Bacterial Meningitis: Clinical Manifestations, Diagnosis and Treatment
VerifiedAdded on 2021/05/31
|3
|1845
|435
Report
AI Summary
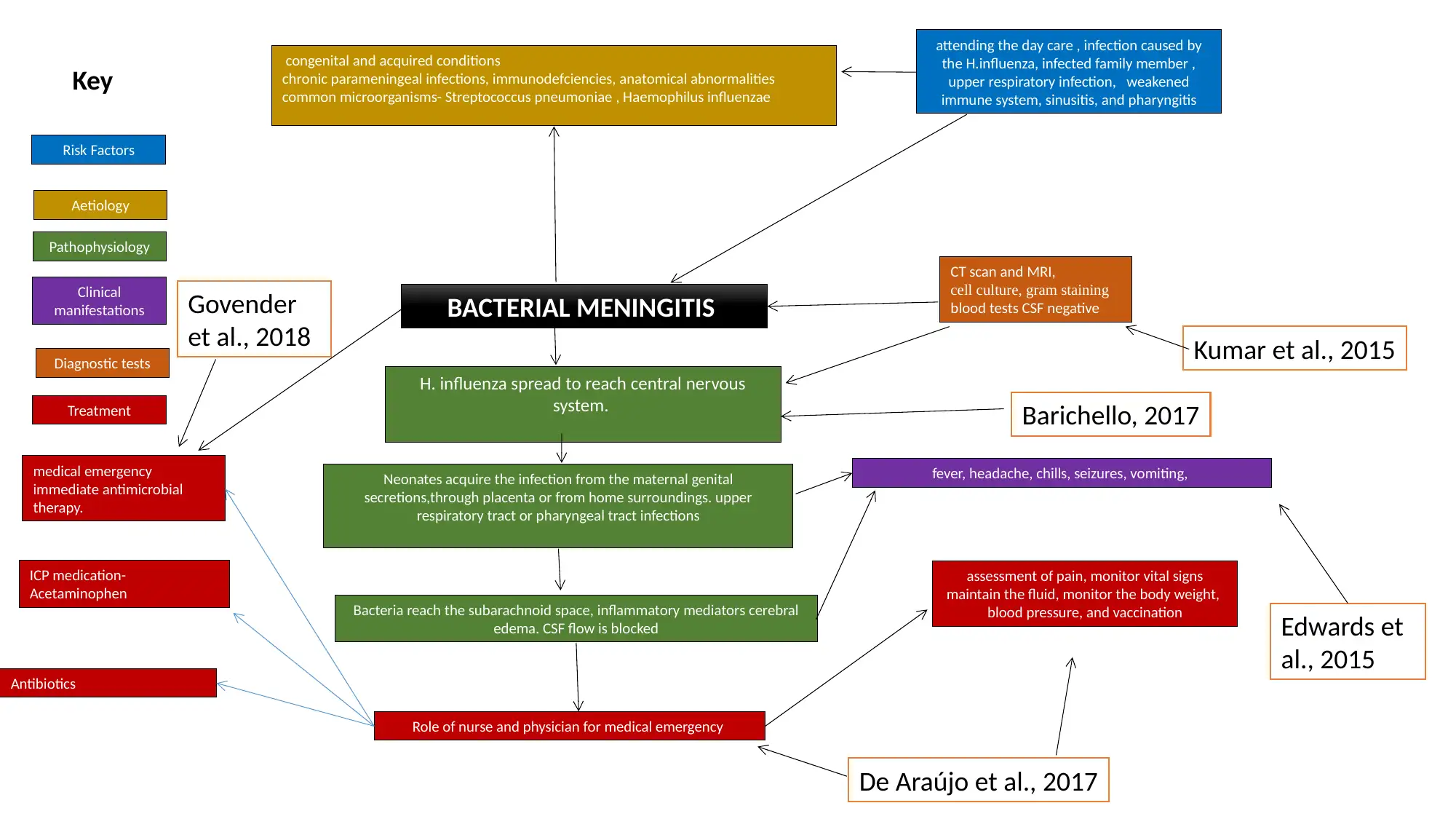
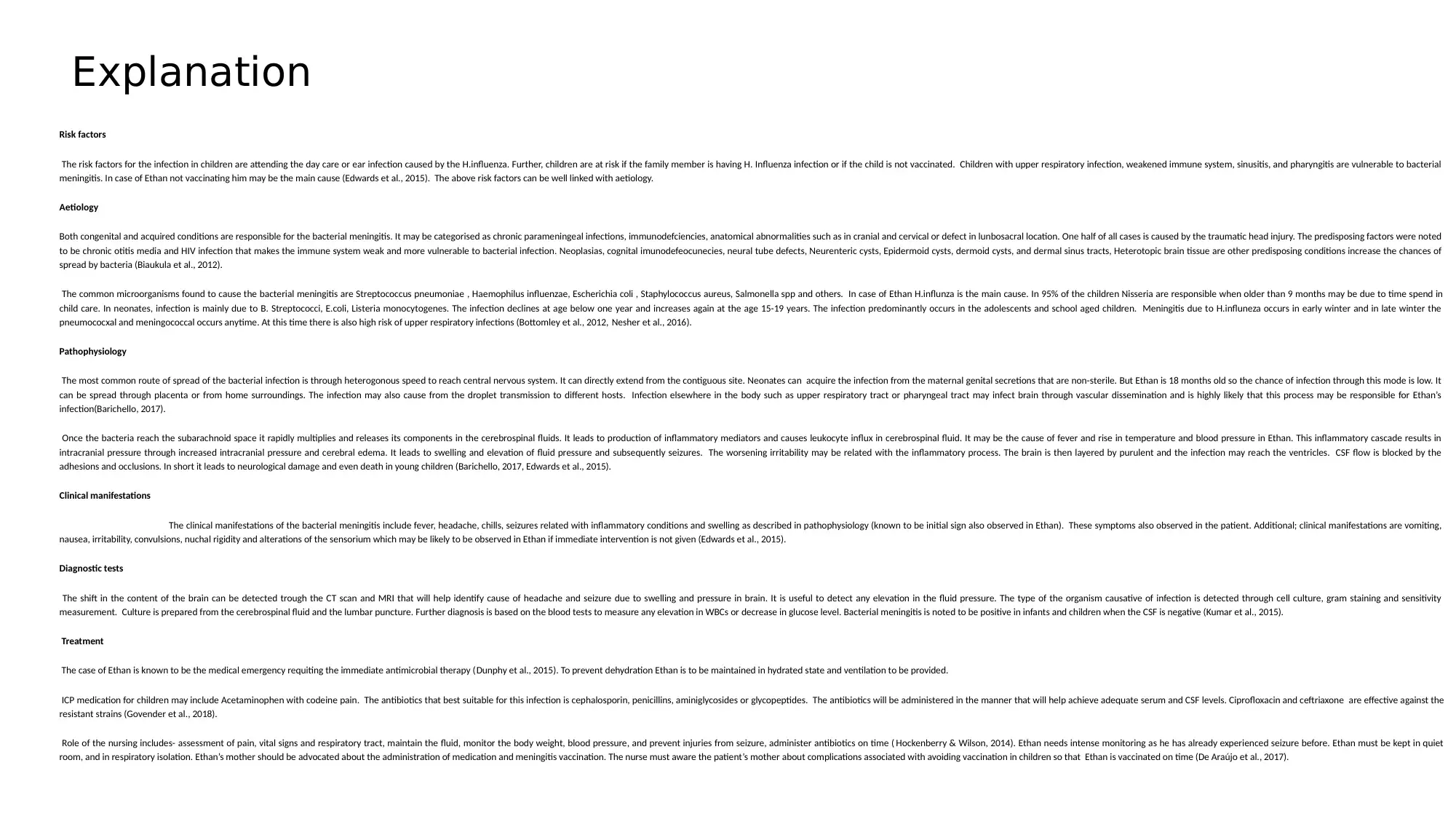
This report provides a detailed analysis of bacterial meningitis, focusing on its various aspects. It begins by outlining the risk factors associated with the infection in children, such as day care attendance, family history of H. influenzae infection, lack of vaccination, and underlying health conditions. The report then delves into the aetiology, highlighting both congenital and acquired conditions, including chronic infections, immunodeficiencies, and anatomical abnormalities. The common microorganisms responsible, such as Streptococcus pneumoniae and Haemophilus influenzae, are also discussed. The pathophysiology section explains how bacteria spread to the central nervous system, leading to inflammation, increased intracranial pressure, and neurological damage. Clinical manifestations, including fever, headache, and seizures, are described, along with diagnostic tests like CT scans, MRI, cell cultures, and blood tests. The treatment section emphasizes the need for immediate antimicrobial therapy, hydration, and ICP medication, as well as the role of nursing in assessment, monitoring, and patient education, including the importance of vaccination. The report concludes with a comprehensive list of references supporting the information presented.
1 out of 3
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.