directly compared predictive
values of depression and anxiety on cognitive ability, significance was only attained by
anxiety while depression did not. The evidence from the two studies, Mattay et al.,
(2003) and Unterrainer et al., (2018) do not adequately explain the explain the difference
in effects of subclinical anxiety levels on cognitive function of individuals. Translational
threats of arbitrary shock paradigm and anxiety levels that cause them is examined in this
study, including the amount of emotional response caused by the different levels of anxiety.
This research explored this difference to help in better understanding of how different
levels of anxiety impair cognition and also help improve measures in place to treat
patients with cognitive problems caused by non-clinical anxiety and depression. Young
and old people have significant differences in how the anxiety levels affect their
cognitive abilities. Old people are less susceptible to different anxiety levels than young
on in relation to depression and cognitive impairment in a population-based sample
across all age groups. Non-clinical anxiety affects both subjective and objective
cognitive and memory processing ability of any individual, though no extensive research
has been done on effects of anxiety on attention and information processing speed.
Goldberg et al., (2003) compared the effect of anxiety and depression on cognitive
function of older and younger people and found that the cognitive ability of the
youngerolder group is lowered in relation to thought process, perception and general
problem solving, more than that of the olderyounger group. However, Unterrainer et al.,
(2018) differ with this observation based on the evidence from their study, that
subclinical low anxiety levels and cognitive function of people are not related regardless
of age. The associations they observed in clinical groups differed with ones in
population-based samples. Higher ratings of anxiety were associated with lower
planning performance independent of age. When they directly compared predictive
values of depression and anxiety on cognitive ability, significance was only attained by
anxiety while depression did not. The evidence from the two studies, Mattay et al.,
(2003) and Unterrainer et al., (2018) do not adequately explain the explain the difference
in effects of subclinical anxiety levels on cognitive function of individuals. Translational
threats of arbitrary shock paradigm and anxiety levels that cause them is examined in this
study, including the amount of emotional response caused by the different levels of anxiety.
This research explored this difference to help in better understanding of how different
levels of anxiety impair cognition and also help improve measures in place to treat
patients with cognitive problems caused by non-clinical anxiety and depression. Young
and old people have significant differences in how the anxiety levels affect their
cognitive abilities. Old people are less susceptible to different anxiety levels than young
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CHAPTER TWO 7
people as will be seen in results section, which is in concurrence with previous studies
(Administration, 2013). This is mostly because old people are more settled and do not
worry about life and all its troubles. They are more interested in living in peace and
integrity. Subjective and objective cognitive functions are key elements in this study
since they determine how anxiety levels influence cognitive functions of both old and
young groups.
Although anxiety has been investigated in ageing, young vs old, it has only been on
clinical levels or as a part of depression. Similarly, anxiety studies on ageing in relation to
demographic factors has only been on a clinical scale. This study works on the
subclinical anxiety level.
Most of the studies on effect of anxiety and depression on cognition have been on the
relation to anxiety in general but there is a recognized investigation that has mainly
targeted the adults (DiMatteo, Lepper, & Croghan, 2000). A number of studies on
anxiety and cognition have targeted individuals who have mild cognitive impairment
(MCI) and dementia, others focusing on formal anxiety disorders (Tales, & Basoudan,
2016). Non-clinical anxiety can affect elements of information processing than the ones
that were earlier recognized (Tales & Basoudan, 2016).
For a very long time most of the studies relating anxiety and age have focused on
subclinical level in the older adults. Few studies have focused on subclinical anxiety among
the youthyoung and older adults. Other studies have focused on effects of depressive
symptoms on cognition in the elderly (Sinn, Milte, Street, & Buckley, 2012) and looked at
anxiety as a part or one with od depression symptoms. Though anxiety and depression has
been associated with negative effect on cognition function, the correlation to the
subclinical anxiety level in the youth and older adults has not been exploredsubclinical
people as will be seen in results section, which is in concurrence with previous studies
(Administration, 2013). This is mostly because old people are more settled and do not
worry about life and all its troubles. They are more interested in living in peace and
integrity. Subjective and objective cognitive functions are key elements in this study
since they determine how anxiety levels influence cognitive functions of both old and
young groups.
Although anxiety has been investigated in ageing, young vs old, it has only been on
clinical levels or as a part of depression. Similarly, anxiety studies on ageing in relation to
demographic factors has only been on a clinical scale. This study works on the
subclinical anxiety level.
Most of the studies on effect of anxiety and depression on cognition have been on the
relation to anxiety in general but there is a recognized investigation that has mainly
targeted the adults (DiMatteo, Lepper, & Croghan, 2000). A number of studies on
anxiety and cognition have targeted individuals who have mild cognitive impairment
(MCI) and dementia, others focusing on formal anxiety disorders (Tales, & Basoudan,
2016). Non-clinical anxiety can affect elements of information processing than the ones
that were earlier recognized (Tales & Basoudan, 2016).
For a very long time most of the studies relating anxiety and age have focused on
subclinical level in the older adults. Few studies have focused on subclinical anxiety among
the youthyoung and older adults. Other studies have focused on effects of depressive
symptoms on cognition in the elderly (Sinn, Milte, Street, & Buckley, 2012) and looked at
anxiety as a part or one with od depression symptoms. Though anxiety and depression has
been associated with negative effect on cognition function, the correlation to the
subclinical anxiety level in the youth and older adults has not been exploredsubclinical
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 8
anxiety hasn’t been studied separately from depression (Balash et al., 2013). It is against
this background that the study examines the difference in subclinical anxiety level
between young and older adults and their links to depression, demographic parameters
and its effects on cognition. This study will also allow us to understand the differences
between young and old in terms of anxiety very well, in relation to many factors before
looking deeply on attention and information processing speed.
The aim of this research is to examine the non-clinical anxiety, and its effects on individuals
and on different degrees.
METHODS
This section briefly describes the methods used to conduct the investigation, including
participants, measuring instruments, and other details of how the research was
conducted.
Ethical Considerations
This study was conducted with the guidance and approval of the Research Ethics
Committee at the University Department of Psychology, which mandates informed
consent of all participants, along with their rights to withdraw from the study at any
time. The informed consent form was signed by all participants. All data collected in
this study was blinded to participant identity and stored under password protection on
the researcher’s computer. All the data is confidential and only accessible to responsible
authorities. All data collected was used for empirical research, and not for any medical
purpose.
anxiety hasn’t been studied separately from depression (Balash et al., 2013). It is against
this background that the study examines the difference in subclinical anxiety level
between young and older adults and their links to depression, demographic parameters
and its effects on cognition. This study will also allow us to understand the differences
between young and old in terms of anxiety very well, in relation to many factors before
looking deeply on attention and information processing speed.
The aim of this research is to examine the non-clinical anxiety, and its effects on individuals
and on different degrees.
METHODS
This section briefly describes the methods used to conduct the investigation, including
participants, measuring instruments, and other details of how the research was
conducted.
Ethical Considerations
This study was conducted with the guidance and approval of the Research Ethics
Committee at the University Department of Psychology, which mandates informed
consent of all participants, along with their rights to withdraw from the study at any
time. The informed consent form was signed by all participants. All data collected in
this study was blinded to participant identity and stored under password protection on
the researcher’s computer. All the data is confidential and only accessible to responsible
authorities. All data collected was used for empirical research, and not for any medical
purpose.
CHAPTER TWO 9
Participants
Two groups of participants were recruited, older and younger adults. The young group
comprised of students (n=52; age 18-25 years, 21 males: 31 females) recruited from the
Psychology Department at the University. The older group of participants (n=52; age
50-80 years, 31 females: 21 males) were recruited from the community. The average
age of the young individuals was 19.92 (SD=1.57) whereas that of older adults was 66.47
(SD=4.52). In the younger group, those who participated received 6 credits; older adult
participants received transportation expense assistance only. The young adults were
recruited through the Psychology Subject Pool System. while the older adults were
identified and approached by via emails and telephone; advertisement in local
newspapers, posters and flyers made the local population aware of the study while the
older adults were identified and approached by the department and requested if they would
want to be part of this study. The selection used inclusion criteria that involved
individuals who were not suffering from any clinical anxiety disorder and illustrated
regular medical visits indicating good health and no history of neurological and
cognitive visual impairments; the participants who exhibited severe depression and
previous history of poor health were excluded. Other exclusions included poor self-
reported general health; past history of head injury or neurological, medical, or
psychological problems; reported cognitive impairment; vision not normal or corrected
to normal; and self-reported medications that impact cognitive functioning. Two males
were excluded from the younger group and one male excluded from the older group due
to severe depression scores in Beck Depression Inventory (BDI). The participants were
briefed about the objectives of the study and its importance to the field of psychology.
After completing the study, debriefing forms were given to them. All the participants
had normal general cognition score (26 or above) that was measured through Montreal
Participants
Two groups of participants were recruited, older and younger adults. The young group
comprised of students (n=52; age 18-25 years, 21 males: 31 females) recruited from the
Psychology Department at the University. The older group of participants (n=52; age
50-80 years, 31 females: 21 males) were recruited from the community. The average
age of the young individuals was 19.92 (SD=1.57) whereas that of older adults was 66.47
(SD=4.52). In the younger group, those who participated received 6 credits; older adult
participants received transportation expense assistance only. The young adults were
recruited through the Psychology Subject Pool System. while the older adults were
identified and approached by via emails and telephone; advertisement in local
newspapers, posters and flyers made the local population aware of the study while the
older adults were identified and approached by the department and requested if they would
want to be part of this study. The selection used inclusion criteria that involved
individuals who were not suffering from any clinical anxiety disorder and illustrated
regular medical visits indicating good health and no history of neurological and
cognitive visual impairments; the participants who exhibited severe depression and
previous history of poor health were excluded. Other exclusions included poor self-
reported general health; past history of head injury or neurological, medical, or
psychological problems; reported cognitive impairment; vision not normal or corrected
to normal; and self-reported medications that impact cognitive functioning. Two males
were excluded from the younger group and one male excluded from the older group due
to severe depression scores in Beck Depression Inventory (BDI). The participants were
briefed about the objectives of the study and its importance to the field of psychology.
After completing the study, debriefing forms were given to them. All the participants
had normal general cognition score (26 or above) that was measured through Montreal
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CHAPTER TWO 10
Cognitive Assessment (MoCA). This approach detects objective cognitive functioning
and mild cognitive impairment and assesses such cognitive domains as attention,
concentration, executive functions, memory, language, visuospatial skills, abstraction,
calculation, and orientation (Julayonont et al., 2013). The instrument consists of a
variety of verbal and pencil-and-paper tasks such as drawing a clock, copying a
diagram of a cube, and doing delayed verbal recall of a list of words. Scoring ranges
from 0 to 30, with higher scores indicating less cognitive impairment (Julayanont and &
Nasreddine, 2017).
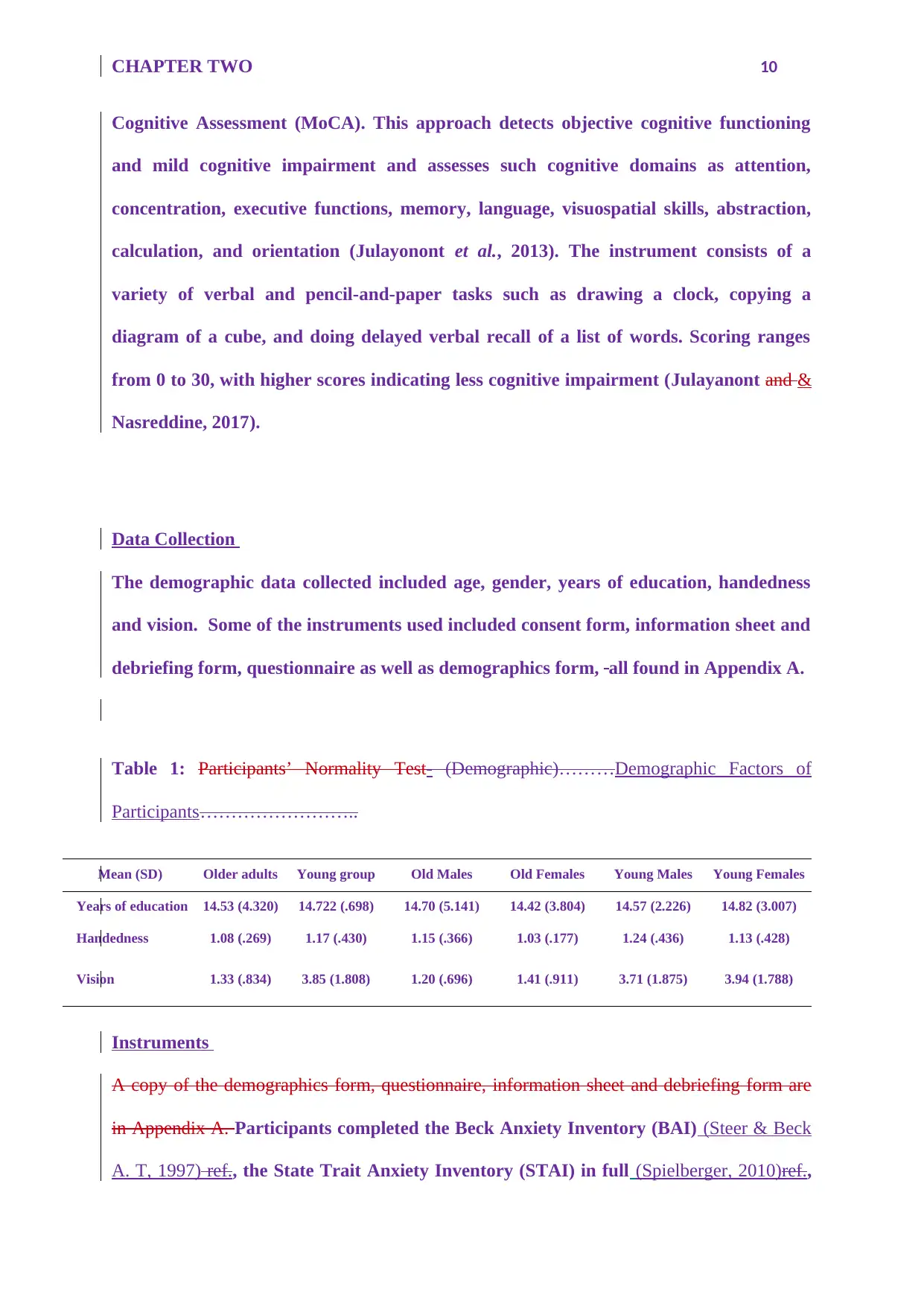
Data Collection
The demographic data collected included age, gender, years of education, handedness
and vision. Some of the instruments used included consent form, information sheet and
debriefing form, questionnaire as well as demographics form, all found in Appendix A.
Table 1: Participants’ Normality Test- (Demographic)………Demographic Factors of
Participants……………………..
Mean (SD) Older adults Young group Old Males Old Females Young Males Young Females
Years of education 14.53 (4.320) 14.722 (.698) 14.70 (5.141) 14.42 (3.804) 14.57 (2.226) 14.82 (3.007)
Handedness 1.08 (.269) 1.17 (.430) 1.15 (.366) 1.03 (.177) 1.24 (.436) 1.13 (.428)
Vision 1.33 (.834) 3.85 (1.808) 1.20 (.696) 1.41 (.911) 3.71 (1.875) 3.94 (1.788)
Instruments
A copy of the demographics form, questionnaire, information sheet and debriefing form are
in Appendix A. Participants completed the Beck Anxiety Inventory (BAI) (Steer & Beck
A. T, 1997) ref., the State Trait Anxiety Inventory (STAI) in full (Spielberger, 2010)ref.,
Cognitive Assessment (MoCA). This approach detects objective cognitive functioning
and mild cognitive impairment and assesses such cognitive domains as attention,
concentration, executive functions, memory, language, visuospatial skills, abstraction,
calculation, and orientation (Julayonont et al., 2013). The instrument consists of a
variety of verbal and pencil-and-paper tasks such as drawing a clock, copying a
diagram of a cube, and doing delayed verbal recall of a list of words. Scoring ranges
from 0 to 30, with higher scores indicating less cognitive impairment (Julayanont and &
Nasreddine, 2017).
Data Collection
The demographic data collected included age, gender, years of education, handedness
and vision. Some of the instruments used included consent form, information sheet and
debriefing form, questionnaire as well as demographics form, all found in Appendix A.
Table 1: Participants’ Normality Test- (Demographic)………Demographic Factors of
Participants……………………..
Mean (SD) Older adults Young group Old Males Old Females Young Males Young Females
Years of education 14.53 (4.320) 14.722 (.698) 14.70 (5.141) 14.42 (3.804) 14.57 (2.226) 14.82 (3.007)
Handedness 1.08 (.269) 1.17 (.430) 1.15 (.366) 1.03 (.177) 1.24 (.436) 1.13 (.428)
Vision 1.33 (.834) 3.85 (1.808) 1.20 (.696) 1.41 (.911) 3.71 (1.875) 3.94 (1.788)
Instruments
A copy of the demographics form, questionnaire, information sheet and debriefing form are
in Appendix A. Participants completed the Beck Anxiety Inventory (BAI) (Steer & Beck
A. T, 1997) ref., the State Trait Anxiety Inventory (STAI) in full (Spielberger, 2010)ref.,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 11
including both the State and Trait subsections (STAI-S and STAI-T), the Beck
Depression Inventory (BDI) (Beck, Aarno T, & Robert A, 1996)ref., the Montreal
Cognitive Assessment (MoCA) version 7.1 (Ziad S Nasreddine & Phillips, 2005)ref., and
the Prospective-Retrospective Memory Questionnaire (PRMQ) (Slavin-Mulford &
Hilsenroth, 2012). Each of these instruments is described below:
Beck Anxiety Inventory (BAI)
The Beck Anxiety Inventory (BAI) was used to determine participant anxiety levels
(Liang, Wang and Zhu, 2016). This test is a 21-item self-assessment using a four-point
Likert scale (0: “not at all” to 3: “severely”) that focuses on somatic symptoms of
anxiety as a way of distinguishing between anxiety and depression (Julian, 2011).
Scoring for the BAI is computed by adding the scores of the 21 items, and thus ranges
from 0 to 63, with higher scores indicating greater anxiety levels. A score between from
0–21 indicates no to mild anxiety; a score between 22 and 35 indicates moderate
anxiety; and a score between 36 and 63 indicates potentially severe anxiety (Beck, 1988.
Reliability of the BAI has been shown with high internal consistency as measured by
Cronbach’s alpha (0.90 to 0.94).
State and Trait Anxiety Inventory (STAI)
The STAI measures the intensity of feelings of anxiety, differentiating between current-
state anxiety in the present and trait anxiety that is a general tendency to perceive
situations as threatening or anxiety-producing (McDowell, 2006). The full STAI has two
separate 20-item scales, the STAI-S Anxiety scale that evaluates current state of anxiety,
and the STAI-T Anxiety scale that evaluates general, long-lasting feelings of anxiety
(Dennis, Coghlan and Vigod, 2013). Reliability of STAI is demonstrated in various
including both the State and Trait subsections (STAI-S and STAI-T), the Beck
Depression Inventory (BDI) (Beck, Aarno T, & Robert A, 1996)ref., the Montreal
Cognitive Assessment (MoCA) version 7.1 (Ziad S Nasreddine & Phillips, 2005)ref., and
the Prospective-Retrospective Memory Questionnaire (PRMQ) (Slavin-Mulford &
Hilsenroth, 2012). Each of these instruments is described below:
Beck Anxiety Inventory (BAI)
The Beck Anxiety Inventory (BAI) was used to determine participant anxiety levels
(Liang, Wang and Zhu, 2016). This test is a 21-item self-assessment using a four-point
Likert scale (0: “not at all” to 3: “severely”) that focuses on somatic symptoms of
anxiety as a way of distinguishing between anxiety and depression (Julian, 2011).
Scoring for the BAI is computed by adding the scores of the 21 items, and thus ranges
from 0 to 63, with higher scores indicating greater anxiety levels. A score between from
0–21 indicates no to mild anxiety; a score between 22 and 35 indicates moderate
anxiety; and a score between 36 and 63 indicates potentially severe anxiety (Beck, 1988.
Reliability of the BAI has been shown with high internal consistency as measured by
Cronbach’s alpha (0.90 to 0.94).
State and Trait Anxiety Inventory (STAI)
The STAI measures the intensity of feelings of anxiety, differentiating between current-
state anxiety in the present and trait anxiety that is a general tendency to perceive
situations as threatening or anxiety-producing (McDowell, 2006). The full STAI has two
separate 20-item scales, the STAI-S Anxiety scale that evaluates current state of anxiety,
and the STAI-T Anxiety scale that evaluates general, long-lasting feelings of anxiety
(Dennis, Coghlan and Vigod, 2013). Reliability of STAI is demonstrated in various
CHAPTER TWO 12
publications (McDowell, 2006). The STAI and the BAI are sometimes suggested to
measure different factors of anxiety (McDowell, 2006). In studies of young adults, the
validity comparison between the BAI and the sister measure BDI, the STAI correlated
more closely with BDI than with BAI, implying that the STAI is actually a closer
measure of depression than anxiety (McDowell, 2006). This measure identifies the
current state of trait anxiety. State anxiety stays for a designated time and often is
resolved (Allan et al., 2014). In comparison, trait anxiety lingers for a long time. The
measure can effectively track trait or state anxiety through differentiation. Therefore, if
any individual develops trait anxiety, it could be easily detected using this parameter.
Beck Depression Inventory (BDI)
The BDI is a 21-element self-reporting scale using a four-choice Likert scale (ranked
from 0 to 3). The possible scores range from 0 to 63, higher scores indicating greater or
more severe depression (de Oliveira and et.al., 2014). The questions in the BDI focus on
cognitive distortions common in those with depressive symptoms, such as “I blame
myself for everything bad that happens” (Farinde, 2013). It is designed for people who
are at least 13 years old, with scores greater than 21 indicating clinical depression, and
scores above 30 indicating severe depression. The BDI is designed to be simple to use
and quick to administer, taking less than 10 minutes (Farinde, 2013). The BDI has been
demonstrated to be valid and reliable in adolescent and elderly populations
(adolescents: Kauth & Zettle, 1990; elderly: Penk & Robinowitz, 1987; Scogin et al.,
1988; Wetherall & Gatz, 2005). Internal consistency of the BDI has been demonstrated
alphas approximating 0.91, and reliability in test-retest results over a one-week period
of 0.93.
publications (McDowell, 2006). The STAI and the BAI are sometimes suggested to
measure different factors of anxiety (McDowell, 2006). In studies of young adults, the
validity comparison between the BAI and the sister measure BDI, the STAI correlated
more closely with BDI than with BAI, implying that the STAI is actually a closer
measure of depression than anxiety (McDowell, 2006). This measure identifies the
current state of trait anxiety. State anxiety stays for a designated time and often is
resolved (Allan et al., 2014). In comparison, trait anxiety lingers for a long time. The
measure can effectively track trait or state anxiety through differentiation. Therefore, if
any individual develops trait anxiety, it could be easily detected using this parameter.
Beck Depression Inventory (BDI)
The BDI is a 21-element self-reporting scale using a four-choice Likert scale (ranked
from 0 to 3). The possible scores range from 0 to 63, higher scores indicating greater or
more severe depression (de Oliveira and et.al., 2014). The questions in the BDI focus on
cognitive distortions common in those with depressive symptoms, such as “I blame
myself for everything bad that happens” (Farinde, 2013). It is designed for people who
are at least 13 years old, with scores greater than 21 indicating clinical depression, and
scores above 30 indicating severe depression. The BDI is designed to be simple to use
and quick to administer, taking less than 10 minutes (Farinde, 2013). The BDI has been
demonstrated to be valid and reliable in adolescent and elderly populations
(adolescents: Kauth & Zettle, 1990; elderly: Penk & Robinowitz, 1987; Scogin et al.,
1988; Wetherall & Gatz, 2005). Internal consistency of the BDI has been demonstrated
alphas approximating 0.91, and reliability in test-retest results over a one-week period
of 0.93.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 34
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.