Analysis of Smoking Practices in Australia: A Report
VerifiedAdded on 2022/11/01
|21
|3638
|319
Report
AI Summary
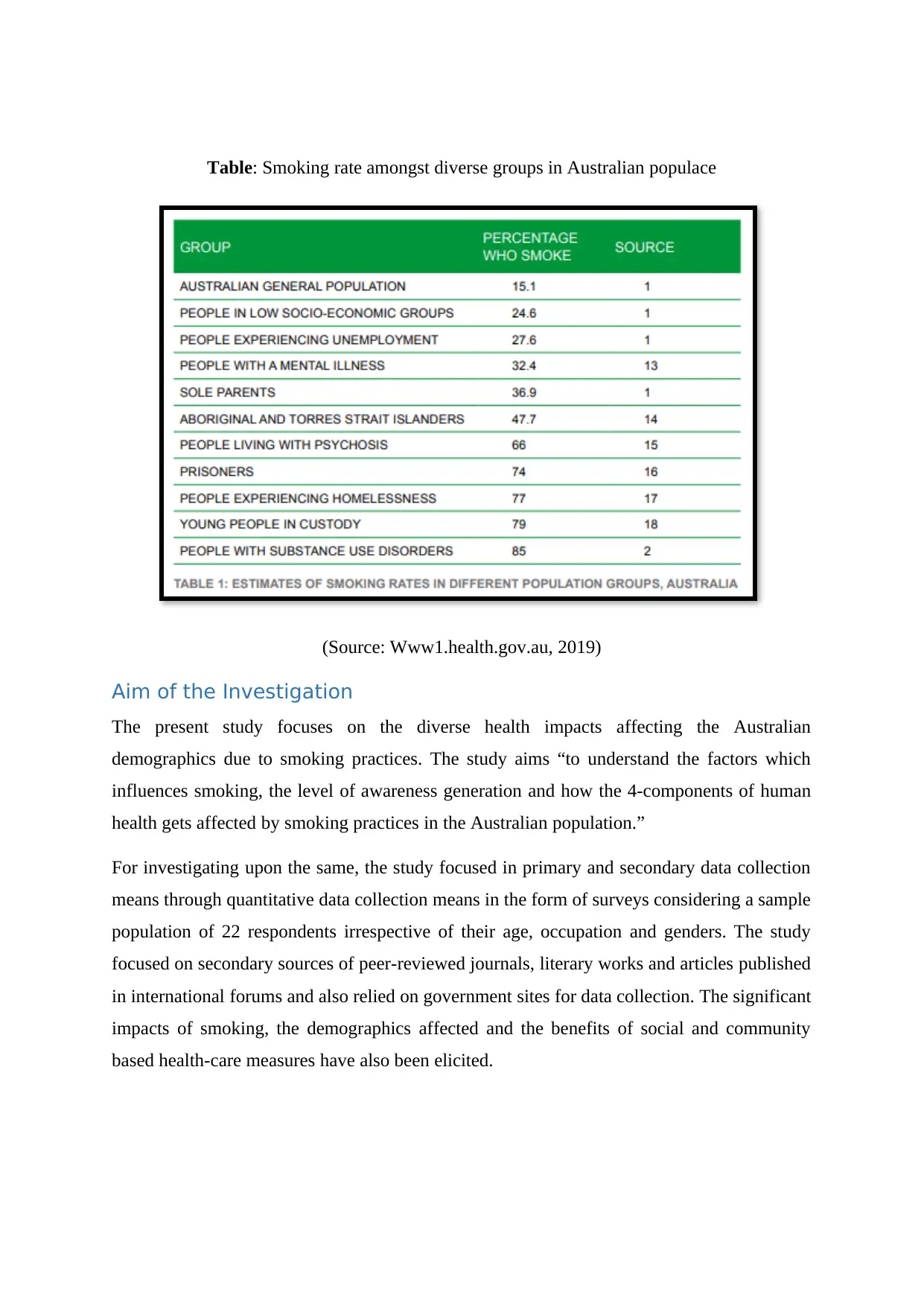
This report provides a comprehensive analysis of smoking practices in Australia, examining the factors that influence smoking uptake and patterns within the population. It explores the health impacts of smoking on physical, mental, social, and emotional well-being, highlighting the disparities across different demographic groups, including indigenous Australians and those with mental health issues. The report investigates the level of awareness regarding smoking prevention and the effectiveness of government strategies, such as taxation, mass media campaigns, and legislative measures. It also discusses the limitations of existing research and suggests areas for future improvements, including addressing cultural behaviors, improving access to cessation support, and strengthening research on interventions for disadvantaged populations. The study utilizes both primary and secondary data, drawing from surveys, peer-reviewed journals, and government sources to provide a detailed overview of the issue, including an analysis of the smoking rates among various age groups and genders, and the impact of smoking on the Wellness Wheel, which encompasses various aspects of an individual's life.
1 out of 21
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.