Biochemistry: Analysis of Blood Transfusion, Grouping and Reactions
VerifiedAdded on 2021/04/21
|25
|3894
|169
Homework Assignment
AI Summary
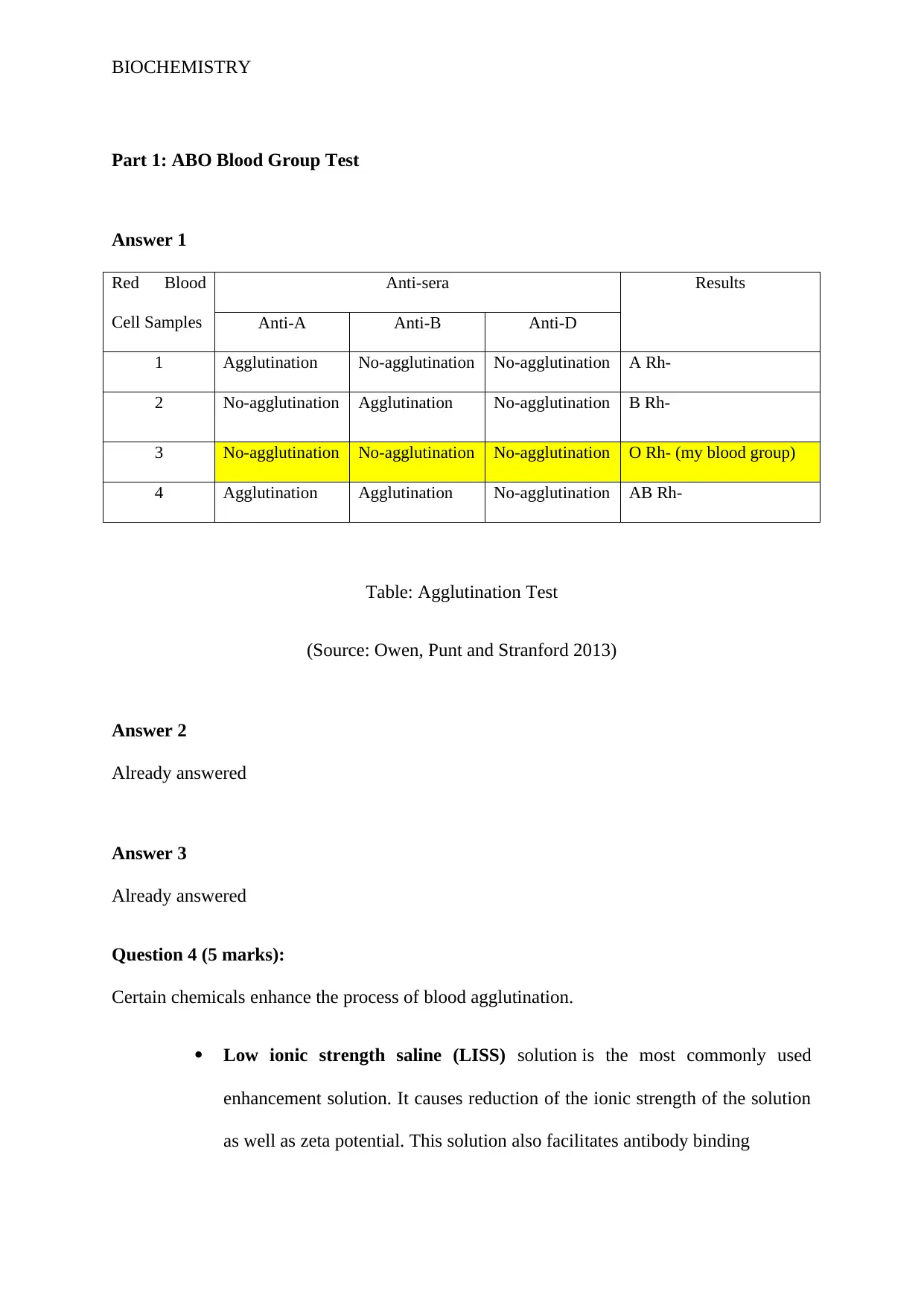
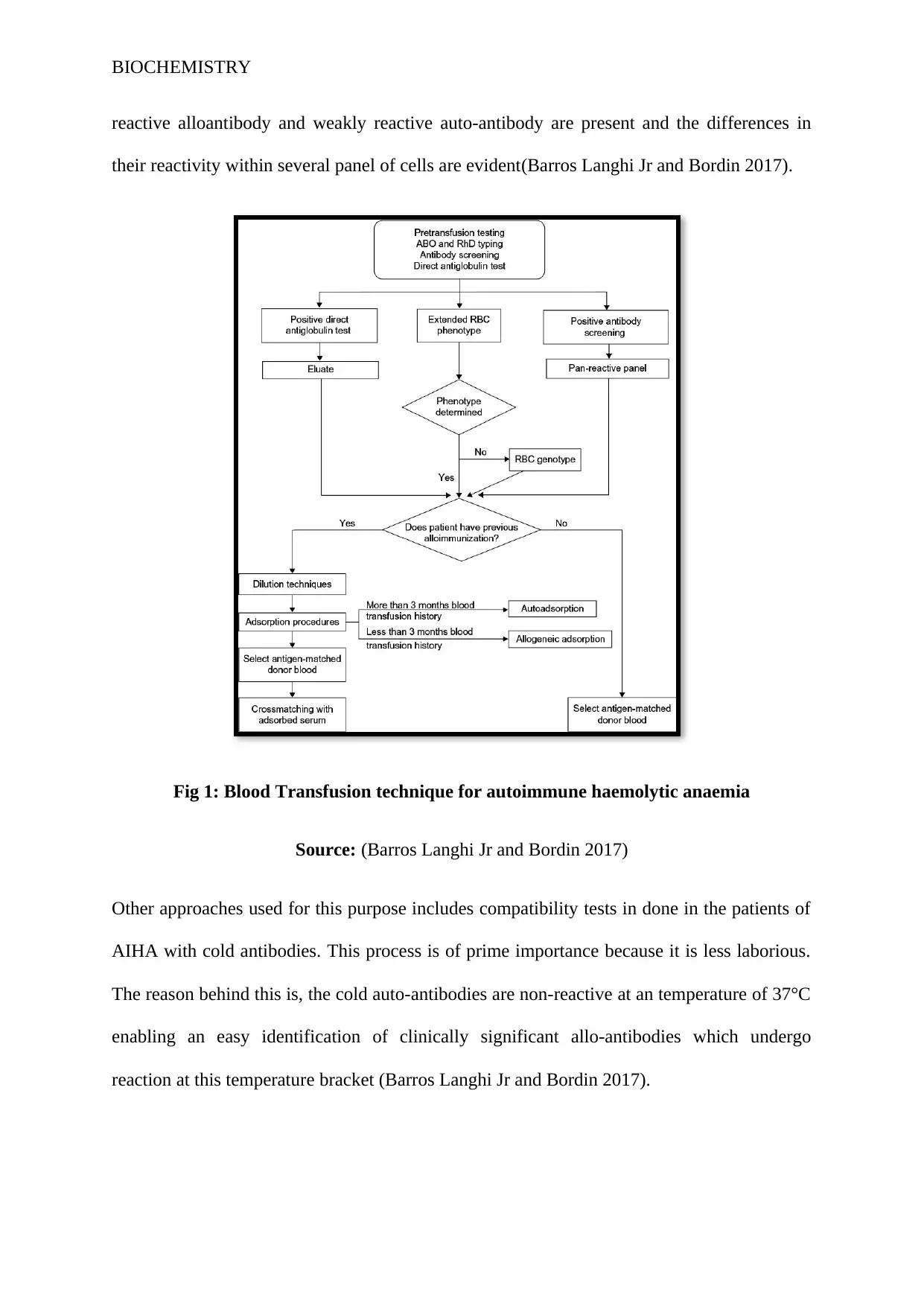
This biochemistry assignment comprehensively explores blood grouping and transfusion. It begins with an analysis of ABO blood group testing, including agglutination results and the use of enhancement solutions like LISS and PEG. The assignment delves into the causes of false positive and false negative results in ABO blood grouping, such as Rouleaux formation and inadequate antibody ratios. It then discusses the role of antisera in blood grouping, including color coding conventions and preservation methods. The assignment also covers the management of patients with autoimmune hemolytic anemia (AIHA) and the challenges in finding compatible blood, along with the different techniques used for compatibility testing. Furthermore, it details the clinical symptoms of mismatched blood transfusions, such as fever, back pain, and potential complications affecting organs. The assignment also addresses transfusion-related acute lung injury (TRALI) and other transfusion reactions, outlining their detection, investigation, and management. Finally, the assignment analyzes antibody screening and the importance of matching blood groups before transfusion, emphasizing the clinical significance of various antibodies and the potential for haemolytic reactions. References are provided throughout the document.



1 out of 25
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.