A Qualitative Analysis: Barriers and Facilitators in CNCP Management
VerifiedAdded on 2023/06/09
|7
|9189
|406
Report
AI Summary
This report presents a qualitative analysis of primary care providers' (PCPs) experiences and attitudes regarding chronic non-cancer pain (CNCP) management. Conducted within the VA Connecticut Healthcare System, the study aimed to identify barriers and facilitators to improve CNCP care for veterans. Data were collected through open-ended surveys completed by 45 PCPs and analyzed using qualitative content analysis to identify recurring themes across system, personal/professional, and interpersonal domains. The findings revealed eleven key themes, including inadequate training, organizational impediments, clinical challenges, and interpersonal issues. Facilitators included intellectual satisfaction, improved communication skills, therapeutic alliances, universal protocols, and access to complementary medicine. The research highlights the need for strategies to mitigate barriers and enhance positive aspects of CNCP management to improve patient care and provider satisfaction. The study underscores the importance of addressing the challenges faced by PCPs in managing CNCP and provides insights for system-wide improvements in pain management within the VHA.
Lincoln et al., J Palliative Care Med 2013
DOI: 10.4172/2165-7386.S3-00
Research Article Open Access
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
Barriers and Facilitators to Chronic Non-cancer Pain Management
in Primary Care: A Qualitative Analysis of Primary Care Providers’
Experiences and Attitudes
L Elizabeth Lincoln1,2*, Linda Pellico3, Robert Kerns2,4,5 and Daren Anderson6
1Department of Medicine, Yale University School of Medicine, USA
2VA Connecticut Health Care System, USA
3Yale University School of Nursing, USA
4Department of Psychiatry and Neurology, Yale University School of Medicine, USA
5Department of Psychology, Yale University, USA
6Community Health Center Inc., USA
Abstract
Objectives: Most patients with chronic non-cancer pain (CNCP) are cared for, by primary care providers (PCPs).
While some of the barriers faced by PCPs have been described, there is little information about PCPs’ experience with
factors that facilitate CNCP care.
Design: The study design was descriptive and qualitative. Data were analyzed using qualitative content analysis.
Krippendorff’s thematic clustering technique was used to identify the repetitive themes regarding PCPs’ experiences
related to CNCP management.
Subjects: Respondents were PCPs (n=45) in the VA Connecticut Healthcare System in two academically affiliated
institutions and six community based sites.
Results: Eleven themes were identified across systems, personal/professional, and interpersonal domains.
Barriers included inadequate training, organizational impediments, clinical quandaries and the frustrations that
accompany them, issues related to share care among PCPs and specialists, antagonistic aspects of provider-patient
interactions, skepticism, and time factors. Facilitators included the intellectual satisfaction of solving difficult diagnostic
and management problems, the ability to develop keener communication skills, the rewards of healing and building
therapeutic alliances with patients, universal protocols, and the availability of complementary and alternative medicine
resources and multidisciplinary care.
Conclusion: PCPs experience substantial difficulties in caring for patients with pain while acknowledging certain
positive aspects. There is a need for strategies that mitigate the barriers to pain management while bolstering the
positive aspects to improve care and provider satisfaction.
*Corresponding author: L Elizabeth Lincoln, Instructor, Department of
Medicine, Harvard Medical School, Massachusetts General Hospital 55 Fruit
St, Yawkey 4B, Suite 4700 Boston, MA 02114, USA, Tel: 203-752-6168; E-mail:
llincoln2@partners.org
Received February 25, 2013; Accepted March 08, 2013; Published March 11,
2013
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators
to Chronic Non-cancer Pain Management in Primary Care: A Qualitative Analysis
of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3:
001. doi:10.4172/2165-7386.S3-001
Copyright: © 2013 Lincoln LE, et al. This is an open-access article distributed
under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
Keywords:Primary care; Chronic pain; Pain management; Primary
care providers; Ambulatory care
Introduction
Pain and effective pain care are among the most critical health
issues facing Americans. In 2011, the Institute of Medicine reported
that about one-third of all Americans experience persistent pain at an
annual cost of as much as $635 billion in medical treatment and lost
productivity. The report noted that military veterans are an especially
vulnerable group, with data documenting a particularly high prevalence
of pain and extraordinary rates of complexity associated with multiple
medical and mental health comorbidities [1].
Pain is the most common symptom reported by patients receiving
care in primary care, accounting for up to 40% of all visits to primary
care providers (PCPs) [2]. More than half of all patients who have
Chronic Non-Cancer Pain (CNCP) receive their care primarily from
PCPs [3].Estimates suggest that as many as 50% of male veterans and
up to 75% of female veterans seen in Veteran’s Health Administration
(VHA) primary care settings report the presence of pain [4-6]. More
recent data suggest that the prevalence of CNCP, particularly painful
musculoskeletal disorders including chronic low back pain, is increasing
annually [7]. Cost effective strategies that improve the management of
CNCP in the primary care setting are needed to address the challenges
posed by this public health crisis.
The VHA has implementeda SteppedCare Model for Pain
Management (SCM-PM) as a national pain care strategy to meet the
needs of veterans [8]. The SCM-PM provides for effective assessment
and treatment of pain within primary care whenever poss
the capacity to escalate treatment options to include specialize
and interdisciplinary approaches, if needed. Critical to the succ
the SCM-PM is the ability of PCPs and multidisciplinary primary
teams to effectively access and manage most common pain co
The SCM-PM is similar to that advocated by the American Acad
of Pain Medicine [9], and it was cited by the Institute of Medicin
potentially important model of care for persons with CNCP [1].
Unfortunately,the literaturesuggeststhat PCPs do not feel
adequately prepared to take on the role of frontline prov
patients with CNCP. Although several studies have describ
attitudesand barriersto prescribingopioidsfor CNCP [10-14],
Journal of Palliative Care & Medicine
J
o
u
r
n
a
l
o
f
P
a
I
I
i
a
t
i
v
e
C
a
r
e
&
M
e
d
i
c
i
n
e
ISSN: 2165-7386
DOI: 10.4172/2165-7386.S3-00
Research Article Open Access
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
Barriers and Facilitators to Chronic Non-cancer Pain Management
in Primary Care: A Qualitative Analysis of Primary Care Providers’
Experiences and Attitudes
L Elizabeth Lincoln1,2*, Linda Pellico3, Robert Kerns2,4,5 and Daren Anderson6
1Department of Medicine, Yale University School of Medicine, USA
2VA Connecticut Health Care System, USA
3Yale University School of Nursing, USA
4Department of Psychiatry and Neurology, Yale University School of Medicine, USA
5Department of Psychology, Yale University, USA
6Community Health Center Inc., USA
Abstract
Objectives: Most patients with chronic non-cancer pain (CNCP) are cared for, by primary care providers (PCPs).
While some of the barriers faced by PCPs have been described, there is little information about PCPs’ experience with
factors that facilitate CNCP care.
Design: The study design was descriptive and qualitative. Data were analyzed using qualitative content analysis.
Krippendorff’s thematic clustering technique was used to identify the repetitive themes regarding PCPs’ experiences
related to CNCP management.
Subjects: Respondents were PCPs (n=45) in the VA Connecticut Healthcare System in two academically affiliated
institutions and six community based sites.
Results: Eleven themes were identified across systems, personal/professional, and interpersonal domains.
Barriers included inadequate training, organizational impediments, clinical quandaries and the frustrations that
accompany them, issues related to share care among PCPs and specialists, antagonistic aspects of provider-patient
interactions, skepticism, and time factors. Facilitators included the intellectual satisfaction of solving difficult diagnostic
and management problems, the ability to develop keener communication skills, the rewards of healing and building
therapeutic alliances with patients, universal protocols, and the availability of complementary and alternative medicine
resources and multidisciplinary care.
Conclusion: PCPs experience substantial difficulties in caring for patients with pain while acknowledging certain
positive aspects. There is a need for strategies that mitigate the barriers to pain management while bolstering the
positive aspects to improve care and provider satisfaction.
*Corresponding author: L Elizabeth Lincoln, Instructor, Department of
Medicine, Harvard Medical School, Massachusetts General Hospital 55 Fruit
St, Yawkey 4B, Suite 4700 Boston, MA 02114, USA, Tel: 203-752-6168; E-mail:
llincoln2@partners.org
Received February 25, 2013; Accepted March 08, 2013; Published March 11,
2013
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators
to Chronic Non-cancer Pain Management in Primary Care: A Qualitative Analysis
of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3:
001. doi:10.4172/2165-7386.S3-001
Copyright: © 2013 Lincoln LE, et al. This is an open-access article distributed
under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
Keywords:Primary care; Chronic pain; Pain management; Primary
care providers; Ambulatory care
Introduction
Pain and effective pain care are among the most critical health
issues facing Americans. In 2011, the Institute of Medicine reported
that about one-third of all Americans experience persistent pain at an
annual cost of as much as $635 billion in medical treatment and lost
productivity. The report noted that military veterans are an especially
vulnerable group, with data documenting a particularly high prevalence
of pain and extraordinary rates of complexity associated with multiple
medical and mental health comorbidities [1].
Pain is the most common symptom reported by patients receiving
care in primary care, accounting for up to 40% of all visits to primary
care providers (PCPs) [2]. More than half of all patients who have
Chronic Non-Cancer Pain (CNCP) receive their care primarily from
PCPs [3].Estimates suggest that as many as 50% of male veterans and
up to 75% of female veterans seen in Veteran’s Health Administration
(VHA) primary care settings report the presence of pain [4-6]. More
recent data suggest that the prevalence of CNCP, particularly painful
musculoskeletal disorders including chronic low back pain, is increasing
annually [7]. Cost effective strategies that improve the management of
CNCP in the primary care setting are needed to address the challenges
posed by this public health crisis.
The VHA has implementeda SteppedCare Model for Pain
Management (SCM-PM) as a national pain care strategy to meet the
needs of veterans [8]. The SCM-PM provides for effective assessment
and treatment of pain within primary care whenever poss
the capacity to escalate treatment options to include specialize
and interdisciplinary approaches, if needed. Critical to the succ
the SCM-PM is the ability of PCPs and multidisciplinary primary
teams to effectively access and manage most common pain co
The SCM-PM is similar to that advocated by the American Acad
of Pain Medicine [9], and it was cited by the Institute of Medicin
potentially important model of care for persons with CNCP [1].
Unfortunately,the literaturesuggeststhat PCPs do not feel
adequately prepared to take on the role of frontline prov
patients with CNCP. Although several studies have describ
attitudesand barriersto prescribingopioidsfor CNCP [10-14],
Journal of Palliative Care & Medicine
J
o
u
r
n
a
l
o
f
P
a
I
I
i
a
t
i
v
e
C
a
r
e
&
M
e
d
i
c
i
n
e
ISSN: 2165-7386
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators to Chronic Non-cancer Pain Management in Primary Care: A
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 2 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
provided with a study information sheet and a paper copy of th
survey questions. Open-ended questions were selected for this
because this tactic offers a less biased approach rather t
participant responses and it facilitates spontaneity from re
[21]. Participants were recruited at practice meetings, via mail
e-mail. Non-respondents were contacted again through e-mail
of the study staff. Study questions were:
1. Describe some barriers that you feel limit your abili
manage chronic pain.
2. Can you describe some of the positive aspects related to
for patients with chronic pain?
3. What are some of the negative aspects about caring for
with chronic pain?
The PCPs’ written comments were typed verbatim into
spreadsheetand verifiedas accurateby comparingthemto the
originalsurveydata.Respondents’commentstotalednearly3000
words; individual comments ranged from one word (“time
words (average, 11 words). Rather than code responses by eac
question, all data were merged in order to comprehend meani
entirety without losing connections between the three survey p
Three of the four authors read the aggregated comments in
and inductively coded the comments. An inductive approa
used to analyze the data since there is fragmented knowledge
to the phenomenon of PCPs’ experience with CNCP using quali
methodology[22]. In inductivecoding,the text progressesfrom
specific to general, so that individual instances are discerned a
related into a larger whole that describes the phenomenon of i
Content analysis using Krippendorff’s method [23] was used to
repetitive themes. Coding consisted of the authors separately
exact words, passages, or sentences, noting unique comments
as recurrent passages related to the research questions.
grouped according to Krippendorff’s analytical technique of clu
to identify phrases and sentences that shared some characteri
an example, statements such as “suspicion,” “lack of trust in t
expertise,” and “many comfortable patients state their pain sc
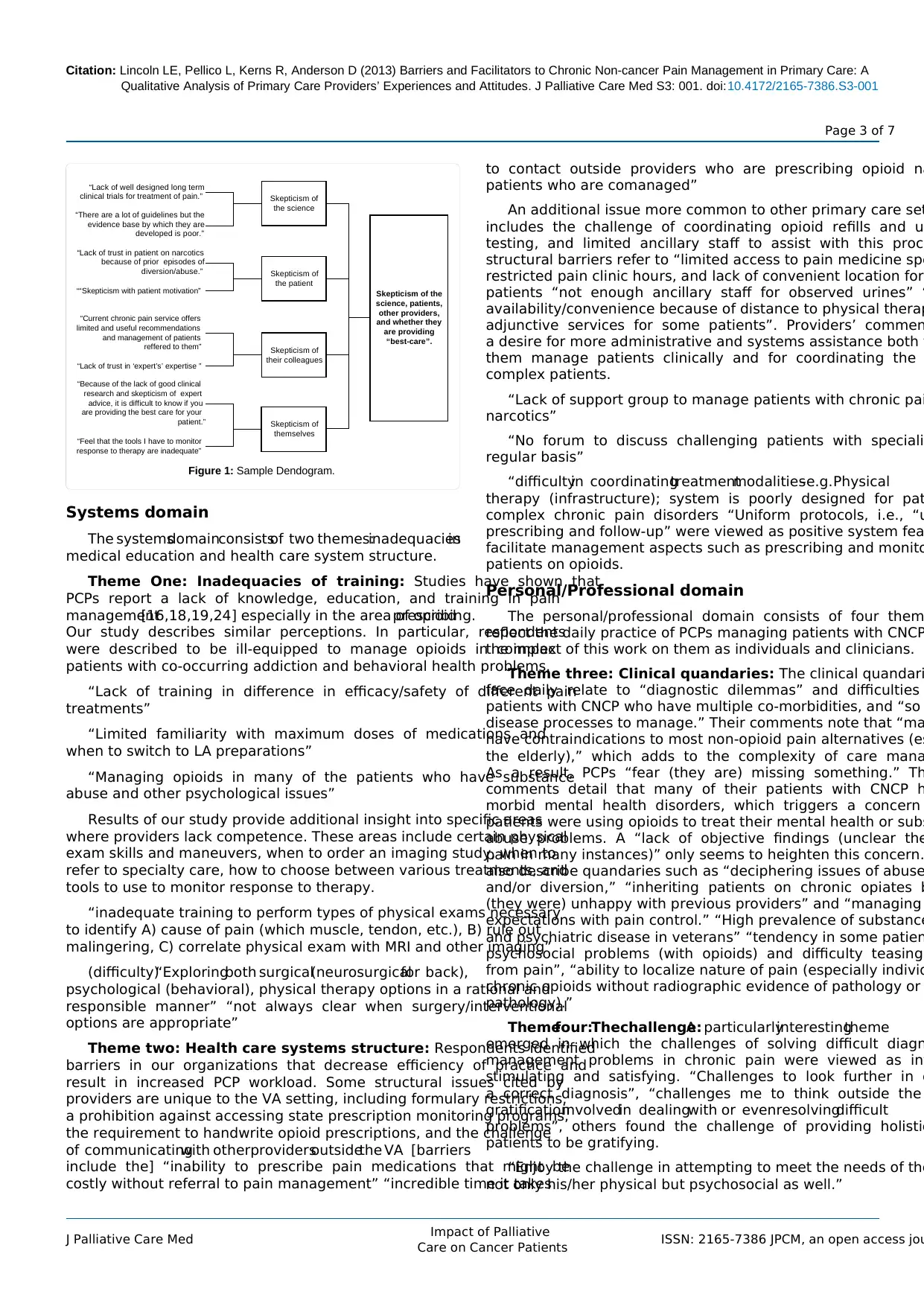
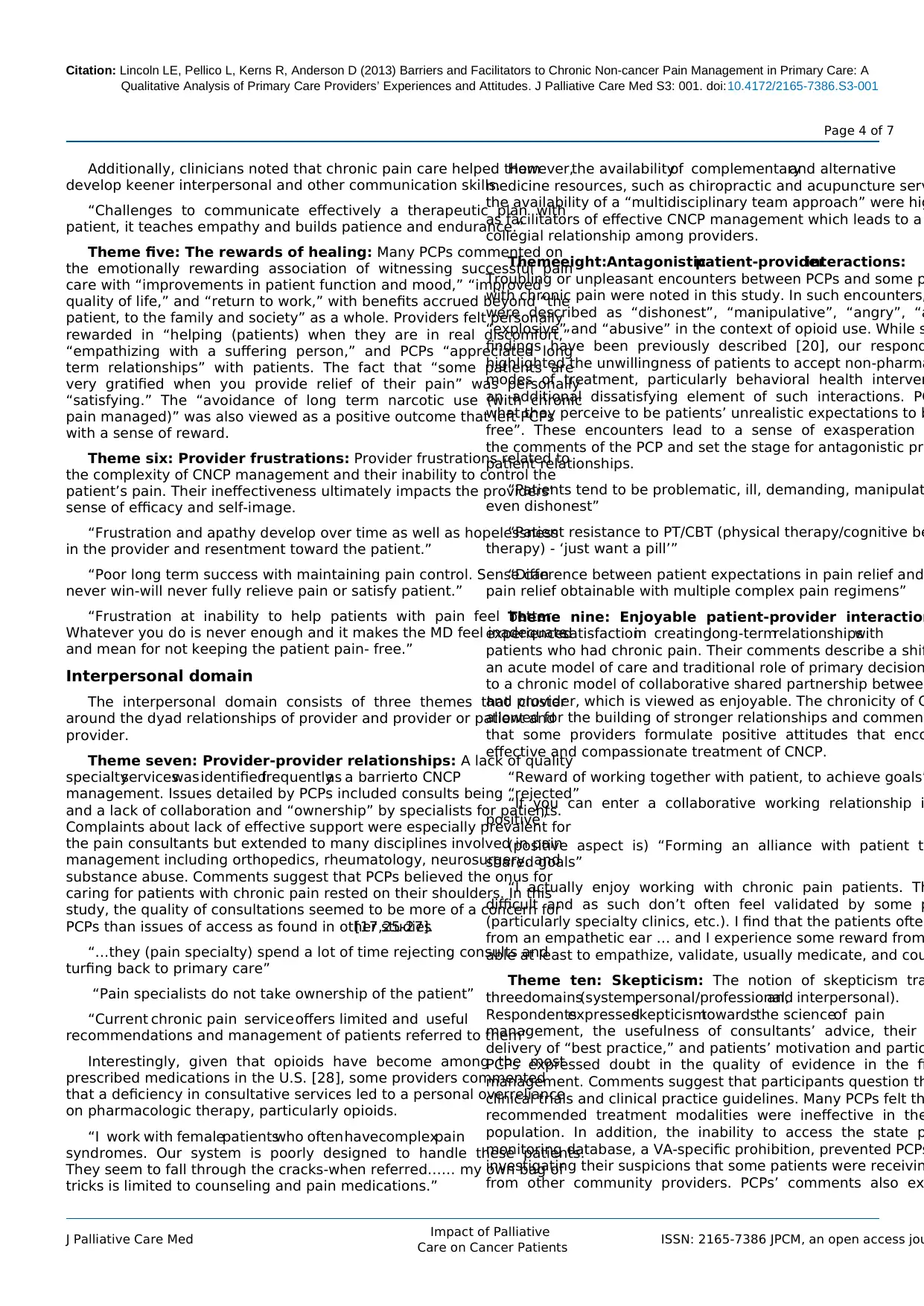
were categorized as skepticism. Dendrograms, or tree-like
were then created to illustrate how data collapsed into cl
example of a dendogram is presented in figure 1.
Authors consisted of a multidisciplinary team including a qu
nurse researcher, two primary care providers, and a pain psyc
The authorsmet frequentlyto discussselectionof passages,text
characteristics, and the transcripts were discussed line by line.
among the researchers was reconciled to represent conse
the meaning of participant comments, and the construction of
was established by group consensus. An audit trail was c
record personal reflections and to provide plausible interpretat
evidence of consistency with the original data set. The audit tr
shared with all authors. In addition, numerous participant quot
included in the results to enhance the credibility of our finding
Results
Eleven themes were identified. The themes are artificially o
into three domains as a taxonomy in which the reader c
the inter-relationships of the themes. They are: System, P
Professional, and Interpersonal domains. Two of the eleve
interrelateacrossthe threedomainsand thereforeare described
separately.
few studies provide a broad overview of CNCP management from
a provider’sperspective.Previoussurveyshaveshownthat PCPs
have concerns about the prescribing of opioids and are fearful of
contributing to addiction. In addition, PCPs note the deficiency in
primary care education and training in pain management, and question
their capacity to provide optimal pain care [15-19]. Limitations of this
research include the fact that some of these studies targeted subsets of
the broader population of primary care patients with CNCP such as
patients having high rates of opioid utilization or addiction, or included
providers other than PCPs. More information is particularly needed
about the experiences and attitudes of PCPs serving the population
of veterans. There are even fewer studies using qualitative analysis
[17,19,20]. Qualitative research offers a method of inquiry that values
the identification of the human experience related to a phenomenon
of interest and may provide a more complete understanding of PCPs’
attitudes and experiences about pain management. Interestingly, to our
knowledge, no study has specifically inquired about the positive aspects
of pain management. While we know about some of the barriers to pain
care, there is relatively little information about factors that providers
feel facilitate the care of patients with chronic pain other than opioid
agreements and a strong therapeutic doctor-patient alliance [17,20].
Our objective in conducting this study was to further describe the
context of CNCP management in primary care by exploring PCPs’
experiences and viewpoints of barriers and facilitators using qualitative
analysis. We expected that the findings would highlight important
opportunities for improving the quality of chronic pain management
in primary care not previously identified. This study was part of a larger
research project to improve the care of veterans with chronic pain at
the VA Connecticut Healthcare System (VACHS) and its findings
will be used to promote knowledge uptake and inform system-wide
improvements in pain management across the VHA.
Methods
Setting
The primary care section of the VACHS provides medical care to
46,000 veterans. Primary care is provided by PCPs in two large academic
medical centers and six community based practices. Comprehensive
specialty care is available to all VACHS patients. Patients have access to
pain specialists who perform consultations and procedures, as well as
to an interdisciplinary pain center.
Sample
All PCPs (N=60)wereinvitedto participatein the studyby
completinga threeitem open responsesurveyand a fifty item
knowledge questionnaire. Only results of the open response survey
are reported here. Forty-five PCPs participated, for a return rate of
75%. Respondents were 60% female and 40% male, with 40 Attending
Physicians, four Advanced Practice Registered Nurses (APRNs), and
one Physician Assistant (PA). Academic faculty numbered 26. Average
time in practice since graduation from training was 17 years. On
average, approximately five percent of each provider’s panel of patients
was being treated with prescription opioid medication.
Design
Surveyquestionswere formedbasedupon currentresearch
findings, overall aims of the study, and researchers’ experience treating
patients with chronic pain. This study was reviewed and approved by
the VACHS Human Studies Subcommittee, and the Yale University
School of Medicine Institutional Review Board. A waiver of written
informedconsentwas approved.All PCPs in the VACHS were
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 2 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
provided with a study information sheet and a paper copy of th
survey questions. Open-ended questions were selected for this
because this tactic offers a less biased approach rather t
participant responses and it facilitates spontaneity from re
[21]. Participants were recruited at practice meetings, via mail
e-mail. Non-respondents were contacted again through e-mail
of the study staff. Study questions were:
1. Describe some barriers that you feel limit your abili
manage chronic pain.
2. Can you describe some of the positive aspects related to
for patients with chronic pain?
3. What are some of the negative aspects about caring for
with chronic pain?
The PCPs’ written comments were typed verbatim into
spreadsheetand verifiedas accurateby comparingthemto the
originalsurveydata.Respondents’commentstotalednearly3000
words; individual comments ranged from one word (“time
words (average, 11 words). Rather than code responses by eac
question, all data were merged in order to comprehend meani
entirety without losing connections between the three survey p
Three of the four authors read the aggregated comments in
and inductively coded the comments. An inductive approa
used to analyze the data since there is fragmented knowledge
to the phenomenon of PCPs’ experience with CNCP using quali
methodology[22]. In inductivecoding,the text progressesfrom
specific to general, so that individual instances are discerned a
related into a larger whole that describes the phenomenon of i
Content analysis using Krippendorff’s method [23] was used to
repetitive themes. Coding consisted of the authors separately
exact words, passages, or sentences, noting unique comments
as recurrent passages related to the research questions.
grouped according to Krippendorff’s analytical technique of clu
to identify phrases and sentences that shared some characteri
an example, statements such as “suspicion,” “lack of trust in t
expertise,” and “many comfortable patients state their pain sc
were categorized as skepticism. Dendrograms, or tree-like
were then created to illustrate how data collapsed into cl
example of a dendogram is presented in figure 1.
Authors consisted of a multidisciplinary team including a qu
nurse researcher, two primary care providers, and a pain psyc
The authorsmet frequentlyto discussselectionof passages,text
characteristics, and the transcripts were discussed line by line.
among the researchers was reconciled to represent conse
the meaning of participant comments, and the construction of
was established by group consensus. An audit trail was c
record personal reflections and to provide plausible interpretat
evidence of consistency with the original data set. The audit tr
shared with all authors. In addition, numerous participant quot
included in the results to enhance the credibility of our finding
Results
Eleven themes were identified. The themes are artificially o
into three domains as a taxonomy in which the reader c
the inter-relationships of the themes. They are: System, P
Professional, and Interpersonal domains. Two of the eleve
interrelateacrossthe threedomainsand thereforeare described
separately.
few studies provide a broad overview of CNCP management from
a provider’sperspective.Previoussurveyshaveshownthat PCPs
have concerns about the prescribing of opioids and are fearful of
contributing to addiction. In addition, PCPs note the deficiency in
primary care education and training in pain management, and question
their capacity to provide optimal pain care [15-19]. Limitations of this
research include the fact that some of these studies targeted subsets of
the broader population of primary care patients with CNCP such as
patients having high rates of opioid utilization or addiction, or included
providers other than PCPs. More information is particularly needed
about the experiences and attitudes of PCPs serving the population
of veterans. There are even fewer studies using qualitative analysis
[17,19,20]. Qualitative research offers a method of inquiry that values
the identification of the human experience related to a phenomenon
of interest and may provide a more complete understanding of PCPs’
attitudes and experiences about pain management. Interestingly, to our
knowledge, no study has specifically inquired about the positive aspects
of pain management. While we know about some of the barriers to pain
care, there is relatively little information about factors that providers
feel facilitate the care of patients with chronic pain other than opioid
agreements and a strong therapeutic doctor-patient alliance [17,20].
Our objective in conducting this study was to further describe the
context of CNCP management in primary care by exploring PCPs’
experiences and viewpoints of barriers and facilitators using qualitative
analysis. We expected that the findings would highlight important
opportunities for improving the quality of chronic pain management
in primary care not previously identified. This study was part of a larger
research project to improve the care of veterans with chronic pain at
the VA Connecticut Healthcare System (VACHS) and its findings
will be used to promote knowledge uptake and inform system-wide
improvements in pain management across the VHA.
Methods
Setting
The primary care section of the VACHS provides medical care to
46,000 veterans. Primary care is provided by PCPs in two large academic
medical centers and six community based practices. Comprehensive
specialty care is available to all VACHS patients. Patients have access to
pain specialists who perform consultations and procedures, as well as
to an interdisciplinary pain center.
Sample
All PCPs (N=60)wereinvitedto participatein the studyby
completinga threeitem open responsesurveyand a fifty item
knowledge questionnaire. Only results of the open response survey
are reported here. Forty-five PCPs participated, for a return rate of
75%. Respondents were 60% female and 40% male, with 40 Attending
Physicians, four Advanced Practice Registered Nurses (APRNs), and
one Physician Assistant (PA). Academic faculty numbered 26. Average
time in practice since graduation from training was 17 years. On
average, approximately five percent of each provider’s panel of patients
was being treated with prescription opioid medication.
Design
Surveyquestionswere formedbasedupon currentresearch
findings, overall aims of the study, and researchers’ experience treating
patients with chronic pain. This study was reviewed and approved by
the VACHS Human Studies Subcommittee, and the Yale University
School of Medicine Institutional Review Board. A waiver of written
informedconsentwas approved.All PCPs in the VACHS were
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators to Chronic Non-cancer Pain Management in Primary Care: A
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 3 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
Systems domain
The systemsdomainconsistsof two themes:inadequaciesin
medical education and health care system structure.
Theme One: Inadequacies of training: Studies have shown that
PCPs report a lack of knowledge, education, and training in pain
management[16,18,19,24] especially in the area of opioidprescribing.
Our study describes similar perceptions. In particular, respondents
were described to be ill-equipped to manage opioids in complex
patients with co-occurring addiction and behavioral health problems.
“Lack of training in difference in efficacy/safety of different pain
treatments”
“Limited familiarity with maximum doses of medications and
when to switch to LA preparations”
“Managing opioids in many of the patients who have substance
abuse and other psychological issues”
Results of our study provide additional insight into specific areas
where providers lack competence. These areas include certain physical
exam skills and maneuvers, when to order an imaging study, when to
refer to specialty care, how to choose between various treatments, and
tools to use to monitor response to therapy.
“inadequate training to perform types of physical exams necessary
to identify A) cause of pain (which muscle, tendon, etc.), B) rule out
malingering, C) correlate physical exam with MRI and other imaging”
(difficulty)“Exploringboth surgical(neurosurgicalfor back),
psychological (behavioral), physical therapy options in a rational and
responsible manner” “not always clear when surgery/interventional
options are appropriate”
Theme two: Health care systems structure: Respondents identified
barriers in our organizations that decrease efficiency of practice and
result in increased PCP workload. Some structural issues cited by
providers are unique to the VA setting, including formulary restrictions,
a prohibition against accessing state prescription monitoring programs,
the requirement to handwrite opioid prescriptions, and the challenge
of communicatingwith otherprovidersoutsidethe VA [barriers
include the] “inability to prescribe pain medications that might be
costly without referral to pain management” “incredible time it takes
to contact outside providers who are prescribing opioid na
patients who are comanaged”
An additional issue more common to other primary care set
includes the challenge of coordinating opioid refills and u
testing, and limited ancillary staff to assist with this proc
structural barriers refer to “limited access to pain medicine spe
restricted pain clinic hours, and lack of convenient location for
patients “not enough ancillary staff for observed urines” “
availability/convenience because of distance to physical therap
adjunctive services for some patients”. Providers’ commen
a desire for more administrative and systems assistance both t
them manage patients clinically and for coordinating the
complex patients.
“Lack of support group to manage patients with chronic pai
narcotics”
“No forum to discuss challenging patients with speciali
regular basis”
“difficultyin coordinatingtreatmentmodalities–e.g.Physical
therapy (infrastructure); system is poorly designed for pat
complex chronic pain disorders “Uniform protocols, i.e., “u
prescribing and follow-up” were viewed as positive system fea
facilitate management aspects such as prescribing and monito
patients on opioids.
Personal/Professional domain
The personal/professional domain consists of four them
reflect the daily practice of PCPs managing patients with CNCP
the impact of this work on them as individuals and clinicians.
Theme three: Clinical quandaries: The clinical quandari
face daily relate to “diagnostic dilemmas” and difficulties
patients with CNCP who have multiple co-morbidities, and “so
disease processes to manage.” Their comments note that “ma
have contraindications to most non-opioid pain alternatives (es
the elderly),” which adds to the complexity of care mana
As a result, PCPs “fear (they are) missing something.” Th
comments detail that many of their patients with CNCP h
morbid mental health disorders, which triggers a concern
patients were using opioids to treat their mental health or subs
abuse problems. A “lack of objective findings (unclear the
pain in many instances)” only seems to heighten this concern.
also describe quandaries such as “deciphering issues of abuse
and/or diversion,” “inheriting patients on chronic opiates b
(they were) unhappy with previous providers” and “managing
expectations with pain control.” “High prevalence of substance
and psychiatric disease in veterans” “tendency in some patien
psychosocial problems (with opioids) and difficulty teasing
from pain”, “ability to localize nature of pain (especially individ
chronic opioids without radiographic evidence of pathology or
pathology).”
Themefour:Thechallenge:A particularlyinterestingtheme
emerged in which the challenges of solving difficult diagn
management problems in chronic pain were viewed as in
stimulating and satisfying. “Challenges to look further in o
a correct diagnosis”, “challenges me to think outside the
gratificationinvolvedin dealingwith or evenresolvingdifficult
problems”, others found the challenge of providing holistic
patients to be gratifying.
“Enjoy the challenge in attempting to meet the needs of the
not only his/her physical but psychosocial as well.”
Skepticism of the
science, patients,
other providers,
and whether they
are providing
“best-care”.
Skepticism of
the science
Skepticism of
the patient
Skepticism of
their colleagues
Skepticism of
themselves
“Lack of well designed long term
clinical trials for treatment of pain.”
“There are a lot of guidelines but the
evidence base by which they are
developed is poor.”
“Lack of trust in patient on narcotics
because of prior episodes of
diversion/abuse.”
““Skepticism with patient motivation”
“Current chronic pain service offers
limited and useful recommendations
and management of patients
reffered to them”
“Lack of trust in ‘expert’s’ expertise ”
“Because of the lack of good clinical
research and skepticism of expert
advice, it is difficult to know if you
are providing the best care for your
patient.”
“Feel that the tools I have to monitor
response to therapy are inadequate”
Figure 1: Sample Dendogram.
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 3 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
Systems domain
The systemsdomainconsistsof two themes:inadequaciesin
medical education and health care system structure.
Theme One: Inadequacies of training: Studies have shown that
PCPs report a lack of knowledge, education, and training in pain
management[16,18,19,24] especially in the area of opioidprescribing.
Our study describes similar perceptions. In particular, respondents
were described to be ill-equipped to manage opioids in complex
patients with co-occurring addiction and behavioral health problems.
“Lack of training in difference in efficacy/safety of different pain
treatments”
“Limited familiarity with maximum doses of medications and
when to switch to LA preparations”
“Managing opioids in many of the patients who have substance
abuse and other psychological issues”
Results of our study provide additional insight into specific areas
where providers lack competence. These areas include certain physical
exam skills and maneuvers, when to order an imaging study, when to
refer to specialty care, how to choose between various treatments, and
tools to use to monitor response to therapy.
“inadequate training to perform types of physical exams necessary
to identify A) cause of pain (which muscle, tendon, etc.), B) rule out
malingering, C) correlate physical exam with MRI and other imaging”
(difficulty)“Exploringboth surgical(neurosurgicalfor back),
psychological (behavioral), physical therapy options in a rational and
responsible manner” “not always clear when surgery/interventional
options are appropriate”
Theme two: Health care systems structure: Respondents identified
barriers in our organizations that decrease efficiency of practice and
result in increased PCP workload. Some structural issues cited by
providers are unique to the VA setting, including formulary restrictions,
a prohibition against accessing state prescription monitoring programs,
the requirement to handwrite opioid prescriptions, and the challenge
of communicatingwith otherprovidersoutsidethe VA [barriers
include the] “inability to prescribe pain medications that might be
costly without referral to pain management” “incredible time it takes
to contact outside providers who are prescribing opioid na
patients who are comanaged”
An additional issue more common to other primary care set
includes the challenge of coordinating opioid refills and u
testing, and limited ancillary staff to assist with this proc
structural barriers refer to “limited access to pain medicine spe
restricted pain clinic hours, and lack of convenient location for
patients “not enough ancillary staff for observed urines” “
availability/convenience because of distance to physical therap
adjunctive services for some patients”. Providers’ commen
a desire for more administrative and systems assistance both t
them manage patients clinically and for coordinating the
complex patients.
“Lack of support group to manage patients with chronic pai
narcotics”
“No forum to discuss challenging patients with speciali
regular basis”
“difficultyin coordinatingtreatmentmodalities–e.g.Physical
therapy (infrastructure); system is poorly designed for pat
complex chronic pain disorders “Uniform protocols, i.e., “u
prescribing and follow-up” were viewed as positive system fea
facilitate management aspects such as prescribing and monito
patients on opioids.
Personal/Professional domain
The personal/professional domain consists of four them
reflect the daily practice of PCPs managing patients with CNCP
the impact of this work on them as individuals and clinicians.
Theme three: Clinical quandaries: The clinical quandari
face daily relate to “diagnostic dilemmas” and difficulties
patients with CNCP who have multiple co-morbidities, and “so
disease processes to manage.” Their comments note that “ma
have contraindications to most non-opioid pain alternatives (es
the elderly),” which adds to the complexity of care mana
As a result, PCPs “fear (they are) missing something.” Th
comments detail that many of their patients with CNCP h
morbid mental health disorders, which triggers a concern
patients were using opioids to treat their mental health or subs
abuse problems. A “lack of objective findings (unclear the
pain in many instances)” only seems to heighten this concern.
also describe quandaries such as “deciphering issues of abuse
and/or diversion,” “inheriting patients on chronic opiates b
(they were) unhappy with previous providers” and “managing
expectations with pain control.” “High prevalence of substance
and psychiatric disease in veterans” “tendency in some patien
psychosocial problems (with opioids) and difficulty teasing
from pain”, “ability to localize nature of pain (especially individ
chronic opioids without radiographic evidence of pathology or
pathology).”
Themefour:Thechallenge:A particularlyinterestingtheme
emerged in which the challenges of solving difficult diagn
management problems in chronic pain were viewed as in
stimulating and satisfying. “Challenges to look further in o
a correct diagnosis”, “challenges me to think outside the
gratificationinvolvedin dealingwith or evenresolvingdifficult
problems”, others found the challenge of providing holistic
patients to be gratifying.
“Enjoy the challenge in attempting to meet the needs of the
not only his/her physical but psychosocial as well.”
Skepticism of the
science, patients,
other providers,
and whether they
are providing
“best-care”.
Skepticism of
the science
Skepticism of
the patient
Skepticism of
their colleagues
Skepticism of
themselves
“Lack of well designed long term
clinical trials for treatment of pain.”
“There are a lot of guidelines but the
evidence base by which they are
developed is poor.”
“Lack of trust in patient on narcotics
because of prior episodes of
diversion/abuse.”
““Skepticism with patient motivation”
“Current chronic pain service offers
limited and useful recommendations
and management of patients
reffered to them”
“Lack of trust in ‘expert’s’ expertise ”
“Because of the lack of good clinical
research and skepticism of expert
advice, it is difficult to know if you
are providing the best care for your
patient.”
“Feel that the tools I have to monitor
response to therapy are inadequate”
Figure 1: Sample Dendogram.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators to Chronic Non-cancer Pain Management in Primary Care: A
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 4 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
Additionally, clinicians noted that chronic pain care helped them
develop keener interpersonal and other communication skills.
“Challenges to communicate effectively a therapeutic plan with
patient, it teaches empathy and builds patience and endurance.”
Theme five: The rewards of healing: Many PCPs commented on
the emotionally rewarding association of witnessing successful pain
care with “improvements in patient function and mood,” “improved
quality of life,” and “return to work,” with benefits accrued beyond “the
patient, to the family and society” as a whole. Providers felt personally
rewarded in “helping (patients) when they are in real discomfort,”
“empathizing with a suffering person,” and PCPs “appreciated long
term relationships” with patients. The fact that “some patients are
very gratified when you provide relief of their pain” was personally
“satisfying.” The “avoidance of long term narcotic use (with chronic
pain managed)” was also viewed as a positive outcome that left PCPs
with a sense of reward.
Theme six: Provider frustrations: Provider frustrations related to
the complexity of CNCP management and their inability to control the
patient’s pain. Their ineffectiveness ultimately impacts the providers’
sense of efficacy and self-image.
“Frustration and apathy develop over time as well as hopelessness
in the provider and resentment toward the patient.”
“Poor long term success with maintaining pain control. Sense can
never win-will never fully relieve pain or satisfy patient.”
“Frustration at inability to help patients with pain feel better.
Whatever you do is never enough and it makes the MD feel inadequate
and mean for not keeping the patient pain- free.”
Interpersonal domain
The interpersonal domain consists of three themes that cluster
around the dyad relationships of provider and provider or patient and
provider.
Theme seven: Provider-provider relationships: A lack of quality
specialtyserviceswas identifiedfrequentlyas a barrierto CNCP
management. Issues detailed by PCPs included consults being “rejected”
and a lack of collaboration and “ownership” by specialists for patients.
Complaints about lack of effective support were especially prevalent for
the pain consultants but extended to many disciplines involved in pain
management including orthopedics, rheumatology, neurosurgery, and
substance abuse. Comments suggest that PCPs believed the onus for
caring for patients with chronic pain rested on their shoulders. In this
study, the quality of consultations seemed to be more of a concern for
PCPs than issues of access as found in other studies[17,25-27].
“…they (pain specialty) spend a lot of time rejecting consults and
turfing back to primary care”
“Pain specialists do not take ownership of the patient”
“Current chronic pain service offers limited and useful
recommendations and management of patients referred to them”
Interestingly, given that opioids have become among the most
prescribed medications in the U.S. [28], some providers commented
that a deficiency in consultative services led to a personal overreliance
on pharmacologic therapy, particularly opioids.
“I work with femalepatientswho often havecomplexpain
syndromes. Our system is poorly designed to handle these patients.
They seem to fall through the cracks-when referred…… my own bag of
tricks is limited to counseling and pain medications.”
However,the availabilityof complementaryand alternative
medicine resources, such as chiropractic and acupuncture serv
the availability of a “multidisciplinary team approach” were hig
as facilitators of effective CNCP management which leads to a
collegial relationship among providers.
Themeeight:Antagonisticpatient-providerinteractions:
Troubling or unpleasant encounters between PCPs and some p
with chronic pain were noted in this study. In such encounters,
were described as “dishonest”, “manipulative”, “angry”, “a
“explosive” and “abusive” in the context of opioid use. While s
findings have been previously described [20], our respond
highlighted the unwillingness of patients to accept non-pharma
modes of treatment, particularly behavioral health interven
an additional dissatisfying element of such interactions. PC
what they perceive to be patients’ unrealistic expectations to b
free”. These encounters lead to a sense of exasperation
the comments of the PCP and set the stage for antagonistic pro
patient relationships.
“Patients tend to be problematic, ill, demanding, manipulat
even dishonest”
“Patient resistance to PT/CBT (physical therapy/cognitive be
therapy) - ‘just want a pill’”
“Difference between patient expectations in pain relief and
pain relief obtainable with multiple complex pain regimens”
Theme nine: Enjoyable patient-provider interaction
experiencedsatisfactionin creatinglong-termrelationshipswith
patients who had chronic pain. Their comments describe a shif
an acute model of care and traditional role of primary decision
to a chronic model of collaborative shared partnership between
and provider, which is viewed as enjoyable. The chronicity of C
allowed for the building of stronger relationships and commen
that some providers formulate positive attitudes that enco
effective and compassionate treatment of CNCP.
“Reward of working together with patient, to achieve goals”
“If you can enter a collaborative working relationship i
positive”
(positive aspect is) “Forming an alliance with patient t
shared goals”
“I actually enjoy working with chronic pain patients. Th
difficult and as such don’t often feel validated by some p
(particularly specialty clinics, etc.). I find that the patients often
from an empathetic ear … and I experience some reward from
able at least to empathize, validate, usually medicate, and cou
Theme ten: Skepticism: The notion of skepticism tra
threedomains(system,personal/professional,and interpersonal).
Respondentsexpressedskepticismtowardsthe scienceof pain
management, the usefulness of consultants’ advice, their
delivery of “best practice,” and patients’ motivation and partic
PCPs expressed doubt in the quality of evidence in the fi
management. Comments suggest that participants question th
clinical trials and clinical practice guidelines. Many PCPs felt th
recommended treatment modalities were ineffective in the
population. In addition, the inability to access the state p
monitoring database, a VA-specific prohibition, prevented PCPs
investigating their suspicions that some patients were receivin
from other community providers. PCPs’ comments also ex
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 4 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
Additionally, clinicians noted that chronic pain care helped them
develop keener interpersonal and other communication skills.
“Challenges to communicate effectively a therapeutic plan with
patient, it teaches empathy and builds patience and endurance.”
Theme five: The rewards of healing: Many PCPs commented on
the emotionally rewarding association of witnessing successful pain
care with “improvements in patient function and mood,” “improved
quality of life,” and “return to work,” with benefits accrued beyond “the
patient, to the family and society” as a whole. Providers felt personally
rewarded in “helping (patients) when they are in real discomfort,”
“empathizing with a suffering person,” and PCPs “appreciated long
term relationships” with patients. The fact that “some patients are
very gratified when you provide relief of their pain” was personally
“satisfying.” The “avoidance of long term narcotic use (with chronic
pain managed)” was also viewed as a positive outcome that left PCPs
with a sense of reward.
Theme six: Provider frustrations: Provider frustrations related to
the complexity of CNCP management and their inability to control the
patient’s pain. Their ineffectiveness ultimately impacts the providers’
sense of efficacy and self-image.
“Frustration and apathy develop over time as well as hopelessness
in the provider and resentment toward the patient.”
“Poor long term success with maintaining pain control. Sense can
never win-will never fully relieve pain or satisfy patient.”
“Frustration at inability to help patients with pain feel better.
Whatever you do is never enough and it makes the MD feel inadequate
and mean for not keeping the patient pain- free.”
Interpersonal domain
The interpersonal domain consists of three themes that cluster
around the dyad relationships of provider and provider or patient and
provider.
Theme seven: Provider-provider relationships: A lack of quality
specialtyserviceswas identifiedfrequentlyas a barrierto CNCP
management. Issues detailed by PCPs included consults being “rejected”
and a lack of collaboration and “ownership” by specialists for patients.
Complaints about lack of effective support were especially prevalent for
the pain consultants but extended to many disciplines involved in pain
management including orthopedics, rheumatology, neurosurgery, and
substance abuse. Comments suggest that PCPs believed the onus for
caring for patients with chronic pain rested on their shoulders. In this
study, the quality of consultations seemed to be more of a concern for
PCPs than issues of access as found in other studies[17,25-27].
“…they (pain specialty) spend a lot of time rejecting consults and
turfing back to primary care”
“Pain specialists do not take ownership of the patient”
“Current chronic pain service offers limited and useful
recommendations and management of patients referred to them”
Interestingly, given that opioids have become among the most
prescribed medications in the U.S. [28], some providers commented
that a deficiency in consultative services led to a personal overreliance
on pharmacologic therapy, particularly opioids.
“I work with femalepatientswho often havecomplexpain
syndromes. Our system is poorly designed to handle these patients.
They seem to fall through the cracks-when referred…… my own bag of
tricks is limited to counseling and pain medications.”
However,the availabilityof complementaryand alternative
medicine resources, such as chiropractic and acupuncture serv
the availability of a “multidisciplinary team approach” were hig
as facilitators of effective CNCP management which leads to a
collegial relationship among providers.
Themeeight:Antagonisticpatient-providerinteractions:
Troubling or unpleasant encounters between PCPs and some p
with chronic pain were noted in this study. In such encounters,
were described as “dishonest”, “manipulative”, “angry”, “a
“explosive” and “abusive” in the context of opioid use. While s
findings have been previously described [20], our respond
highlighted the unwillingness of patients to accept non-pharma
modes of treatment, particularly behavioral health interven
an additional dissatisfying element of such interactions. PC
what they perceive to be patients’ unrealistic expectations to b
free”. These encounters lead to a sense of exasperation
the comments of the PCP and set the stage for antagonistic pro
patient relationships.
“Patients tend to be problematic, ill, demanding, manipulat
even dishonest”
“Patient resistance to PT/CBT (physical therapy/cognitive be
therapy) - ‘just want a pill’”
“Difference between patient expectations in pain relief and
pain relief obtainable with multiple complex pain regimens”
Theme nine: Enjoyable patient-provider interaction
experiencedsatisfactionin creatinglong-termrelationshipswith
patients who had chronic pain. Their comments describe a shif
an acute model of care and traditional role of primary decision
to a chronic model of collaborative shared partnership between
and provider, which is viewed as enjoyable. The chronicity of C
allowed for the building of stronger relationships and commen
that some providers formulate positive attitudes that enco
effective and compassionate treatment of CNCP.
“Reward of working together with patient, to achieve goals”
“If you can enter a collaborative working relationship i
positive”
(positive aspect is) “Forming an alliance with patient t
shared goals”
“I actually enjoy working with chronic pain patients. Th
difficult and as such don’t often feel validated by some p
(particularly specialty clinics, etc.). I find that the patients often
from an empathetic ear … and I experience some reward from
able at least to empathize, validate, usually medicate, and cou
Theme ten: Skepticism: The notion of skepticism tra
threedomains(system,personal/professional,and interpersonal).
Respondentsexpressedskepticismtowardsthe scienceof pain
management, the usefulness of consultants’ advice, their
delivery of “best practice,” and patients’ motivation and partic
PCPs expressed doubt in the quality of evidence in the fi
management. Comments suggest that participants question th
clinical trials and clinical practice guidelines. Many PCPs felt th
recommended treatment modalities were ineffective in the
population. In addition, the inability to access the state p
monitoring database, a VA-specific prohibition, prevented PCPs
investigating their suspicions that some patients were receivin
from other community providers. PCPs’ comments also ex
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators to Chronic Non-cancer Pain Management in Primary Care: A
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 5 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
lack of trust in pain specialists further enhanced by a perception that
many recommended treatment plans were ineffective in improving
patient outcomes. Respondents also expressed concern about cross
coveringother providers’patients,noting that “patientsare on
strange combinations of multiple short and long pain medications.”
An additional factor contributing to the theme of suspicion is what
respondents referred to as the “subjective nature of pain” and the lack
of objective measures to corroborate complaints of pain. Respondents
expressed skepticism about the numeric one to ten scale used to assess
pain, noting “many comfortable patients state their pain score is 10.”
Finally, PCPs’ comments reveal skepticism of patients’ motivation
and commitment to adhere to a plan of care. They were suspicious
of patients whom they felt may have secondary gain motives. PCPs
expressed mistrust of patients who might be diverting or abusing
opioids and those whom they felt were receiving opioids from multiple
providers. Providers reported this as a barrier since it led to the loss of
a trusting relationship. Refer to the dendrogram (Figure 1) for specific
supporting comments.
Theme eleven: Lack of time: Time pressure was a theme that was
found in the system, personal/professional, and interpersonal domains.
Providers’ describe busy office visits without enough time to address
all the issues, limited appointment availability for specialty clinics
and resultantlong wait times,and burdensome,time-consuming
prescription refill activities. They report that patients with chronic
pain often required more time than other visits and also needed more
frequent visits overall compared with other patients. This perception
that CNCP patients on opioids have a higher number of clinic visits is
supported by the literature [29,30]. PCPs also noted that patients with
pain generate more non-visit work such as coordination of care and
frequent medication refills, which result in an increased workload for
PCPs and staff. Addressing pain in the context of a primary care visit
sometimes resulted in neglecting other non-pain related conditions. As
noted by PCPs, “there are so many other disease processes to manage,”
that “there is not enough time to really think critically.” They also note
that time pressure impacts negatively on their ability to care for other
patients as well. Additionally, patients “demanding to be seen between
appointments,” and “pestering” the PCP and staff are considered both
“time consuming and energy consuming.”
“Time; Office visits are so compressed as it is; it’s difficult to spend
appropriatetime assessingchangein function,emotionalaspects
which feed into pain, etc.”
“Time; ideally should be seeing these folks more often than we have
time for”
“…. large amount of time spent on phone, in person, outside of
usual office visit”
“It takes away time from other patients”
“Frequent walk ins and phone calls and interruptions while in
clinic seeing other patients, patients can be challenging, demanding,
come in between appointments, demand to be seen.”
Discussion
This study provided a rich and descriptive picture of providers’
experiencesand viewpointsaboutchronic pain managementin
primary care. Through the application of a rigorous and structured
qualitative method, Krippendorf’s method, we were able to identify
and elaboratethree distinct,yet overlapping,domains,namely
System, Personal/Professional, and Interpersonal, that may provide an
important framework that can be employed to inform the development
and enactment of quality improvement efforts. The findings de
the context of pain care in primary care settings and poi
challenges of providing care to persons with CNCP that m
addressed to meet the needs of this vulnerable population. Im
we also identified themes that characterize perceived positive
of this work that may serve as incentives for engaging in
improvement efforts.
Across the three domains, multiple barriers of caring for pe
with CNCP were identified. System factors included inadeq
education and deficient competencies to assess and mana
common chronic pain conditions, as well as organizational
that impede the enactment of even well- developed comp
treatment plans. A second primary domain focused on Persona
Professional factors that are associated with the provision of op
pain care. Themes highlighted the complexity of managing
persons with multiple comorbidities, especially mental hea
substance use disorders, and both the clinical quandaries
commonly confronted and the pervasive experience of frustrat
accompanies these challenges. The third domain that was isola
the analyses relates to the interpersonal aspects of pain care,
challenging issues related to share care among PCPs and
as well as difficult aspects of provider – patient interactio
identification of multiple specific themes within this domain ma
to better isolate targets for improvement.
The fact that primarycare providersfind pain management
challenging, is not a new observation. Studies have shown tha
harbor significantly negative feelings about pain care [15,20] a
unable to meet the needs of patients with CNCP [15-19]. Our s
however, provides a rich and more nuanced picture of what pr
care providers feel about the topic and adds more detail, with
observations that can help guide future improvement activ
addition, the significant positive elements about pain care
by providers in this study suggest a real opportunity to a
underlying problems and convert pain care into a satisfying as
primary care practice.
However, the challenges outlined in this study will nee
addressed. Providers need training and support in opioid mana
physical diagnosis, and a broader understanding of the ro
pharmacologic interventions. Providers need better communic
coordination of care with pain specialists and a stronger collab
with specialists to ensure that accountability is clarified and co
are appropriate. Improving partnerships with specialists an
to specialty care for primary care patients is part of the Steppe
Model advocated by the American Academy of Pain Medicine [
an important element of a new initiative in VHA called SCAN-EC
(Specialty Care Access Network- Extension of Community Heal
Outcomes). In SCAN-ECHO, specialists provide ongoing case ba
learning and collaborative, consultative care via videoconfe
to PCPs in remote settings in order to support the develo
competencies in pain assessment and management. Another s
beingtrialedat the VHA are electronicconsults,which provide
answers to specific questions posed by PCPs without a visit enc
by various specialists including pain specialists.
The primary care team including nurses, medical assist
receptionists, needs to work together to address the incre
load that patients with pain entail and to develop efficient work
to manage administrative issues such as opioid agreemen
toxicology monitoring, and telephone communication. The
Centered Medical Home model calls for a collaborative, te
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 5 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
lack of trust in pain specialists further enhanced by a perception that
many recommended treatment plans were ineffective in improving
patient outcomes. Respondents also expressed concern about cross
coveringother providers’patients,noting that “patientsare on
strange combinations of multiple short and long pain medications.”
An additional factor contributing to the theme of suspicion is what
respondents referred to as the “subjective nature of pain” and the lack
of objective measures to corroborate complaints of pain. Respondents
expressed skepticism about the numeric one to ten scale used to assess
pain, noting “many comfortable patients state their pain score is 10.”
Finally, PCPs’ comments reveal skepticism of patients’ motivation
and commitment to adhere to a plan of care. They were suspicious
of patients whom they felt may have secondary gain motives. PCPs
expressed mistrust of patients who might be diverting or abusing
opioids and those whom they felt were receiving opioids from multiple
providers. Providers reported this as a barrier since it led to the loss of
a trusting relationship. Refer to the dendrogram (Figure 1) for specific
supporting comments.
Theme eleven: Lack of time: Time pressure was a theme that was
found in the system, personal/professional, and interpersonal domains.
Providers’ describe busy office visits without enough time to address
all the issues, limited appointment availability for specialty clinics
and resultantlong wait times,and burdensome,time-consuming
prescription refill activities. They report that patients with chronic
pain often required more time than other visits and also needed more
frequent visits overall compared with other patients. This perception
that CNCP patients on opioids have a higher number of clinic visits is
supported by the literature [29,30]. PCPs also noted that patients with
pain generate more non-visit work such as coordination of care and
frequent medication refills, which result in an increased workload for
PCPs and staff. Addressing pain in the context of a primary care visit
sometimes resulted in neglecting other non-pain related conditions. As
noted by PCPs, “there are so many other disease processes to manage,”
that “there is not enough time to really think critically.” They also note
that time pressure impacts negatively on their ability to care for other
patients as well. Additionally, patients “demanding to be seen between
appointments,” and “pestering” the PCP and staff are considered both
“time consuming and energy consuming.”
“Time; Office visits are so compressed as it is; it’s difficult to spend
appropriatetime assessingchangein function,emotionalaspects
which feed into pain, etc.”
“Time; ideally should be seeing these folks more often than we have
time for”
“…. large amount of time spent on phone, in person, outside of
usual office visit”
“It takes away time from other patients”
“Frequent walk ins and phone calls and interruptions while in
clinic seeing other patients, patients can be challenging, demanding,
come in between appointments, demand to be seen.”
Discussion
This study provided a rich and descriptive picture of providers’
experiencesand viewpointsaboutchronic pain managementin
primary care. Through the application of a rigorous and structured
qualitative method, Krippendorf’s method, we were able to identify
and elaboratethree distinct,yet overlapping,domains,namely
System, Personal/Professional, and Interpersonal, that may provide an
important framework that can be employed to inform the development
and enactment of quality improvement efforts. The findings de
the context of pain care in primary care settings and poi
challenges of providing care to persons with CNCP that m
addressed to meet the needs of this vulnerable population. Im
we also identified themes that characterize perceived positive
of this work that may serve as incentives for engaging in
improvement efforts.
Across the three domains, multiple barriers of caring for pe
with CNCP were identified. System factors included inadeq
education and deficient competencies to assess and mana
common chronic pain conditions, as well as organizational
that impede the enactment of even well- developed comp
treatment plans. A second primary domain focused on Persona
Professional factors that are associated with the provision of op
pain care. Themes highlighted the complexity of managing
persons with multiple comorbidities, especially mental hea
substance use disorders, and both the clinical quandaries
commonly confronted and the pervasive experience of frustrat
accompanies these challenges. The third domain that was isola
the analyses relates to the interpersonal aspects of pain care,
challenging issues related to share care among PCPs and
as well as difficult aspects of provider – patient interactio
identification of multiple specific themes within this domain ma
to better isolate targets for improvement.
The fact that primarycare providersfind pain management
challenging, is not a new observation. Studies have shown tha
harbor significantly negative feelings about pain care [15,20] a
unable to meet the needs of patients with CNCP [15-19]. Our s
however, provides a rich and more nuanced picture of what pr
care providers feel about the topic and adds more detail, with
observations that can help guide future improvement activ
addition, the significant positive elements about pain care
by providers in this study suggest a real opportunity to a
underlying problems and convert pain care into a satisfying as
primary care practice.
However, the challenges outlined in this study will nee
addressed. Providers need training and support in opioid mana
physical diagnosis, and a broader understanding of the ro
pharmacologic interventions. Providers need better communic
coordination of care with pain specialists and a stronger collab
with specialists to ensure that accountability is clarified and co
are appropriate. Improving partnerships with specialists an
to specialty care for primary care patients is part of the Steppe
Model advocated by the American Academy of Pain Medicine [
an important element of a new initiative in VHA called SCAN-EC
(Specialty Care Access Network- Extension of Community Heal
Outcomes). In SCAN-ECHO, specialists provide ongoing case ba
learning and collaborative, consultative care via videoconfe
to PCPs in remote settings in order to support the develo
competencies in pain assessment and management. Another s
beingtrialedat the VHA are electronicconsults,which provide
answers to specific questions posed by PCPs without a visit enc
by various specialists including pain specialists.
The primary care team including nurses, medical assist
receptionists, needs to work together to address the incre
load that patients with pain entail and to develop efficient work
to manage administrative issues such as opioid agreemen
toxicology monitoring, and telephone communication. The
Centered Medical Home model calls for a collaborative, te
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators to Chronic Non-cancer Pain Management in Primary Care: A
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 6 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
approach to primary care [31]. Many of the systems issues cited in this
study could be improved through more effective use of a health care
team. The use of nurse care coordinators to provide support for patients
with chronic pain has been shown to improve patient satisfaction and
pain scores [32-34]. Opioid renewal clinics can improve pain care
by assigning dedicated staff to manage the opioid prescription and
monitoring process for high risk patients [35]. Other collaborative
and interdisciplinary approaches may help with the management of
patients with complex psychosocial and behavioral issues. Chronic
pain is prevalent in two-thirds of patients with major depressive
illness [36,37]. Optimizing depression in a primary care setting with
the assistance of a mental health liaison improves pain levels [38,39].
Efforts to integrate mental health care into primary care as is practiced
at the VHA should be expanded.
One particularly frequent theme that appeared in our study and
that of Matthias et al. was that of the challenging, antagonistic patient
encounter [20]. The physician-patient relationship is predicated on
trust, communication, and a patient centered partnership in which the
patient and provider work together towards a common aim. Comments
from this study suggest that such relationships often are compromised
by suspicion and lack of trust and that antagonism, frustration, and
even nihilism often pervade the encounter. In pain care, differing
expectations between patients and PCPs are common [40,41]. Lack
of concordance between patient and physician goals may contribute
many of the negative feelings about pain care expressed by study
respondents. This aspect of pain care needs to be addressed specifically.
Primary care providers need training in how to handle challenging and
unpleasant encounters and need to acquire tools, many of which are
more commonly employed by behavioral health staff, to manage these
negative emotions and better handle difficult encounters to improve
the likelihood of a positive outcome.
Our institution has piloted a peer support intervention for PCPs
who may be experiencing tension in the relationship with an individual
patient with chronic pain. In this model, PCPs can present their
experience to a committee that includes PCPs who are knowledgeable
in pain care, a behavioral health provider, and an addictions specialist.
PCPs are able to share their frustrations, receive emotional support,
and are also assisted in developing a specific plan of care. Occasionally,
members of the committee will meet with the PCP and patient together,
to help facilitateunderstandingand defusetension.Preliminary
feedback of this process from PCPs has been highly positive.
The positive factors identified in this study that facilitate CNCP
care in the primary care setting are of equal interest and have been
less described in the literature. They largely encompassed humanistic,
altruistic and relational aspects of caring for an individual with chronic
pain. Positive relationships can contribute to provider satisfaction in
CNCP management [17,20]. Enhancing patient-centered skills in the
context of shared decision making may improve the experience of
providers and patients. Training providers in empathy, a positive aspect
of pain care cited in this study, may be especially helpful in CNCP care
[42,43]. Novel approaches to training providers and medical students
in shareddecisionmakingand affectiveskills improvesprovider
satisfaction, relationships, and interest in caring for patients with pain
[44,45]. Providers described feeling rewarded when they were able to
alleviate suffering and provide comfort to patients, and see them regain
functionality and have improved well-being.
Additionalfacilitatorsto CNCP careincludedthe intellectual
satisfactionof solving difficult diagnostic,management,and
communication problems. Having universal protocols in place, the
availabilityof complementaryand alternativemedicineresources,
especially chiropractic services, and multidisciplinary care of c
patients were other promoters of successful pain care.
Skepticism among PCPs about the science of pain managem
another interesting finding from this study that merits further a
PCPs suggested that pain management guidelines were not su
by robust clinical evidence noting in particular the lack o
evidence for the efficacy and safety of opioids for the managem
long term CNCP [46]. PCPs may find it beneficial to have
practice algorithms for specific syndromes and symptom comp
Such an approach to management may help to resolve s
uncertainties around the need for imaging tests and in decidin
pharmacologic and non-pharmacologic treatment options to co
for individual patients.
This study had several limitations. The sample size, consist
PCPs from one VA medical system, was small. However, o
response rate, the varied clinical settings, and the detaile
of the responses suggest that we were able to capture a
representative picture for a VHA health system that includes a
and non-academic sites, and large as well as smaller communi
practices. Additionally, 100% of the providers surveyed were p
care providers. Most providers served male veterans, limit
generalizability to female patients and non-veterans. A distrac
may have been the increased complexity of primary care patie
VHA setting. We used written survey data, which limited our ca
to further explore participant responses. Additionally, there is c
that participants with either strong positive or negative opinion
take the time to respond to the survey while participants with
positions may not respond. Therefore, valuable observations m
be available for interpretation.
Conclusion
Findings from our study should help to inform efforts to imp
the management of CNCP in primary care. Pain care gets
attention in medical training and in research, despite the fact t
prevalence of chronic pain exceeds that of ischemic heart dise
diabetes combined [47]. Given the high prevalence of pain in p
care, chronic pain management should be considered a primar
competencythroughaccreditationand board requirements.The
increasing awareness of the problems posed by prescriptio
abuse and diversion, coupled with the recognition that pa
undertreatedin medicine,leavesprimarycare providerscaught
in the middle with limited tools and skills. Current practic
unsustainable, leaving both patients and providers unsatis
leading to an overreliance on opioids and a burgeoning prescri
drug abuse crisis. Sustained focus on these critical issues is ne
ensure that primary care can continue to place patients at the
of care and do so in a manner that is rewarding and pr
satisfying for the primary care provider.
Acknowledgements
This material is supported in part by the Department of Veterans Affairs,
Veterans Health Administration, Office of Research and Development, Health
Services Research and Development Service Research Enhancement Award
Program (REAP 08-266); a Program for Research Leadership Award from The
Patrick and Catherine Weldon Donaghue Medical Research Foundation and
Mayday Fund.
References
1. Institute of Medicine Consensus Report (2011) Relieving pain in America: a
blueprint for transforming prevention, care, education, and research.
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 6 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
approach to primary care [31]. Many of the systems issues cited in this
study could be improved through more effective use of a health care
team. The use of nurse care coordinators to provide support for patients
with chronic pain has been shown to improve patient satisfaction and
pain scores [32-34]. Opioid renewal clinics can improve pain care
by assigning dedicated staff to manage the opioid prescription and
monitoring process for high risk patients [35]. Other collaborative
and interdisciplinary approaches may help with the management of
patients with complex psychosocial and behavioral issues. Chronic
pain is prevalent in two-thirds of patients with major depressive
illness [36,37]. Optimizing depression in a primary care setting with
the assistance of a mental health liaison improves pain levels [38,39].
Efforts to integrate mental health care into primary care as is practiced
at the VHA should be expanded.
One particularly frequent theme that appeared in our study and
that of Matthias et al. was that of the challenging, antagonistic patient
encounter [20]. The physician-patient relationship is predicated on
trust, communication, and a patient centered partnership in which the
patient and provider work together towards a common aim. Comments
from this study suggest that such relationships often are compromised
by suspicion and lack of trust and that antagonism, frustration, and
even nihilism often pervade the encounter. In pain care, differing
expectations between patients and PCPs are common [40,41]. Lack
of concordance between patient and physician goals may contribute
many of the negative feelings about pain care expressed by study
respondents. This aspect of pain care needs to be addressed specifically.
Primary care providers need training in how to handle challenging and
unpleasant encounters and need to acquire tools, many of which are
more commonly employed by behavioral health staff, to manage these
negative emotions and better handle difficult encounters to improve
the likelihood of a positive outcome.
Our institution has piloted a peer support intervention for PCPs
who may be experiencing tension in the relationship with an individual
patient with chronic pain. In this model, PCPs can present their
experience to a committee that includes PCPs who are knowledgeable
in pain care, a behavioral health provider, and an addictions specialist.
PCPs are able to share their frustrations, receive emotional support,
and are also assisted in developing a specific plan of care. Occasionally,
members of the committee will meet with the PCP and patient together,
to help facilitateunderstandingand defusetension.Preliminary
feedback of this process from PCPs has been highly positive.
The positive factors identified in this study that facilitate CNCP
care in the primary care setting are of equal interest and have been
less described in the literature. They largely encompassed humanistic,
altruistic and relational aspects of caring for an individual with chronic
pain. Positive relationships can contribute to provider satisfaction in
CNCP management [17,20]. Enhancing patient-centered skills in the
context of shared decision making may improve the experience of
providers and patients. Training providers in empathy, a positive aspect
of pain care cited in this study, may be especially helpful in CNCP care
[42,43]. Novel approaches to training providers and medical students
in shareddecisionmakingand affectiveskills improvesprovider
satisfaction, relationships, and interest in caring for patients with pain
[44,45]. Providers described feeling rewarded when they were able to
alleviate suffering and provide comfort to patients, and see them regain
functionality and have improved well-being.
Additionalfacilitatorsto CNCP careincludedthe intellectual
satisfactionof solving difficult diagnostic,management,and
communication problems. Having universal protocols in place, the
availabilityof complementaryand alternativemedicineresources,
especially chiropractic services, and multidisciplinary care of c
patients were other promoters of successful pain care.
Skepticism among PCPs about the science of pain managem
another interesting finding from this study that merits further a
PCPs suggested that pain management guidelines were not su
by robust clinical evidence noting in particular the lack o
evidence for the efficacy and safety of opioids for the managem
long term CNCP [46]. PCPs may find it beneficial to have
practice algorithms for specific syndromes and symptom comp
Such an approach to management may help to resolve s
uncertainties around the need for imaging tests and in decidin
pharmacologic and non-pharmacologic treatment options to co
for individual patients.
This study had several limitations. The sample size, consist
PCPs from one VA medical system, was small. However, o
response rate, the varied clinical settings, and the detaile
of the responses suggest that we were able to capture a
representative picture for a VHA health system that includes a
and non-academic sites, and large as well as smaller communi
practices. Additionally, 100% of the providers surveyed were p
care providers. Most providers served male veterans, limit
generalizability to female patients and non-veterans. A distrac
may have been the increased complexity of primary care patie
VHA setting. We used written survey data, which limited our ca
to further explore participant responses. Additionally, there is c
that participants with either strong positive or negative opinion
take the time to respond to the survey while participants with
positions may not respond. Therefore, valuable observations m
be available for interpretation.
Conclusion
Findings from our study should help to inform efforts to imp
the management of CNCP in primary care. Pain care gets
attention in medical training and in research, despite the fact t
prevalence of chronic pain exceeds that of ischemic heart dise
diabetes combined [47]. Given the high prevalence of pain in p
care, chronic pain management should be considered a primar
competencythroughaccreditationand board requirements.The
increasing awareness of the problems posed by prescriptio
abuse and diversion, coupled with the recognition that pa
undertreatedin medicine,leavesprimarycare providerscaught
in the middle with limited tools and skills. Current practic
unsustainable, leaving both patients and providers unsatis
leading to an overreliance on opioids and a burgeoning prescri
drug abuse crisis. Sustained focus on these critical issues is ne
ensure that primary care can continue to place patients at the
of care and do so in a manner that is rewarding and pr
satisfying for the primary care provider.
Acknowledgements
This material is supported in part by the Department of Veterans Affairs,
Veterans Health Administration, Office of Research and Development, Health
Services Research and Development Service Research Enhancement Award
Program (REAP 08-266); a Program for Research Leadership Award from The
Patrick and Catherine Weldon Donaghue Medical Research Foundation and
Mayday Fund.
References
1. Institute of Medicine Consensus Report (2011) Relieving pain in America: a
blueprint for transforming prevention, care, education, and research.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Citation: Lincoln LE, Pellico L, Kerns R, Anderson D (2013) Barriers and Facilitators to Chronic Non-cancer Pain Management in Primary Care: A
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 7 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
2. Kroenke K (2003) Patients presenting with somatic complaints: epidemiology,
psychiatric comorbidity and management. Int J Methods Psychiatr Res 12: 34-
43.
3. Breuer B, Cruciani R, Portenoy RK (2010) Pain management by primary care
physicians, pain physicians, chiropractors, and acupuncturists: a national
survey. South Med J 103: 738-747.
4. Kerns RD, Otis J, Rosenberg R, Reid MC (2003) Veterans’ reports of pain and
associations with ratings of health, health-risk behaviors, affective distress, and
use of the healthcare system. J Rehabil Res Dev 40: 371-379.
5. Haskell SG, Heapy A, Reid MC, Papas RK, Kerns RD (2006) The Prevalence
and age-related characteristics of pain in a sample of women veterans receiving
primary care. J Womens Health (Larchmit) 15: 862-869.
6. Crosby FE, Colestro J, Ventura MR, Graham K (2006) Survey of pain among
veterans in Western New York. Pain Manag Nurs 7: 12-22.
7. Haskell SG, Ning Y, Krebs E, Goulet J, Mattocks K, et al. (2012) The prevalence
of painful musculoskeletal conditions in female and male veterans in 7 years
after return from deployment in Operation Enduring Freedom/Operation Iraqi
Freedom. Clin J Pain 28: 163-167.
8. Veterans Health Administration (2009) VHA Directive 2009-053: Pain
Management. Washington, DC: Department of Veterans Affairs.
9. Dubois MY, Gallagher RM, Lippe PM (2009) Pain Medicine Position Paper.
Pain Med 10: 972-1000.
10. Hutchinson K, Moreland AM, de C Williams AC, Weinman J, Horne R (2007)
Exploring beliefs and practice of opioid prescribing for persistent non-cancer
pain by general practitioners. Eur J Pain 11:93-98.
11. Potter M, Schafer S, Gonzalez-Mendez E, Gjeltema K, Lopez A, et al. (2001)
Opioids for chronic nonmalignant pain. Attitudes and practices of primary care
physicians in the UCSF/Stanford collaborative research network. J Fam Pract
50: 145-151.
12. Nwokeji ED, Rascati KL, Brown CM, Eisenberg A (2007) Influences of attitudes
on family physicians’ willingness to prescribe long-acting opioid analgesics for
patients with chronic nonmalignant pain. Clin Ther: 2589-2602.
13. Bhamb B, Brown D, Hariharan J, Anderson J, Balousek S, et al. (2006) Survey
of select practice behaviors by primary care physicians on the use of opioids for
chronic pain. Curr Med Opin 9: 1859-1865.
14. Turk DC, Brody MC, Okifuji EA (1994) Physicians’ attitudes and practices
regarding the long-term prescribing of opioids for non-cancer pain. Pain 59:
201-208.
15. Dobscha SK, Corson K, Flores JA, Tansill EC, Gerrity MS ( 2008) Veterans
Affairs primary care clinicians’ attitudes toward chronic pain and correlates of
opioid prescribing rates. Pain Med 9: 564-571.
16. Upshur CC, Luckmann RS, Savageau JA (2006) Primary care provider
concerns about management of chronic pain in community clinic populations. J
Gen Intern Med 21: 652-655.
17. Barry DT, Irwin KS, Jones ES, Becker WC, Tetrault JM, et al. (2010) Opioids,
chronic pain, and addiction in primary care. J Pain 11: 1442-1445.
18. Ponte CD, Johnson-Tribino J ( 2005) Attitudes and knowledge about pain: an
assessment of West Virginia family physicians. Fam Med 37: 477-480.
19. Leverence RR, Williams RL, Potter M, Fernald D, Unverzagt M, et al. (2011)
Chronic non-cancer pain: a siren for primary care--a report from the PRImary
Care MultiEthnic Network ( PRIME Net). J Am Board Fam Med 24: 551-561.
20. Matthias MS, Parpart AL, Nyland KA, Huffman MA, Stubbs DL, et al. (2010)
The patient-provider relationship in chronic pain care: provider’s perspectives.
Pain Med 11: 1688-1697.
21. Niedomysl T, Malmberg B (2009) Do open-ended survey questions on
migration motives create coder variability problems? Population, Space, and
Place 15: 79-86.
22. Elo S, Kyngas H (2008) The qualitative content analysis process. J Adv Nurs
62: 107-115.
23. Krippendorf K (2004) Content analysis: an introduction to its methodology.
Sage Publications, Inc, California.
24. Corrigan C, Desnick L, Marshall S, Bentov N, Rosenblatt RA (2011) What can
we learn from first-year medical students’ perceptions of pain in the primary
care setting? Pain Medicine 12: 1216-1222.
25. Vadivelu N, Kombo N, Hines RL (2009) The urgent need for pain management
training. Academic Medicine 84: 408.
26. Breuer B, Pappagallo M, Tai JY, Portenoy RK (2007) U.S. board-certified pain
physician practices: uniformity and census data of their locations. J Pain 8:
244-250.
27. The Mayday Fund Special Committee on Pain and the Practice of medicine
(2009) A call to revolutionize chronic pain care in America: an opportunity in
health care reform.
28. Kuehn BM (2009) Opioid prescriptions soar. JAMA 297: 249-251.
29. Blyth FM, March LM, Brnabic AJ, Cousins MJ (2004) Chronic pain and frequent
use of health care. Pain 111: 51-58.
30. Buckley D, Calvert J, Lapidus J, Morris C (2010) Chronic Opioid therapy and
preventive services in rural primary care: an Oregon rural practice-based
research network study. Ann Fam Med 8: 237-244.
31. Joint Principles for the Medical Education of Physicians as Preparation for
Practice in the Patient-Centered Medical Home (2010).
32. Dobscha SK, Corson K, Perrin NA, Hanson GC, Leibowitz RQ, et al. (2009)
Collaborative care for chronic pain in primary care: a cluster randomized trial.
JAMA 301: 1242-1252.
33. Matthias MS, Bair MJ, Nyland KA, Huffman MA, Stubbs DL, et al. (2010) Self-
managment support and communication from nurse care managers compared
with primary care physicians: a focus group study of patients with chronic
musculoskeletal pain. Pain Manag Nurs 11: 26-34.
34. Bair MJ, Matthias MS, Nyland KA, Huffman MA, Stubbs DL, et al. (2009)
Barriers and facilitators to chronic pain self-management: a qualitative study
of primary care patients with comorbid musculoskeletal pain and depression.
Pain Med 10: 1280-1290.
35. Wiedemer NL, Harden PS, Arndt IO, Gallagher RM (2007) The opioid renewal
clinic: a primary care, managed approach to opioid therapy in chronic pain
patients at risk for substance abuse. Pain Med 8: 573-584.
36. Bair MJ, Robinson RL, Katon W, Kroenke K (2003) Depression and Pain
Comorbidity: A Literature Review. Arch Intern Med 163: 2433-2445.
37. Arnow BA, Hunkeler Em, Blasey CM, Lee J, Constantino MJ, et al. (2006)
Comorbid depression, chronic pain , and disability in primary care. Psychosom
Med 68: 262-268.
38. Kroenke K, Bair MJ, Damush TM, Wu J, Hoke S, et al. ( 2009) Optimized
antidepressant therapy and pain self-management in primary care patients
with depression and musculoskeletal pain: a randomized controlled trial. JAMA
301: 2099-2110.
39. Kroenke K, Bair M, Damush T, Hoke S, Nicholas G, et al. (2007) Stepped Care
for Affective Disorders and Musculoskeletal Pain (SCAMP) study: design and
practical implications of an intervention for comorbid pain and depression. Gen
Hosp Psychiat 29: 506-517.
40. Frantsve LM, Kerns RD (2007) Patient–provider interactions in the management
of chronic pain: current findings within the context of shared medical decision
making. Pain Med 8: 25-35.
41. Parsons S, Harding G, Breen A, Foster N, Pincus T, et al. (2007) The Influence
of patients’ and primary care practitioners’ beliefs and expectations about
chronic musculoskeletal pain on the process of care: a systematic review of
qualitative studies. Clinical J Pain 23: 91-98.
42. Banja JD (2008) Toward a more empathic relationship in pain medicine. Pain
Med 9: 1125-1129.
43. Gallagher RM (2006) Empathy: a timeless skill for the pain medicine toolbox.
Pain Med 7: 213-214.
44. Sullivan MD, Leigh J, Gaster B (2006) Brief report: training internists in shared
decision making about chronic opioid treatment for noncancer pain. J Gen
Intern Med 21: 360-362.
45. Murinson BB, Nenortas E, Mayer RS, Mezei L, Kozachik S, et al. (2011) A
new program in pain medicine for medical students: integrating core curriculum
knowledge with emotional and reflective development. Pain Med 12: 186-195.
46. Martell RD, O’Connor PG, Kerns RD, Becker WC, et al. (2007) Systematic
Review: opioid treatment for chronic back pain: prevalence, efficacy, and
association with addiction. Ann Internal Med 146: 116-127.
47. http://www.painmed.org/patient/facts.html%20.
Qualitative Analysis of Primary Care Providers’ Experiences and Attitudes. J Palliative Care Med S3: 001. doi:10.4172/2165-7386.S3-001
Page 7 of 7
J Palliative Care Med ISSN: 2165-7386 JPCM, an open access jou
Impact of Palliative
Care on Cancer Patients
2. Kroenke K (2003) Patients presenting with somatic complaints: epidemiology,
psychiatric comorbidity and management. Int J Methods Psychiatr Res 12: 34-
43.
3. Breuer B, Cruciani R, Portenoy RK (2010) Pain management by primary care
physicians, pain physicians, chiropractors, and acupuncturists: a national
survey. South Med J 103: 738-747.
4. Kerns RD, Otis J, Rosenberg R, Reid MC (2003) Veterans’ reports of pain and
associations with ratings of health, health-risk behaviors, affective distress, and
use of the healthcare system. J Rehabil Res Dev 40: 371-379.
5. Haskell SG, Heapy A, Reid MC, Papas RK, Kerns RD (2006) The Prevalence
and age-related characteristics of pain in a sample of women veterans receiving
primary care. J Womens Health (Larchmit) 15: 862-869.
6. Crosby FE, Colestro J, Ventura MR, Graham K (2006) Survey of pain among
veterans in Western New York. Pain Manag Nurs 7: 12-22.
7. Haskell SG, Ning Y, Krebs E, Goulet J, Mattocks K, et al. (2012) The prevalence
of painful musculoskeletal conditions in female and male veterans in 7 years
after return from deployment in Operation Enduring Freedom/Operation Iraqi
Freedom. Clin J Pain 28: 163-167.
8. Veterans Health Administration (2009) VHA Directive 2009-053: Pain
Management. Washington, DC: Department of Veterans Affairs.
9. Dubois MY, Gallagher RM, Lippe PM (2009) Pain Medicine Position Paper.
Pain Med 10: 972-1000.
10. Hutchinson K, Moreland AM, de C Williams AC, Weinman J, Horne R (2007)
Exploring beliefs and practice of opioid prescribing for persistent non-cancer
pain by general practitioners. Eur J Pain 11:93-98.
11. Potter M, Schafer S, Gonzalez-Mendez E, Gjeltema K, Lopez A, et al. (2001)
Opioids for chronic nonmalignant pain. Attitudes and practices of primary care
physicians in the UCSF/Stanford collaborative research network. J Fam Pract
50: 145-151.
12. Nwokeji ED, Rascati KL, Brown CM, Eisenberg A (2007) Influences of attitudes
on family physicians’ willingness to prescribe long-acting opioid analgesics for
patients with chronic nonmalignant pain. Clin Ther: 2589-2602.
13. Bhamb B, Brown D, Hariharan J, Anderson J, Balousek S, et al. (2006) Survey
of select practice behaviors by primary care physicians on the use of opioids for
chronic pain. Curr Med Opin 9: 1859-1865.
14. Turk DC, Brody MC, Okifuji EA (1994) Physicians’ attitudes and practices
regarding the long-term prescribing of opioids for non-cancer pain. Pain 59:
201-208.
15. Dobscha SK, Corson K, Flores JA, Tansill EC, Gerrity MS ( 2008) Veterans
Affairs primary care clinicians’ attitudes toward chronic pain and correlates of
opioid prescribing rates. Pain Med 9: 564-571.
16. Upshur CC, Luckmann RS, Savageau JA (2006) Primary care provider
concerns about management of chronic pain in community clinic populations. J
Gen Intern Med 21: 652-655.
17. Barry DT, Irwin KS, Jones ES, Becker WC, Tetrault JM, et al. (2010) Opioids,
chronic pain, and addiction in primary care. J Pain 11: 1442-1445.
18. Ponte CD, Johnson-Tribino J ( 2005) Attitudes and knowledge about pain: an
assessment of West Virginia family physicians. Fam Med 37: 477-480.
19. Leverence RR, Williams RL, Potter M, Fernald D, Unverzagt M, et al. (2011)
Chronic non-cancer pain: a siren for primary care--a report from the PRImary
Care MultiEthnic Network ( PRIME Net). J Am Board Fam Med 24: 551-561.
20. Matthias MS, Parpart AL, Nyland KA, Huffman MA, Stubbs DL, et al. (2010)
The patient-provider relationship in chronic pain care: provider’s perspectives.
Pain Med 11: 1688-1697.
21. Niedomysl T, Malmberg B (2009) Do open-ended survey questions on
migration motives create coder variability problems? Population, Space, and
Place 15: 79-86.
22. Elo S, Kyngas H (2008) The qualitative content analysis process. J Adv Nurs
62: 107-115.
23. Krippendorf K (2004) Content analysis: an introduction to its methodology.
Sage Publications, Inc, California.
24. Corrigan C, Desnick L, Marshall S, Bentov N, Rosenblatt RA (2011) What can
we learn from first-year medical students’ perceptions of pain in the primary
care setting? Pain Medicine 12: 1216-1222.
25. Vadivelu N, Kombo N, Hines RL (2009) The urgent need for pain management
training. Academic Medicine 84: 408.
26. Breuer B, Pappagallo M, Tai JY, Portenoy RK (2007) U.S. board-certified pain
physician practices: uniformity and census data of their locations. J Pain 8:
244-250.
27. The Mayday Fund Special Committee on Pain and the Practice of medicine
(2009) A call to revolutionize chronic pain care in America: an opportunity in
health care reform.
28. Kuehn BM (2009) Opioid prescriptions soar. JAMA 297: 249-251.
29. Blyth FM, March LM, Brnabic AJ, Cousins MJ (2004) Chronic pain and frequent
use of health care. Pain 111: 51-58.
30. Buckley D, Calvert J, Lapidus J, Morris C (2010) Chronic Opioid therapy and
preventive services in rural primary care: an Oregon rural practice-based
research network study. Ann Fam Med 8: 237-244.
31. Joint Principles for the Medical Education of Physicians as Preparation for
Practice in the Patient-Centered Medical Home (2010).
32. Dobscha SK, Corson K, Perrin NA, Hanson GC, Leibowitz RQ, et al. (2009)
Collaborative care for chronic pain in primary care: a cluster randomized trial.
JAMA 301: 1242-1252.
33. Matthias MS, Bair MJ, Nyland KA, Huffman MA, Stubbs DL, et al. (2010) Self-
managment support and communication from nurse care managers compared
with primary care physicians: a focus group study of patients with chronic
musculoskeletal pain. Pain Manag Nurs 11: 26-34.
34. Bair MJ, Matthias MS, Nyland KA, Huffman MA, Stubbs DL, et al. (2009)
Barriers and facilitators to chronic pain self-management: a qualitative study
of primary care patients with comorbid musculoskeletal pain and depression.
Pain Med 10: 1280-1290.
35. Wiedemer NL, Harden PS, Arndt IO, Gallagher RM (2007) The opioid renewal
clinic: a primary care, managed approach to opioid therapy in chronic pain
patients at risk for substance abuse. Pain Med 8: 573-584.
36. Bair MJ, Robinson RL, Katon W, Kroenke K (2003) Depression and Pain
Comorbidity: A Literature Review. Arch Intern Med 163: 2433-2445.
37. Arnow BA, Hunkeler Em, Blasey CM, Lee J, Constantino MJ, et al. (2006)
Comorbid depression, chronic pain , and disability in primary care. Psychosom
Med 68: 262-268.
38. Kroenke K, Bair MJ, Damush TM, Wu J, Hoke S, et al. ( 2009) Optimized
antidepressant therapy and pain self-management in primary care patients
with depression and musculoskeletal pain: a randomized controlled trial. JAMA
301: 2099-2110.
39. Kroenke K, Bair M, Damush T, Hoke S, Nicholas G, et al. (2007) Stepped Care
for Affective Disorders and Musculoskeletal Pain (SCAMP) study: design and
practical implications of an intervention for comorbid pain and depression. Gen
Hosp Psychiat 29: 506-517.
40. Frantsve LM, Kerns RD (2007) Patient–provider interactions in the management
of chronic pain: current findings within the context of shared medical decision
making. Pain Med 8: 25-35.
41. Parsons S, Harding G, Breen A, Foster N, Pincus T, et al. (2007) The Influence
of patients’ and primary care practitioners’ beliefs and expectations about
chronic musculoskeletal pain on the process of care: a systematic review of
qualitative studies. Clinical J Pain 23: 91-98.
42. Banja JD (2008) Toward a more empathic relationship in pain medicine. Pain
Med 9: 1125-1129.
43. Gallagher RM (2006) Empathy: a timeless skill for the pain medicine toolbox.
Pain Med 7: 213-214.
44. Sullivan MD, Leigh J, Gaster B (2006) Brief report: training internists in shared
decision making about chronic opioid treatment for noncancer pain. J Gen
Intern Med 21: 360-362.
45. Murinson BB, Nenortas E, Mayer RS, Mezei L, Kozachik S, et al. (2011) A
new program in pain medicine for medical students: integrating core curriculum
knowledge with emotional and reflective development. Pain Med 12: 186-195.
46. Martell RD, O’Connor PG, Kerns RD, Becker WC, et al. (2007) Systematic
Review: opioid treatment for chronic back pain: prevalence, efficacy, and
association with addiction. Ann Internal Med 146: 116-127.
47. http://www.painmed.org/patient/facts.html%20.
1 out of 7



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.