Australian Health Workforce Planning and International Migration
VerifiedAdded on 2023/04/08
|16
|2512
|340
Report
AI Summary
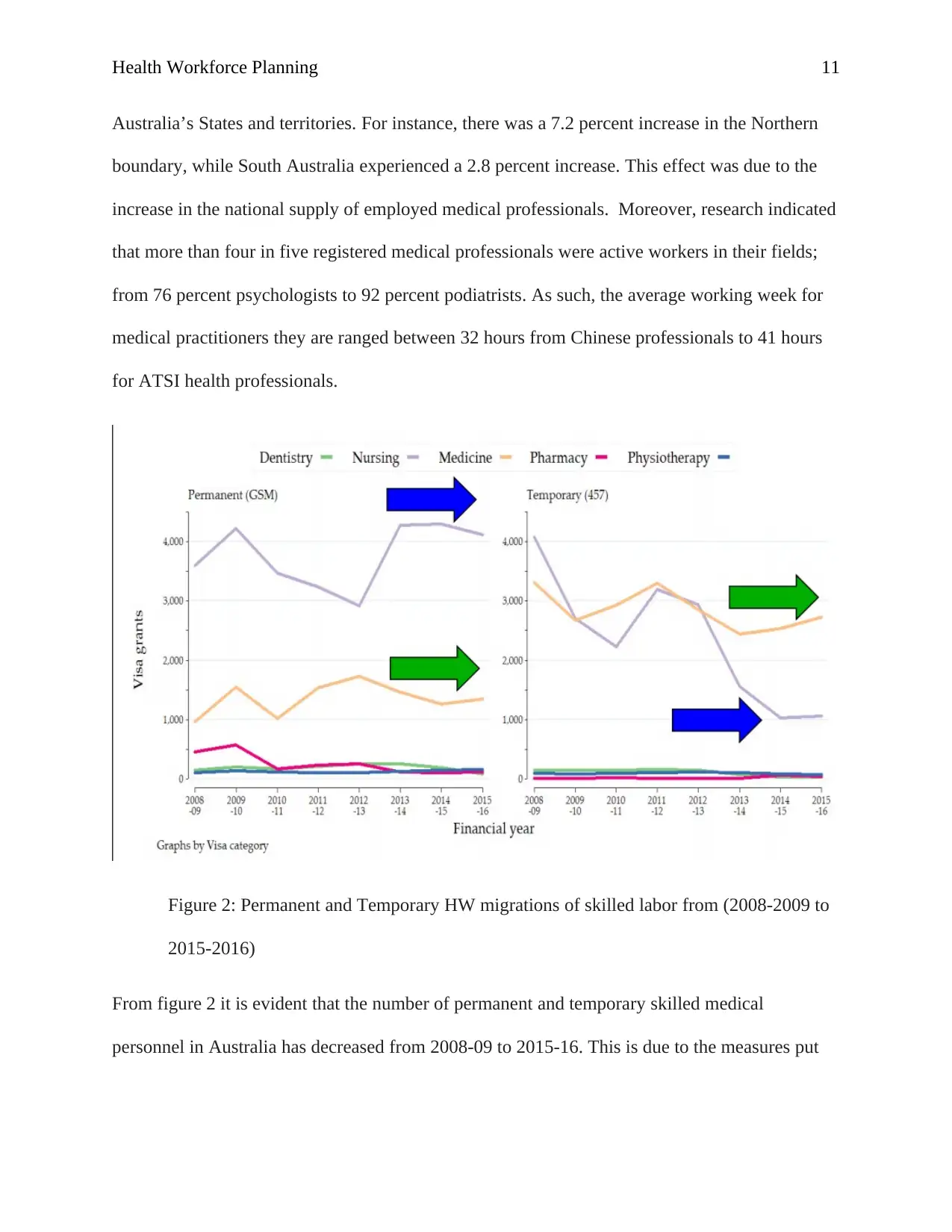
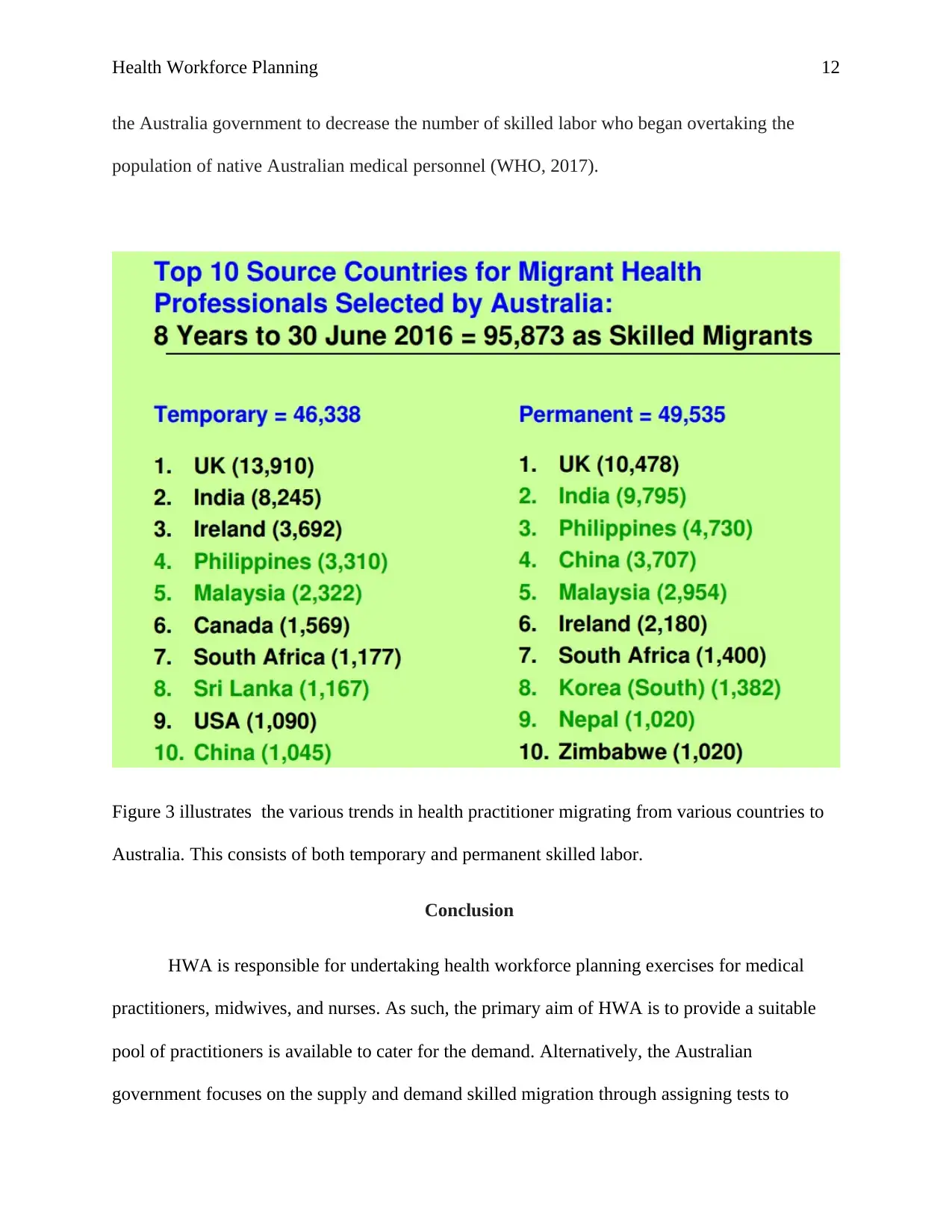
This report provides a comprehensive analysis of health workforce planning in Australia, focusing on the impact of international migration. It examines the Australian government's strategies, including the Health Workforce Australia (HWA), skilled migration policies, and the Modified Occupation Demand List (MODL). The report presents data on the proportion of the clinical health workforce, including medical practitioners, nurses, and midwives, who have initial qualifications from overseas countries. It also explores the challenges faced by the Australian health workforce, such as self-sufficiency, demographic shifts, and cost barriers. The report discusses the strategies developed by the Australian government to address these challenges, including temporary and permanent skilled migration programs. Main findings highlight the supply and resource-driven approach to health workforce planning in Australia and the cycles of oversupply and shortages. The report concludes with recommendations for improving health workforce planning and addressing the negative effects of health worker migration, emphasizing the need for strategies to retain, recruit, and support health professionals trained overseas. The report also presents data on the number of ENs and RNs, Registered midwives, and medical practitioners in Australia from 2011 to 2015. The report also presents data on the number of permanent and temporary skilled medical personnel in Australia from 2008-09 to 2015-16 and trends in health practitioner migrating from various countries to Australia.


1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.