Analysis of Anger Temperament's Impact on Coronary Heart Disease Risk
VerifiedAdded on 2021/01/01
|9
|2600
|378
Report
AI Summary
This report analyzes the Atherosclerosis Risk in Communities study, focusing on the relationship between anger temperament and the risk of coronary heart disease (CHD). The study investigates how anger, both as a temperament trait and a reaction, can increase the likelihood of CHD, including conditions like myocardial infarction. It examines the advantages and disadvantages of the study design, the reasons for excluding certain participants, and the impact of participant attrition. The report details the implications of differences in anger traits among various groups, including normotensive and hypertensive individuals. It also explores the cumulative incidence and incidence rates within different subgroups, the relationship between these rates, and the application of rate ratios. Finally, the report delves into the statistical significance of the association between anger temperament and CHD risk, including the interpretation of findings and the potential for randomized intervention trials to test the hypothesis that anger increases CHD risk. The conclusion summarizes the identified risks associated with atherosclerosis.
The Atherosclerosis Risk in
communities
communities
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

INTRODUCTION
The atherosclerosis refers to a situation of human body when arteries become narrow by
build up of plaque due to which blood flow is not carried out easily. It include an issue that blood
cells containing oxygen and minerals from heart to other body parts are not properly flowing due
to narrowed arteries. The present assignment will focus on problem of coronary disease of heart
due to which flow of blood get affected and impacts negatively on body functions. It include
description about effects of an angry temperament on coronary heart disease (CHD) risk and
their analysis of participants taken for study with appropriate reasons.
TASK
Q1 Advantages and disadvantages of the study including anger temperament & anger reaction
The impacts of anger temperament and anger reaction may leads to increase risk of
coronary heart disease which results into narrowing of arteries and create problem in blood
flowing. Moreover, blood vessels become narrow because of build up plaque in artery wall and
insufficient flow of oxygen is not takes place on human body. The Atherosclerosis risk can be
evaluated along with purpose of studying chance of occurring an acute myocardial infarction
(MI)/fatal CHD, silent MI or cardiac vascularisation procedures.
Advantages – The study of anger temperament and reaction provide support to more
accurately identify symptoms of coronary heart disease risk. It involves to make prediction about
types of atherosclerosis including carotid artery problem, coronary artery disease, peripheral
artery issues, kidney problem which can determined by thoroughly studied anger reaction of an
individual.
Disadvantages – The demerits of studying anger temperament in order to investigate
more than one heart issue as it may create confusion as well. Moreover, different age group or
previous history of some other disease may leads to anger reaction but it does not mean about
Atherosclerosis risk for them.
1
The atherosclerosis refers to a situation of human body when arteries become narrow by
build up of plaque due to which blood flow is not carried out easily. It include an issue that blood
cells containing oxygen and minerals from heart to other body parts are not properly flowing due
to narrowed arteries. The present assignment will focus on problem of coronary disease of heart
due to which flow of blood get affected and impacts negatively on body functions. It include
description about effects of an angry temperament on coronary heart disease (CHD) risk and
their analysis of participants taken for study with appropriate reasons.
TASK
Q1 Advantages and disadvantages of the study including anger temperament & anger reaction
The impacts of anger temperament and anger reaction may leads to increase risk of
coronary heart disease which results into narrowing of arteries and create problem in blood
flowing. Moreover, blood vessels become narrow because of build up plaque in artery wall and
insufficient flow of oxygen is not takes place on human body. The Atherosclerosis risk can be
evaluated along with purpose of studying chance of occurring an acute myocardial infarction
(MI)/fatal CHD, silent MI or cardiac vascularisation procedures.
Advantages – The study of anger temperament and reaction provide support to more
accurately identify symptoms of coronary heart disease risk. It involves to make prediction about
types of atherosclerosis including carotid artery problem, coronary artery disease, peripheral
artery issues, kidney problem which can determined by thoroughly studied anger reaction of an
individual.
Disadvantages – The demerits of studying anger temperament in order to investigate
more than one heart issue as it may create confusion as well. Moreover, different age group or
previous history of some other disease may leads to anger reaction but it does not mean about
Atherosclerosis risk for them.
1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Q2
a) Reason for excluding around 1,140 participants through evidence of coronary problem of heart
The 1,140 participants get excluded because they have previous history of myocardial
infarction (MI), coronary bypass surgery or electrocardiographic evidence of MI. people having
problem of MI or other proofs about any relevant operation are not applicable for studying
increased Atherosclerosis risk due to anger temperament or anger reaction of people. Moreover.
Such individuals are applicable to fulfil desired aim that is to determine which component or
anger- prone personality can be more strongly predicts about coronary heart disease (CHD) risk
in human body. However, it is essential to avoid these individuals in order to make an
appropriate population fro collecting required data to conclude actual results in proper way.
b) Impact of study results by losing 7% of original cohort by second visit
The 7% of people might be losing because around 93% of people are identified to be at
the baseline of Atherosclerosis risk which are actually applicable for making desired results. It is
required that group individuals who were selected should have border line problem of the given
heart disease but in second visit involves check up of them which indicates that only 93% of
them are liable for this study. Initially, people are selected as per views about their health status
of heart but in the second visit medical diagnosis make sure about actual stage of coronary heart
problem. However, it has been analysed that rest of 7% people are suffering from this issues and
few of them had already undergone through relevant surgical treatment so that they are not
applicable for study. Hence, such individuals might be losing of original cohort by the second
visit which affects result of study.
Q3
a) Implications of noticeable differences among low and high anger trait
Anger is a common emotion, experienced by all human being in response to unwanted
and unexpected behaviour of others. As per the table 1, population is characterised for trait anger
temperament by hypothesis. In this, male percentage in low anger trait is 42.9 and in high anger
trait is 41.3. When an individual consuming cigarette so its percentage rate of anger is 35.6 in
normotensive and it is assumed that in Hypertension its consumption percentage is 36.7.
2
a) Reason for excluding around 1,140 participants through evidence of coronary problem of heart
The 1,140 participants get excluded because they have previous history of myocardial
infarction (MI), coronary bypass surgery or electrocardiographic evidence of MI. people having
problem of MI or other proofs about any relevant operation are not applicable for studying
increased Atherosclerosis risk due to anger temperament or anger reaction of people. Moreover.
Such individuals are applicable to fulfil desired aim that is to determine which component or
anger- prone personality can be more strongly predicts about coronary heart disease (CHD) risk
in human body. However, it is essential to avoid these individuals in order to make an
appropriate population fro collecting required data to conclude actual results in proper way.
b) Impact of study results by losing 7% of original cohort by second visit
The 7% of people might be losing because around 93% of people are identified to be at
the baseline of Atherosclerosis risk which are actually applicable for making desired results. It is
required that group individuals who were selected should have border line problem of the given
heart disease but in second visit involves check up of them which indicates that only 93% of
them are liable for this study. Initially, people are selected as per views about their health status
of heart but in the second visit medical diagnosis make sure about actual stage of coronary heart
problem. However, it has been analysed that rest of 7% people are suffering from this issues and
few of them had already undergone through relevant surgical treatment so that they are not
applicable for study. Hence, such individuals might be losing of original cohort by the second
visit which affects result of study.
Q3
a) Implications of noticeable differences among low and high anger trait
Anger is a common emotion, experienced by all human being in response to unwanted
and unexpected behaviour of others. As per the table 1, population is characterised for trait anger
temperament by hypothesis. In this, male percentage in low anger trait is 42.9 and in high anger
trait is 41.3. When an individual consuming cigarette so its percentage rate of anger is 35.6 in
normotensive and it is assumed that in Hypertension its consumption percentage is 36.7.
2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
b) Number of normotensive males with low anger-temperament
The number of normotensive males percentage in low anger temperament is around 42.9
and 48.5 and it can be observed that there is differences in their anger percentage rate. It is the
distribution of population characteristics for traits anger temperament by hypothesis status.
Among normotensive persons, the age adjusted risk is combined with male percentage was 2.48
times who reporting as having strong, angry temperament compared with their counterparts that
are being less prone to an angry temperament. This study is examined that the proposed
hypothesis effect of Ramadan fasting in males over the time period and this is analysed that the
relationship of pattern of heart disease variation with body mass index change. Such data us
recommended that a strong, angry temperament rather than anger reaction to criticism, frustrated
and unfair treatment places normotensive.
c) Percentage of hypertensives females
Table 1 represents data about cardiovascular risk factor profiles for trait anger-reaction and
temperament, respectively, by hypertensive status. In this regard, number of hypertensive
females as compared to male population is near about 58.7 at less than or equal to 8 position.
While for more than that, percentage of females is 45.4. Therefore, it has estimated from this
result that as compared to males, females are much sensitive towards Coronary heart disease and
anger temperament.
Q4 Participants who were followed their second clinic examination
Under this present research survey, 12,990 participates were followed up for the
occurrence of acute myocardial infection from the date of second clinical examination. It has
taken during December 31, 1995. At second clinical visit, total 14,348 students were examined.
Under this stage, in period of Dec 31, 1990, June 30, 1991 and Jan 31, 1992, the number of
participants for myocardial infection, coronary bypass surgery with 222 additional members is
12,990.
Q5 Cumulative incidence for the relevant four subgroups
Cumulative incidence can be defined as a measure of frequency with respect to a specific
period of time (Chang and et. al., 2014). Here, duration of time may be taken as an entire life of
an individual therefore, incidence proportion is also termed as lifetime risks. In this regard, it can
be calculated by dividing number of cases during a certain period with number of subjects at risk
3
The number of normotensive males percentage in low anger temperament is around 42.9
and 48.5 and it can be observed that there is differences in their anger percentage rate. It is the
distribution of population characteristics for traits anger temperament by hypothesis status.
Among normotensive persons, the age adjusted risk is combined with male percentage was 2.48
times who reporting as having strong, angry temperament compared with their counterparts that
are being less prone to an angry temperament. This study is examined that the proposed
hypothesis effect of Ramadan fasting in males over the time period and this is analysed that the
relationship of pattern of heart disease variation with body mass index change. Such data us
recommended that a strong, angry temperament rather than anger reaction to criticism, frustrated
and unfair treatment places normotensive.
c) Percentage of hypertensives females
Table 1 represents data about cardiovascular risk factor profiles for trait anger-reaction and
temperament, respectively, by hypertensive status. In this regard, number of hypertensive
females as compared to male population is near about 58.7 at less than or equal to 8 position.
While for more than that, percentage of females is 45.4. Therefore, it has estimated from this
result that as compared to males, females are much sensitive towards Coronary heart disease and
anger temperament.
Q4 Participants who were followed their second clinic examination
Under this present research survey, 12,990 participates were followed up for the
occurrence of acute myocardial infection from the date of second clinical examination. It has
taken during December 31, 1995. At second clinical visit, total 14,348 students were examined.
Under this stage, in period of Dec 31, 1990, June 30, 1991 and Jan 31, 1992, the number of
participants for myocardial infection, coronary bypass surgery with 222 additional members is
12,990.
Q5 Cumulative incidence for the relevant four subgroups
Cumulative incidence can be defined as a measure of frequency with respect to a specific
period of time (Chang and et. al., 2014). Here, duration of time may be taken as an entire life of
an individual therefore, incidence proportion is also termed as lifetime risks. In this regard, it can
be calculated by dividing number of cases during a certain period with number of subjects at risk
3
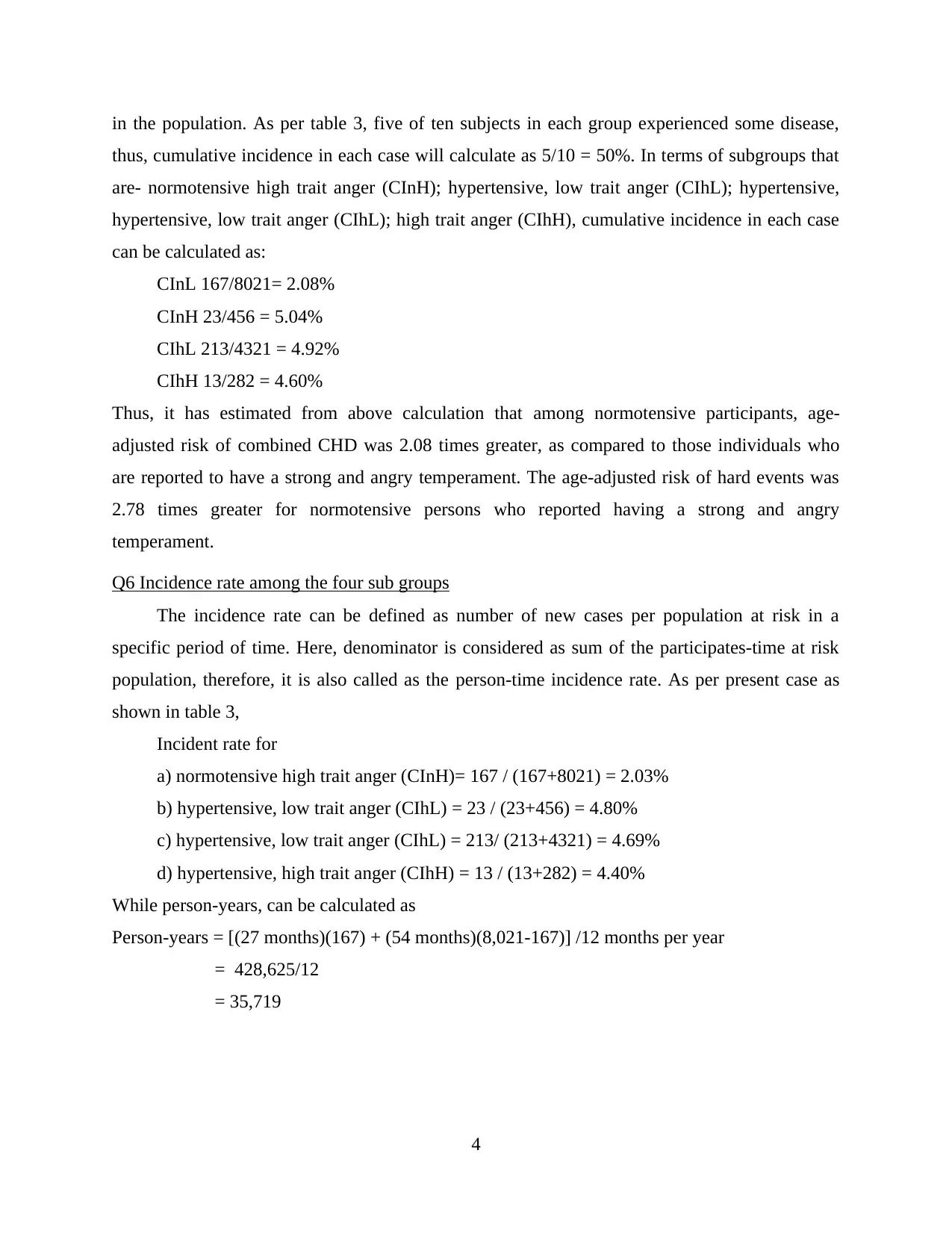
in the population. As per table 3, five of ten subjects in each group experienced some disease,
thus, cumulative incidence in each case will calculate as 5/10 = 50%. In terms of subgroups that
are- normotensive high trait anger (CInH); hypertensive, low trait anger (CIhL); hypertensive,
hypertensive, low trait anger (CIhL); high trait anger (CIhH), cumulative incidence in each case
can be calculated as:
CInL 167/8021= 2.08%
CInH 23/456 = 5.04%
CIhL 213/4321 = 4.92%
CIhH 13/282 = 4.60%
Thus, it has estimated from above calculation that among normotensive participants, age-
adjusted risk of combined CHD was 2.08 times greater, as compared to those individuals who
are reported to have a strong and angry temperament. The age-adjusted risk of hard events was
2.78 times greater for normotensive persons who reported having a strong and angry
temperament.
Q6 Incidence rate among the four sub groups
The incidence rate can be defined as number of new cases per population at risk in a
specific period of time. Here, denominator is considered as sum of the participates-time at risk
population, therefore, it is also called as the person-time incidence rate. As per present case as
shown in table 3,
Incident rate for
a) normotensive high trait anger (CInH)= 167 / (167+8021) = 2.03%
b) hypertensive, low trait anger (CIhL) = 23 / (23+456) = 4.80%
c) hypertensive, low trait anger (CIhL) = 213/ (213+4321) = 4.69%
d) hypertensive, high trait anger (CIhH) = 13 / (13+282) = 4.40%
While person-years, can be calculated as
Person-years = [(27 months)(167) + (54 months)(8,021-167)] /12 months per year
= 428,625/12
= 35,719
4
thus, cumulative incidence in each case will calculate as 5/10 = 50%. In terms of subgroups that
are- normotensive high trait anger (CInH); hypertensive, low trait anger (CIhL); hypertensive,
hypertensive, low trait anger (CIhL); high trait anger (CIhH), cumulative incidence in each case
can be calculated as:
CInL 167/8021= 2.08%
CInH 23/456 = 5.04%
CIhL 213/4321 = 4.92%
CIhH 13/282 = 4.60%
Thus, it has estimated from above calculation that among normotensive participants, age-
adjusted risk of combined CHD was 2.08 times greater, as compared to those individuals who
are reported to have a strong and angry temperament. The age-adjusted risk of hard events was
2.78 times greater for normotensive persons who reported having a strong and angry
temperament.
Q6 Incidence rate among the four sub groups
The incidence rate can be defined as number of new cases per population at risk in a
specific period of time. Here, denominator is considered as sum of the participates-time at risk
population, therefore, it is also called as the person-time incidence rate. As per present case as
shown in table 3,
Incident rate for
a) normotensive high trait anger (CInH)= 167 / (167+8021) = 2.03%
b) hypertensive, low trait anger (CIhL) = 23 / (23+456) = 4.80%
c) hypertensive, low trait anger (CIhL) = 213/ (213+4321) = 4.69%
d) hypertensive, high trait anger (CIhH) = 13 / (13+282) = 4.40%
While person-years, can be calculated as
Person-years = [(27 months)(167) + (54 months)(8,021-167)] /12 months per year
= 428,625/12
= 35,719
4
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
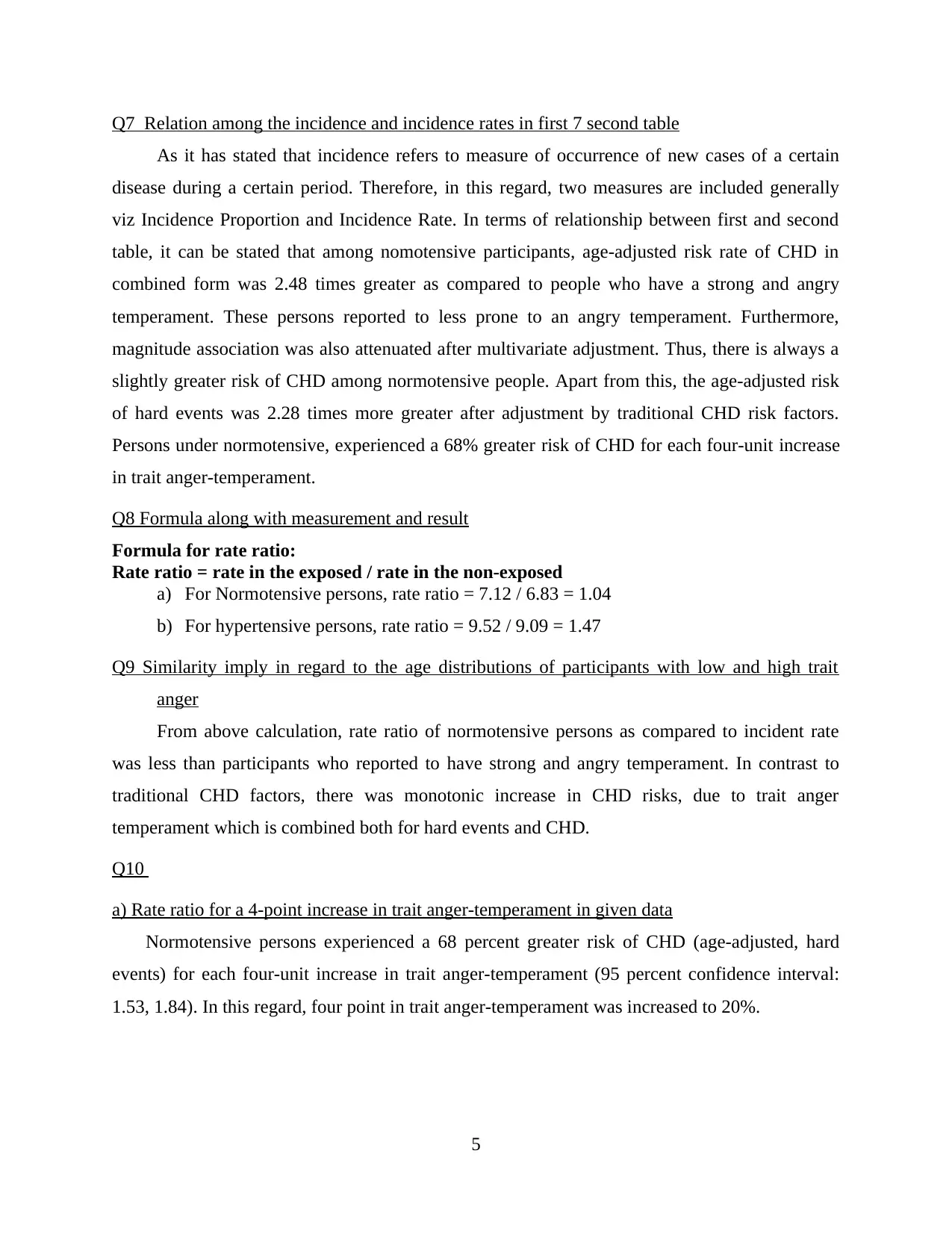
Q7 Relation among the incidence and incidence rates in first 7 second table
As it has stated that incidence refers to measure of occurrence of new cases of a certain
disease during a certain period. Therefore, in this regard, two measures are included generally
viz Incidence Proportion and Incidence Rate. In terms of relationship between first and second
table, it can be stated that among nomotensive participants, age-adjusted risk rate of CHD in
combined form was 2.48 times greater as compared to people who have a strong and angry
temperament. These persons reported to less prone to an angry temperament. Furthermore,
magnitude association was also attenuated after multivariate adjustment. Thus, there is always a
slightly greater risk of CHD among normotensive people. Apart from this, the age-adjusted risk
of hard events was 2.28 times more greater after adjustment by traditional CHD risk factors.
Persons under normotensive, experienced a 68% greater risk of CHD for each four-unit increase
in trait anger-temperament.
Q8 Formula along with measurement and result
Formula for rate ratio:
Rate ratio = rate in the exposed / rate in the non-exposed
a) For Normotensive persons, rate ratio = 7.12 / 6.83 = 1.04
b) For hypertensive persons, rate ratio = 9.52 / 9.09 = 1.47
Q9 Similarity imply in regard to the age distributions of participants with low and high trait
anger
From above calculation, rate ratio of normotensive persons as compared to incident rate
was less than participants who reported to have strong and angry temperament. In contrast to
traditional CHD factors, there was monotonic increase in CHD risks, due to trait anger
temperament which is combined both for hard events and CHD.
Q10
a) Rate ratio for a 4-point increase in trait anger-temperament in given data
Normotensive persons experienced a 68 percent greater risk of CHD (age-adjusted, hard
events) for each four-unit increase in trait anger-temperament (95 percent confidence interval:
1.53, 1.84). In this regard, four point in trait anger-temperament was increased to 20%.
5
As it has stated that incidence refers to measure of occurrence of new cases of a certain
disease during a certain period. Therefore, in this regard, two measures are included generally
viz Incidence Proportion and Incidence Rate. In terms of relationship between first and second
table, it can be stated that among nomotensive participants, age-adjusted risk rate of CHD in
combined form was 2.48 times greater as compared to people who have a strong and angry
temperament. These persons reported to less prone to an angry temperament. Furthermore,
magnitude association was also attenuated after multivariate adjustment. Thus, there is always a
slightly greater risk of CHD among normotensive people. Apart from this, the age-adjusted risk
of hard events was 2.28 times more greater after adjustment by traditional CHD risk factors.
Persons under normotensive, experienced a 68% greater risk of CHD for each four-unit increase
in trait anger-temperament.
Q8 Formula along with measurement and result
Formula for rate ratio:
Rate ratio = rate in the exposed / rate in the non-exposed
a) For Normotensive persons, rate ratio = 7.12 / 6.83 = 1.04
b) For hypertensive persons, rate ratio = 9.52 / 9.09 = 1.47
Q9 Similarity imply in regard to the age distributions of participants with low and high trait
anger
From above calculation, rate ratio of normotensive persons as compared to incident rate
was less than participants who reported to have strong and angry temperament. In contrast to
traditional CHD factors, there was monotonic increase in CHD risks, due to trait anger
temperament which is combined both for hard events and CHD.
Q10
a) Rate ratio for a 4-point increase in trait anger-temperament in given data
Normotensive persons experienced a 68 percent greater risk of CHD (age-adjusted, hard
events) for each four-unit increase in trait anger-temperament (95 percent confidence interval:
1.53, 1.84). In this regard, four point in trait anger-temperament was increased to 20%.
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
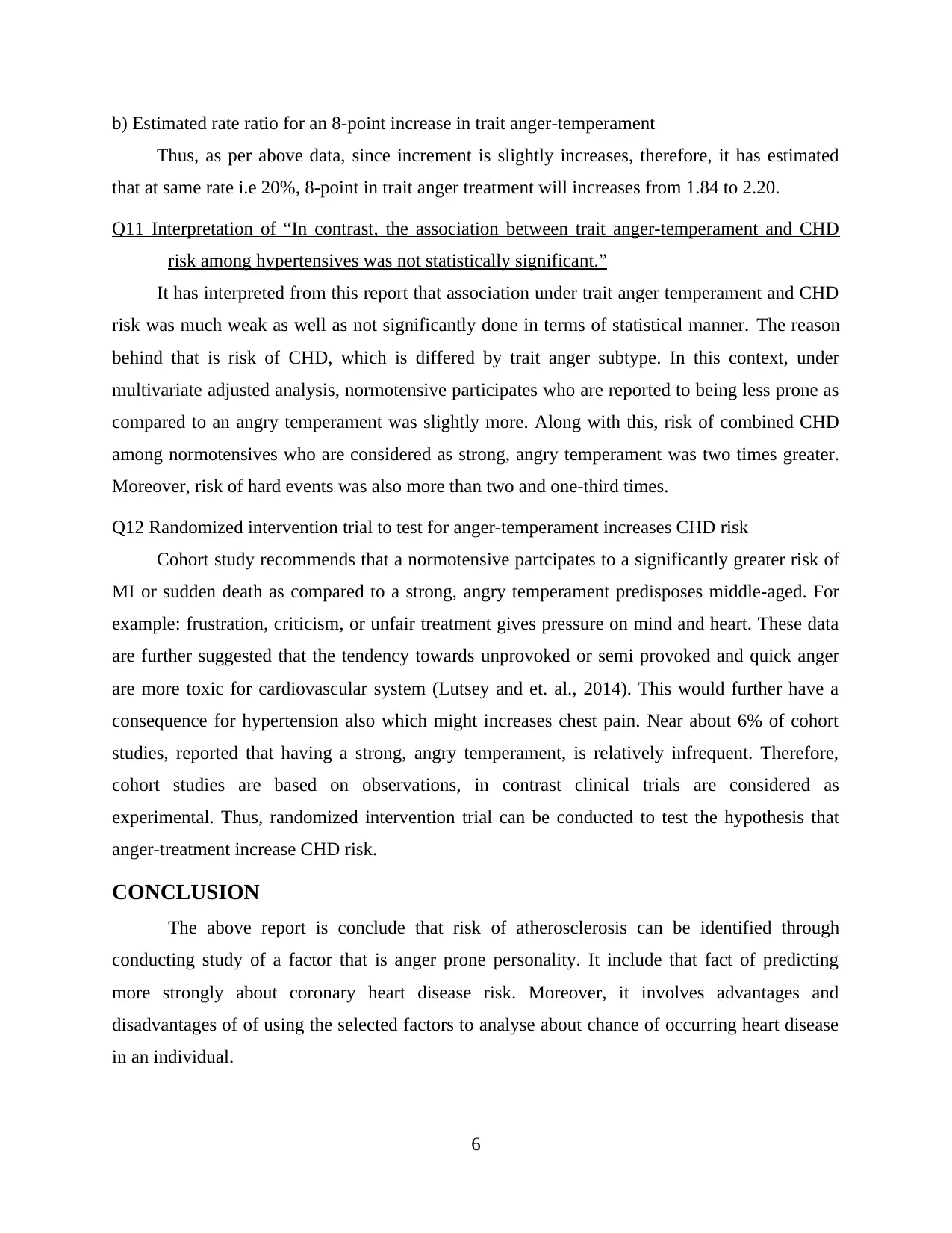
b) Estimated rate ratio for an 8-point increase in trait anger-temperament
Thus, as per above data, since increment is slightly increases, therefore, it has estimated
that at same rate i.e 20%, 8-point in trait anger treatment will increases from 1.84 to 2.20.
Q11 Interpretation of “In contrast, the association between trait anger-temperament and CHD
risk among hypertensives was not statistically significant.”
It has interpreted from this report that association under trait anger temperament and CHD
risk was much weak as well as not significantly done in terms of statistical manner. The reason
behind that is risk of CHD, which is differed by trait anger subtype. In this context, under
multivariate adjusted analysis, normotensive participates who are reported to being less prone as
compared to an angry temperament was slightly more. Along with this, risk of combined CHD
among normotensives who are considered as strong, angry temperament was two times greater.
Moreover, risk of hard events was also more than two and one-third times.
Q12 Randomized intervention trial to test for anger-temperament increases CHD risk
Cohort study recommends that a normotensive partcipates to a significantly greater risk of
MI or sudden death as compared to a strong, angry temperament predisposes middle-aged. For
example: frustration, criticism, or unfair treatment gives pressure on mind and heart. These data
are further suggested that the tendency towards unprovoked or semi provoked and quick anger
are more toxic for cardiovascular system (Lutsey and et. al., 2014). This would further have a
consequence for hypertension also which might increases chest pain. Near about 6% of cohort
studies, reported that having a strong, angry temperament, is relatively infrequent. Therefore,
cohort studies are based on observations, in contrast clinical trials are considered as
experimental. Thus, randomized intervention trial can be conducted to test the hypothesis that
anger-treatment increase CHD risk.
CONCLUSION
The above report is conclude that risk of atherosclerosis can be identified through
conducting study of a factor that is anger prone personality. It include that fact of predicting
more strongly about coronary heart disease risk. Moreover, it involves advantages and
disadvantages of of using the selected factors to analyse about chance of occurring heart disease
in an individual.
6
Thus, as per above data, since increment is slightly increases, therefore, it has estimated
that at same rate i.e 20%, 8-point in trait anger treatment will increases from 1.84 to 2.20.
Q11 Interpretation of “In contrast, the association between trait anger-temperament and CHD
risk among hypertensives was not statistically significant.”
It has interpreted from this report that association under trait anger temperament and CHD
risk was much weak as well as not significantly done in terms of statistical manner. The reason
behind that is risk of CHD, which is differed by trait anger subtype. In this context, under
multivariate adjusted analysis, normotensive participates who are reported to being less prone as
compared to an angry temperament was slightly more. Along with this, risk of combined CHD
among normotensives who are considered as strong, angry temperament was two times greater.
Moreover, risk of hard events was also more than two and one-third times.
Q12 Randomized intervention trial to test for anger-temperament increases CHD risk
Cohort study recommends that a normotensive partcipates to a significantly greater risk of
MI or sudden death as compared to a strong, angry temperament predisposes middle-aged. For
example: frustration, criticism, or unfair treatment gives pressure on mind and heart. These data
are further suggested that the tendency towards unprovoked or semi provoked and quick anger
are more toxic for cardiovascular system (Lutsey and et. al., 2014). This would further have a
consequence for hypertension also which might increases chest pain. Near about 6% of cohort
studies, reported that having a strong, angry temperament, is relatively infrequent. Therefore,
cohort studies are based on observations, in contrast clinical trials are considered as
experimental. Thus, randomized intervention trial can be conducted to test the hypothesis that
anger-treatment increase CHD risk.
CONCLUSION
The above report is conclude that risk of atherosclerosis can be identified through
conducting study of a factor that is anger prone personality. It include that fact of predicting
more strongly about coronary heart disease risk. Moreover, it involves advantages and
disadvantages of of using the selected factors to analyse about chance of occurring heart disease
in an individual.
6
REFERENCE
Books and Journals
Lutsey, P. L. and et. al., 2014. Fibroblast growth factor‐23 and incident coronary heart disease,
heart failure, and cardiovascular mortality: the Atherosclerosis Risk in Communities
study. Journal of the American Heart Association. 3(3). p.e000936.
Chang, P. P. and et. al., 2014. Incidence and survival of hospitalized acute decompensated heart
failure in four US communities (from the Atherosclerosis Risk in Communities Study).
The American journal of cardiology. 113(3). pp.504-510.
Srinath, R., and et. al., 2015. Endogenous testosterone and its relationship to preclinical and
clinical measures of cardiovascular disease in the atherosclerosis risk in communities
study. The Journal of Clinical Endocrinology & Metabolism. 100(4). pp.1602-1608.
Deal, J. A., and et. al., 2015. Hearing impairment and cognitive decline: a pilot study conducted
within the atherosclerosis risk in communities neurocognitive study. American journal of
epidemiology. 181(9). pp.680-690.
Cobb, L. K., and et. al., 2014. The association of spousal smoking status with the ability to quit
smoking: The Atherosclerosis Risk in Communities Study. American journal of
epidemiology. 179(10). pp.1182-1187.
Schneider, A. L. C., and et. al., 2015. Vitamin D, vitamin D binding protein gene
polymorphisms, race and risk of incident stroke: the Atherosclerosis Risk in Communities
(ARIC) study. European journal of neurology. 22(8). pp.1220-1227.
7
Books and Journals
Lutsey, P. L. and et. al., 2014. Fibroblast growth factor‐23 and incident coronary heart disease,
heart failure, and cardiovascular mortality: the Atherosclerosis Risk in Communities
study. Journal of the American Heart Association. 3(3). p.e000936.
Chang, P. P. and et. al., 2014. Incidence and survival of hospitalized acute decompensated heart
failure in four US communities (from the Atherosclerosis Risk in Communities Study).
The American journal of cardiology. 113(3). pp.504-510.
Srinath, R., and et. al., 2015. Endogenous testosterone and its relationship to preclinical and
clinical measures of cardiovascular disease in the atherosclerosis risk in communities
study. The Journal of Clinical Endocrinology & Metabolism. 100(4). pp.1602-1608.
Deal, J. A., and et. al., 2015. Hearing impairment and cognitive decline: a pilot study conducted
within the atherosclerosis risk in communities neurocognitive study. American journal of
epidemiology. 181(9). pp.680-690.
Cobb, L. K., and et. al., 2014. The association of spousal smoking status with the ability to quit
smoking: The Atherosclerosis Risk in Communities Study. American journal of
epidemiology. 179(10). pp.1182-1187.
Schneider, A. L. C., and et. al., 2015. Vitamin D, vitamin D binding protein gene
polymorphisms, race and risk of incident stroke: the Atherosclerosis Risk in Communities
(ARIC) study. European journal of neurology. 22(8). pp.1220-1227.
7
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.