A Report on the Financial Management of PBS Expenditure in Australia
VerifiedAdded on 2021/04/24
|12
|3056
|36
Report
AI Summary
This report provides a critical analysis of the Australian Pharmaceutical Benefits Scheme (PBS), focusing on its financial management and the escalating costs of subsidized medicines. It examines the PBS's operational background, statistical data, and the factors contributing to increased expenditure, such as improper medication management, pricing discrepancies compared to other countries, and the absence of an independent expert decision-making panel. The report highlights the increasing financial burden on the Australian economy, with expenditures rising significantly over the years. It then proposes several recommendations to address these issues, including establishing an independent expert panel for decision-making, stricter regulations on generic medicine pricing, and raising customer awareness about cost-effective drug choices. The conclusion emphasizes the need for reforms to control the growing expenditure and ensure the long-term sustainability of the PBS.

HEALTH FINANCIAL MANAGEMENT
Student Name –
Student ID -
1
Student Name –
Student ID -
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Executive summary.................................................................................................3
Introduction............................................................................................................4
General discussion of issue.....................................................................................4
Exploring Issue........................................................................................................7
Conclusion............................................................................................................10
References............................................................................................................11
2
Executive summary.................................................................................................3
Introduction............................................................................................................4
General discussion of issue.....................................................................................4
Exploring Issue........................................................................................................7
Conclusion............................................................................................................10
References............................................................................................................11
2
Executive summary
Australian Pharmaceutical Benefits Scheme is a medical scheme by the
Australian government to provide affordable, protective and effective medicines to
people. This scheme is a 50 years old scheme functional since World War 1st. The
PBS scheme is working efficiently to fulfil its objective yet there has been a huge
escalation in the expenditure of PBS from last few decades. The rise in PBS
expenditure has lead to financial burdens on the Australian economy. From 1991 to
2002 there has been more than $3 billion rises in expenditure followed by 6% yearly
rise from 2010-2011. The cost of prescription drugs is very high in Australia where
the government pays almost 80% of the cost portion. The statistical studies indicate
that Australian pharmaceutical prices were lower from USA, UK and other countries
till 19th century but in recent statistics (2011) there is a huge increase in Australian
medicine expenditure compared to other countries.
The issues leading to growth in PBS expenditure involves improper
medication management, no expert decision-making team and improper pharmacy
agreements lead to increase in PBS cost. There are certain changes required in PBS
system to overcome the extra growing expenditure rate. These changes involve proper
expert panel to make decisions, managing medicine listing, pricing and subsidiaries as
well as creating customer awareness. These recommendations can help to get a
control over growing expenditure and better functionality of Pharmaceutical Benefits
Scheme.
3
Australian Pharmaceutical Benefits Scheme is a medical scheme by the
Australian government to provide affordable, protective and effective medicines to
people. This scheme is a 50 years old scheme functional since World War 1st. The
PBS scheme is working efficiently to fulfil its objective yet there has been a huge
escalation in the expenditure of PBS from last few decades. The rise in PBS
expenditure has lead to financial burdens on the Australian economy. From 1991 to
2002 there has been more than $3 billion rises in expenditure followed by 6% yearly
rise from 2010-2011. The cost of prescription drugs is very high in Australia where
the government pays almost 80% of the cost portion. The statistical studies indicate
that Australian pharmaceutical prices were lower from USA, UK and other countries
till 19th century but in recent statistics (2011) there is a huge increase in Australian
medicine expenditure compared to other countries.
The issues leading to growth in PBS expenditure involves improper
medication management, no expert decision-making team and improper pharmacy
agreements lead to increase in PBS cost. There are certain changes required in PBS
system to overcome the extra growing expenditure rate. These changes involve proper
expert panel to make decisions, managing medicine listing, pricing and subsidiaries as
well as creating customer awareness. These recommendations can help to get a
control over growing expenditure and better functionality of Pharmaceutical Benefits
Scheme.
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Introduction
The primary objective of Australian government healthcare system is to
provide affordable, protective and clinically effective medications to Australian
people ensuring taxpayers money value. The Australian Pharmaceutical Benefits
Scheme (PBS) plays an important role in achieving this objective as an essential part
of the healthcare system in Australia. PBS is operational from more than 50years in
Australia (part of National Medicines Policy) providing lifesaving essential medicines
at affordable rates to the public (Biggs, 2018). However, critical observations indicate
a huge escalation in subsidised medicine cost in Australia leading to the essentiality of
reviewing the PBS structure (Duckett et al. 2013).
This study is a critical analysis report on Australian Pharmaceutical Benefits
Scheme involving a study on its general background, statistics, processes and issues to
detect the possible reason behind increasing cost of PBS. Further, report involves
certain options to get a control over this growing cost of PBS expenditures and
pharmaceutical prices.
General discussion of issue
Functional since 1919, PBS is working to provide subsidised medicine to
sufferers of World War 1 to Australian people of 21st century. This scheme involves a
list of prescribed medicines that are provided to the patient at government-subsidised
cost (9.4 The Pharmaceutical Benefits Scheme, 2018). The cost of prescription drugs
in Australia is very high that involves minimum $1.3 billion/year or $3.5 million/day
covering 14% budget of PBS (Mellish et al. 2015). According to Blanch, Pearson &
Haber (2014) studies only one drug named atorvastatin cost around $700 million/year
to the Australian government and the individual patient. Australian PBS pays
$51/30tablet box whereas New Zealand scheme pays only $5.80/90tablets box of
40mg atorvastatin. This example indicates a critical abnormality in the financial
management system of pharmaceutical benefits scheme of Australia. The below-
provided table demonstrates expenditure on PBS by commonwealth since 1991
(Mellish et al. 2015).
Date (to June) Expenditure on PBS
4
The primary objective of Australian government healthcare system is to
provide affordable, protective and clinically effective medications to Australian
people ensuring taxpayers money value. The Australian Pharmaceutical Benefits
Scheme (PBS) plays an important role in achieving this objective as an essential part
of the healthcare system in Australia. PBS is operational from more than 50years in
Australia (part of National Medicines Policy) providing lifesaving essential medicines
at affordable rates to the public (Biggs, 2018). However, critical observations indicate
a huge escalation in subsidised medicine cost in Australia leading to the essentiality of
reviewing the PBS structure (Duckett et al. 2013).
This study is a critical analysis report on Australian Pharmaceutical Benefits
Scheme involving a study on its general background, statistics, processes and issues to
detect the possible reason behind increasing cost of PBS. Further, report involves
certain options to get a control over this growing cost of PBS expenditures and
pharmaceutical prices.
General discussion of issue
Functional since 1919, PBS is working to provide subsidised medicine to
sufferers of World War 1 to Australian people of 21st century. This scheme involves a
list of prescribed medicines that are provided to the patient at government-subsidised
cost (9.4 The Pharmaceutical Benefits Scheme, 2018). The cost of prescription drugs
in Australia is very high that involves minimum $1.3 billion/year or $3.5 million/day
covering 14% budget of PBS (Mellish et al. 2015). According to Blanch, Pearson &
Haber (2014) studies only one drug named atorvastatin cost around $700 million/year
to the Australian government and the individual patient. Australian PBS pays
$51/30tablet box whereas New Zealand scheme pays only $5.80/90tablets box of
40mg atorvastatin. This example indicates a critical abnormality in the financial
management system of pharmaceutical benefits scheme of Australia. The below-
provided table demonstrates expenditure on PBS by commonwealth since 1991
(Mellish et al. 2015).
Date (to June) Expenditure on PBS
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
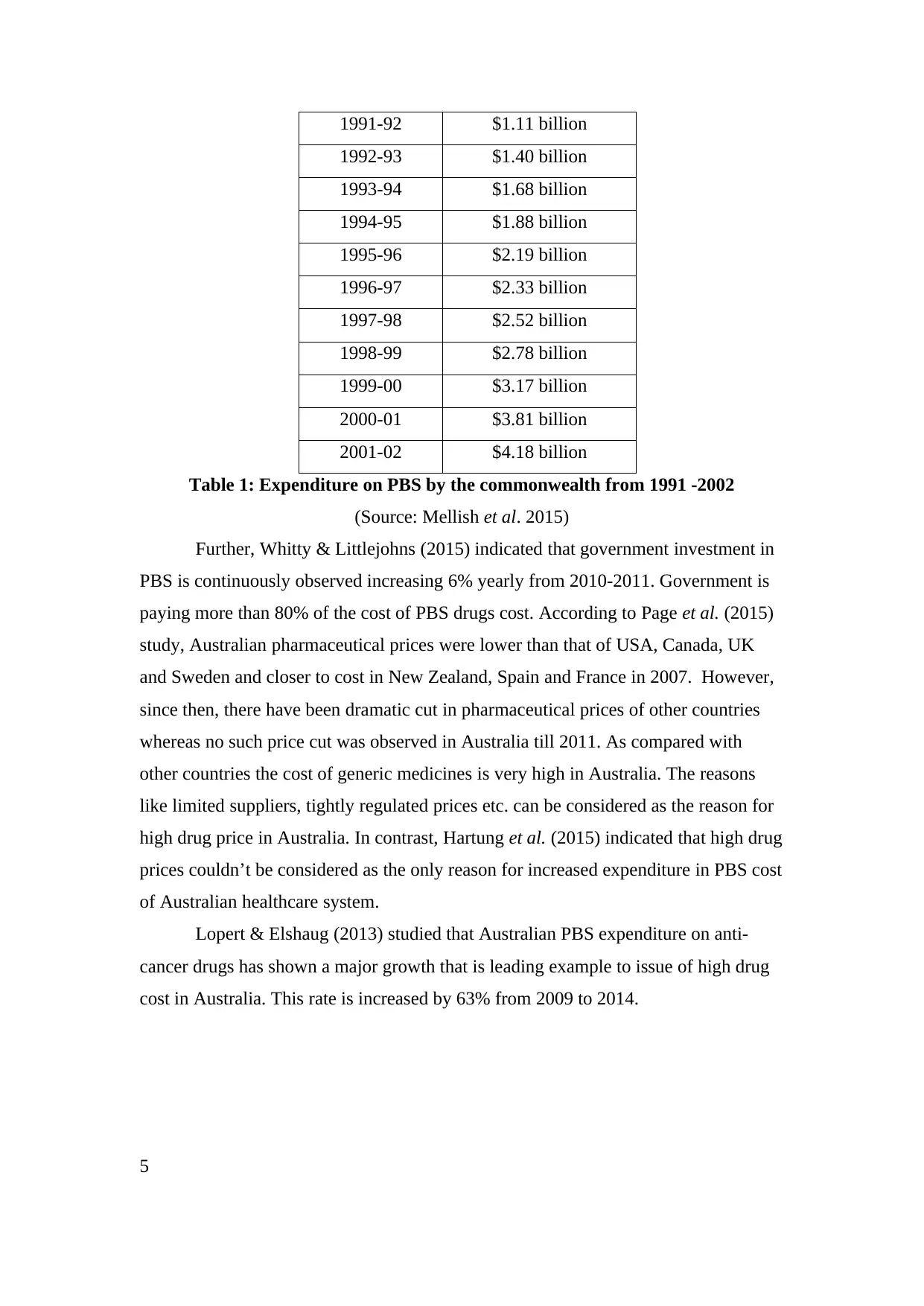
1991-92 $1.11 billion
1992-93 $1.40 billion
1993-94 $1.68 billion
1994-95 $1.88 billion
1995-96 $2.19 billion
1996-97 $2.33 billion
1997-98 $2.52 billion
1998-99 $2.78 billion
1999-00 $3.17 billion
2000-01 $3.81 billion
2001-02 $4.18 billion
Table 1: Expenditure on PBS by the commonwealth from 1991 -2002
(Source: Mellish et al. 2015)
Further, Whitty & Littlejohns (2015) indicated that government investment in
PBS is continuously observed increasing 6% yearly from 2010-2011. Government is
paying more than 80% of the cost of PBS drugs cost. According to Page et al. (2015)
study, Australian pharmaceutical prices were lower than that of USA, Canada, UK
and Sweden and closer to cost in New Zealand, Spain and France in 2007. However,
since then, there have been dramatic cut in pharmaceutical prices of other countries
whereas no such price cut was observed in Australia till 2011. As compared with
other countries the cost of generic medicines is very high in Australia. The reasons
like limited suppliers, tightly regulated prices etc. can be considered as the reason for
high drug price in Australia. In contrast, Hartung et al. (2015) indicated that high drug
prices couldn’t be considered as the only reason for increased expenditure in PBS cost
of Australian healthcare system.
Lopert & Elshaug (2013) studied that Australian PBS expenditure on anti-
cancer drugs has shown a major growth that is leading example to issue of high drug
cost in Australia. This rate is increased by 63% from 2009 to 2014.
5
1992-93 $1.40 billion
1993-94 $1.68 billion
1994-95 $1.88 billion
1995-96 $2.19 billion
1996-97 $2.33 billion
1997-98 $2.52 billion
1998-99 $2.78 billion
1999-00 $3.17 billion
2000-01 $3.81 billion
2001-02 $4.18 billion
Table 1: Expenditure on PBS by the commonwealth from 1991 -2002
(Source: Mellish et al. 2015)
Further, Whitty & Littlejohns (2015) indicated that government investment in
PBS is continuously observed increasing 6% yearly from 2010-2011. Government is
paying more than 80% of the cost of PBS drugs cost. According to Page et al. (2015)
study, Australian pharmaceutical prices were lower than that of USA, Canada, UK
and Sweden and closer to cost in New Zealand, Spain and France in 2007. However,
since then, there have been dramatic cut in pharmaceutical prices of other countries
whereas no such price cut was observed in Australia till 2011. As compared with
other countries the cost of generic medicines is very high in Australia. The reasons
like limited suppliers, tightly regulated prices etc. can be considered as the reason for
high drug price in Australia. In contrast, Hartung et al. (2015) indicated that high drug
prices couldn’t be considered as the only reason for increased expenditure in PBS cost
of Australian healthcare system.
Lopert & Elshaug (2013) studied that Australian PBS expenditure on anti-
cancer drugs has shown a major growth that is leading example to issue of high drug
cost in Australia. This rate is increased by 63% from 2009 to 2014.
5
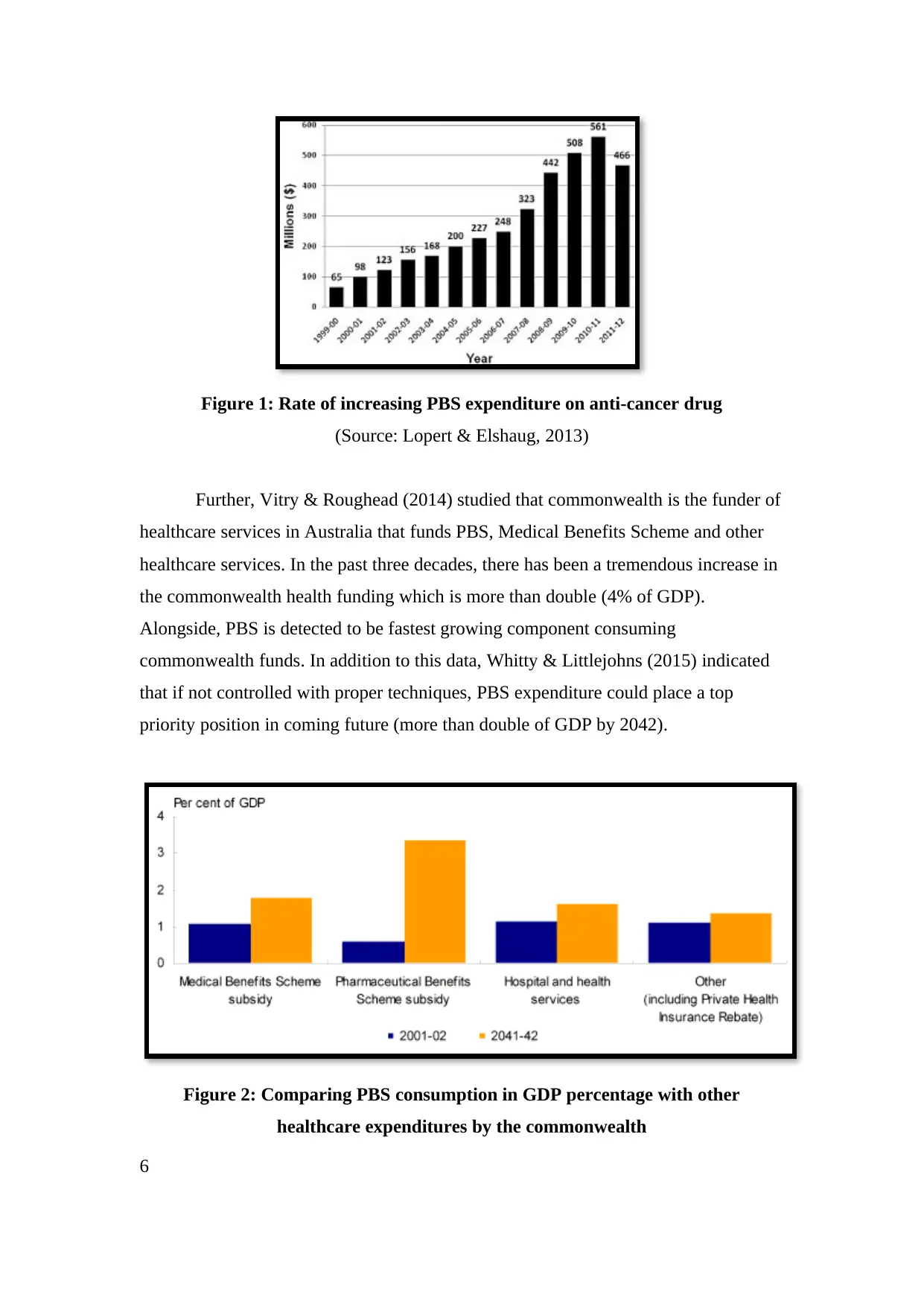
Figure 1: Rate of increasing PBS expenditure on anti-cancer drug
(Source: Lopert & Elshaug, 2013)
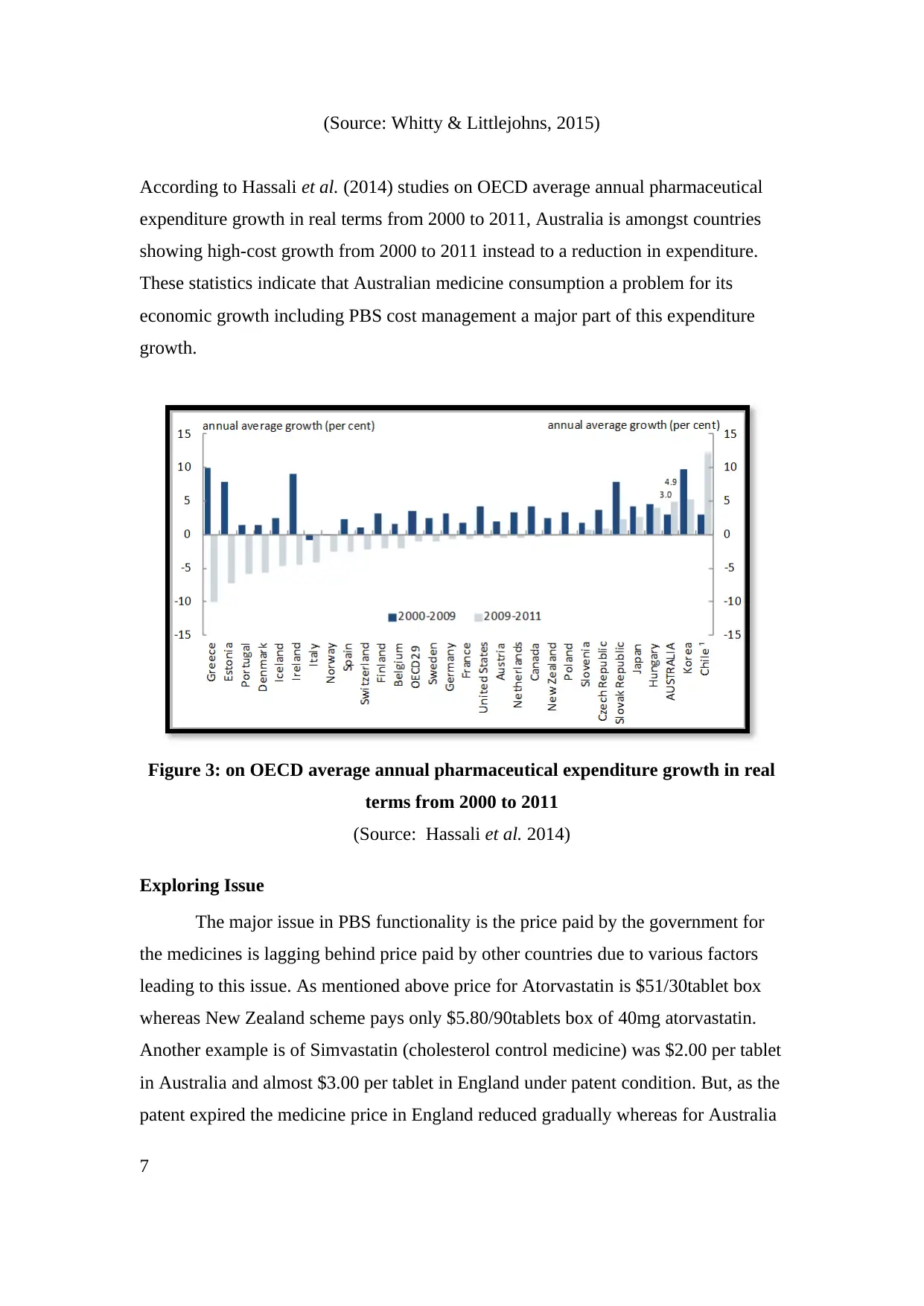
Further, Vitry & Roughead (2014) studied that commonwealth is the funder of
healthcare services in Australia that funds PBS, Medical Benefits Scheme and other
healthcare services. In the past three decades, there has been a tremendous increase in
the commonwealth health funding which is more than double (4% of GDP).
Alongside, PBS is detected to be fastest growing component consuming
commonwealth funds. In addition to this data, Whitty & Littlejohns (2015) indicated
that if not controlled with proper techniques, PBS expenditure could place a top
priority position in coming future (more than double of GDP by 2042).
Figure 2: Comparing PBS consumption in GDP percentage with other
healthcare expenditures by the commonwealth
6
(Source: Lopert & Elshaug, 2013)
Further, Vitry & Roughead (2014) studied that commonwealth is the funder of
healthcare services in Australia that funds PBS, Medical Benefits Scheme and other
healthcare services. In the past three decades, there has been a tremendous increase in
the commonwealth health funding which is more than double (4% of GDP).
Alongside, PBS is detected to be fastest growing component consuming
commonwealth funds. In addition to this data, Whitty & Littlejohns (2015) indicated
that if not controlled with proper techniques, PBS expenditure could place a top
priority position in coming future (more than double of GDP by 2042).
Figure 2: Comparing PBS consumption in GDP percentage with other
healthcare expenditures by the commonwealth
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
(Source: Whitty & Littlejohns, 2015)
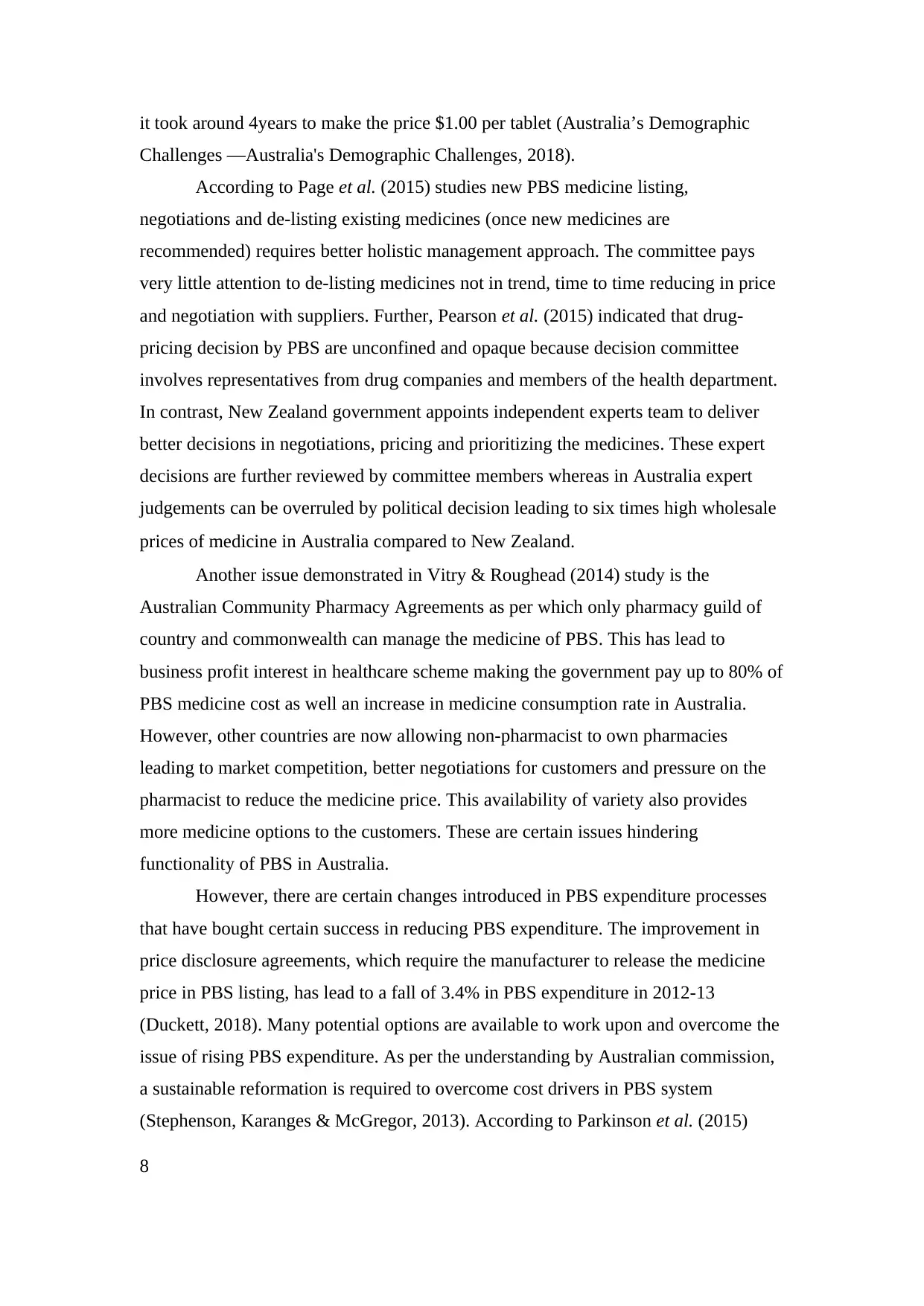
According to Hassali et al. (2014) studies on OECD average annual pharmaceutical
expenditure growth in real terms from 2000 to 2011, Australia is amongst countries
showing high-cost growth from 2000 to 2011 instead to a reduction in expenditure.
These statistics indicate that Australian medicine consumption a problem for its
economic growth including PBS cost management a major part of this expenditure
growth.
Figure 3: on OECD average annual pharmaceutical expenditure growth in real
terms from 2000 to 2011
(Source: Hassali et al. 2014)
Exploring Issue
The major issue in PBS functionality is the price paid by the government for
the medicines is lagging behind price paid by other countries due to various factors
leading to this issue. As mentioned above price for Atorvastatin is $51/30tablet box
whereas New Zealand scheme pays only $5.80/90tablets box of 40mg atorvastatin.
Another example is of Simvastatin (cholesterol control medicine) was $2.00 per tablet
in Australia and almost $3.00 per tablet in England under patent condition. But, as the
patent expired the medicine price in England reduced gradually whereas for Australia
7
According to Hassali et al. (2014) studies on OECD average annual pharmaceutical
expenditure growth in real terms from 2000 to 2011, Australia is amongst countries
showing high-cost growth from 2000 to 2011 instead to a reduction in expenditure.
These statistics indicate that Australian medicine consumption a problem for its
economic growth including PBS cost management a major part of this expenditure
growth.
Figure 3: on OECD average annual pharmaceutical expenditure growth in real
terms from 2000 to 2011
(Source: Hassali et al. 2014)
Exploring Issue
The major issue in PBS functionality is the price paid by the government for
the medicines is lagging behind price paid by other countries due to various factors
leading to this issue. As mentioned above price for Atorvastatin is $51/30tablet box
whereas New Zealand scheme pays only $5.80/90tablets box of 40mg atorvastatin.
Another example is of Simvastatin (cholesterol control medicine) was $2.00 per tablet
in Australia and almost $3.00 per tablet in England under patent condition. But, as the
patent expired the medicine price in England reduced gradually whereas for Australia
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
it took around 4years to make the price $1.00 per tablet (Australia’s Demographic
Challenges —Australia's Demographic Challenges, 2018).
According to Page et al. (2015) studies new PBS medicine listing,
negotiations and de-listing existing medicines (once new medicines are
recommended) requires better holistic management approach. The committee pays
very little attention to de-listing medicines not in trend, time to time reducing in price
and negotiation with suppliers. Further, Pearson et al. (2015) indicated that drug-
pricing decision by PBS are unconfined and opaque because decision committee
involves representatives from drug companies and members of the health department.
In contrast, New Zealand government appoints independent experts team to deliver
better decisions in negotiations, pricing and prioritizing the medicines. These expert
decisions are further reviewed by committee members whereas in Australia expert
judgements can be overruled by political decision leading to six times high wholesale
prices of medicine in Australia compared to New Zealand.
Another issue demonstrated in Vitry & Roughead (2014) study is the
Australian Community Pharmacy Agreements as per which only pharmacy guild of
country and commonwealth can manage the medicine of PBS. This has lead to
business profit interest in healthcare scheme making the government pay up to 80% of
PBS medicine cost as well an increase in medicine consumption rate in Australia.
However, other countries are now allowing non-pharmacist to own pharmacies
leading to market competition, better negotiations for customers and pressure on the
pharmacist to reduce the medicine price. This availability of variety also provides
more medicine options to the customers. These are certain issues hindering
functionality of PBS in Australia.
However, there are certain changes introduced in PBS expenditure processes
that have bought certain success in reducing PBS expenditure. The improvement in
price disclosure agreements, which require the manufacturer to release the medicine
price in PBS listing, has lead to a fall of 3.4% in PBS expenditure in 2012-13
(Duckett, 2018). Many potential options are available to work upon and overcome the
issue of rising PBS expenditure. As per the understanding by Australian commission,
a sustainable reformation is required to overcome cost drivers in PBS system
(Stephenson, Karanges & McGregor, 2013). According to Parkinson et al. (2015)
8
Challenges —Australia's Demographic Challenges, 2018).
According to Page et al. (2015) studies new PBS medicine listing,
negotiations and de-listing existing medicines (once new medicines are
recommended) requires better holistic management approach. The committee pays
very little attention to de-listing medicines not in trend, time to time reducing in price
and negotiation with suppliers. Further, Pearson et al. (2015) indicated that drug-
pricing decision by PBS are unconfined and opaque because decision committee
involves representatives from drug companies and members of the health department.
In contrast, New Zealand government appoints independent experts team to deliver
better decisions in negotiations, pricing and prioritizing the medicines. These expert
decisions are further reviewed by committee members whereas in Australia expert
judgements can be overruled by political decision leading to six times high wholesale
prices of medicine in Australia compared to New Zealand.
Another issue demonstrated in Vitry & Roughead (2014) study is the
Australian Community Pharmacy Agreements as per which only pharmacy guild of
country and commonwealth can manage the medicine of PBS. This has lead to
business profit interest in healthcare scheme making the government pay up to 80% of
PBS medicine cost as well an increase in medicine consumption rate in Australia.
However, other countries are now allowing non-pharmacist to own pharmacies
leading to market competition, better negotiations for customers and pressure on the
pharmacist to reduce the medicine price. This availability of variety also provides
more medicine options to the customers. These are certain issues hindering
functionality of PBS in Australia.
However, there are certain changes introduced in PBS expenditure processes
that have bought certain success in reducing PBS expenditure. The improvement in
price disclosure agreements, which require the manufacturer to release the medicine
price in PBS listing, has lead to a fall of 3.4% in PBS expenditure in 2012-13
(Duckett, 2018). Many potential options are available to work upon and overcome the
issue of rising PBS expenditure. As per the understanding by Australian commission,
a sustainable reformation is required to overcome cost drivers in PBS system
(Stephenson, Karanges & McGregor, 2013). According to Parkinson et al. (2015)
8
studies, PBS expenditures can be controlled by, freezing expenditures at the current
stage, decreasing PBS subsidies amount and reducing coverage of prescribed drugs in
PBS. The freezing expenditures of medicine at current stage involve a balance where
new medicines will only be listed with the removal of similar existing medicines in
PBS list. This process will provide a huge control over continuously increasing PBS
expenditure cost. Further, Vitry & Roughead (2014) suggested that establishing an
independent team to manage PBS decision and limiting the role of government will
significantly improve negotiations and management of price listing in medicines. The
Pharmaceutical Management Agency (PHARMAC) of New Zealand is a perfect
example to follow in this case. This independent entity will help to rationalise the
decision-making process supported with the logical and technical skill of experts.
Page et al. (2015) studied another method to overcome growing PBS
expenditure that involves tough regulations on generic medicine pricing in Australia.
The generic drugs are extremely costly in Australia being 7times costlier than New
Zealand. The companies in Australia producing generic medicine have very low R&D
and manufacturing cost. Therefore, it is justified that a control over high generic
medicine cost is a must because it covers approximately 88% savings in Australia.
There is a need of 50% cut-off in generic medicine price compared to originator price
as soon as the patent expires.
Lastly, Hartung et al. (2015) studied future reforming strategies of cost-
effective PBS choices. This involves encouraging people to use cost-effective drugs
from the therapeutic list as per their Doctor’s advice. People can smartly select their
drug by applying a sense of strategy that can be explained to them by the expert
group. This group can help people to understand the benefit of their choices to
themselves as well as government. Therefore, these three strategies of establishing an
independent entity, tougher generic pricing rules and awareness among people
regarding medicine use can help to save more than $1.6 million yearly in PBS
expenditure (Duckett, 2018). In this manner, the PBS can work differently getting
control over the issue of growing expenditure.
9
stage, decreasing PBS subsidies amount and reducing coverage of prescribed drugs in
PBS. The freezing expenditures of medicine at current stage involve a balance where
new medicines will only be listed with the removal of similar existing medicines in
PBS list. This process will provide a huge control over continuously increasing PBS
expenditure cost. Further, Vitry & Roughead (2014) suggested that establishing an
independent team to manage PBS decision and limiting the role of government will
significantly improve negotiations and management of price listing in medicines. The
Pharmaceutical Management Agency (PHARMAC) of New Zealand is a perfect
example to follow in this case. This independent entity will help to rationalise the
decision-making process supported with the logical and technical skill of experts.
Page et al. (2015) studied another method to overcome growing PBS
expenditure that involves tough regulations on generic medicine pricing in Australia.
The generic drugs are extremely costly in Australia being 7times costlier than New
Zealand. The companies in Australia producing generic medicine have very low R&D
and manufacturing cost. Therefore, it is justified that a control over high generic
medicine cost is a must because it covers approximately 88% savings in Australia.
There is a need of 50% cut-off in generic medicine price compared to originator price
as soon as the patent expires.
Lastly, Hartung et al. (2015) studied future reforming strategies of cost-
effective PBS choices. This involves encouraging people to use cost-effective drugs
from the therapeutic list as per their Doctor’s advice. People can smartly select their
drug by applying a sense of strategy that can be explained to them by the expert
group. This group can help people to understand the benefit of their choices to
themselves as well as government. Therefore, these three strategies of establishing an
independent entity, tougher generic pricing rules and awareness among people
regarding medicine use can help to save more than $1.6 million yearly in PBS
expenditure (Duckett, 2018). In this manner, the PBS can work differently getting
control over the issue of growing expenditure.
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Conclusion
The study involves a critical analysis of the Pharmaceutical Benefits Scheme
of Australian government working to release the uncertain burden of drug expenses
for Australian people. The PBS scheme in process of fulfilling its objective is
becoming a financial disturbance on Australian economy with continuously growing
expenditures. From 1991 to 2001 the expenditure grew from $1.11 billion to $4.18
billion with nearly 6% yearly increase from 2010-2011. This uncontrolled PBS
expenditure is due to detected issues like uncontrolled drug rates, improper drug
listing, no negotiations, lacking proper expert panel in decision committee, scheme
agreements and unawareness among people. These issues are leading to an improper
increase in PBS expenditure.
However, the study involves certain recommendations to overcome these
issues to balance PBS expenditure. Firstly, implementing independent expert panel, to
handle PBS decisions with their skilful and logical suggestion. Further, freezing
expenditures, decreasing PBS subsidiaries and reducing prescribed drug coverage
could also help to minimise expenses. Further, the control over generic medicine
pricing can also help to control PBS expenditure rate. Lastly, creating awareness
among people to pick medicine in a smarter and safer manner would be beneficial for
the government as well as people themselves. The functionality of PBS is good but a
control over growing expenditure will help to get a better healthcare system in
Australia.
10
The study involves a critical analysis of the Pharmaceutical Benefits Scheme
of Australian government working to release the uncertain burden of drug expenses
for Australian people. The PBS scheme in process of fulfilling its objective is
becoming a financial disturbance on Australian economy with continuously growing
expenditures. From 1991 to 2001 the expenditure grew from $1.11 billion to $4.18
billion with nearly 6% yearly increase from 2010-2011. This uncontrolled PBS
expenditure is due to detected issues like uncontrolled drug rates, improper drug
listing, no negotiations, lacking proper expert panel in decision committee, scheme
agreements and unawareness among people. These issues are leading to an improper
increase in PBS expenditure.
However, the study involves certain recommendations to overcome these
issues to balance PBS expenditure. Firstly, implementing independent expert panel, to
handle PBS decisions with their skilful and logical suggestion. Further, freezing
expenditures, decreasing PBS subsidiaries and reducing prescribed drug coverage
could also help to minimise expenses. Further, the control over generic medicine
pricing can also help to control PBS expenditure rate. Lastly, creating awareness
among people to pick medicine in a smarter and safer manner would be beneficial for
the government as well as people themselves. The functionality of PBS is good but a
control over growing expenditure will help to get a better healthcare system in
Australia.
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

References
Books
Duckett, S. J., Breadon, P., Ginnivan, L., & Venkataraman, P. (2013). Australia's bad
drug deal: high pharmaceutical prices. Melbourne: Grattan Institute.
Journals
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of
prescription opioid use, costs and related harms in Australia. British journal of
clinical pharmacology, 78(5), 1159-1166.
Hartung, D. M., Bourdette, D. N., Ahmed, S. M., & Whitham, R. H. (2015). The cost
of multiple sclerosis drugs in the US and the pharmaceutical industry Too big to
fail?. Neurology, 84(21), 2185-2192.
Hassali, M. A., Alrasheedy, A. A., McLachlan, A., Nguyen, T. A., Al-Tamimi, S. K.,
Ibrahim, M. I. M., & Aljadhey, H. (2014). The experiences of implementing
generic medicine policy in eight countries: a review and recommendations for a
successful promotion of generic medicine use. Saudi pharmaceutical
journal, 22(6), 491-503.
Lopert, R., & Elshaug, A. G. (2013). Australia’s ‘fourth hurdle’drug review
comparing costs and benefits holds lessons for the United States. Health
affairs, 32(4), 778-787.
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B.
J., ... & Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme
data collection: a practical guide for researchers. BMC research notes, 8(1), 634.
Page, E., Kemp-Casey, A., Korda, R., & Banks, E. (2015). Using Australian
Pharmaceutical Benefits Scheme data for pharmacoepidemiological research:
challenges and approaches. Public Health Res Pract, 25(4), e2541546.
Parkinson, B., Sermet, C., Clement, F., Crausaz, S., Godman, B., Garner, S., ... &
Elshaug, A. G. (2015). Disinvestment and value-based purchasing strategies for
pharmaceuticals: an international review. Pharmacoeconomics, 33(9), 905-924.
Pearson, S. A., Pesa, N., Langton, J. M., Drew, A., Faedo, M., & Robertson, J. (2015).
Studies using Australia's Pharmaceutical Benefits Scheme data for
pharmacoepidemiological research: a systematic review of the published literature
11
Books
Duckett, S. J., Breadon, P., Ginnivan, L., & Venkataraman, P. (2013). Australia's bad
drug deal: high pharmaceutical prices. Melbourne: Grattan Institute.
Journals
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of
prescription opioid use, costs and related harms in Australia. British journal of
clinical pharmacology, 78(5), 1159-1166.
Hartung, D. M., Bourdette, D. N., Ahmed, S. M., & Whitham, R. H. (2015). The cost
of multiple sclerosis drugs in the US and the pharmaceutical industry Too big to
fail?. Neurology, 84(21), 2185-2192.
Hassali, M. A., Alrasheedy, A. A., McLachlan, A., Nguyen, T. A., Al-Tamimi, S. K.,
Ibrahim, M. I. M., & Aljadhey, H. (2014). The experiences of implementing
generic medicine policy in eight countries: a review and recommendations for a
successful promotion of generic medicine use. Saudi pharmaceutical
journal, 22(6), 491-503.
Lopert, R., & Elshaug, A. G. (2013). Australia’s ‘fourth hurdle’drug review
comparing costs and benefits holds lessons for the United States. Health
affairs, 32(4), 778-787.
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B.
J., ... & Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme
data collection: a practical guide for researchers. BMC research notes, 8(1), 634.
Page, E., Kemp-Casey, A., Korda, R., & Banks, E. (2015). Using Australian
Pharmaceutical Benefits Scheme data for pharmacoepidemiological research:
challenges and approaches. Public Health Res Pract, 25(4), e2541546.
Parkinson, B., Sermet, C., Clement, F., Crausaz, S., Godman, B., Garner, S., ... &
Elshaug, A. G. (2015). Disinvestment and value-based purchasing strategies for
pharmaceuticals: an international review. Pharmacoeconomics, 33(9), 905-924.
Pearson, S. A., Pesa, N., Langton, J. M., Drew, A., Faedo, M., & Robertson, J. (2015).
Studies using Australia's Pharmaceutical Benefits Scheme data for
pharmacoepidemiological research: a systematic review of the published literature
11
(1987–2013). Pharmacoepidemiology and drug safety, 24(5), 447-455.
Stephenson, C. P., Karanges, E., & McGregor, I. S. (2013). Trends in the utilisation of
psychotropic medications in Australia from 2000 to 2011. Australian & New
Zealand Journal of Psychiatry, 47(1), 74-87.
Vitry, A., & Roughead, E. (2014). Managed entry agreements for pharmaceuticals in
Australia. Health Policy, 117(3), 345-352.
Whitty, J. A., & Littlejohns, P. (2015). Social values and health priority setting in
Australia: an analysis applied to the context of health technology
assessment. Health Policy, 119(2), 127-136.
Websites
9.4 The Pharmaceutical Benefits Scheme. (2018). Ncoa.gov.au. Retrieved 4 April
2018, from http://www.ncoa.gov.au/report/appendix-vol-1/9-4-pharmaceutical-
benefits-scheme.html
Australia’s Demographic Challenges —Australia's Demographic Challenges.
(2018). Demographics.treasury.gov.au. Retrieved 4 April 2018, from
http://demographics.treasury.gov.au/content/_download/australias_demographic_c
hallenges/html/adc-05.asp
Biggs, A. (2018). The Pharmaceutical Benefits Scheme - an Overview – Parliament of
Australia. Aph.gov.au. Retrieved 4 April 2018, from
https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/
Parliamentary_Library/Publications_Archive/archive/pbs
Duckett, S. (2018). Australia's Bad Drug Deal: High Pharmaceutical
Prices. Grattan.edu.au. Retrieved 4 April 2018, from https://grattan.edu.au/wp-
content/uploads/2014/04/Australias_Bad_Drug_Deal_FINAL.pdf
12
Stephenson, C. P., Karanges, E., & McGregor, I. S. (2013). Trends in the utilisation of
psychotropic medications in Australia from 2000 to 2011. Australian & New
Zealand Journal of Psychiatry, 47(1), 74-87.
Vitry, A., & Roughead, E. (2014). Managed entry agreements for pharmaceuticals in
Australia. Health Policy, 117(3), 345-352.
Whitty, J. A., & Littlejohns, P. (2015). Social values and health priority setting in
Australia: an analysis applied to the context of health technology
assessment. Health Policy, 119(2), 127-136.
Websites
9.4 The Pharmaceutical Benefits Scheme. (2018). Ncoa.gov.au. Retrieved 4 April
2018, from http://www.ncoa.gov.au/report/appendix-vol-1/9-4-pharmaceutical-
benefits-scheme.html
Australia’s Demographic Challenges —Australia's Demographic Challenges.
(2018). Demographics.treasury.gov.au. Retrieved 4 April 2018, from
http://demographics.treasury.gov.au/content/_download/australias_demographic_c
hallenges/html/adc-05.asp
Biggs, A. (2018). The Pharmaceutical Benefits Scheme - an Overview – Parliament of
Australia. Aph.gov.au. Retrieved 4 April 2018, from
https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/
Parliamentary_Library/Publications_Archive/archive/pbs
Duckett, S. (2018). Australia's Bad Drug Deal: High Pharmaceutical
Prices. Grattan.edu.au. Retrieved 4 April 2018, from https://grattan.edu.au/wp-
content/uploads/2014/04/Australias_Bad_Drug_Deal_FINAL.pdf
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.