Evidence-Based Practice: Automated Blood Pressure Devices for Children
VerifiedAdded on 2020/05/28
|14
|2665
|164
Report
AI Summary
This report examines the use of automated blood pressure devices compared to manual sphygmomanometers, focusing on their application in children within hospital settings. The study explores the advantages and disadvantages of both methods, highlighting the importance of accurate blood pressure measurement for effective patient care. The report analyzes evidence-based practices, including the PICO framework, to address the research question: “Is using an automated blood pressure monitoring system on children more accurate in monitoring the level of blood pressure compared to manual sphygmomanometers?” It discusses the limitations of manual methods, such as cuff size issues and the time-consuming nature of the process, in contrast to the efficiency of automated devices. The report also appraises the evidence, considering factors like device costs and the potential for human error, and concludes with recommendations for best practices in blood pressure monitoring, emphasizing the need for calibrated devices and medical expertise for accurate results. This report is a valuable resource for healthcare professionals seeking to optimize blood pressure measurement techniques.

0
AUTOMATED BLOOD PRESSURE DEVICE
Automated Blood Pressure Device
Name of the student
University name
Author’s note
AUTOMATED BLOOD PRESSURE DEVICE
Automated Blood Pressure Device
Name of the student
University name
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
AUTOMATED BLOOD PRESSURE DEVICE
Table of Contents
Introduction......................................................................................................................................2
Problem and answerable question...................................................................................................2
Locating the evidence......................................................................................................................3
Appraising the evidence..................................................................................................................5
Summary of practice........................................................................................................................7
Conclusion.......................................................................................................................................8
References........................................................................................................................................9
Appendix 1.....................................................................................................................................12
Appendix 2.....................................................................................................................................13
AUTOMATED BLOOD PRESSURE DEVICE
Table of Contents
Introduction......................................................................................................................................2
Problem and answerable question...................................................................................................2
Locating the evidence......................................................................................................................3
Appraising the evidence..................................................................................................................5
Summary of practice........................................................................................................................7
Conclusion.......................................................................................................................................8
References........................................................................................................................................9
Appendix 1.....................................................................................................................................12
Appendix 2.....................................................................................................................................13
2
AUTOMATED BLOOD PRESSURE DEVICE
Introduction
The essay focuses upon the concept of evidence based practices in nursing care. The
evidence based practise methods helps in redesigning a safe, efficient and effective care. It helps
the practitioners approach questions related to health care in an evaluative and qualitative
manner. A study has been conducted in the assignment researching the benefits of using
automated device for measuring the blood pressure of children in hospitals rather than manual
devices. There are different school of thoughts both stating for and against the use of automated
measurement devices over the manual ones. The question raised here has been supported through
sufficient evidences and resources which have been further critically reviewed for reliability and
validity.
Problem and answerable question
The blood pressure can be measured using both manual and automated measuring
techniques. The manual device is also known as the auscularity device whereas the automated
device is known as oscillometric device. As commented by Myers (2014), measuring accurate
blood pressure helps in monitoring the proper functioning of different body systems and organs.
The erroneous blood pressure measurement may result in wrong treatments being administered
to the patients. Therefore, acute measurements procedures and techniques need to be developed.
The focus of the assignment is use of automated blood pressure devices over manual devices for
measuring the blood pressure of children within hospitals. A number of arguments have been
placed in favour of use of the automated techniques over manual measurement processes. As
commented by Mansoor et al.(2016), the automated readings helps in representing the true blood
pressure because of the built-in deflation rate of the device. However as argued by
AUTOMATED BLOOD PRESSURE DEVICE
Introduction
The essay focuses upon the concept of evidence based practices in nursing care. The
evidence based practise methods helps in redesigning a safe, efficient and effective care. It helps
the practitioners approach questions related to health care in an evaluative and qualitative
manner. A study has been conducted in the assignment researching the benefits of using
automated device for measuring the blood pressure of children in hospitals rather than manual
devices. There are different school of thoughts both stating for and against the use of automated
measurement devices over the manual ones. The question raised here has been supported through
sufficient evidences and resources which have been further critically reviewed for reliability and
validity.
Problem and answerable question
The blood pressure can be measured using both manual and automated measuring
techniques. The manual device is also known as the auscularity device whereas the automated
device is known as oscillometric device. As commented by Myers (2014), measuring accurate
blood pressure helps in monitoring the proper functioning of different body systems and organs.
The erroneous blood pressure measurement may result in wrong treatments being administered
to the patients. Therefore, acute measurements procedures and techniques need to be developed.
The focus of the assignment is use of automated blood pressure devices over manual devices for
measuring the blood pressure of children within hospitals. A number of arguments have been
placed in favour of use of the automated techniques over manual measurement processes. As
commented by Mansoor et al.(2016), the automated readings helps in representing the true blood
pressure because of the built-in deflation rate of the device. However as argued by
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
AUTOMATED BLOOD PRESSURE DEVICE
Daskalopoulou et al.(2015), the clinicians suggest occasional checking of the automated blood
pressure readings against the mercury sphygmomanometer. This is done to remove the chances
of any errors which may have crept during the process of blood pressure measurement. However,
finding the right size of cuff for accurate measurement of blood pressure in children often
becomes difficult (Lin, Chang, Chou & Lin, 2014). Therefore, the emphasis is shifted upon the
use of automated blood pressure measurement devices with a built-in deflation rate.
The research has been further substantiated with the help of developing a proper research
question. The question has been developed in the PICO format where the P stands for
Population, I stand for intervention, C stands for comparison and O stands for Outcome.
Therefore, the question which can be raised over here is: “Is using an automated blood pressure
monitoring system (I) on children (P) more accurate in monitoring the level of blood pressure
(O) compared to manual sphygmomanometers (C)?”
Locating the evidence
A number of evidence bases have been referred to in order to retrieve adequate
information regarding the benefits of choosing automated blood pressure measuring techniques
over manual sphygmomanometers. In order to understand the differences one needs to develop
sufficient idea regarding the different types of blood pressure measuring devices, their
functioning and efficiencies. The blood pressure is divided into two components- systolic and
diastolic pressure. The systolic pressure is when the heart is pumping and the diastolic pressure is
recorded when the heart is at rest. In this respect, mercury sphygmomanometers are one of the
old school manual methods of measuring blood pressure. The physician has to manually inflate
or deflate the cuffs around the arm till the systolic and diastolic pressures are recorded (Benmira
AUTOMATED BLOOD PRESSURE DEVICE
Daskalopoulou et al.(2015), the clinicians suggest occasional checking of the automated blood
pressure readings against the mercury sphygmomanometer. This is done to remove the chances
of any errors which may have crept during the process of blood pressure measurement. However,
finding the right size of cuff for accurate measurement of blood pressure in children often
becomes difficult (Lin, Chang, Chou & Lin, 2014). Therefore, the emphasis is shifted upon the
use of automated blood pressure measurement devices with a built-in deflation rate.
The research has been further substantiated with the help of developing a proper research
question. The question has been developed in the PICO format where the P stands for
Population, I stand for intervention, C stands for comparison and O stands for Outcome.
Therefore, the question which can be raised over here is: “Is using an automated blood pressure
monitoring system (I) on children (P) more accurate in monitoring the level of blood pressure
(O) compared to manual sphygmomanometers (C)?”
Locating the evidence
A number of evidence bases have been referred to in order to retrieve adequate
information regarding the benefits of choosing automated blood pressure measuring techniques
over manual sphygmomanometers. In order to understand the differences one needs to develop
sufficient idea regarding the different types of blood pressure measuring devices, their
functioning and efficiencies. The blood pressure is divided into two components- systolic and
diastolic pressure. The systolic pressure is when the heart is pumping and the diastolic pressure is
recorded when the heart is at rest. In this respect, mercury sphygmomanometers are one of the
old school manual methods of measuring blood pressure. The physician has to manually inflate
or deflate the cuffs around the arm till the systolic and diastolic pressures are recorded (Benmira
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
AUTOMATED BLOOD PRESSURE DEVICE
et al., 2016). However as argued by Chu et al.(2017), there are a number of limitations of using
the manual method of recording blood pressure such as appropriate adjustment of the cuff while
measuring the blood pressure. Children have thin arms resulting in loose fitting of the cuff,
which often results in erroneous recording of blood pressure. Additionally, the children often
become impatient during manual recording of the blood pressure which takes longer. The
automatic recording of blood pressure takes lesser time comparatively. The inflatable part of the
cuff needs to cover atleast 80% of the part of the patient’s arm (Neuhauser, Ellert, Thamm &
Adler, 2015). A child’s cuff measures less than 24 cms in diameter. Therefore, using a large cuff
may result in low blood pressure readings. However as argued by Benmira et al.(2016) most of
the hospitals lack different sized cuffs which affects accurate measurements.
As commented by Lin et al. (2016), fraudulent marking of the lower meniscus of
mercury can also result in inaccurate measurements being taken. Another variation which can be
used over here is an aneroid sphygmomanometer. The features of the devices are similar to
mercury sphygmomanometer excepting that here instated of using mercury for recording the
blood pressure, a dial gauge is used, which is connected to the cuff. As argued by Neuhauser,
Ellert, Thamm & Adler (2015), the dial gauge of the aneroid sphygmomanometers requires
recalibration on a frequent basis further questioning the accuracy of the device. The automated
blood pressure monitoring device measures the oscillations of the arteries using pressure sensors.
The oscillations are processed using an algorithm to convert them into systolic and diastolic
values which are displayed on a digital interface. The electronic sensors attached with the cuff
can accurately sense the systole and diastole pressures which control the deflation rate tightly
(Duncombe, Voss & Harris, 2017). Moreover, slight movement during the measurement of the
AUTOMATED BLOOD PRESSURE DEVICE
et al., 2016). However as argued by Chu et al.(2017), there are a number of limitations of using
the manual method of recording blood pressure such as appropriate adjustment of the cuff while
measuring the blood pressure. Children have thin arms resulting in loose fitting of the cuff,
which often results in erroneous recording of blood pressure. Additionally, the children often
become impatient during manual recording of the blood pressure which takes longer. The
automatic recording of blood pressure takes lesser time comparatively. The inflatable part of the
cuff needs to cover atleast 80% of the part of the patient’s arm (Neuhauser, Ellert, Thamm &
Adler, 2015). A child’s cuff measures less than 24 cms in diameter. Therefore, using a large cuff
may result in low blood pressure readings. However as argued by Benmira et al.(2016) most of
the hospitals lack different sized cuffs which affects accurate measurements.
As commented by Lin et al. (2016), fraudulent marking of the lower meniscus of
mercury can also result in inaccurate measurements being taken. Another variation which can be
used over here is an aneroid sphygmomanometer. The features of the devices are similar to
mercury sphygmomanometer excepting that here instated of using mercury for recording the
blood pressure, a dial gauge is used, which is connected to the cuff. As argued by Neuhauser,
Ellert, Thamm & Adler (2015), the dial gauge of the aneroid sphygmomanometers requires
recalibration on a frequent basis further questioning the accuracy of the device. The automated
blood pressure monitoring device measures the oscillations of the arteries using pressure sensors.
The oscillations are processed using an algorithm to convert them into systolic and diastolic
values which are displayed on a digital interface. The electronic sensors attached with the cuff
can accurately sense the systole and diastole pressures which control the deflation rate tightly
(Duncombe, Voss & Harris, 2017). Moreover, slight movement during the measurement of the
5
AUTOMATED BLOOD PRESSURE DEVICE
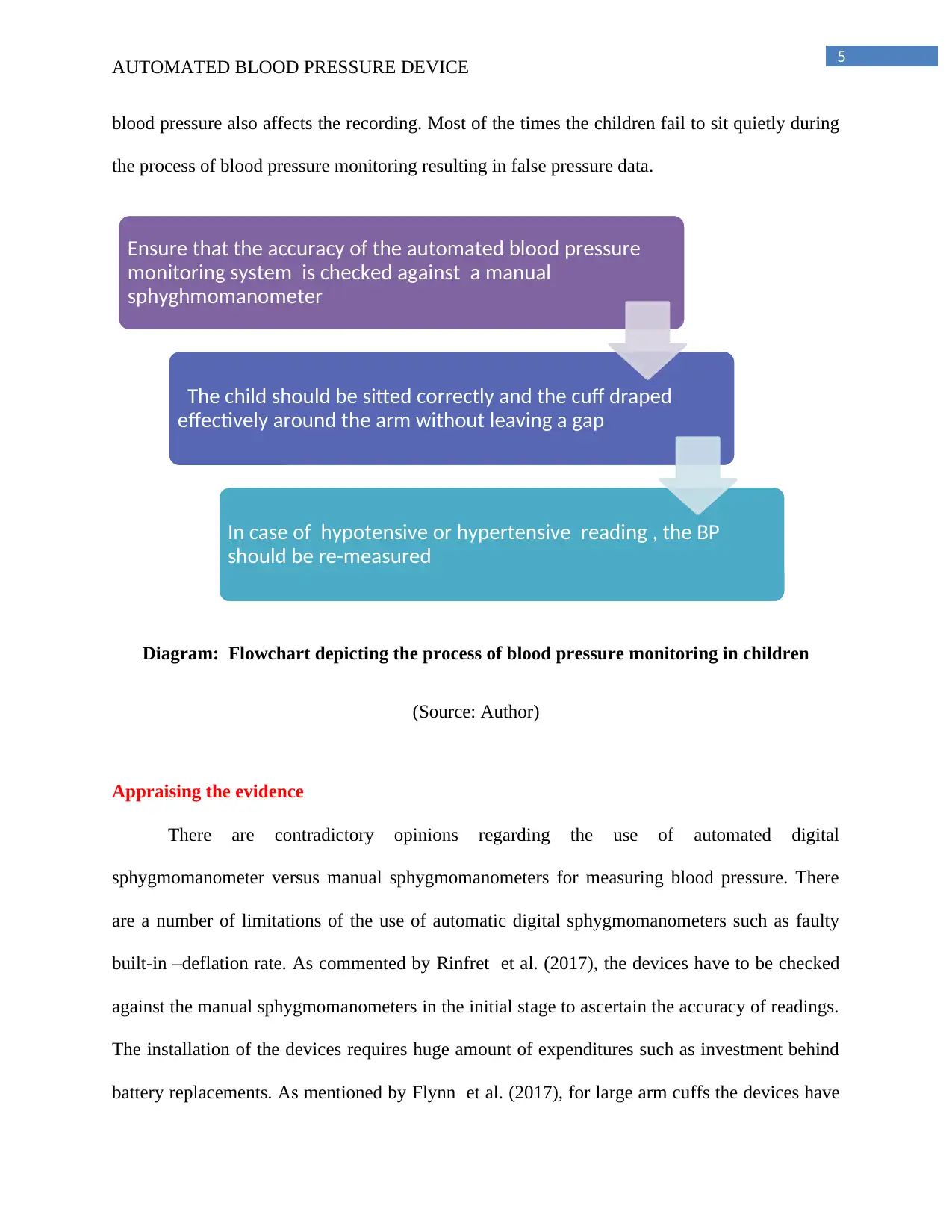
blood pressure also affects the recording. Most of the times the children fail to sit quietly during
the process of blood pressure monitoring resulting in false pressure data.
Diagram: Flowchart depicting the process of blood pressure monitoring in children
(Source: Author)
Appraising the evidence
There are contradictory opinions regarding the use of automated digital
sphygmomanometer versus manual sphygmomanometers for measuring blood pressure. There
are a number of limitations of the use of automatic digital sphygmomanometers such as faulty
built-in –deflation rate. As commented by Rinfret et al. (2017), the devices have to be checked
against the manual sphygmomanometers in the initial stage to ascertain the accuracy of readings.
The installation of the devices requires huge amount of expenditures such as investment behind
battery replacements. As mentioned by Flynn et al. (2017), for large arm cuffs the devices have
Ensure that the accuracy of the automated blood pressure
monitoring system is checked against a manual
sphyghmomanometer
The child should be sitted correctly and the cuff draped
effectively around the arm without leaving a gap
In case of hypotensive or hypertensive reading , the BP
should be re-measured
AUTOMATED BLOOD PRESSURE DEVICE
blood pressure also affects the recording. Most of the times the children fail to sit quietly during
the process of blood pressure monitoring resulting in false pressure data.
Diagram: Flowchart depicting the process of blood pressure monitoring in children
(Source: Author)
Appraising the evidence
There are contradictory opinions regarding the use of automated digital
sphygmomanometer versus manual sphygmomanometers for measuring blood pressure. There
are a number of limitations of the use of automatic digital sphygmomanometers such as faulty
built-in –deflation rate. As commented by Rinfret et al. (2017), the devices have to be checked
against the manual sphygmomanometers in the initial stage to ascertain the accuracy of readings.
The installation of the devices requires huge amount of expenditures such as investment behind
battery replacements. As mentioned by Flynn et al. (2017), for large arm cuffs the devices have
Ensure that the accuracy of the automated blood pressure
monitoring system is checked against a manual
sphyghmomanometer
The child should be sitted correctly and the cuff draped
effectively around the arm without leaving a gap
In case of hypotensive or hypertensive reading , the BP
should be re-measured
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
AUTOMATED BLOOD PRESSURE DEVICE
to be connected to an AC adaptor. The high cost associated with the devices does not restrict the
purchasing ability of the same. As argued by De Caen et al. (2015), the blood pressure reading
is also affected by the general health conditions of the patient. For example, the ones suffering
from hypertension might depict elevated levels of mercuric pressure. The problem situation may
be further analysed to find out the presence of some other health concerns such as presence of
high cholesterol content in the blood. This results in narrowing of the blood vessels resulting in
high pressure of blood within the arteries. As argued by Franssen et al. (2017), the chances of
human errors in automatic digital sphygmomanometers is minimum as most of the critical
operations are performed automatically.
Another concern which has been raised by experienced physicians regarding the manual
sphygmomanometers usage has been termed as clinical inertia. As mentioned by Daskalopoulou
et al. (2015), a physician can heat the onset of the korotkoff sounds somewhere between 140 and
138. Therefore, in most cases the physician to choose upon a particular number. Therefore, the
diagnosis often takes a hypothetical turn which may affect the quality of the care services.
However, as argued by Neuhauser, Ellert, Thamm & Adler (2015), children have higher level of
foetal haemoglobin which has less oxygen carrying capacity. In order to cope up with the
deprivation the heart has to pump more blood which raises the normal blood pressure level.
Therefore, along with the recording techniques in place certain degree of medical expertise is
also required. As argued by Rinfret et al. (2017), wrong interpretation of the results may affect
the particular treatment methods being administered to the child.
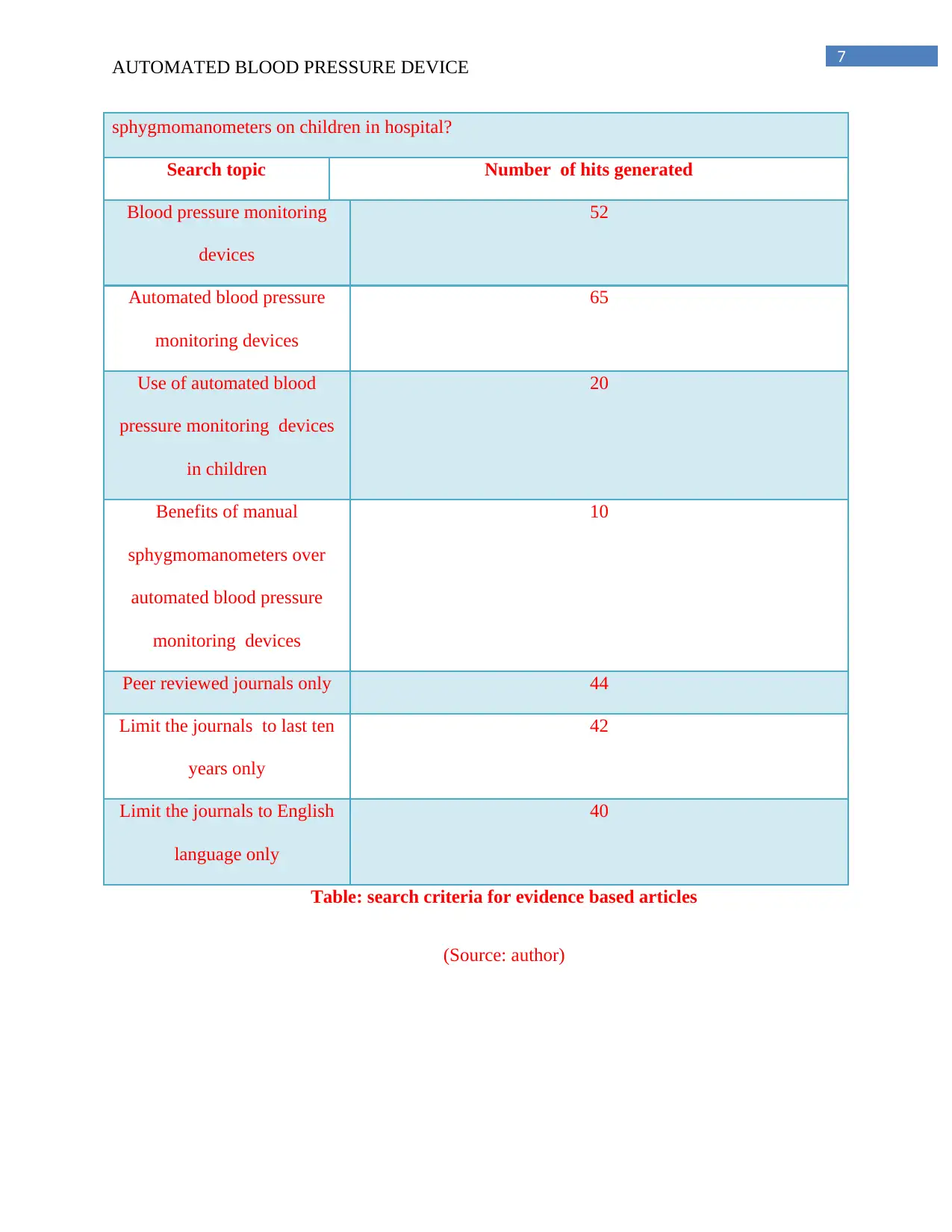
Database: CINAHL, Cochrane library , MEDLINE, Joanna Briggs
Is it appropriate to use automated blood pressure monitoring devices instead of manual
AUTOMATED BLOOD PRESSURE DEVICE
to be connected to an AC adaptor. The high cost associated with the devices does not restrict the
purchasing ability of the same. As argued by De Caen et al. (2015), the blood pressure reading
is also affected by the general health conditions of the patient. For example, the ones suffering
from hypertension might depict elevated levels of mercuric pressure. The problem situation may
be further analysed to find out the presence of some other health concerns such as presence of
high cholesterol content in the blood. This results in narrowing of the blood vessels resulting in
high pressure of blood within the arteries. As argued by Franssen et al. (2017), the chances of
human errors in automatic digital sphygmomanometers is minimum as most of the critical
operations are performed automatically.
Another concern which has been raised by experienced physicians regarding the manual
sphygmomanometers usage has been termed as clinical inertia. As mentioned by Daskalopoulou
et al. (2015), a physician can heat the onset of the korotkoff sounds somewhere between 140 and
138. Therefore, in most cases the physician to choose upon a particular number. Therefore, the
diagnosis often takes a hypothetical turn which may affect the quality of the care services.
However, as argued by Neuhauser, Ellert, Thamm & Adler (2015), children have higher level of
foetal haemoglobin which has less oxygen carrying capacity. In order to cope up with the
deprivation the heart has to pump more blood which raises the normal blood pressure level.
Therefore, along with the recording techniques in place certain degree of medical expertise is
also required. As argued by Rinfret et al. (2017), wrong interpretation of the results may affect
the particular treatment methods being administered to the child.
Database: CINAHL, Cochrane library , MEDLINE, Joanna Briggs
Is it appropriate to use automated blood pressure monitoring devices instead of manual
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
AUTOMATED BLOOD PRESSURE DEVICE
sphygmomanometers on children in hospital?
Search topic Number of hits generated
Blood pressure monitoring
devices
52
Automated blood pressure
monitoring devices
65
Use of automated blood
pressure monitoring devices
in children
20
Benefits of manual
sphygmomanometers over
automated blood pressure
monitoring devices
10
Peer reviewed journals only 44
Limit the journals to last ten
years only
42
Limit the journals to English
language only
40
Table: search criteria for evidence based articles
(Source: author)
AUTOMATED BLOOD PRESSURE DEVICE
sphygmomanometers on children in hospital?
Search topic Number of hits generated
Blood pressure monitoring
devices
52
Automated blood pressure
monitoring devices
65
Use of automated blood
pressure monitoring devices
in children
20
Benefits of manual
sphygmomanometers over
automated blood pressure
monitoring devices
10
Peer reviewed journals only 44
Limit the journals to last ten
years only
42
Limit the journals to English
language only
40
Table: search criteria for evidence based articles
(Source: author)
8
AUTOMATED BLOOD PRESSURE DEVICE
Summary of practice
The manual sphygmomanometers are the most accepted old school method of monitoring
and recording blood pressure. A loose end in the cuff of a blood pressure monitoring device may
result in the recording of wrong results (Sheppard et al., 2014). On the other hand the automated
blood pressure monitoring devices work with the help of electronic sensors and sense the systolic
and diastolic pressure automatically at the same controlling the deflation rate. However, the
automated devices require huge amount of investments making it difficult for maximum number
of hospitals to purchase them (Benmira et al., 2016). Therefore, most of the hospitals are still
using the manual methods of blood pressure recording. Thus, both the methods need a certain
amount of medical expertise which will help in focussing upon the general health condition of
the patient before arriving at a result. Additionally, maintaining standard cuff sizes will help in
measuring the blood pressure accurately across a wide age group (De Caen et al., 2015). The
devices should be calibrated frequently to provide accurate results along with controlling the
cost of the medical equipments and devices.
Conclusion
In this respect, a number of issues have been identified with both the manual and the
automated methods of blood pressure recording. However, the accuracy is dependent upon the
cuff sizes which are different depending upon the age and health of an individual. A healthy
individual may require a wider cuff whereas a lean child may need a thinner cuff. The
automated blood pressure monitoring devices though easier to use specially with the children
requires huge investments. Therefore, there are loopholes pertaining to the use of both the device
and requires suitable policies and intervention strategies.
AUTOMATED BLOOD PRESSURE DEVICE
Summary of practice
The manual sphygmomanometers are the most accepted old school method of monitoring
and recording blood pressure. A loose end in the cuff of a blood pressure monitoring device may
result in the recording of wrong results (Sheppard et al., 2014). On the other hand the automated
blood pressure monitoring devices work with the help of electronic sensors and sense the systolic
and diastolic pressure automatically at the same controlling the deflation rate. However, the
automated devices require huge amount of investments making it difficult for maximum number
of hospitals to purchase them (Benmira et al., 2016). Therefore, most of the hospitals are still
using the manual methods of blood pressure recording. Thus, both the methods need a certain
amount of medical expertise which will help in focussing upon the general health condition of
the patient before arriving at a result. Additionally, maintaining standard cuff sizes will help in
measuring the blood pressure accurately across a wide age group (De Caen et al., 2015). The
devices should be calibrated frequently to provide accurate results along with controlling the
cost of the medical equipments and devices.
Conclusion
In this respect, a number of issues have been identified with both the manual and the
automated methods of blood pressure recording. However, the accuracy is dependent upon the
cuff sizes which are different depending upon the age and health of an individual. A healthy
individual may require a wider cuff whereas a lean child may need a thinner cuff. The
automated blood pressure monitoring devices though easier to use specially with the children
requires huge investments. Therefore, there are loopholes pertaining to the use of both the device
and requires suitable policies and intervention strategies.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
AUTOMATED BLOOD PRESSURE DEVICE
References
Benmira, A., Perez-Martin, A., Schuster, I., Aichoun, I., Coudray, S., Bereksi-Reguig, F., &
Dauzat, M. (2016). From Korotkoff and Marey to automatic non-invasive oscillometric
blood pressure measurement: does easiness come with reliability?. Expert review of
medical devices, 13(2), 179-189.
Chu, G., Zhang, Z., Xu, M., Huang, D., & Dai, Q. (2017). Validation of a smartphone
auscultatory blood pressure kit Accutension XYZ-110 in adults according to the
ANSI/AAMI/ISO 81060-2: 2013 standard. Blood pressure monitoring, 22(5), 290-294.
Daskalopoulou, S. S., Rabi, D. M., Zarnke, K. B., Dasgupta, K., Nerenberg, K., Cloutier, L., ... &
McKay, D. W. (2015). The 2015 Canadian Hypertension Education Program
recommendations for blood pressure measurement, diagnosis, assessment of risk,
prevention, and treatment of hypertension. Canadian Journal of Cardiology, 31(5), 549-
568.
De Caen, A. R., Berg, M. D., Chameides, L., Gooden, C. K., Hickey, R. W., Scott, H. F., ... &
Schexnayder, S. M. (2015). Part 12: pediatric advanced life support. Circulation, 132(18
suppl 2), S526-S542.
Duncombe, S. L., Voss, C., & Harris, K. C. (2017). Oscillometric and auscultatory blood
pressure measurement methods in children: a systematic review and meta-
analysis. Journal of hypertension, 35(2), 213-224.
AUTOMATED BLOOD PRESSURE DEVICE
References
Benmira, A., Perez-Martin, A., Schuster, I., Aichoun, I., Coudray, S., Bereksi-Reguig, F., &
Dauzat, M. (2016). From Korotkoff and Marey to automatic non-invasive oscillometric
blood pressure measurement: does easiness come with reliability?. Expert review of
medical devices, 13(2), 179-189.
Chu, G., Zhang, Z., Xu, M., Huang, D., & Dai, Q. (2017). Validation of a smartphone
auscultatory blood pressure kit Accutension XYZ-110 in adults according to the
ANSI/AAMI/ISO 81060-2: 2013 standard. Blood pressure monitoring, 22(5), 290-294.
Daskalopoulou, S. S., Rabi, D. M., Zarnke, K. B., Dasgupta, K., Nerenberg, K., Cloutier, L., ... &
McKay, D. W. (2015). The 2015 Canadian Hypertension Education Program
recommendations for blood pressure measurement, diagnosis, assessment of risk,
prevention, and treatment of hypertension. Canadian Journal of Cardiology, 31(5), 549-
568.
De Caen, A. R., Berg, M. D., Chameides, L., Gooden, C. K., Hickey, R. W., Scott, H. F., ... &
Schexnayder, S. M. (2015). Part 12: pediatric advanced life support. Circulation, 132(18
suppl 2), S526-S542.
Duncombe, S. L., Voss, C., & Harris, K. C. (2017). Oscillometric and auscultatory blood
pressure measurement methods in children: a systematic review and meta-
analysis. Journal of hypertension, 35(2), 213-224.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10
AUTOMATED BLOOD PRESSURE DEVICE
Flynn, J. T., Kaelber, D. C., Baker-Smith, C. M., Blowey, D., Carroll, A. E., Daniels, S. R., ... &
Gidding, S. S. (2017). Clinical practice guideline for screening and management of high
blood pressure in children and adolescents. Pediatrics, p.1904.
Franssen, M., Farmer, A., Grant, S., Greenfield, S., Heneghan, C., Hobbs, R., ... & Milner, S.
(2017). Telemonitoring and/or self-monitoring of blood pressure in hypertension
(TASMINH4): protocol for a randomised controlled trial. BMC cardiovascular
disorders, 17(1), 58.
Lin, Z. M., Chang, C. H., Chou, N. K., & Lin, Y. H. (2014, April). Bluetooth Low Energy (BLE)
based blood pressure monitoring system. In Intelligent Green Building and Smart Grid
(IGBSG), 2014 International Conference on (pp. 1-4). IEEE.
Myers, M. G. (2014). Replacing manual sphygmomanometers with automated blood pressure
measurement in routine clinical practice. Clinical and Experimental Pharmacology and
Physiology, 41(1), 46-53.
Neuhauser, H. K., Ellert, U., Thamm, M., & Adler, C. (2015). Calibration of blood pressure data
after replacement of the standard mercury sphygmomanometer by an oscillometric device
and concurrent change of cuffs. Blood pressure monitoring, 20(1), 39-42.
Rinfret, F., Cloutier, L., L'Archevêque, H., Gauthier, M., Laskine, M., Larochelle, P., ... & Van
Nguyen, P. (2017). The gap between manual and automated office blood pressure
measurements results at a hypertension clinic. Canadian Journal of Cardiology, 33(5),
653-657.
AUTOMATED BLOOD PRESSURE DEVICE
Flynn, J. T., Kaelber, D. C., Baker-Smith, C. M., Blowey, D., Carroll, A. E., Daniels, S. R., ... &
Gidding, S. S. (2017). Clinical practice guideline for screening and management of high
blood pressure in children and adolescents. Pediatrics, p.1904.
Franssen, M., Farmer, A., Grant, S., Greenfield, S., Heneghan, C., Hobbs, R., ... & Milner, S.
(2017). Telemonitoring and/or self-monitoring of blood pressure in hypertension
(TASMINH4): protocol for a randomised controlled trial. BMC cardiovascular
disorders, 17(1), 58.
Lin, Z. M., Chang, C. H., Chou, N. K., & Lin, Y. H. (2014, April). Bluetooth Low Energy (BLE)
based blood pressure monitoring system. In Intelligent Green Building and Smart Grid
(IGBSG), 2014 International Conference on (pp. 1-4). IEEE.
Myers, M. G. (2014). Replacing manual sphygmomanometers with automated blood pressure
measurement in routine clinical practice. Clinical and Experimental Pharmacology and
Physiology, 41(1), 46-53.
Neuhauser, H. K., Ellert, U., Thamm, M., & Adler, C. (2015). Calibration of blood pressure data
after replacement of the standard mercury sphygmomanometer by an oscillometric device
and concurrent change of cuffs. Blood pressure monitoring, 20(1), 39-42.
Rinfret, F., Cloutier, L., L'Archevêque, H., Gauthier, M., Laskine, M., Larochelle, P., ... & Van
Nguyen, P. (2017). The gap between manual and automated office blood pressure
measurements results at a hypertension clinic. Canadian Journal of Cardiology, 33(5),
653-657.
11
AUTOMATED BLOOD PRESSURE DEVICE
Sheppard, J. P., Holder, R., Nichols, L., Bray, E., Hobbs, F. R., Mant, J., ... & McManus, R. J.
(2014). Predicting out-of-office blood pressure level using repeated measurements in the
clinic: an observational cohort study. Journal of hypertension, 32(11), 2171.
AUTOMATED BLOOD PRESSURE DEVICE
Sheppard, J. P., Holder, R., Nichols, L., Bray, E., Hobbs, F. R., Mant, J., ... & McManus, R. J.
(2014). Predicting out-of-office blood pressure level using repeated measurements in the
clinic: an observational cohort study. Journal of hypertension, 32(11), 2171.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.