Report on Autosomal Recessive Familial Hypercholesterolemia (ARH)
VerifiedAdded on 2023/06/13
|19
|4804
|317
Report
AI Summary
This report provides an overview of autosomal recessive familial hypercholesterolemia (ARH), a rare genetic disorder characterized by elevated serum cholesterol levels. It details the role of the LDLRAP1 gene, its cytogenic properties, and its impact on cholesterol metabolism. The report also examines the prevalence of ARH, particularly in regions like Saudi Arabia, where consanguineous marriages contribute to higher incidence rates. Diagnostic methods, including clinical and molecular analyses, are discussed, along with treatment options. Family and twin studies are referenced to emphasize the genetic basis of the disease. The report concludes with a summary of the key aspects of ARH, highlighting its clinical manifestations and management strategies.
[Type text]
Autosomal Recessive Familial Hypercholesterolemia
By: Faten AlQahtani
1801412
Autosomal Recessive Familial Hypercholesterolemia
By: Faten AlQahtani
1801412
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Autosomal recessive familial hypercholesterolemia
Table of contents
Table of Abbreviation ………………………………………………………….…………………2
Table of figures …………………………………………………………………………………...3
Abstract……………………………………………………………………………………………4
Introduction………………………………………………………………..………………………5
Prevalence in the World…………………………………………………..…………… …………6
Prevalence of Familial Hypercholesterolemia in Saudi Arabia…...………………………………7
Diagnosis…………………………………………………………………………………………..9
Low-density Lipoprotein Receptor Adaptor Protein 1(LDLRAP1)………………………..……10
Family study and twins study in ARH………………………………………………...…………13
Treatment…………………………………………………………………………………..…….14
Conclusion…………………………………………...…………………………………………..15
References………………………………………………………………………………………..17
1 | P a g e
Table of contents
Table of Abbreviation ………………………………………………………….…………………2
Table of figures …………………………………………………………………………………...3
Abstract……………………………………………………………………………………………4
Introduction………………………………………………………………..………………………5
Prevalence in the World…………………………………………………..…………… …………6
Prevalence of Familial Hypercholesterolemia in Saudi Arabia…...………………………………7
Diagnosis…………………………………………………………………………………………..9
Low-density Lipoprotein Receptor Adaptor Protein 1(LDLRAP1)………………………..……10
Family study and twins study in ARH………………………………………………...…………13
Treatment…………………………………………………………………………………..…….14
Conclusion…………………………………………...…………………………………………..15
References………………………………………………………………………………………..17
1 | P a g e
Autosomal recessive familial hypercholesterolemia
Table of Abbreviation
LDLRAP1 Low-Density Lipoprotein Receptor Adaptor Protein 1
LDL-C Low-Density Lipoprotein Cholesterol
CVD Cardiovascular Disease
LDLR Low-Density Lipoprotein Receptor
LDLs Low-Density Lipoproteins
APOB Apolipoprotein B
PCSK9 Proprotein Convertase Subtilisin/Kexin Type 9
ARH Autosomal Recessive Hypercholesterolemia
APOA Apolipoprotein A
HeFH Heterozygous Familial Hypercholesterolemia
HoFH Homozygous Familial Hypercholesterolemia
FH Familial Hypercholesterolemia
MEDPED Make Early Diagnosis to Prevent Early Deaths
DLCN Dutch Lipid Clinic Network
NGS Next-Generation Sequencing
PTD Phosphotyrosine Binding Domain
2 | P a g e
Table of Abbreviation
LDLRAP1 Low-Density Lipoprotein Receptor Adaptor Protein 1
LDL-C Low-Density Lipoprotein Cholesterol
CVD Cardiovascular Disease
LDLR Low-Density Lipoprotein Receptor
LDLs Low-Density Lipoproteins
APOB Apolipoprotein B
PCSK9 Proprotein Convertase Subtilisin/Kexin Type 9
ARH Autosomal Recessive Hypercholesterolemia
APOA Apolipoprotein A
HeFH Heterozygous Familial Hypercholesterolemia
HoFH Homozygous Familial Hypercholesterolemia
FH Familial Hypercholesterolemia
MEDPED Make Early Diagnosis to Prevent Early Deaths
DLCN Dutch Lipid Clinic Network
NGS Next-Generation Sequencing
PTD Phosphotyrosine Binding Domain
2 | P a g e
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Autosomal recessive familial hypercholesterolemia
Table of figures
Fig 1. The estimated prevalence of Familial Hypercholesterolemia in Saudi Arabia. A.
Expected Heterozygous Familial Hypercholesterolemia (HeFH) cases. B. Expected
Homozygous Familial Hypercholesterolemia (HoFH) cases; (Alallaf et al, 2017).
The Spectrum of Familial Hypercholesterolemia (FH) in Saudi Arabia: Prime Time
for Patient FH Registry. The open cardiovascular medicine journal, 11, pp.66-75.
Fig.2 LDLRAP1 gene. a.CytogenicLocation of LDLRAP1gene on the short (p) arm of
chromosome 1 at position 36.11. b. Represented exons. c. Mutations seen in
LDLRAP1 (Henderson et al, 2016). The genetics and screening of familial
hypercholesterolemia. Journal of biomedical science, 23(1), p.39.
3 | P a g e
Table of figures
Fig 1. The estimated prevalence of Familial Hypercholesterolemia in Saudi Arabia. A.
Expected Heterozygous Familial Hypercholesterolemia (HeFH) cases. B. Expected
Homozygous Familial Hypercholesterolemia (HoFH) cases; (Alallaf et al, 2017).
The Spectrum of Familial Hypercholesterolemia (FH) in Saudi Arabia: Prime Time
for Patient FH Registry. The open cardiovascular medicine journal, 11, pp.66-75.
Fig.2 LDLRAP1 gene. a.CytogenicLocation of LDLRAP1gene on the short (p) arm of
chromosome 1 at position 36.11. b. Represented exons. c. Mutations seen in
LDLRAP1 (Henderson et al, 2016). The genetics and screening of familial
hypercholesterolemia. Journal of biomedical science, 23(1), p.39.
3 | P a g e
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Autosomal recessive familial hypercholesterolemia
Abstract
Autosomal recessive familial hypercholesterolemia is a rare genetic disease that poses an
incremental risk to the general health. This paper aims at providing a detailed background to the
condition including its characterization and manifestation. The article further focuses on
highlighting the prevalence of the disease in highly endemic regions like Saudi Arabia
andtheworldwide epidemiological impact of the condition. In addition to dealing with the
relevance of LDLRAP1 gene in determining the discourse of familial hypercholesterolemia, this
assignment will focus on analyzing the cytogenic properties of the gene, its discovery and its
specific role in the pathophysiology of autosomal recessive familial hypercholesterolemia. The
overall purpose of family and twin studies will also be integrated into the paper to provide an
emphasis on the genetic baselines of the disease under discussion. Finally, the treatment will be
described as well as a conclusive summary of the disease under discussion.
4 | P a g e
Abstract
Autosomal recessive familial hypercholesterolemia is a rare genetic disease that poses an
incremental risk to the general health. This paper aims at providing a detailed background to the
condition including its characterization and manifestation. The article further focuses on
highlighting the prevalence of the disease in highly endemic regions like Saudi Arabia
andtheworldwide epidemiological impact of the condition. In addition to dealing with the
relevance of LDLRAP1 gene in determining the discourse of familial hypercholesterolemia, this
assignment will focus on analyzing the cytogenic properties of the gene, its discovery and its
specific role in the pathophysiology of autosomal recessive familial hypercholesterolemia. The
overall purpose of family and twin studies will also be integrated into the paper to provide an
emphasis on the genetic baselines of the disease under discussion. Finally, the treatment will be
described as well as a conclusive summary of the disease under discussion.
4 | P a g e
Autosomal recessive familial hypercholesterolemia
Introduction
Familial hypercholesterolemia is a genetically acquired disease that is characterized by
elevated levels of serum cholesterol although in most cases, triglyceride levels are within the
normal range(Tada et al., 2015). Cholesterol is a fat-like and waxy substance that can be
obtained from exogenous sources such as foods products from animals mainly meat, dairy
products, egg yolks, and fish (Pusey, 2006). However, due to endogenous mechanisms, the body
produces cholesterol through the gastrointestinal food metabolism (Clifton et al., 2014).
Cholesterol plays a significant role in the body’s physiology and anatomy. It is essential in the
processing of several hormones, building cell membranes, and producing compounds that
facilitate lipolysis (Sherwood, 2015). In contrast, extreme elevation of cholesterol in the
bloodstream contributes to the elevation of low-density lipoprotein cholesterol (LDL-C)
commonly known as bad cholesterol. Consequently, high levels of LDL-C is attributed to the
deposition of cholesterol on the arterial walls particularly the coronary arteries thus increasing
the risk for accelerated atherosclerosis and cardiovascular disease (CVD)(Alallaf et al., 2017). In
addition, inherited hypercholesterolemia causes excess systemic cholesterol buildup. For
instance, tendon xanthomas result from the accumulation of cholesterol in the tendons while
cholesterol deposits under the eyelids skin and in the cornea result in xanthelasmata and arcus
cornealis respectively(Tada et al., 2015). This defects show the grave importance of analyzing
the pathophysiology of familial hypercholesterolemia.
As a primary cause of inherited high cholesterol, familial hypercholesterolemia results
from the mutation of the LDLR gene which is responsible for the synthesis of the low-density
5 | P a g e
Introduction
Familial hypercholesterolemia is a genetically acquired disease that is characterized by
elevated levels of serum cholesterol although in most cases, triglyceride levels are within the
normal range(Tada et al., 2015). Cholesterol is a fat-like and waxy substance that can be
obtained from exogenous sources such as foods products from animals mainly meat, dairy
products, egg yolks, and fish (Pusey, 2006). However, due to endogenous mechanisms, the body
produces cholesterol through the gastrointestinal food metabolism (Clifton et al., 2014).
Cholesterol plays a significant role in the body’s physiology and anatomy. It is essential in the
processing of several hormones, building cell membranes, and producing compounds that
facilitate lipolysis (Sherwood, 2015). In contrast, extreme elevation of cholesterol in the
bloodstream contributes to the elevation of low-density lipoprotein cholesterol (LDL-C)
commonly known as bad cholesterol. Consequently, high levels of LDL-C is attributed to the
deposition of cholesterol on the arterial walls particularly the coronary arteries thus increasing
the risk for accelerated atherosclerosis and cardiovascular disease (CVD)(Alallaf et al., 2017). In
addition, inherited hypercholesterolemia causes excess systemic cholesterol buildup. For
instance, tendon xanthomas result from the accumulation of cholesterol in the tendons while
cholesterol deposits under the eyelids skin and in the cornea result in xanthelasmata and arcus
cornealis respectively(Tada et al., 2015). This defects show the grave importance of analyzing
the pathophysiology of familial hypercholesterolemia.
As a primary cause of inherited high cholesterol, familial hypercholesterolemia results
from the mutation of the LDLR gene which is responsible for the synthesis of the low-density
5 | P a g e
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Autosomal recessive familial hypercholesterolemia
lipoprotein receptor (Di Taranto et al., 2015) .The latter plays a vital role in the clearance of
cholesterol from the bloodstream since the receptor binds to the low-density lipoproteins (LDLs)
which serve as cholesterol carriers (Tada et al., 2015). Ultimately, the removal of the LDLs from
the blood acts as a homeostatic mechanism for the apparent regulation of cholesterol level.
However, as previously stated, mutations in the LDLR genes lower the number of LDL receptors
as well as disrupt the process of LDL removal from the bloodstream leading to the accumulation
of cholesterol (Santos et al, 2016).Besides LDLR, other gene mutations that have implicated in
familial hypercholesterolemia include alteration in the low-density lipoprotein receptor adaptor
protein 1(LDLRAP1). Also, Apolipoprotein B (APOB) and Proprotein Convertase
Subtilisin/Kexin Type 9 (PCSK9) genes leading to the broader classification of the inherited
hypercholesterolemia disorders(Santos et al, 2016) .Autosomal recessive hypercholesterolemia
(ARH) is a rare defect where a person is born with two muted copies of the LDLRAP1 gene in
each cell. LDLRAP1 is a gene that encodes Apolipoprotein A (APOA), a specific clathrin
adaptor protein(Tada et al., 2015) .However, patients with ARH carry two defective alleles of the
gene resulting in the inability to internalize the LDL receptor(Alallaf et al., 2017).
Prevalence in the World
Globally, autosomal recessive hypercholesterolemia has rarely occurred in comparison to
the autosomal dominant familial hypercholesterolemia (Gidding et al., 2015). The latter is
relatively common since heterozygous carriers of the defective genes are clinically affected with
an estimate of the two-fold increase in average levels of serum cholesterol with ranges of 250-
450 mg/dL or 6.5-11.6 mmol/L(Alallaf et al., 2017).On the other hand, autosomal recessive
hypercholesterolemia has severe clinical manifestations with an approximate four-to-fivefold
elevation of normal cholesterol to above 400mg/dL(Tada et al., 2015) .Due to its severity, ARH
6 | P a g e
lipoprotein receptor (Di Taranto et al., 2015) .The latter plays a vital role in the clearance of
cholesterol from the bloodstream since the receptor binds to the low-density lipoproteins (LDLs)
which serve as cholesterol carriers (Tada et al., 2015). Ultimately, the removal of the LDLs from
the blood acts as a homeostatic mechanism for the apparent regulation of cholesterol level.
However, as previously stated, mutations in the LDLR genes lower the number of LDL receptors
as well as disrupt the process of LDL removal from the bloodstream leading to the accumulation
of cholesterol (Santos et al, 2016).Besides LDLR, other gene mutations that have implicated in
familial hypercholesterolemia include alteration in the low-density lipoprotein receptor adaptor
protein 1(LDLRAP1). Also, Apolipoprotein B (APOB) and Proprotein Convertase
Subtilisin/Kexin Type 9 (PCSK9) genes leading to the broader classification of the inherited
hypercholesterolemia disorders(Santos et al, 2016) .Autosomal recessive hypercholesterolemia
(ARH) is a rare defect where a person is born with two muted copies of the LDLRAP1 gene in
each cell. LDLRAP1 is a gene that encodes Apolipoprotein A (APOA), a specific clathrin
adaptor protein(Tada et al., 2015) .However, patients with ARH carry two defective alleles of the
gene resulting in the inability to internalize the LDL receptor(Alallaf et al., 2017).
Prevalence in the World
Globally, autosomal recessive hypercholesterolemia has rarely occurred in comparison to
the autosomal dominant familial hypercholesterolemia (Gidding et al., 2015). The latter is
relatively common since heterozygous carriers of the defective genes are clinically affected with
an estimate of the two-fold increase in average levels of serum cholesterol with ranges of 250-
450 mg/dL or 6.5-11.6 mmol/L(Alallaf et al., 2017).On the other hand, autosomal recessive
hypercholesterolemia has severe clinical manifestations with an approximate four-to-fivefold
elevation of normal cholesterol to above 400mg/dL(Tada et al., 2015) .Due to its severity, ARH
6 | P a g e
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Autosomal recessive familial hypercholesterolemia
has been highlighted as the significant contributor to the emerging cases of aortic valve stenosis,
coronary artery disease, and cutaneous xanthoma in childhood(Tada et al., 2015) .Statistically,
autosomal dominant hypercholesterolemia affects approximately in 1:250 to 1:500 individuals
while autosomal recessive hypercholesterolemia has an estimated prevalence ratio of 1:1,000,000
live births(Kosmas, 2017).Research findings indicate that up to date, not more than 10,000 cases
of ARH have been reported with the affected geographical populations being the Mexicans,
Lebanese, Indians, Italian, Turkish, and the Syrians(Kosmas, 2017). In addition, current literature
indicates that only 36 families with 14 different mutations have been reported
worldwide(Kosmas, 2017).However, the clinical similarities between ARH and the autosomal
dominant hypercholesterolemia among populations necessitate the implementation of statins as
lipid-lowering treatment in addition to the conventional dietary monitoring strategies during
patient management(Alallaf et al., 2017).
Prevalence of Familial Hypercholesterolemia in Saudi Arabia
Familial hypercholesterolemia is among the leading causes of premature cardiovascular
disease in Saudi Arabia(Alallaf et al., 2017). Familial hypercholesterolemia has been reported to
be a dominant genetic disease of potential morbidity and mortality (Henneman et al, 2015).
According to the International Familial Hypercholesterolemia Foundation, the cases of familial
hypercholesterolemia are often undiagnosed or misdiagnosed in Saudi Arabia. Although no
evidence in literature provides the exact frequency of familial hypercholesterolemia in Saudi
Arabia, the figures in developed countries are used to give the country’s estimates(Alallaf et al.,
2017). Based on the 2015 population census report, in the United States, the prevalence of the
disease was approximately 1 case per 500 people (Batais et al., 2017) .With the overall
population of 25,795, 938 in Saudi Arabia, the prevalence in the latter would be estimated as
7 | P a g e
has been highlighted as the significant contributor to the emerging cases of aortic valve stenosis,
coronary artery disease, and cutaneous xanthoma in childhood(Tada et al., 2015) .Statistically,
autosomal dominant hypercholesterolemia affects approximately in 1:250 to 1:500 individuals
while autosomal recessive hypercholesterolemia has an estimated prevalence ratio of 1:1,000,000
live births(Kosmas, 2017).Research findings indicate that up to date, not more than 10,000 cases
of ARH have been reported with the affected geographical populations being the Mexicans,
Lebanese, Indians, Italian, Turkish, and the Syrians(Kosmas, 2017). In addition, current literature
indicates that only 36 families with 14 different mutations have been reported
worldwide(Kosmas, 2017).However, the clinical similarities between ARH and the autosomal
dominant hypercholesterolemia among populations necessitate the implementation of statins as
lipid-lowering treatment in addition to the conventional dietary monitoring strategies during
patient management(Alallaf et al., 2017).
Prevalence of Familial Hypercholesterolemia in Saudi Arabia
Familial hypercholesterolemia is among the leading causes of premature cardiovascular
disease in Saudi Arabia(Alallaf et al., 2017). Familial hypercholesterolemia has been reported to
be a dominant genetic disease of potential morbidity and mortality (Henneman et al, 2015).
According to the International Familial Hypercholesterolemia Foundation, the cases of familial
hypercholesterolemia are often undiagnosed or misdiagnosed in Saudi Arabia. Although no
evidence in literature provides the exact frequency of familial hypercholesterolemia in Saudi
Arabia, the figures in developed countries are used to give the country’s estimates(Alallaf et al.,
2017). Based on the 2015 population census report, in the United States, the prevalence of the
disease was approximately 1 case per 500 people (Batais et al., 2017) .With the overall
population of 25,795, 938 in Saudi Arabia, the prevalence in the latter would be estimated as
7 | P a g e

Autosomal recessive familial hypercholesterolemia
51,591 autosomal dominant cases. On the other hand, with the 1: 300,000-600,000 ratios of
autosomal recessive hypercholesterolemia, the expected examples of ARH in Saudi Arabia
would be 56 to 106 (see fig.1)(Alallaf et al., 2017).The high prevalence in the country is
attributed to the culture of consanguineous marriages which increase the chances of the transfer
of mutated genes along the family pedigree. However, unavailability of data for the statistical
analysis of familial hypercholesterolemia in Saudi Arabia is mainly due to the lack of genetic
screening and national registries for the disease(Alallaf et al., 2017).Research indicates that
currently, more than eighty molecularly and clinically confirmed cases of homozygous familial
hypercholesterolemia are undergoing LDL-apheresis treatment after every two weeks in a single
center located in Riyadh, the capital city of Saudi Arabia(Alallaf et al., 2017).Moreover, the
increasing rates of the wrongdiagnosis have been attributed to the substantial deficit in the
knowledge, awareness, and detection of familial hypercholesterolemia among practicing
clinicians in Saudi Arabia(Batais et al., 2017).
Fig 1. The estimated prevalence of Familial Hypercholesterolemia in Saudi Arabia. A.
Expected Heterozygous Familial Hypercholesterolemia (HeFH) cases. B. Expected
Homozygous Familial Hypercholesterolemia (HoFH) cases; (Alallaf et al, 2017). The
Spectrum of Familial Hypercholesterolemia (FH) in Saudi Arabia: Prime Time for
Patient FH Registry. The open cardiovascular medicine journal, 11, pp.66-75.
8 | P a g e
51,591 autosomal dominant cases. On the other hand, with the 1: 300,000-600,000 ratios of
autosomal recessive hypercholesterolemia, the expected examples of ARH in Saudi Arabia
would be 56 to 106 (see fig.1)(Alallaf et al., 2017).The high prevalence in the country is
attributed to the culture of consanguineous marriages which increase the chances of the transfer
of mutated genes along the family pedigree. However, unavailability of data for the statistical
analysis of familial hypercholesterolemia in Saudi Arabia is mainly due to the lack of genetic
screening and national registries for the disease(Alallaf et al., 2017).Research indicates that
currently, more than eighty molecularly and clinically confirmed cases of homozygous familial
hypercholesterolemia are undergoing LDL-apheresis treatment after every two weeks in a single
center located in Riyadh, the capital city of Saudi Arabia(Alallaf et al., 2017).Moreover, the
increasing rates of the wrongdiagnosis have been attributed to the substantial deficit in the
knowledge, awareness, and detection of familial hypercholesterolemia among practicing
clinicians in Saudi Arabia(Batais et al., 2017).
Fig 1. The estimated prevalence of Familial Hypercholesterolemia in Saudi Arabia. A.
Expected Heterozygous Familial Hypercholesterolemia (HeFH) cases. B. Expected
Homozygous Familial Hypercholesterolemia (HoFH) cases; (Alallaf et al, 2017). The
Spectrum of Familial Hypercholesterolemia (FH) in Saudi Arabia: Prime Time for
Patient FH Registry. The open cardiovascular medicine journal, 11, pp.66-75.
8 | P a g e
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Autosomal recessive familial hypercholesterolemia
Diagnosis
The diagnosis of autosomal recessive familial hypercholesterolemia not only depends on
biochemistry tests but mainly on the clinical and molecular analyses(Alallaf et al., 2017).
Conventionally, biochemistry screening tests that analyze the lipid profile to determine
cholesterol levels are considered insufficient to make a diagnosis for familial
hypercholesterolemia conclusively. Mainly because of factors such as age, gender, certain drugs,
ethnicity, pathological and physiological conditions which contribute to the variation of the
results, ultimately leading to false negative or false positive values(Alallaf et al., 2017).The
clinical criteria is to integrate the reports of repeated measurements of very high LDL-C or total
cholesterol levels with the presence of xanthomas as well as considering family histories of signs
and symptoms of dyslipidemia in making the diagnosis(Alallaf et al., 2017).Based on the clinical
criteria, there exist conventional diagnostic systems that are applied in the determination of
familial hypercholesterolemia(Alallaf et al., 2017).They include the Make Early Diagnosis to
Prevent Early Deaths (MEDPED) criteria (USA), the Simon Broome Register Group (United
Kingdom) released by the European Atherosclerosis Society, and the Dutch Lipid Clinic
Network (DLCN) (Alallaf et al., 2017). Molecular genetic tests for autosomal recessive familial
hypercholesterolemia include targeted variant analysis through the capillary method and
sequence analysis of the entire coding region using the high-throughput next-generation
sequencing (NGS)-based strategy(Alallaf et al., 2017).Conversely, after discovering causative
mutation, it is always necessary to carry out cascade screening in first degree relatives such as
parents to determine the underlying dominant patterns of inheritance.
9 | P a g e
Diagnosis
The diagnosis of autosomal recessive familial hypercholesterolemia not only depends on
biochemistry tests but mainly on the clinical and molecular analyses(Alallaf et al., 2017).
Conventionally, biochemistry screening tests that analyze the lipid profile to determine
cholesterol levels are considered insufficient to make a diagnosis for familial
hypercholesterolemia conclusively. Mainly because of factors such as age, gender, certain drugs,
ethnicity, pathological and physiological conditions which contribute to the variation of the
results, ultimately leading to false negative or false positive values(Alallaf et al., 2017).The
clinical criteria is to integrate the reports of repeated measurements of very high LDL-C or total
cholesterol levels with the presence of xanthomas as well as considering family histories of signs
and symptoms of dyslipidemia in making the diagnosis(Alallaf et al., 2017).Based on the clinical
criteria, there exist conventional diagnostic systems that are applied in the determination of
familial hypercholesterolemia(Alallaf et al., 2017).They include the Make Early Diagnosis to
Prevent Early Deaths (MEDPED) criteria (USA), the Simon Broome Register Group (United
Kingdom) released by the European Atherosclerosis Society, and the Dutch Lipid Clinic
Network (DLCN) (Alallaf et al., 2017). Molecular genetic tests for autosomal recessive familial
hypercholesterolemia include targeted variant analysis through the capillary method and
sequence analysis of the entire coding region using the high-throughput next-generation
sequencing (NGS)-based strategy(Alallaf et al., 2017).Conversely, after discovering causative
mutation, it is always necessary to carry out cascade screening in first degree relatives such as
parents to determine the underlying dominant patterns of inheritance.
9 | P a g e
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
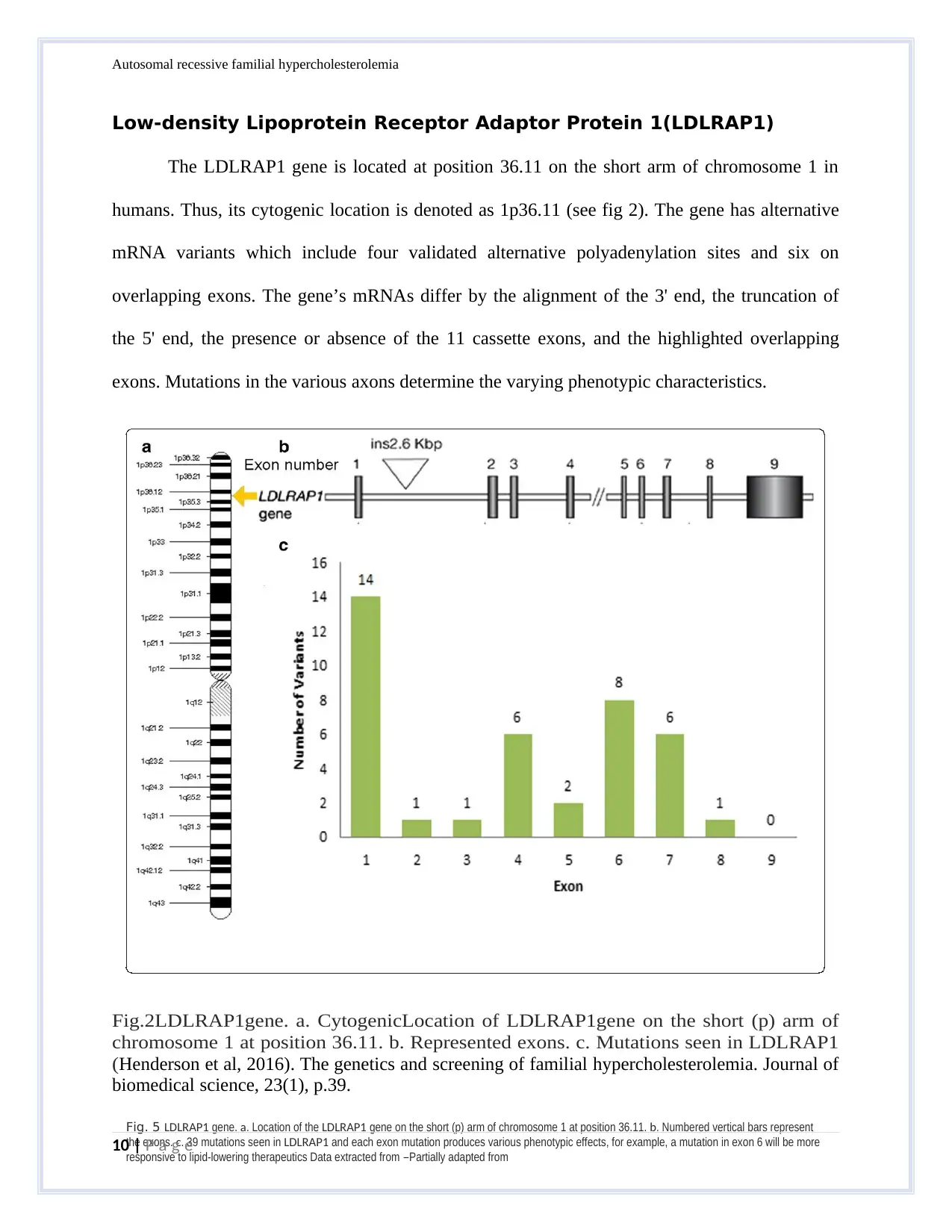
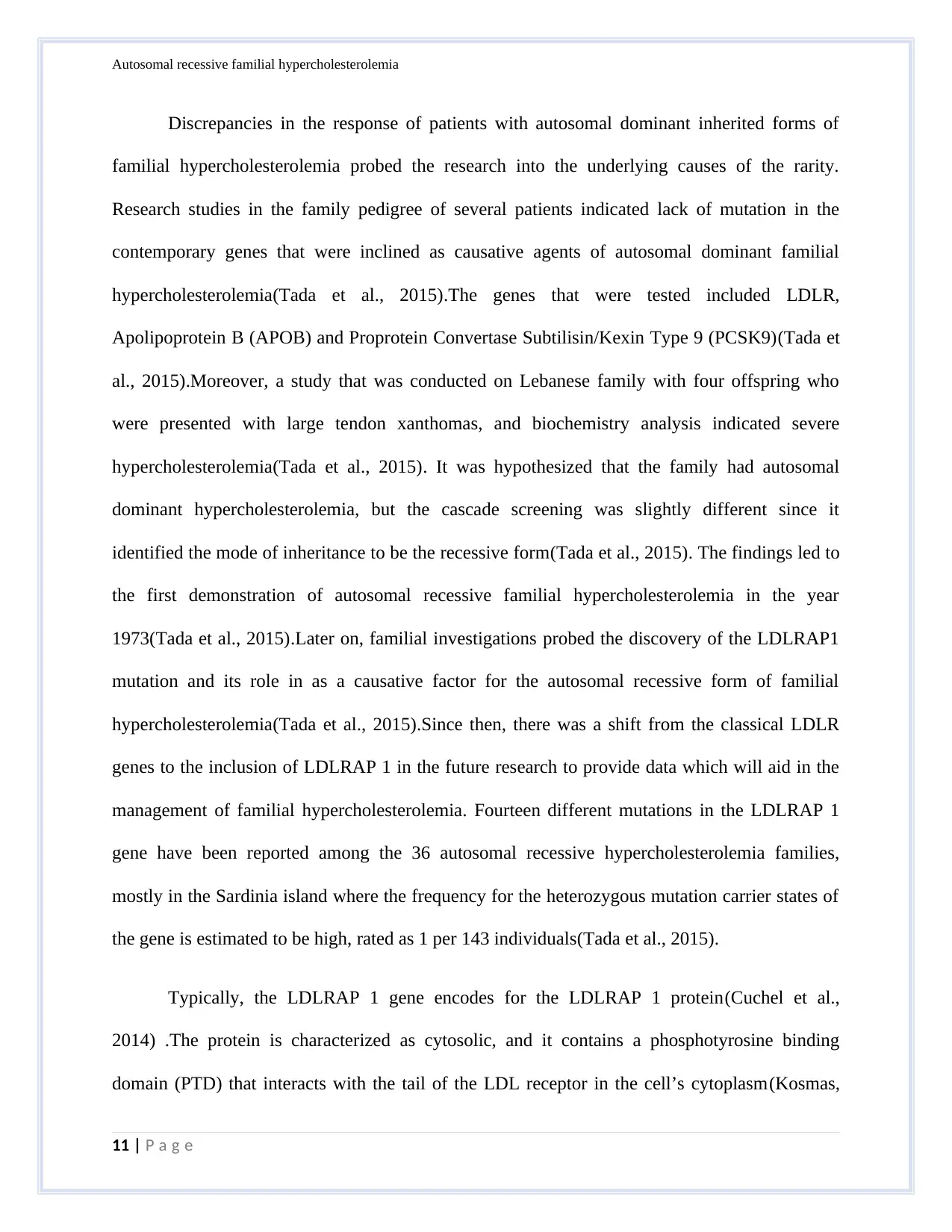
Fig. 5 LDLRAP1 gene. a. Location of the LDLRAP1 gene on the short (p) arm of chromosome 1 at position 36.11. b. Numbered vertical bars represent
the exons. c. 39 mutations seen in LDLRAP1 and each exon mutation produces various phenotypic effects, for example, a mutation in exon 6 will be more
responsive to lipid-lowering therapeutics Data extracted from –Partially adapted from
Autosomal recessive familial hypercholesterolemia
Low-density Lipoprotein Receptor Adaptor Protein 1(LDLRAP1)
The LDLRAP1 gene is located at position 36.11 on the short arm of chromosome 1 in
humans. Thus, its cytogenic location is denoted as 1p36.11 (see fig 2). The gene has alternative
mRNA variants which include four validated alternative polyadenylation sites and six on
overlapping exons. The gene’s mRNAs differ by the alignment of the 3' end, the truncation of
the 5' end, the presence or absence of the 11 cassette exons, and the highlighted overlapping
exons. Mutations in the various axons determine the varying phenotypic characteristics.
Fig.2LDLRAP1gene. a. CytogenicLocation of LDLRAP1gene on the short (p) arm of
chromosome 1 at position 36.11. b. Represented exons. c. Mutations seen in LDLRAP1
(Henderson et al, 2016). The genetics and screening of familial hypercholesterolemia. Journal of
biomedical science, 23(1), p.39.
10 | P a g e
the exons. c. 39 mutations seen in LDLRAP1 and each exon mutation produces various phenotypic effects, for example, a mutation in exon 6 will be more
responsive to lipid-lowering therapeutics Data extracted from –Partially adapted from
Autosomal recessive familial hypercholesterolemia
Low-density Lipoprotein Receptor Adaptor Protein 1(LDLRAP1)
The LDLRAP1 gene is located at position 36.11 on the short arm of chromosome 1 in
humans. Thus, its cytogenic location is denoted as 1p36.11 (see fig 2). The gene has alternative
mRNA variants which include four validated alternative polyadenylation sites and six on
overlapping exons. The gene’s mRNAs differ by the alignment of the 3' end, the truncation of
the 5' end, the presence or absence of the 11 cassette exons, and the highlighted overlapping
exons. Mutations in the various axons determine the varying phenotypic characteristics.
Fig.2LDLRAP1gene. a. CytogenicLocation of LDLRAP1gene on the short (p) arm of
chromosome 1 at position 36.11. b. Represented exons. c. Mutations seen in LDLRAP1
(Henderson et al, 2016). The genetics and screening of familial hypercholesterolemia. Journal of
biomedical science, 23(1), p.39.
10 | P a g e
Autosomal recessive familial hypercholesterolemia
Discrepancies in the response of patients with autosomal dominant inherited forms of
familial hypercholesterolemia probed the research into the underlying causes of the rarity.
Research studies in the family pedigree of several patients indicated lack of mutation in the
contemporary genes that were inclined as causative agents of autosomal dominant familial
hypercholesterolemia(Tada et al., 2015).The genes that were tested included LDLR,
Apolipoprotein B (APOB) and Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9)(Tada et
al., 2015).Moreover, a study that was conducted on Lebanese family with four offspring who
were presented with large tendon xanthomas, and biochemistry analysis indicated severe
hypercholesterolemia(Tada et al., 2015). It was hypothesized that the family had autosomal
dominant hypercholesterolemia, but the cascade screening was slightly different since it
identified the mode of inheritance to be the recessive form(Tada et al., 2015). The findings led to
the first demonstration of autosomal recessive familial hypercholesterolemia in the year
1973(Tada et al., 2015).Later on, familial investigations probed the discovery of the LDLRAP1
mutation and its role in as a causative factor for the autosomal recessive form of familial
hypercholesterolemia(Tada et al., 2015).Since then, there was a shift from the classical LDLR
genes to the inclusion of LDLRAP 1 in the future research to provide data which will aid in the
management of familial hypercholesterolemia. Fourteen different mutations in the LDLRAP 1
gene have been reported among the 36 autosomal recessive hypercholesterolemia families,
mostly in the Sardinia island where the frequency for the heterozygous mutation carrier states of
the gene is estimated to be high, rated as 1 per 143 individuals(Tada et al., 2015).
Typically, the LDLRAP 1 gene encodes for the LDLRAP 1 protein(Cuchel et al.,
2014) .The protein is characterized as cytosolic, and it contains a phosphotyrosine binding
domain (PTD) that interacts with the tail of the LDL receptor in the cell’s cytoplasm(Kosmas,
11 | P a g e
Discrepancies in the response of patients with autosomal dominant inherited forms of
familial hypercholesterolemia probed the research into the underlying causes of the rarity.
Research studies in the family pedigree of several patients indicated lack of mutation in the
contemporary genes that were inclined as causative agents of autosomal dominant familial
hypercholesterolemia(Tada et al., 2015).The genes that were tested included LDLR,
Apolipoprotein B (APOB) and Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9)(Tada et
al., 2015).Moreover, a study that was conducted on Lebanese family with four offspring who
were presented with large tendon xanthomas, and biochemistry analysis indicated severe
hypercholesterolemia(Tada et al., 2015). It was hypothesized that the family had autosomal
dominant hypercholesterolemia, but the cascade screening was slightly different since it
identified the mode of inheritance to be the recessive form(Tada et al., 2015). The findings led to
the first demonstration of autosomal recessive familial hypercholesterolemia in the year
1973(Tada et al., 2015).Later on, familial investigations probed the discovery of the LDLRAP1
mutation and its role in as a causative factor for the autosomal recessive form of familial
hypercholesterolemia(Tada et al., 2015).Since then, there was a shift from the classical LDLR
genes to the inclusion of LDLRAP 1 in the future research to provide data which will aid in the
management of familial hypercholesterolemia. Fourteen different mutations in the LDLRAP 1
gene have been reported among the 36 autosomal recessive hypercholesterolemia families,
mostly in the Sardinia island where the frequency for the heterozygous mutation carrier states of
the gene is estimated to be high, rated as 1 per 143 individuals(Tada et al., 2015).
Typically, the LDLRAP 1 gene encodes for the LDLRAP 1 protein(Cuchel et al.,
2014) .The protein is characterized as cytosolic, and it contains a phosphotyrosine binding
domain (PTD) that interacts with the tail of the LDL receptor in the cell’s cytoplasm(Kosmas,
11 | P a g e
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 19
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.