Recent Advances and Challenges in Bacterial Meningitis Research
VerifiedAdded on 2020/06/03
|12
|3131
|40
AI Summary
Bacterial meningitis continues to be a critical area of medical research due to its high morbidity and mortality rates. This document synthesizes key studies from 2013-2016 that contribute valuable insights into the etiology, diagnosis, and treatment of this severe infection. Notably, recent efforts have focused on improving rapid diagnostic techniques through advanced technologies like MALDI-TOF mass spectrometry (Segawa et al., 2014) and electrochemical DNA biosensors based on ZnO nanostructures (Tak et al., 2014). These innovations promise quicker pathogen identification, potentially transforming clinical outcomes. Furthermore, treatment protocols have been refined with guidelines emphasizing the use of specific antibiotics tailored to pathogen profiles (Van de Beek et al., 2016; McGill et al., 2016). Epidemiological studies have illuminated trends in bacterial meningitis incidence and causative agents across different demographics and geographies (Okike et al., 2014; Castelblanco et al., 2014), which are crucial for developing targeted public health interventions. Additionally, the exploration of induced hypothermia as a therapeutic intervention has shown potential benefits in reducing inflammation in bacterial meningitis patients (Mourvillier et al., 2013). Collectively, these research efforts underscore the importance of interdisciplinary approaches to tackle this complex disease, suggesting future directions that include enhanced molecular diagnostics and personalized medicine strategies. As new challenges emerge, ongoing research will be pivotal in adapting to changing epidemiological landscapes and improving patient care.
Bacterial Meningitis
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
INTRODUCTION...........................................................................................................................1
Risk factors and causes....................................................................................................................1
Aetiology of Bacterial Meningitis...................................................................................................1
Types and causative organisms.......................................................................................................2
Pathophysiology..............................................................................................................................3
Clinical presentation........................................................................................................................4
Diagnostic tests................................................................................................................................5
Acute treatment based upon Australian guidelines.........................................................................5
Public health considerations............................................................................................................6
CONCLUSION................................................................................................................................6
REFERENCES................................................................................................................................7
INTRODUCTION...........................................................................................................................1
Risk factors and causes....................................................................................................................1
Aetiology of Bacterial Meningitis...................................................................................................1
Types and causative organisms.......................................................................................................2
Pathophysiology..............................................................................................................................3
Clinical presentation........................................................................................................................4
Diagnostic tests................................................................................................................................5
Acute treatment based upon Australian guidelines.........................................................................5
Public health considerations............................................................................................................6
CONCLUSION................................................................................................................................6
REFERENCES................................................................................................................................7

Table of Figures
Figure 1Pathophysiology of bacterial meningitis............................................................................4
Figure 2 CSF Parameters for diagnosis (Source: Meningitis – encephalitis, 2018)........................5
Figure 1Pathophysiology of bacterial meningitis............................................................................4
Figure 2 CSF Parameters for diagnosis (Source: Meningitis – encephalitis, 2018)........................5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
INTRODUCTION
Bacterial meningitis is that state where an individual suffers from brain and spinal cord
inflammation. The report makes comprehensive discussion regarding pathophysiology, aetiology
and causative organism. It will also make discussion regarding clinical presentation and
diagnostic tests performed by health care professionals to diagnose the disease.
Risk factors and causes
Bacterial meningitis is a serious medical condition which can prove to be deadly for
individuals suffering from it. It is the situation of inflammation of brain and spinal cord
membranes, which is typically caused by any infection, which can be in the form of bacteria,
virus or by any other microorganism. It is rare but serious infection, in which viral meningitis is
treatable, where recovery is quite swift (Mourvillier and et.al., 2013). However, bacterial
meningitis is treated as a medical emergency, which can prove to be fatal if prompt treatment is
not given to the patient.
Meningitis is usually caused by infection. It is communicable and hence can be transferred
fr4om one individual to the other in the form of coughing, sneezing or kissing. It can also spread
if an individual has touched contaminated personal items and surface of others, who are already
suffering from it. Bacterial meningitis can take place at any age, but the main suspects of it are
infants. There are other factors that can increase the risk of this disease are:
Any anatomical trauma in the form of skull fracture or any kind of surgery which has
allowed or given the space to bacteria to enter into nervous system.
Infection in the area of neck and head area.
Spending time with various communities or large group of people in the form of school,
social gatherings, etc (Castelblanco, Lee and Hasbun, 2014).
Travelling or living at some specific location, such as, Sub Saharan region.
Having a weak immune system due to any chronic medical condition or treatment.
Working in some medical laboratories where meningitis pathogens are already present. It
duly increases its prevalence in the individual. Hence, microbiologists have clear exposure to
it (Castelblanco, Lee and Hasbun, 2014).
Aetiology of Bacterial Meningitis
Meningitis is usually called as an infection and hence can take place due to attack of
viruses and bacteria. However, bacterial meningitis in considered to be more dreadful condition
1
Bacterial meningitis is that state where an individual suffers from brain and spinal cord
inflammation. The report makes comprehensive discussion regarding pathophysiology, aetiology
and causative organism. It will also make discussion regarding clinical presentation and
diagnostic tests performed by health care professionals to diagnose the disease.
Risk factors and causes
Bacterial meningitis is a serious medical condition which can prove to be deadly for
individuals suffering from it. It is the situation of inflammation of brain and spinal cord
membranes, which is typically caused by any infection, which can be in the form of bacteria,
virus or by any other microorganism. It is rare but serious infection, in which viral meningitis is
treatable, where recovery is quite swift (Mourvillier and et.al., 2013). However, bacterial
meningitis is treated as a medical emergency, which can prove to be fatal if prompt treatment is
not given to the patient.
Meningitis is usually caused by infection. It is communicable and hence can be transferred
fr4om one individual to the other in the form of coughing, sneezing or kissing. It can also spread
if an individual has touched contaminated personal items and surface of others, who are already
suffering from it. Bacterial meningitis can take place at any age, but the main suspects of it are
infants. There are other factors that can increase the risk of this disease are:
Any anatomical trauma in the form of skull fracture or any kind of surgery which has
allowed or given the space to bacteria to enter into nervous system.
Infection in the area of neck and head area.
Spending time with various communities or large group of people in the form of school,
social gatherings, etc (Castelblanco, Lee and Hasbun, 2014).
Travelling or living at some specific location, such as, Sub Saharan region.
Having a weak immune system due to any chronic medical condition or treatment.
Working in some medical laboratories where meningitis pathogens are already present. It
duly increases its prevalence in the individual. Hence, microbiologists have clear exposure to
it (Castelblanco, Lee and Hasbun, 2014).
Aetiology of Bacterial Meningitis
Meningitis is usually called as an infection and hence can take place due to attack of
viruses and bacteria. However, bacterial meningitis in considered to be more dreadful condition
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
in comparison to the of viral one. Since, it is communicable disease, its spread is quite common
at over crowded locations and smoky areas. Bacterial meningitis is generally caused by certain
bacteria’s, such as, Meningococcus or Pneumococcus (Okike and et.al, 2014). These types of
bacteria generally live in nose and throat and are usually harmless to the body. But if they enter
to individual’s blood stream and surrounding the membranes of brain, then it can become the
leading cause of meningitis (Bijlsma and et.al., 2016).
The early diagnosis and then treatment is vital, as bacterial meningitis is a medical
emergency that could lead the patient to death in just a few hours. The common symptoms
related to this disease are, fever, nausea, vomiting, disorientation and confusion, irritability,
agitation, drowsiness and tiredness, lack of energy in the body, dizziness and sore throat (McGill
and et.al., 2016).
The microorganisms responsible for bacterial meningitis may vary by the age group.
Infants can get infected with this disease through their mother, where they can pass group
B Streptococcus and Escherichia coli to the babies during labor and at the time of birth (Segawa
and et.al., 2014). Eating food prepared by the individual who did not wash hands after toilet is
another major cause of this disease. Contaminated food and water are the other leading cause of
bacterial meningitis.
Types and causative organisms
Bacteria can easily travel from body to blood stream and then reach to spinal cord and
brain causing acute meningitis to the patient. But it occurrence is also common in case when
bacterias directly invade meninges. It can be caused due to group B Streptococcus and
Escherichia coli as sinus or ear infection, skull fractures and surgeries (Van de Beek and et.al.,
2016). There are various types of bacteria that can result in meningitis. Leading causes of this
disease and type of bacteria involved in it are,
Streptococcus pneumoniae: It is considered to be one of the most common cause of bacterial
meningitis in infants, youngsters and adults. It commonly causes pneumonia, ear and sinus
infection which ultimately leads to meningitis if not controlled in specific time period (Okike
and et.al., 2014).
Neisseria meningitidis: It is another leading cause of meningitis. It generally causes upper
respiratory infection but it can cause meningitis if it enters into the blood stream. It is
2
at over crowded locations and smoky areas. Bacterial meningitis is generally caused by certain
bacteria’s, such as, Meningococcus or Pneumococcus (Okike and et.al, 2014). These types of
bacteria generally live in nose and throat and are usually harmless to the body. But if they enter
to individual’s blood stream and surrounding the membranes of brain, then it can become the
leading cause of meningitis (Bijlsma and et.al., 2016).
The early diagnosis and then treatment is vital, as bacterial meningitis is a medical
emergency that could lead the patient to death in just a few hours. The common symptoms
related to this disease are, fever, nausea, vomiting, disorientation and confusion, irritability,
agitation, drowsiness and tiredness, lack of energy in the body, dizziness and sore throat (McGill
and et.al., 2016).
The microorganisms responsible for bacterial meningitis may vary by the age group.
Infants can get infected with this disease through their mother, where they can pass group
B Streptococcus and Escherichia coli to the babies during labor and at the time of birth (Segawa
and et.al., 2014). Eating food prepared by the individual who did not wash hands after toilet is
another major cause of this disease. Contaminated food and water are the other leading cause of
bacterial meningitis.
Types and causative organisms
Bacteria can easily travel from body to blood stream and then reach to spinal cord and
brain causing acute meningitis to the patient. But it occurrence is also common in case when
bacterias directly invade meninges. It can be caused due to group B Streptococcus and
Escherichia coli as sinus or ear infection, skull fractures and surgeries (Van de Beek and et.al.,
2016). There are various types of bacteria that can result in meningitis. Leading causes of this
disease and type of bacteria involved in it are,
Streptococcus pneumoniae: It is considered to be one of the most common cause of bacterial
meningitis in infants, youngsters and adults. It commonly causes pneumonia, ear and sinus
infection which ultimately leads to meningitis if not controlled in specific time period (Okike
and et.al., 2014).
Neisseria meningitidis: It is another leading cause of meningitis. It generally causes upper
respiratory infection but it can cause meningitis if it enters into the blood stream. It is
2
generally found in teenagers and young adults. It can also cause local epidemics in college
dormitories, boarding schools and other military bases (Okike and et.al., 2014).
Haemophilus influenzae: It is common cause of meningitis in children. However, its
immunization and vaccination has reduced its occurrence to minimum. Listeria monocytogenes: These types of bacteria are generally found in unpasteurized
cheeses, luncheon meats and hot dogs. People with weak immune system, such as, pregnant
women, infants and older adults are more susceptible to it. It can cross barrier of placenta and
cause infection in late pregnancy among pregnant ladies and in the new born also
(Tak, Gupta and Tomar, 2014).
Other common bacteria that are leading cause of bacterial meningitis are, Group
B Streptococcus, Meningococcus bacteria and Pneumococcus bacteria. The attack of
microorganism may vary by age groups and immune system of the body (Okike and et.al., 2014).
Pathophysiology
Bacterial meningitis has one of the most common symptom, that is fever. The body
temperature above 38 degrees is a matter of risk for the patient. The pathophysiology works here
is endogenous cytokines affecting thermoregulatory neurons of hypothalamus which are
responsible for bringing change in temperature. Neck stiffness is another major symptom whose
mechanism is related to traction and inflamed meninges are commonly painful which results in
limited motion of the neck through the spine, that is, restricted cervical spine movement. Altered
mental scale in the patient can be judged through decreased Glasgow Coma Scale (GCS)
(Castelblanco, Lee and Hasbun, 2014). Intracranial pressure leads to brain herniation which
ultimately results in damage in the structure of blood stream governing consciousness, that is
reticular formation.
Another leading symptom of bacterial meningitis is seizures whose mechanism works
based upon inflammation in membrane permeability. However, the exact pathophysiology of
bacterial meningitis is unknown (Tak, Gupta and Tomar, 2014).
3
dormitories, boarding schools and other military bases (Okike and et.al., 2014).
Haemophilus influenzae: It is common cause of meningitis in children. However, its
immunization and vaccination has reduced its occurrence to minimum. Listeria monocytogenes: These types of bacteria are generally found in unpasteurized
cheeses, luncheon meats and hot dogs. People with weak immune system, such as, pregnant
women, infants and older adults are more susceptible to it. It can cross barrier of placenta and
cause infection in late pregnancy among pregnant ladies and in the new born also
(Tak, Gupta and Tomar, 2014).
Other common bacteria that are leading cause of bacterial meningitis are, Group
B Streptococcus, Meningococcus bacteria and Pneumococcus bacteria. The attack of
microorganism may vary by age groups and immune system of the body (Okike and et.al., 2014).
Pathophysiology
Bacterial meningitis has one of the most common symptom, that is fever. The body
temperature above 38 degrees is a matter of risk for the patient. The pathophysiology works here
is endogenous cytokines affecting thermoregulatory neurons of hypothalamus which are
responsible for bringing change in temperature. Neck stiffness is another major symptom whose
mechanism is related to traction and inflamed meninges are commonly painful which results in
limited motion of the neck through the spine, that is, restricted cervical spine movement. Altered
mental scale in the patient can be judged through decreased Glasgow Coma Scale (GCS)
(Castelblanco, Lee and Hasbun, 2014). Intracranial pressure leads to brain herniation which
ultimately results in damage in the structure of blood stream governing consciousness, that is
reticular formation.
Another leading symptom of bacterial meningitis is seizures whose mechanism works
based upon inflammation in membrane permeability. However, the exact pathophysiology of
bacterial meningitis is unknown (Tak, Gupta and Tomar, 2014).
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
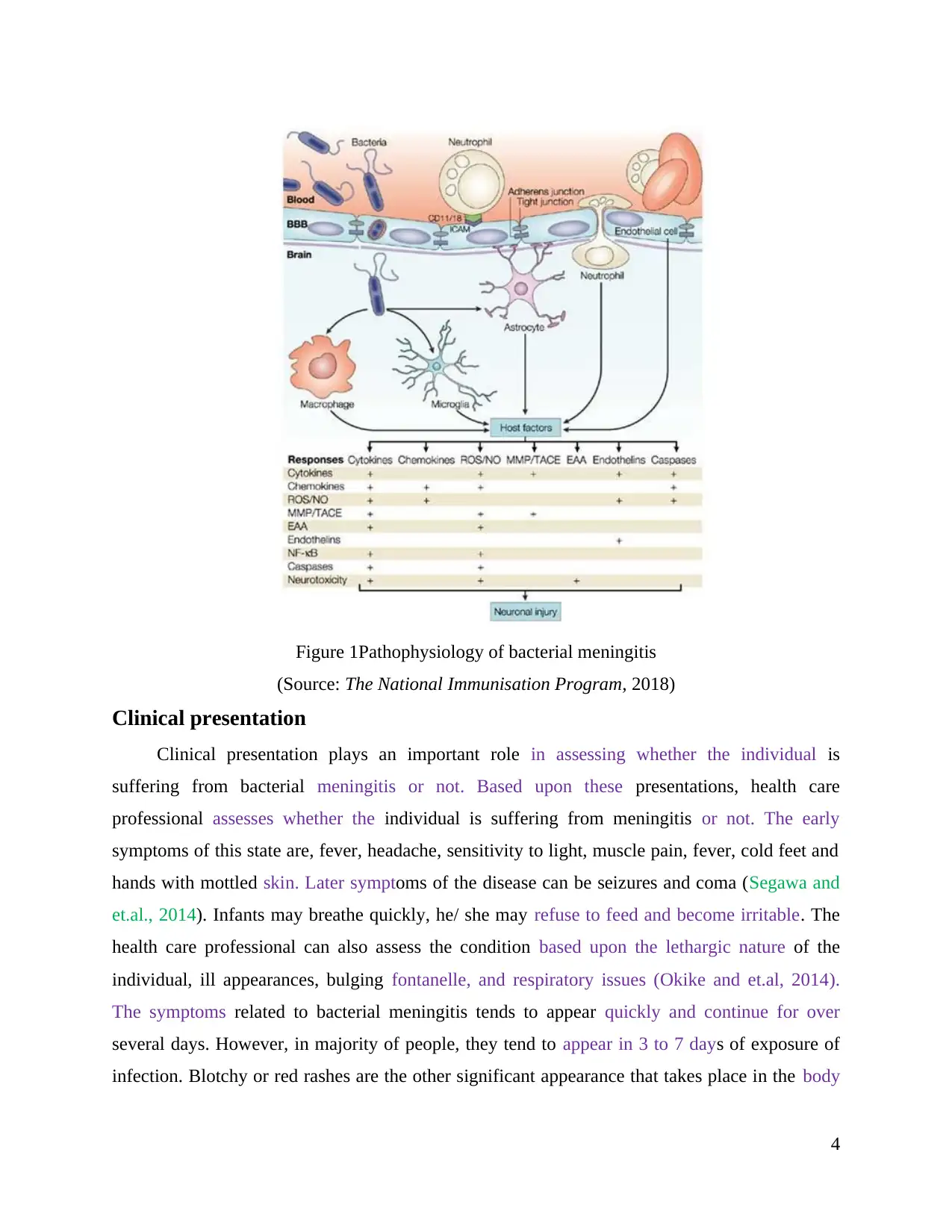
Figure 1Pathophysiology of bacterial meningitis
(Source: The National Immunisation Program, 2018)
Clinical presentation
Clinical presentation plays an important role in assessing whether the individual is
suffering from bacterial meningitis or not. Based upon these presentations, health care
professional assesses whether the individual is suffering from meningitis or not. The early
symptoms of this state are, fever, headache, sensitivity to light, muscle pain, fever, cold feet and
hands with mottled skin. Later symptoms of the disease can be seizures and coma (Segawa and
et.al., 2014). Infants may breathe quickly, he/ she may refuse to feed and become irritable. The
health care professional can also assess the condition based upon the lethargic nature of the
individual, ill appearances, bulging fontanelle, and respiratory issues (Okike and et.al, 2014).
The symptoms related to bacterial meningitis tends to appear quickly and continue for over
several days. However, in majority of people, they tend to appear in 3 to 7 days of exposure of
infection. Blotchy or red rashes are the other significant appearance that takes place in the body
4
(Source: The National Immunisation Program, 2018)
Clinical presentation
Clinical presentation plays an important role in assessing whether the individual is
suffering from bacterial meningitis or not. Based upon these presentations, health care
professional assesses whether the individual is suffering from meningitis or not. The early
symptoms of this state are, fever, headache, sensitivity to light, muscle pain, fever, cold feet and
hands with mottled skin. Later symptoms of the disease can be seizures and coma (Segawa and
et.al., 2014). Infants may breathe quickly, he/ she may refuse to feed and become irritable. The
health care professional can also assess the condition based upon the lethargic nature of the
individual, ill appearances, bulging fontanelle, and respiratory issues (Okike and et.al, 2014).
The symptoms related to bacterial meningitis tends to appear quickly and continue for over
several days. However, in majority of people, they tend to appear in 3 to 7 days of exposure of
infection. Blotchy or red rashes are the other significant appearance that takes place in the body
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
which can be used to assess that the individual is suffering from bacterial meningitis (Prasad and
et.al., 2014).
Diagnostic tests
For accurate diagnosis through physical examination it is important that the individual
discusses accurate clinical features he / she must have been facing. The diagnosis can be
confirmed through laboratory findings, where patient has to go through lumbar puncture in order
to evaluate the condition of Spinal fluid. Another CSF laboratory test is an analysis of 4 sterile
tubes with approximately 1 ml of CSF each. The first tube is generally reserved for gram stain
and culture test. The cultured happens to be positive for 80% of the meningitis patients (Okike
and et.al., 2014). The second tube is sent for glucose and protein level because Patients having
elevated CSF protein count and low glucose level generally represents that they are suffering
from bacterial meningitis. The third tube is sent to laboratory for cell count and differentials.
Patients suffering from meningitis have inflated White Blood Count. The fourth tube is used for
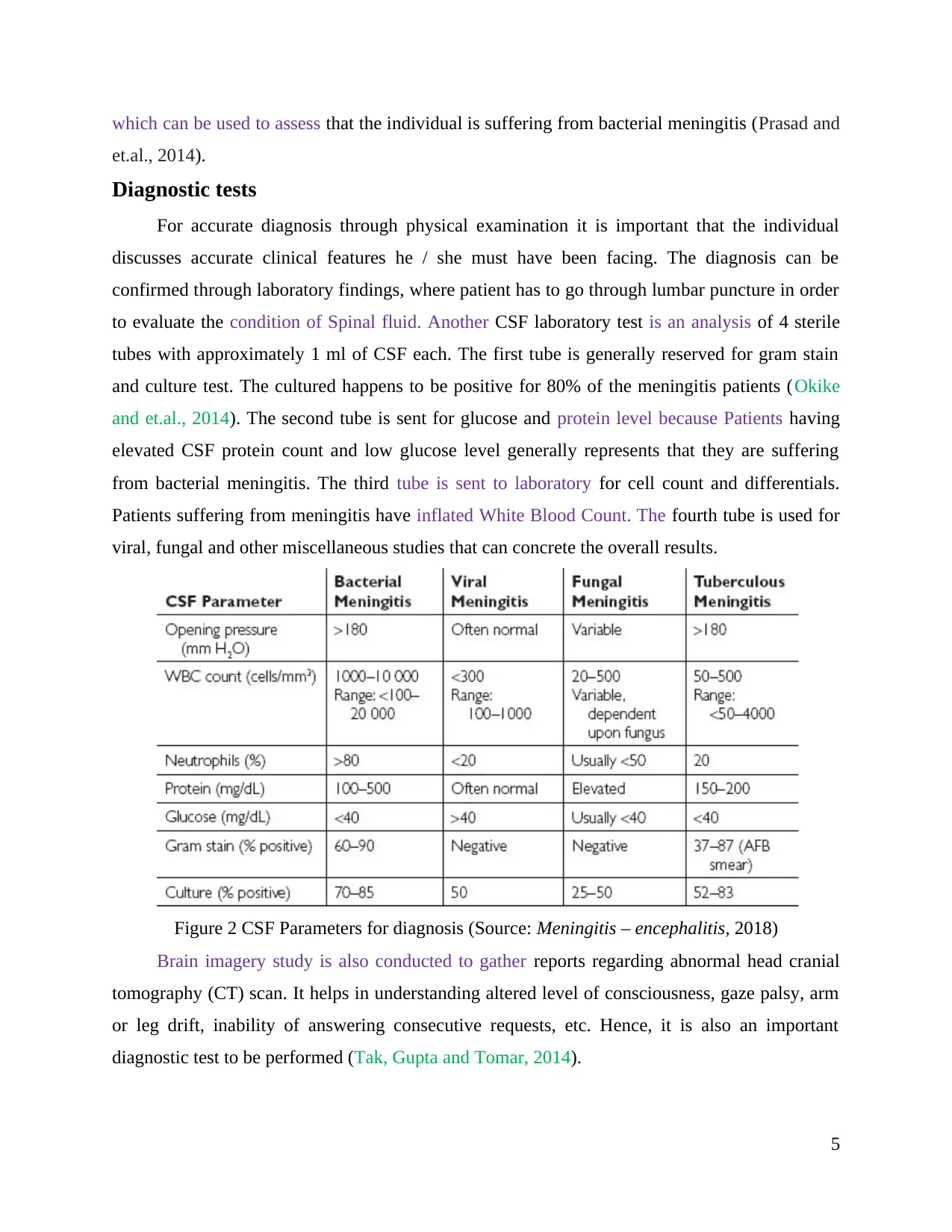
viral, fungal and other miscellaneous studies that can concrete the overall results.
Figure 2 CSF Parameters for diagnosis (Source: Meningitis – encephalitis, 2018)
Brain imagery study is also conducted to gather reports regarding abnormal head cranial
tomography (CT) scan. It helps in understanding altered level of consciousness, gaze palsy, arm
or leg drift, inability of answering consecutive requests, etc. Hence, it is also an important
diagnostic test to be performed (Tak, Gupta and Tomar, 2014).
5
et.al., 2014).
Diagnostic tests
For accurate diagnosis through physical examination it is important that the individual
discusses accurate clinical features he / she must have been facing. The diagnosis can be
confirmed through laboratory findings, where patient has to go through lumbar puncture in order
to evaluate the condition of Spinal fluid. Another CSF laboratory test is an analysis of 4 sterile
tubes with approximately 1 ml of CSF each. The first tube is generally reserved for gram stain
and culture test. The cultured happens to be positive for 80% of the meningitis patients (Okike
and et.al., 2014). The second tube is sent for glucose and protein level because Patients having
elevated CSF protein count and low glucose level generally represents that they are suffering
from bacterial meningitis. The third tube is sent to laboratory for cell count and differentials.
Patients suffering from meningitis have inflated White Blood Count. The fourth tube is used for
viral, fungal and other miscellaneous studies that can concrete the overall results.
Figure 2 CSF Parameters for diagnosis (Source: Meningitis – encephalitis, 2018)
Brain imagery study is also conducted to gather reports regarding abnormal head cranial
tomography (CT) scan. It helps in understanding altered level of consciousness, gaze palsy, arm
or leg drift, inability of answering consecutive requests, etc. Hence, it is also an important
diagnostic test to be performed (Tak, Gupta and Tomar, 2014).
5

Acute treatment based upon Australian guidelines
Based upon the features of the examinations and history, acute treatment can be given to the
individual suffering from bacterial meningitis. The treatment starts with antibiotics in order to
promptly manage the condition of patient. It must not be delayed for more than 30 minutes
(Okike and et.al, 2014). If the patient is of more than 2 months, then steroids are also given to
him / her for better results. It helps in the reduction of the risk of hearing loss. Further, steps are
taken for seizure and fluid management. Carefully managing fluids and electrolytes in the body
is an important aspect of meningitis (Tak, Gupta and Tomar, 2014). As a part of treatment, health
care professional also has to monitor certain aspects of body in adequate intervals. Neurological
management in the form of blood pressure which is to be assessed in every 15 minutes, weight
and head circumference which is required to be measured every day and level of electrolyte and
glucose is to be checked in every 6 to 12 hours. Treatment also includes ensuring adequate
analgesia (Farrar and et.al., 2013).
Meningitis is considered to be a medical emergency which can develop quickly in the matter
of few hours. Treatment can not be delayed for more than 1 – 2 hours. Pharmalogical treatment
includes, injectable antibiotics and replacement of fluids. Careful fluid management is required
to be undertaken with electrolyte balance. In such cases, intravenous fluids, in the form of
normal saline (0.9% sodium chloride solution) with additional glucose. It must be given 3 ml / kg
/ hour. However, in case of excessive dehydration the dose can be increased.
The type of antibiotic given to the patient have high dependence on what type of bacteria is
causing meningitis in the body. Commonly used treatment for meningitis may include a class of
antibiotics in the form of cephalosporins specially Claforan (cefotaxime)
and Rocephin (ceftriaxone). Various penicillin-type antibiotics, aminoglycoside drugs such
as gentamicin, and others, can also be used for the patients.
Public health considerations
There are various guidelines that have been given by the government of Australia so as to
reduce the occurrence of bacterial meningitis among the population. The department of health
has collaborated with states and territories so as to closely monitor the incidences of bacterial
meningitis (McGill and et.al., 2016). The chief of the team has hired a specific set of people who
can analyse its epidemiology in various cities and territories. The responses are then analysed
and coordinated with statistics of national level. The government of Australia have also come up
6
Based upon the features of the examinations and history, acute treatment can be given to the
individual suffering from bacterial meningitis. The treatment starts with antibiotics in order to
promptly manage the condition of patient. It must not be delayed for more than 30 minutes
(Okike and et.al, 2014). If the patient is of more than 2 months, then steroids are also given to
him / her for better results. It helps in the reduction of the risk of hearing loss. Further, steps are
taken for seizure and fluid management. Carefully managing fluids and electrolytes in the body
is an important aspect of meningitis (Tak, Gupta and Tomar, 2014). As a part of treatment, health
care professional also has to monitor certain aspects of body in adequate intervals. Neurological
management in the form of blood pressure which is to be assessed in every 15 minutes, weight
and head circumference which is required to be measured every day and level of electrolyte and
glucose is to be checked in every 6 to 12 hours. Treatment also includes ensuring adequate
analgesia (Farrar and et.al., 2013).
Meningitis is considered to be a medical emergency which can develop quickly in the matter
of few hours. Treatment can not be delayed for more than 1 – 2 hours. Pharmalogical treatment
includes, injectable antibiotics and replacement of fluids. Careful fluid management is required
to be undertaken with electrolyte balance. In such cases, intravenous fluids, in the form of
normal saline (0.9% sodium chloride solution) with additional glucose. It must be given 3 ml / kg
/ hour. However, in case of excessive dehydration the dose can be increased.
The type of antibiotic given to the patient have high dependence on what type of bacteria is
causing meningitis in the body. Commonly used treatment for meningitis may include a class of
antibiotics in the form of cephalosporins specially Claforan (cefotaxime)
and Rocephin (ceftriaxone). Various penicillin-type antibiotics, aminoglycoside drugs such
as gentamicin, and others, can also be used for the patients.
Public health considerations
There are various guidelines that have been given by the government of Australia so as to
reduce the occurrence of bacterial meningitis among the population. The department of health
has collaborated with states and territories so as to closely monitor the incidences of bacterial
meningitis (McGill and et.al., 2016). The chief of the team has hired a specific set of people who
can analyse its epidemiology in various cities and territories. The responses are then analysed
and coordinated with statistics of national level. The government of Australia have also come up
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

with National Immunization programme that can help in increasing the overall immunization
rates by funding for free vaccination to people who can not afford it (Sykes, 2013). The same is
communicated by health care professionals to general public so that occurrence of meningitis can
be reduced to the minimum.
CONCLUSION
In the end, it can be stated that, bacterial meningitis can be a deadly disease if not handled
correctly at the initial stage. Doctors opt for better physical and laboratory diagnosis so that
treatment can be started as soon as patient present. The report also stated that Australia has come
up with a vaccination programme so that immunize the of people can be strengthened and
occurrence of meningitis can be reduced to minimum.
7
rates by funding for free vaccination to people who can not afford it (Sykes, 2013). The same is
communicated by health care professionals to general public so that occurrence of meningitis can
be reduced to the minimum.
CONCLUSION
In the end, it can be stated that, bacterial meningitis can be a deadly disease if not handled
correctly at the initial stage. Doctors opt for better physical and laboratory diagnosis so that
treatment can be started as soon as patient present. The report also stated that Australia has come
up with a vaccination programme so that immunize the of people can be strengthened and
occurrence of meningitis can be reduced to minimum.
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REFERENCES
Books and Journals
Bijlsma, M.W., Brouwer, M.C., Kasanmoentalib, E.S., Kloek, A.T., Lucas, M.J., Tanck, M.W.,
van der Ende, A. & van de Beek, D., (2016). Community-acquired bacterial meningitis in
adults in the Netherlands, 2006–14: a prospective cohort study. The Lancet Infectious
Diseases, 16(3), pp.339-347.Castelblanco, R. L., Lee, M., & Hasbun, R. (2014).
Epidemiology of bacterial meningitis in the USA from 1997 to 2010: a population-based
observational study. The Lancet Infectious Diseases, 14(9), 813-819.
Farrar, J., Hotez, P.J., Junghanss, T., Kang, G., Lalloo, D. & White, N.J., (2013). Manson's
Tropical Diseases E-Book. Elsevier Health Sciences. Mourvillier, B. & et.al. (2013).
Induced hypothermia in severe bacterial meningitis: a randomized clinical
trial. Jama, 310(20), 2174-2183.
Okike, I. O., Johnson, A. P., Henderson, K. L., Blackburn, R. M., Muller-Pebody, B., Ladhani, S.
N., ... & Heath, P. T. (2014). Incidence, etiology, and outcome of bacterial meningitis in
infants aged< 90 days in the United Kingdom and Republic of Ireland: prospective,
enhanced, national population-based surveillance. Clinical Infectious Diseases, 59(10),
e150-e157.
Okike, I. O., Ribeiro, S., Ramsay, M. E., Heath, P. T., Sharland, M., & Ladhani, S. N. (2014).
Trends in bacterial, mycobacterial, and fungal meningitis in England and Wales 2004–11:
an observational study. The Lancet infectious diseases, 14(4), 301-307.
Prasad, R., Kapoor, R., Srivastava, R., Mishra, O. P., & Singh, T. B. (2014). Cerebrospinal fluid
TNF-α, IL-6, and IL-8 in children with bacterial meningitis. Pediatric neurology, 50(1),
60-65.
Sykes, J. E. (2013). Canine and Feline Infectious Diseases-E-BOOK. Elsevier Health Sciences.
Tak, M., Gupta, V., & Tomar, M. (2014). Flower-like ZnO nanostructure based electrochemical
DNA biosensor for bacterial meningitis detection. Biosensors and Bioelectronics, 59,
200-207.
Van de Beek, D., Cabellos, C., Dzupova, O., Esposito, S., Klein, M., Kloek, A. T., ... & Pfister,
H. W. (2016). ESCMID guideline: diagnosis and treatment of acute bacterial
meningitis. Clinical microbiology and infection, 22, S37-S62.
8
Books and Journals
Bijlsma, M.W., Brouwer, M.C., Kasanmoentalib, E.S., Kloek, A.T., Lucas, M.J., Tanck, M.W.,
van der Ende, A. & van de Beek, D., (2016). Community-acquired bacterial meningitis in
adults in the Netherlands, 2006–14: a prospective cohort study. The Lancet Infectious
Diseases, 16(3), pp.339-347.Castelblanco, R. L., Lee, M., & Hasbun, R. (2014).
Epidemiology of bacterial meningitis in the USA from 1997 to 2010: a population-based
observational study. The Lancet Infectious Diseases, 14(9), 813-819.
Farrar, J., Hotez, P.J., Junghanss, T., Kang, G., Lalloo, D. & White, N.J., (2013). Manson's
Tropical Diseases E-Book. Elsevier Health Sciences. Mourvillier, B. & et.al. (2013).
Induced hypothermia in severe bacterial meningitis: a randomized clinical
trial. Jama, 310(20), 2174-2183.
Okike, I. O., Johnson, A. P., Henderson, K. L., Blackburn, R. M., Muller-Pebody, B., Ladhani, S.
N., ... & Heath, P. T. (2014). Incidence, etiology, and outcome of bacterial meningitis in
infants aged< 90 days in the United Kingdom and Republic of Ireland: prospective,
enhanced, national population-based surveillance. Clinical Infectious Diseases, 59(10),
e150-e157.
Okike, I. O., Ribeiro, S., Ramsay, M. E., Heath, P. T., Sharland, M., & Ladhani, S. N. (2014).
Trends in bacterial, mycobacterial, and fungal meningitis in England and Wales 2004–11:
an observational study. The Lancet infectious diseases, 14(4), 301-307.
Prasad, R., Kapoor, R., Srivastava, R., Mishra, O. P., & Singh, T. B. (2014). Cerebrospinal fluid
TNF-α, IL-6, and IL-8 in children with bacterial meningitis. Pediatric neurology, 50(1),
60-65.
Sykes, J. E. (2013). Canine and Feline Infectious Diseases-E-BOOK. Elsevier Health Sciences.
Tak, M., Gupta, V., & Tomar, M. (2014). Flower-like ZnO nanostructure based electrochemical
DNA biosensor for bacterial meningitis detection. Biosensors and Bioelectronics, 59,
200-207.
Van de Beek, D., Cabellos, C., Dzupova, O., Esposito, S., Klein, M., Kloek, A. T., ... & Pfister,
H. W. (2016). ESCMID guideline: diagnosis and treatment of acute bacterial
meningitis. Clinical microbiology and infection, 22, S37-S62.
8

McGill, F., Heyderman, R. S., Panagiotou, S., Tunkel, A. R., & Solomon, T. (2016). Acute
bacterial meningitis in adults. The Lancet, 388(10063), 3036-3047.
Castelblanco, R. L., Lee, M., & Hasbun, R. (2014). Epidemiology of bacterial meningitis in the
USA from 1997 to 2010: a population-based observational study. The Lancet Infectious
Diseases, 14(9), 813-819.
Segawa, S., Sawai, S., Murata, S., Nishimura, M., Beppu, M., Sogawa, K., ... & Iwadate, Y.
(2014). Direct application of MALDI-TOF mass spectrometry to cerebrospinal fluid for
rapid pathogen identification in a patient with bacterial meningitis. Clinica Chimica
Acta, 435, 59-61.
Tak, M., Gupta, V., & Tomar, M. (2014). Flower-like ZnO nanostructure based electrochemical
DNA biosensor for bacterial meningitis detection. Biosensors and Bioelectronics, 59,
200-207.
Online
Meningitis – encephalitis. (2018). [Online]. Available through <
https://www.rch.org.au/clinicalguide/guideline_index/Meningitis_Guideline/>
The National Immunisation Program. (2018). [Online]. Available through <
http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/content/home>
9
bacterial meningitis in adults. The Lancet, 388(10063), 3036-3047.
Castelblanco, R. L., Lee, M., & Hasbun, R. (2014). Epidemiology of bacterial meningitis in the
USA from 1997 to 2010: a population-based observational study. The Lancet Infectious
Diseases, 14(9), 813-819.
Segawa, S., Sawai, S., Murata, S., Nishimura, M., Beppu, M., Sogawa, K., ... & Iwadate, Y.
(2014). Direct application of MALDI-TOF mass spectrometry to cerebrospinal fluid for
rapid pathogen identification in a patient with bacterial meningitis. Clinica Chimica
Acta, 435, 59-61.
Tak, M., Gupta, V., & Tomar, M. (2014). Flower-like ZnO nanostructure based electrochemical
DNA biosensor for bacterial meningitis detection. Biosensors and Bioelectronics, 59,
200-207.
Online
Meningitis – encephalitis. (2018). [Online]. Available through <
https://www.rch.org.au/clinicalguide/guideline_index/Meningitis_Guideline/>
The National Immunisation Program. (2018). [Online]. Available through <
http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/content/home>
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.